Stereoscopic neuroanatomy lectures using a three …timkilleen.com/files/AA2015.pdf · their...
29
Accepted Manuscript Title: Stereoscopic neuroanatomy lectures using a three-dimensional virtual reality environment Author: Ralf A. Kockro MD Christina Amaxopoulou MD Tim Killeen MRCS Wolfgang Wagner MD Robert Reisch MD Angelika Gutenberg MD Alf Giese MD Eckart Stofft MD Axel T. Stadie MD PII: S0940-9602(15)00084-9 DOI: http://dx.doi.org/doi:10.1016/j.aanat.2015.05.006 Reference: AANAT 50963 To appear in: Received date: 10-9-2014 Revised date: 25-5-2015 Accepted date: 27-5-2015 Please cite this article as: Kockro, R.A., Amaxopoulou, C., Killeen, T., Wagner, W., Reisch, R., Gutenberg, A., Giese, A., Stofft, E., Stadie, A.T.,Stereoscopic neuroanatomy lectures using a three-dimensional virtual reality environment., Annals of Anatomy (2015), http://dx.doi.org/10.1016/j.aanat.2015.05.006 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Transcript of Stereoscopic neuroanatomy lectures using a three …timkilleen.com/files/AA2015.pdf · their...

Accepted Manuscript
Title: Stereoscopic neuroanatomy lectures using athree-dimensional virtual reality environment
Author: Ralf A. Kockro MD Christina Amaxopoulou MDTim Killeen MRCS Wolfgang Wagner MD Robert Reisch MDAngelika Gutenberg MD Alf Giese MD Eckart Stofft MDAxel T. Stadie MD
PII: S0940-9602(15)00084-9DOI: http://dx.doi.org/doi:10.1016/j.aanat.2015.05.006Reference: AANAT 50963
To appear in:
Received date: 10-9-2014Revised date: 25-5-2015Accepted date: 27-5-2015
Please cite this article as: Kockro, R.A., Amaxopoulou, C., Killeen, T., Wagner, W.,Reisch, R., Gutenberg, A., Giese, A., Stofft, E., Stadie, A.T.,Stereoscopic neuroanatomylectures using a three-dimensional virtual reality environment., Annals of Anatomy(2015), http://dx.doi.org/10.1016/j.aanat.2015.05.006
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.

Page 1 of 28
Accep
ted
Man
uscr
ipt
Stereoscopic neuroanatomy lectures using a three-dimensional virtual reality environment.
Ralf A Kockro MD,1,3 Christina Amaxopoulou MD,2 Tim Killeen MRCS,1,4 Wolfgang Wagner MD,3 Robert Reisch MD,1,3 Angelika Gutenberg MD,3 Alf Giese MD,3 Eckart Stofft MD,5 Axel T Stadie MD.3
1. Department of Neurosurgery, Klinik Hirslanden, Zurich, Switzerland
2. Department of Radiology, Children’s Hospital Zurich, Switzerland
3. Department of Neurosurgery, University Hospital Mainz, Germany
4. Paraplegia Laboratory, University Hospital Balgrist, Zurich, Switzerland
5. Department of Anatomy, University Hospital, Mainz. Germany
Running title: 3D virtual reality in neuroanatomy teaching
Corresponding author:
Ralf A. Kockro, MDDepartment of NeurosurgeryKlinik HirslandenWitellikerstrasse 408032 ZurichSwitzerlandTel.: +41 44 387 21 30Fax.: +41 44 387 21 31Email: [email protected]
Conflict of Interest Statement
Ralf A Kockro is a co-inventor of the Dextroscope Virtual Reality system. He no longer
has any financial interest in the company and has no other conflict of interest to
declare. The other authors declare that they are not aware of any real or potential
conflict of interest in relation to this study.

Page 2 of 28
Accep
ted
Man
uscr
ipt
Abstract
Introduction: Three-dimensional (3D) computer graphics are increasingly used to
supplement the teaching of anatomy. While most systems consist of a program which
produces 3D renderings on a workstation with a standard screen, the Dextrobeam
virtual reality VR environment allows the presentation of spatial neuroanatomical
models to larger groups of students through a stereoscopic projection system.
Materials and Methods: Second-year medical students (n=169) were randomly
allocated to receive a standardised pre-recorded audio lecture detailing the anatomy of
the third ventricle accompanied by either a two-dimensional (2D) PowerPoint
presentation (n=80) or a 3D animated tour of the third ventricle with the DextroBeam.
Students completed a 10-question multiple-choice exam based on the content learned
and a subjective evaluation of the teaching method immediately after the lecture.
Results: Students in the 2D group achieved a mean score of 5.19 (±2.12) compared to
5.45 (±2.16) in the 3D group, with the results in the 3D group statistically non-inferior to
those of the 2D group (p<0.0001). The students rated the 3D method superior to 2D
teaching in four domains (spatial understanding, application in future anatomy classes,
effectiveness, enjoyableness) (p<0.01). Conclusion: Stereoscopically-enhanced 3D
lectures are valid methods of imparting neuroanatomical knowledge and are well
received by students. More research is required to define and develop the role of large-
group VR systems in modern neuroanatomy curricula.
Keywords
Three-dimensional; virtual reality; neuroanatomy; medical education; medical students;
anatomical models; Dextrobeam; third ventricle.

