
Statistics about unknown primary tumors Riccardo Capocaccia National Centre for Epidemiology,...
21
Statistics about unknown primary tumors Riccardo Capocaccia National Centre for Epidemiology, Surveillance and Health Promotion Istituto Superiore di Sanità, Rome
-
Upload
morgan-lambert -
Category
Documents
-
view
214 -
download
0
Transcript of Statistics about unknown primary tumors Riccardo Capocaccia National Centre for Epidemiology,...

Statistics about unknown primary tumors
Riccardo Capocaccia
National Centre for Epidemiology, Surveillance and Health Promotion
Istituto Superiore di Sanità, Rome

Content
• Source of population-based data
• Definition of Unknown Primary Tumours
• Morphological groups
• Analysis of incidence and survival by morphological group, age, sex, time, population
• Estimates of cure
• Conclusions

Population-based Cancer Registries
• Collect data from all cancer patients diagnosed in a defined population
• Sources: pathology reports, death certificates, hospital admission/discharge, population archives, clinical records, drugs, etc.
• Exhaustive and representative data• Relevant clinical information often missing• Follow-up only for vital status• Information generally collected at the beginning
of the diagnostic workup
Aims of population-based Cancer Registries
• Providing cancer incidence data
• Etiological studies
• Providing survival data
• Providing prevalence data
• Providing information for Health Care management: impact of prevention, diagnostic delay, adherence to guidelines, costs, etc.

Survival studies
Clinical
• RCT: evaluation of the effectiveness of treatment
• Patients selected by hospital, age, stage, co-morbidity
• Indicate the highest achievable survival in selected patient groups
• Ad hoc data collection design
Population-based
• Evaluation of the effectiveness of the heath care systems
• Include all cancer patients belonging to a demographically defined population (country, region, local area, ...)
• Estimate the average survival actually achieved in the general population
• Data currently collected by disease (cancer) registries

EUROCARE-4• 23 countries
• 93 cancer registries
• 13.5 millions patients
• Diagnosed 1978-2002
• Follow-up to Dec 31, 2003
• ICD-O 3 classification (topo/morpho)
• malignant tumours only
NORTH ICELANDNORTH ICELAND FINLANDFINLAND SWEDENSWEDEN NORWAYNORWAY DENMARKDENMARKUK & IRELAND UK & IRELAND ENGLAND ENGLAND WALESWALES SCOTLANDSCOTLAND IRELANDIRELAND N. IRELANDN. IRELAND EAST Poland Czech Republic CENTRE NetherlandsCENTRE Netherlands GermanyGermany BelgiumBelgium AUSTRIAAUSTRIA SwitzerlandSwitzerland FranceFranceSOUTH ItalySOUTH Italy SpainSpain PortugalPortugal MALTAMALTA SLOVAKIASLOVAKIA

EUROCARE-4 GEOGRAPHIC COVERAGEEUROCARE-4 GEOGRAPHIC COVERAGE
South and West Europe
United Kingdom
Eastern Europe
Nordic countries

Data available
• Demographic: age, sex, place of living• Vital status• Dates: birth, diagnosis, death• Diagnosis: site (IVDO-3), morphology
(ICDO-3), microscopic verification
• sparsely: stage at diagnosis• no grading• no treatment

Unknown Primary Cancers(UPC or CUP)
We start analysing all incident cases with topography code C80.9, irrespective of histology.
This definition selects a number of 343,425 UPC incident cases from a total of 9,256,282 cancer diagnoses during the period 1978-2002, with an overall proportion of 3.7 %.

Morphology distribution of UPC: percent of all cancers
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
1978-2002
other
lymphoma
mesothelioma
sarcoma
melanoma
neuroendocrine
mucinous
adenocarcinoma
squamous
carcinoma NOS
cancer NOS

