
Standardizing Patient Race, Ethnicity and Language Data Collection: Overview October 1, 2010...
11
Standardizing Patient Race, Ethnicity and Language Data Collection: Overview October 1, 2010 Memphis, TN Aligning Forces for Quality National Program Office
-
Upload
barry-harrell -
Category
Documents
-
view
214 -
download
0
Transcript of Standardizing Patient Race, Ethnicity and Language Data Collection: Overview October 1, 2010...

Standardizing Patient Race, Ethnicity
and Language Data Collection:Overview
October 1, 2010Memphis, TN
Aligning Forces for Quality National Program Office
2
Why are we here?
• Understand key decision points in implementing standardized race, ethnicity and language (R/E/L) data collection within your organization
• To provide you with the knowledge and tools to train staff on the standardized collection of R/E/L data

3
What are disparities in health care quality?
• “Racial and ethnic minorities tend to receive a lower quality of healthcare than non-minorities”
• Less likely to receive:– Cancer screening– Cardiovascular therapy– Kidney dialysis– Transplants – Curative surgery for lung cancer– Hip and knee replacement – Pain medicines in the ER
4
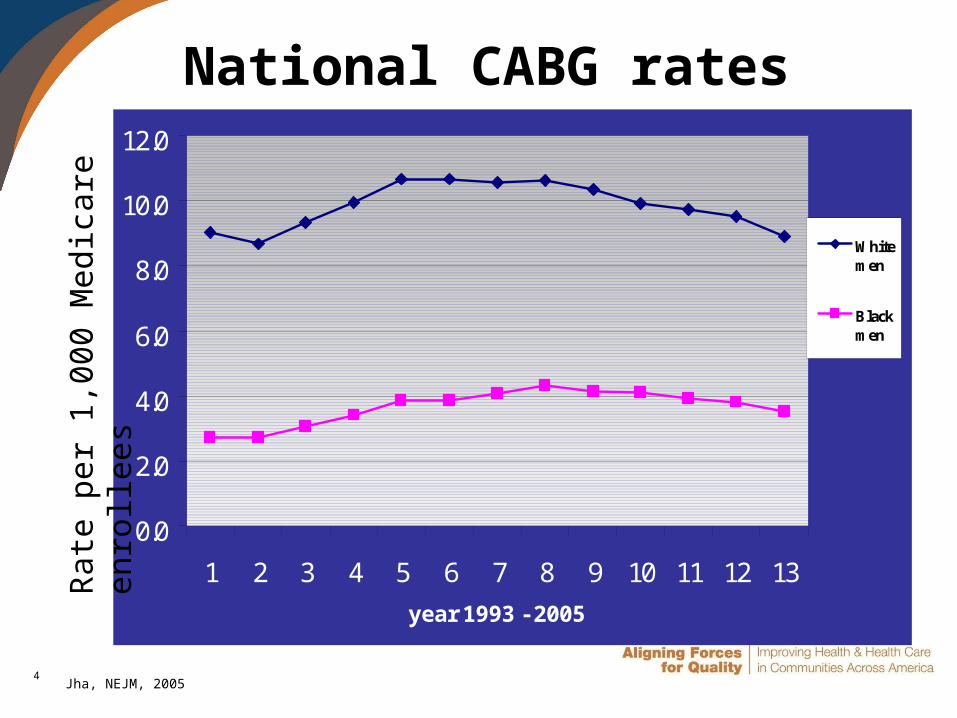
National CABG rates
0.0
2.0
4.0
6.0
8.0
10.0
12.0
1 2 3 4 5 6 7 8 9 10 11 12 13
year 1993 - 2005
Whitemen
Blackmen
Jha, NEJM, 2005
Rate
per
1,0
00
Med
icare
en
roll
ees

5
Growing U.S. minority population
0
50
100
150
200
250
300
2010 2015 2020 2025 2030 2035 2040 2045 2050
Po
pu
lati
on
in
mil
lio
ns
Non-Hispanic White
Other
Population Projections, 2010 to 2050
Source: U.S. Census Bureau, 2009 National Population Projections (Supplemental) 4. Projections of the Population by Sex, Race, and Hispanic Origin for the United States: 2010 to 2050
6
Increasing legislative and regulatory attention to R/E/L
data• American Recovery and Reinvestment Act of 2009
– Hospitals and providers will need to collect R/E/L data to be eligible for “meaningful use” incentive payments
– Race/Ethnicity categories to follow Office of Management and Budget guidelines
• Patient Protection and Affordable Care Act of 2010 – Health programs receiving federal money are required to
collect R/E/L data
• Revised Joint Commission standards– Expand requirements related to the collection of patient
language data, including preferred spoken language and written communication needs
– New requirement to collect patient-level demographic data on race and ethnicity

7
OMB guidelines: Race, ethnicity and language
categoriesRace• Black• White• Asian• American
Indian/Alaska Native
• Native Hawaiian/ Pacific Islander
• Multiracial*• Declined*• Unavailable*
Language• English• Spanish• Other• Declined • Unavailable
*This designation indicates a modification to the OMB R/E categories
Ethnicity• Hispanic• Not Hispanic• Declined*• Unavailable*
8
Three steps in addressing disparities
• Standardized collection of self-reported R/E/L data– Categories are standardized
– Patient self-reports
• Stratification and analysis of performance measures
• Use of stratified data to identify and develop quality improvement interventions targeted to specific patient populations
Disparities in care represent a failure in quality

9
What is the current status of R/E/L data collection?
• Most hospitals collect data but not in a standardized manner– Few hospitals use data collected to
drive quality improvement
• Few ambulatory providers collect or use data– More common in health centers and
integrated health systems than in smaller physician practices

10
What change needs to happen?
• Develop the capacity and infrastructure to collect standardized race, ethnicity and language information from all patients
• This will affect: – Registration system and processes– Staff training and workflow– Patient communications– How data are used to monitor quality
11
What will we cover today?
• Building blocks toward equitable care– National health care disparities – Linking R/E/L data to quality– Increasing attention R/E/L data
• Key Decision Points– Changes at the organizational level
• Nuts and Bolts– Tools to train your staff
• Available resources


















