Sri Lanka & MDG 4: beyond 2015
44
Sri Lanka & MDG 4: beyond 2015 SAPA meeting:Lahore,Pakistan November 2014 Prof Dulanie Gunasekera University of Sri Jaywardnepura Sri Lanka
-
Upload
dulanie -
Category
Healthcare
-
view
139 -
download
0
Transcript of Sri Lanka & MDG 4: beyond 2015
Sri Lanka & MDG 4: beyond 2015SAPA meeting:Lahore,Pakistan
November 2014Prof Dulanie Gunasekera
University of Sri JaywardnepuraSri Lanka
MDG & SL statistics
• MDG-4
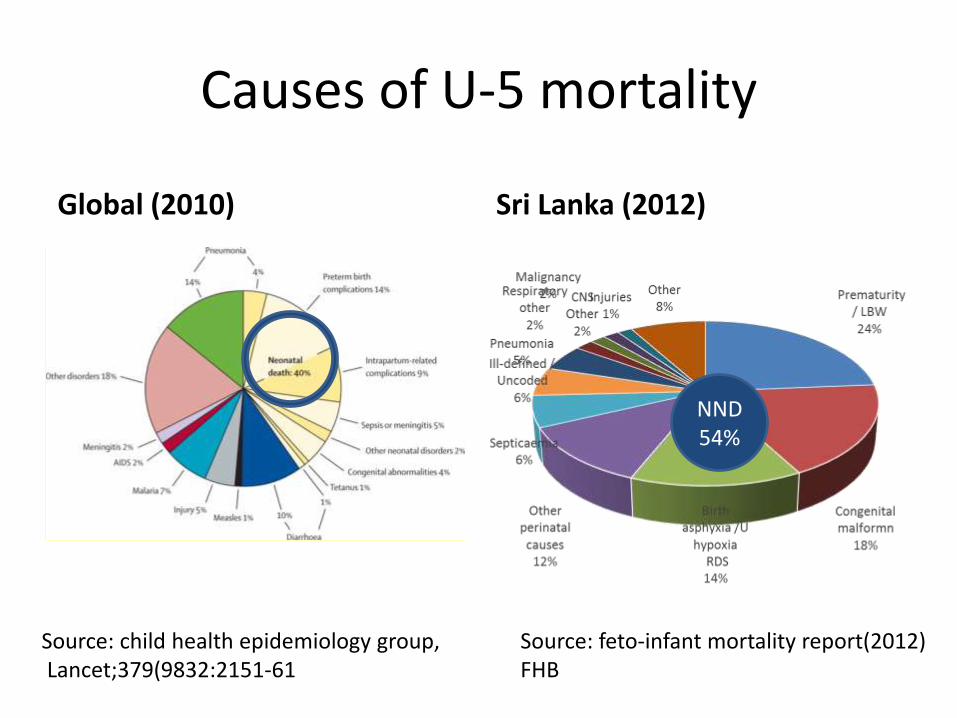
Causes of U-5 mortality
Global (2010) Sri Lanka (2012)
Source: feto-infant mortality report(2012) FHB
Source: child health epidemiology group,Lancet;379(9832:2151-61
NND54%

Causes of Infant deaths- SL (2012)
Source: FHB 2012
Asphyxia 12%
Sepsis10%
Prematurity & LWB26%
Congenital abnormalities
41%
Other11%
Asphyxia
Sepsis
Prematurity & LWB
Congenitial Abnormalities
Other

Percentage distribution of infant deaths according to age at death 2012 (FHB)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2007 2008 2009 2010 2011 2012
Early neonatal deaths
Late neonatal deaths
Post neonatal deaths
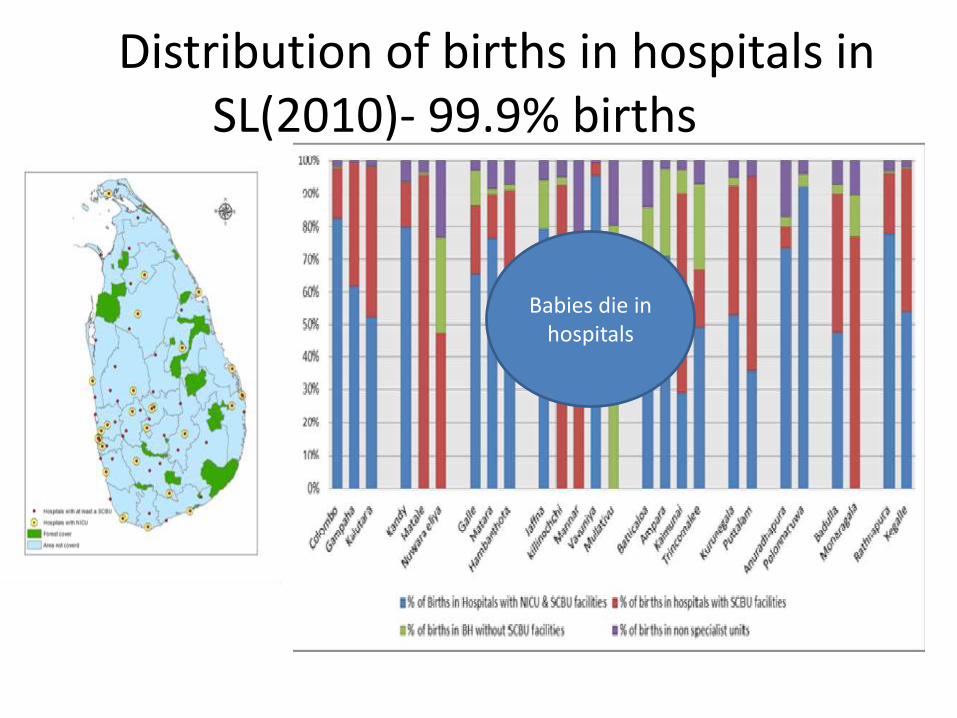
Distribution of births in hospitals in SL(2010)- 99.9% births
Babies die in hospitals
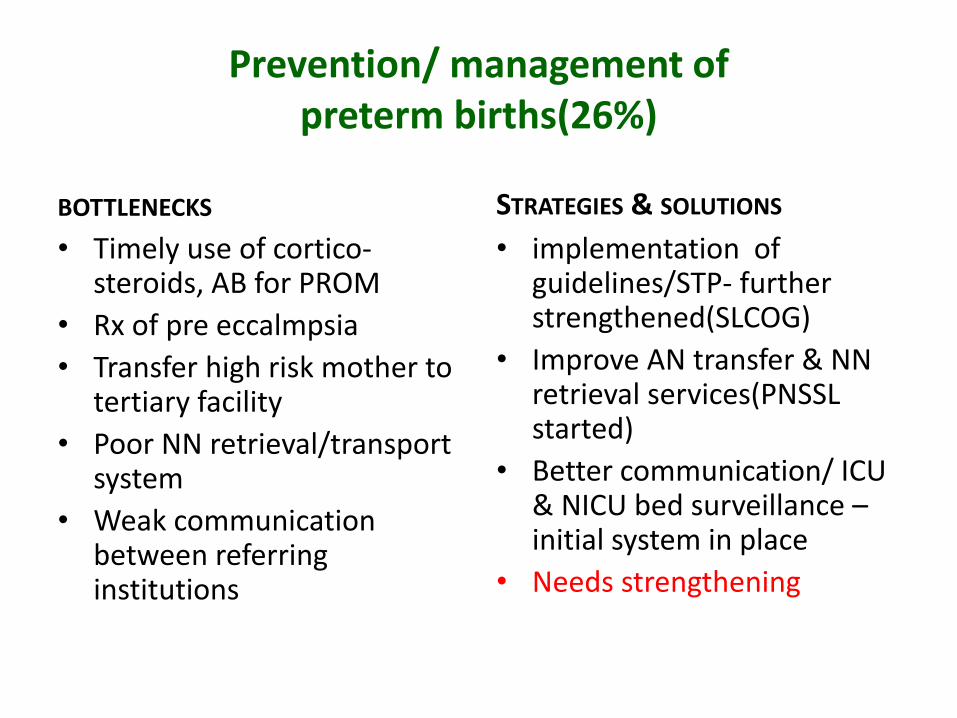
Prevention/ management of preterm births(26%)
BOTTLENECKS
• Timely use of cortico-steroids, AB for PROM
• Rx of pre eccalmpsia
• Transfer high risk mother to tertiary facility
• Poor NN retrieval/transport system
• Weak communication between referring institutions
• implementation of guidelines/STP- further strengthened(SLCOG)
• Improve AN transfer & NN retrieval services(PNSSL started)
• Better communication/ ICU & NICU bed surveillance –initial system in place
• Needs strengthening
STRATEGIES & SOLUTIONS
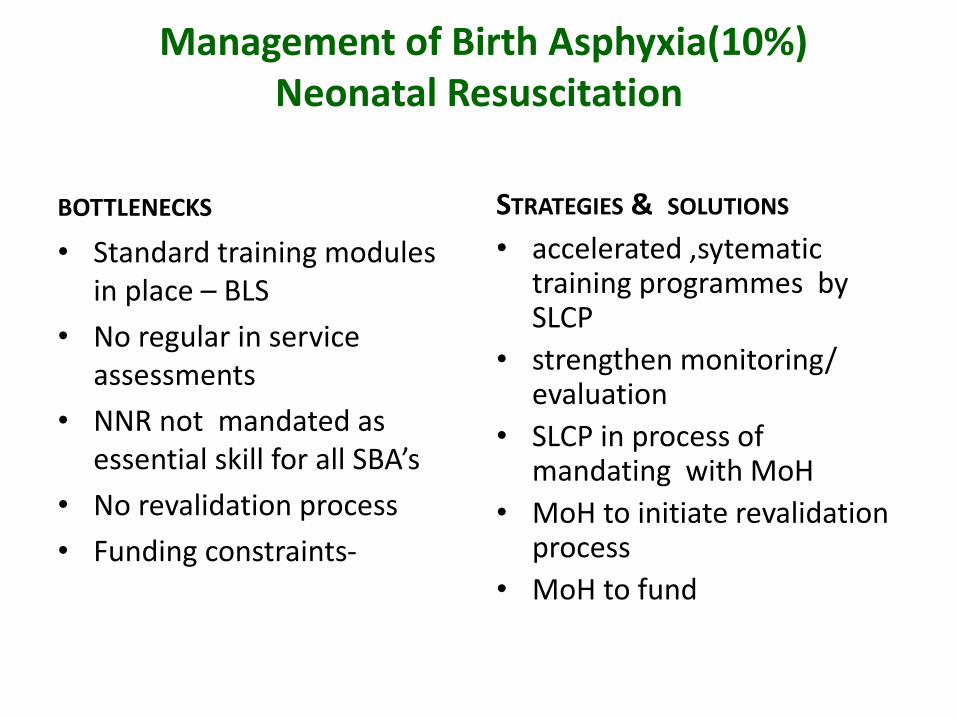
Management of Birth Asphyxia(10%)Neonatal Resuscitation
BOTTLENECKS
• Standard training modules in place – BLS
• No regular in service assessments
• NNR not mandated as essential skill for all SBA’s
• No revalidation process
