Strategies for Enhancing Proprioception and Neuromuscular ... · 78 Hewett et al and Related...
19
76 CLINICAL ORTHOPAEDICS AND RELATED RESEARCH Number 402, pp. 76–94 © 2002 Lippincott Williams & Wilkins, Inc. Proprioception and neuromuscular control of the knee are compromised after ligament injury and must be regained if the athlete is to return to high level sports at a normal injury risk level. The anterior cruciate ligament deficient and re- constructed knee will be used as a model to de- scribe differences in proprioception and neuro- muscular control to those of an uninjured knee. The purpose of the current review is threefold. First, the basic science of proprioception and neuromuscular control specific to the knee will be summarized and reviewed. The review will in- clude an overview of terminology, neurophysiol- ogy, and the effects of injury on the function of both lower limbs. Second, tools used for assess- ment and rehabilitation of proprioceptive deficits will be evaluated. Specific rehabilitation proce- dures that incorporate prophylactic condition- ing that focus on transitioning the injured athlete back into sport will be presented. Finally, the lit- erature with respect to gender variation in pro- prioception and neuromuscular control will be evaluated. The goal of the current review is to provide the clinician and the clinical scientist with sufficient background information for the development of quantitative methods to evaluate a patient’s functional capacity and to assist in preventative, preoperative, and postoperative decision-making strategies. Basic Science of Proprioception and Neuromuscular Control of the Knee Defining Proprioception The task of defining proprioception is one that has been attempted previously and has created controversy in the scientific community. 33 Ini- tially, definitions such as “the ability to receive input from muscles, tendons and joints and process information in a meaningful way in the central nervous system,” and “assists in the knowledge of where a limb is in space,” pre- vailed in the literature. 33 Controversy contin- ues to prevail because a universally accepted definition remains to be formulated. This in- ability to generate an acceptable, all-encom- passing definition on the terms proprioception and neuromuscular control, show the com- plexity of the topic and the difficulty in pro- ceeding with valid and reliable research. 33 Sherrington 51 first described propriocep- tion in 1906 in his classic contribution to the literature regarding nervous system function. Difficulty in the direct interpretation of his writing has led to significant confusion in the scientific community. 33 However, for the cur- rent review, a working definition of proprio- ception based on a paraphrase of Sherrington’s Strategies for Enhancing Proprioception and Neuromuscular Control of the Knee Timothy E. Hewett, PhD; Mark V. Paterno, MS, PT, ATC; and Gregory D. Myer, MS From the Cincinnati Children’s Sports Medicine Biody- namics Center and The Human Performance Laboratory, The Children’s Hospital Research Foundation, Cincin- nati, OH. Reprint requests to Timothy E. Hewett, PhD, Cincinnati Children’s Sports Medicine Biodynamics Center, 3333 Burnet Avenue, MLC 10001, Cincinnati, OH 45229-3039. DOI: 10.1097/01.blo.0000026962.51742.99
Transcript of Strategies for Enhancing Proprioception and Neuromuscular ... · 78 Hewett et al and Related...

76
CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 402, pp. 76–94© 2002 Lippincott Williams & Wilkins, Inc.
Proprioception and neuromuscular control ofthe knee are compromised after ligament injuryand must be regained if the athlete is to return tohigh level sports at a normal injury risk level.The anterior cruciate ligament deficient and re-constructed knee will be used as a model to de-scribe differences in proprioception and neuro-muscular control to those of an uninjured knee.The purpose of the current review is threefold.First, the basic science of proprioception andneuromuscular control specific to the knee willbe summarized and reviewed. The review will in-clude an overview of terminology, neurophysiol-ogy, and the effects of injury on the function ofboth lower limbs. Second, tools used for assess-ment and rehabilitation of proprioceptive deficitswill be evaluated. Specific rehabilitation proce-dures that incorporate prophylactic condition-ing that focus on transitioning the injured athleteback into sport will be presented. Finally, the lit-erature with respect to gender variation in pro-prioception and neuromuscular control will beevaluated. The goal of the current review is toprovide the clinician and the clinical scientistwith sufficient background information for thedevelopment of quantitative methods to evaluatea patient’s functional capacity and to assist in
preventative, preoperative, and postoperativedecision-making strategies.
Basic Science of Proprioception andNeuromuscular Control of the KneeDefining Proprioception
The task of defining proprioception is one thathas been attempted previously and has createdcontroversy in the scientific community.33 Ini-tially, definitions such as “the ability to receiveinput from muscles, tendons and joints andprocess information in a meaningful way inthe central nervous system,” and “assists in theknowledge of where a limb is in space,” pre-vailed in the literature.33 Controversy contin-ues to prevail because a universally accepteddefinition remains to be formulated. This in-ability to generate an acceptable, all-encom-passing definition on the terms proprioceptionand neuromuscular control, show the com-plexity of the topic and the difficulty in pro-ceeding with valid and reliable research.33
Sherrington51 first described propriocep-tion in 1906 in his classic contribution to theliterature regarding nervous system function.Difficulty in the direct interpretation of hiswriting has led to significant confusion in thescientific community.33 However, for the cur-rent review, a working definition of proprio-ception based on a paraphrase of Sherrington’s
Strategies for Enhancing Proprioceptionand Neuromuscular Control of the Knee
Timothy E. Hewett, PhD; Mark V. Paterno, MS, PT, ATC; and Gregory D. Myer, MS
From the Cincinnati Children’s Sports Medicine Biody-namics Center and The Human Performance Laboratory,The Children’s Hospital Research Foundation, Cincin-nati, OH.Reprint requests to Timothy E. Hewett, PhD, CincinnatiChildren’s Sports Medicine Biodynamics Center, 3333Burnet Avenue, MLC 10001, Cincinnati, OH 45229-3039.DOI: 10.1097/01.blo.0000026962.51742.99

Number 402September, 2002 Enhancing Control of the Knee 77
early work will be used as the standard defini-tion. Sherrington defined proprioception as theculmination of all neural inputs originatingfrom joints, tendons, muscles, and associateddeep tissue proprioceptors. These inputs areprojected to the central nervous system for pro-cessing and ultimately result in the regulationof reflexes and motor control. This definitionviews proprioception primarily as a sensory ac-tivity, occurring along the afferent pathway.More recently, the definition of the propriocep-tive system has been expanded to include the
complex interaction between the sensory path-ways and the motor pathway (efferent system).This system has come to be known as the sen-sorimotor system.33
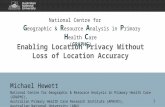
Neurophysiology of Proprioception andNeuromuscular Control of the JointWhen a proprioceptive stimulus is presented tothe body, input occurs at three separate loca-tions, including the visual system, the vestibularsystem, and the peripheral mechanoreceptors(Fig 1). These peripheral mechanoreceptors are
Fig 1. A flow chart of lower limb dy-namic neuromuscular response to sen-sory receptor input is shown.

