Spotlight Errors in Sepsis Management. This presentation is based on the May 2015 AHRQ WebM&M...
30
Spotlight Errors in Sepsis Management
-
Upload
gerald-henry-webster -
Category
Documents
-
view
217 -
download
1
Transcript of Spotlight Errors in Sepsis Management. This presentation is based on the May 2015 AHRQ WebM&M...
Spotlight
Errors in Sepsis Management
2
• This presentation is based on the May 2015AHRQ WebM&M Spotlight Case– See the full article at http://webmm.ahrq.gov – CME credit is available
• Commentary by: David Shimabukuro, MD, University of California, San Francisco (UCSF)– Editor, AHRQ WebM&M: Robert Wachter, MD– Spotlight Editor: Bradley A. Sharpe, MD– Managing Editor: Erin Hartman, MS
Source and Credits

3
Objectives
At the conclusion of this educational activity,
participants should be able to:• Define sepsis, severe sepsis, and septic shock• Describe the severe sepsis/septic shock
resuscitation bundle• Recognize commonly encountered pitfalls in the
implementation of the resuscitation bundle• List best practices to reduce sepsis-related
mortality
4
Case: Sepsis Management
A 72-year-old woman with pulmonary hypertension, chronic obstructive pulmonary disease (COPD) on home oxygen, and coronary artery disease presented to the hospital with left-sided abdominal pain and shortness of breath. She had been hospitalized for an exacerbation of her COPD 3 weeks prior but had been doing well at home on home oxygen. In the emergency department, she was ill appearing and in some respiratory distress. Her vital signs were notable for a temperature of 38.6° C, heart rate of 115 beats per minute, blood pressure of 104/68 mm Hg, respiratory rate of 28 breaths per minute, and oxygen saturation of 86% on her baseline 2 liters.
5
Case: Sepsis Management (2)
She was found to have decreased breath sounds at the left base and appeared dehydrated. She had a white blood cell count of 21.4 x 109/L, creatinine of 2.1 mg/dL (up from a baseline of 1.3 mg/dL), a lactate of 3.9 mg/dL, and an international normalized ratio (INR) of 1.5. A chest radiograph revealed an infiltrate in the left lower lobe and she was diagnosed with pneumonia. She was given 1 liter of normal saline in the emergency department but, because of her history of pulmonary hypertension and coronary artery disease, she was not given any additional intravenous fluids. Blood cultures were drawn and she received levofloxacin (administered approximately 3 hours after presentation).
6
Case: Sepsis Management (3)
She was admitted to the transitional care unit but slowly worsened. Twenty-four hours after admission, her blood cultures grew methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin was added to her antibiotic regimen. Despite the antibiotics and additional intravenous fluids, she continued to deteriorate. The patient developed respiratory failure requiring mechanical ventilation as well as septic shock requiring vasopressors. Her illness progressed and in discussions with her family, the decision was made to withdraw life-sustaining therapies and allow her to die peacefully. She died on hospital day 4 with her family at her bedside.
7
Background
• Every year in the US, approximately 750,000 adults are diagnosed with sepsis, severe sepsis, or septic shock
• Mortality rate of more than 30%• Sepsis affects each patient differently but is
always initiated by an infection• Sepsis always involves activation of the host
inflammatory response and often includes dysregulation of the clotting−bleeding balance leading to end-organ damage
8
Sepsis
• Sepsis is defined by presence of at least 2 elements of the systemic inflammatory response syndrome (SIRS) with a documented or suspected infection
• Elements of SIRS include vital sign and laboratory data: – Temperature > 38.3°C or < 36°C– Heart Rate > 90 beats per minute– Tachypnea– White blood cell (WBC) count > 12x109/L or < 4x109/L– Hyperglycemia (glucose > 140 mg/dL) in the absence of
diabetes– C-reactive protein more than twice the upper limit of normal– Procalcitonin more than twice the upper limit of normal
9
Severe Sepsis
• Severe sepsis is defined as sepsis plus evidence of end-organ damage likely related to the location of the infection or from a dysregulated host response
• End-organ damage can be identified by several factors (see next slide)
10
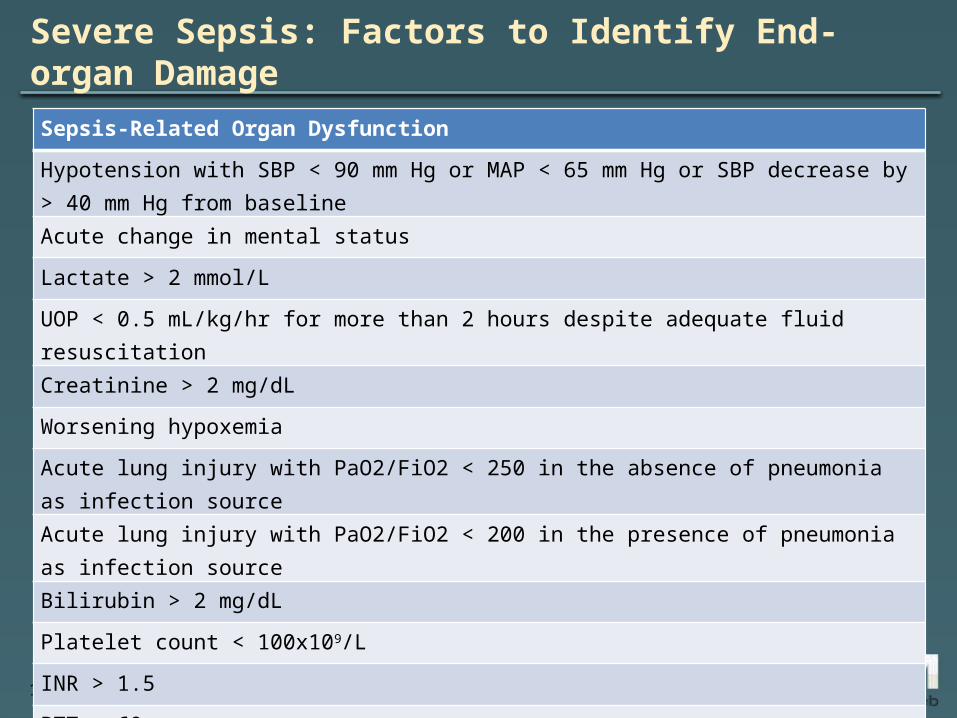
Severe Sepsis: Factors to Identify End-organ Damage
Sepsis-Related Organ Dysfunction
Hypotension with SBP < 90 mm Hg or MAP < 65 mm Hg or SBP decrease by > 40 mm Hg from baseline
Acute change in mental status
Lactate > 2 mmol/L
UOP < 0.5 mL/kg/hr for more than 2 hours despite adequate fluid resuscitation
Creatinine > 2 mg/dL
Worsening hypoxemia
Acute lung injury with PaO2/FiO2 < 250 in the absence of pneumonia as infection source
Acute lung injury with PaO2/FiO2 < 200 in the presence of pneumonia as infection source
Bilirubin > 2 mg/dL
Platelet count < 100x109/L
INR > 1.5
PTT > 60 s
11
Septic Shock
• Septic shock is defined as severe sepsis with lactate ≥ 4 mmol/L or hypotension (mean arterial pressure [MAP] < 65 mm Hg; systolic blood pressure < 90 mm Hg) not responsive to a fluid bolus
• In this case, the patient presented to the emergency department with severe sepsis – She had 4 SIRS criteria, suspected pulmonary
infection, and end-organ dysfunction
12
Initial Management
• Initial management involves treatment with the "resuscitation bundle"
• The bundle, updated in the Surviving Sepsis Campaign in 2013, includes numerous elements that must be completed in a timely manner

