
Starting SGLT-2 inhibitors before Incretin Therapies - Is Empagliflozin...
37
Starting SGLT-2 inhibitors before Incretin Therapies - Is Empagliflozin a Game Changer? Fernando Ovalle, MD Professor of Medicine Division of Endocrinology, Diabetes & Metabolism University of Alabama at Birmingham School of Medicine
Transcript of Starting SGLT-2 inhibitors before Incretin Therapies - Is Empagliflozin...

Starting SGLT-2 inhibitors before Incretin Therapies
- Is Empagliflozin a Game Changer?
Fernando Ovalle, MD Professor of Medicine
Division of Endocrinology, Diabetes & Metabolism University of Alabama at Birmingham School of Medicine

Presenter Disclosures
Types of Support –
• Advisory Panel / Consultant - Lilly, NovoNordisk, Janssen, Sanofi • Board Member - none • Employee - none • Research Support – NIH, JDRF, UAB, Merck, AstraZeneca, Sanofi, NovoNordisk,
GlaxoSmitKline, Janssen, Lilly, Medtronic, Pfizer, GI Dynamics • Speaker’s Bureau – Janssen, Novo Nordisk • Stock/Shareholder - none • Other - none
Fernando Ovalle, MD

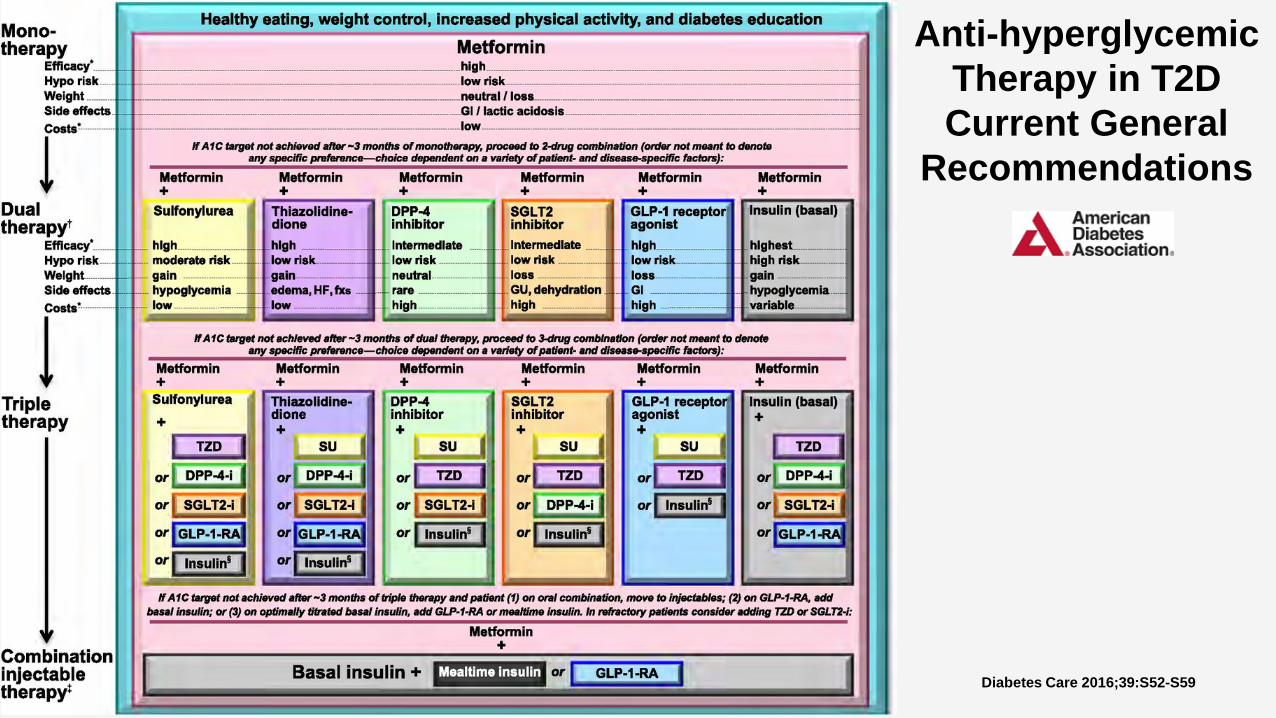
Anti-hyperglycemic Therapy in T2D Current General
Recommendations
Diabetes Care 2016;39:S52-S59

UKPDS Study Group. Lancet 1998; 352:837–853.
Reasons for the current approach UKPDS: intensive glucose control reduces complications in T2D
UKPDS randomized years
0
6
7
8
9
0 5 10 15
Conventional
Intensive
6.2% = upper limit of normal range Med
ian
HbA
1C (%
)
–30
–25
–20
–15
–10
–5
0
Rel
ativ
e ris
k re
duct
ion
(%)
12%
25%
16%
6%
P = 0.029
P = 0.0099
P = 0.052
P = 0.44

Stratton IM et al. BMJ. 2000;321(7258):405-412.

