
Starting and Helping People with Type 2 - Johnson & … and Helping People with Type 2 Diabetes on...
46
Transcript of Starting and Helping People with Type 2 - Johnson & … and Helping People with Type 2 Diabetes on...


Starting and Helping People with Type 2 Diabetes on Insulin
Elaine Cooke, BSc(Pharm), RPh, CDE
Pharmacist and Certified Diabetes Educator
Maple Ridge, BC

After attending this session, participants will be able to:
Objectives
• Understand the unique needs and challenges to consider when
initiating insulin therapy in people with type 2 diabetes
• Recognize hypoglycemia, its causes and the physical and
psychological impact it has on people with diabetes
• Explain how self-monitoring of blood glucose (SMBG) can assist
people using insulin to recognize issues, problem solve and adjust
their insulin when blood glucose (BG) is not at target
• Recognize SMBG “best practices” and counsel people with type 2
diabetes on insulin therapy accordingly
3

4
Diabetes Progression

•50% of ß-cell function is already lost at diagnosis
•ß-cell function will continue to decline despite treatment
Impaired
glucose
tolerance
100
75
50
25
Years from Diagnosis
Bet
a C
ell
Fu
nct
ion
(%
)
-12 -10 -6 -2 0 2 6 10 14
Postprandial
hyperglycemia
Type 2
diabetes
phase I Type 2
diabetes
phase II
Type 2 diabetes
phase III
Lebovitz HE Diabetes Rev 1999:7 139-53.
Stages of Type 2 Diabetes in
Relationship to ß-cell Function
Type 2 Diabetes is a Progressive Disease

6
Issues, Barriers and Patient Needs

Clinician barriers to insulin therapy may be due to:
Barriers to Starting Insulin Therapy
• Perceived complexity of the therapeutic regimen
• Belief that it is not effective in type 2 diabetes
• Fear of hypoglycemic episodes, weight gain and associated
cardiovascular risks
• Fear that insulin therapy will require careful monitoring, more
physician time, and other practice resources
7
Davis SN, Renda SM. Diabetes Educator 2006; 32(4):146S-52S.

Barriers to Starting Insulin Therapy
Insulin therapy may have negative
connotations for some patients:
• Sense of loss of control over
one’s life
• Reduced quality of life
• Sense of personal failure to control
the disease
• Side effects such as weight gain
and hypoglycemia
• Daily, possibly painful, injections
Establish a sense of patient control
by informing patients that:
• Their symptoms will improve with
insulin therapy
• They will be taking a more active
role in managing their diabetes
• Basal insulin regimens are easy to
administer and can be administered
at bedtime
• There are strategies to prevent
hypoglycemia
8
Davis SN, Renda SM. Diabetes Educator 2006; 32(4):146S-52S.

9
Initiating Insulin in Type 2 Diabetes

10
Insulin can be used:
• At diagnosis
• During illness, surgery or
pregnancy
• At any time glycemic targets are
not being met
- Glycemic targets must be individualized.
Target for most individuals with diabetes
is a glycated hemoglobin (A1C) ≤ 7.0%
Insulin in Type 2 Diabetes
CDA Clinical Practice Guidelines. Can J Diabetes 2013;37(Suppl 1):S1-S212;
Harper W, et al. Can J Diabetes 2013;37(Suppl 1):S61-S68, Chapter 13.

Polling Question:
Which of the following is not a barrier to starting insulin? A. Clinician fear it will require more time and practice resources B. Sense of personal failure to control diabetes C. Concerns over cost of therapy D. Concerns that injections will be painful

12
Tailor treatment to the individual. There are many options:
• Start with a basal insulin in addition to oral antihyperglycemic agents
• Start with a premixed insulin in addition to oral antihyperglycemic agents
• Start with intensive insulin therapy (less common and not generally
recommended)
Insulin in Type 2 Diabetes
CDA Clinical Practice Guidelines. Can J Diabetes 2013;37(Suppl 1):S1-S212, Appendix 3.
Resource Slide

Basal Insulin added to Oral Antihyperglycemic
Insulin
• Neutral protamine hagedorn (NPH), glargine U-100, detemir, glargine U-300, degludec
(U-100 and U-200)
Dosing
• Starting dose is generally 10 units daily at bedtime. Can be administered at other times
of day.
Titration
• Several titration regimens are acceptable
• For glargine U-100 or detemir, one regimen is to increase dose by 1 unit every night
until fasting BG has reached their individual target (e.g., 4.0-7.0 mmol/L [ADA 90-130
mg/dL])
• Stop titrating if 2 episodes of hypoglycemia occur in a week or any nocturnal
hypoglycemia
• Insulin glargine U-300 and insulin degludec should not be up-titrated more often than
every 3-4 days due to their longer duration of activity
13
CDA Clinical Practice Guidelines. Can J Diabetes 2013;37(Suppl 1):S1-S212, Appendix 3; CDA Insulin Prescription Tool for Healthcare Providers
[http://guidelines.diabetes.ca/bloodglucoselowering/insulinprescriptiontool]; Toujeo Package Insert; Tresiba Package Insert
Standards of Medical Care in Diabetes—2016 January 2016 Volume 39, Supplement 1-American Diabetes Association Garber, AJ, et al.Endocrine Practice,
2013;19(Suppl 2):1-38.