Page 3 of 28
Accep
ted
Man
uscr
ipt
1. Introduction
Internationally, there is a decline in the use of cadaveric dissection as a means
of familiarising medical students with human anatomy, in part driven by the high
cost of maintaining the infrastructure and expertise necessary for dissection
(Gartner, 2003; Korf et al., 2008). There is also evidence that medical schools
are devoting larger proportions of limited curriculum time to, for example, the
development of communication, clinical or research skills, at the expense of
anatomy teaching (Marks, 2002; Sugand et al., 2010; Turney, 2007). These
trends are in turn leading to increased innovation in the way anatomy is taught.
Cadaveric teaching is now supplemented or supplanted by a mixture of
lectures, presentations, physical models and, increasingly, computer
simulations (Tam et al., 2009). While the latter are still dominated by an array of
platforms displaying content in two dimensions (2D), advances in three-
dimensional (3D) imaging have led to the introduction of a number of systems
allowing students to immerse themselves in a virtual reality (VR) environment in
which faithful representations of anatomical regions can be observed and
manipulated.
Most research into the efficacy of such systems and their reception by students
has focused on individual or small group teaching, with 3D models presented on
standard workstations through locally installed programs or using internet-
based, e-learning platforms. Several make use of freely-available datasets,
such as those resulting from the US, Korean and Chinese Visible Human (VH)
projects (Liu et al., 2013; Spitzer et al., 1996), some of which are pre-

Page 4 of 28
Accep
ted
Man
uscr
ipt
segmented (Kockro & Hwang, 2009; Levinson et al., 2007; Liu et al., 2013;
Temkin et al., 2006). In others, reconstructions of clinical or research magnetic
resonance imaging (MRI) or computed tomography scans form the basis of the
models (Gopalakrishnakone et al., 2011; Serra et al., 2002).
While the use of small-group, individual and online teaching using 3D
anatomical models will doubtless increase as the technology and delivery
methods improve, it is likely that medical students will continue to be taught
using a combination of methods, including didactic lectures. No attempt has
hitherto been made to assess the feasibility of presenting 3D models to larger
groups of students to enhance the delivery of such lectures. Although designed
to preoperatively visualise, plan and present neurosurgical interventions in a 3D
environment, the DextroBeam system is a robust and versatile platform for the
display of high resolution, 3D neuroanatomical models via a stereoscopic
projector to large groups (Kockro et al., 2007). We carried out a randomised trial
in which the anatomy of the third ventricle was presented to a large group of
students in a seminar room using a 3D anatomical model or a traditional
PowerPoint presentation with identical content and duration. Efficacy in terms of
anatomical knowledge retained and a subjective evaluation by the students
were recorded.

Page 5 of 28
Accep
ted
Man
uscr
ipt
2. Materials and Methods
Second-year medical students of the University of Mainz, Germany, who had
completed their regular lecture series on cranial anatomy but had yet to begin
their cadaveric dissection neuroanatomy course were recruited to the study.
Participation was voluntary. Students were randomly allocated based on the
initial letter of their surname in groups of approximately 20 to a lecture in which
they would watch either a 2D or 3D presentation. The students participating in
the study did not know the instructors. The sole exclusion criterion was any self-
reported abnormality of stereoscopic vision. Under applicable local legislation,
ethical approval was not required. Permission to carry out the study was
received from the dean’s office.
2.1 2D teaching session
Students allocated to the 2D session watched an automated PowerPoint
presentation (Microsoft, Redmond, USA) in which the topographic anatomy of
the human ventricular system was presented. The presentation was designed
by neurosurgeons with an interest in clinical anatomy teaching. The anatomy
was displayed using images taken from standard textbooks (Fritsch & Kühnel,
2001; Rauber & Kopsch, 1988, 1987; Schünke et al., 2009) and the details
referred to in the commentary were highlighted using arrows and/or coloured
outlines of the respective structures, with the names of the labelled structures
also appearing on the slide. In order to eliminate bias arising from differences in
the speed of delivery of a live, oral presentation, the audio aspect of the
presentation was pre-recorded as an audio file and played in synchrony with the

Page 6 of 28
Accep
ted
Man
uscr
ipt
slides. The script for this audio component (Table 1), in the German language
and consisting of 501 words and created from relevant explanations in three
German anatomy textbooks (Fritsch & Kühnel, 2001; Rauber & Kopsch, 1988,
1987), was recorded using Quicktime (Apple, Cupertino, USA). Playback was
through a laptop connected to the audio system in the seminar room. The
sessions lasted 20 minutes.
2.2 3D teaching session
The 3D teaching session was performed using the DextroBeam system (Bracco
Advanced Medical Technologies, Princeton, USA). This is a stereo-projector
system capable of projecting a stereoscopic image on a special screen. Images
intended for the left and right eye are split using polarising filters placed in front
of the projector’s lens and the 3D image is perceived stereoscopically by
viewers wearing passively polarising glasses. For a detailed discussion of the
system and the technology behind it, please see Serra et al, 2002.
Students were asked to wear stereoscopic glasses for the duration of the
presentation, which was accompanied by the same audio file used in the 2D
presentation. The virtual 3D model (1024 x 768, XGA resolution) used in this
session was created from a cranial MRI and cranial MRI angiogram of a healthy
individual (512 x 512 matrix with 1.5mm slice thickness). The DextroBeam 3D
image processing and segmentation tools were used to create a virtual 3D
ventricular system including all the anatomical structures presented in the 2D
presentation. Anatomical structures mentioned in the audio commentary were
highlighted with the identical colours used for the corresponding structure in the
2D presentation. Using the DextroBeam’s stereoscopic movie recording feature,