No prior heart attack Prior heart attack
5
0
10
15
20
25
30
35
40
50
Inci
den
ce (%
)
People without diabetes People with diabetes
INCIDENCE OF MYOCARDIAL INFARCTION IN SUBJECTS WITH TYPE 2 DIABETES AND IN NONDIABETIC SUBJECTS WITH AND WITHOUT PRIOR
MYOCARDIAL INFARCTION OVER A PERIOD OF SEVEN YEARS
Adapted from N Engl J Med 1998;339:229-34
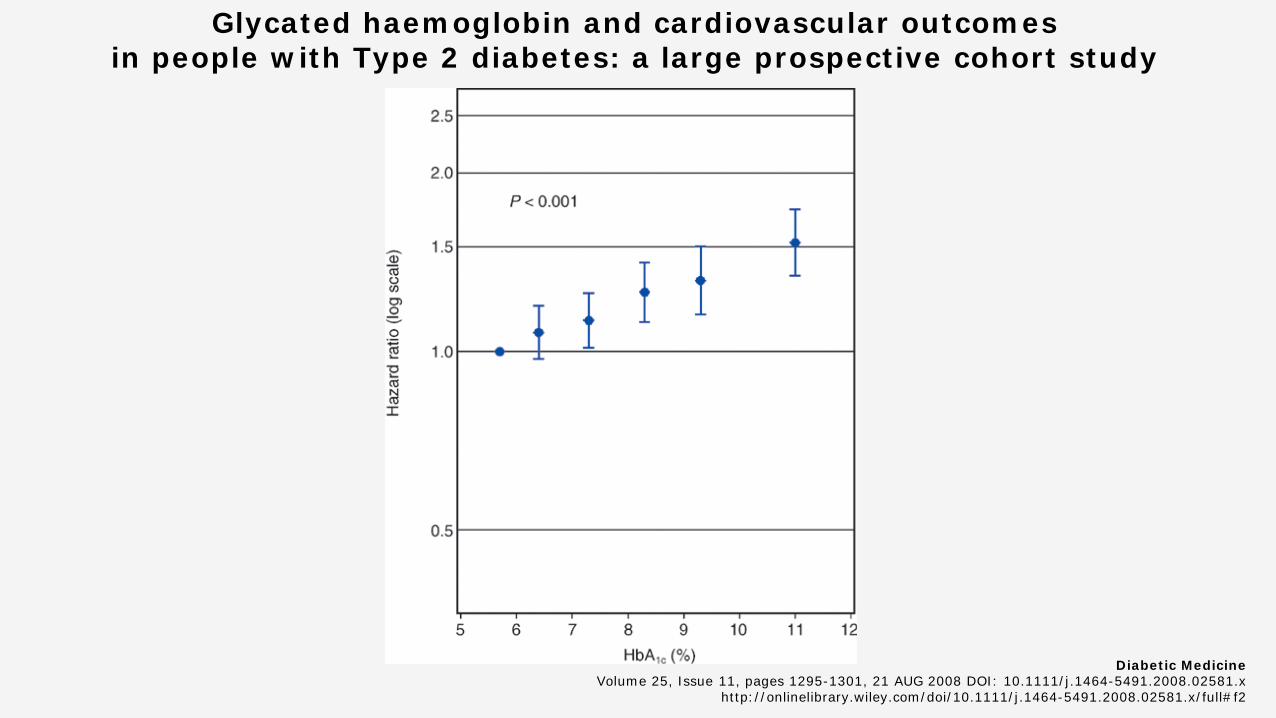
Glycated haemoglobin and cardiovascular outcomes in people with Type 2 diabetes: a large prospective cohort study
Diabetic Medicine Volume 25, Issue 11, pages 1295-1301, 21 AUG 2008 DOI: 10.1111/j.1464-5491.2008.02581.x
http://onlinelibrary.wiley.com/doi/10.1111/j.1464-5491.2008.02581.x/full#f2

