Storia naturale delle scelte terapeutiche della BPCO · Definition of COPD Chronic obstructive...
78
www.fisiokinesiterapia.biz Storia naturale delle scelte terapeutiche della BPCO H
-
Upload
trinhthuan -
Category
Documents
-
view
216 -
download
0
Transcript of Storia naturale delle scelte terapeutiche della BPCO · Definition of COPD Chronic obstructive...

www.fisiokinesiterapia.biz
Storia naturale delle scelte terapeutiche della BPCO
H

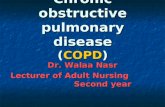
Definition of COPDDefinition of COPD
Chronic obstructive pulmonary disease(COPD) is a disease state characterized by airflow limitation that is not fullyreversible. The airflow limitation is usuallyboth progressive and associated with anabnormal inflammatory response of thelungs to noxious particles or gases.

FEV
1 (%
FE
V1
(% p
rdprd ))
100100
75 75
50 50
25 25
002525 5050 7575
DisabilityDisability ((relapsesrelapses))
DeathDeathAgeAge ((yearsyears))
NeverNever smokedsmoked
O2O2
MVMV
COPD time course
DyspnoeaDyspnoea

The vicious circle of COPD
SocialSocialactivityactivity
SocialSocialisolationisolation
PhysicalPhysicalactivityactivity DepressionDepression
DepressingDepressinglevelslevels ofoffitnessfitness
ShortnessShortness ofofbreathbreath
DyspneaDyspnea
COPD
Pre-agonicsymptoms

Normale borderline LIEVE MODERATA GRAVE
PROGRESSIONE BPCO
Tosse ed espettorazione Dispnea da sforzo Dispnea a riposo
Gas ematici: normali Ipossia e/o ipercapnia
Normale iperinflazione
Età e precocità diagnostica

While smokers who are unable orunwilling to quit may derive limited
benefit from partial smoking reduction, complete smoking
cessation remains a necessity forthose wanting to minimise all of
the harmfuleffects of smoking.

Therapy at each stage of COPD

Fattori correlati alla ridotta sopravvivenza

FEV1
dyspnea

0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 50 100 150 200 250 300 350
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 50 100 150 200 250 300 350
APACHE score
<25
25-40
>40
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 50 100 150 200 250 300 350
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 50 100 150 200 250 300 350
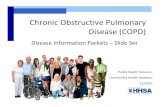
Body Mass Index(kg/m2)
>22
18-22
<18
Activities DailyLiving
Age (years)
Cum
ulat
ive
Prop
ortio
nSu
rviv
ing
Follow up time, Days
Four predictors of survival in COPD. Connors et al., AJRCCM 1996; 154: 959-967
0
1 or 2>2
<60
60-75
>75

N Engl J Med 2004;350:1005-12.
Kaplan–Meier Survival Curves for BODE and according to ATS .

Am J Respir Crit Care Med Vol 171. pp 972–977, 2005

Objectives of COPD ManagementObjectives of COPD Management
• Prevent disease progression • Relieve symptoms• Improve exercise tolerance• Improve health status• Prevent and treat exacerbations• Prevent and treat complications• Reduce mortality• Minimize side effects from
treatment

Am J Respir Crit Care Med Vol 171. pp 446–452, 2005
Patients with frequent exacerbations are more likely to becomehousebound and need targeting in rehabilitation programs.

Distanza percorsa nel 6MWDHui KP, Hewitt AB (Chest 2003; 124: 94-7)
Tolleranza allo sforzo
Carico massimo raggiunto su treadmillRies Al et Al. (AJCCM 2003; 167: 880-8)
Dispnea
Bauldoff GF et Al. (Chest 2002; 122: 948-54)
Affaticabilità dei muscoli scheletrici
M.J.Mador AJRCCM 2001; 163: 930-5)

Quality of Life (Short-Form 36)Williams JEA et Al. ( Thorax 2003; 58: 515-8)
Qualità di BenessereRies Al et Al. (Am.J.Crit.Care Med. 2003)

physiology
survival
haemodinamicssleepneuropsicological
exercise908070605040302010
4 5 6 7 8 9 10PaO2 Kpa
SGR
Q
Thorax 1996; 51:44