• Funding constraints-
• accelerated ,sytematictraining programmes by SLCP
• strengthen monitoring/ evaluation
• SLCP in process of mandating with MoH
• MoH to initiate revalidation process
• MoH to fund
STRATEGIES & SOLUTIONS
Neonatal ResuscitationAdvanced Neonatal Resuscitation Module
BOTTLENECKS
• For MO’s – NALS optional a present
• Need to make requirement
• Emergency equipment - not ideal in labourrooms/theaters
• Training models –(mannikins) not freely available for simulation in units
• MoH/SLCP – to mandate NALS for MO’s in SCBU
• Regular training- MoH /SLCP
• MoH - provide funding- for training, equipment (rather than WHO/UNICEF)
• Stringent maintenance requirements (check lists) -implementation- MoH
STRATEGIES & SOLUTIONS
Basic Newborn CareEssential newborn care Module
BOTTLENECKS
• Need to inculcate staff on ENC concepts -
• to deliver the baby to mother’s abdomen
• skin-to-skin contact
• Temperature control (KMC)
• Establishing breast feeding
• Delayed cord clamping (small baby)
• Mandatory training & re-validation of ENCC for SBA’s
MoH /SLCP to initiate
• Regular W/shops on ENCC
• Promote clinical audit by medical & nursing staff
STRATEGIES & SOLUTIONS
Basic newborn careKangaroo Mother Care(KMC)
BOTTLENECKS
• Implementation of KMC at the facility level not ideal
• Staff not confident
• No system to deliver KMC at community level
• KMC not scaled up as intervention.
• Train/ motivate staff-paediatrician to play leadership role, scale up
• PHM to educate/train PN mothers at home
• Set up Mother-Baby Units(MBU)- low cost units, ideal for KMC
STRATEGIES & SOLUTIONS
Prevention of neonatal infections(10%)barrier nursing principles
BOTTLENECKS
• hand washing protocol-poorly followed
• Barrier nursing principles
• Poor supplies of -
• Antiseptic liquid soap (iodophore-iodine or chlorhexidine scrub) -
• Single use clean, dry towels
• Use of hand alcohol scrub –not universal
• Infection control training
• Adequate funding for consumables
• Adequate supplies
• Infection audits & check lists