Meta-analysis: impact of intensive glucose control on coronary heart disease* events
Reproduced from Ray KK, et al. Lancet 2009; 373:1765–1772.
Intensive treatment/standard treatment
Odds ratio (95% CI)
Odds ratio (95% CI)
Participants Events
UKPDS 3,071/1549 426/259 0.75 (0.54–1.04)
PROactive 2,605/2633 164/202 0.81 (0.65–1.00)
ADVANCE 5,571/5,569 310/337 0.92 (0.78–1.07)
VADT 892/899 77/90 0.85 (0.62–1.17)
ACCORD 5,128/5123 205/248 0.82 (0.68–0.99)
Overall 17,267/15,773 1,182/1,136 0.85 (0.77–0.93)
0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
Intensive treatment better Standard treatment better
*Included non-fatal myocardial infarction and death from all cardiac mortality.
Anti-hyperglycemic Therapy in T2D Current General
Recommendations
Diabetes Care 2016;39:S52-S59
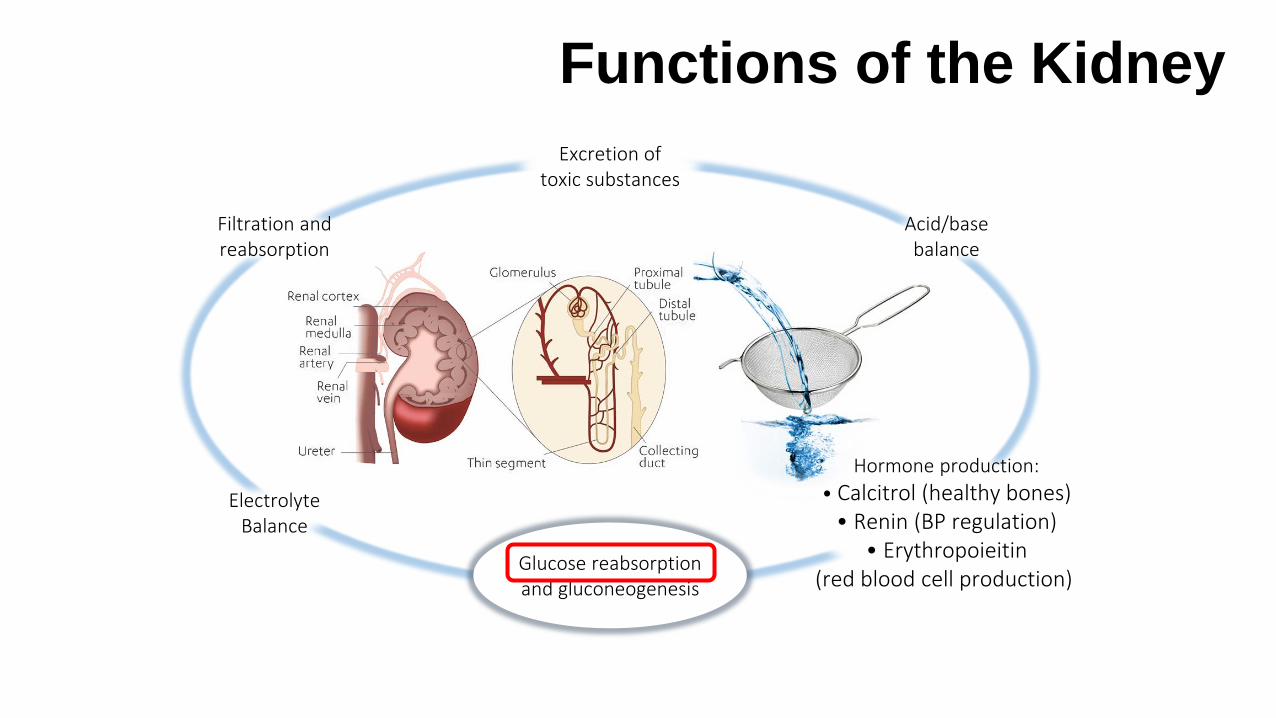
Functions of the Kidney
Filtration and reabsorption
Acid/base balance
Electrolyte Balance
Excretion of toxic substances
Hormone production: • Calcitrol (healthy bones)
• Renin (BP regulation) • Erythropoieitin
(red blood cell production) Glucose reabsorption and gluconeogenesis
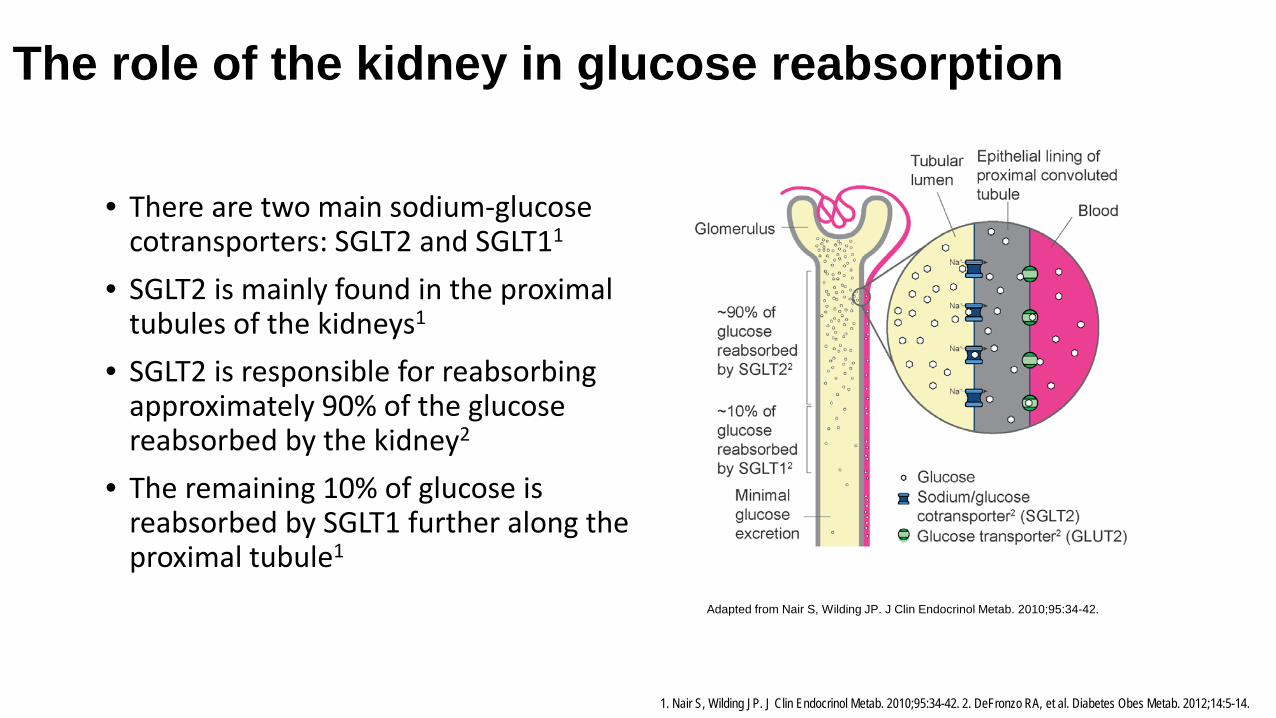
• There are two main sodium-glucose cotransporters: SGLT2 and SGLT11
• SGLT2 is mainly found in the proximal tubules of the kidneys1
• SGLT2 is responsible for reabsorbing approximately 90% of the glucose reabsorbed by the kidney2
• The remaining 10% of glucose is reabsorbed by SGLT1 further along the proximal tubule1
Adapted from Nair S, Wilding JP. J Clin Endocrinol Metab. 2010;95:34-42.
1. Nair S, Wilding JP. J Clin Endocrinol Metab. 2010;95:34-42. 2. DeFronzo RA, et al. Diabetes Obes Metab. 2012;14:5-14.
The role of the kidney in glucose reabsorption