located in various locations throughout thebody including skin, joints, ligaments, ten-dons, and muscles. The role of the mechanore-ceptors is that of a “transducer to convert me-chanical energy of a new action potential.”3
Basically, the mechanoreceptor is a special-ized nerve plexus serving a mechanical role toprovide position sense and conscious aware-ness by initiating reflexes to stabilize jointsand avoid injury. Previous studies all substan-tiate the role of mechanoreceptors in variousjoint structures as acceptors of informationfrom the environment for processing by thecentral nervous system.28,29,47,48
After the acceptance of the input, the mes-sage then is transferred to the central nervoussystem and is processed at one of three levels.Reaction at the spinal level is a reflex re-sponse. This represents a fast response that isnecessary for protective reflexive joint stabi-lization. This also helps mediate movementfrom higher levels of the central nervous sys-tem. The second level of motor control is viathe lower brain (basal ganglia, brainstem, andcerebellum). This area acts as a way station forcommand from higher levels. It also is in-volved in the timing of motor activities, learn-ing of planned movements, and control ofcomplex movement patterns of a sustainedand repetitive nature. Finally, processing canoccur at the cerebral level, where there is con-trol of voluntary movement. After the process-ing of information a motor response occurs.This represents the slowest neural response be-cause of the presence of multiple synapses andincreased distance of impulse propagation.34
The anterior cruciate ligament deficient kneeprovides clinical researchers with an excellentmodel to study neural signaling and proprio-ceptive deficits in the knee. Currently, it iswell-established that injury to the anterior cru-ciate ligament results in mechanical instabilityof the knee.15,17,20,41,42,49 Deficiency of the an-terior cruciate ligament often is associated withgiving-way in patients returning to activitiesrequiring cutting, twisting, acceleration anddeceleration maneuvers, often despite rehabil-itation after injury, rendering them function-
ally unstable.15,41,42,49 The rule of thirds sug-gests that 1⁄3 of all patients with anterior cruci-ate ligament deficiency are unable to return toactivities of daily living because of instability,1⁄3 can function with recurrent instability dur-ing activities of daily living but cannot resumesports activities, and the final 1⁄3 can resumesports activities without experiencing recur-rent instability.42 Snyder-Mackler et al53 alsohave shown a lack of correlation between an-terior cruciate ligament insufficiency and func-tional instability in a select group of athletes.They describe patients with increased jointlaxity and functional stability as copers andpatients with increased joint laxity and func-tional instability as non-copers. Surgeons of-ten recommend anterior cruciate ligament re-construction to patients who desire to return tohigh levels of activity. However, even after sta-tic mechanical stability is restored surgicallythrough anterior cruciate ligament reconstruc-tion, the patient may continue to experiencefunctional instability (giving-way episodes orperceived instability) during dynamic activity.These findings show the complex nature ofjoint stability.4,19,43
Several authors have studied the hypothesisthat mechanical stability does not guaranteefunctional stability, and have suggested evi-dence that the anterior cruciate ligament has asensory and proprioceptive function, in additionto its role as a static stabilizer.28,29,47,48 Anatomicand histologic studies have shown a rich neuro-logic innervation and the presence of specificproprioceptive mechanoreceptors in the fibersof the anterior cruciate ligament.16,28,29,47,48
These studies have helped validate the presenceof proprioceptive mechanoreceptors and showtheir role in the afferent pathways of the senso-rimotor system. A study by Pitman et al44 mea-sured somatosensory evoked potential record-ings in the cerebral cortex after stimulation ofthe anterior cruciate ligament. They found evi-dence of proprioceptive receptors within thefibers of the intact anterior cruciate ligament inhumans and the presence of cerebral activity af-ter stimulation, validating the successful trans-mission of this message. Finally, other studies
Clinical Orthopaedics78 Hewett et al and Related Research

have explored the modulation of muscle activ-ity after stress is placed on the anterior cruciateligament.37,46,54 These authors reported that co-incident with forced increases in anterior tibialtranslation, muscle responses were observed.Specifically, increases in hamstring activationand inhibition of quadriceps activity were re-ported. Therefore, a motor response to a propri-oceptive stimulus and a complete sensorimotorloop is complete via the sensorimotor system.
Assessment of Proprioceptive andNeuromuscular Control of the KneeVarious methods have been developed to at-tempt to assess the proprioceptive and neuro-muscular control of the joint. Assessment ofjoint position sense was one of the first meth-ods used to determine a patient’s propriocep-tive aptitude. This method involves the settingof the limb at a certain, predetermined angleand then asking the subject to reproduce theangle, measuring the deviation from the previ-ous angle. Although this is an easy test to ex-ecute clinically, it has been criticized for itshigh measurement variability and inherent lackof reliability. In addition, it only analyzes aportion of proprioception, joint position sense,and fails to take into account joint kinesthe-sia.7 A second method that is used to assessproprioception is threshold to perception ofpassive movement.7 This testing method eval-uates the patient’s ability to detect movementin the limb. The patient’s limb is placed at acertain angle and the patient is blinded to itslocation. The limb then is moved passively ata very slow speed, typically. 0.5� per second.The subject is asked to tell the tester when mo-tion in the limb is first detected and the mea-surement of distance traveled between thetime motion started to the time motion was de-tected by the subject then is recorded. This hasbeen found to be a fairly reliable assessmenttool for measuring proprioception, however, itfails to assess any characteristics of joint posi-tion sense, because it solely assesses kines-thetic awareness.7
A third method to assess proprioceptionand neuromuscular control includes the mea-
surement of muscle activation and latency ofmuscular reflexes after a stimulus. This methodhas been used frequently in the study of the pa-tient with anterior cruciate ligament deficiency.Anterior tibial translation force is applied andreactive hamstring latency is measured.54,60 Fi-nally, the use of balance assessment and sta-bilometry can be used to assess postural controland inferences can be made to proprioceptivecapabilities and neuromuscular control. Theneed to assess proprioceptive ability and neuro-muscular control accurately is widely acceptedin the scientific community; however, there isgreat disagreement to the most appropriate andaccurate means of accomplishing that task.Beynnon et al7 summarized it well with theirconclusion that “the importance of propriocep-tion as a clinical outcome measure is well rec-ognized, but the best measurement techniquehas yet to be determined.”
Proprioceptive Deficits in the Patient withan Anterior Cruciate Ligament DeficiencyDeficits in conscious, voluntary knee kines-thesia and proprioception after anterior cruci-ate ligament rupture have been reported inseveral studies.3–5,14,16,38,60 Independently, theseauthors studied the proprioceptive capacity ofsubjects with anterior cruciate ligament defi-ciency. The methodology varied significantlyamong these studies with respect to the meansof proprioceptive assessment, ranging fromactive and passive repositioning to thresholdto detection of passive movement. For exam-ple, Barrack et al3 studied the threshold for de-tection of passive motion in 11 athletes withanterior cruciate ligament deficiencies. Theyfound a significantly higher mean thresholdvalue that was indicative of a proprioceptivedeficit. Wojtys and Huston60 studied muscle tim-ing and recruitment after forced anterior tibialtranslation in athletes with anterior cruciateligament deficiency. These authors found sig-nificant changes in muscle timing and recruit-ment after anterior cruciate ligament rupture.These studies were able to incorporate assess-ment, not only of the afferent pathway, butalso the efferent response, and to achieve a
Number 402September, 2002 Enhancing Control of the Knee 79

more complete examination of the sensorimo-tor system. Although the methodology varied,the results of these studies consistently showedproprioceptive deficits in the subjects with an-terior cruciate ligament deficiency.
Timing of Proprioceptive Return AfterAnterior Cruciate LigamentReconstructionThe return of proprioceptive function after an-terior cruciate ligament reconstruction has beenreported.4,13,19 Studies by Co et al13 and Harri-son et al19 evaluated the proprioceptive abilityof patients with anterior cruciate ligament re-constructed knees. Independently, these au-thors concluded that the proprioceptive abilityof the reconstructed knee was equal to that ofcontrols. Co et al13 assessed proprioceptionthrough the use of reproduction of passive mo-tion, relative reproduction of joint position, andthreshold to detection of passive motion, in ad-dition to measuring the vertical component ofheel strike force during gait. Harrison et al19
measured proprioception through the use ofsingle leg stance and postural sway and con-cluded that anterior cruciate ligament recon-structed knees were equal to controls. Barrett4reported that proprioceptive ability (as assessedby the perception of passive motion) improvedafter anterior cruciate ligament reconstruction.In addition, Barrett4 showed that functional out-come was highly correlated with propriocep-tive measures in the patient who had anteriorcruciate ligament reconstruction. Conversely, astudy by MacDonald et al35 using threshold toperception of passive motion, found no im-provement in proprioceptive function after thereconstruction. Therefore, controversy existsregarding the timing and return of propriocep-tive function of the anterior cruciate ligamentreconstruction.
From a clinical standpoint, attempts to as-sess functional stability often are inconclusive.After anterior cruciate ligament reconstructionand restoration of mechanical stability, the goalis to maximize functional stability and returnthe patient to his or her preinjury level of activ-ity. Return of a patient to high level sports be-
fore functional stability has been achieved maylead to a new injury or failure of the recon-struction. No reliable method for the objectivedetermination of functional stability of thelower extremity currently is available. The de-cision to return the patient to unrestricted activ-ity usually is based on a combination of musclestrength measurements, functional tests, andtime from surgery. Use of quadriceps and ham-string strength measurements alone as criteriafor return to sports has been shown to be an in-adequate assessment, because patients can havefunctional instability even when strength hasreturned.32,39 In addition, it has been reportedthat commonly used functional performancetests using one-legged hopping and jumpingmaneuvers have low sensitivity for detectingfunctional limitations.2 In separate studies,Tegner et al55 and Barber et al2 found that anunacceptably high proportion of patients whoseknees were functionally unstable had normallimb symmetry scores on one-legged hop tests.Noyes et al39 reported that only 50% of patientswith anterior cruciate ligament deficiency hadabnormal limb symmetry on a single-leg hoptest and 62% had abnormal limb symmetry ontwo tests. Lephart et al32 reported on three func-tional performance tests designed to predictfunctional recovery (carioca maneuver, shuttlerun, and cocontraction semicircular maneuver).The mean functional score differences betweenpatients with an anterior cruciate ligament defi-ciency and healthy subjects were significantlydifferent, however, the variability among thepatients with instability was large enough tocategorize a significant percentage of the pa-tients with anterior cruciate ligament deficiencyas being healthy.32 Therefore, the criteria cur-rently used to return patients to full functionmay not accurately assess their functional sta-bility and their ability to return to their highestfunctional level.
Co et al13 studied 10 subjects with anteriorcruciate ligament reconstruction at an averageof 32 months postoperative to assess proprio-ception and neuromuscular control status afteranterior cruciate ligament reconstruction. Theyused three joint proprioception tests that in-
Clinical Orthopaedics80 Hewett et al and Related Research

