Sterile Drug Products Used During Delivery and the...
36
Sterile Drug Products Used During Delivery and the Postpartum Period PharMEDium Lunch and Learn Series ProCE, Inc. www.ProCE.com 1 Sterile Drug Products Used During Delivery and the Postpartum Period LUNCH AND LEARN February 12, 2016 Featured Speaker: Kylie N. Barnes, Pharm.D., BCPS Clinical Assistant Professor University of Missouri ‐ Kansas City School of Pharmacy 1 CE Activity Information & Accreditation ProCE, Inc. (Pharmacist and Tech CE) 1.0 contact hour Funding: This activity is self‐funded through 2 PharMEDium. It is the policy of ProCE, Inc. to ensure balance, independence, objectivity and scientific rigor in all of its continuing education activities. Faculty must disclose to participants the existence of any significant financial interest or any other relationship with the manufacturer of any commercial product(s) discussed in an educational presentation. Dr. Barnes has no relevant commercial and/or financial relationships to disclose.
Transcript of Sterile Drug Products Used During Delivery and the...

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 1
Sterile Drug Products Used During Delivery and the Postpartum Period
LUNCH AND LEARN
p
February 12, 2016
Featured Speaker: Kylie N. Barnes, Pharm.D., BCPS
Clinical Assistant ProfessorUniversity of Missouri ‐ Kansas City School of Pharmacy
1
CE Activity Information & Accreditation
ProCE, Inc. (Pharmacist and Tech CE)
1.0 contact hour
Funding: This activity is self‐funded through
2
g y gPharMEDium.
It is the policy of ProCE, Inc. to ensure balance, independence, objectivity and scientific rigor in all of its continuing education activities. Faculty must disclose to participants the existence of any significant financial interest or any other relationship with the manufacturer of any commercial product(s) discussed in an educational presentation. Dr. Barnes has no relevant commercial and/or financial relationships to disclose.

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 2
Submission of an online self‐assessment and evaluation is the
Online Evaluation, Self-Assessmentand CE Credit
Submission of an online self assessment and evaluation is the only way to obtain CE credit for this webinar
Go to www.ProCE.com/PharMEDiumRx
Print your CE Statement online
Live CE Deadline: March 11, 2016
CPE Monitor
3
– CE information automatically uploaded to NABP/CPE Monitor within 1 to 2 weeks of the completion of the self‐assessment and evaluation
Event Code
Code will be provided at the end of today’s activityEvent Code not needed for On‐Demand
Ask a Question
Submit your questions to your site manager.
Questions will be answered at the end of the presentation.
4
Your question. . . ?

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 3
Resources
Visit www.ProCE.com/PharMEDiumRx to access:
Handouts– Handouts
– Activity information
– Upcoming live webinar dates
– Links to receive CE credit
5
Sterile Drug Products Used During Delivery and the Post-partum Period
Kylie N. Barnes, Pharm.D., BCPS
PharMEDium, LLCSpring 2016
6
Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 4
Learning Objectives: Pharmacists1. Evaluate what medications will likely be needed as
supportive care for the patients based on the differentsupportive care for the patients based on the different types of delivery (e.g., natural vaginal delivery, induction, emergency c-section, etc).
2. Evaluate pain management options for pregnant patients during delivery, including PCAs, epidurals, and injectable options.
3 Determine the need for analgesia and/or sedation in a3. Determine the need for analgesia and/or sedation in a pregnant patient in active or scheduled delivery.
4. Design individualized treatment regimens for pregnant patients with pre-eclampsia, eclampsia, hyperemesis, clotting disorder/thrombosis during pregnancy, pre-term labor, or a Group B streptococcus + status pre-delivery. 7
Learning Objectives: Technicians1. List the medications likely needed as supportive care for
the patients based on the different types of delivery (e.g.,the patients based on the different types of delivery (e.g., natural vaginal delivery, induction, emergency c-section, etc).
2. Recognize the pain management options for pregnant patients during delivery, including PCAs, epidurals, and injectable options.
3 Summarize the need for analgesia and/or sedation in a3. Summarize the need for analgesia and/or sedation in a pregnant patient in active or scheduled delivery.
4. Recognize the medications used in pregnant patients with pre-eclampsia, eclampsia, hyperemesis, clotting disorders/thrombosis during pregnancy, pre-term labor, or a Group B streptococcus + status pre-delivery. 8
Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 5
Plan Varies by Delivery Method
• Term vaginal delivery
• Induced vaginal delivery
• Scheduled cesarean delivery
• Emergency cesarean deliveryEmergency cesarean delivery
9
Term Vaginal Delivery
• Routine to give all women an IV during• Routine to give all women an IV during labor– Precautionary to prevent dehydration
– Saves a step later should there be an emergency
• Heparin lock an option p p– Open vein in the event of an emergency
– Not tethered to IV pole
10