STRATEGIES & SOLUTIONS
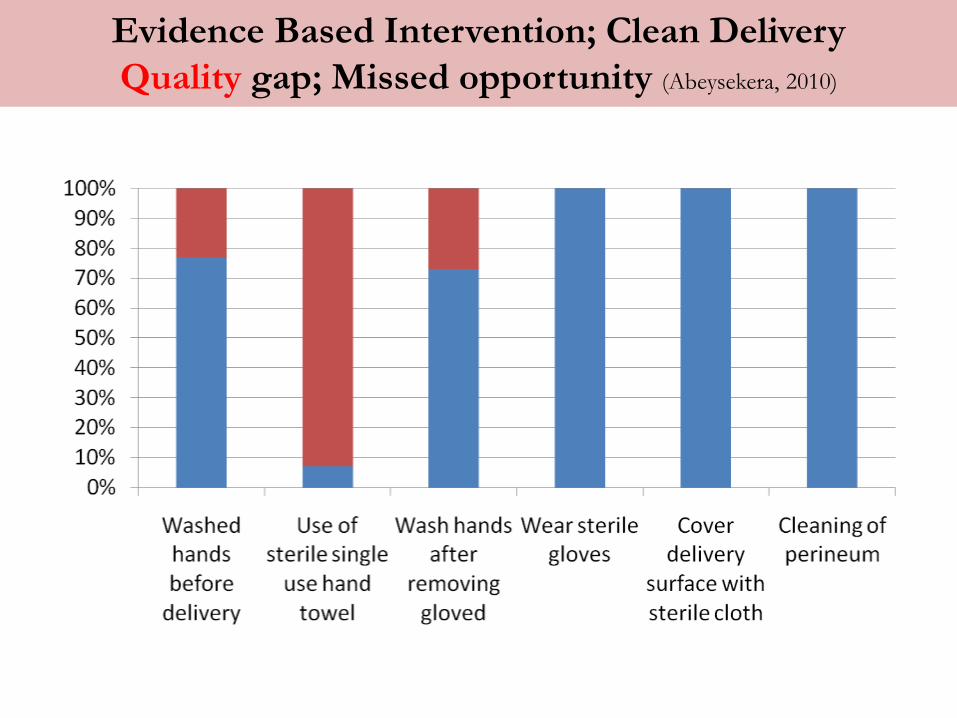
Evidence Based Intervention; Clean Delivery
Quality gap; Missed opportunity (Abeysekera, 2010)
Scaling up carefor the
Sick Newborn
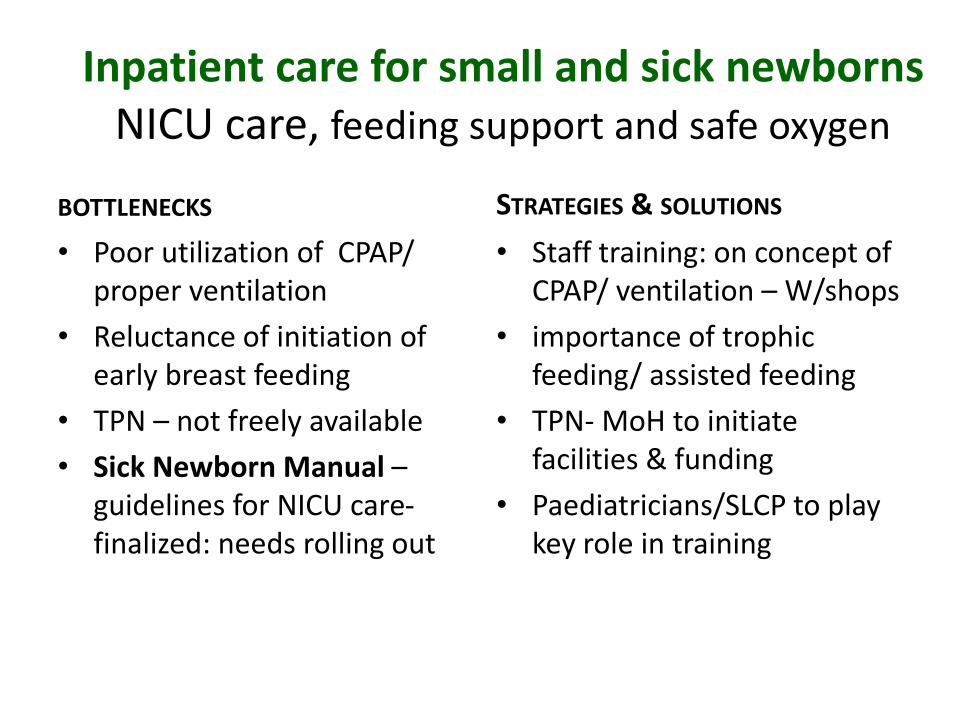
Inpatient care for small and sick newbornsNICU care, feeding support and safe oxygen
BOTTLENECKS
• Poor utilization of CPAP/ proper ventilation
• Reluctance of initiation of early breast feeding
• TPN – not freely available
• Sick Newborn Manual –guidelines for NICU care-finalized: needs rolling out
• Staff training: on concept of CPAP/ ventilation – W/shops
• importance of trophic feeding/ assisted feeding
• TPN- MoH to initiate facilities & funding
• Paediatricians/SLCP to play key role in training
STRATEGIES & SOLUTIONS
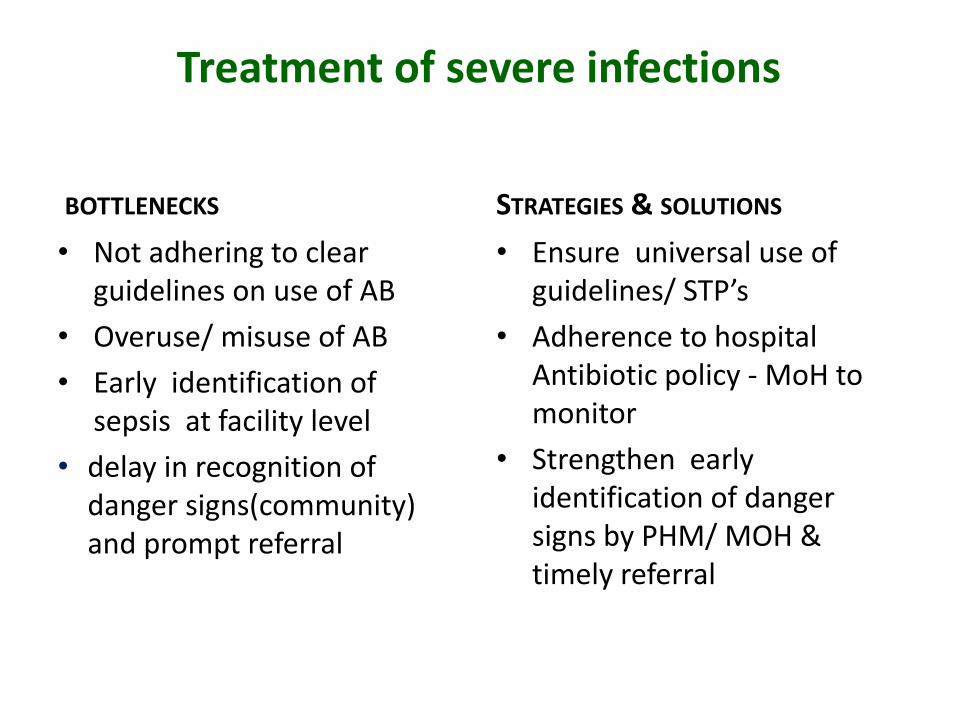
Treatment of severe infections
BOTTLENECKS
• Not adhering to clear guidelines on use of AB
• Overuse/ misuse of AB
• Early identification of sepsis at facility level
• delay in recognition of danger signs(community) and prompt referral
• Ensure universal use of guidelines/ STP’s
• Adherence to hospital Antibiotic policy - MoH to monitor
• Strengthen early identification of danger signs by PHM/ MOH & timely referral
STRATEGIES & SOLUTIONS
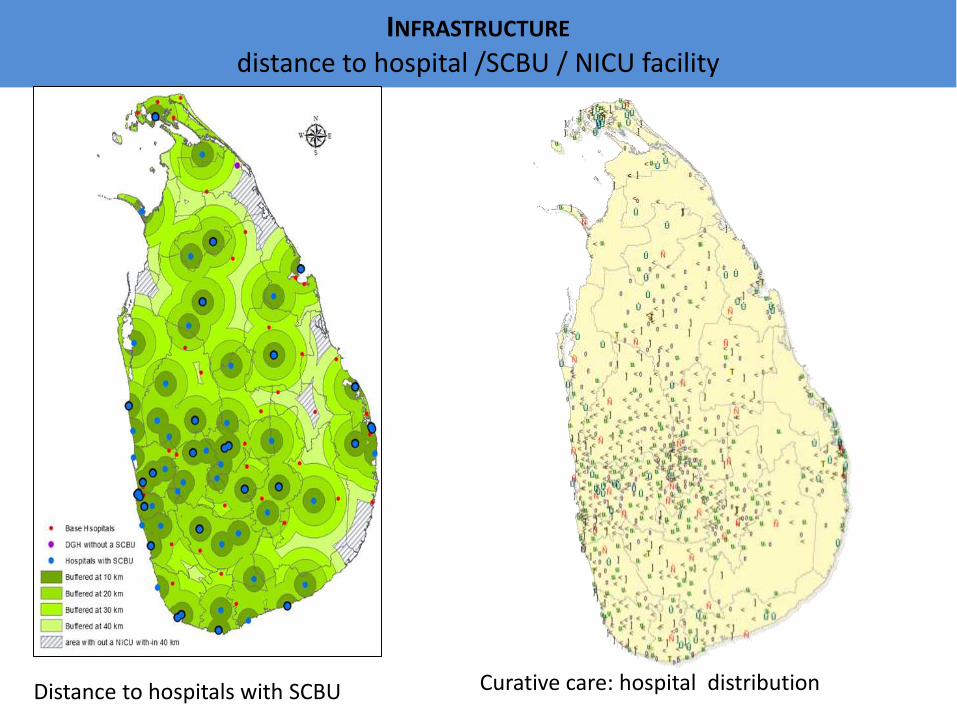
INFRASTRUCTURE
distance to hospital /SCBU / NICU facility
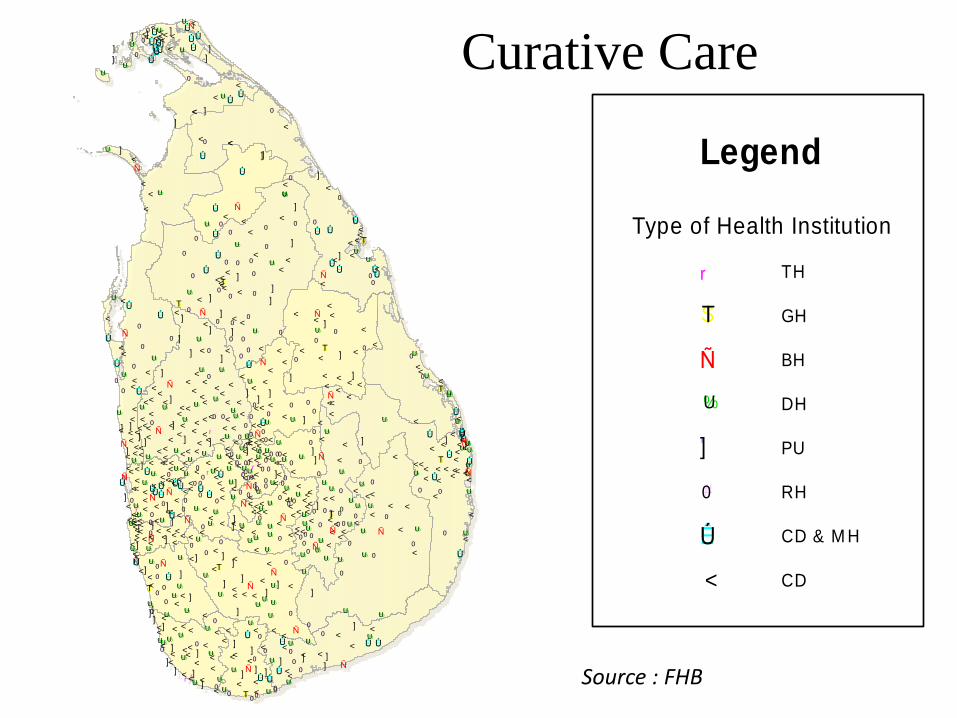
Curative care: hospital distribution Distance to hospitals with SCBU
Human resources & equipment
BOTTLE NECKS
• Staffing constrains
• Adequate equipment
• Standard setting for SCBU/NICU
STRATEGIES & SOLUTIONS
• Standard setting –Minimum requirements for levels of SCBU/NICU
• Minimum staffing ratio –nurses, doctors, MW
• EmNOC survey (2012) - did needs analysis- MoH to conform to needs
Reducing post neonatal causes
• Congenital defects
CHD (11%)
• Neural tube defects(5%)
• Severe RI (7%)
• DHF(<1%)
• Infrastructure
• Human resources/ staffing
• Financing
• Pre-preg FA supplementation
• Early detection
• AB policy
• Pneumococcal vaccine?