The role of the kidney in glucose reabsorption
References: 1. DeFronzo RA, Davidson JA, Del Prato S. The role of the kidneys in glucose homeostasis: a new path towards normalizing glycaemia. Diabetes Obes Metab. 2012 Jan;14(1):5-14. 2. Clifford J. Bailey. Medscape Education Diabetes & Endocrinology. The Role of the Kidney in Glucose Control.. CME Released: 02/26/2013 ; Valid for credit through 02/26/2014.
~180L filtered per day by the kidney1
A normal kidney A kidney in a patient with type 2 diabetes
Average blood glucose of ~100mg/dL2 Average blood glucose of ~150mg/dL2
~180g of glucose filtered per day2
No increase in SGLT2 cotransporters2
~250g of glucose filtered per day2
glucose reabsorption and elimination of glucose in the urine2
Hyperglycaemia
Increase in SGLT2 cotransporters2

Overview of approved SGLT-2 inhibitors by FDA

Diabetes, Obesity and Metabolism, 2013; 15: 372-382
Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise
Blood Glucose effect of SGLT2 inhibitors

Diabetes, Obesity and Metabolism, 2013; 15: 372-382
Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise
Blood Glucose effect of SGLT2 inhibitors

Blood Pressure effect of SGLT2 inhibitors
Change in (A) systolic blood pressure (SBP) and (B) diastolic blood pressure (DBP) for the overall population and for patients with SBP ≥140 mm Hg and DBP ≥90 mm Hg (last observation carried forward [LOCF]). LS indicates least-squares; SE, standard error; CI, confidence interval; PBO, placebo; CANA, canagliflozin.
The Journal of Clinical Hypertension, 2014; 16