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 6
Induced Vaginal Delivery
• More than 22% of all deliveries involve• More than 22% of all deliveries involve induction– Elective vs. indicated
11
Induced Vaginal Delivery: Pitocin
• Most commonly used drug in the US –synthetic form of oxytocin
• Physiology of oxytocin-stimulated labor is similar to spontaneous labor– Stimulates an increase in intracellular calcium
in uterine myometriumin uterine myometrium
– Causes contractions of the uterus. Used to:• Start labor
• Increase the speed of labor
• Stop bleeding following delivery 12

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 7
Induced Vaginal Delivery: Pitocin
• Individual patients vary in sensitivity and• Individual patients vary in sensitivity and response
• Uterine response occurs 3-5 minutes after infusion
• Steady level of oxytocin in plasma achieved S y y pby 40 minutes
• Typically have better response closer to term
13
Induced Vaginal Delivery: PitocinLabor Stimulation with Pitocin
Regimen Starting Dose Incremental Dosage Interval g g(mU) Increase (mU/min)
g(min)
Low-dose 0.5 – 2 1 – 2 15 – 40
High-dose 6 3 – 6 * 15 – 40
*incremental increase is reduced to 3 mU/min in presence ofincremental increase is reduced to 3 mU/min in presence of hyperstimulation and reduced to 1 mU/min with recurrent hyperstimulation
*Adapted from ACOG Practice Bulletin: Induction of Labor August 2009 14

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 8
Induced Vaginal Delivery: Pitocin
E h h it l t i ll h th i• Each hospital typically has their own titration protocol
• Pitocin generally diluted 10 units in 1000 mL of an isotonic solution – concentration of 10 mU/mL
• Administered by infusion pump that allows precise control of the flow rate
15
“Routine” C-Section
• Represents 31 8% of deliveries in the US• Represents 31.8% of deliveries in the US– Most common surgical procedure
• Spinal anesthesia
• Epidural anesthesia
• General anesthesia• General anesthesia
16

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 9
Emergency C-Section
• Only 0 5 1% of all deliveries• Only 0.5 – 1% of all deliveries
• Usually in response to acute hemorrhage, fetal bradycardia, umbilical cord prolapse, or uterine rupture
• Very quick process – fetal morbidity and V y q p ymortality can be greatly affected by a delay of just a few minutes
17
Emergency C-Section
• Coordination of at least six individuals:• Coordination of at least six individuals: surgeon, assistant for the surgeon, anesthesiologist, scrub technologist, circulating nurse and pediatrician
• Currently no standardized protocols exist
• General anesthesia is commonly used
18

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 10
Additional Concerns
• Drugs used for pain control during labor and deliveryand delivery
• Drugs used for complications– Preterm Labor
– Group B Streptococcus +
– Pre-eclampsia / EclampsiaPre eclampsia / Eclampsia
– Anticoagulation
– Nausea and vomiting/hyperemesis
19
PAIN CONTROL DURING LABOR AND DELIVERY
20