Page 7 of 28
Accep
ted
Man
uscr
ipt
we created an animated tour around and through the ventricular anatomy
featuring the same structures, key perspectives and labelling identical to that of
the 2D presentation.
2.3 Multiple-choice questions
Immediately following their teaching session, each participant was asked to
complete a short examination consisting of ten multiple-choice questions
(MCQs) relating to the topographical anatomy of the third ventricle (Table 2).
These questions were not formally validated but were developed and agreed on
by an expert committee of four neurosurgeons and anatomists as being
representative of the level of neuroanatomical knowledge required for success
in the course examinations. They were informally tested on an independent
group of students who had completed their neuroanatomy curriculum.
Participants were given 10 minutes to anonymously answer the questions by
indicating the correct answer. The students then completed an anonymous
questionnaire asking for their age and gender and four questions in which they
could subjectively rate their learning experience (Table 3).
2.4 Statistical methods
Each correct answer in the MCQ examination was awarded one point, with a
maximum of 10 points achievable. There was no negative marking. Statistical
analysis was performed using SPSS v.15 (IBM, Armonk, NY, USA) and JMP
(SAS, Cary, NC, USA). For the analysis of demographic data and the rating
responses, χ-square and a two-sided Fisher’s exact test were employed. A two-
sample, one-sided t-test was used to assess for non-inferiority of the

Page 8 of 28
Accep
ted
Man
uscr
ipt
experimental teaching method. Non-inferiority testing differs from a standard
comparison of means in that the null hypothesis states that the method
assessment (3D teaching) is neither equivalent nor superior to the control
sample (2D teaching). Rejection of the null hypothesis thus confirms the method
being tested is at least equivalent to the sample compared, with equivalence
bounded by a practical equivalence term δ, set a priori in this case as a
difference of 1 point on the MCQ test. Direct comparison of the means was
precluded in our sample as an analysis demonstrated that the sample size
available did not generate sufficient statistical power for an assessment. For all
tests, statistical significance was defined by a p value of ≤ 0.05.
3. Results
3.1 Demographic data
One hundred and sixty-nine students volunteered to take part in this study. As
no student declared an abnormality of stereoscopic vision, all volunteers were
randomised to the 3D or 2D teaching. Eighty-nine (52.7%) watched the 3D, VR
training, with 80 (47.3%) attending the 2D, PowerPoint-based session.
Demographic details were available for all students. Gender distribution was
comparable to that of other German medical schools (Liebhardt et al., 2010),
with 106 (62.7%) female participants. The mean age of students was 22.5 years
(range 20 – 32 years). Students had completed between two and six semesters
of medical school, with a majority (84.6%) in their fourth semester.
3.2 MCQ examination results
The mean score of the ten-question MCQ test performed by students who
watched the 2D presentation was 5.19 (median 5; S.D. 2.12). In the group

Page 9 of 28
Accep
ted
Man
uscr
ipt
receiving 3D teaching, the mean score was 5.45 (median 6; S.D. 2.16). The 3D
presentation was shown to be statistically non-inferior to traditional 2D
presentation (p<0.0001). Comparison of the two means showed a non-
significant trend (p=0.215) towards superiority of 3D teaching, although the
study was underpowered to definitively detect any difference, so this result
should be interpreted with caution. Non-parametric subgroup analysis based on
gender (p=0.145), age group (p=0.458) and number of completed semesters
(p=0.904) did not reveal any significant difference between the groups.
3.3 Results of evaluation questionnaire
The evaluation questionnaire was completed by 100% of student participants.
This high rate of compliance was achieved by presenting the students with the
questionnaire immediately after the MCQ test. Students consistently and
significantly rated the 3D VR presentation sessions more highly compared to
usual teaching than the 2D presentation across all four evaluation domains
(Figure 2; Fisher’s exact test; p<0.001 in all cases).
4. Discussion
Learning neuroanatomy involves the mastery of 3D spatial information as
applied to the structures and relations of the human nervous system. Acquiring
such spatial knowledge necessarily requires the initial perception of 3D
information from which a 3D mental image is constructed by each learner and
which may be continually augmented and refined through further learning and
validation (Marks, 2000). While 3D information may be synthesised from 2D
sources such as books and traditional lectures, one of the strengths of

Page 10 of 28
Accep
ted
Man
uscr
ipt
cadaveric dissection is that spatial relations and complex structures can be
viewed and manipulated in context (Marks, 2000; Older, 2004).
Several groups have presented and/or evaluated VR teaching systems for
undergraduate education. In 2006, Temkin et al described an interactive web-
based 3D model based on the VH dataset, some elements of which were
rendered in blue-red stereoscopic 3D (Temkin et al., 2006). In the same year,
the VH dataset was also used to create an interactive, fully 3D model of the
human temporal bone which was used for neurosurgical training (Kockro &
Hwang 2009). Neither of these systems were subjected to randomised
evaluation. Subsequent trials of related systems yielded mixed results, with VR
teaching of the carpal bones (Garg et al., 1999; Garg et al. 2002; Garg et al.,
2001) and shoulder (Hariri, et al., 2004) not convincingly assessed as superior
to standard teaching, while similar studies in which the middle ear (Nicholson et
al., 2006; Venail et al., 2010) and biliary system (Beermann et al., 2010) were
taught showed a clear benefit of VR. In such small-group settings, VR and other
computer-based methods may not be superior to anatomical models (Khot et
al., 2013; Preece et al., 2013), which are becoming increasingly diverse,
detailed and lifelike as costs fall and 3D printing methods open up new
possibilities.
Such physical models and their virtual counterparts, viewed using workstation-
based or online 3D systems, seek to reproduce the three-dimensionality of
dissection and are now established educational adjuncts in many medical
schools. One disadvantage of such systems, however, is their limited scalability,
with the maximum number of contemporaneous participants limited to around

