
Standards of Care & Documentation - LHSC
82
Standards of Care & Documentation: The A & I Flowsheet CCTC SITE SPECIFIC NURSING ORIENTATION SEPT 2019
Transcript of Standards of Care & Documentation - LHSC

Standards of Care &
Documentation:The A & I Flowsheet
C C T C S I T E S P E C I F I C
N U R S I N G O R I E N TAT I O N
S E P T 2 0 1 9

2020/02/101
GENERAL NURSING CARE
CCTC Standards
2020/02/101

2020/02/102
Critical Care Trauma Centre
Website
2020/02/102

2020/02/103
Assessment of Patient
Critically ill patients:
•Require continuous monitoring
•Are at risk for developing sudden condition
changes or complications due to invasive
monitoring devices

2020/02/104
Assessment of Patient
Two primary documentation forms:
•CCTC 12 Hour Assessment/Intervention
Flowsheet
•CCTC 24 hour Flowsheet
2020/02/104
2020/02/105
Assessment of Patient
Capture:
•Assessments & Plans
•Significant Changes
• Interventions
•Responses to Interventions
2020/02/105
2020/02/106
Maintain Patient Safety
2020/02/106
• No bay or room will be without a clinical nurse in
attendance.
Participate in Care Planning
• Participate in Rounds
• Document & communicate the plan

2020/02/107
Accountability
•Monitoring and
coordinating care for
assigned patients
•Communicating
relevant information
2020/02/107
2020/02/108
General Nursing Care Standards:
Oral Hygiene
• Mouth care every 4hr & PRN
• Teeth brushed every 12hr
• Chlorohexidine mouth rinse every 12hr for
intubated patients or those with a
tracheostomy
2020/02/108

2020/02/109
General Nursing Care Standards:
Skin Integrity and Hygiene
• Full bath early in night shift with
• Peri-care/catheter care is provided every
6-12hr and PRN
• Hair wash weekly and PRN
2020/02/109

2020/02/1010
Skin Integrity
• At start of shift:
•Thorough skin assessment
•Braden Risk Assessment Daily
• All immobile patients are repositioned and
have their skin inspected q2h- 4h and PRN
• Consider if patient is on optimal bed surface
2020/02/1010
2020/02/1011
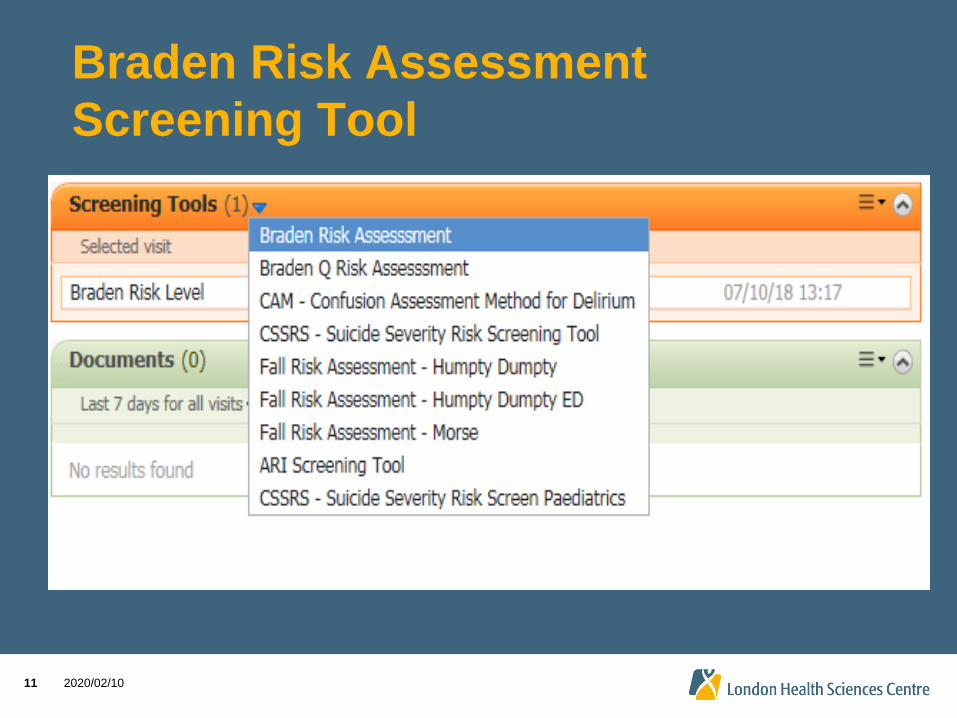
Braden Risk Assessment
Screening Tool
2020/02/1011