Sopravvivenza dei pazienti con BPCO
0
10
20
30
40
50
60
70
80
90
100
10 20 30 40 50 60 70
COT MRC O2 NOT MRC controllo

La piaga delle riacutizzazioni

(CHEST 2000; 117:662–671)

Host factors that associated with treatment failure:• FEV1 < 35% (46.4% vs 22.4%; p < 0.047),
• home oxygen (60.7% vs 15.6%; p < 0.0001),
• Frequency of exacerbation (3.6+/-2.0 vs 1.6 +/- 0.91; p < 0.001),
• history of previous pneumonia (64.3% vs 35.1 p < 0.007),
• history of sinusitis (28.6% vs 8.8%; p < 0.009) and
• use of maintenance steroids (32.1% vs 15.2% p < 0.052).
(CHEST 2000; 117:662–671)

Am J Respir Crit Care Med Vol 164. pp 1002–1007, 2001
A total of 86 cases and 86 control subjects were included, (FEV1 39% prd)
Multivariate logistic regression showed the following risk (or protective) factors of COPD hospitalization:
• three or more COPD admissions in the previous year (oddsratio [OR] 6.21, p<0.008);
• FEV1 (OR 0.96 per percentual unit, p<0.0005);
• underprescription of long-term oxygen therapy (LTOT) (OR 22.64, p<0.007);
• and current smoking (OR 0.30, p<0.022).


One-year survival for 1016 COPD with acute exacerbation
0,5
0,6
0,7
0,8
0,9
1
Follow-up Time, Days
Prop
ortio
n su
rviv
ing
0 100 200 300
N = 1016
Connors, AJRCCM 1998
H

Am J Respir Crit Care Med Vol 161. pp 1608–1613, 2000

Time course of pulmonary function before admission into ICU.A two-year retrospective study of COLD patients with hypercapnia
M Vitacca, K Foglio, S Scalvini, S Marangoni, A Quadri and N Ambrosino
Controlled study:Time course of 2 years before admission in ICU for 16 pts vs 15 controls.
The results indicated that:
Basal body weight,Rate of deterioration over time in:•FEV1•VC,•blood gas values,•bicarbonates, •RVD
may be related to the necessity of ICU admission in COLD patients with hypercapnic respiratory insufficiency.
1992

Raccomandazioni per la ventilazione meccanica Domiciliare. Aggiornamento anno 2003. Parte 1
AIPO, GRUPPO DI STUDIO RIABILITAZIONE LUCIANO PESCE
Documento
Vol 18/5 2003 368-375

Indicazione di trattamento elettiva:paz. senza sufficienti garanzie di autonomia ventilatoria
VMD per via non invasiva
Ventilazione meccanica domiciliareVentilazione meccanica domiciliare
La VMN come strumentodi protezione sulle riacutizzazioni
severe che necessitano diospedalizzazione ?

0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10
PP (41)
MYO (13)KS (53)
TB (55)
COPD (50)BRO (10)
Robert, Rev. Mal. Resp, 1983,11:923
PER
CEN
T SU
RVI
VAL

35
50
65
80
M0 M12 M24
OLTOLT+PSV
35
50
65
80
M0 M12 M24
OLTOLT+PSV
PaC
O2
on a
ir (m
mH
g)
PaC
O2
on o
xyge
n(m
mH
g)
30
45
60
75
M0 M12 M24
OLTOLT+PSV
45
60
75
90
M0 M12 M24
OLTOLT+PSV
PaO
2on
air
(mm
Hg)
PaO
2on
oxy
gen
(mm
Hg)
* p=0.010* p=0.009
ABGsABGs Clini E et al 2002

SURVIVAL CURVES
0.500.550.600.650.700.750.800.850.900.951.00
0 100 200 300 400 500 600 700
Days
Sur
viva
l
OLT
OLT+PSV
Clini E et al 2002
days
survivalsurvival

-20
-10
0
10
20
OLTOLT+PSV
Cha
nge
(day
s/pt
/yea
r)
-3
-1.5
0
1.5
3OLTOLT+PSV
Cha
nge
(nr/p
t/yea
r)
Days spent in hospital Number of hospital stay
CLINICAL OUTCOMECLINICAL OUTCOMEComparisonComparison of hospital of hospital admissionsadmissions
Clini E et al 2002