cluded reproduction of passive motion, rela-tive reproduction, and threshold to detectionof passive motion. They found the anteriorcruciate ligament reconstructed limb to be es-sentially equal to the contralateral limb and acontrol group in proprioceptive function. Har-rison et al19 examined 17 patients with anteriorcruciate ligament reconstruction and com-pared them with a control group. Patients were10 to 18 months postoperative. Functional sta-bility was determined through subjective scor-ing by two physical therapists during single-leg stance with the patient’s eyes open andclosed. Postural sway was measured on a forceplate. The authors found no significant differ-ence in balance measures between involvedand noninvolved limbs; however, the authorsstated that the usefulness of single-leg stand-ing balance for anterior cruciate ligament re-constructed knees at 10 to 18 months postop-eratively is questionable because of the patientbeing too functionally advanced for thesemeasurements to detect variation betweenlimbs. The studies by Co et al13 and Harrisonet al19 show no significant difference betweenthe anterior cruciate ligament reconstructedknee and the noninvolved limb. However, thesubjects were studied at a minimum of 10months postoperatively.
Patients with anterior cruciate ligament re-construction have significant deficits in single-leg balance at 6 months and greater postoper-ative.24 At 6 months postoperative, the patientwith anterior cruciate ligament reconstructioncontinues to have significant proprioceptivedeficits (Fig 2). This finding is important whenconsidering aggressive anterior cruciate liga-ment rehabilitation protocols, which advocatereturn to twisting and rotational sports as earlyas 3 to 4 months postoperatively.50 If proprio-ceptive deficits continue to exist at this point,regardless of strength and range of motion(ROM), clinicians may be subjecting their ath-letes to a high risk of graft failure or reinjury.
Bilaterality of Proprioceptive DeficitsSignificant postural balance deficits may existin the involved and uninvolved limb of pa-
tients with anterior cruciate ligament defi-ciency. Hewett et al24 reported that the pri-mary single-leg balance abnormality was inthe sagittal plane in these patients. In addition,similar deficits were present in the involvedand uninvolved limb. This deficit persisted inthe involved limb up to 1 year postoperatively(Fig 3). This finding of balance deficits in theinvolved limb after anterior cruciate ligamentinjury and after anterior cruciate ligament re-construction is not unique. Other studies havesuggested similar findings of proprioceptive
Number 402September, 2002 Enhancing Control of the Knee 81
Fig 2. The mean postural instability in the ante-rior cruciate ligament (ACL)-deficient limb of sub-jects preoperative and 3, 6, 9, and 12 monthspostoperative compared with age and gender-matched control subjects is shown.
Fig 3. The mean postural instability in the nonin-volved contralateral limb of subjects with anteriorcruciate ligament (ACL) deficiency preoperativeand 3, 6, 9, and 12 months postoperative com-pared with age and gender-matched control sub-jects is shown.

deficits in the anterior cruciate ligament defi-cient knee.3–5,14,16,38,60
Proprioceptive deficits also have been welldocumented in the noninvolved limb. Corri-gan et al14 found proprioceptive deficits inboth limbs of athletes with unilateral anteriorcruciate ligament deficiency. Their study usedthreshold to perception of passive motion andposition sense to assess proprioception in thesubjects. Friden et al16 also examined patientswith unilateral anterior cruciate ligament defi-ciency and found increased postural sway inthe frontal plane in both lower extremities.Wojtys and Huston60 found deficits in lowerextremity muscle timing and recruitment or-der bilaterally when assessing patients withanterior cruciate ligament deficiency. The re-sults of Hewett et al24 are consistent with thesefindings and raise an interesting question re-garding use of the contralateral limb as a con-trol during proprioceptive testing. These re-sults indicate that clinicians should not use thecontralateral limb as a control when assessingproprioceptive parameters, because deficitssimilar to the involved limb are seen on thenoninvolved side.
Stabilometry as a Measure ofProprioception in the Anterior CruciateLigament Deficient KneeSeveral studies have explored the use of pos-tural balance deficits as a means of assessing apatient’s functional stability.16,24 Postural bal-ance is a complex function that relies on theinterplay of several factors, including proprio-ception, dynamic joint restraints, static jointrestraints, and postural equilibrium. Dynamicjoint restraints are muscle-tendon units thatmaintain limb and joint position and react tochanging loads and forces. Static joint re-straints include ligaments and bony architec-ture that limit joint motion. Postural equilib-rium refers to higher level functions includingvisual and vestibular input. Stabilometry is anobjective and quantitative method for evaluat-ing postural balance.16,19,38,57,59 In the past,stabilometry studies were done on a static forceplate with measurement of body sway in thesagittal plane, coronal plane, or both.16 More
recently, mobile platforms that measure bodysway in two dimensions about a center of pres-sure have been developed.24
Stabilometry first was used in orthopaedicresearch to study instability of the ankle. Troppet al58 showed that stabilometric measures cor-related with functional stability of the ankle, butnot mechanical stability. In addition, these au-thors were able to show that an abnormal sta-bilometric score was predictive of future ankleinjury.57–59 Several authors have shown deficitsin stabilometric score for anterior cruciate defi-cient knees as compared with controls.19,38,61
Mizuta et al38 compared stable and unstablecruciate deficient knees with a control groupand found that the unstable group had signifi-cant stabilometric deficits relative to the othertwo groups. They concluded that stabilometrywas a useful tool for assessment of subjectivefunctional knee stability.
Gender Differences in ProprioceptionA deficit exists in the knowledge base func-tional stability with respect to gender. Fewstudies have examined neuromuscular controldifferences between males and females.23,27
Previous studies have shown that women par-ticipating in jumping and cutting sports have afourfold to sixfold higher incidence of knee in-jury than males.1,27,62 One possibility for thesedifferences with respect to knee injuries may beattributable to deficits in proprioception andneuromuscular control in female athletes.24
Two previous studies by Black et al8 and Hel-lenbrandt and Braun22 have explored posturalsway in healthy subjects and found no differ-ences between genders. Both of these studiestested subjects on stable force platforms. Dif-ferences between gender in postural sway on adynamic platform have not been reported pre-viously. Therefore, an unknown relationshipbetween neuromuscular control and gender ex-ists and needs additional assessment.
Gender Differences in Single-Leg StabilityHewett et al24 examined single-leg stability ofmale control subjects compared with femalecontrol subjects and reported that the femalesubjects had significantly more stability than
Clinical Orthopaedics82 Hewett et al and Related Research

