STRESS INCONTINENCE. GENUINE STRESS INCONTINENCE: Involuntary leakage of urine associated with...
38
STRESS STRESS INCONTINENCE INCONTINENCE
-
Upload
chloe-james -
Category
Documents
-
view
219 -
download
0
Transcript of STRESS INCONTINENCE. GENUINE STRESS INCONTINENCE: Involuntary leakage of urine associated with...

STRESSSTRESS INCONTINENCE INCONTINENCE
GENUINE STRESS GENUINE STRESS INCONTINENCE:INCONTINENCE:
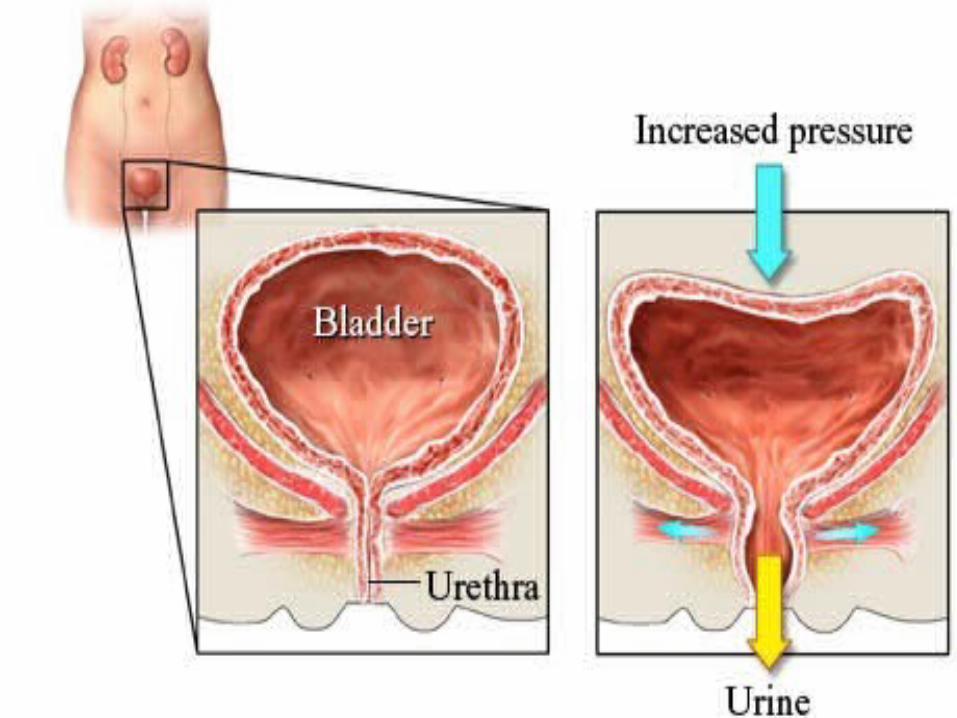
Involuntary leakage of urine associated with Involuntary leakage of urine associated with stressful activity like coughing,sneezing,straining stressful activity like coughing,sneezing,straining or other physical activity in the absence of or other physical activity in the absence of detrusor contraction which she finds socially & detrusor contraction which she finds socially & hygienically unacceptable.hygienically unacceptable.
URGE INCONTENANCEURGE INCONTENANCE::Maintained by urethral closure pressure –Maintained by urethral closure pressure –Intravesical pressure minus intraurethral pressure.Intravesical pressure minus intraurethral pressure.
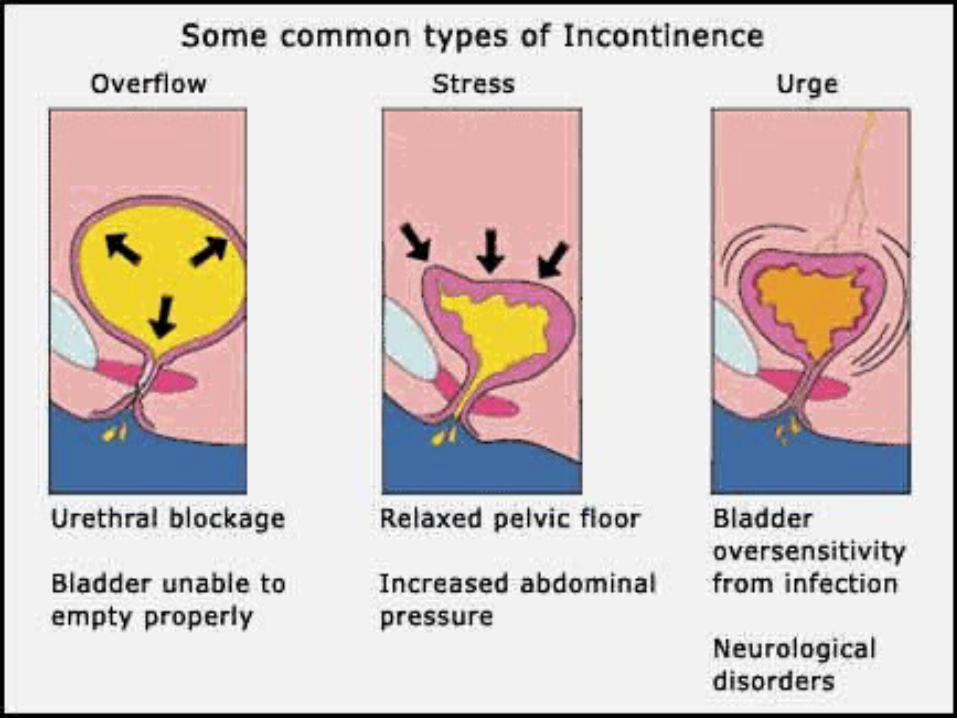
involuntary urine loss may follow a strong involuntary urine loss may follow a strong desire & need to void.Mainly due to detrussor desire & need to void.Mainly due to detrussor muscle overactivity.muscle overactivity.