La ventilazione non invasivanel trattamento della IRA su IRC:una rivoluzione epidemiologica

0
10
20
30
40
50
60
70
80
< 7,20 7,21-7,25 7,26-7,30 7,31-7,35
Soo Hoo, CHEST 2000
RESPONSE TO MEDICAL THERAPY in COPD RELAPSE
% of Intubation
< 7.20 7.21-7.25
7.26- 7.30 7.31.7.35
Time tonor.h
69±60 36±29 31±24 30±18
Death,%
50 20 8 0
TimeEI
2±2 5±4 8±10 13±18
Death%
21 6 9 5
NMV has a role ?

Failure =(NPI × 0.21)+(FVC% × 0.14) -8.28.
Success =(NPI×0.11) +(FVC% ×0.20) -7.53.
ERJ 1996; 9:1487-1493

ETMask ETMask
Endotracheal Tube vs Mask(Complimentary or alternative role ?)
Respiratory failureRespiratory failureEvolving ARFEvolving ARF Resolving ARFResolving ARF
Preventive application
Curative application as EI
Instead of EI Weaningmethod
Post extubationfailure
Modified by U. Meduri

The YONIV Trial for COPD
Inclusion criteria• On arrival on ward
– RR > 23 bpm– pH 7.30-7.35– PaCO2 > 6 kPa
Plant Lancet 2000
Exclusion criteria
Patients requiring immediate ETI pH < 7.207.2 < pH < 7.25 on two occasions (1 hour) GCS < 8 and PaCO2 > 8 kPaPaO2 < 6 kPa despite max tolerated FiO2Cardiorespiratory arrest
0
5
10
15
20
25
pH >= 7.30
Con failNIV failCon diedNIV died
Success mortality

YONIV Study in GW outcome by enrollment pH
05
101520253035404550
pH < 7.30 pH >= 7.30
Con failNIV failCon diedNIV died
Plant Lancet 2000
failure
mortality

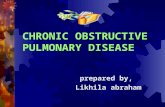
NIV for acute exacerbations of COPD in ICU
(from Brochard L. et al. NEJM 1995;333:817-822)
OUTCOMES
Endotr. intubation, n (%) *
Hospital stay, days *
In-hospital mortality, n (%) *
Complications, % *
NIV (43)
11 (26)
23±17
4 (9)
16
M.T.(42)
31 (74)
35±33
12 (29)
48
* = NIV significantly different from M.T.

NMV MT
No ET 100 % 45%
MV, h 69±36 220±281
H mortality 8% 18%
2-momortality
11% 62%
Confalonieri Am J Respir. Crit. Care Med 1999
Outcome for COPD and CAP in GW


Predictors of failure in hypercapnic pts

(from Antonelli M. et al. ICM 2001;27: 1718-1728)
Predictors of failure in hypoxemic ARF

Risk stratification of NPPV failure was assessed in 1,033 consecutive patients admitted toexperienced hospital units, including two intensive care units, six respiratory intermediate care units, and five general wards. NPPV was successful in 797 patients.

NIV failure:
20-25% in COPD 8-70% in ARF
where EI ?ICU transfert ? ethic decisions

PTPdi/min (cmH20 x s/min)
-1000
100200300400500600700
i-PSV n-PSV T-piece S.B.
**
AJRCCM 164:638-42,2001

WEANING TIME (DAYS)
PR
OB
AB
ILIT
Y O
F R
EM
AIN
ING
ON
MV
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 10 20 30 40 50 60
MaskInvasive
(Nava et al. Ann Intern Med 1998;128:721-728)
PSV + EI
PSV + NMV
OUTCOMES
Duration of MV, days @
Time in ICU, days @
Nosocomial pneumonia, n @
N-PSV
10.2 (6.8)
15.1 (5.4)
0
I-PSV
6 (11.8)
24.0 (13.7)
7