2020/02/1012
2020/02/1012

2020/02/1013
2020/02/1013

2020/02/1014
2020/02/1014

2020/02/1015
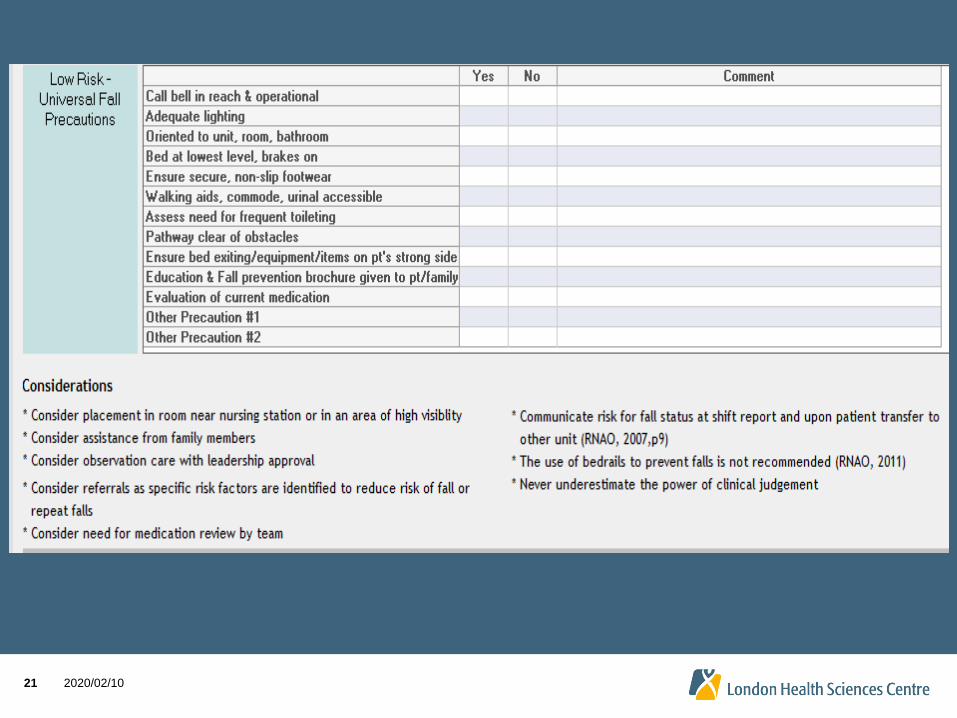
Critical Care Falls Risk & Treatment
Interference
All patients in adult critical care will
be deemed “high risk for falls and
treatment interference”, therefore,
Falls risk screening will not be
required until transfer.
2020/02/1015

2020/02/1016
Critical Care Falls Risk &
Interference Prevention
•All patients in critical care will have all of
the LHSC Standard AND Enhanced falls
risk reduction strategies implemented (as
deemed appropriate at the time), along
with the additional safety measures
that are already standards of care in
CCTC.
2020/02/1016

2020/02/1017
Falls Risk Assessment
•PRIOR TO TRANSFER, all patients in
critical care will be screened in Power
Chart with the MORSE Falls Risk
Screening Tool. A yellow arm bracelet
will be applied if indicated before
transfer.
2020/02/1017

2020/02/1018
Falls Risk Assessment (Morse)
Screening Tool
2020/02/1018

2020/02/1019
2020/02/1019

2020/02/1020
2020/02/1020
2020/02/1021
2020/02/1021

2020/02/1022
2020/02/1022

2020/02/1023
Behavioural Safety Assessment
(BSA)
• The policy has been implemented in order to
communicate risk and to ensure a safe
environment for staff, patients and everyone in the
care environment.
• Screening tool is tasked to each nurse for each
shift 0700 and 1900
2020/02/1023

2020/02/1024
2020/02/1024

2020/02/1025
BSA Scoring
• Score of 0 indicates low risk for violent behaviour
• Score of 1-3 indicates moderate risk for violent
behaviour
• Score of 4-8 indicates high risk for violent behaviour
• Score of great than 8 indicates very high risk for
violent behaviour

