SPLEEN. Professor Anwar Sheikha THE SPLEEN MAN IN THE SPLEEN LAND.

Journal of the College of Physicians and Surgeons Pakistan 2013, Vol. 23 (6): 427-429 427
INTRODUCTIONSplenic rupture is usually due to trauma to the spleen,whether external trauma (blunt or penetrating) oriatrogenic injury (e.g., during operative proceduresfor other reasons) and is rarely a spontaneousphenomenon.1 Spontaneous splenic rupture was firstdefined by Wiedemann as resulting from an incidentwithout external force. Knoblich distinguished the non-traumatic rupture of a pathological spleen from theextremely rare non-traumatic splenic rupture of unknownorigin.2 Although spontaneous splenic rupture is a rareevent, it has been reported in patients with infectiousmononucleosis, malaria, leishmaniasis, leukemia, hemo-lytic anemia, polycythemia vera and sarcoidosis.1
Rupture has also been reported in apparently normalspleen caused by stresses such as vomiting or cough.3
In 1861, Rokitansky first reported a traumatic splenicrupture in a leukemic patient, and in 1874, Atkinson firstdescribed the rupture of an apparently normal spleen.4
We present here a rare case of a patient withspontaneous rupture of the spleen associated withamyloidosis.
CASE REPORTIn October 2010, a 61-year-old man who was referred tothe Department of Cardiology because of acute onset of
generalized abdominal pain and history of hypertension(HTN) and no positive sign in abdominal examinationinitially. Thoraco-abdominal CT angiography wasperformed in order to rule out aortic dissection, whichrevealed negative result.
After 8 hours, he complained of severe abdominalpain and blood pressure (BP) fell to 90/60 mmHg.Physical examination of the abdomen was changed togeneralized tenderness and rebound tenderness. Anultrasonography revealed free fluid in the abdominalcavity and rupture of the spleen. The patient alsoshowed decreased hematocrit levels.
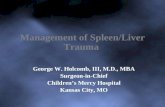
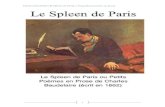
The patient was referred to the emergency surgeryservice with immediate resuscitation performed.Exploratory laparotomy revealed a hemoperitoneum of1000 cc secondary to splenic rupture. Intraoperativefindings showed the spleen divided into two sectionssharply and smoothly. So, splenectomy was performed.During operation, he was transfused with 2 units ofpacked red blood cells (RBC). After surgery, patient'sgeneral condition was satisfactory. The patient wasdischarged on the fourth postoperative day. Thepathological report of the surgical specimen reportedsplenic infiltration by amyloidosis (Figures 1 and 2).
Postoperative bone marrow biopsy revealed noevidence of amyloidosis. Also, examination of otherorgans showed no significant abnormality. One yearfollow-up showed that the patient had not received anymedications for the treatment of amyloidosis.
DISCUSSIONSpontaneous rupture of the spleen may be due tointrinsic pathology of the spleen or may be idiopathic inhealthy spleens. Idiopathic or true spontaneous splenicrupture occur in histologically normal spleen.1
CASE REPORT
Spontaneous Rupture of the Spleen Secondary to AmyloidosisHesam Shobeiri, Majid Einakchi, Mahtab Khajeh and Mohammad Reza Motie
ABSTRACT
Spontaneous splenic rupture (SSR) is a rare condition. It may be an idiopathic event or may occur secondary to apathological condition of the spleen. Systemic amyloidosis is characterized by the extracellular deposition of amyloidproteins in one or more organs. The spleen can be affected in 41% of patients. Amyloidosis and consequently, splenicrupture may occur as a complication of amyloid infiltration. We present the case of a 61-year-old male with abdominal painand hypotension. There were peritoneal signs during physical examination and falling hematocrit was reported in thelaboratory tests. The patient was suspected of having an aortic dissection. Thoraco-abdominal computed tomography (CT)angiogram was negative and ultrasonography revealed splenic rupture and free fluid in the abdominal cavity. The patientunderwent laparotomy when found hemoperitoneum as a consequence of splenic rupture. The subsequenthistopathological report of the spleen revealed amyloidosis. Thus, in patients with abdominal pain and hypotension, weshould suspect the possibility of a spontaneous splenic rupture, even without trauma or infection history.
