
Stages of Anesthesia Analgesia without amnesia Stage I: Analgesia Nausea, vomiting, hyperreactivity,...
39
Stages of Anesthesia Stage I: Analgesia • Analgesia without amnesia Stage II: Excitement • Nausea, vomiting, hyperreactivity, irregular respiration Stage III: Surgical Anesthesia • Sleep, normal respiration and blood pressure Stage IV: Medullary Depression • Depression of vasomotor and respiratory centers – coma and death
-
Upload
teresa-sims -
Category
Documents
-
view
216 -
download
0
Transcript of Stages of Anesthesia Analgesia without amnesia Stage I: Analgesia Nausea, vomiting, hyperreactivity,...

Stages of AnesthesiaStage I: Analgesia
• Analgesia without amnesia
Stage II: Excitement
• Nausea, vomiting, hyperreactivity, irregular respiration
Stage III: Surgical Anesthesia
• Sleep, normal respiration and blood pressure
Stage IV: Medullary Depression
• Depression of vasomotor and respiratory centers – coma and death
WHAT ARE COMMON CAUSES OF PERIOP CARDIAC ARREST?

Anesthestic-related Cardiac Arrest and Its Mortality:A Report Covering 72,959 Anesthetics over 10 Years from a US Teaching Hospital
72,959 anesthetics over 10 year study
144 cardiac arrests (19.7 per 10,000 95% CI)
15 anesthesia attributable and contributory
129 patient disease condition or surgery
• medication-related in 40%, • complications associated
with central venous access in 20%,
• airway-related complications in 20%,
• unknown or possible vagal reaction in 13%,
• and perioperative myocardial infarction in a single case
Newland MC, Ellis SJ, Lydiatt CA, Peters KR, Tinker JH , Romberger DJ , Ullrich FA, Anderson JR (2002) Anesthesiology 97:108–15

Crisis management during anesthesia: cardiac arrest
• ECG rhythm at the time of the arrest was reported in 86 cases (67%).– sinus bradycardia (23%)– asystole (22%)– Tach/v tach/v-fib (14%); – Pulseless electrical activity (7%)
• 29 reports in which details of oxygen sat were included– 11 of the 29 were associated
with hypoxaemia and the rest were associated with other causes, mostly direct drug effects and autonomic stimulationW B Runciman, R W Morris, L M Watterson, J A Williamson and A D Paix
Qual. Saf. Health Care 2005;14;e14 doi:10.1136/qshc.2002.004473

WHAT TO DO SHOULD CARDIAC ARREST OCCUR PERIOPERATIVELY?

ClassificationArrest
V-fib
Pulseless VT
PEA
Asystole
Pre-arrest
Tachycardia
Bradycardia
Afib/Flutter


Ventricular Fibrillation / Tachycardia
• most common cause of sudden cardiac arrests– ends in death within minutes unless corrective measures
are promptly taken.
• useless quivering of heart no blood flow• Tx: only one therapy works defibrillation• Defibrillation success: chances drop every minute

