

Spontaneous breathing during ARDS - Critical Care...
27
Spontaneous breathing efforts during ARDS ventilation Laurent Brochard
Transcript of Spontaneous breathing during ARDS - Critical Care...

Spontaneous breathing efforts during ARDS ventilation
Laurent Brochard

Conflicts of interest
• Our clinical research laboratory has received research grantsfor clinical research projects from the following companies: – Maquet (NAVA)
– Covidien (PAV+)
– Dräger (SmartCare)
– General Electric (FRC)
– Respironics (NIV)
– Fisher Paykel (Optiflow)

Acute Respiratory Distress Syndrome
TimingWithin 1 week of a known clinical insult or
new/worsening respiratory symptoms
Chest
Imaging aBilateral opacities – not fully explained by effusions,
lobar/lung collapse, or nodules
Origin of
Edema
Respiratory failure not fully explained by cardiac failure
or fluid overload;
Need objective assessment (e.g., echocardiography) to
exclude hydrostatic edema if no risk factor present
Mild Moderate Severe
Oxygenation b
200<PaO2/FiO2< 300
with
PEEP or CPAP ≥
5 cmH2Oc
100<PaO2/FiO2<200
with
PEEP ≥ 5 cmH2O
PaO2/FiO2<100
with
PEEP ≥ 5 cmH2O
aChest X-ray or CT ScanbIf altitude higher than 1000m,correction factor should be made as follows: PaO2/FiO2 x (barometric pressure/760)cThis may be delivered non-invasively in the Mild ARDS group

300 250 200 150 100 50
Low Tidal Volume Ventilation
Higher PEEP
HFO
Prone Positioning
ECMO
Low – Moderate PEEP
Neuromuscular Blockade
PaO2/FiO2
Increasing Severity of Lung Injury
Mild ARDS Moderate ARDS Severe ARDS
Incr
eas
ing
Inte
nsi
ty o
f In
terv
en
tio
n
NIV
ECCO2-R
Ferguson N et al ICM 2012

Why is spontaneous breathingdesirable?
• Preserve Respiratory Muscle Function (avoid VIDD)
• Improve VA/Q and Regional Ventilation
Levine S et al. N Engl J Med 2008;358:1327-1335

Papazian L. NEJM 2010
PNO 4% vs 12%

Modes of ventilation
• Controlled MV
• Assist Control?
• Bilevel Pressure Ventilation?
• Pressure Support ventilation?

Volume Assist-Control
Pes (cm H2O)
Paw (cm H2O)
Flow (L/sec)
Akouniamaki E et al CHEST in press

Presure Assist-Control
Paw (cm H2O)
Flow (L/sec)
EAdi (µV)
Akouniamaki E et al CHEST in press

Entrainment: reverse triggering
Akouniamaki E et al CHEST in press
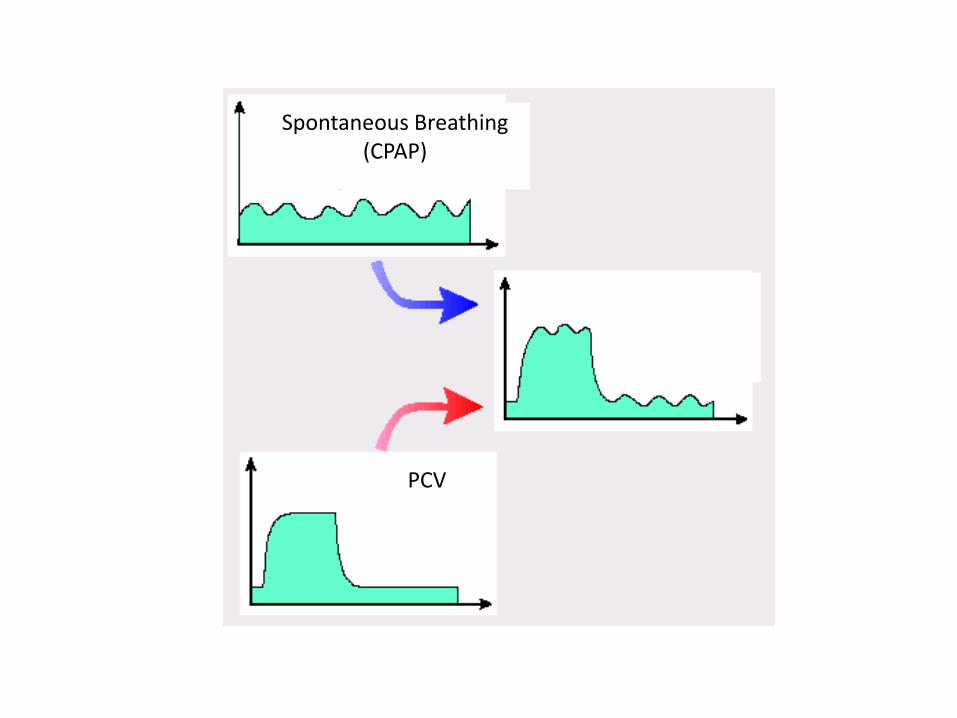
Spontaneous Breathing (CPAP)
PCV
Not BiPap!!