Key words: Spontaneous splenic rupture. Amyloidosis. Splenectomy.
Department of Surgery, Surgical Oncology Research Centre,Mashhad University of Medical Sciences, Mashhad, Iran.
Correspondence: Dr. Mohammad Reza Motie, AssistantProfessor of Surgery, Surgical Oncology Research Centre,Imam Reza Hospital, Faculty of Medicine, Mashhad Universityof Medical Sciences, Mashhad, Iran.E-mail: [email protected]
Received: September 05, 2011; Accepted: August 17, 2012.

Orloff and Peskin in 1958 described true spontaneousrupture of the spleen. They considered four criteria whenmaking their decision. There should be no history oftrauma either prior to operation or retrospectively afteroperation. Secondly, there should be no evidence ofdisease that can affect the spleen. Thirdly, there shouldbe no evidence of perisplenic adhesions or scarring ofthe spleen, suggestive of trauma or previous rupture.The spleen should be normal on gross and histologicexamination apart from findings of hemorrhage andrupture.5 In 1991, Crate and Payne included a fifthcriterion. It was that full virological studies of acutephase and convalescent sera should show no significantrise in viral antibody titers suggesting recent viralinfection of types associated with splenic involvement.6
It is a rare surgical entity with very few cases reported inthe literature.6,7 Pathological splenic rupture is rare andoccurs in a diseased spleen. Spontaneous splenicrupture secondary to malaria infection is the mostcommon cause of pathological splenic rupture.1 Causesof pathological rupture are shown in Table I.1,5 Theactual reason for the rupture is not yet fully described.
The size of the spleen plays a significant role in rupture.However, rupture of the spleen has been reported innormal-sized organs. The patient we report also had anormal-sized spleen. The suggested mechanisms forspontaneous splenic rupture are as follows: (a) increasein intrasplenic pressure because of cellular hyperplasia,(b) compression of the spleen due to elevated intra-abdominal pressure during physiological activities suchas coughing, sneezing, defecating and vascularocclusion because of reticuloendothelial hyperplasialeading to thrombosis and infarct. This results ininterstitial and sub-capsular hemorrhage and stripping ofthe capsule, which causes further sub capsularhemorrhage.1
In this patient, splenic rupture was due to infiltration byamyloid tissue in the spleen. Systemic amyloidosis is agroup of diseases characterized by the extracellulardisposition of amyloid fibrillar protein in one or moreorgans. Renal or cardiac amyloid infiltration may evenlead to organ failure and death. Splenic infiltration isidentified in 41% of cases with systemic amyloidosis andsplenic rupture may occurr as a complication of amyloidinfiltration.8
Seventeen cases of splenic rupture in patients withsystemic amyloidosis have been reported since 1948upto 2003. Although this number does not define theactual incidence of spontaneous rupture of the spleen inamyloidosis, it suggests that splenic rupture is a rarecomplication in this disease.9
Hesam Shobeiri, Majid Einakchi, Mahtab Khajeh and Mohammad Reza Motie
428 Journal of the College of Physicians and Surgeons Pakistan 2013, Vol. 23 (6): 427-429
Figure 1: The pathological assessment of surgical specimen showingsplenic infiltration by amyloidosis.
Figure 2: The pathological assessment of surgical specimen showingsplenic infiltration by amyloidosis.
Table I: Causes of pathological rupture of the spleen.