UNCONSCIOUS INCONTINENCEUNCONSCIOUS INCONTINENCE::
No awareness of urinary leak.Results No awareness of urinary leak.Results from neuropathic bladder due to retension from neuropathic bladder due to retension of urine & overflow.of urine & overflow.
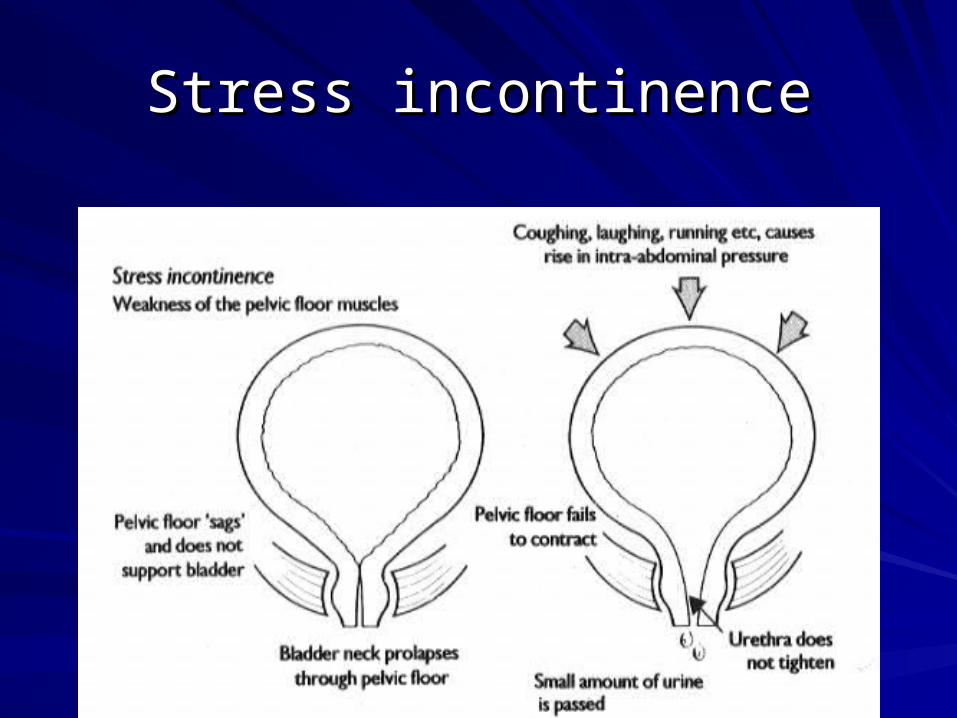
Stress incontinenceStress incontinence
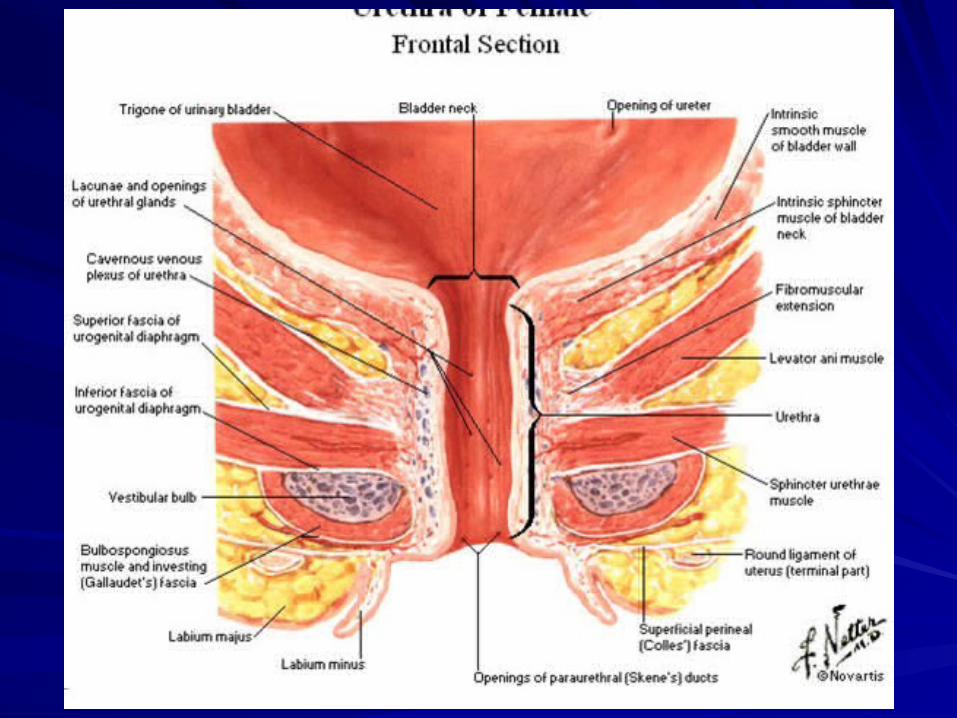
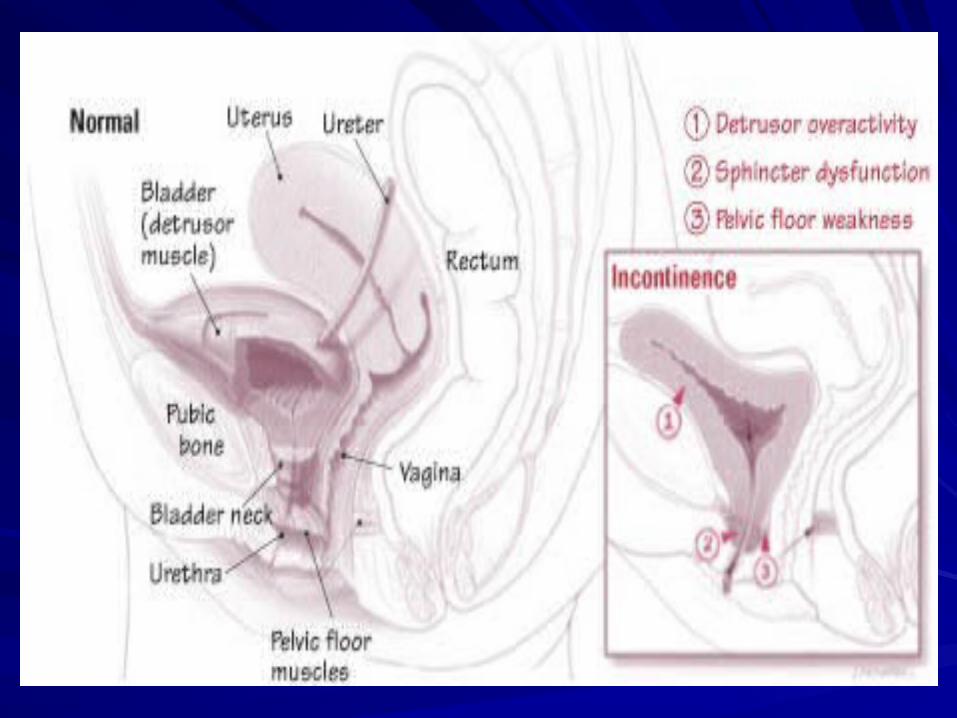
Mechanism:Mechanism:
Depends mainly on internal spincter at the neck Depends mainly on internal spincter at the neck of the bladder.of the bladder.
Normally 20cm of water ; when urethrovesical Normally 20cm of water ; when urethrovesical angle is >100 degrees.angle is >100 degrees.
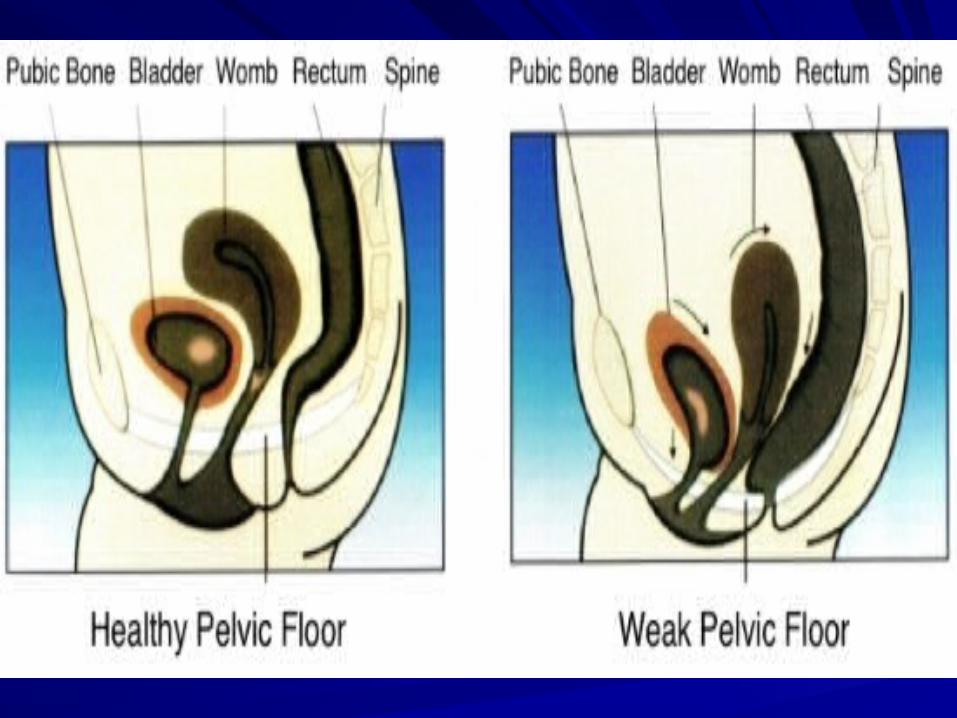
-when upper urethra & bladder neck remain -when upper urethra & bladder neck remain above levator muscles.above levator muscles.