2020/02/1026
If a Violent Episode Occurs
• If you are unable to manage a situation without risk of harm to staff, patients, or visitors, call 55555 and initiate a Code White
• Engage Security to provide support as appropriate
• Ensure the safety of staff and other patients
• Complete a report in the AEMS system

2020/02/1027
Communication Strategies
Applying a Purple Armband Conversation
• “Your loved on has an individualized plan of
care in place to communicate the measures
we need to put in place to support them and
to make their stay pleasant. We use this
armband to tell others that care for your loved
one that there has been an individualized care
plan created.”
• “I am applying this armband to your wrist to
indicate that we have documented extra
strategies to support your care.”
2020/02/1028
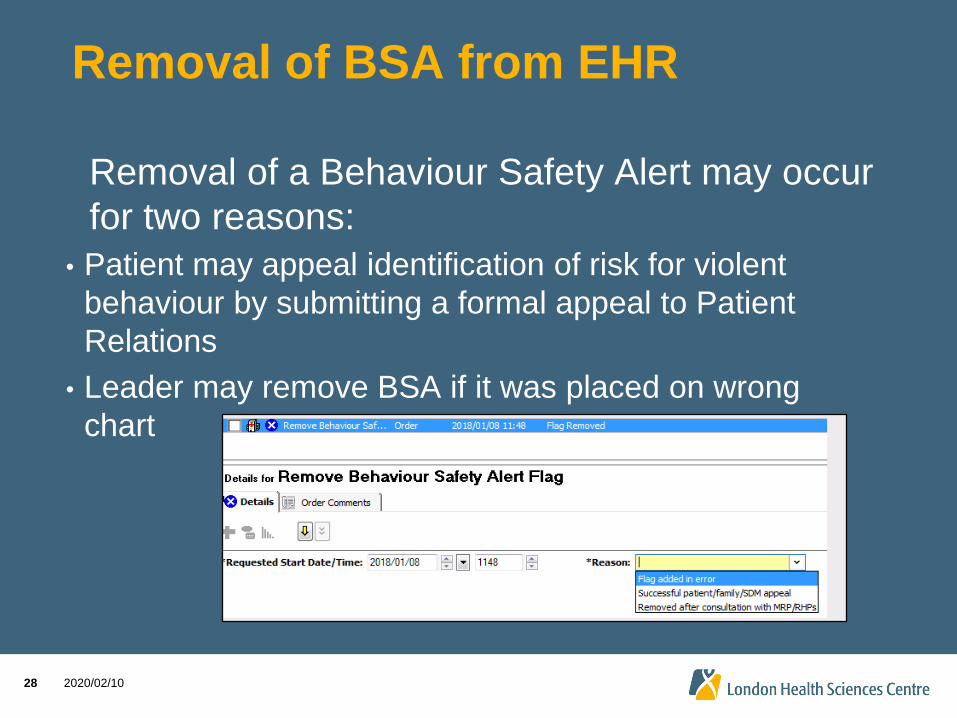
Removal of BSA from EHR
Removal of a Behaviour Safety Alert may occur
for two reasons:
• Patient may appeal identification of risk for violent
behaviour by submitting a formal appeal to Patient
Relations
• Leader may remove BSA if it was placed on wrong
chart

2020/02/1029
2020/02/1029

2020/02/1030
12 Hour Nursing
Assessment/Intervention
Flowsheet
2020/02/1030
2020/02/1031
Patient Identifier/Date
2020/02/1031
2020/02/1032
2 Patient Identifiers
1. Prior to placing the armband, the first staff
member will spell the client’s last name and state
their first name and DOB from a reliable source
document (e.g. government-issued ID or reliable
photo ID),
2. The second staff member will spell the client’s
last name and state their first name and DOB out
loud from the armband,
3. Place the armband on the client2020/02/1032