Ventricular Fibrillation / Tachycardia
• Survival reduced 7-10%/min (without CPR)
• Rapid defibrillation is key
• CPR prolongs VF, slows deterioration
Minutes: collapse to 1st shock
Eisemberg JAMA 1979; 241:1905-1907
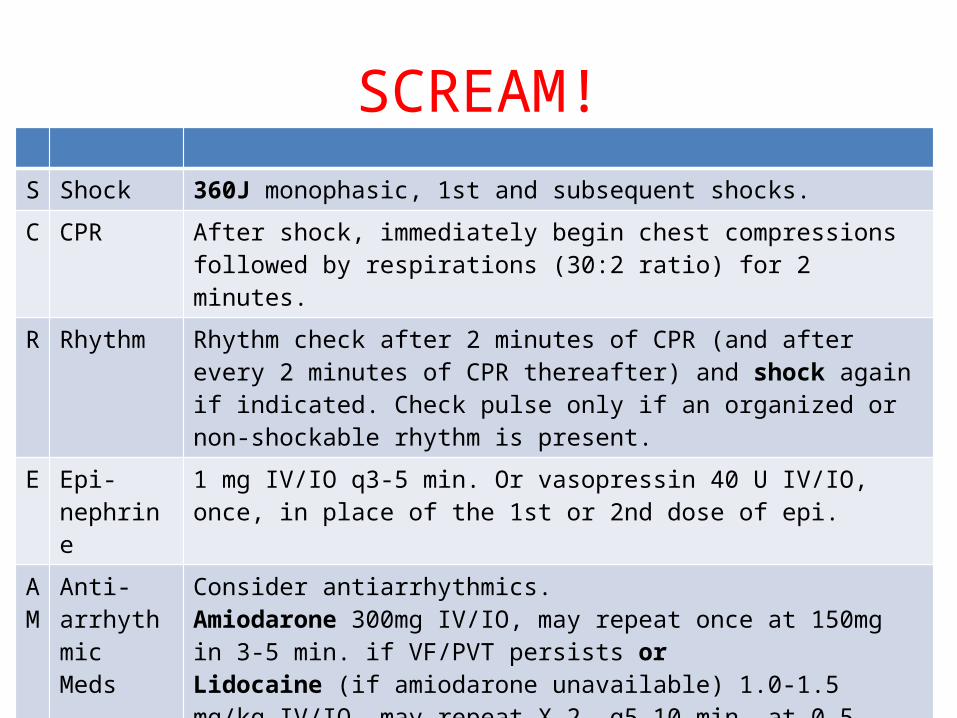
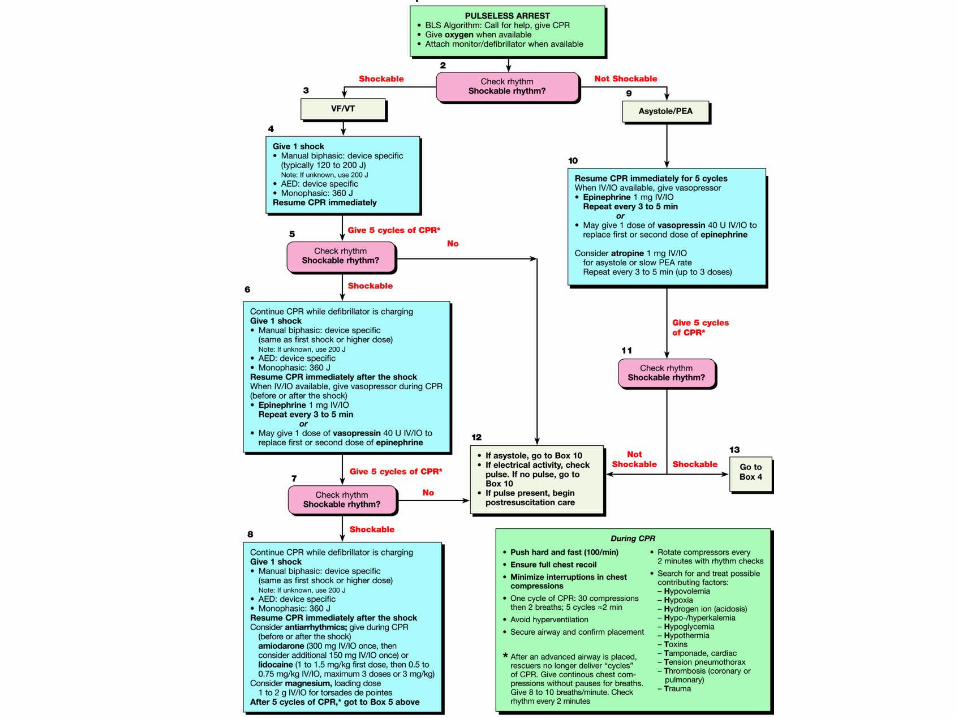
SCREAM!S Shock 360J monophasic, 1st and subsequent shocks.
C CPR After shock, immediately begin chest compressions followed by respirations (30:2 ratio) for 2 minutes.
R Rhythm Rhythm check after 2 minutes of CPR (and after every 2 minutes of CPR thereafter) and shock again if indicated. Check pulse only if an organized or non-shockable rhythm is present.
E Epi-nephrine
1 mg IV/IO q3-5 min. Or vasopressin 40 U IV/IO, once, in place of the 1st or 2nd dose of epi.
AM
Anti-arrhythmicMeds
Consider antiarrhythmics. Amiodarone 300mg IV/IO, may repeat once at 150mg in 3-5 min. if VF/PVT persists or Lidocaine (if amiodarone unavailable) 1.0-1.5 mg/kg IV/IO, may repeat X 2, q5-10 min. at 0.5-0.75 mg/kg, (3mg/kg max. loading dose) if VF/PVT persists,orMagnesium Sulfate1-2 g IV/IO diluted in 10mL D5W(5-20 min. push) for torsades de pointes or suspected/ known hypomagnesemia.

EPINEPHRINE

Alpha Adrenoreceptor Review
• a1 Receptors - Stimulation leads to Constriction of Vascular Smooth Muscle– Increases Peripheral
Vascular Resistance (PVR).
• a2 Receptors – Stimulation Inhibits NE Release

Beta Adrenoreceptor Review
• ß1 Receptors - Stimulation Results in Increased Heart Rate, Conduction Velocity and Contractility
• ß2 Receptors - Relaxation of Vascular Smooth Muscle, Skeletal Muscle and Bronchial Smooth Muscle
Epinephrine
• Stimulates a and ß Adrenergic Receptors– Low Doses - ß Effects predominate – High doses, a effects predominate.
• Increases Heart Rate, Increased Contractility.– Net Effect - Increase in Cardiac Output due to
effect of ß1 Receptor • Constricts Arterioles of Skin, Mucous
Membranes, and Viscera.– Net Effect – Increase in PVR due to effect of
a1 Receptor

Epinephrine
• Indications– Increases:• Heart rate• Force of contraction• Conduction velocity
– Peripheral vasoconstriction– Bronchial dilation

Epinephrine
• Dosing– 1 mg IV push; may repeat every 3 to 5 minutes– May use higher doses (0.2 mg/kg) if lower dose is
not effective– Endotracheal Route• 2.0 to 2.5 mg diluted in 10 mL normal saline