Dengue H’gic Fever
• early case detection- clinical- public awareness
lab – Dengue NS1 Ag test
• Improving case management – staff training(WHO team, Thailand), incorporated into paediatric PG curriculum
• Dengue corners in hospitals/wards
• PREVENTION – vector control – breeding site surveillance
• legal action taken
• Dengue Task Force/ Centre for Clinical Mx of DHF
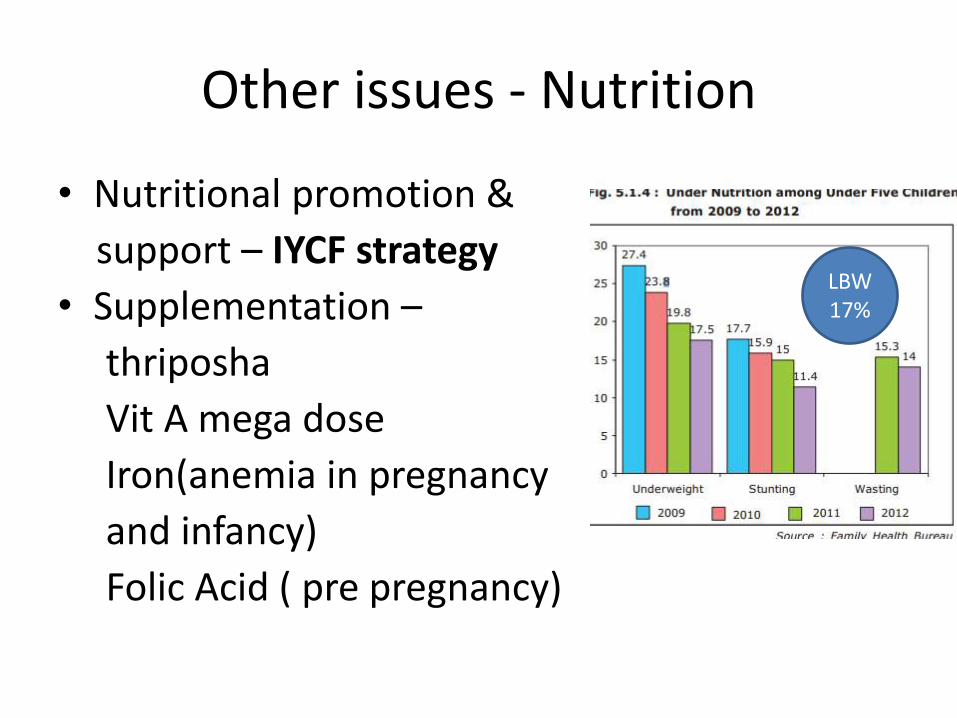
Other issues - Nutrition
• Nutritional promotion &
support – IYCF strategy
• Supplementation –
thriposha
Vit A mega dose
Iron(anemia in pregnancy
and infancy)
Folic Acid ( pre pregnancy)
LBW 17%
Medical Information System(MIS)
• Transition into real time data base- E-IMMR
• Networking NICU/SCBU/maternity units
• Bed surveillance system initiated
• Feto- infant mortality survey & birth defect register initiated
• NN morbidity/paed. death reviews to start soon
Policy Framework• National Policy on Maternal and
Child Health, 2012
• Sri Lanka Code for Promotion,
Breastfeeding and Marketing of
Designated Products, 2002
• National Strategic Plan on Maternal
and Newborn Health, 2012-2016
• National Nutrition Policy, 2010
• IYCF strategy – 2007
• LBW prevention strategy( being
formulated)
Post 2015 agenda reduce NNMR
• Improve facilities/staffing of the neonatal units
• identify levels of NB care
• Staff training -improve knowledge/skills
• Establish NN retrieval system & proper communication
–
• Neonatal Forum established (2014)
24
Post 2015 agendaReduce U-5 MR- post NN causes
• Advanced Paediatric Life support
• PICU bed surveillance system & increase PICU beds
• Immunization - Pneumococcal vaccine?
• Case management- Paediatric STPs, DHF training
• Anaemia & nutritional support
• Expand paediatric cardiology
• Paediatric / neonatal retrieval system
• Paediatric death reviews

Thank you
• Acknowledgments:
• Dr. Srilal de Silva
• Dr. Dhammica Rowel
• Family Health Bureau
NN information system
New born formats used in all the hospitals
Information from the same included into the eIMMR
NICU surveillance & bed system(networking NICU’s) to be initiaited
feto infant mortality surveillance/birth defect surveillance initiated
NN morbidity audits – to be initiated

Born Too Soon
Of the 6.9 million who die
before their 5th birthday…..