2020/02/1033
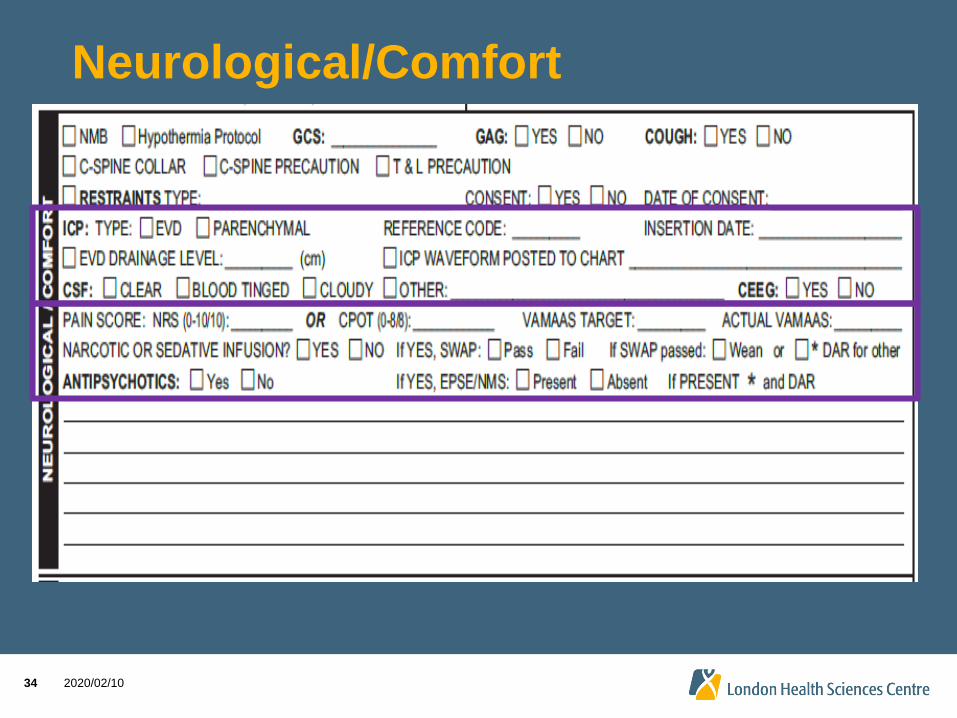
Neurological/Comfort
2020/02/1033
Gag is normal if stimulation of BOTH sides of
the oral pharynx elicits response
• Normal cough should be able to bring secretions forward
• If cough is weak, note this here on lines
2020/02/1034
Neurological/Comfort
2020/02/1034

2020/02/1035
Respiratory
2020/02/1035

2020/02/1036
Cardiovascular/Hemodynamic
2020/02/1036

2020/02/1037
When to Print an ECG Tracing
• Admission
• Every 12 hours & PRN
• After any rhythm change
• When the rhythm returns to normal
• When IV cardiac meds are being given
• Before discontinuing the cardiac monitor

2020/02/1038
Cardiovascular/Hemodynamic
2020/02/1038

2020/02/1039
Capillary Refill
2020/02/1039
• Testing Capillary Refill
1. Hold hand above the heart
2. Apply light pressure to blanch the fingernail bed
3. Release and measure the time until the
circulation returns to normal
• Normal < 2
• Sluggish > 3
• Abnormal > 5

2020/02/1040
IV Infusions
2020/02/1040
Rt IJ Introducer
Rt IJ TL : Brown
White
Blue
Lt forehand #18 PIV
Norepi and Vasopressin
CVP/RL infusion
Dilaudid and Propofol infusions
Insulin Infusion
Heparin Infusion

2020/02/1041
Sepsis Screen
2020/02/1041

2020/02/1042

2020/02/1043

2020/02/1044
2020/02/1044

2020/02/1045
2020/02/1045

2020/02/1046
Critical Care Protocol-Initial
Assessment
46
Screening: Acute Respiratory Illness/Travel
Screen
• Failed ARI, no travel- admit on Droplet + Contact
precautions
• Failed ARI with travel- admit on Droplet + Contact
precautions with Enhanced PPE
• Unable to assess- admit on Droplet + Contact
precautions with Enhanced PPE

2020/02/1047
Enhanced Precautions

2020/02/1048
Droplet + Contact with Enhanced
PPE
•Order as Droplet/Contact with Enhanced
PPE
48

2020/02/1049
Droplet + Contact Precautions
• Acute respiratory
infection
(undiagnosed)
• Pneumonia
• Influenza

2020/02/1050
Droplet + Contact Precautions
• Gloves required for all patient and environment contact
• Long sleeve gown required if skin or clothing will contact patient/patient environment