Epinephrine
• Precautions– Raising blood pressure and increasing heart rate
may cause myocardial ischemia, angina, and increased myocardial oxygen demand

VASOPRESSIN

Vasopressin
• In Vivo – released from posterior pituitary in response to decreased ECF volume
• Very powerful vasoconstrictor• Indications– Used to “clamp” down on vessels– No direct effects on heart

Vasopressin
• Dosing– One time dose of 40 units only– May be substituted for epinephrine– If no response in 10-20 minutes resume
epinephirne, do nor repeat doses of vasopressin• Not supported by human data
– May be given down the endotracheal tube• DO NOT double the dose• Dilute in 10 mL of NS

Vasopressin
• Precautions– May result in an initial increase in blood pressure
immediately following return of pulse– Myocardial ischemia and angina• Increased peripheral vascular resistance

ANTI-ARRYTHMICS

Antiarrhythmics
• Interact with Electrolyte Channels in Atrial Muscle and/or Ventricular Muscle and/or SA Node and/or AV Node and/or Purkinjie Fibers– Class I – Sodium Channel Blockers: Procainamide,
Lidocaine, Flecainide, Propafenone– Class II – ß Blockers– Class III – K Channel Blockers: Amiodarone,
Sotalol, Ibutilide.– Class IV – Calcium Channel Blockers: Non
Dihydropyridines.– Other – Adenosine, Digoxin, Magnesium Sulfate

Amiodarone
• MOA: – delays repolarization (prolongs refractory period)– Blocks a and b adrenergic receptors– Affects sodium, potassium and calcium channels.
• Indications– For refractory V Fib and Sustained V Tachycardia –
Antiarrhythmic of 1st Choice– Powerful antiarrhythmic with substantial toxicity,
especially in the long term

Amiodarone
• Dosing– Should be diluted in 20 to 30 mL of D5W• 300 mg bolus after first Epinephrine dose• Repeat doses at 150 mg
Amiodarone
• Precautions– May produce vasodilation & shock (hypotension,
dizziness)– May have negative inotropic effects (bradycardia
and heart block)– Terminal elimination• Half-life lasts up to 40 days
Lidocaine
• MOA: – Depresses automaticity– Depresses excitability– Raises ventricular fibrillation threshold– Decreases ventricular irritability

Lidocaine
• Dosing– Initial dose: 1.0 to 1.5 mg/kg IV• For refractory VF may repeat 1.0 to 1.5 mg/kg IV in 3 to
5 minutes; maximum total dose, 3 mg/kg• A single dose of 1.5 mg/kg IV in cardiac arrest is
acceptable• Endotracheal administration: 2 to 2.5 mg/kg diluted in
10 mL of NS
Lidocaine
• Precautions– Bradycardia, hypotension, heart block, sinus node
depression

Magnesium Sulfate
• Indications– Cardiac arrest associated with torsades de pointes
or suspected hypomagnesemic state• Dosing– 1 to 2 g diluted in 10 mL of D5W IV push
• Precautions– Occasional fall in blood pressure with rapid
administration– Use with caution if renal failure is present

Asystole / Pulseless Electrical Activity
• Asystole: lack of ventricular electrical activity & lack of ventricular mechanical activity
• PEA: presence of organized ventricular electrical activity but not accompanied by meaningful ventricular mechanical activity (sufficient to generate a palpable pulse)

PEA!
P Problem search
E Epinephrine 1 mg IV/IO q3-5 min. Or vasopressin 40 U IV/IO, once, in place of the 1st or 2nd dose of epi.
A Atropine 1 mg IV/IO q3-5 min. (3mg max.)
Hypovolemia Tablets
Hypoxia Tamponade, Cardiac
Hydrogen Ion (Acidosis) Tension Pneumothorax
Hyper-/Hypokalemia Thrombosis, coronary (ACS)
Hypothermia Thrombosis, pulmonary (embolism)
Hypoglycemia Trauma

Acetylcholine Overview and Effects
• Heart – Decrease in Heart Rate by Reducing the Firing Rate of the SA node and Increasing Conduction Time through the AV node.
• Blood Vessels – Cause Mild Dilatation of Blood Vessels

Cholinergic Antagonists - Atropine
• Atropine– Blocks Muscarinic Receptors – Post-
Ganglionic Receptors in Parasympathetic Transmission
– SA Node Effects - Increase Firing Rate– AV Node Effects – Decrease Conduction Time– Overall – Increased Heart Rate, Minimal BP
Effect
Reference: Grauer Page 78

Atropine Sulfate
• Dosing– 1 mg IV push – Repeat every 3 to 5 minutes– May give via ET tube (2 to 2.5 mg) diluted in 10
mL of NS– Maximum Dose: 0.04 mg/kg

Atropine Sulfate
• Precautions– Increases myocardial oxygen demand– May result in unwanted tachycardia or
dysrhythmia
ADDITIONAL

Tracheal administration of medications
• Doses: 2 – 3 times iv dose• Dilute in 10cc distilled H2O or NS
• N aloxone• A tropine• V asopressin• E pinephrine• L idocaine


