Diabetes, Obesity and Metabolism, 2013; 15: 372-382
Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise
Body weight effect of SGLT2 inhibitors
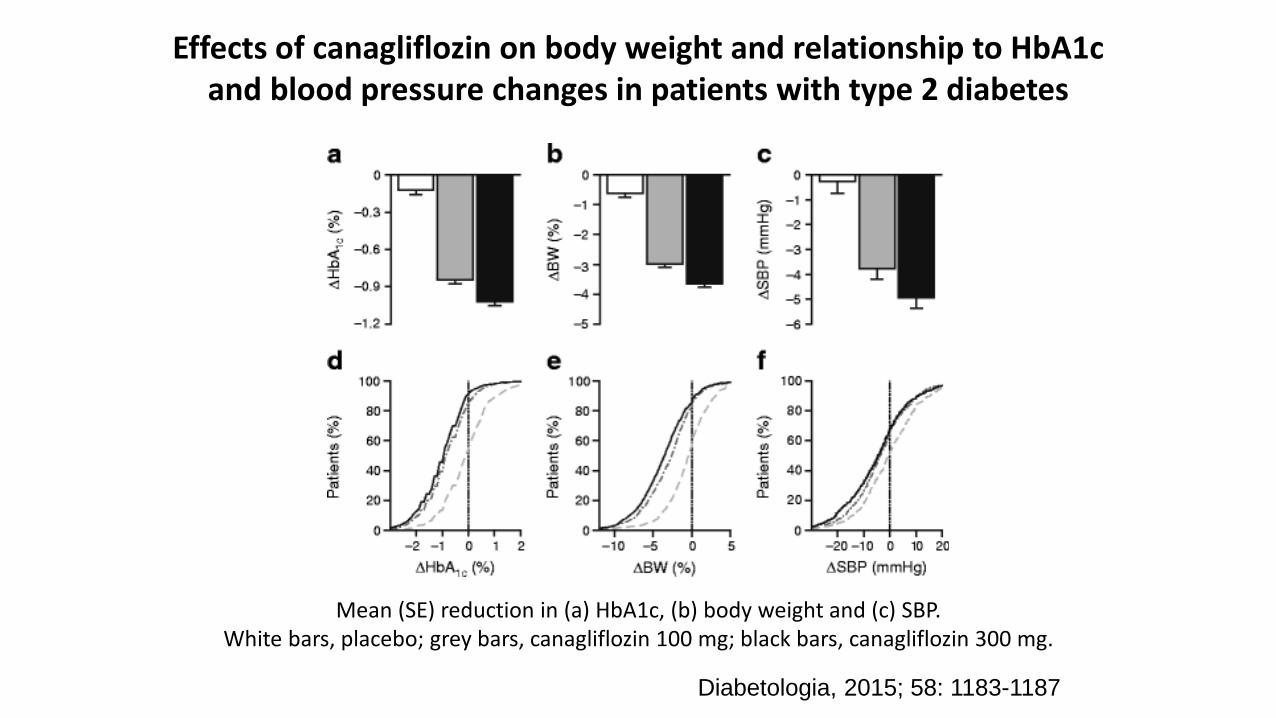
Effects of canagliflozin on body weight and relationship to HbA1c and blood pressure changes in patients with type 2 diabetes
Mean (SE) reduction in (a) HbA1c, (b) body weight and (c) SBP. White bars, placebo; grey bars, canagliflozin 100 mg; black bars, canagliflozin 300 mg.
Diabetologia, 2015; 58: 1183-1187

Undesirable side effects • Genitourinary infections • Volume related events – orthostasis • Bone? (mostly long bones, related to falls) • Bladder cancer? • Diabetes Ketoacidosis • Lower extremity amputations?
Other effects • LDL HDL Triglycerides • HGP Glucagon