Preterm birth is the second leading cause of death for children under 5 years, after pneumonia
1.1 million babies die directly from complications of preterm birth
Over 40% die in their first
month
Source: CHERG/WHO estimates for 2010, Li Liu et al Lancet in press, 2012
Ñ
<<<']
<
<']<Ñ<
%U']< < <
#0']<
<']<<<<<<<<<%U
<<
%U
Ñ
%U
%U
%U
%U%U
%U
%U%U
%U
%U
%U
%U
%U
']']
#0#0
<<<
<<<
<
<
<
<<
<<
<
<<
<
<
<<<
<
<
<
#0
#0
#0
#0 #0
rr
Ñ
Ñ
%U
%U
%U
%U%U
%U%U
%U
%U
%U
%U%U
%U
']
']']%U
%U
']
']
#0
#0
#0
#0
#0
#0
#0
#0
#0
#0
#0
#0
#0
#0
#0
#0#0
#0
#0
#0
#0
#0#0
#0
#0 <
<
<
<<
<
<<#0 <
<<
<
<
<
<<
<<
<
<
< <
<
<<
<
r
%U
%U%U
%U
%U%U
%U
%U
']
#0
#0
#0 #0#0
#0
#0#0
ÊÚ ÊÚÊÚ
ÊÚ
<<<<<<<<
<
<
<<
<
<<
#0
$T
Ñ
Ñ
Ñ
%U
%U
%U
%U
%U%U
%U
%U
%U
%U
']']
']
']
']']
']
']
#0
#0
#0
#0
#0
<
<<<
<
<<
<
<<
<
<<
<$T
Ñ Ñ%U
%U
%U
%U
%U
%U
%U
']
']
']
']
#0
#0
#0
#0
#0
#0
ÊÚ<
<
<
<
<<
<
ÊÚ
r
Ñ
Ñ
Ñ
%U
%U
%U
%U
%U
%U
']
']']
#0
#0
#0
#0
#0
ÊÚÊÚ
ÊÚ
ÊÚ <
ÊÚÊÚ
ÊÚ
ÊÚ<
<<
<
<
<<
<
<<
<<
<
<
<
<
<<<
<
<
<<
<
< <
<
<<
<
<
<
<
Ñ
Ñ
%U
%U %U ']
']']']
#0
#0
#0
#0
#0#0
ÊÚ
ÊÚ<
<
<
<
<
< <
#0<< #0
<
<
<<#0
<
Ñ
%U
%U
%U
%U']
'] ']
']
'] #0#0
#0
#0
#0
ÊÚ ÊÚ
ÊÚ
ÊÚ
ÊÚ
<<
<
<<
#0 <
<
<<
rr
%U%U%U
%U
%U
%U
%U
%U
%U']
']
']
']']
']']
']
']
#0
#0#0
#0
<
<
<
<<
<
<
<
<
<
< <<
<<
<
<
<<
<
<
<
<
Ñ%U
%U
%U
%U
%U
%U
%U
%U
%U
']
#0
#0#0
#0
#0
#0
#0
<
<<
<
<
<
<
<<
rÑ
Ñ
%U
%U
%U
%U
%U
%U
%U
%U
%U
%U%U
%U
%U%U
%U
']
']']
']']
']
']
']
']
']
']
']
#0
#0
#0
#0#0#0
#0
<
<
<
<
<
<
<
<
<
< <
<
<
<
<
<
<
<
<<
<
<<
<
<
<
<
<
<
<
<
<
<
<
<<
<
<
<
<
<
<<
<
<
<
<<
<
<
<<
<
<
$T
Ñ
Ñ
%U
%U
%U
%U
%U%U
%U%U
%U
%U
%U
%U
%U
']
#0
#0 #0
#0
#0 #0
#0
#0
#0
#0
#0
#0
#0
#0
#0
<<
<
<
<
<
<<
<<
<
<
<
']
<
<<Ñ
<
%U
Ñ
%U ']<
<<
<
ÊÚ
']']
<
Ñ
<<
#0
ÊÚ
%U
ÊÚ
#0%U
<<#0%U
$T<
%U%U
ÊÚ<%U%UÊÚ<ÊÚ
<
<Ñ
ÊÚ<']
$T<%U
<
ÊÚ
#0#0ÊÚ<
%U
ÊÚ
<<<
ÊÚ
#0
<
']#0
ÊÚ
#0
ÊÚ
Ñ
ÊÚ<
#0
ÊÚ
#0
%U
#0
#0<
ÊÚ
%U<<
<']<
Ñ
< < <<
<
%U
<
ÊÚ<
#0
ÊÚ<
%U