2020/02/1051
Droplet + Contact Precautions
Visitors
• Wear gloves and gown if
providing DIRECT care
• Wear procedure/surgical
mask and eye protection
within 2 metres of patient
• Visitors are to perform
hand hygiene prior to
entering and exiting the
room and removal of PPE
2020/02/1052
Droplet + Contact Precautions
Transporting
• Staff to wear gloves and
gown if assisting in the
“hands on” transfer/care
• Staff to wear fluid resistant
mask, eye protection or
face shield
• Patient to perform hand
hygiene and wear
procedural mask

2020/02/1053
Specialized Precautions

2020/02/1054
a. 2000
b. 2200
c. 2400
d. Does it really matter?
You admit a patient from the emergency department
at 2200. You identify the patient requires
droplet/contact precautions to be ordered and wear
the appropriate PPE. Later at 2400, when the dust
settles, you order the precautions in Power Chart.
What time will you enter when the precautions had
started?

2020/02/1055
Your patient has a history of MRSA and is currently
being admitted for suspected pneumonia (failed
ARI). What precaution sign(s) will you post outside
the room and enter into PowerChart?
a. Droplet/Contact
b. Enhanced Precautions
c. Contact
d. A and C

2020/02/1056
LHSC Infection Prevention &
Control

2020/02/1057
Safe Handling of Illicit Drug or
Unknown Substances

2020/02/1058
Safe Handling of Illicit Drug or
Unknown Substances
• Inadvertent skin exposure to illicit drugs like fentanyl or carfentanil are unlikely to cause toxicity however absorption can occur through mucous membranes if the drug remains on the skin and there is subsequent oral contact (e.g. hand goes in mouth).
• There is a new policy (Safe Handling of Illicit Drugs or Unknown Substances) that establishes the requirements for staff/affiliates to minimize exposure when removing illicit drugs/other substances in order to provide patient care.
2020/02/1059
What is your role if you see and
unknown substance or
something you think is an illicit
drug?

2020/02/1060
Risk Assessment

2020/02/1061

2020/02/1062

2020/02/1063
Double bag the substance using a
biohazard bag:

2020/02/1064
Doffing PPE

2020/02/1065
Call Security:

2020/02/1066
Sepsis Screen
2020/02/1066

2020/02/1067
Gentio-urinary
2020/02/1067
2020/02/1068
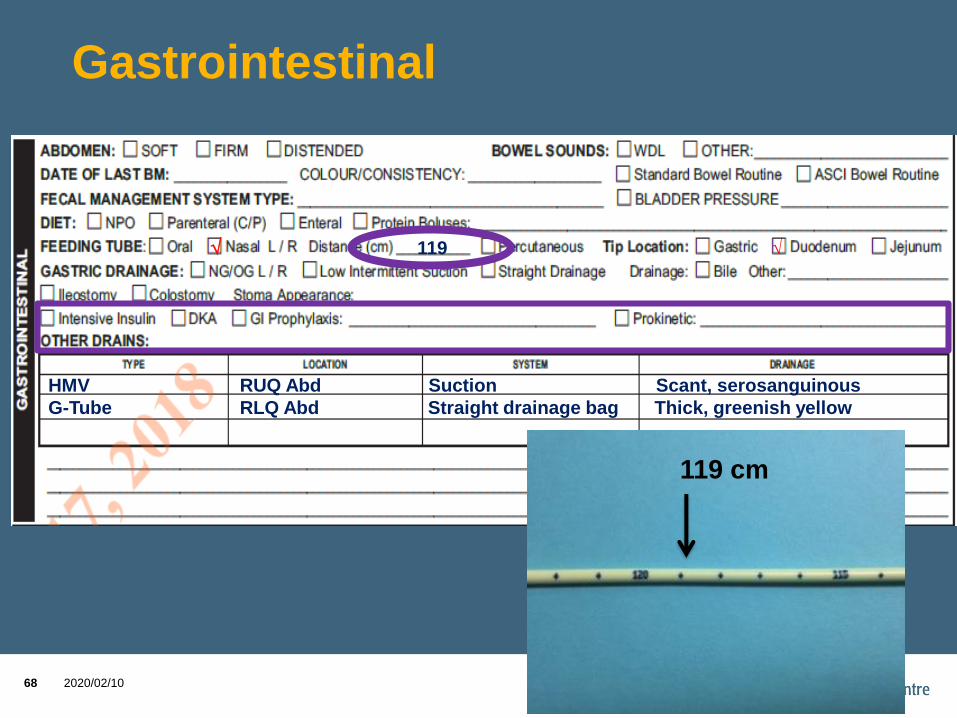
Gastrointestinal
2020/02/1068
119 cm
119 √
HMV RUQ Abd Suction Scant, serosanguinous
G-Tube RLQ Abd Straight drainage bag Thick, greenish yellow