Number 402September, 2002 Enhancing Control of the Knee 83
males on the involved and noninvolved knee(Fig 4). However, in the subjects with an ante-rior cruciate ligament deficiency, the maleshad significantly more stability than the fe-males preoperatively on the involved and non-involved limb.24
In postoperative examination, the males con-tinued to have greater total stability than femaleswith significant differences remaining betweenthese groups at 6 months, at 9 months, and at 12months postoperative (Fig 4). The males’ insta-bility on the involved limb peaked at 3 monthspostoperative, whereas the females had the mostinstability at 6 months postoperative.24
The finding of proprioceptive differencesbetween genders raises important issues. First,females with intact knees have greater single-leg balance than males with intact knees. Thisdifference is presumed to be attributable to thelower center of gravity in female control sub-jects.30 However, after injury to the anteriorcruciate ligament, females seem to experiencegreater deficits in balance than males. In addi-tion, the return of single-leg balance after ante-rior cruciate ligament reconstruction is slowerin females than males. Females have signifi-cantly greater deficits in single-leg balance thanmales after anterior cruciate ligament ruptureand may need more time to recover from ante-
rior cruciate ligament reconstruction to regainfunctional stability and be prepared to return toa maximum level of function. Therefore, re-searchers should group single-leg stability databy gender and analyze the groups separately.These findings also indicate that the clinicianneeds to stress proprioception exercises earlierin the rehabilitation for the female patients toaid in a faster return of proprioceptive abilities.
An important question to consider is whetherfemale subjects with anterior cruciate ligamentrupture possess deficits in balance or posturalcontrol before injury, which creates a predispo-sition to injury or the alternative possibility, thatanterior cruciate ligament injury is more trau-matic to the proprioceptive systems of femalesthan males.24 If the anterior cruciate ligament in-jury in females results in greater proprioceptivedamage, anterior cruciate ligament injury maybe significantly more traumatic to women andthese increased deficits need to be addressed inthe postoperative course of rehabilitation. Thepossibility that females with postural swaydeficits possess a greater propensity to knee in-jury suggests the need for prescreening for sin-gle-leg balance before athletic participation toassess for injury risk.
Proprioceptive and NeuromuscularControl Deficits in the Female AthletesThe alarmingly high incidence of females pre-senting with noncontact knee injuries caused byjumping and cutting sports coupled with thegeometric growth in female participation inthese high risk sports has significantly increasedthe gender gap in the incidence of noncontactknee injury. Hewett et al23 observed three neu-romuscular imbalances, which were termeddynamic neuromuscular imbalance. The firstimbalance is the tendency for females to be lig-ament-dominant. Ligament dominance refers tothe absence of muscle control of mediolateralknee motion that results in high valgus kneetorques and high ground reaction forces. Typi-cally during single-leg landing, pivoting or de-celeration, as often occurs during knee ligamentinjury, the female athlete allows the ground re-action force to control the direction of motionof the lower extremity joints, and the ligament
Fig 4. The mean postural instability grouped bygender for control subjects (CTRL) and the in-volved limb subjects with an anterior cruciate lig-ament deficiency (ACL) who had reconstructionrecorded from an unstable platform is shown. Fe-male control subjects have more stability than malecontrol subjects. Females with anterior cruciate lig-ament deficiency have less stability than male sub-jects with anterior cruciate ligament deficiency.

Clinical Orthopaedics84 Hewett et al and Related Research
to take on a significant percentage of the force.This lack of dynamic muscular control of thejoint leads to high forces and high valgustorques at the knee (Fig 5). The second imbal-ance is termed quadriceps dominance. Withquadriceps dominance, female athletes activatetheir knee extensors preferentially over theirknee flexors during sports movements to stabi-lize their knee, which accentuates and perpetu-ates strength and recruitment imbalances be-tween these muscles. This cycle of quadricepsdominance should be addressed and overcomewith dynamic neuromuscular training. The thirdimbalance is dominant leg dominance. Domi-nant leg dominance is the imbalance betweenmuscular strength and recruitment on oppositelimbs, with the nondominant limb often havingweaker and less coordinated hamstring muscu-lature. During single-leg landing, pivoting or de-celeration, the female athlete may have a lack ofdynamic muscular control of the nondominantknee, which may predispose the knee to injury.23
The enhancement of neuromuscular balanceis an important concept for the development ofany neuromuscular training program. Enhance-ment of balance is important in every plane: the
coronal, the sagittal, and the transverse.23 Theneuromuscular control problem in females ba-sically is an imbalance of three important neu-romuscular parameters. With ligament domi-nance, there exists an imbalance between theneuromuscular and ligamentous control of thejoint. With quadriceps dominance, there is animbalance between quadriceps and knee flexorstrength and coordination. With dominant legdominance, there is an imbalance between thetwo lower extremities in strength and coordina-tion. Therefore, an important neuromuscularreeducation concept is that the trainer or thera-pist must create balance in each of these para-meters. The neuromuscular training program,which was developed to achieve this goal, willbe detailed in the following section.
Clinical Use of Strategies for ImprovingProprioception and Neuromuscular Controlof The Knee: Injury Prevention andPreoperative and Postoperative PlanningPotential for Preparticipation Screening
The assessment of potential injury risk beforesports participation followed by interventionmay decrease the relative injury incidence in
Fig 5A–B. The increased valgus knee motion in (A) the female athlete, compared with (B) the maleathlete when landing from a jump is shown.
A B

athletes.11 The three muscular imbalances de-tailed previously give a framework for prepar-ticipation screening of female athletes that serveas a model for any population prone to injury tothe anterior cruciate ligament. Preparticipationscreening of athletes may be used to identifythose athletes predisposed to knee injury andthose who would benefit from a training pro-gram to enhance strength, proprioception, andneuromuscular stabilization of the knee. Forceplates, optoelectronic digitizing cameras, anddynamometers used by biomedical researchersare not readily accessible to athletic trainers andcoaches. Simple methods to determine whichathletes are at increased risk of injury, which arereadily available to coaches, trainers, and ath-letes might allow for large scale screening forinjury-prone athletes and clearly identify thoseathletes who need preparticipation training. Theknowledge gained from methodologies such asthese could have a major impact on how femaleathletes prepare for sports participation.23
McKeag36 reported that 10% to 12% of ado-lescent athletes have deficiencies during prepar-ticipation testing that may preclude them fromparticipation; these deficiencies include side-to-side strength imbalances, flexibility imbalances,and inadequate conditioning or skill level.Smith and Laskowski52 reported that 4% of ath-letes have musculoskeletal deficits that eitherpreclude them from playing or require referralfor additional evaluation. With the ever-increas-ing popularity of sports such as soccer, volley-ball, basketball, and softball and the rapidly in-creasing number of participants each year, evenhigher numbers of injuries could be avoided inthe future. To participate in high-risk jumpingand cutting sports, athletes may need to be eval-uated and show proficiency in strength, flexibil-ity, and advanced motor skills tests.36 Withouttesting and deficit correction, the increased riskof serious knee injury in female athletes maymaintain its pattern of geometric growth.
Prophylactic Neuromuscular Training forInjury PreventionChandy and Grana11 found that significantlymore female than male high school athletes had
knee injuries that required surgery and sug-gested, “emphasis be placed on functional eval-uation and conditioning of the quadriceps andhamstring muscles to prevent these injuries.”Beck and Wildermuth6 stated that noncontactanterior cruciate ligament injuries are “due tocoordination failure” and involve “a combina-tion of high velocity and momentary loss ofnormal protective muscle support.” Traininghas been shown to increase active knee stabi-lization in the laboratory and decrease the inci-dence of serious knee injury, including anteriorcruciate ligament injury, on the court or field inan athletic population. Training and strengthdifferences may account for only part of the in-creased incidence of knee injury in female ath-letes, but lowering these high figures by even apercentage could have a significant effect onthe number of knee injuries in female athletes.
Caraffa et al10 showed in a prospective con-trolled study that neuromuscular training ofhigh level male soccer players significantlydecreased the incidence of anterior cruciateligament injury. After a progressive five-phasetraining program on balance boards, injury in-cidence decreased more than sevenfold inthese male athletes. Hewett et al27 reported aplyometric and strength training program thatdecreased peak landing forces and valgus andvarus torques at the knee (Fig 6). These au-thors also showed a marked imbalance be-tween hamstrings and quadriceps strength infemale athletes before training. In addition,males had knee flexor moments during land-ing from a jump, which were three times higherthan females. The training program significantlyincreased hamstrings power and strength, in-creased hamstrings to quadriceps peak torqueratios and decreased right to left leg imbal-ances in hamstrings strength. This programalso was tested to determine whether it has asignificant effect on injury rates in athletesduring competition. Female athletes trainedwith the program were three to four times lesslikely to suffer serious knee injuries. The re-sults observed with this program justify the al-teration of current protocols for preparing fe-males for participation in high-risk sports. Such
Number 402September, 2002 Enhancing Control of the Knee 85