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 11
Pain Control During Labor and Delivery
• Available methods of analgesia• Available methods of analgesia– Parenteral
– Regional• Epidural
• Spinal
21
Pain Control: Parenteral• Can be given in intermittent doses by
ti t tpatient request
• Don’t relieve pain, but reduce anxiety and result in sedation
• May be set up via patient-controlled administration (PCA) pain pumps
Agent Usual Dose Frequency Onset
Meperidine 25-50mg IV Q 1-2 hours 5 minutes
Fentanyl 50-100 mcg IV Q 1 hour 1 minute
Butorphanol 1-2mg IV Q 4 hours 1-2 minutes
Morphine 2-5mg IV Q 4 hours 5 minutes
Nalbuphine 10mg IV Q 3 hours 2-3 minutes
*Adapted from ACOG Practice Bulletin: Obstetric analgesia and anesthesia July 200222

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 12
Pain Control: Regional
• Partial to complete loss of painp p
sensation below T8 to T10
• Epidural – offers the most effective form of pain relief – Catheter is placed in the epidural space; continuous
infusion of local anesthetic agents or narcotics
– Can be used for c-section delivery or postpartum tubal ligation
– Commonly combine a low-dose local anesthetic (e.g., bupivacaine, or ropivacaine) with an opioid agonist (fentanyl)
23
Pain Control: Regional
• Spinal block – single-shot spinal analgesia p g p g– Excellent pain relief for short duration procedures
• C-section delivery
• Second stage of labor
• Rapidly progressing labor
• Postpartum tubal ligation p g
– Long-acting local anesthetic often used, with or without opioid agonist
– Duration approximately 30-250 minutes depending on agent(s) used
24

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 13
Pain Control: ComplicationsComplication Incidence (%)
Fever > 100.4° FNulliparous women 19%Nulliparous womenMultiparous women
19%1%
Postdural puncture headacheSpinalEpidural
1.5-3%2%
Transient fetal heart decelerations 8%
i h i id dd dPruritus – when opioid addedEpiduralSpinal
1.3-26%41-85%
Inadequate pain relief (epidural) 9-15
*Adapted from ACOG Practice Bulletin: Obstetric analgesia and anesthesia July 2002 25
Pain Control During Labor and Delivery
• In the event the neonate appears depressed• In the event the neonate appears depressed – Naloxone 0.1 mg/kg IV may be indicated to
reverse the effects of the analgesia
• Mother and baby will be on continuous watch
26
Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 14
Pain Control During Labor and Delivery: Breastfeeding
• Intrapartum opioid use may:– Decrease neonatal rooting reflexes and delay
initiation of breastfeeding
– Increase agitation and irritation in infant
27
PRE-TERM LABOR
28
Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 15
Pre-Term Labor
• Labor between 20 -37 weeks gestation
• ~12% of all births occur before term
• Leading cause of neonatal mortality
• Most common reason for antenatal hospitalization
• Accounts for:~70% of neonatal deaths
~36% of infant deaths~25-50% of cases of long-term neurologic
impairment in children 29
Pre-Term Labor
• Approximately 30% spontaneously resolves• Approximately 30% spontaneously resolves
• 50% of patients hospitalized with pre-term labor deliver at term
• Delays in delivery are reserved for women where a delay will benefit the newborn y
30

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 16
Pre-Term Labor: Treatment• Nonpharm
– Bed rest
– Abstention from intercourse/orgasm
– Hydration
• Pharm– Tocolytic drugs – inhibit uterine contractionsTocolytic drugs inhibit uterine contractions
– Antibiotics – treat intrauterine bacterial infections
– Corticosteroids – maturation of fetal lungs
– Magnesium sulfate – fetal neuroprotection
31
Pre-Term Labor: Tocolytic Agents
Agent/Class Maternal Side Effects Fetal or Newborn Side Effects
Contraindications
Calcium channel blockers
Dizziness, flushing, hypotension
No known ADRs Hypotension and preload-dependent cardiac lesions, such as aortic insufficiency
NSAIDs Nausea, esophageal reflux, gastritis, and emesis
Oligohydramnios Platelet dysfunction or bleeding disorder, hepatic disorders, GI ulcerative disease, renal dysfunction, asthma
Magnesium sulfate
Flushing, diaphoresis, nausea,loss of deep tendon reflexes, respiratory depression, and cardiac arrest
Neonataldepression
Myasthenia gravis
32