Infections
•• Malaria
•• Infectious mononucleosis
•• Cytomegalovirus
•• Typhoid
•• HIV
•• Splenic candidiasis
•• Acute or chronic pancreatitis
Malignancies
•• Hematological malignancies
•• Hairy-cell leukemia
•• Lymphoma
•• Other leukemia
•• Rarely hepatocellular carcinoma, angiosarcoma, malignant histiocytosis
Metabolic disorders
•• Gaucher disease
Congenital anomalies
•• Splenic cyst and hamartomas
Other diseases
•• Amyloidosis
•• Systemic lupus erythematosus
•• Pregnancy
•• Rheumatic disease

Spontaneous splenic rupture (true or pathological),commonly presents as an abdominal emergency.Patients usually present in the emergency departmentwith sudden onset of pain in the left upper abdomen.Examination reveals hypotension, tachycardia, abdo-minal tenderness and guarding. The Kehr sign may ormay not be present. Hemogram usually reveals fallinghematocrit.5 Peritoneal signs may be absent during earlystages of acute hemoperitoneum, and the classic signsof splenic rupture may not be present. Therefore, in apatient with abdominal pain and hypotension, splenicrupture should be considered as a differential diagnosis.Imaging studies including ultrasound or CT scanning areuseful to confirm the diagnosis. Based on the findings ofthese studies according to the level of splenic injury, thedegree of splenic injury can be determined pre-operatively.1
Although the sensitivity of ultrasound for the detection offree intra-abdominal fluid is 98 – 100%, its sensitivity forthe detection of acute splenic parenchymal lesions is72 – 78%. The specificity of ultrasound for the detectionof splenic rupture is about 91 – 100%.2
There exists no consensus on the ideal treatment ofspontaneous splenic rupture. Splenectomy is atraditional treatment in hemodynamically unstablepatients but in hemodynamically stable patients withstable hemoglobin levels, successful non-operativetreatment has been reported. This is particularlyimportant in pediatric patients who are at increased riskfor postsplenectomy sepsis. Splenic angioembolizationis also increasingly being used.1 Some authorsrecommended surgical treatment in all cases that can bedifferentiated between idiopathic or secondary to ruptureto splenic pathology, in which delay in the treatmentcould change the course of the disease.1 The survival ofpatients following splenectomy is probably correlatedwith the course of the underlying disease.4
In conclusion, in patients with spontaneous splenicrupture, the decision to operate is primarily clinical, andtreatment should not be delayed pending imagingstudies because the consequences of late diagnosis andtreatment can be serious. Rapid diagnosis, aggressiveresuscitation, and surgical intervention can lead to asuccessful outcome in patients, especially in non-traumatic spontaneous spleen rupture.
REFERENCES1. Báez-García JD, Martínez-Hernández Magro P, Iriarte-Gallego
G, Báez-Aviña JA. Spontaneous rupture of the spleensecondary to amyloidosis. Cir Cir 2010; 78:538-42.
2. Görg C, Cölle J, Görg K, Prinz H, Zugmaier G. Spontaneousrupture of the spleen: ultrasound patterns, diagnosis and follow-up. Br J Radiol 2003; 76:704-11.
3. Toubia NT, Tawk MM, Potts RM, Kinasewitz GT. Cough andspontaneous rupture of a normal spleen. Chest 2005; 128:1884-6.
4. Gedik E, Girgin S, Aldemir M, Keles C, Tuncer MC, Aktas A.Non-traumatic splenic rupture: report of seven cases and reviewof the literature. World J Gastroenterol 2008; 14:6711-6.
5. Jeevan K, Akshay S. Asymptomatic spontaneous splenicrupture: a hair-raising experience in the operating room. InternetJ Surg 2009; 20:1.
6. Crate ID, Payne MJ. Is the diagnosis of spontaneous ruptureof a normal spleen valid. J R Army Med Corps 1991; 137:50-1.
7. Tu AS, Tran MHT, Larsen CR. Spontaneous splenic rupture:report of five cases and a review of the literature. Emerg Radiol1997; 4:415-8.
8. Powsner RA, Simms RW, Chudnovsky A, Lee VW, Skinner M.Scintigraphic functional hyposplenism in amyloidosis. J Nucl Med1998; 39:221-3.
9. Oran B, Wright DG, Seldin DC, McAneny D, Skinner M,Sanchorawala V. Spontaneous rupture of the spleen in ALamyloidosis. Am J Hematol 2003; 74:131-5.
Spontaneous rupture of the spleen secondary to amyloidosis
Journal of the College of Physicians and Surgeons Pakistan 2013, Vol. 23 (6): 427-429 429