training, if effectively implemented on a wide-spread basis, could help to significantly de-crease the number of athletes injured each year.
Hewett et al26 reported the first prospectivestudy of the effects of neuromuscular training(using a plyometric training program) on kneeinjury in the high-risk female sports population.The rate of serious knee injury was 0.43 in un-trained females, 0.12 in trained females, and0.09 in males (injuries per 1000 exposures). Chisquare analysis indicated a significant effect oftraining on group injury rates (Fig 7). Untrainedfemales had a significantly higher incidence ofserious knee injury than trained females andmales. Trained females were not different thanuntrained males. Training resulted in evengreater differences in noncontact injuries be-
Clinical Orthopaedics86 Hewett et al and Related Research
Fig 6A–C. A serial progression of a squat jump maneuver is shown, from (A) squat to (B) spring to (C)jump.
A B C
Fig 7. The relative injury per 1000 player expo-sures in untrained female athletes, trained femaleathletes, and untrained male athletes is shown.

Number 402September, 2002 Enhancing Control of the Knee 87
tween the female groups. This prospectivestudy showed a decreased incidence of seriousknee injury after neuromuscular training in thehigh-risk female sports population.
Clinical Relevance of Preoperative andPostoperative Proprioceptive DeficitsProprioceptive and neuromuscular controldeficits exist after anterior cruciate ligamentrupture and well into the postoperative rehabil-itation period. Clinicians should be aware ofthese deficits and focus rehabilitative interven-tions in these areas. Through the assessment ofpostural balance, Mizuta et al38 compared sub-jective complaints of functional instabilitywith a stabilometric measurement on a forceplate and found an impaired standing balancein the functionally unstable group. They con-cluded stabilometry was a useful method forevaluating functional instability of the knee.However, Mizuta et al38 used a stable forceplate for stability measures rather than a sta-bilometry system with an unstable platform.Balance assessments are general measures ofinputs from multiple variables. Even when ex-perimental protocols attempt to eliminate cer-tain variables such as audio and visual input,testing measures usually are unable to indicatespecifically which variables are abnormal.
Preoperative single-leg stability of subjectswith anterior cruciate ligament deficiency canshow a significant deficit of the involved limband the noninvolved limb when compared withthe control group.24 This significant deficit inboth limbs persisted at 3, 6, and 9 months post-operative (Fig 2). The mean values for the sin-gle-leg stability at 12 months postoperativeshowed significant deficits in the noninvolvedlimb; however, no significant difference wasseen in the involved limb. In addition, when to-tal stability of the subjects’ involved limb ver-sus the noninvolved limb was compared, nosignificant difference was seen preoperatively.
Rehabilitation for RegainingProprioception After Injury and SurgeryProtocols for the anterior cruciate ligament de-ficient and reconstructed knee have been de-veloped and previously described in detail.21
Immediate motion and early, protected weight-bearing now are standard protocols. Rehabili-tation programs should be evaluated based andtailored within the limits of the individual pa-tient. Patients should reach full ROM andweightbearing by 5 to 6 weeks. A running pro-gram should be started at approximately 3 to 4months with a functional program includingcutting and pivoting initiated at 5 to 6 months.Return to high-risk sports should occur be-tween 6 to 9 months.
In the past several years, rehabilitation pro-tocols were published that attempted to outlinethe fastest and most aggressive means to reha-bilitate the patient after anterior cruciate liga-ment reconstruction.5,21,50 When exploring thecurrent literature regarding rehabilitation afteran anterior cruciate ligament reconstruction,there is significant controversy regarding thesafest and most efficient means to rehabilitatethese patients. Because immediate motion wasadvocated after intraarticular anterior cruciateligament reconstruction, clinicians have pushedto accelerate rehabilitation after anterior cruci-ate ligament reconstruction in an attempt to ad-vance the patient to return to sports as quicklyas possible.50
Rehabilitation after anterior cruciate liga-ment reconstruction is a multifaceted task. Pro-tocols for rehabilitation have been developedbased on scientific data and clinical experience,which provides the patient the opportunity toreturn to sports in a rapid time frame withoutcompromising the safety of the patient. Focusshould be placed on decreasing the risk oflong-term complications such as graft failureor laxity, patellofemoral conversion, and lossof motion while considering patient goals andconcomitant injury. Therefore, different proto-cols after anterior cruciate ligament reconstruc-tion have been developed, accelerated and de-layed, and patients can be placed into specificgroups after surgery. Patients are candidates foraccelerated programs unless they possess acomplex avascular meniscus repair, concomi-tant alternate ligament reconstruction, con-comitant patellofemoral realignment proce-dures, and significant articular cartilage lesionsor had revision surgery. These patients are pro-

gressed by the guidelines of a delayed protocol.A detailed description of these rehabilitationprotocols is beyond the scope of the current re-view; however, the progression of the proprio-ception and neuromuscular control componentsof one current anterior cruciate ligament proto-col will be reviewed.21
Training of the proprioceptive and neuro-muscular control systems should begin earlyin the rehabilitation process. In the first weekof Phase I of rehabilitation, simple weightshifting can initiate this process. Weight shift-ing acts as a lead into the initiation of a weight-bearing program. Progression to weightbear-ing can be taught with the aid of a bathroomscale. The patient should be taught to feel theprogression of weight from 25% to 100% withthe feedback of the scale and then be taught topartial weightbear with crutches.21
Proprioception training continues in thesecond phase of the program with the initiationof balance board and stabilometry training.21
The initiation of closed kinetic chain activitiesassists in recruitment of neuromuscular controlof the hamstring musculature. Exercises suchas wall sits, minisquats, and lunges help initi-ate quadriceps and hamstring cocontraction andcan be progressed by adding resistance compo-nents, using unstable surfaces and adding varusand valgus stress. When the patient is able tobear 100% of his or her body weight safely,progression to single-leg standing activitiescan be used to additionally challenge the lowerextremity musculature and recruit the neuro-muscular system for proximal stabilization atthe hip. Finally, the patient should be initiatedon a cup-walking program. This helps retrainthe patient to resume a normal gait pattern byforcing exaggeration of knee and hip flexionduring the swing phase of gait, rather thanhaving a rigid knee, which frequently is com-pensated with hip hiking.21
Phase III incorporates a progression of priorproprioceptive activities to more advancedlevels. Activities such as lateral stepping overcups, 90� rotation steps, and single-leg stand-ing activities using resistance in the unin-volved leg with Theraband, all challenge the
patient to use their sensorimotor system andcompensate for the deficits. Additional chal-lenges to the neuromuscular pathways can beadded through balance perturbations and si-multaneous activities that require use of theupper extremity while executing activities thatrequire the use of the lower extremity. In ad-dition, upper body plyometric tosses whilesingle-leg standing on the involved limb canchallenge the athlete additionally.
Phase IV represents a continued progres-sion of the current proprioceptive activities.Single-leg standing activities are progressedto standing on a trampoline or foam roll. PhaseV incorporates not only a progression of cur-rent proprioception drills but also the initiationof a straight-line running program if certainbaseline criteria with respect to strength andgraft integrity, are met. Additional challengescan be made through the addition of backwardrunning and submaximal effort lateral shuffleand cross over drills.
Phase VI represents a progression to morefunctional, sports-specific activities. Pendingthe successful initiation of the straight-linerunning program and attainment of certainbaseline criteria, cutting and pivoting activi-ties are initiated. These drills should beginwith activities that require less hard cutting,such as figure eight running in a very largearea (20 to 30 yards) at submaximal speed.From this point, increasing speed can advancethe athlete, decreasing the area of the figureeight and the addition of more advanced cut-ting activities. More advanced activities in-clude lateral cutting drills, shuttle runs, andpivoting drills. It is crucial at this time to caterthe cutting drills to the athlete’s goals and hisor her return to sport needs.
Plyometric training also is initiated at thistime. Starting with simple hopping drills, suchas box hops on a soft surface is a good meansto initiate this activity. The athlete then can beadvanced to more aggressive jumping drills.The crucial concept with any plyometric pro-gram is good technique. This serves as a goodintroduction to plyometrics and can introducethe concept of technique perfection. More
Clinical Orthopaedics88 Hewett et al and Related Research