#0<<
<%U<']']
']#0
#0
<
<<
']< <<
%U
Ñ <<
<<
#0
']
']
#0
<<
< <
$T
<
#0
#0<
ÊÚ
<
#0#0
%U#0
']']
<
%U
<<
']ÊÚ
<%U
#0
']#0<
Ñ'] ÊÚ<
<$T#0%U
']
%U<
#0
']
<< ']
ÊÚ<
ÊÚ
%U
<
%U
%U<Ñ']%UÊÚ
< <
']<
%U<%U']%UÑÑ<']ÊÚ
ÊÚ
%U
ÊÚ
<<
<<<
<
<
< %U ÊÚ
ÊÚÑ%U
']
ÊÚÊÚ
%U
#0
<ÊÚ<<<<
<ÊÚ<#0
<<']']
<<<
%U
ÊÚ#0']
%U
ÊÚÊÚ
<
ÊÚrÊÚÊÚ
%U
']
']
#0
$T'] #0
']
']#0<
#0
%U<<
']
']#0
#0
<<<<
ÊÚ
#0
#0
#0
%U
<$T#0 Ñ
']#0#0
#0 #0
#0#0 <
<<%U
#0']
#0
']
%U
<
%U
#0 <#0
<
<#0#0#0
ÊÚ
<
<
%U
$T<ÊÚ<
#0<
<#0
#0
ÊÚ
<<<
< <ÊÚ
%U
']
<
<<Ñ
<<
'] Curative Care
Type of Health Institution
THr
GH$T
BHÑ
DH%U
PU']
RH#0
CD & M HÊÚ
CD<
Legend
Source : FHB
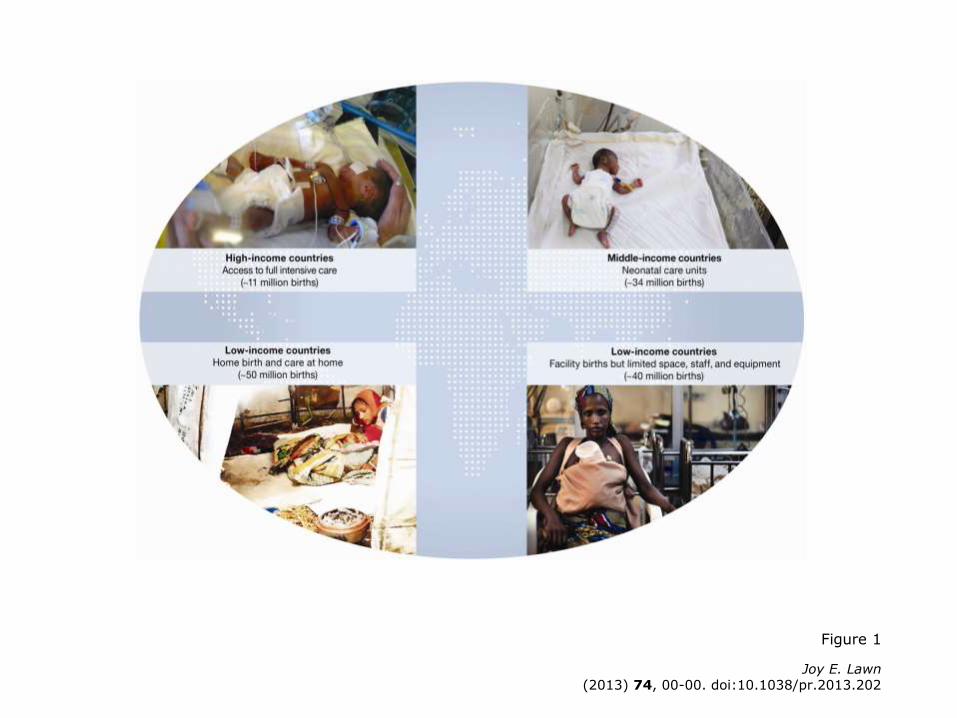
Figure 1
Joy E. Lawn(2013) 74, 00-00. doi:10.1038/pr.2013.202
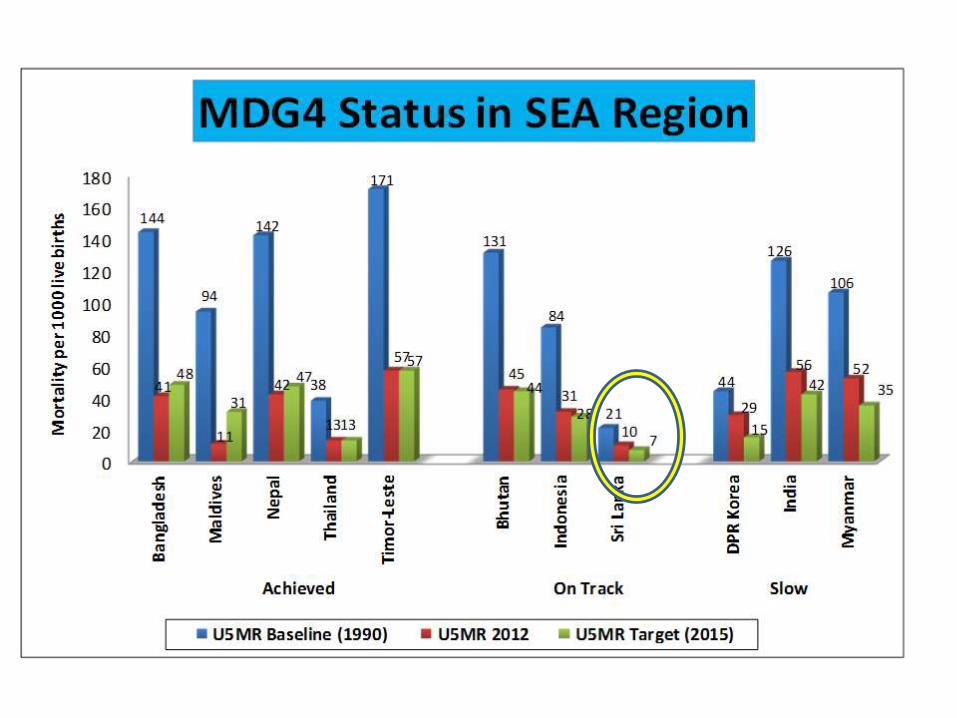
Where do we stand?MDG 4 - Reduce child mortality
– Under 5 mortality fell 41% from 1990– Sub-Saharan Africa doubled its average rate of reduction : 1.2 % in 1990-2000 to
2.4 per cent during 2000-2010
MDG 5a - Improve maternal healthMaternal mortality fell 47% from 1990
MDG 5b - Universal access to reproductive healthBy 2008, more than 50%women aged 15 -49yrs were using contraception
MDG 6 - HIV/AIDS, malaria and other diseasesNew HIV infections declined; Proportion of women living with HIV remains stable at
50%
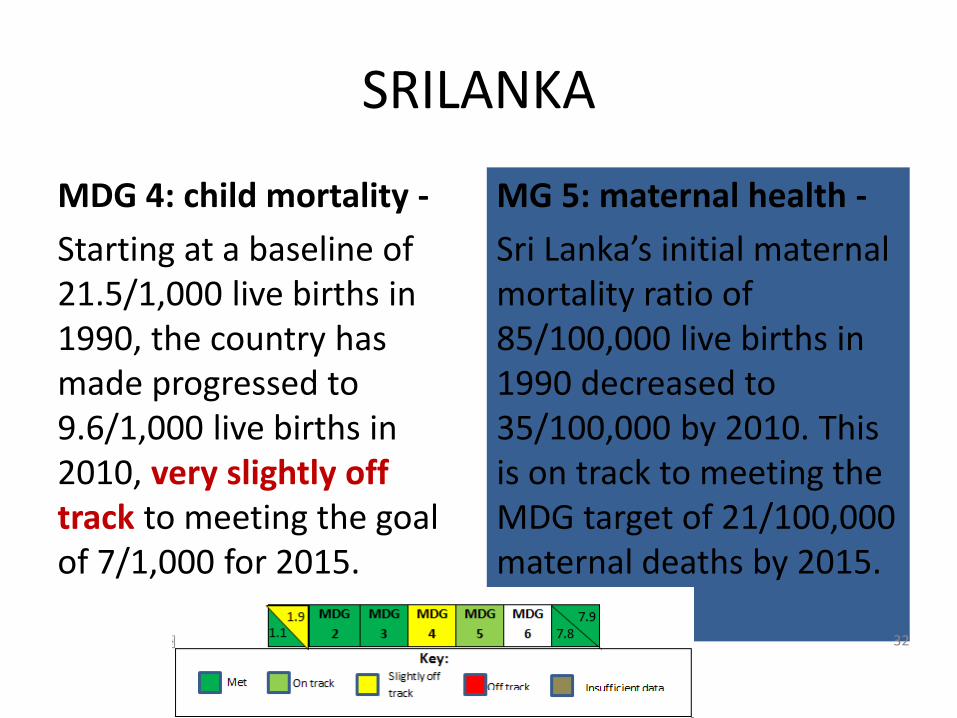
SRILANKA
MDG 4: child mortality -
Starting at a baseline of 21.5/1,000 live births in 1990, the country has made progressed to 9.6/1,000 live births in 2010, very slightly off track to meeting the goal of 7/1,000 for 2015.
MG 5: maternal health -
Sri Lanka’s initial maternal mortality ratio of 85/100,000 live births in 1990 decreased to 35/100,000 by 2010. This is on track to meeting the MDG target of 21/100,000 maternal deaths by 2015.
32

Intervention packages for reduction of neonatal deaths by current mortality rates