2020/02/1069
Integumentary
2020/02/1069
Previous Stage
3 PI from
home, approx
3 x 3 in size.
Dressing intact
Midline abd
incision with
abethera in
place
Rt IJ TLC
PIV
bilateral
AC
Ex Fix in place
Hip
incision
with
staples
well
approx/
OTA

2020/02/1070
Other
2020/02/1070

2020/02/1071
Resuscitation Status
This ordered resuscitation status will be viewable in the
Summaries Viewpoint
Hover
over to
view
details

2020/02/1072
2020/02/1072

2020/02/1073
When to STAR & DAR
• STAR & DAR when:
➢ Changes from initial assessment
➢ Events happen (e.g., bedside tracheostomy, family meeting, drop in BP, etc.)
* = Significant Findings
= Findings remain unchanged
Reassess findings minimum every 4 hours
2020/02/1074
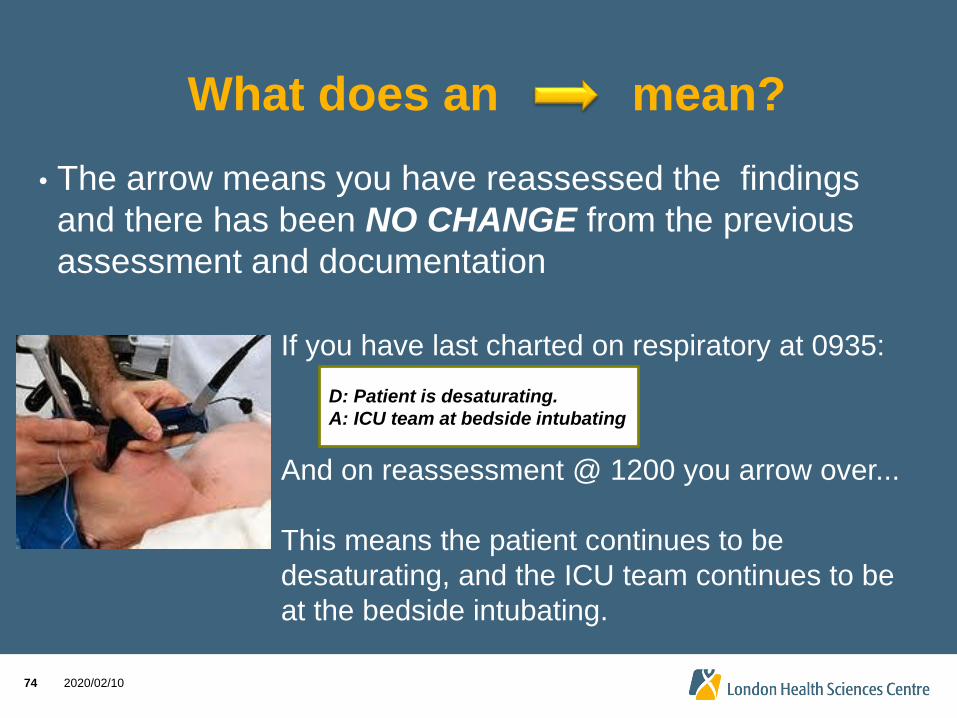
What does an mean?
• The arrow means you have reassessed the findings
and there has been NO CHANGE from the previous
assessment and documentation
If you have last charted on respiratory at 0935:
D: Patient is desaturating.
A: ICU team at bedside intubating
And on reassessment @ 1200 you arrow over...
This means the patient continues to be
desaturating, and the ICU team continues to be
at the bedside intubating.