simple jumping drills serve as a lead in to themore advanced plyometric training.
Neuromuscular and ProprioceptivePreparation for Return to SportsSuccessful completion of physical therapy dur-ing the 4- to 6-month postoperative period placesthe athlete in a precarious position. This is thepoint in which they often are released for fullactivity, especially with the advent of acceler-ated rehabilitation. At this point, the athlete isprepared to begin functional proprioceptivetraining in preparation for sport competition,yet is not necessarily ready to begin sports ac-tivities. The physical therapist or athletic trainershould attempt to bridge the gap in the athlete’sperceived and actual sports readiness. The pa-tient must understand that although the recon-struction of the ligament may have created astatically stable joint, the athlete may not havea functionally stable knee during dynamicmovements.31,33 Coordination between active(muscle) and passive (ligament) restraints isrequired to control tibiofemoral motion andcreate a dynamically stable knee. The passivemechanical function of the anterior cruciateligament graft must be complimented with neu-romuscular afferent input that increases jointposition sense and reflex stabilization of theknee through proper efferent response. A dy-namically stable knee is the product of intactsoft tissue restraints and an appropriately func-tioning proprioceptive system.31 Although thedefinitions of proprioception may vary, its rolein creating a dynamically stable joint and theimportance of its development during rehabili-tation of the athlete is accepted universally. Aprogressive, functional rehabilitation programis required to provide the athlete with an effec-tive means for facilitating positive adaptationsto the proprioceptive function of the knee.Functional neuromuscular and proprioceptivetraining should provide the athlete with a dy-namically functional joint that is prepared to re-spond to the extreme forces generated duringathletic competition, reducing the risk of rein-jury and optimally preparing the athlete toachieve preinjury performance levels.18
Functional neuromuscular and propriocep-tive training may be defined as movementtraining progressions that facilitate the devel-opment of multijoint neuromuscular engramsthat combine joint stabilization, acceleration,deceleration and kinesthesia through intermit-tent protocols that progress from low intensitymovements focused in a single plane to multi-planar power training. Functional neuromuscu-lar and proprioceptive training must incorporatean appropriate balance between developing theproprioceptive abilities of the athlete and a ex-posing the athlete to a contraindicated move-ment that puts them in pain or at risk of injury.Introduction of this type of training in the reha-bilitation program may create acute soreness;however, the trainer should use discretion as tothe appropriate intensity and progression of ex-ercises. Proper training progression should takethe athlete through a combination of high-riskmaneuvers in a controlled situation. This type ofproprioceptive stress may aid the developmentof spinal reflexes that more quickly and effec-tively stabilize the joint than the voluntary mus-cular movements that require an afferent-effer-ent pathway and cerebral input. This voluntarymuscle response may be too slow to manage theground reaction forces induced from the highrisk maneuvers encountered during competitiveplay.9,31 Functional proprioceptive training canincrease the speed and efficiency of motor re-sponses through the creation of motor engramsthat bring functional activities from cerebral tobrain stem level control. The goal of the func-tional proprioceptive training is to bring the ath-lete to a level of athletic skill and ability equal tothe preinjury state, especially in females and allpatients with anterior cruciate ligament recon-structed knees.
Development of Functional Dynamic BalanceThe first level of proficiency that must be at-tained before return to sports participation isthe ability of the injured knee to maintain bal-ance and stability. Adequate groundwork fordynamic stability proficiency should be estab-lished through postoperative rehabilitation.
Number 402September, 2002 Enhancing Control of the Knee 89

Stabilometry is a tool that can be used to assessthe athlete’s single-leg balance aptitude. Fe-males have a greater loss of single-leg posturalbalance when returning from a knee injurywhen compared with males. They also will re-turn to their preinjury state slower than theirmale counterparts.24 Therefore, progressionthrough the early stages of sports reentry maybe delayed for female athletes. A standard levelof proficiency in postural balance before returnto sport is important to protect athletes fromreinjuring the affected joint. Tropp et al56 re-ported that athletes who could not accomplishpostural balance within two standard deviationsof normal had a significantly higher risk of in-jury. Increased proficiency in bipedal and sin-gle-leg balance can be gained through balanceboard training. Training progressions shouldbegin with patients early in physical therapywith balance board activities with the athlete ina bipedal stance and progress to single-leg drillsin more advanced phases. Early goals are tohave the patient maintain stance on the boardregardless of ability to control board position.As balance improves the athlete should moveto a more flexed athletic position and shouldmaintain stance on the board with greater con-trol of movement. The trainer should encouragethe athlete to bring visual focus away from hisor her feet and incorporate ball drills that pro-vide a distraction from the balance task (Fig 8).The balance board training provides an effec-tive method for programming the neuromuscu-lar system to send afferent unbalanced stanceinformation, provide the efferent response, andthen process the difference between actualmovement and the intended movement. Thisprocess of neural recognition and muscular re-sponse helps develop motor engrams that workto correct future motor control errors. The bal-ance board training will provide hundreds ofsuch engramming opportunities per exercisebout.31 Improvement of an athlete’s posturalbalance should decrease risk of reinjury. Troppet al56 were able to reduce injury rates in ath-letes returning to sport from prior injury with 10weeks of balance board training. Another pro-gressive balance board protocol significantly
reduced knee injuries in elite soccer players.10
Several authors advocate the use of balanceboard proprioceptive training well past theacute postsurgical rehabilitation phase, not onlyfor restoration of functionality, but for its pro-phylactic effect on ligament reinjury.10,24,56
Development of FunctionalNeuromuscular and ProprioceptiveSymmetryA secondary proficiency level that must be as-sessed early in functional proprioceptive train-
Clinical Orthopaedics90 Hewett et al and Related Research
Fig 8. A balance board drill used in dynamicneuromuscular analysis training for enhancingcore body control and dynamic knee stability.

ing is the athlete’s ability to achieve symmet-ric bipedal gait. Proficient walking gait shouldhave been established previously, althoughrunning gait may not have been corrected tothe preinjury form. A running gait retrainingprogram improves symmetry of lower extrem-ity musculature contribution, which may pre-vent abnormal loading of the ligaments andsoft tissue and increase strength and enduranceduring sports competition.25 Gait retraining isdone best on a treadmill in front of a mirror toprovide simultaneous visual and verbal trainerfeedback to the athlete. An early goal in gaitretraining is to normalize ROM in the in-volved and the noninvolved limbs.40 The in-volved limb often has limited joint ROM, es-pecially at the hip. Incline treadmill runningcan increase ROM across all joints, but espe-cially at the hip. Care should be taken to mon-itor the athlete for signs of patellofemoral painand address this issue as it arises. Backwardsincline training (Fig 9) also should be used toincrease ROM and to increase quadricepsfunctional strength while simultaneously re-ducing patellofemoral stress.12 The ability ofinclined backwards training to increase func-tional quadriceps strength and limit patello-femoral stress was shown by Snyder-Macklerand coauthors,53 who reported increased func-tional gait with improved quadriceps strengthafter the use of inclined backwards treadmilltraining. In addition to the ROM and strengthbenefits from this training, the athlete may cre-ate neuromuscular engrams that will proveuseful when their sport requires backward lo-comotion. Once the athlete has increased lowerextremity joint ROM to normal levels and hasattained lower extremity symmetry, treadmillspeeds can be increased to assess the athlete’ssprinting form. Sprinting will continue to im-prove ROM, especially at the hip and the ankle.Attention should be directed toward obtain-ing a normal rhythmic stride. An unbalancedsprinting rhythm is indicative of an unbal-anced limb contribution and is most evidentthrough the audible monitoring of foot con-tact. If the athlete presents with this problemof unbalanced sprinting gait, the contributing
factors are likely either pain or limited ROMin the involved leg. If patellofemoral pain anddecreased joint ROM are determined to be thelimiting factors, then increased backwardsrunning may assist the athlete through thisprogression12 Pain-free symmetric sprintinggait should be the ultimate goal of this profi-ciency level.
Simultaneous gait retraining and a progres-sive plyometric program teaches the athlete toproperly initiate, control, and decelerate groundreaction forces that he or she will encounter incompetitive play when jumping, landing, andcutting. Special attention should be directed to-ward the female athlete, because she often isligament dominant.23 Ligament dominance re-sults in high knee valgus moments and highground reaction forces.27 During single-leglanding, pivoting, or deceleration, the motion offemale athlete’s knee typically is directed by
Number 402September, 2002 Enhancing Control of the Knee 91
Fig 9. This photograph shows backward treadmillrunning for the athlete attempting to return to sports.