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 17
Pre-Term Labor: Tocolytic AgentsClass Example Agent and Dose
Calciumchannel
Nifedipine 10-20mg oral loading dose, repeated every 3 to 6 hours until contractions are rare, then followed by long-acting formulations of 30-60mg everychannel
blockerscontractions are rare, then followed by long acting formulations of 30 60mg every 8-12 hours for 48 hours
NSAIDs Indomethacin 50mg oral loading dose, followed by 25 – 50 mg by mouth every 6 hoursTherapy generally limited to 48 hoursUsed before 32 weeks gestation
Magnesiumsulfate
Magnesium sulfate 4-6 g in 10% to 20% solution loading dose given over 30 minutes, followed by maintenance dose of 2g/hourThe IV rate is increased by 1 g/hour until the patient has less than one contractionThe IV rate is increased by 1 g/hour until the patient has less than one contraction per 10 minutes or until the maximal dose of 3 or 4 g/hour is reached IV fluids are restricted to 125 mL/hourDeep tendon reflexes and vital signs, including respiratory rate, should be recorded hourly
33
Pre-Term Labor: Tocolytic Agents
• Effective for up to 48 hours
• Not indicated for use before neonatal viability
• Special circumstances – after an event known to cause pre-term labor (e.g., intra-bd i l )abdominal surgery)
• Women with pre-term contractions, but not cervical change (dilation < 2 cm) in general should not receive tocolytics
34

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 18
Pre-Term Labor: Tocolytic Agents
Contraindications to TocolysisContraindications to Tocolysis
Intrauterine fetal demiseLethal fetal anomaly
Nonreassuring fetal statusSevere preeclampsia or eclampsia
Maternal bleeding with hemodynamic instabilityChorioamnionitisChorioamnionitis
Preterm premature rupture of membranesMaternal contraindications to tocolysis (agent specific)
35
Pre-Term Labor: Antibiotics
• Given in pre term labor to prevent neonatal• Given in pre-term labor to prevent neonatal Group B streptococcus infection
• Intrapartum prophylaxis with penicillin or ampicillin recommended
(more information later) ( )
36

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 19
Pre-Term Labor: Corticosteroids
• Direct improvement in neonatal outcomes– Lower severity and frequency of:
• Respiratory distress syndrome
• Intracranial hemorrhage
• Necrotizing enterocolitis
• Death
• Single course recommended for pregnant women between 24 – 34 weeks of gestation– May be given at week 23 in women at risk for
pre-term delivery with 7 days37
Pre-Term Labor: Corticosteroids
• Betamethasone 12mg intramuscularly every 24 hours x 2 doses
• Dexamethasone 6mg intramuscularly every 12 hours x 4 doses
• First dose still given, even if unlikely patient will be able to receive second dose
38

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 20
Pre-Term Labor: Magnesium Sulfate
• When given with neuroprotection intent• When given with neuroprotection intent– Pre-delivery administration reduces the
occurrence of cerebral palsy
– Does not prolong labor
39
GROUP B STREPTOCOCCUS POSITIVE
40

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 21
Group B Streptococcus + (GBS)
• Asymptomatic, rectovaginal colonization– Approximately 20-30% of pregnant women
• Increases risk for perinatal sepsis and maternal infection
• Prevention– All pregnant women screened at 35-37 weeks
gestation for GBS colonization
– Women who are GBS + receive antibiotic prophylaxis during delivery
41
Group B Streptococcus + (GBS): Treatment
First Line Agent Alternative RegimenP i illi G 5 illi it i iti ll A i illi 2 IV i iti ll th 1Penicillin G 5 million units initially; then 2.5 to 3 million units every 4 hours IV until delivery
Ampicillin 2 g IV initially; then 1 g every 4 hours until delivery
Penicillin Allergy: low risk for anaphylaxis
Penicillin Allergy: high risk for anaphylaxisp y p y
(immediate urticarial or bronchospasms)
Cefazolin 2 g IV initially; then 1 g every 8 hours IV until delivery
Clindamycin 900 mg IV every 8 hours (if susceptibility is known)
Vancomycin 1 g IV every 12 hours42