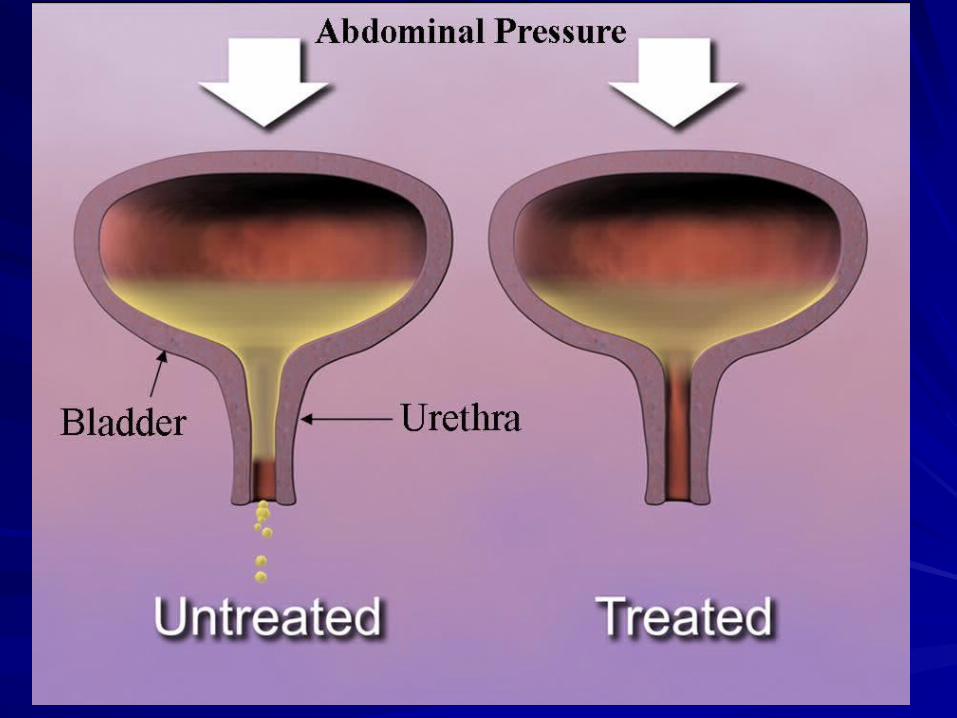
-when abdominal pressure is transmitted -when abdominal pressure is transmitted equally to the bladder & urethra.equally to the bladder & urethra.
Atony or damage to pudental nerve during vaginal Atony or damage to pudental nerve during vaginal delivery.delivery.
Bladder neck descends below the levator ani Bladder neck descends below the levator ani muscles.muscles.
Urethro-vesical angle is lost.Urethro-vesical angle is lost.
Abdominal pressure transmitted only to bladder.Abdominal pressure transmitted only to bladder.
Reducing urethral closure pressure.Reducing urethral closure pressure.
URINARY INCONTINENCEURINARY INCONTINENCE
Contributing Factors:Contributing Factors:
Vascular plexus as well as longitudinal fibres of Vascular plexus as well as longitudinal fibres of urethra maintain tone during filling phase.urethra maintain tone during filling phase.
2100ps of smooth muscle(lissospincter) one 2100ps of smooth muscle(lissospincter) one pulls spincter anteriorly & the other posteriorly pulls spincter anteriorly & the other posteriorly maintaining urethrovesical angle.maintaining urethrovesical angle.
Tone of levator muscles.Tone of levator muscles.
Pudental nerve.Pudental nerve.
Pubovaginal fascia.Pubovaginal fascia.
MANAGEMENT:MANAGEMENT:
Primary clinical evaluation:Primary clinical evaluation:Detailed historyDetailed history::
-Menopausal obese women with previous -Menopausal obese women with previous vaginal deliveries.vaginal deliveries.