14
What to discuss with the Patient
Type and starting dose of insulin
• Explain onset, peak, duration, preparation
and storage
Titration schedule
• When to check and what BG targets are being
used for titration
How to use injection device
Injection site and rotation of injections
Hypoglycemia: symptoms, treatment, prevention
• Sick day guidelines
• Driving guidelines
Follow-up date to discuss concerns
Insulin Pen Start Checklist Help Sheet [http://www.diabetes.ca/CDA/media/documents/clinical-practice-
and-education/professional-resources/insulin-pen-checklist-help.pdf]
Resource Slide

Getting Started with Insulin:
Patient Handout
15
Resource Slide

Provide Patient
Insulin Type, Dose and Action
• Type and starting dose of insulin
• Onset, peak, duration and storage
16
Insulin Type Onset Peak Duration
Basal Insulins
Intermediate-acting insulin (cloudy):
• Insulin NPH 1 - 3 h 5 - 8 h Up to 18 h
Long-acting basal insulin analogues (clear)
• Insulin detemir • Insulin glargine U-100 • Insulin glargine U-300 • Insulin degludec
90 min 90 min
Up to 6 h1 60 min
Not applicable
Up to 24 h (detemir 16-24 h)
Up to 24 h (glargine 24 h)
Up to 30 h
Up to 42 h
Harper W, et al. Can J Diabetes 2013;37(Suppl 1):S61-S68, Chapter 13; Toujeo Package Insert; Tresiba Package Insert 1Per Package Insert, onset of action
develops over 6 hours after administration.
Resource Slide

17
• Consult directions with each pen
• New pen needle for each injection
• Re-suspend cloudy insulin (NPH),
tap to send any air bubbles to end
of needle
• Prime with a 2 unit shot each time;
a drop of insulin should appear.
Repeat until a drop appears
Insulin Pens
• Dial dose and perform injection
90⁰ • Count to at least 10, then
remove needle and discard in
sharps container
• Use pen needle length of 4 to 6 mm
Insulin Pen Start Checklist Help Sheet
[http://www.diabetes.ca/CDA/media/documents/clinical-practice-and-
education/professional-resources/insulin-pen-checklist-help.pdf]; Gibney MA, et
al. Curr Med Res Opin 2010;26(6):1519-30.
Resource Slide

Injection Site Rotation
Injection Site
• Abdomen fastest, most consistent absorption, followed by the outer arm, thigh
and buttock
Site Rotation
• Divide injection site into quadrants, use one quadrant weekly separating all
injections by a finger width
Site Preparation • Clean with soap and water
• Alcohol is not required; if used let dry completely
• With 4-6 mm pen needles a skin lift is usually not required unless very lean;
hold skin and lift until injection complete
18
FIT Forum for Injection Technique Canada [https://www.bd.com/resource.aspx?IDX=25063]; FIT Technique Plus Technique for All
[http://www.fit4diabetes.com/files/8713/6544/1790/FIT_Technique_Plus_-_Technique_for_All.pdf]
Resource Slide

19
Hypoglycemia
Lower rates of hypoglycemia have been
observed with rapid acting analogues
than regular insulin
Use of long-acting basal insulin
analogues reduces the risk of nocturnal
hypoglycemia compared to NPH
Causes of hypoglycemia: • Missed meals, smaller or delayed meals
• Too much medication
• Unplanned or extra activity
• Consuming alcohol
CDA Clinical Practice Guidelines. Can J Diabetes 2013;37(Suppl 1):S1-S212; Meece J. Diabetes
Educ 2006;32;9S-18S.

20
Symptoms of Hypoglycemia Symptoms vary from person to person
Early Signs • Trembling, shaking
• Dizzy, light headed
• Palpitations
• Sweating
• Anxiety
• Hunger
• Nausea
• Tingling
• Headache
• Blurred vision
Late Signs • Difficulty concentrating
• Confusion
• Changed behaviour
• Drunk-like behaviour
• Trouble speaking
• Loss of consciousness
Clayton D, et al. Can J Diabetes 2013;37(Suppl 1): Chapter 14.