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 22
Group B Streptococcus + (GBS)
• Best results when given at least 4 hours before• Best results when given at least 4 hours before delivery
• If GBS status is not known at the time of delivery, give antibiotics if:– Less than 37 weeks gestation
– Rupture of membranes occurred at least 18 hoursRupture of membranes occurred at least 18 hours earlier
– Temperature at or greater than 100.4ºF
• Scheduled C-section delivery, antibiotics are not needed
43
Risk Factors:• Previous infant with GBS
disease?• GBS bacteriuria this pregnancy?• Delivery < 37 weeks’ gestation
No
Yes
Collect rectal and vaginal swab for GBS culture at 35-37 weeks’ gestation GBS+
NoGive PCN
(or alternative in case of allergy)
GBS-Not done,
incomplete, or unknown
No prophylaxis needed
Risk factors:Intrapartum fever > 38 C (100.4 F)Membrane rupture > 18 hours
Yes
No44

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 23
PRE-ECLAMPSIA / ECLAMPSIA
45
Pre-eclampsia
• Disorder in pregnancy characterized by• Disorder in pregnancy characterized by poor perfusion of many vital organs that is completely reversible with the termination of pregnancy
• Occurs in about 4% of pregnancies
• Often asymptomatic, but most related to – Hypertension (> 140/90 mmHg after week 20)
– Proteinuria (> 0.3 g in 24 hour urine collection)
46

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 24
Pre-eclampsia
Other Signs and Symptoms of Pre-eclampsia and Eclampsia g y p p p
Cerebral FeaturesHeadache DizzinessTinnitus
DrowsinessChange in respiratory rate
Tachycardia
Visual FeaturesDiplopia
ScotomataBlurred Vision
Amaurosis
Fever
Gastrointestinal FeaturesNausea
VomitingEpigastric painHematemesis
Renal FeaturesOliguriaAnuria
HematuriaHemoglobinuria
47
Preeclampsia Treatment
• Delivery if pregnancy is at term
• IV magnesium sulfate to prevent seizures– Loading dose of 4-6 g IV over 15 to 30
minutes, followed by 1-2 g/hr as continuous infusion
– Deep tendon reflexes and respiratory statusDeep tendon reflexes and respiratory status checked at least every 2 hours
– If overdosage occurs (e.g., apnea) • Calcium gluconate 10mL of 10% solution IV over 3
minutes is an effective antidote 48

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 25
Preeclampsia Treatment
• If a patient is on magnesium and has an eclamptic seizure:– Diazepam 5 to 10 mg IV
– Lorazepam 4 mg IV
– Pentobarbital 125 mg IV
• Most seizures terminate spontaneously• Most seizures terminate spontaneously within 1-2 minutes– Avoidance of injury
– Protection of the airway to prevent aspiration 49
Preeclampsia Treatment• Frequent monitoring of BP, urine protein,
CMP, and platelet counts
• Begin drug therapy for BP if > 140/90mmHg
• Start IV hypertensives if SBP 160-180 or DBP >110 (PO okay if preeclampsia)
Drug Intravenous Dose Interval between Doses
Hydralazine 5-10mg Q 15-20 minutes until desired response
Labetalol 20mg bolus, followed by 40mg
If not effective within 10 minutes, then 80mg every 10 minutes to a maximum total dose of 220mg
Nifedipine 10mg orally 4-8 hours
*Adapted from ACOG Practice Bulletin: Diagnosis and Management of Preeclampsia and Eclampsia January 2002 50