Assist-control VentilationVolume vs. Pressure-targeted modes: what’s the difference?
Volume-control: TransPulmonary Pressure
is controlled
Pressure-control: TransPulmonary Pressure
is NOT controlled


High and low Paw with APRV/BIPAP (white squares) and ACV (black circles). Daily ratio of PaO2 to FiO2 (grey columns cases and white columns controls)

Outcomes of patients included in the matched-case study
Gonzales ICM 2010

Pressure-Preset Modes
No i-synchronization
• APRV
Full i-synchronization
• BIPAPassist, , BiPAP PS AssistPressure controlled, etc.
Partial i-synchronization
• BIPAP, DuoPAP, BiVent,
• Bilevel, etc.
Akoumianaki E et al. ESICM 2012

VT change in the presence of spontaneous breaths according to i-synchronization
No spontaneous breaths
6ml/kg/IBW
VT
(ml)
Non i-Synchronized modesNon i-Synchronized modes
10 ml/kg/IBW
6 ml/kg/IBW
VT
(ml)
4 ml/kg/IBW
VT
(ml)
Fully i-Synchronized modes
6 ml/kg/IBW
10 ml/kg/IBW
time (sec)

METHODS: settings
Artificial lung settings
• CRrs: 30ml/cmH2O
• RRrs: 5 cmH2O/lt/min
• Pmus: -10 cmH2O
• RR: 20, 30 br/min
• Ti: 0.8 sec
Ventilator settings
• PAWinsp: 30 cmH2O
• PEEP : 15 cmH2O
• RR: 15/min
• I:E ratios: 1:3 and 3:1

0
10
20
30
40
50
60
0
200
400
600
800
1000
0 1 2 3 4 5Noi-Synchronization
Partiali- Synchronization
PS 0
Partiali- Synchronization
PS 15
Fulli-Synchronization
Co
effi
cie
nt
of
vari
atio
n (
%)
Tid
al v
olu
me
(m
l)
Coefficient of variationTidal volume
RESULTS: I:E 1/3, RR 20

0
10
20
30
40
50
60
0
200
400
600
800
RESULTS: I/E 3:1, RR 20
Co
effi
cie
nt
of
vari
atio
n (
%)
Tid
al v
olu
me
(m
l)
Noi-Synchronization
Partiali-Synchronization
PS 0
Partiali-Synchronization
PS 15
Fulli-Synchronization
Coefficient of variation
Tidal volume

Bench study: preliminary conclusions
In the presence of spontaneous breathing the same settingsacross different Pressure-Preset modes lead to differentvalues of VT, Ptp and breathing variability
As i-synchronization increases, VT and Ptp increase whilevariability decreases
These effects of i-synchronization are less pronounced athigher I:E ratio
Clinicians should be aware that i-synchronization may beharmful when high VT is undesirable (ARDS)

JAMA 2008

BIPAP APRV (EXPRESS) at H24:
• Target sedation based on (SB) as a %of total Vmn total• Delta Pressure for Vt ≤ 6 ml/kg

Patient DATA
Trends

The mode of ventilation allowing SB may depend
on the stage/severity of ARDS
• Early: controlled with NMBA, (no entrainment?)
• At 48h: non synchronous pressure targetedventilation (« APRV »)
• Later: synchronous pressure targeted ventilation (« Assist Pressure Control, Pressure Support Ventilation »)


