0102030405060708090
100
0-30 31-45 46-60 61-75 >75
No MV MV
Hospital and 1 year survival of pts admitted to ICU with acute exacerbation of COPD.
MG Seneff. JAMA 1995; 274
40
50
60
70
80
90
100
30 90 180 270 360
MV No MV
010203040506070
MV
.
Res
p.
No
resp
.
prio
r.
age
func
tion.
H180 day
Mortality %
Apache III
Alive %Predmortality %

0
10
20
30
40
50
60
70
earliest usually latest
1 week2 week3 week> 3 week
0
2
4
6
8
10
12
14
N° ICUs
Fischer L Intensive Care Med 2000
When tracheo ?
% tracheo of long term MV

The long term weaning center

RICOVERI UTIR Gussago
11%12%
55%
8,8%
19,2%
BPCOPost CCHRistrettiNeurom.Neurologici
Anni 1992-2004= 960 pazienti

Time (hours)
Pro
babi
lity
to re
mai
n un
der M
V
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 100 200 300 400 500 600 700 800 900 1000 1100
p<0.0001
Vitacca M. Am J Respir Crit Care Med 2001; 164: 225-230

PaCO2 mmHg
-60 -40 -20 0 20 40 60
1
patie
nts
% of decay
PaCO2 mmHg
-40 -20 0 20 40
1
patie
nts
% of decay
FEV1 % prd
-100 -50 0 50
1
patie
nts
% of decay
FEV1 % prd
-50 0 50 100
1
patie
nts
% of decay
MIP % prd
-50 0 50 100
1
patie
nts
% of decay
MIP % prd
-80 -60 -40 -20 0 20
1
patie
nts
% of decay
Vitacca et al Monaldi 2005
Decay in respiratory function after ICU admission


1-YEAR SURVIVAL CURVES IN 125 PATIENTS
Months of follow up
Cum
ulat
ive
Pro
porti
on S
urvi
ving
0,50
0,55
0,60
0,65
0,70
0,75
0,80
0,85
0,90
0,95
1,00
0 2 4 6 8 10 12 14
COPD (n° 76)NON-COPD (n° 49)
Months of follow up
Cum
ulat
ive
Pro
porti
on S
urvi
ving
0,65
0,70
0,75
0,80
0,85
0,90
0,95
1,00
0 2 4 6 8 10 12 14
NON MV (44%)MV (55%)

EFFECTS OF ACUTE ON CHRONIC RESPIRATORY FAILURE ON LONG-TERM HYPERCAPNIA AND THREE-MONTH SURVIVAL.
Michele Vitacca MD, Luca Bianchi MD, Luca Barbano MD, Mara Ziliani MD,Nicolino Ambrosino FCCP §.
Patients and interventions:
Seventy-three COPD patients recovering from a recent severeexacerbation underwent evaluation of: AntropometricBreathing pattern,Mechanics, Lung function and arterial blood gases
at discharge from a Respiratory Intensive Care Unit.
2005

Accuracy of prediction and Equations of accuracy for survival and hypercapnia.
Alive = -9.60010.09+(0.1734* %
IBW)
Dead = -8.1086.46+(0.136 * % IBW)
Equations
68475319066.7Total
4635249765.2Alive
52373877.8Dead
Alive (n)Dead (n)% of Accuracy
(%) in prediction
PaCO2≥48mmHg = •-
23.28+(0.0583*Poesmax)+(0.0271*PTPmin)+(96.5
4*TI/TTOT)-18.42 + (90.38 * TI/tot) + (21.12
*PTI)
PaCO2 <48mmHg = •--22.86 + (102.87
26.71+(0.0992* TI/Tot)Poesmax) + (13.1 * PTI0.0194*PTPmin)+(105.71
*TI/TTOT))
Equations
494825975.676Total
4401408091PaCO2 ≥48 mmHg
49111967.944PaCO2 <48 mmHg
PaCO2 ≥48 mmHgPaCO2 <48 mmHg% of Accuracy (%)in
distinction
M. Vitacca et al Chest 2005

POST - RIICU Location 113 pts
0
10
20
30
40
50
60
70 COPD (n°75)
Non COPD(n°38)
44/18
23/5
5/5 2/6 1/4
FSM-Gussago
%
55% 25% 8.8% 7% 4.4%