-Complains of passage of single spurt of urine -Complains of passage of single spurt of urine at the height of physical exertion.at the height of physical exertion.
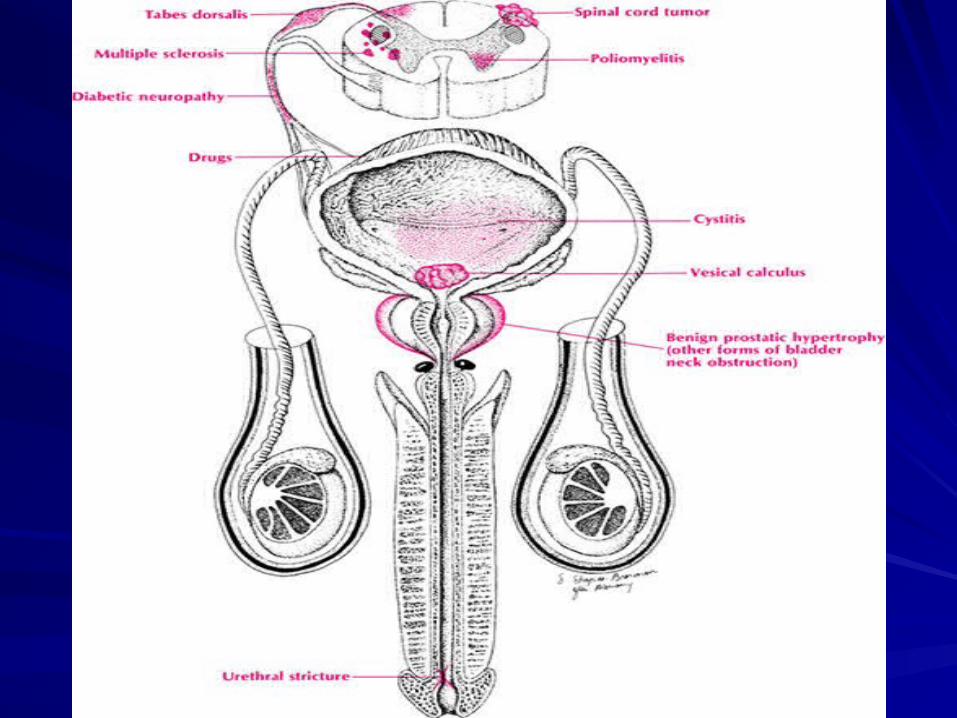
-Rule out local pathology of bladder & urethra.-Rule out local pathology of bladder & urethra. -Rule out organic neurological diseases -Rule out organic neurological diseases
Eg:Multiple sclerosis,tabes dorsalis etc.Eg:Multiple sclerosis,tabes dorsalis etc. -Major pelvic dissection on uterus or rectum.-Major pelvic dissection on uterus or rectum.
Physical examination:Physical examination:
Pelvic & speculum examination.Pelvic & speculum examination.
Thorough neurological acessment.Thorough neurological acessment.
Pelvic supports & tone of levator muscles.Pelvic supports & tone of levator muscles.
Urethral urethrovesical junction mobility.Urethral urethrovesical junction mobility.
Acess senile vaginal changes.Acess senile vaginal changes.
INVESTIGATIONS:INVESTIGATIONS:
STRESS TESTSTRESS TEST::
Patient voids urinePatient voids urineBladder cathetorisedBladder cathetorisedResidual urine sent for cultureResidual urine sent for culture250ml of saline water instilled into bladder250ml of saline water instilled into bladderPatient squats on preweighed absorbent Patient squats on preweighed absorbent padpadAsked to cough or strainAsked to cough or strain
Urine leak notedUrine leak noted
Patient strained in lithotomy positionPatient strained in lithotomy position
Absorbent pad weighed:Net weight Absorbent pad weighed:Net weight gain>2gms –indicative of GSIgain>2gms –indicative of GSI
COTTON SWAB STICK TESTCOTTON SWAB STICK TEST;;
Initially cotton swab will be parallel to the Initially cotton swab will be parallel to the floor.floor.
No GSI:Angle of swab stick<10-15degreesNo GSI:Angle of swab stick<10-15degrees
GSI:>20degrees commonly50-70degreesGSI:>20degrees commonly50-70degrees
MARSHALL & BONNEY’S TEST: MARSHALL & BONNEY’S TEST: In patient with positive stress test absence of In patient with positive stress test absence of leakage of urine on bladder neck elevation leakage of urine on bladder neck elevation indicative of beneficial outcome following indicative of beneficial outcome following surgery.surgery.
BONNEY’s test:Two fingers are placed in vagina BONNEY’s test:Two fingers are placed in vagina & urethrovesical angle elevated.& urethrovesical angle elevated.