Estimated effect of the number of neonatal lives saved by the different intervention packages by the year 2025
33
The Lancet Newborn Interventions Review Group and The Lancet Every Newborn Study Group . Every Newborn 3 - Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet Early Online Publication, 23 June 2014. doi:10.1016/S0140-6736(14)61001-1
Monitoring for quality issues
PRIORITY BOTTLENECKS
• Administrative, procurement and proper resource allocation issues.
• Out of pocket payments required by clients
• Quality issues and lack of proper monitoring / accountability mechanism
STRATEGIES AND SOLUTIONS
STRATEGIES AND SOLUTIONS
• Proper record keeping, monitoring / accountability mechanism in place
• Child Death audit have not initiated in the facilities (SCNUs) managing severe infections

Goal 4: Reduce Child Mortality
MDG 4 Target
Reduce by two-thirds, between 1990 and
2015, the under-five mortality rate
Indicator
Under-five mortality rate
Infant mortality rate
Proportion of 1 year-old children
immunized against measles
35
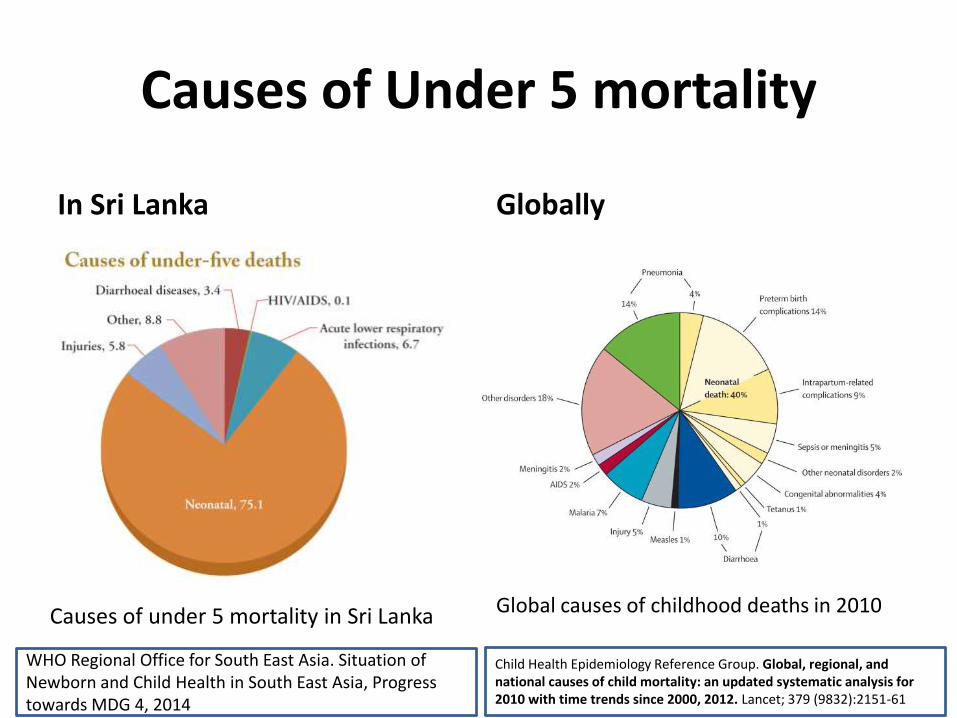
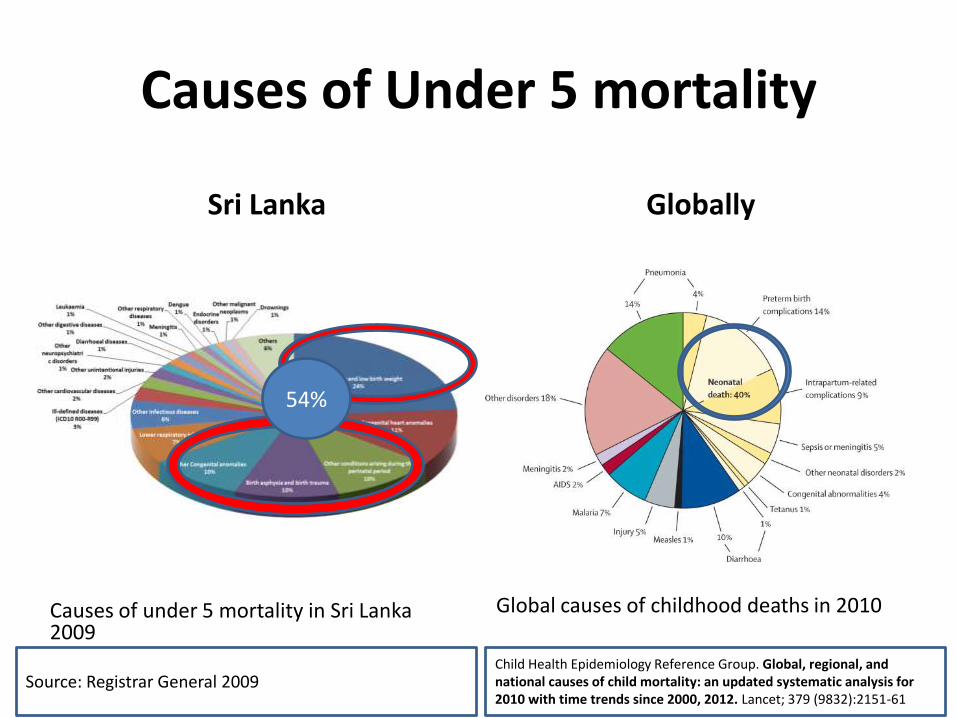
Causes of Under 5 mortality
In Sri Lanka Globally
Neonatal 75.1
Child Health Epidemiology Reference Group. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000, 2012. Lancet; 379 (9832):2151-61
Global causes of childhood deaths in 2010
WHO Regional Office for South East Asia. Situation of Newborn and Child Health in South East Asia, Progress towards MDG 4, 2014
Causes of under 5 mortality in Sri Lanka
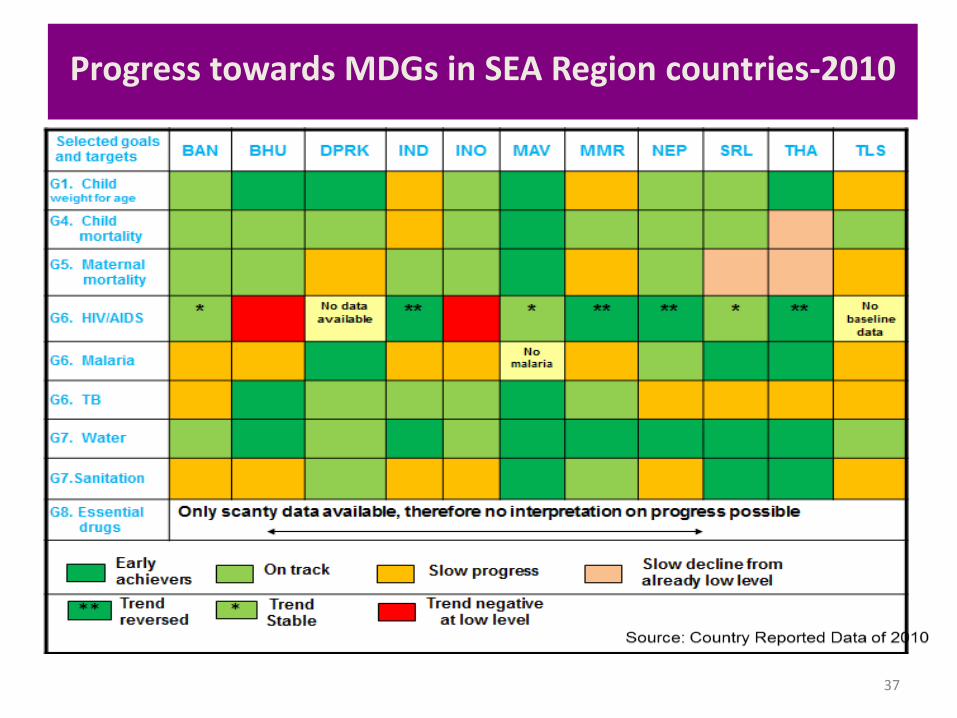
Progress towards MDGs in SEA Region countries-2010
37

RH services- preconception
BOTTLE NECKS
• Preconception folic acid
• Family counseling by PHM
STRATEGIES & SOLUTIONS
• In place – compliance?
• Strengthen awareness-publicity campaigns
• Mass media
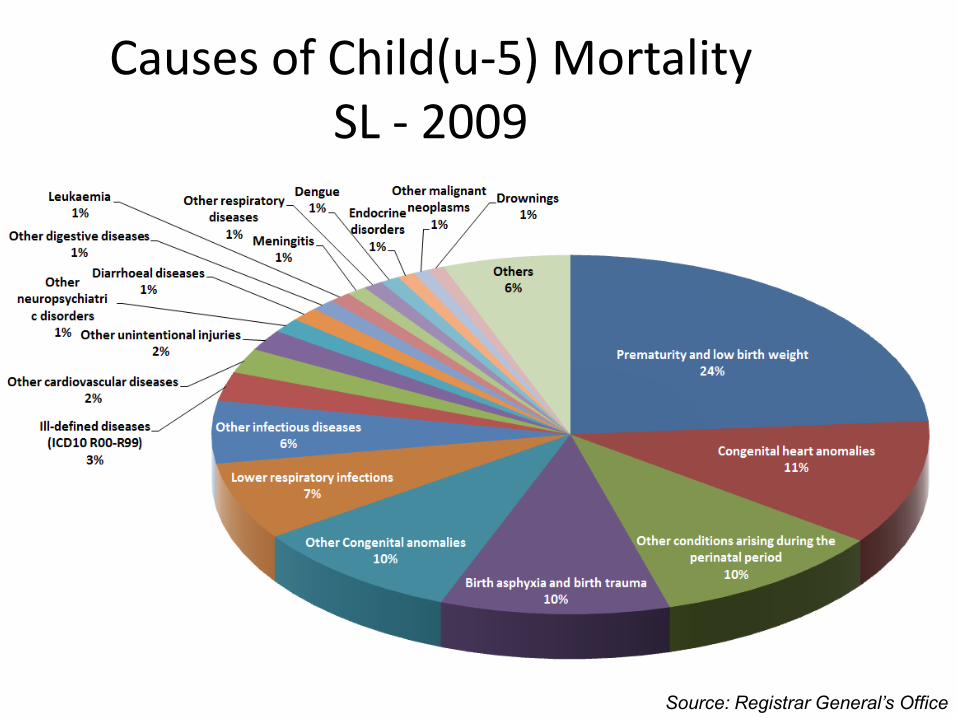