Hypoglycemia Treatment
Check BG and treat if below 4.0 mmol/L (ADA 70 mg/dL)
Give 15 g fast acting carbohydrate preferably as 3 to 4 dextrose
tablets or: • 15 mL (3 teaspoons) or 3 packets of table sugar
• 175 mL (3/4 cup) juice or regular soft drink
• 6 lifesavers (1=2.5 g of carbohydrate)
• 15 mL (1 tablespoonful) of honey
• 4 x dextrose 4 g tablets
Wait 15 minutes, retest BG and retreat with another 15 g
carbohydrate if BG < 4.0 mmol/L (ADA 70 mg/dL)
If next meal is more than 1 hour away once hypoglycemia has been
reversed, have a snack with 15 g carbohydrate and a protein source
21
Briscoe V, et al. Clinical Diabetes 2006;24;115-21; CDA Clinical Practice Guidelines. Can J Diabetes 2013;37 (Suppl 1):S1-S212
Standards of Medical Care in Diabetes—2016 January 2016 Volume 39, Supplement 1-American Diabetes Association Garber, AJ, et al.Endocrine Practice,
2013;19(Suppl 2):1-38.
.

Prevention of Hypoglycemia for all Insulin-Treated Drivers
22
Measure BG level immediately before and at least every 4 hours
during long drives
Do not drive when BG level is < 4.0 mmol/L (ADA 70 mg/dL) • Do not begin to drive without having some carbohydrate-containing food when
your BG level is 4.0 to 5.0 mmol/L (ADA 70 to 90 mg/dL)
Stop and treat yourself as soon as hypoglycemia and/or impaired
driving is suspected • You should not drive for at least 45 to 60 minutes after effective treatment of
mild to moderate hypoglycemia
Insulin Pen Start Checklist Help Sheet; CDA Getting Started with Insulin 2013
Standards of Medical Care in Diabetes—2016 January 2016 Volume 39, Supplement 1-American Diabetes Association Garber, AJ, et al.Endocrine Practice,
2013;19(Suppl 2):1-38.
.

Polling Question:
Which of the following should be discussed with patients starting insulin? A. Onset, peak, duration, preparation and storage of insulin B. Injection site selection and rotation C. Hypoglycemia recognition, treatment and prevention D. All of the above

24
Patient Education and Tools
Patient should leave from insulin start
session with:
• Insulin, pen or syringes and sharps container
• Dose of insulin, when to inject and titration
protocol
• Knowing injection technique: how, where, site
rotation
• Hypoglycemia sheet for signs, symptoms and
treatment
• Log book, test times and BG targets
• Appointment for follow-up call

25
Intensifying Insulin Therapy

Adding Bolus Insulin
Basal Plus Strategy:
26
Dosing • Starting dose: 2 to 4 units
• Patient can be taught self titration, or dose increase can be done by the health
care practitioner
• The mealtime (bolus) insulin dose may be initiated at one meal daily (generally
the largest meal of the day)
Titration • To safely increase dose, glucose levels should be measured at least prior to
insulin dose, then titrated by 1 unit daily to either of the following targets:
• 2 hour post-meal glucose of ≤ 10.0 mmol/L (ADA 180 md/dL)
(or ≤ 8.0 mmol/L [144 mg/dL] in certain cases)
• Pre-next meal glucose of 4.0 to 7.0 mmol/L (ADA 90 to 130 mg/dL)
CDA Clinical Practice Guidelines. Can J Diabetes 2013;37(Suppl 1):S1-S212, Appendix 3; CDA Insulin Prescription Tool for Healthcare Providers
[http://guidelines.diabetes.ca/bloodglucoselowering/insulinprescriptiontool]; Harper W, et al. Can J Diabetes 2013;37(Suppl 1):S61-S68, Chapter 13
Standards of Medical Care in Diabetes—2016 January 2016 Volume 39, Supplement 1-American Diabetes Association Garber, AJ, et al.Endocrine Practice,
2013;19(Suppl 2):1-38.
.

27
Using SMBG

28
Benefits of SMBG
SMBG identifies glycemic excursions to
allow for day-to-day adjustments of
activity, diet and medication. It can:
• Determine preprandial and postprandial
hyperglycemia
• Confirm hypoglycemia, allowing for appropriate
treatment
• Detect glycemic excursions, providing
immediate feedback to patients about the effect
of food choices, activity and medication on
glycemic control
Awareness of SMBG and A1C provide the best
information to assess glycemic control and help
patients on insulin make changes and regain control CDA Clinical Practice Guidelines. Can J Diabetes
2013;37(Suppl 1):S1-S212; Parkin CG, et al. J Diabetes
Sci Technol. 2009;3:500-8. .