MARSHALL’s test:Bladder neck elevated with MARSHALL’s test:Bladder neck elevated with open allis clamp.On straining absence of open allis clamp.On straining absence of leakage of urine indicates POSITIVE TEST.leakage of urine indicates POSITIVE TEST.
URETHROSCOPY:URETHROSCOPY:
Information about opening pressure & Information about opening pressure & urethrovesical angle.urethrovesical angle.
Rule out urethritis,diverticulae,rigid urethra.Rule out urethritis,diverticulae,rigid urethra.
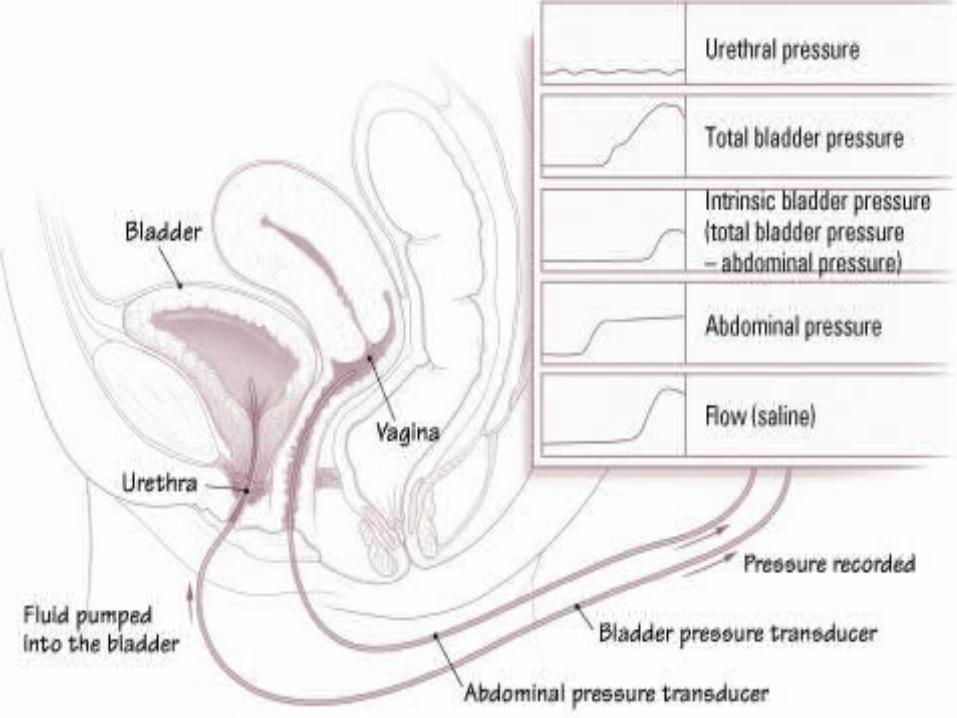
URODYNAMIC EVALUATION:URODYNAMIC EVALUATION:
CYSTOSCOPY:measures pressure in CYSTOSCOPY:measures pressure in bladder & urethra during artificial filling bladder & urethra during artificial filling with CO2 or fluid.with CO2 or fluid.URETHROCYSTOMETRY:URETHROCYSTOMETRY:
-Normally:At rest-150ml urine causes 2--Normally:At rest-150ml urine causes 2-8cm water pressure.8cm water pressure.
-Urethral pressure average 40cm water -Urethral pressure average 40cm water leads to incontinence.leads to incontinence.
UROFLOWMETRY:UROFLOWMETRY:MICTURITIONCYSTURETHROGRAPHY:MICTURITIONCYSTURETHROGRAPHY:Normally 100degrees well marked posterior Normally 100degrees well marked posterior urethrovesical angle is noted.urethrovesical angle is noted.Loss of this angle – stress incontinence.Loss of this angle – stress incontinence.UROPROFILOMETRY:Measures dynamic UROPROFILOMETRY:Measures dynamic urethral pressures.urethral pressures.
-diagnoses urethral instability & diverticulum.-diagnoses urethral instability & diverticulum. -GOLD STANDARD in diagnosis of GSI.-GOLD STANDARD in diagnosis of GSI.