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 26
Preeclampsia
• Goals of therapypy– Decrease blood pressure
– Prevent or control seizures
– Deliver a viable infant
• Risk for eclampsia can continue for up to 6 weeks after delivery– Must continue to monitor blood pressure and
urine protein levels 51
ANTICOAGULATION
52
Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 27
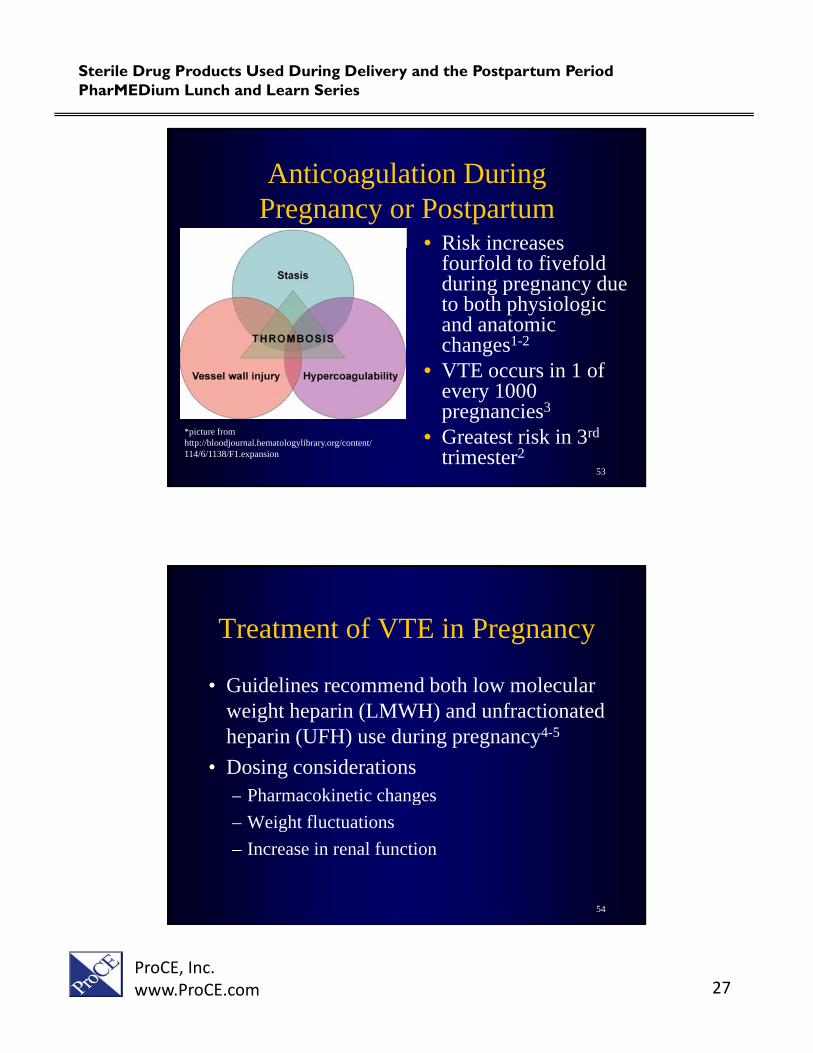
Anticoagulation During Pregnancy or Postpartum
• Risk increasesRisk increases fourfold to fivefold during pregnancy due to both physiologic and anatomic changes1-2
• VTE i 1 f• VTE occurs in 1 of every 1000 pregnancies3
• Greatest risk in 3rd
trimester2
*picture from http://bloodjournal.hematologylibrary.org/content/ 114/6/1138/F1.expansion
53
Treatment of VTE in Pregnancy
• Guidelines recommend both low molecular• Guidelines recommend both low molecular weight heparin (LMWH) and unfractionated heparin (UFH) use during pregnancy4-5
• Dosing considerations– Pharmacokinetic changesg
– Weight fluctuations
– Increase in renal function
54