Page 11 of 28
Accep
ted
Man
uscr
ipt
five. Another drawback, perhaps paradoxically, is that it seems that the more
freedom students are allowed in manipulating and exploring models on their
own, the higher the risk that the learning experience is degraded by time spent
off-task or through key concepts being overlooked (Garg et al., 1999; Levinson
et al., 2007; Phelps et al., 2004; Silén et al., 2008). Many of these tools are
based on concepts allied to the discovery- and enquiry-based schools of
learning theory, which hold that students should be given the tools and freedom
to gain knowledge themselves (Barrows, 1986). Critiques of this approach
argue that expert guidance during the learning process is necessary,
particularly when knowledge is first being accumulated, as students lack the
basic framework to “internally” guide their own learning (Kirschner et al., 2006).
Delivering 3D neuroanatomical content to a larger group as a stereoscopically-
enhanced animated lecture, as described here, allows students to visualise and
lay down memories of structures in 3D while receiving instruction from an expert
neuroanatomist who can ensure the pertinence of the delivered content. While
the presentations used in the study were fully standardised in order to reduce
bias, in everyday use, 3D lectures need not lack interactivity – lecturers can
respond to questions or requests for clarification and illustrate their responses
by manipulating the model.
Despite the relative simplicity of the 3D computer models used in this study –
lacking shadows, texture, detail and haptic elements – the results of the MCQ
test demonstrated that VR teaching in neuroanatomy is at least equivalent in
terms of efficacy to PowerPoint presentations based on elaborate, yet 2D,
textbook representations. The stereoscopic three-dimensionality of VR teaching

Page 12 of 28
Accep
ted
Man
uscr
ipt
directly incorporates the intrinsic spatial relationships of the anatomical sites
studied, and thus may confer a spatial knowledge advantage which is beyond
the ability of MCQs to reliably test. Habitual exposure to this critical aspect of
neuroanatomy during undergraduate training may catalyse the acquisition of the
practical anatomical awareness required, for instance, in a postgraduate
surgical career.
Students exposed to VR teaching in this study overwhelmingly approved of its
use. Three-quarters of students rated the ability of the 3D lecture to convey
spatial understanding as good or very good. This is significant, as traditional
didactic lectures are rated poorly on this aspect, with this method coming last in
a survey of six different anatomy teaching techniques (Kerby et al., 2011), a
finding replicated in the 2D group in this study (24% good / very good). While
the novelty of the 3D VR teaching experience against a possible background of
“PowerPoint fatigue” – presentations using the Microsoft software are
ubiquitous in medical schools – may explain some of the enthusiasm, this
striking finding is in keeping with other studies evaluating the effect of individual
/ small-group VR teaching on student approval and motivation (Beermann et al.,
2010; Garg et al., 2002; Murgitroyd et al., 2015; Silén et al., 2008; Venail et al.,
2010; for a meta-analysis, see Yammine & Violato, 2014). Students motivated
and engaged by innovative learning methods are more likely to learn and retain
knowledge (Battulga et al., 2012; Huang et al., 2010; Shim et al., 2003) and
more engaging teaching may improve learning outcomes indirectly, through
increased overall motivation, improved attendance and inspiring students to use
novel methods in their self-directed learning.

Page 13 of 28
Accep
ted
Man
uscr
ipt
The cost of stereoscopic projectors and polarising glasses have dropped
significantly in recent years and the main cost of acquiring and using such
systems now arises from the proprietary software and expertise necessary to
construct the models. The DextroBeam system is only a step in the rapid
evolution of VR teaching platforms, with novel systems enabling the display of
stereoscopic models without the need for special glasses in development
(Abildgaard et al., 2010). We are currently developing a further teaching
intervention with an upgraded Dextrobeam setup and publication of this data will
hopefully include accompanying videos.
The potential advantages of VR teaching are not limited to undergraduate
application. With limitations on junior surgeons’ working hours and fewer
opportunities to learn surgical anatomy in the operating theatre, immersive 3D
anatomy learning has a role to play in supplementing more traditional methods
at all levels of training (Coulter & Brennan, 2013; Kirkman et al., 2014; Kockro,
2013; Lemole et al., 2007; Murgitroyd et al., 2015; Schirmer et al., 2013)
Previous studies assessing small-group 3D VR anatomy have shown that
individual spatial ability is a predictor of improved learning outcomes following
3D learning (Berney et al., 2015; Phelps et al., 2004; Yammine & Violato, 2014)
and by extension it has been suggested that male students may benefit more
from 3D teaching than females (Battulga et al., 2012; Beermann et al., 2010).
While we did not assess our participants’ spatial ability, our limited subgroup
analysis did not show any such gender effect, nor did age or number of medical
school semesters completed show an association with MCQ results.