SGLT-2 inhibitor effect on Endogenous Glucose Production
Basal EGP before and after ingestion of dapagliflozin or placebo EGP was measured on day 0 with the euglycemic clamp, on days 1 and 2 before subjects ingested dapagliflozin or placebo, and on days 2, 3, and 14 during dapagliflozin treatment.
J Clin Invest. 2014;124(2):509–514. doi:10.1172/JCI70704
Plasma glucose, insulin, and glucagon concentrations and EGP in the study. On day 2, the 3H-glucose infusion was started 3 hours before drug ingestion (time 0) and continued for 4 hours after drug ingestion
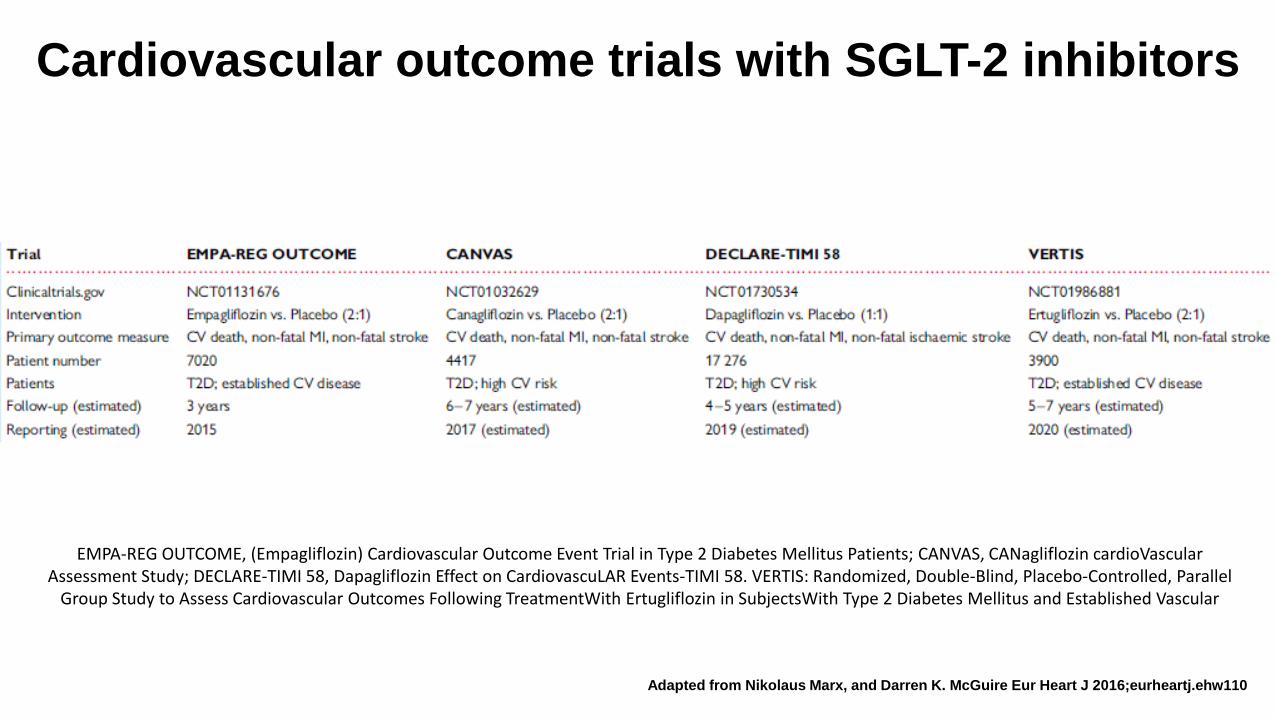
Cardiovascular outcome trials with SGLT-2 inhibitors
EMPA-REG OUTCOME, (Empagliflozin) Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients; CANVAS, CANagliflozin cardioVascular Assessment Study; DECLARE-TIMI 58, Dapagliflozin Effect on CardiovascuLAR Events-TIMI 58. VERTIS: Randomized, Double-Blind, Placebo-Controlled, Parallel
Group Study to Assess Cardiovascular Outcomes Following TreatmentWith Ertugliflozin in SubjectsWith Type 2 Diabetes Mellitus and Established Vascular
Adapted from Nikolaus Marx, and Darren K. McGuire Eur Heart J 2016;eurheartj.ehw110

EMPA-REG OUTCOME - Trial design Objective - to examine the long-term effects of empagliflozin versus placebo, in addition to standard of care, on CV morbidity and mortality in patients with type 2 diabetes and high risk of CV events Randomized, double-blind, placebo-controlled CV outcomes trial Total Randomized and Treated (n=7020)
• Placebo (n=2333) • Empagliflozin 10 mg (n=2345) • Empagliflozin 25 mg (n=2342)
• Study medication was given in addition to standard of care. • Key inclusion criteria:
• Adults with type 2 diabetes and CV disease (heart attack, stroke, etc.) • HbA1c 7–10%; eGFR ≥30 mL/min/1.73m2 (MDRD)
• 1° outcome = ‘3-point MACE’ (CV death, non-fatal MI, non-fatal stroke)
Zinman B et al. N Engl J Med 2015

Cumulative incidence function. HR, hazard ratio
EMPA-REG OUTCOME Cardiovascular death
Zinman B et al. N Engl J Med 2015
HR 0.62 (95% CI 0.49, 0.77)
p=0.0001
N=7020
38%