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 28
Treating a Newly Diagnosed VTE in Pregnancy
Hemodynamically Stable Hemodynamically Unstabley y y y
Patient presentationNormal heart rate / blood pressureOxygenating well
Unstable heart rate and/or blood pressureLarge clotsOther maternal comorbidities
TreatmentTherapeutic LMWH – anticipatingdischarge from the hospital
IV UFH: 80 units/kg IV one time followed by 80 units/kg/hour by continuous IV infusion. The dose is adjusted to maintain aPTT atTreatment discharge from the hospital
relatively soonis adjusted to maintain aPTT at 1.5 to 2.5 times control
(or based on hospital protocol)
*Adapted from ACOG Practice Bulletin: Thromboemolism in Pregnancy September 2011 55
Recommended Thromboprophylaxis for Pregnancies
Clinical Scenario Antepartum Management
Postpartum Management
Low-risk thrombophilia w/oprevious VTE
Surveillance orProphylactic LMWH or UFH
Surveillance or postpartum anticoagulation if patient hasprevious VTE Prophylactic LMWH or UFH anticoagulation if patient has risk factors
Low-risk thrombophilia w/ single previous VTE
Surveillance or Prophylactic LMWH or UFH
Postpartum anticoagulation therapy
High-risk thrombophilia w/o previous VTE
Prophylactic LMWH or UFH Postpartum anticoagulation therapy
Thrombophilia or no thrombophilia with > 2
Prophylactic or therapeutic LMWH or UFH
Postpartum anticoagulation therapy
episodes of VTE – not on long-term anticoagulation
Thrombophilia or no thrombophilia with > 2 episodes of VTE – receiving long-term anticoagulation
Therapeutic dose LMWH or UFH
Resumption of long-term anticoagulation therapy
*Adapted from ACOG Practice Bulletin: Thromboembolism in Pregnancy September 2011 56

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 29
Current Recommendations
• Most practitioners will use LMWH until week 36
• Switch the heparin in preparation for delivery– Shorter half-life
L i k f id l i l h i h– Lower risk of epidural or spinal hematoma with regional anesthesia
• Typically withhold neuraxial blockade for 10-12 hours after last prophylactic dose of LMWH or 24 hours after last therapeutic dose of LMWH
57
Current RecommendationsManagement Type Dosage
Enoxaparin 40mg subQ once dailyProphylactic
Indication for LMWHDalteparin 5,000 units subQ once dailyTinzaparin 4,500 units subQ once daily
Enoxaparin 1mg/kg subQ every 12 hoursTherapeutic
Indication for LMWH
Enoxaparin 1mg/kg subQ every 12 hoursDalteparin 200 units/kg subQ once dailyTinzaparin 175 units/kg subQ once dailyDalteparin 100 units/kg subQ once daily
*Adapted from ACOG Practice Bulletin: Thromboembolism in Pregnancy September 2011 58

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 30
Current RecommendationsManagement Type Dosage
1st trimesterUFH 5,000 – 7,000 units SC every
12 hours
Prophylactic Indication for UFH
2nd
trimester UFH 7,500 to 10,000 units SC
every 12 hours
3rd trimesterUFH 10,000 units sub-Q every 12 hours unless aPTT is elevated
Therapeutic Indication for UFH
UFH 10,000 units or more sub-Q every 12 hours in doses adjusted to target aPTT in the
therapeutic range 6 hours after injection
*Adapted from ACOG Practice Bulletin: Thromboembolism in Pregnancy September 2011 59
Postpartum Anticoagulation
• Start heparin or LMWH no sooner than 4 6
Prophylactic LMWH/UFH for 4-6 weeks
• Start heparin or LMWH no sooner than 4-6 hours after vaginal delivery or 6-12 hour after cesarean delivery
PostpartumAnticoagulation
Vitamin K antagonists for 4-6 weeks with a target INR of 2-3 until initial UFH or
LMWH therapy overlap until the INR is 2 or more for 2 days
*Adapted from ACOG Practice Bulletin: Thromboembolism in Pregnancy September 2011 60

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 31
Postpartum Anticoagulation
• Some patients will need to continue therapy• Some patients will need to continue therapy for more than 6 weeks after delivery
• Preferred agents
WarfarinLMWH
– Do not accumulate in breastmilk
– Do not induce an anticoagulant effect in the infant
Unfractionated Heparin
61
NAUSEA / VOMITING HYPEREMESIS
62