Page 14 of 28
Accep
ted
Man
uscr
ipt
Several factors not tested in this study may account for the apparent
discrepancy between the students’ subjectively excellent learning experience
and the statistically indiscernible MCQ results. The study only had one
assessment time-point, immediately after teaching. It may be that the 3D
context provided in stereoscopically-enhanced lectures allows for better
retention of anatomical knowledge over time, meaning the benefit of 3D over 2D
lectures would become apparent only later. Proof of this hypothesis may reveal
a key advantage of 3D teaching and could be achieved by reassessing students
at multiple time-points, something that was beyond the scope of the current
study.
Furthermore, students were not rewarded for good performance in the MCQ
examination, nor did it count towards their grade or chances of progression.
Participation was presented as an opportunity for formative assessment on an
area which was to be tested at the end of the semester. As such, the students
may not have been fully motivated to apply themselves in the test and this may
account for the relatively low mean scores (52-55%) in both groups, although
the test was relatively demanding and consisted of several ranking and
matching questions which must be answered perfectly to score a point.
Finally, the anatomy of the third ventricle was thought to lend itself to 3D
teaching due to its moderate complexity, difficulty to visualise and relevance to
both undergraduate neuroanatomy and neurosurgery (Schirmer et al., 2013).
Previous studies in which superiority of 3D teaching was demonstrated tended
to use more complex regions, such as the temporal bone and biliary tree, as

Page 15 of 28
Accep
ted
Man
uscr
ipt
their substrate (Beermann et al., 2010; Nicholson et al., 2006), while negative
findings were seen using simpler structures. Future studies of 3D teaching
should explore this effect by comparing regions of different complexity, while
also assessing the role of the dimensionality of the teaching substrate on
knowledge retention over serial time-points. The optimal role of VR teaching
may ultimately lie in offering expert teachers the ability to not only demonstrate
the anatomy of a region, but also how to approach and manipulate its structures
efficiently and safely in 3D, something very difficult to achieve with static 2D
images or animations.
5. Conclusion
This study demonstrates that the use of stereoscopic, computer-generated,
anatomical models delivered using a 3D projection system can enhance
undergraduate neuroanatomy lectures. The 3D presentation, despite being
based on a computer model simplified to the extent of merely illustrating the
core 3D anatomical relationships, was shown to be at least as effective as a 2D
presentation using classical textbook drawings. These findings, combined with
the clear preference of the students in favour of the 3D teaching method, should
be taken as encouragement to continue to develop more elaborate, realistic
virtual models and 3D courseware with the aim of providing a high-fidelity,
virtual teaching environment transmitting anatomical knowledge in its inherent,
3D form.
Acknowledgements

Page 16 of 28
Accep
ted
Man
uscr
ipt
The authors thank the medical students of Mainz University who agreed to take
part in this study for their time and enthusiasm. The Clinical Research Priority
Program (CRPP) for Neuro-Rehab of the University of Zurich provided
resources for Tim Killeen.
References
Abildgaard, A., Witwit, A.K., Karlsen, J.S., Jacobsen, E.A., Tennøe, B., Ringstad, G., Due-Tønnessen, P., 2010. An autostereoscopic 3D display can improve visualization of 3D models from intracranial MR angiography. Int. J. Comput. Assist. Radiol. Surg. 5, 549–54.
Barrows, H.S., 1986. A taxonomy of problem-based learning methods. Med. Educ. 20, 481–486.
Battulga, B., Konishi, T., Tamura, Y., Moriguchi, H., 2012. The effectiveness of an interactive 3-dimensional computer graphics model for medical education. Interact. J. Med. Res. 1, e2.
Beermann, J., Tetzlaff, R., Bruckner, T., Schöebinger, M., Müller-Stich, B.P., Gutt, C.N., Meinzer, H.-P., Kadmon, M., Fischer, L., 2010. Three-dimensional visualisation improves understanding of surgical liver anatomy. Med. Educ. 44, 936–40.
Berney, S., Bétrancourt, M., Molinari, G., Hoyek, N., 2015. How spatial abilities and dynamic visualizations interplay when learning functional anatomy with 3D anatomical models. Anat. Sci. Educ. Feb 16, 1-7.
Coulter, I., Brennan, P., 2013. Simulation in Neurosurgery: A Survey of Experiences and Perceptions in the UK. Bull. R. Coll. Surg. Engl. 95, 304–307.
Fritsch, H., Kühnel, W., 2001. Taschenatlas der Anatomie, Band 3, Nervensystem und Sinnesorgane, 7th Editio. ed. Thieme, Stuttgart.
Garg, A., Norman, G., Spero, L., Maheshwari, P., 1999. Do virtual computer models hinder anatomy learning? Acad. Med. 74, S87-9.
Garg, A., Norman, G., Sperotable, L., 2001. How medical students learn spatial anatomy. Lancet 357, 363–364.
Garg, A.X., Norman, G.R., Eva, K.W., Spero, L., Sharan, S., 2002. Is there any real virtue of virtual reality?: the minor role of multiple orientations in learning anatomy from computers. Acad. Med. 77, S97–9.