the ground reaction force, rather than by theathlete’s musculature. To correct ligamentdominance in female athletes, a neuromusculartraining program must be designed to teach theathlete to control dynamic knee motion in thecoronal (valgus and varus) plane. One conceptthat the athlete is taught is that the knee is a sin-gle-plane hinge, not a ball and socket joint.Reeducation of the female neuromuscular sys-tem away from multiplanar motion of the kneeto dynamic control of knee motion in the sagit-tal plane alone can be achieved through a pro-gression of plyometric exercises.23 Initially, thephysical therapist or other rehabilitation spe-cialist should choose movements that allow theathlete to gain proper joint kinesthesia duringjumping and landing. Correction of ligamentdominance must be accomplished through heavyfocus on proper form and technique. Jumpingand landing technique should be evaluated crit-ically by the trainer or therapist and constantfeedback should be given to the athlete in amanner similar to that given when teaching aspecific skill required for sport.45 Verbal feed-back such as soft-silent landing, straight as anarrow, land light as a feather, and touch and gois repeated to promote proper technique. Re-programming the neuromuscular system in fe-males requires significant interaction betweentherapist or trainer and athlete, because the ther-apist or trainer must be diligent to provide suf-ficient feedback to develop permanent neuro-muscular programs.
What We Have LearnedAt least five important conclusions can bemade from this review of the literature with re-spect to the loss and return of proprioceptionafter ligament rupture and reconstruction andthe assessment of proprioception before andafter ligament injury and during the rehabilita-tion process. First, after anterior cruciate liga-ment reconstruction, patients continue to havedeficits in proprioception and neuromuscularjoint control at least 6 months and for as muchas 1 year postoperatively and in some casesbeyond 1 year when compared with a controlgroup. Second, patients with anterior cruciate
ligament deficiency have impaired proprio-ception and neuromuscular control of the kneein the involved and noninvolved limbs whencompared with a control group. Third, whenassessing proprioception and neuromuscularcontrol of patients with either anterior cruciateligament deficiency or after reconstruction,the contralateral limb may not be a suitablecontrol because of the bilateral deficits. Fourth,it is important to incorporate beginning, inter-mediate, and advanced proprioceptive trainingexercises throughout the postoperative reha-bilitation protocol. Finally, females with ante-rior cruciate ligament deficient knees and afteranterior cruciate ligament reconstruction pos-sess greater deficits in proprioception and neu-romuscular control of the knee and possiblymore functional instability than their malecounterparts.
Future Research ChallengesDetermination of the functional instability of apatient with an anterior cruciate ligament defi-cient knee is a problem that has challenged re-searchers and clinicians for decades. Previousstudies have established that anterior cruciateligament deficiency results in mechanical in-stability; however, functional instability inthese patients is significantly more difficult todetermine. Therefore, the challenge presentedto researchers and clinicians is to determinemeans of assessment, diagnosis, prescreeningfor functional instability in patients and ath-letes and to enhance rehabilitation and pro-phylactic intervention protocols. A final chal-lenge is to determine precisely how long aftersurgical reconstruction functional deficits ex-ist in these populations.
References1. Arendt E, Dick R: Knee injury patterns among men
and women in collegiate basketball and soccer:NCAA data and review of literature. Am J SportsMed 23:694–701, 1995.
2. Barber SD, Noyes FR, Mangine RE, et al: Quantita-tive assessment of functional limitations in normaland anterior cruciate ligament-deficient knees. ClinOrthop 255:204–214, 1990.
3. Barrack RL, Skinner HB, Buckley SL: Propriocep-tion in the anterior cruciate deficient knee. Am JSports Med 17:1–6, 1989.
Clinical Orthopaedics92 Hewett et al and Related Research

4. Barrett DS: Proprioception and function after ante-rior cruciate reconstruction. J Bone Joint Surg73B:833–837, 1991.
5. Beard DJ, Dodd CAF, Trundle HR, SimpsonAHRW: Proprioception enhancement for anteriorcruciate ligament deficiency: A prospective random-ized trial of two physiotherapy regimes. J Bone JointSurg 76B:654–659, 1994.
6. Beck JL, Wildermuth BP: The female athlete’s knee.Clin Sports Med 4:345–366, 1985.
7. Beynnon BD, Renstrom PA, Konradsen L, et al: Val-idation of Techniques to Measure Knee Propriocep-tion. In Lephart SM, Fu FH (eds). Proprioception andNeuromuscular Control in Joint Stability. Cham-paigne, IL, Human Kinetics 127–138, 2000.
8. Black FO, Wall C, Roucette HE, Kitch R: Normalsubject postural sway during the Romberg test. AmJ Otolaryngol 3:309–318, 1982.
9. Brand RA: Knee ligaments: A new view. J BiomechEng 108:106–110, 1986.
10. Caraffa A, Cerulli G, Projetti M, et al: Prevention ofanterior cruciate ligament injuries in soccer: Aprospective controlled study of proprioceptive train-ing. Knee Surg Sports Traumatol Arthroscopy4:19–21, 1996.
11. Chandy TA, Grana WA: Secondary school athleticinjury in boys and girls: A three-year comparison.Phys Sportsmed 13:106–111, 1985.
12. Cipriani D, Armstrong C, Gaul S: Backwards walk-ing at three levels of treadmill inclination: An elec-tromyographic and kinematic analysis. J OrthopSports Phys Ther 22:95–102, 1995.
13. Co FH, Skinner HB, Cannon WD: Effect of recon-struction of the anterior cruciate ligament on propri-oception of the knee and the heel strike transient. JOrthop Res 11:696–704, 1993.
14. Corrigan JP, Cashman WF, Brady MP: Propriocep-tion in the cruciate deficient knee. J Bone Joint Surg74B:247–250, 1992.
15. Feagin JAJ, Curl W: Isolated tears of the anteriorcruciate ligament: Five year follow-up study. Am JSports Med 4:95–100, 1976.
16. Friden T, Zatterstrom R, Lindstrand A, Moritz U: Astabilometric technique for evaluation of lower limbinstabilities. Am J Sports Med 17:118–122, 1989.
17. Giove TP, Miller SJ, Kent BE, et al: Nonoperativetreatment of the torn anterior cruciate ligament. JBone Joint Surg 65A:184–192, 1983.
18. Griffin LY, Agel J, Albohm MJ, et al: Noncontactanterior cruciate ligament injuries: Risk factors andprevention strategies. J Am Acad Orthop Surg8:141–50, 2000.
19. Harrison EL, Duenkel N, Dunlop R, Russell G: Eval-uation of single-leg standing following anterior cru-ciate ligament surgery and rehabilitation. Phys Ther74:245–252, 1994.
20. Hawkins RJ, Misamore GW, Merritt TR: Followupof the acute nonoperated isolated anterior cruciateligament tear. Am J Sports Med 14:205–210, 1986.
21. Heckmann TP, Noyes FR, Barber-Westin SD: Reha-bilitation After Autogeneic and Allogeneic AnteriorCruciate Ligament Reconstruction. In EllenbeckerTS (ed). Knee Ligament Rehabilitation. Philadel-phia, WB Saunders 132–149, 2000.
22. Hellenbrandt FA, Braun GL: The influence of sexand age on the postural sway of man. Am J Phys An-thropol 14:347–360, 1939.
23. Hewett TE, Myer GD, Ford KR: Dynamic neuro-muscular training for preventing knee injury in fe-male athletes. J Orthop Sports Phys Ther 2002. Inpress.
24. Hewett TE, Paterno MV, Noyes FR: Differences insingle leg balance on an unstable platform betweenfemale and male normal, ACL-deficient and ACL-reconstructed knees. The Twenty-fifth Annual Meet-ing of the American Orthopaedic Society for SportsMedicine, Traverse City, MI, 455, 1999.
25. Hewett TE, Paterno MV, Noyes FR: NeuromuscularContributions to Knee Kinematics and Kinetics:Normal Versus Pathological State. In Lephart SM,Fu FH (eds). Proprioception and NeuromuscularControl in Joint Stability. Champaigne, IL, HumanKinetics 77–88, 2000.
26. Hewett TE, Riccobene JV, Lindenfeld TN: The ef-fect of neuromuscular training on the incidence ofknee injury in female athletes: A prospective study.Am J Sports Med 27:699–706, 1999.
27. Hewett TE, Stroupe AL, Nance TA, Noyes FR: Ply-ometric training in female athletes: Decreased im-pact forces and increased hamstring torques. Am JSports Med 24:765–773, 1996.
28. Johansson H, Sjolander P, Sojka P: A sensory rolefor the cruciate ligaments. Clin Orthop 268:161–178,1991.
29. Kennedy JC, Alexander IJ, Hayes KC: Nerve supplyof the human knee and its functional importance. AmJ Sports Med 10:329–335, 1982.
30. Klafs C, Arnheim D: Modern Principles of AthleticTraining. Ed 4. St Louis, CV Mosby 1977.
31. Laskowski ER, Newcomer-Aney K, Smith J: Refin-ing rehabilitation with proprioceptive training: Ex-pediting return to play. Phys Sportsmed 25:89–102,1997.
32. Lephart SC, Perrin DH, Fu FH, et al: Relationship be-tween selected physical characteristics and functionalcapacity in the anterior cruciate ligament-insufficientathlete. J Orthop Sports Phy Ther 16:174–181, 1992.
33. Lephart SM, Fu FH (eds): Proprioception and Neu-romuscular Control in Joint Stability. Champaigne,IL, Human Kinetics 2000.
34. Lephart SM, Henry TJ: Functional rehabilitation forthe upper and lower extremity. Orthop Clin NorthAm 26:579–592, 1995.
35. MacDonald PB, Heeden D, Pacin O, Sutherland K:Proprioception in anterior cruciate ligament-defi-cient and reconstructed knees. Am J Sports Med24:774–778, 1996.
36. McKeag DB: Preseason physical examination for theprevention of sports injuries. Sports Med 2:413–431,1985.
37. Miyatsu M, Atsuta Y, Watakabe M: The physiologyof mechanoreceptors in the anterior cruciate ligament:An experimental study in decerebrate-spinalised ani-mals. J Bone Joint Surg 75B:653–657, 1993.
38. Mizuta H, Shiraishi M, Kubota K, et al: A stabilo-metric technique for evaluation of functional insta-bility in anterior cruciate ligament-deficient knee.Clin J Sports Med 2:235–239, 1992.
Number 402September, 2002 Enhancing Control of the Knee 93