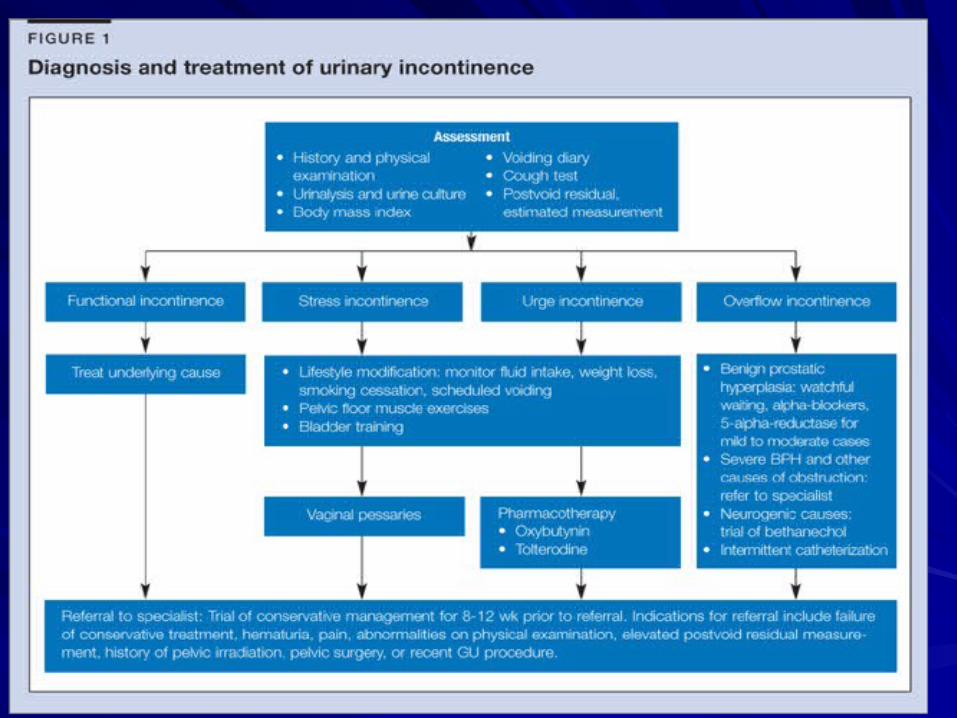
TREATMENT:Conservative & TREATMENT:Conservative & Surgical repair.Surgical repair.
CONSERVATIVE:1CONSERVATIVE:1STST line especially in line especially in
1)younger women1)younger women
2)elderly & frail women unfit for 2)elderly & frail women unfit for surgery.surgery.
3)during 6months after surgery3)during 6months after surgery
4)previous failed surgery4)previous failed surgery
5)detrussor instability5)detrussor instability

1)PHYSIOTHERAPY:pelvic floor exercises for 1)PHYSIOTHERAPY:pelvic floor exercises for 4months with or without electrical 4months with or without electrical stimulation.weight loss & exercise.stimulation.weight loss & exercise.2)DRUGS:alpha adrenergic drugs – constrict 2)DRUGS:alpha adrenergic drugs – constrict bladder neck –decrease frequency of stress bladder neck –decrease frequency of stress incontinence.incontinence.3)INTRAURETHRAL & VAGINAL DEVICES:3)INTRAURETHRAL & VAGINAL DEVICES:4)ELECTRICAL STIMULATION to pelvic floor 4)ELECTRICAL STIMULATION to pelvic floor muscles.muscles.
5)ARTIFICIAL URINARY SPINCTER:in 5)ARTIFICIAL URINARY SPINCTER:in neurological conditions & previous surgical neurological conditions & previous surgical failure.failure.
GENUINE STRESS GENUINE STRESS INCONTINENCE:postmenopausal women with INCONTINENCE:postmenopausal women with senile changes in vagina-oestrogen replacement senile changes in vagina-oestrogen replacement therapy or local oestrogen cream.therapy or local oestrogen cream.
-treat chronic cough,constipation & allergic -treat chronic cough,constipation & allergic rhinitis.rhinitis.
Vaginal operations:Vaginal operations:
Anterior colporraphyAnterior colporraphyKELLEY’S REPAIR:Anterior colporraphy KELLEY’S REPAIR:Anterior colporraphy with plication of bladder neckwith plication of bladder neckPACEY’S REPAIR:apposing medial fibres PACEY’S REPAIR:apposing medial fibres of puborectalis muscle in midline under of puborectalis muscle in midline under bladder neck. ABDOMINAL bladder neck. ABDOMINAL OPERATIONSOPERATIONS
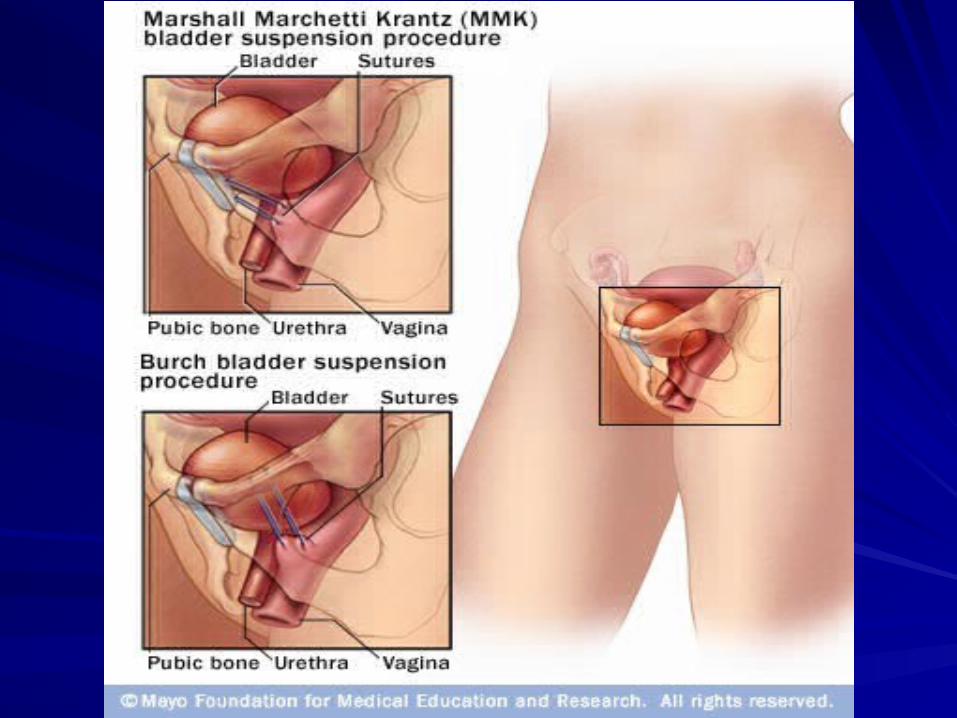
Abdominal operations:Abdominal operations:
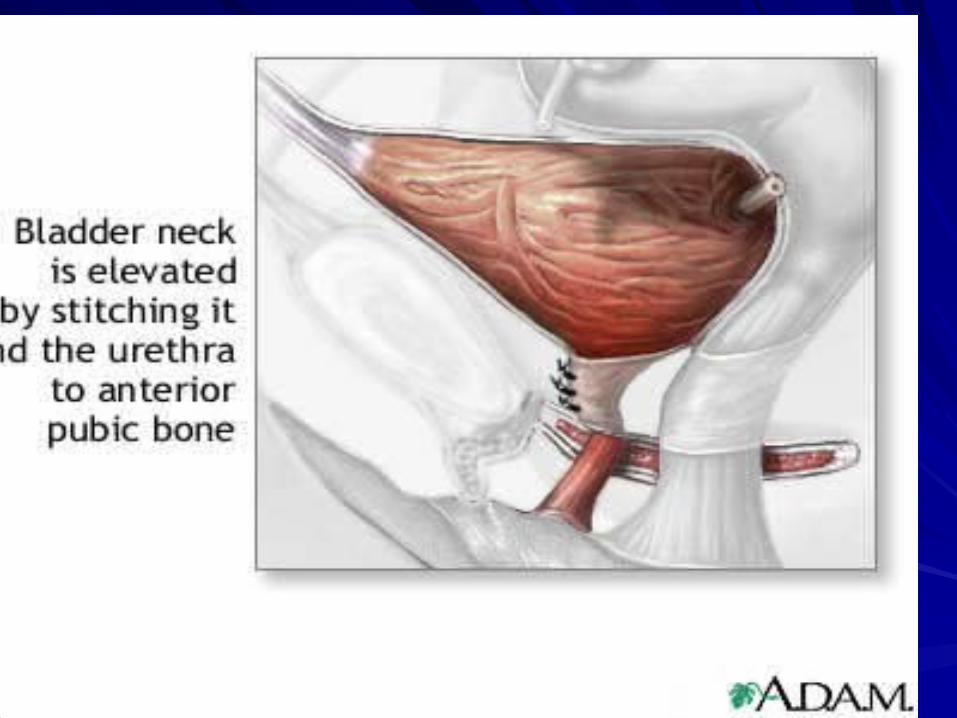
MARSHALL-MARCHETTI-KRANZ MARSHALL-MARCHETTI-KRANZ OPERATION:sutures bladder neck & OPERATION:sutures bladder neck & vaginal vault to periosteum of pubic vaginal vault to periosteum of pubic symphysis back.symphysis back.
BURCH COLPOSUSPENSION:vaginal BURCH COLPOSUSPENSION:vaginal suspension using ileopectineal ligament.suspension using ileopectineal ligament.
Combined abdominal & vaginal:Combined abdominal & vaginal:
PEREYRA OPERATIONPEREYRA OPERATION
LAPROSCOPIC COLPOSUSPENSIONLAPROSCOPIC COLPOSUSPENSION
INTRAVESICAL BLADDER NECK PLICATIONINTRAVESICAL BLADDER NECK PLICATION
PERIURETHRAL COLLAGEN INJECTIONPERIURETHRAL COLLAGEN INJECTION
Complications of surgeryComplications of surgery
Injury to bladder & urethra.Injury to bladder & urethra.Retropubic space haematoma.Retropubic space haematoma.Infection.Infection.Breakdown of sutures.Breakdown of sutures.Voiding difficulties,retension.Voiding difficulties,retension.Erosion of non-absorbable sutures into Erosion of non-absorbable sutures into bladder,urethra or vagina-fistula, bladder,urethra or vagina-fistula, infection,stone formation.infection,stone formation.