Regular SMBG Frequency
29
Situation SMBG Recommendation
Using multiple daily injections of insulin
(≥ 4 times per day)
Using an insulin pump
SMBG ≥ 4 times per day
Using insulin < 4 times per day SMBG at least as often as insulin is being given
Pregnant (or planning a pregnancy),
whether using insulin or not
Hospitalized or acutely ill
SMBG individualized and may involve
SMBG ≥ 4 times per day
Starting a new medication known to
cause hyperglycemia (e.g. steroids)
Experiencing an illness known to
cause hyperglycemia (e.g. infection)
SMBG individualized and may involve
SMBG ≥ 2 times per day
CDA Clinical Practice Guidelines Expert Committee. Appendix 4. Can J Diabetes 2013;37(Suppl 1):S197-S212.
http://guidelines.diabetes.ca/BloodGlucoseLowering/SMBGRecommendationSheet

Increased SMBG Frequency
30
Situation SMBG Recommendation
Using drugs known to cause hypoglycemia
(e.g. sulfonylureas, meglitinides)
SMBG at times when symptoms of
hypoglycemia occur or at times when
hypoglycemia has previously occurred
Has an occupation that requires strict
avoidance of hypoglycemia
SMBG as often as required by employer
Not meeting glycemic targets SMBG ≥ 2 times per day, to assist in lifestyle
and/or medication changes until such time as
glycemic targets are met
Newly diagnosed with diabetes
(< 6 months)
SMBG ≥ 1 time per day (at different times of
day) to learn the effects of various meals,
exercise and/or medications on BG
Treated with lifestyle and oral agents and
is meeting glycemic targets
Some people with diabetes might benefit from
very infrequent checking (SMBG once or twice
per week) to ensure that glycemic targets are
being met between A1C tests
CDA Clinical Practice Guidelines Expert Committee. Appendix 4. Can J Diabetes 2013;37(Suppl 1):S197-S212.
http://guidelines.diabetes.ca/BloodGlucoseLowering/SMBGRecommendationSheet

31
• Requires a review of all parameters that affect BG
• Involves reviewing a record of glucose values, food, physical activity,
medication administration and other factors that may affect blood sugar
Do not react to one BG value. 3 to 4 days of information are required to determine
a pattern
Organize results so that all BG values occurring at the same time of day can be
seen and reviewed together
Pattern Management
Mensing C, Ed. The Art and Science of Diabetes Self Management Education, 2006 American Association of Diabetes Educators; Chapter 16, pp 357-370.
Resource Slide

If more than one pattern appears, prioritize the work of bringing the
pattern back into target range:
Prioritizing Treatment
32
1. Always fix hypoglycemia (< 4.0 mmol/L [ADA 70 mg/dL]) first
2. Bring fasting BG into target next
3. Work on hyperglycemia patterns, usually looking at pre-meal values followed
by post-meal values
Remember to:
• Adjust only one insulin at a time
• Adjust the insulin dose by no more than 10% at a time
• Reassess BG values after several days before making further changes
Rodbard D. J Diabetes Sci Technol 2007;1:62–71
Standards of Medical Care in Diabetes—2016 January 2016 Volume 39, Supplement 1-American Diabetes Association Garber, AJ, et al.Endocrine Practice,
2013;19(Suppl 2):1-38.

33
Adjusting Insulin When adjusting insulin you need to adjust
the insulin that affects the BG value you are
concerned with
Blood glucose value at: Adjust:
Fasting/pre-breakfast Bedtime basal
Pre-lunch Breakfast bolus
Pre-supper Lunch bolus
Bedtime Supper bolus
CDA Clinical Practice Guidelines Expert Committee. Appendix 4. Can J Diabetes 2013;37
(Suppl 1):S197-S212.

34
Adjusting Insulin If on BID combinations of premixed insulin,
typically pre-breakfast and pre-supper, you
need to be aware of what insulin affects the
BG value
Blood glucose value at: Adjust:
Fasting/pre-breakfast Pre-supper premix
Pre-lunch Pre-breakfast premix
Pre-supper Pre-breakfast premix
Bedtime Pre-supper premix
CDA Clinical Practice Guidelines Expert Committee. Appendix 4. Can J Diabetes 2013;37
(Suppl 1):S197-S212.