Raccomandazioni per la ventilazione meccanica Domiciliare. Aggiornamento anno 2003. Parte 1
AIPO, GRUPPO DI STUDIO RIABILITAZIONE LUCIANO PESCE
Documento
Vol 18/5 2003 368-375

Indicazione di trattamento obbligatoriapaz. senza autonomia ventilatoria
VMD per via tracheostomica
Ventilazione meccanica domiciliareVentilazione meccanica domiciliare

3624 3012 180 630
40
50
60
70
80
90
100
KyphoscoliosisTuberculosis seq.
COPDBronchiectasis
Duchenne= 126pts
Months
Prob
abili
ty%
Con
tinui
ngw
ithN
IPPV
N = 276
Leger P et al, Chest, 1994, 105:100

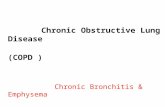
Survival of 12 years HMV in Gussago Hospital
154
83 vivi54%
52 (63%)NMV
31(37%)VMI
36NMV
16 OSAS
Time (Months)
Cum
ulat
ive
Prop
ortio
n Su
rviv
ing
-0.2
0.0
0.2
0.4
0.6
0.8
1.0
0 12 24 36 48 60 72 84 96 108 120 132 144 156
COPDALS
RCWD
NMD
Other



Specialista + ambulatorio dedicato
H
MMG
Il follow up

Nurse Home programAssesment in ER
Treatment at dischargepharmacologicalnon pharmacological
8 week of follow upnurse visit at 24 h (1 h)free nurse visitsfree phonenurse phone calls to pat.
Failure of programmemore of 5 visits, ER admission
Hernandez ERJ 2003

MMG
PNEUMOR
TELEASSISTENZA PNEUMOLOGICA
•
centro servizi
INTERNET o TELEFONO
HOSPITAL

Strumenti disponibili
Telefonoe-mail
ECGSatO2
tracciato di flusso
diario clinico cartella infermieristica
SatO293%

0
0.5
1
1.5
2
2.5
3
H/m/preH/m/post
0
0.5
1
1.5
2
2.5
GP calls/m/preGP calls/m/post
0102030405060708090
100
% pts presentinga relapse pre% pts presentinga relapse post
0102030405060708090
100
% pts who calledGP/m/pre% pts who calledGP/m/post
p<0.005 p<0.005
p<0.0005 p<0.0005
Vitacca et al 2005

05
10152025303540
Admission tohospital
Physician follow-up in
hospital
Other pract.follow-up in
hospital
Home visit
Survey on 1928 italian patients with HMV

ALTERNATIVE FACILITIES
HOME
34%
48%
3% 4%7%
2% 2%0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Self sufficient
Family carers
Nonprofessional
carers
Professionalnon nursing
carers
Nursing care
Residentialcare
Nursing home
Survey on 1928 italian patients with HMV

Domains of End-of-Life Care from Patients’Perspectives
Singer et al. JAMA 1999; 281:163-8
0
10
20
30
40
50
60
70
80
DialysisHIV/AIDSLTMV
Painrelief
Avoidprolongation
of life
Senseof
control
Reliefof
burden
Strengtheningrelationshipwith beloved

CHEST 2002;122

These programs are underutilizedlower awareness of Hospice eligibility criteria than oncologistsunpredicatability of deathlimitations on insurances
hospice care offers expertize for palliation; bridge to homeeligibility criteria and services available need to be known

CONCLUSIONI
Grazie al miglioramento delle cure, sempre più pazienti respiratoriarrivano a vivere una condizione di prolungata sopravvivenzacon problematiche di grave cronicità
La gestione della BPCO è divenuta ormai una complessa presa in carico(di tutte le figure professionali) di sintomi fisici e psicosociali,dipendenze, problematiche multidisciplinari e multifattoriali.
Operatori sanitari e famiglia devono sempre più collaborare per prendere comuni decisioni cliniche ed etiche

H
Programmi ospedalieri
spedalizzazione domiciliaretelesorveglianza
CONCLUSIONI
Casa RSA/Hospice

the current results do notsupport the widespreadprovision of ambulatoryoxygen to patients withoxygen-dependent chronicobstructive pulmonarydisease

ERJ 1996;9:1487-1493