13
Resuscitation Bundle
• Based on a NEJM study published in 2001, the bundle includes the following:– Measuring serum lactate levels– Drawing blood cultures (before antibiotics)– Treating with appropriate broad-spectrum
antibiotics– For septic shock, targeting goals for CVP (8−12
mm Hg), MAP (≥ 65 mm Hg), and superior vena cava oxygen saturation (70%)
14
Resuscitation Bundle (2)
• Antibiotics should be given early—within 3 hours in the ED and 1 hour if patient is in hospital
• Intravenous fluids should be given promptly with an initial bolus of 30 mL/kg (~ 2−3 liters)
• Vasopressors can be used in septic shock to achieve the target goals for CVP and MAP
• Other components guide management of ventilation, use of steroids, transfusion thresholds, and conversations about goals of care
15
Antibiotics
• Early, appropriate broad-spectrum antibiotics are essential in managing sepsis
• One study showed that for patients with severe sepsis, every hour delay is associated with a 7% increase in mortality
• Empiric antibiotics should be based on local resistance patterns and the patient's risk factors for resistant organisms (e.g., MRSA)

16
Antibiotics in This Case
• In this case, the timing of antibiotics was appropriate as the patient was in the ED (goal is within 3 hours)
• She had been hospitalized 3 weeks prior so was at risk for resistant organisms
• She should have been treated empirically with vancomycin and an agent with broad-spectrum gram-negative coverage (e.g., cefepime, piperacillin/tazobactam)

17
Errors in Sepsis Management
• Errors in sepsis management range from inadvertent and/or purposeful deviations to omissions from resuscitation bundle
• Certain elements are essential even if the patient with sepsis appears well and concern for serious infection is low. These include:– Checking a serum lactate– Drawing blood cultures– Starting empiric antibiotics