2020/02/1075
1200 1300 1430 1600 1830
* *
*
1 1300 D – Left pupil nonreactive and larger than the right pupil. A- Notified Dr. Dre with Neurosurgery, and Dr. Imonit the CCTC resident. Will reassess hourly and report further neurological changes to teams ---------------------------------------------------CBD
14 1430 D - Family meeting, (refer to note in progress section) A – support provided to wife & children ---------------------------------------------------------------------CBD 1830 D – Both pupils now nonreactive. Patient extending without stimulation.
A - Drs Dre and Imonit notified, and are assessing patient now. ----------------CBD

2020/02/1077
Bedside Assessment Tools

2020/02/1078
2020/02/1078
2020/02/1079
Delirium assessment
• Screen in 2nd half of shift and
document time of assessment
inside the A&I sheet
• If MAAS is <2 record UTA and
document reason in DAR note
• If MAAS is >2, screen using
the ICDSC checklist
Standards

2020/02/1080
Delirium Assessment
2020/02/1080
2020/02/1081
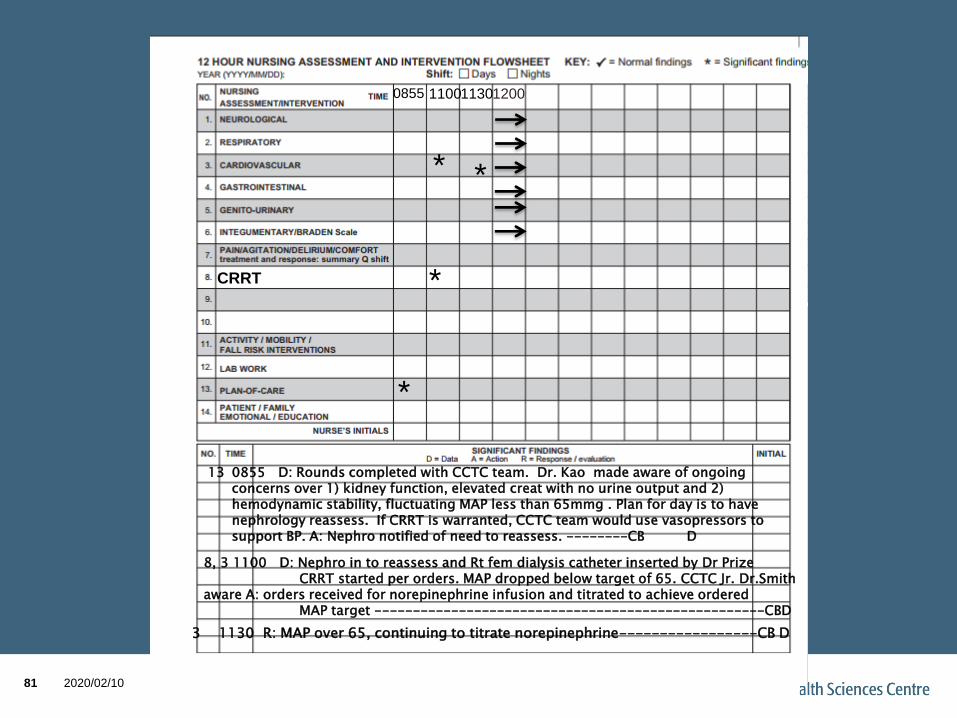
CRRT
1100
*
*
8, 3 1100 D: Nephro in to reassess and Rt fem dialysis catheter inserted by Dr Prize CRRT started per orders. MAP dropped below target of 65. CCTC Jr. Dr.Smith
aware A: orders received for norepinephrine infusion and titrated to achieve ordered MAP target ---------------------------------------------------CBD
1130
*
3 1130 R: MAP over 65, continuing to titrate norepinephrine-----------------CB D
*
0855
13 0855 D: Rounds completed with CCTC team. Dr. Kao made aware of ongoing concerns over 1) kidney function, elevated creat with no urine output and 2) hemodynamic stability, fluctuating MAP less than 65mmg . Plan for day is to have nephrology reassess. If CRRT is warranted, CCTC team would use vasopressors to support BP. A: Nephro notified of need to reassess. --------CB D
1200
2020/02/1085
References
• All Standards of Care, Protocol and Procedures
are from the Critical Care Trauma Website.
Retrieved on Jan 2 2017:
http://www.lhsc.on.ca/About_Us/CCTC/
2020/02/1085


