Kaplan-Meier estimate. HR, hazard ratio
EMPA-REG OUTCOME All-Cause Mortality
32% HR 0.68
(95% CI 0.57, 0.82) p<0.0001
Zinman B et al. N Engl J Med 2015

Cumulative incidence function. HR, hazard ratio
N=7020
EMPA-REG OUTCOME Hospitalization for heart failure
HR 0.65 (95% CI 0.50, 0.85)
p=0.0017
35%
Zinman B et al. N Engl J Med 2015

Clinical Therapeutics DOI: (10.1016/j.clinthera.2016.04.037)
EMPA-REG OUTCOME

Clinical Therapeutics DOI: (10.1016/j.clinthera.2016.04.037)
EMPA-REG OUTCOME
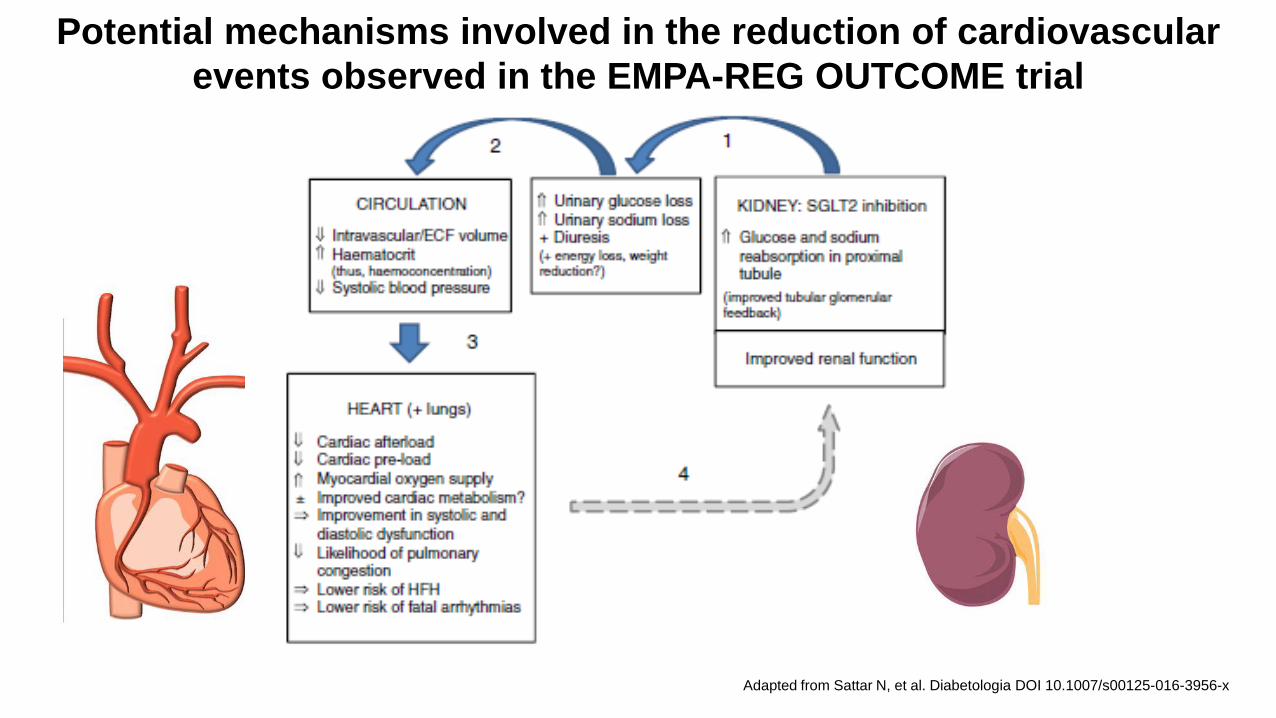
Potential mechanisms involved in the reduction of cardiovascular events observed in the EMPA-REG OUTCOME trial
Adapted from Sattar N, et al. Diabetologia DOI 10.1007/s00125-016-3956-x
Summary • SGLT-2 inhibitors are relatively new drugs for the management of hyperglycemia in
diabetes. They are highly effective at improving glycemia, and also have beneficial effects on weight and blood pressure. In general, they are well tolerated, and the risk benefit ratio seems to be reasonable.
• In the Empa-Reg Outcome trial patients with type 2 diabetes and high CV risk treated with empagliflozin had significantly reduced risk of heart failure hospitalization, and death (CV and All Cause). Also, in those with GFR <60 ml/min, empagliflozin lead to a significant reduction in the composite renal end-point of creatinine doubling, ESRD or renal death.
• Is the EMPA-REG Outcome Trial a game changing study? • YES, but needs to be independently confirmed. In the meantime, a SGLT2
inhibitor with demonstrated cardiovascular outcome benefit should be added to the anti-hyperglycemic therapy to reduce the risk of cardiovascular and all-cause mortality in patients with diabetes and clinical evidence of cardiovascular disease

Thank you

Extra Slides

Hattersley AT, Thorens B. N Engl J Med 2015;373:974-976.
Renal Absorption of Glucose and Glucagon Secretion According to the Presence or Absence of a Sodium-Coupled Glucose Transporter Type 2 (SGLT2) Inhibitor.