18
Time to Antibiotics
• The time pressure to implement the bundle elements is real
• Achieving all of them quickly is difficult• Many institutions have created "sepsis
teams" to improve efficient bundle compliance
19
UCSF Sepsis Team
• At UCSF, inpatient Sepsis Team is comprised of a critical care nurse practitioner (NP), a rapid response nurse, and a pharmacist– The NP communicates with primary physician
and facilitates ordering bundle elements– The rapid response nurse helps bedside nurse
quickly implement the orders (e.g., antibiotics)– The pharmacist facilitates rapid antibiotic
administration
20
UCSF Sepsis Team (2)
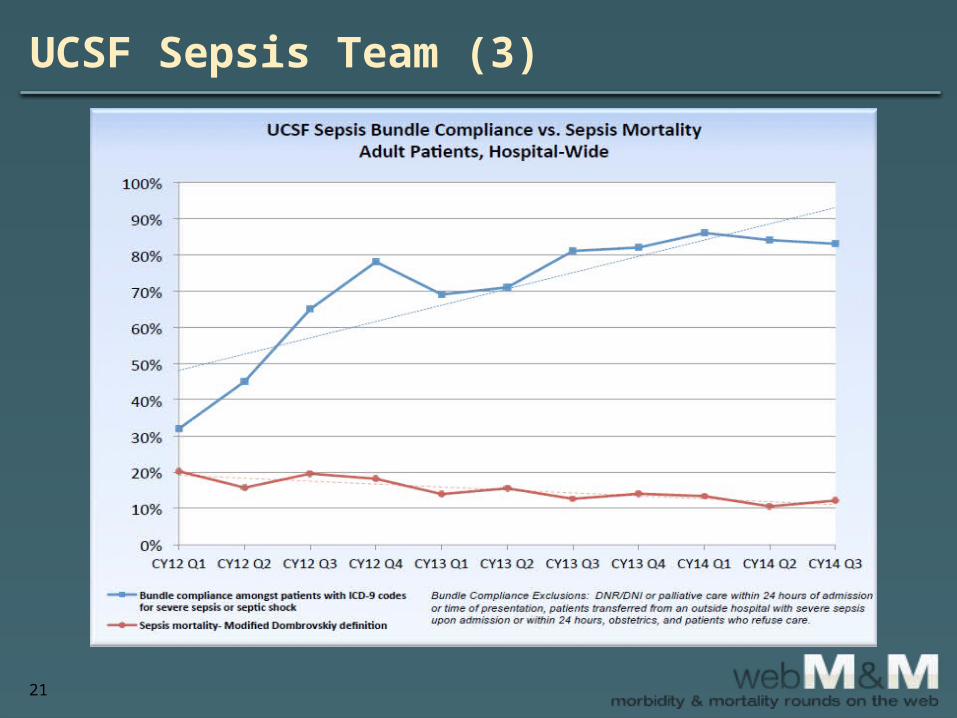
• Since the creation of UCSF sepsis team in fall 2012, inpatient bundle compliance has increased from less than 5% to nearly 80%
• Over the same time period, bundle compliance in UCSF ED has increased from 40% to over 90%
• UCSF institutional adult sepsis mortality has fallen from just over 20% to approximately 12%
21
UCSF Sepsis Team (3)
22
Initial Recognition of Sepsis
• Initial recognition of sepsis can be difficult• Practitioners may often attribute early
symptoms to other conditions such as pain, delirium, or medication effects
• Severe sepsis/septic shock can mimic other serious conditions such as pancreatitis, cardiogenic shock, and hemorrhagic shock
• The Surviving Sepsis Campaign guidelines recommend a sepsis screening tool to mitigate this
23
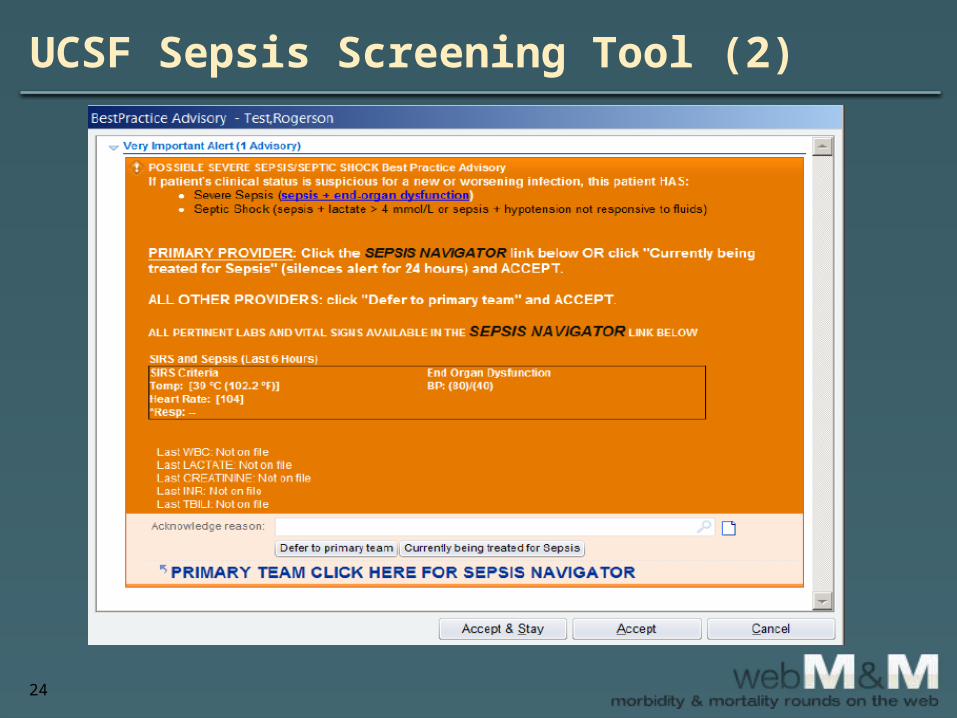
UCSF Sepsis Screening Tool
• UCSF has created real-time electronic surveillance of vital signs and laboratory values
• Whenever severe sepsis criteria are met an alert to nurses and providers is generated
• The "Sepsis Alert" generated is present whenever the bedside nurse or other providers access that patient’s electronic record
24
UCSF Sepsis Screening Tool (2)