39. Noyes FR, Barber SD, Mangine RE: Abnormallower limb symmetry determined by function hoptests after anterior cruciate ligament rupture. Am JSports Med 19:513–518, 1991.
40. Noyes FR, Dunworth LA, Andriacchi TP, et al: Kneehyperextension gait abnormalities in unstable knees:Recognition and preoperative gait retraining. Am JSports Med 24:35–45, 1996.
41. Noyes FR, Matthews DS, Mooar PA, Grood ES: Thesymptomatic anterior cruciate-deficient knee: Part II:The results of rehabilitation, activity modification,and counseling on functional disability. J Bone JointSurg 65A:163–174, 1983.
42. Noyes FR, Mooar PA, Matthews DS, Butler DL: Thesymptomatic anterior cruciate-deficient knee: Part I:The long-term functional disability in athletically activeindividuals. J Bone Joint Surg 65A:154–162, 1983.
43. Nyland J, Brosky T, Currier D, et al: Review of theafferent neural system of the knee and its contribu-tion to motor learning. J Orthop Sports Phys Ther19:2–11, 1994.
44. Pitman MI, Nainzadeh N, Menche D, et al: The intra-operative evaluation of the neurosensory function of theanterior cruciate ligament in humans using somatosen-sory evoked potentials. Arthroscopy 8:442–447, 1992.
45. Prapavessis H, McNair PJ: Effects of instruction andjumping technique and experience jumping onground reaction forces. J Orthop Sports Phys Ther29:352–356, 1999.
46. Raunest J, Sager M, Burgener E: Proprioceptivemechanisms in the cruciate ligaments: An EMGstudy on reflex activity in thigh muscles. J TraumaInjury Infect Crit Care 41:488–493, 1996.
47. Schultz RA, Miller DC, Kerr CS, Micheli L:Mechanoreceptors in human cruciate ligaments: Ahistological study. J Bone Joint Surg 66A:1072–1076,1984.
48. Schutte MJ, Dabezies EJ, Zimny ML, Happel LT:Neural anatomy of the human anterior cruciate liga-ment. J Bone Joint Surg 69A:243–247, 1987.
49. Seitz H, Schlenz I, Muller E, Vecsei V: Anterior in-stability of the knee despite an intensive rehabilita-tion program. Clin Orthop 328:159–164, 1996.
50. Shelbourne KD, Klootwyk TE, Wilckens JH, De-Carlo MS: Ligament stability two to six years after
anterior cruciate ligament reconstruction with auto-genous patellar tendon graft and participation in ac-celerated rehabilitation program. Am J Sports Med23:575–579, 1995.
51. Sherrington CS: The Integrative Action of the Ner-vous System. New Haven, CT, Yale University Press1906.
52. Smith J, Laskowski E: The preparticipation physicalexamination: Mayo Clinic experience with 2,739 ex-aminations. Mayo Clin Proc 73:419–429, 1998.
53. Snyder-Mackler L, Ladin Z, Schepsis AA, YoungJC: Electrical stimulation of the thigh muscles afterreconstruction of the anterior cruciate ligament: Ef-fects of electrically elicited contraction of the quadri-ceps femoris and hamstring muscles on gait and onstrength of the thigh muscles. J Bone Joint Surg73A:1025–1036, 1991.
54. Solomonow M, Baratta R, Zhou BH, et al: The syn-ergistic action of the anterior cruciate ligament andthigh muscles in maintaining joint stability. Am JSports Med 15:207–213, 1987.
55. Tegner Y, Lysholm J, Lysholm M, Gillquist J: A per-formance test to monitor rehabilitation and evaluateanterior cruciate ligament injuries. Am J Sports Med14:156–159, 1986.
56. Tropp H, Askling C, Gillquist J: Prevention of anklesprains. Am J Sports Med 13:259–262, 1985.
57. Tropp H, Ekstrand J, Gillquist J: Factors affectingstabilometry recordings of single limb stance. Am JSports Med 12:185–188, 1984.
58. Tropp H, Ekstrand J, Gillquist J: Stabilometry infunctional instability of the ankle and its value in pre-dicting injury. Med Sci Sports Exerc 16:64–66, 1984.
59. Tropp H, Odenrick P: Postural control in single-limbstance. J Orthop Res 6:833–839, 1988.
60. Wojtys EM, Huston LJ: Neuromuscular performancein normal and anterior cruciate ligament-deficientlower extremities. Am J Sports Med 22:89–104, 1994.
61. Zatterstrom R, Friden T, Lindstrand A, Moritz U:The effect of physiotherapy on standing balance inchronic anterior cruciate ligament insufficiency. AmJ Sports Med 22:531–536, 1994.
62. Zelisko JA, Noble HB, Porter M: A comparison ofmen’s and women’s professional basketball injuries.Am J Sports Med 10:297–299, 1982.
Clinical Orthopaedics94 Hewett et al and Related Research