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 32
Hyperemesis Gravidarum
• Represents the extreme end of the spectrump p– Persistent vomiting not related to other causes
– Clinical diagnosis of exclusion
• Approximately 0.3-3% of pregnancies
• Acute starvation – usually large ketonuria
• Discrete measure weight loss – Typically at least 5% of prepregnancy weight
• Electrolyte, thyroid and liver abnormalities may be present 63
Hyperemesis Gravidarum
• Most common indication for hospitalization• Most common indication for hospitalization during the first part pregnancy
• Some women experience significant psychosocial morbidity caused by nausea and vomiting of pregnancy, resulting in a decision for pregnancy termination – Poor support from partners reported in 85%
– Common to have subacute disease states (e.g., depression, somatization, hypochondriasis)
64

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 33
Hyperemesis Gravidarum
• Effects on fetus• Effects on fetus– Low birth weight
– Small for gestational age infants
– Premature infants
– Pregnancy related hypertension
65
Hyperemesis Gravidarum: Treatment
• In severe cases:In severe cases:• Ondansetron 4-8 mg IV Q 8 hours
• Metoclopramide 5-10 mg IV Q 8 hours
• Also available as continuous subcutaneous pumps
66

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 34
Hyperemesis Gravidarum: Treatment
• Ondansetron better at controlling vomitingOndansetron better at controlling vomiting, but had a similar effect to metoclopramide in managing nausea1
• Complications of worsening side effects with pumps have been seen in 25-31% of patients2
1. Kashifard M, Basirat Z, Kashifard M, et al. Ondansetrone or metoclopramide? Which is more effective in severe nausea and vomiting of pregnancy? A randomized trial double-blind study. Clin Exp Obstet Gynecol 2013;40:127-30. 2. Reichmann JP, Kirkbride MS. Reviewing the evidence for using continuous subcutaneous metoclopramide and ondansetron to treat nausea and vomiting duringpregnancy. Manag Care 2012;21:44-7. 67
Hyperemesis Gravidarum: Treatment
• Methylprednisolone 16mg TID x 3 days followed• Methylprednisolone 16mg TID x 3 days, followed by a 2 week taper with oral promethazine– One RTC found steroids reduce the rates of hospital
readmission within 2 weeks1
– Another found steroids have no effect on need for rehospitalization2
• Risk for oral cleft when used in 1st trimester – use should be “last resort” and avoided before 10 weeks
1. Safari HR, Fassett MJ, Souter IC, et al. The efficacy of methylprednisolone in the treatment of hyperemesis gravidarum: a randomized, double-blind, controlled study. Am J Obstet Gynecol 1998;179:921-4.
2. Yost NP, McIntire DD, Wians FH, et al. A randomized, placebo-controlled trial of corticosteroids for hyperemesis due to pregnancy. Obstet Gynecol2003;102:1250-4. 68

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 35
Hyperemesis Gravidarum: Hospitalization
• Inpatient management required when:• Inpatient management required when:– Cannot tolerate liquids without vomiting
– Has not responded to outpatient management
69
Hyperemesis Gravidarum: Treatment
• Intravenous hydration used when not tolerating oral liquidsIntravenous hydration used when not tolerating oral liquids for prolonged periods or signs of dehydration are present
• Prolonged vomiting present add:– Thiamine, dextrose, and vitamins
• Enteral tube feeding (nasogastric or nasoduodenal) should be initiated as first-line when nonresponsive to medicine
d t i t i i htand cannot maintain weight
• Total parenteral nutrition is potentially life-threatening due to associated sepsis and thromboembolic events – Reserved for patients unable to tolerate enteral feedings
ACOG Practice Bulletin: Nausea and Vomiting September 201570

Sterile Drug Products Used During Delivery and the Postpartum PeriodPharMEDium Lunch and Learn Series
ProCE, Inc.www.ProCE.com 36
Questions?
71