Causes of Child(u-5) Mortality SL - 2009
Source: Registrar General’s Office
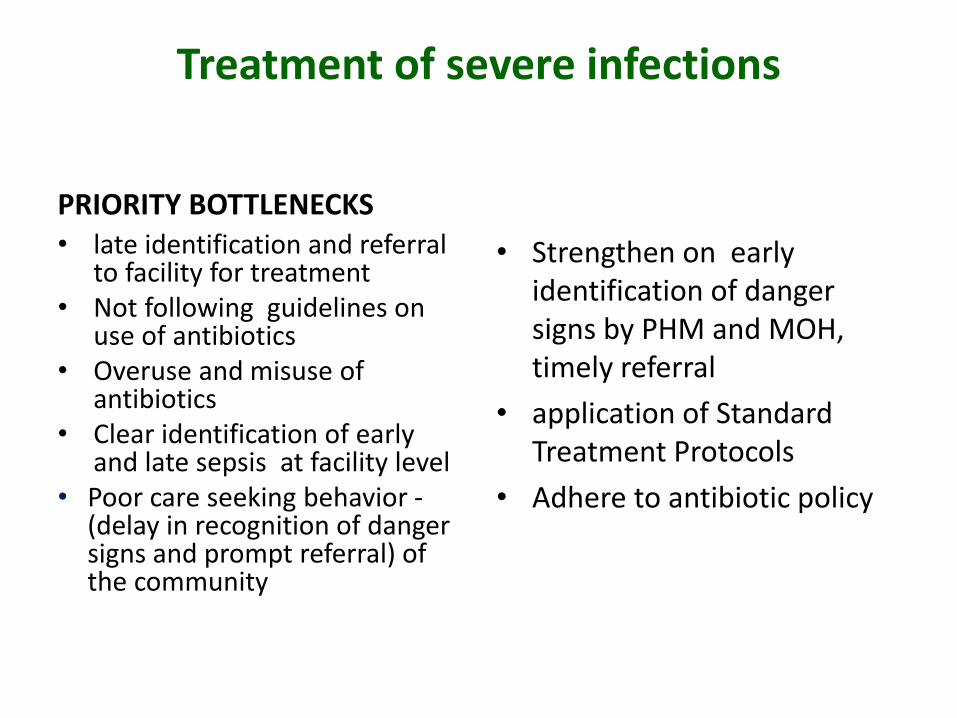
Treatment of severe infections
PRIORITY BOTTLENECKSSTRATEGIES AND SOLUTIONS
STRATEGIES AND SOLUTIONS
• late identification and referral to facility for treatment
• Not following guidelines on use of antibiotics
• Overuse and misuse of antibiotics
• Clear identification of early and late sepsis at facility level
• Poor care seeking behavior -(delay in recognition of danger signs and prompt referral) of the community
• Strengthen on early identification of danger signs by PHM and MOH, timely referral
• application of Standard Treatment Protocols
• Adhere to antibiotic policy
13th Annual Academic Sessions Perinatal Society of Sri Lanka 2014
41
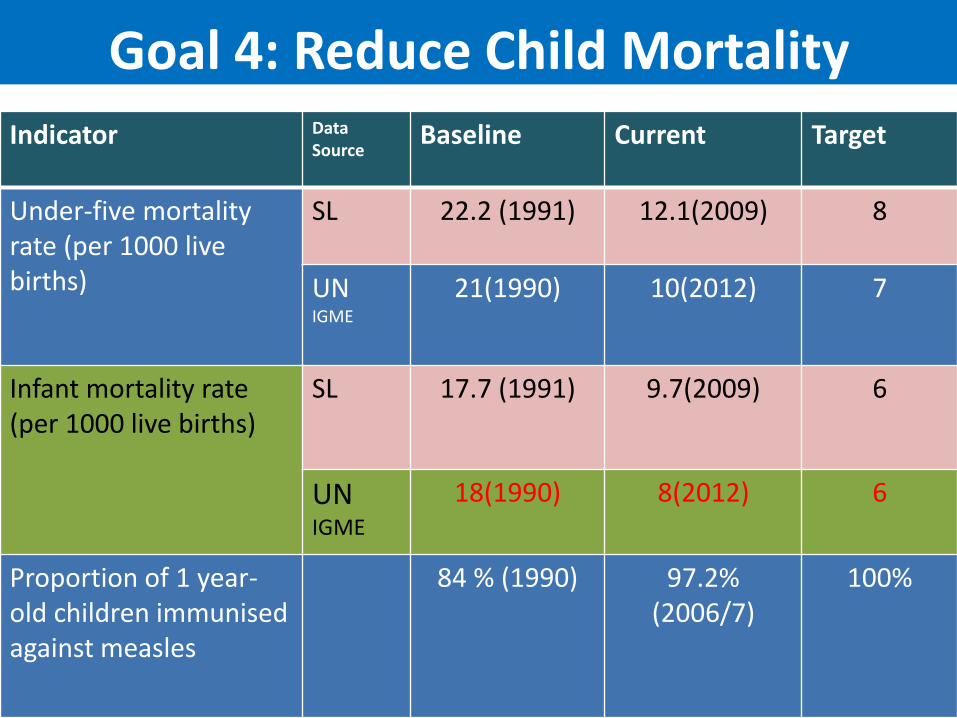
Goal 4: Reduce Child Mortality
Indicator Data Source
Baseline Current Target
Under-five mortality rate (per 1000 live births)
SL 22.2 (1991) 12.1(2009) 8
UNIGME
21(1990) 10(2012) 7
Infant mortality rate (per 1000 live births)
SL 17.7 (1991) 9.7(2009) 6
UNIGME
18(1990) 8(2012) 6
Proportion of 1 year-old children immunised against measles
84 % (1990) 97.2% (2006/7)
100%
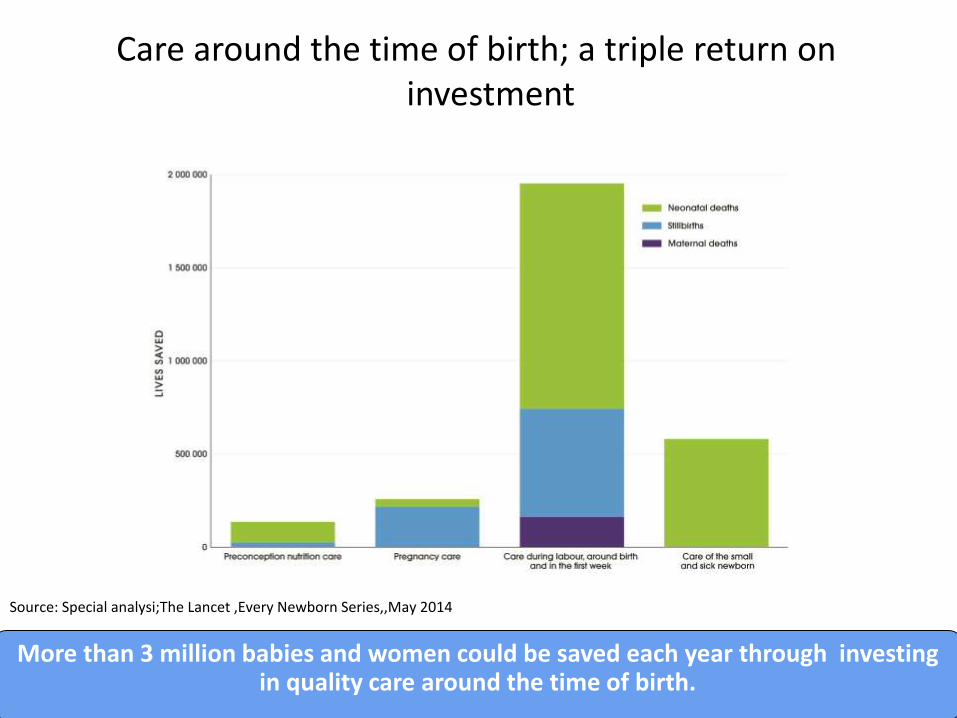
Care around the time of birth; a triple return on investment
Source: Special analysi;The Lancet ,Every Newborn Series,,May 2014
More than 3 million babies and women could be saved each year through investing in quality care around the time of birth.
Causes of Under 5 mortality
Sri Lanka Globally
Neonatal 75.1
Child Health Epidemiology Reference Group. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000, 2012. Lancet; 379 (9832):2151-61
Global causes of childhood deaths in 2010
Source: Registrar General 2009
Causes of under 5 mortality in Sri Lanka 2009
54%
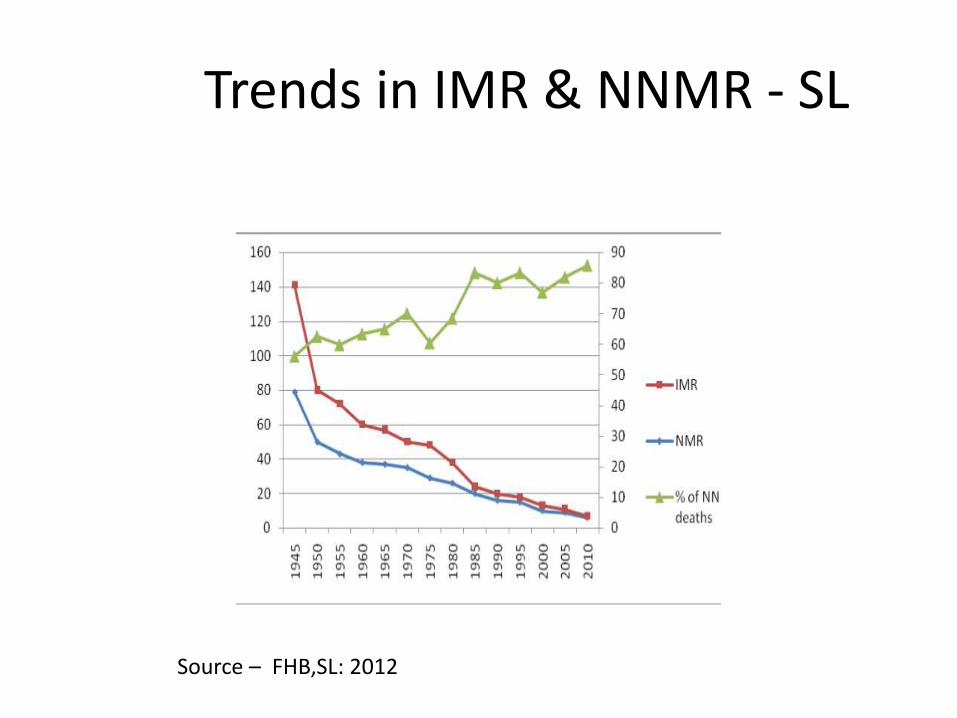
Trends in IMR & NNMR - SL
Source – FHB,SL: 2012