Unknown Primary Cancers
We finally define UPC as incident cases of solid tumours and topography code C80.9.
This definition selects a number of 316,625 UPC incident cases from a total of 9,256,282 cancer diagnoses during the period 1978-2002, with an overall proportion of 3.4 %, that becomes 3.2 % in 1995-2002
Comparisons with other studies
• Randèn et al (Sweden) Acta Oncol 2009: about 2.7%
• Levi et al (Switzerland) Eur J Cancer 2002: 2%
• Muir (USA) Cancer, 1995: 2%
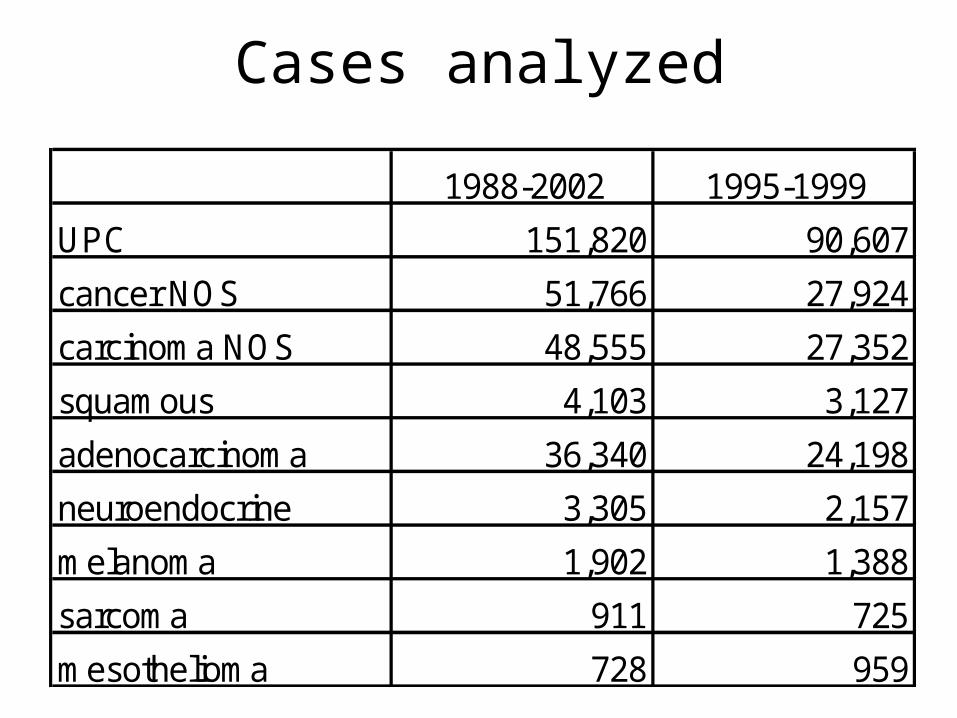
Cases analyzed
1988-2002 1995-1999
UPC 151,820 90,607
cancer NOS 51,766 27,924
carcinoma NOS 48,555 27,352
squamous 4,103 3,127
adenocarcinoma 36,340 24,198
neuroendocrine 3,305 2,157
melanoma 1,902 1,388
sarcoma 911 725
mesothelioma 728 959
Unknown Primary Cancers
• Incidence rates about 11x100,000, higher for men and slightly decreasing
• Survival poor: 10% at 1 year, 7% at 5 years
• Survival not differing by gender• Survival highly variable with age and
between populations• Probable lack of standardization in
registration and coding procedures

Cancer NOS
• Account for 1/3 of all UPC
• Incidence rates about 3x100,000, higher for men and decreasing
• Survival poor, not differing by gender, but much better for age < 30

Carcinoma NOS
• Accounts for another 1/3 of all UPC
• Incidence rates about 3x100,000, higher for men and slightly decreasing
• Survival poor: 9% at 1 year, 4% at 5 years
• Survival not differing by gender
• Survival still variable with age, but less that for Cancer NOS

Adenocarcinoma
• Incidence increasing, abour 3x100,000 in 2001
• Incidence higher for men
• Survival not exceeding 10% at 5 years for all age classes
• Survival not differing by gender
Squamous Cell Carcinoma
• Incidence stable, about 0.3x100,000
• M/F ratio = 2
• Survival 45% at 1 year, 30% at 5 years
• Survival better for men
• Survival decreasing with age

Neuroendocrine Cancers
• Incidence rates sharply increasing up to 0.4 x 100,000 in 2001
• Survival at 40% at 1 year, 15% at 5 years, and continues decreasing
• Survival higher for women and for ages <50

Other Specific Morphologies
• Incidence rates increasing
• Survival very poor for mesothelioma, intermediate (50% at 1 year) for sarcoma and melanoma
• Survival not differing by gender
• Survival better for age <30 for sarcoma, not very dependent on age for melanoma and mesothelioma

Conclusions
• UPC represent in Europe about 3.4% of all cancer diagnoses• They report for 2/3 unspecific and for 1/3 specific
morphologies• Incidence is decreasing for unspecific and increasing or
stable for specific ones• Survival is generally poor, intermediate for SCC, sarcoma
and melanoma• In almost all groups, it is better for women and for young age
classes• No evidence for increasing survival apart from SCC• There is suggestion that a limited proportion of cases can be
cured• Cancer registries may tend to overreport UPC cases when
the site of origins is detected late • Need for a higher degree of standardization in rporting and
coding practices


