Page 17 of 28
Accep
ted
Man
uscr
ipt
Gartner, L.P., 2003. Anatomical sciences in the allopathic medical school curriculum in the United States between 1967-2001. Clin. Anat. 16, 434–9.
Gopalakrishnakone, P., Jianfeng, L., Sun, G.P., Abeykoon, A., Noel, O., Fernando, N., Cheok, A.D., 2011. A multimodal virtual anatomy learning tool for medical education. [Online] Available from http://www.academia.edu/1268456/A_Multimodal_Virtual_Anatomy_Learning_Tool_for_Medical_Education. Accessed 17th April 2015.
Hariri, S., Rawn, C., Srivastava, S., Youngblood, P., Ladd, a, 2004. Evaluation of a surgical simulator for learning clinical anatomy. Med. Educ. 38, 896–902.
Huang, H.-M., Rauch, U., Liaw, S.-S., 2010. Investigating learners’ attitudes toward virtual reality learning environments: Based on a constructivist approach. Comput. Educ. 55, 1171–1182.
Kerby, J., Shukur, Z.N., Shalhoub, J., 2011. The relationships between learning outcomes and methods of teaching anatomy as perceived by medical students. Clin. Anat. 24, 489–97.
Khot, Z., Quinlan, K., Norman, G.R., Wainman, B., 2013. The relative effectiveness of computer-based and traditional resources for education in anatomy. Anat. Sci. Educ. 6, 211–215.
Kirkman, M. a, Ahmed, M., Albert, A.F., Wilson, M.H., Nandi, D., Sevdalis, N., 2014. The use of simulation in neurosurgical education and training. J. Neurosurg. 121, 228–46.
Kirschner, P.A., Sweller, J., Clark, R.E., 2006. Why minimal guidance during instruction does not work: an analysis of the failure of constructivist, discovery, problem-based, experiential, and inquiry-based teaching. Educ. Psychol. 41, 75–86.
Kockro, R., Hwang, P., 2009. Virtual Temporal Bone: An Interactive
3‐Dimensional Learning Aid for Cranial Base Surgery. Neurosurgery 64,
216–230.
Kockro, R.A., 2013. Neurosurgery Simulators - Beyond the Experiment. World Neurosurg. 80, 120–121.
Kockro, R.A., Stadie, A., Schwandt, E., Reisch, R., Charalampaki, C., Ng, I., Yeo, T.T., Hwang, P., Serra, L., Perneczky, A., 2007. A collaborative virtual reality environment for neurosurgical planning and training. Neurosurgery 61, 379–91.

Page 18 of 28
Accep
ted
Man
uscr
ipt
Korf, H.-W., Wicht, H., Snipes, R.L., Timmermans, J.-P., Paulsen, F., Rune, G., Baumgart-Vogt, E., 2008. The dissection course - necessary and indispensable for teaching anatomy to medical students. Ann. Anat. 190, 16–22.
Lemole, G.M., Banerjee, P.P., Luciano, C., Neckrysh, S., Charbel, F.T., 2007. Virtual reality in neurosurgical education: part-task ventriculostomy simulation with dynamic visual and haptic feedback. Neurosurgery 61, 142–8.
Levinson, A.J., Weaver, B., Garside, S., McGinn, H., Norman, G.R., 2007. Virtual reality and brain anatomy: a randomised trial of e-learning instructional designs. Med. Educ. 41, 495–501.
Liebhardt, H., Fegert, J., Dittrich, W., Nürnberger, F., 2010. Medizin studieren mit Kind. Ein Trend der Zukunft. Dtsch Arztebl 107, 1613–1615.
Liu, K., Fang, B., Wu, Y., Li, Y., Jin, J., Tan, L., Zhang, S., 2013. Anatomical education and surgical simulation based on the Chinese Visible Human: a three-dimensional virtual model of the larynx region. Anat. Sci. Int. 88, 254–258.
Marks, S.C., 2002. Clinical Anatomy for Health Care and Medical Education in the 21 st Century. J. Japanese Res. Soc. Clin. Anat. 1, 4–7.
Marks, S.C., 2000. The role of three-dimensional information in health care and medical education: the implications for anatomy and dissection. Clin. Anat. 13, 448–52.
Murgitroyd, E., Marduska, M., Gonzalez, J., Watson, A., 2015. 3D digital anatomy modelling – Practical or pretty? Surgeon. 2–5.
Nicholson, D.T., Chalk, C., Funnell, W.R.J., Daniel, S.J., 2006. Can virtual reality improve anatomy education? A randomised controlled study of a computer-generated three-dimensional anatomical ear model. Med. Educ. 40, 1081–7.
Older, J., 2004. Anatomy: A must for teaching the next generation. Surgeon. 2, 79–90.
Phelps, A., Fritchle, A., Hoffman, H., 2004. Passive vs. active virtual reality learning: The effects on short- and long-term memory of anatomical structures. Stud. Health Technol. Inform. 98, 298-300.
Preece, D., Williams, S.B., Lam, R., Weller, R., 2013. “Let’s Get Physical”: Advantages of a physical model over 3D computer models and textbooks in learning imaging anatomy. Anat. Sci. Educ. 6, 216–224.
Rauber, A., Kopsch, F., 1988. Anatomie des Menschen Lehrbuch und Atlas, Band IV: Topographie der Organsysteme, Systematik der Leitungsbahnen. Thieme, Stuttgart.