25
UCSF Sepsis Screening Tool (3)
• While the automated screening is not perfect, UCSF internal data analysis shows that alerts have a positive predictive value of around 70%
• Institutions should work to develop systematic ways to screen patients in the ED and inpatient units to allow for earlier detection of sepsis
26
Feedback
• Collecting and disseminating data on bundle compliance and clinical outcomes can be essential to improving sepsis care
• Feedback should be actively provided to individuals, units, and the institution as a whole
27
This Case
• In the presented case, the emergency department may or may not have had a severe sepsis/septic shock treatment protocol in place
• Had a protocol or formal process been in place, the patient might have received the appropriate antibiotic therapy
• Such treatment could have altered her hospital course
28
Take-Home Points
• Sepsis, severe sepsis, and septic shock are on a continuum and are commonly referred to as "sepsis"
• Sepsis is a very heterogeneous disease – Difficult to diagnose in its early stages – Difficult to treat in its later stages– However, routine screening may aid in early
identification
29
Take-Home Points (2)
• Sepsis intervention– Early and timely intervention should include
elements of a well-established bundle • Antibiotics• Source control• Fluid resuscitation• Maintenance of MAP
– Such intervention can attenuate the course of sepsis and possibly decrease associated mortality
– However, supportive care is the mainstay of treatment

30
Take-Home Points (3)
• Institutions should create robust patient safety and quality improvement programs that– Ensure appropriate screening – Ensure severe sepsis/septic shock bundle
compliance
• To be successful, program must have a multidisciplinary approach involving nurses, providers, and hospital administration














![Achtung: animierte GIFs in der Präsentation sind im PDF ... · Today we added support for WebM files on 4chan’s image boards. […] we only accept WebM files with one video stream](https://static.fdocuments.net/doc/165x107/5b5706be7f8b9ac5358d979b/achtung-animierte-gifs-in-der-praesentation-sind-im-pdf-today-we-added.jpg)