The role of the kidney in glucose reabsorption
Glucose reabsorption from the glomerular filtrate through a proximal tubular epithelial cell into the blood. GLUT, glucose
transporter; SGLT, sodium–glucose co-transporter.
Hasan F, Alsahli M, Gerich JE. Diabetes Research & Clinical Practice. 104 (2009) 297-322

Proposed mechanisms whereby SGTL2 inhibitors exert adverse effects on bone
Taylor SI,et al. www.thelancet.com/diabetes-endocrinology Vol 3 January 2015 http://dx.doi.org/10.1016/S2213-8587(14)70227-X

FDA warning – May 2016 • In the ongoing Canagliflozin Cardiovascular Assessment Study (CANVAS) clinical trial, the trial’s independent
data monitoring committee (IDMC) identified an increased risk of leg and foot amputations. The amputations occurred about twice as often in patients treated with canagliflozin compared to patients treated with placebo, which is an inactive treatment. An interim analysis showed that over a year’s time, the risks of amputation for patients in the trial were equivalent to:
• 7 out of every 1,000 patients treated with 100 mg daily of canagliflozin • 5 out of every 1,000 patients treated with 300 mg daily of canagliflozin • 3 out of every 1,000 patients treated with placebo
• Patients in the CANVAS trial have been followed for an average of 4.5 years to date. The IDMC has recommended, based on an overall assessment, that the CANVAS trial continue.
• The IDMC has also reported that a second, similar trial evaluating canagliflozin, the CANVAS-R trial, has not shown the same risks of increased leg and foot amputations to date. Patients in the CANVAS-R trial have been followed for an average of 9 months.
http://www.fda.gov/Drugs/DrugSafety/ucm500965.htm

Antihypertensive drug therapy and the risk of lower extremity amputations in pharmacologically treated type 2 diabetes patients
Abstract • Purpose • The objective of this study was to determine the association between different antihypertensive drug therapies and lower extremity
amputations (LEAs) in type 2 diabetes patients. • Methods • Data were obtained from the PHARMO Record Linkage System comprising pharmacy records and data on hospitalizations for all 450 000
residents of eight Dutch cities. In a nested case-control study among 12 140 type 2 diabetes patients who used antihypertensive drugs, 26 cases with a first LEA and 94 controls without a LEA matched on age, sex and calendar time were identified. Logistic regression was used to estimate the relative risk of LEA and to adjust for potential confounding factors.
• Results • Among type 2 diabetes patients who used antihypertensive drugs, subjects who used thiazide diuretics, alone or in combination, had a
higher risk of LEA compared to subjects who used Angiotensin Converting Enzyme (ACE) inhibitor monotherapy (crude odds ratio (OR): 6.11 [95% confidence interval (CI): 1.32–28.27]). The use of thiazide diuretics was also associated with an increased risk of LEA when compared to the use of any non-thiazide antihypertensive drug (adjusted OR: 7.04 [1.10–45.30]). The increased risk of LEA associated with the use of thiazides compared to the use of non-thiazides depended on the duration of use (adjusted OR≤365 days, 4.82 [0.61–38.34] and adjusted OR>365 days, 26.16 [1.02–674.02], p-trend = 0.01).
• Conclusions • Treatment with thiazide diuretics compared to treatment with other antihypertensive drugs was associated with excess amputations in
type 2 diabetes patients. Due to several limitations of this study, our findings do not preclude the use of thiazides in type 2 diabetes mellitus patients as yet.
Erkens, J. A., et al. (2004). Pharmacoepidem. Drug Safe., 13: 139–146










![Sodium-glucose cotransporter-2 inhibitors (SGLT-2i) in the ...group of SGLT-2i users vs 0.06% in the other glucose-lowering groups (odds ratio [OR], 1.71; 95% confidence interval](https://static.fdocuments.net/doc/165x107/5f288f8337f0e842db70dd8a/sodium-glucose-cotransporter-2-inhibitors-sglt-2i-in-the-group-of-sglt-2i.jpg)