Page 19 of 28
Accep
ted
Man
uscr
ipt
Rauber, A., Kopsch, F., 1987. Anatomie des Menschen Lehrbuch und Atlas, Band III. Nervensystem Sinnesorgane. Thieme, Stuttgart.
Schirmer, C.M., Elder, J.B., Roitberg, B., Lobel, D. a., 2013. Virtual reality-based simulation training for ventriculostomy: An Evidence-based approach. Neurosurgery 73, 66–73.
Schünke, M., Schulte, E., Schumacher, U., Voll, M., Wesker, K., 2009. Prometheus LernAtlas der Anatomie: Kopf, Hals und Neuroanatomie, 2nd Editio. ed. Thieme, Stuttgart.
Serra, L., Kockro, R., Goh, L.C., Ng, H., Lee, E.C.K., 2002. The DextroBeam: a stereoscopic presentation system for volumetric medical data. Stud. Health Technol. Inform. 85, 478–84.
Shim, K.-C., Park, J.-S., Kim, H.-S., Kim, J.-H., Park, Y.-C., Ryu, H.-I., 2003. Application of virtual reality technology in biology education. J. Biol. Educ. 37, 71–74.
Silén, C., Wirell, S., Kvist, J., Nylander, E., Smedby, O., 2008. Advanced 3D visualization in student-centred medical education. Med. Teach. 30, e115–e124.
Spitzer, V., Ackerman, M.J., Scherzinger, a L., Whitlock, D., 1996. The visible human male: a technical report. J. Am. Med. Informatics Assoc. 3, 118–130.
Sugand, K., Abrahams, P., Khurana, A., 2010. The anatomy of anatomy: a review for its modernization. Anat. Sci. Educ. 3, 83–93.
Tam, M., Hart, A., Williams, S., 2009. Is learning anatomy facilitated by computer-aided learning? A review of the literature. Med. Teach. 31, 393–396.
Temkin, B., Acosta, E., Malvankar, A., Vaidyanath, S., 2006. An interactive three-dimensional virtual body structures system for anatomical training over the internet. Clin. Anat. 19, 267–74.
Turney, B.W., 2007. Anatomy in a modern medical curriculum. Ann. R. Coll. Surg. Engl. 89, 104–7.
Venail, F., Deveze, A., Lallemant, B., Guevara, N., Mondain, M., 2010. Enhancement of temporal bone anatomy learning with computer 3D rendered imaging software. Med. Teach. 32, e282–8.
Yammine, K., Violato, C., 2014. A meta-analysis of the educational effectiveness of three-dimensional visualization technologies in teaching anatomy. Anat. Sci. Educ. Dec 31, 1-14.

Page 20 of 28
Accep
ted
Man
uscr
iptTable 1. Full transcript of accompanying audio track played alongside both
2D and 3D presentations. Translated from the original German.
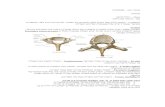
Along its lateral axis, the unpaired third ventricle is small, but is relatively extensive in the dorso-ventral plane. The ventricle has a floor and, from the roof posteriorly, expansions known as recesses. Rostrally, the third ventricle is connected to both lateral ventricles through the intraventricular foraminae. Caudally, the ventricle is continuous with the mesencephalic cerebral aqueduct although the longitudinal axis of the ventricle – a line connecting the rostral and posterior epithalamic commisures – is angulated ventrally with respect to the long axis of the aqueduct.
The roof of the third ventricle consists of the tela chorioidea with the choroid plexus of the third ventricle. The latter continues as the choroid plexus of the lateral ventricle in the region of the intraventricular foramina. In the epithalamus, the suprapineal recess arches dorsally over the pineal gland. The pineal recess forms a shallow hollow in the pineal gland. Above the pineal recess cross the fibres of the habenular commissure, while the epithalmic commissure lies under the recess.
The anterior wall of the third ventricle is formed by the lamina terminalis. The lamina terminalis is bounded caudally by the optic recess, formed from the horizontal bulge produced by the optic chiasm. Behind the optic chiasm, the funnel-shaped infundibulum and the infundibular recess form a convex impression in the floor of the ventricle.
The floor of the ventricle is part of the hypothalamus and consists mainly of a thin, grey lamella. The infundibulum continues as the pituitary stalk. Behind the infundibulum lies the tuber cinereum, beyond which are found the paired mammillary bodies. In the large, upper part of the lateral walls, the thalamus bulges out in the form of a flat oval. In 75% of cases, at variable positions and to varying degrees, the two thalami are connected through the ventricular lumen by the interthalamic adhesion (massa intermedia). Caudal to the floor of the third ventricle, in the angle formed by the floor of the midbrain, the cerebral peduncles and the pons, lies the interpeduncular cistern before which, surrounding the chiasm, is the chiasmatic cistern. In the interpeduncular cistern the basilar artery bifurcates in the interpendicular fossa behind the mammillary bodies into the two posterior cerebral arteries. In relation to the skull base, this bifurcation is usually at the level of the dorsum sellae.