Polling Question:
In what order should you address recognized patterns in blood glucose records? A. Fasting blood glucose, hypoglycemia then hyperglycemia B. Hypoglycemia, hyperglycemia then fasting blood glucose C. Hypoglycemia, fasting blood glucose then hyperglycemia

Summary
Due to progressive beta cell loss, insulin will be required in the
majority of individuals with type 2 diabetes
Basal insulin at bedtime is the most common method of starting
insulin in type 2 diabetes and patients can self-titrate
Use Basal Plus strategy to intensify insulin therapy
SMBG is essential in making changes to therapy using pattern
management
It is important to educate patients on the following: • Insulin: action, dose, storage, titration, injection technique and site
• Hypoglycemia
• Driving guidelines
36


Insulin Initiation and Titration
CDA Insulin Initiation and Titration Suggestions/Prescription Form
38
Resource Slide

Getting Started with Insulin:
Patient Handout
39
Resource Slide

Sick Day Guidelines
HealthLink BC Guidelines
40
Resource Slide

Bolus Insulins
41
Insulin Type Onset Peak Duration
Bolus (prandial) Insulins
Rapid-acting insulin analogues (clear):
• Insulin aspart
• Insulin glulisine
• Insulin lispro
10 - 15 min
10 - 15 min
10 - 15 min
1 - 1.5 h
1 - 1.5 h
1 - 2 h
3 - 5 h
3 - 5 h
3.5 - 4.75 h
Short-acting insulins (clear):
• Insulin regular
30 min
2 - 3 h
6.5 h
Resource Slide
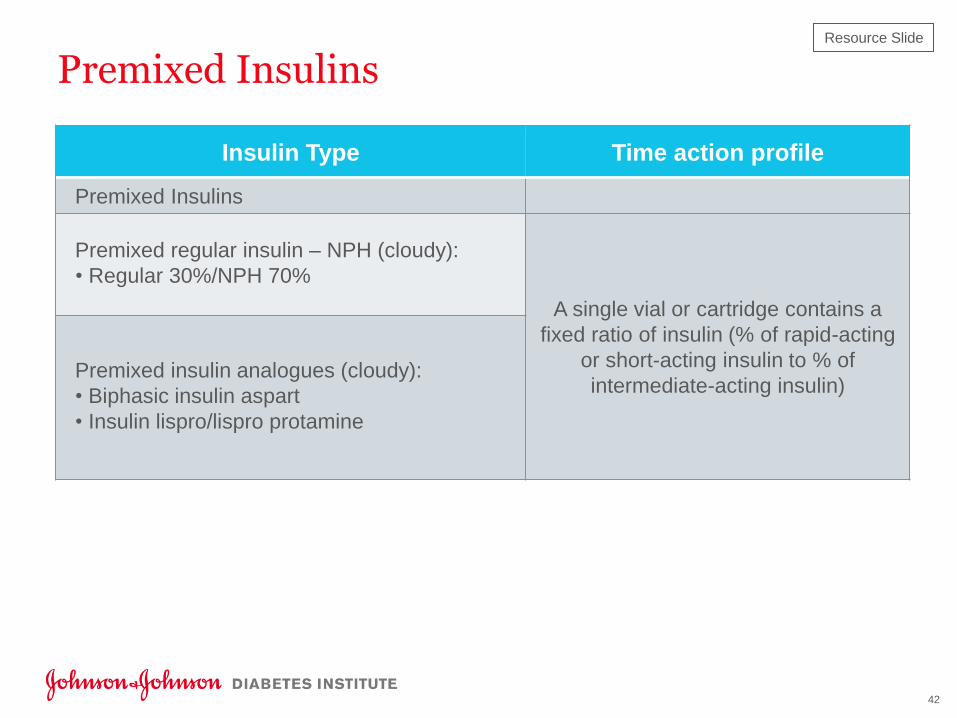
Premixed Insulins
HealthLink BC Guidelines
42
Insulin Type Time action profile
Premixed Insulins
Premixed regular insulin – NPH (cloudy):
• Regular 30%/NPH 70%
A single vial or cartridge contains a
fixed ratio of insulin (% of rapid-acting
or short-acting insulin to % of
intermediate-acting insulin) Premixed insulin analogues (cloudy):
• Biphasic insulin aspart
• Insulin lispro/lispro protamine
Resource Slide

Insulin Pen Start Checklist and Help Sheet
Checklist and Help Sheet
43
Resource Slide

Fit Canada Injection Technique
FIT Forum Best Practices FIT Technique for All
44
Resource Slide

Driving Guidelines
Getting Started with Insulin New Driving Guidelines
45
Resource Slide

CDA SMBG Tools
SMBG Recommendation Tool for Healthcare Providers Self-SMBG Frequency & Pattern Tool
46
Resource Slide


