Page 21 of 28
Accep
ted
Man
uscr
ipt
Table 2. Multiple choice questions on the applied anatomy of the third
ventricle. Correct responses in bold italic type.
1. Order the following epithalamic structures in the correct order, from cranial to caudal.
1. Cerebral aqueduct2. Suprapineal recess3. Habenular commissure4. Pineal recess
a. 1-3-4-2b. 2-3-1-4c. 4-1-3-2d. 2-3-4-1e. 3-4-1-2
2. Which structure lies beneath the floor of the third ventricle and may be injured during its perforation?
a. Lamina terminalisb. Basilar arteryc. Interventricular foramen of
Monroed. Optic chiasme. Thalamus
3. Which structure often hinders direct access from the interventricular foramen to the cerebral aqueduct?
a. Interthalamic adhesionb. Thalamusc. Commisura habenularumd. Pineal bodye. Optic chiasm
4. Which response(s) is/are correct?1. The neurosurgeon can gain access to the
third ventricle by opening the lamina terminalis.
2. Access from the fourth ventricle to the third ventricle can be gained through the interventricular foramen.
3. The thalamus can be found in the floor of the third ventricle.
a. 1 and 3 are correctb. 1, 2 and 3 are correctc. Only 1 is correctd. Only 2 is correcte. No response is correct
5. Which structure can the surgeon follow through the interventricular foramen from the lateral to the third ventricle?
a. Pineal recessb. Choroid plexusc. Epithalamic commissured. Infundibulume. Mammillary bodies
6. Which structure can be found in the floor of the third ventricle?
1. Infundibular recess2. Interthalamic adhesion3. Pineal recess4. Mammillary bodies
a. 1, 3 and 4 are correctb. 2 and 4 are correctc. Only 4 is correctd. Only 2 is correcte. 1 and 4 are correct
7. Which structure is found along the caudal extension of a line drawn between the interventricular foramen and the tubercinereum?
a. Choroid plexusb. Suprapineal recessc. Lamina terminalisd. Interpeduncular cisterne. Cerebral aqueduct

Page 22 of 28
Accep
ted
Man
uscr
ipt
8. Order these anatomical structures in the following order: cranial – caudal – rostral –dorsal – lateral
1. Lamina terminalis2. Mammillary bodies3. Thalamus4. Choroid plexus5. Pineal recess
a. 1-2-3-4-5b. 4-2-1-5-3c. 4-2-5-1-3d. 4-5-3-2-1e. 2-4-3-5-1
9. Which of the following statements is correct?
1. The epithalamic commissure forms the upper border of the entrance of the cerebral aqueduct.
2. The habenular commissure merges with the pineal body.
3. The pineal body lies dorsal to the pineal recess.
a. All statements are correctb. Only 1 is correctc. Only 2 is correctd. Only 3 is correcte. Statements 1 and 3 are
correct
10. The choroid plexus is found on which aspect of the third ventricle?
a. Cranialb. Caudalc. Laterald. Anteriore. Posterior
Table 3. Subjective evaluation questions given completed by all students
immediately after either 2D or 3D neuroanatomy teaching.
Question Response 2D group; n(%) 3D group; n(%)1. This teaching method’s usefulness in imparting spatial understanding of the topographical anatomy of the third ventricle is…
Very goodGoodAveragePoorVery Poor
7 (8.8)12 (15)48 (60)9 (11.3)4 (5)
15 (16.9)52 (58.4)21 (23.6)0 (0)0 (0)
2. This method of teaching should be used in future courses.
Agree stronglyAgree somewhatNeutralDisagree somewhatDisagree strongly
18 (22.5)21 (26.3)15 (18.8)24 (30)2 (2.5)
58 (65.2)28 (31.5)2 (2.2)0 (0)0 (0)
3. This method of teaching anatomy is an effective and practical tool for teaching anatomy.
Agree stronglyAgree somewhatNeutralDisagree somewhatDisagree strongly
23 (28.7)20 (25)8 (10)28 (35)1 (1.3)
70 (78.7)19 (21.3)0 (0)0 (0)0 (0)
4. This method of teaching was enjoyable.
Agree stronglyAgree somewhatNeutralDisagree somewhatDisagree strongly
12 (15)12 (15)33 (41.3)21 (26.3)2 (2.5)
19 (21.3)50 (56.2)18 (20.2)2 (2.2)0 (0)

Page 23 of 28
Accep
ted
Man
uscr
iptFigure Legends
Figure 1. Screenshots from the 2D presentation, delivered using Microsoft
PowerPoint. The presentation was played automatically. A - D show examples
of the slides used in order of presentation. Structures were labelled, with the
wording used consistent between 2D and 3D presentations.
Figure 2. Screenshots from the 3D presentation, delivered using the
DextroBeam system. A) 3D overview of the position of the third ventricle within
the head. The automatic presentation then proceeds to zoom to the region of
interest (B), before proceeding to present the anatomical structures in turn (Fig.
3). Colouring is as follows: off-white; skull base, light blue; ventricular system,
yellow; optic nerves, red; blood vessels, green (anterior); tuber cinereum, green
(posterior); pineal body, dark blue; recessus opticus.
Figure 3. Further screenshots from the 3D presentation. The presentation
moves smoothly between key views in a “tour” of the anatomy consistent in
content and order with those of the 2D presentation. Colouring is as follows: off-
white; skull base, yellow; cranial nerves, red; blood vessels, green (anterior);
tuber cinereum, green (posterior); pineal body, blue; recessus opticus, lilac;
pituitary stalk, purple; choroid plexus, pink; mammillary bodies. As the
screenshots are from a 3D tour, in some images (notably Fig. 3, D), the targets
of the labelling are partially obscured by overlapping imagery. When viewed in

Page 24 of 28
Accep
ted
Man
uscr
ipt
stereoscopic 3D, the labels are aligned with their respective targets so that
clarity is maintained.
Figure 4. Results of the MCQ test showing the percentage of students in
each group achieving particular scores out of 10.

Page 25 of 28
Accep
ted
Man
uscr
ipt
Figure 1

Page 26 of 28
Accep
ted
Man
uscr
ipt
Figure 2

Page 27 of 28
Accep
ted
Man
uscr
ipt
Figure 3

Page 28 of 28
Accep
ted
Man
uscr
ipt
Figure 4