Spinal cord disorders
25
SPINAL CORD DISORDRS ALI ABDULLAH ALBALUSHI OMSB EMERGENCY MEDICINE, R-4
Transcript of Spinal cord disorders

SPINAL CORD DISORDRS
ALI ABDULLAH ALBALUSHIOMSB
EMERGENCY MEDICINE, R-4

OUTLINE
• ANATOMY
• DIFFERENT SPINAL CORD DISORDERS
• CONCLUSION
• QUISTIONS

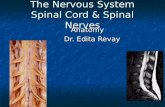
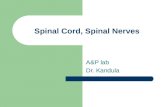
ANATOMY
Spinal cord: foramen magnum 1st/2nd lumbar vertebrae .
Cervical enlargement: C5-T1: gives rise to brachial plexus, innervates UE; L2-S3: gives rise to lumbosacral plexus,
Gray matter – central (cell bodies)White matter – peripheral (ascending and descending tracts)


1) All are true about the anatomy of the spinal cord except :
A. It is 40 cm long
B. Supplied by a single anterior spinal artery & paired vertibral artery
C. The posterior column carry the afferent ascending fibers for properiocetion &
vibration & cross at level of medulla
D. In the spinothalamic tract, sacral fibers are represented most medially
E. In corticospinal tract, the fibers cross at level of medulla & cervical fibers are
located medially

2) All are true regarding complete spinal cord syndrom except:
A. It is a total loss of sensory, autonomic & voluntary motor innervation distal to the
level of the spinal cord injury
B. Deep tendon reflexes my persist
C. The most common cause is trauma
D. 99% of patients with persistent symptoms beyond 24 hrs do not have a functional
recovery
E. 1% of patients will have some evident of cord function below the level of injury

3) All are true about spinal shock except :
A. It is the loss of muscle tone & reflexes with complete cord syndrom during
the acute phase of injury
B. The intensity of the spinal shock increases with the height of the level in the
spinal cord
C. It typically lasts less than 24 hrs
D. Bulbocavernous reflex is present
E. The termination of spinal shock phase of injury is heralded by return of
balbocavernous reflex

4) Central cord syndrom, all are true except :
A. It is the post prevalent of the partial cord syndroms
B. Upper extremities are affected more & distal muscles are affected to a greater
degree
C. The most common mechanism is motor vehicle crush
D. It is caused most often by hyperextension
E. Elderly are affected more & prognosis is better in patients younger than 50 yrs

5) All are true about Brown- Sequard Syndrom except:
A. Usually, it results from penetration injuries
B. Characterized by ipsilateral motor weakness & vibration / position loss &
contralateral pain/ tempreture loss
C. It can be associated with A-V malformation
D. Ipsilateral pain & tempreture loss may be noted 1 – 2 levels above the lesion
E. It has the worst prognosis of any incomplete spinal cord syndroms

6) Regarding anterior cord syndrom, all of the following are
true except :
A. Posterior column is preserved
B. Most cases reposted after aortic surgeries
C. It can be caused by hypotension
D. Generally, the prognosis is good

7) Regarding Conus Medullaris & Cauda Equina syndroms ,
What is false ?
A. It is very difficult to separate the two syndroms clinically
B. Conus Medullaris usually presents with overflow incontinence or sexual
dysfunction
C. Usually, Conus Medullaris presents unilaterally
D. Cauda Equina is a LMN picture with hyporeflexia
E. Saddle sensory loss is common in both syndroms

Sensory Motor Sphincter involvement
Central cord Variable Upper extremity weakness> lower extremity weakness, distal > proximal
Variable
Brown-Séquard syndromeBEST SCENARIO = BS = BEST OUTCOME
Ipsilateral position and vibration loss
Motor loss ipsilateral to cord lesion Variable
Contralateral pain and temperature loss
Anterior cord syndrome Loss of pin and touch Motor loss or weakness below level Variable
Vibration, position preserved
Transverse cord/complete Total loss of sensation (as well as autonomic fc) below level of cord injury
Total loss of voluntary motor function below cord level, DTRs absent/abnl/normal
Sphincter control lostAutonomic dysfc: may cause hypotension (neurogenic shock), priapism
Conus medullaris (terminal end of the spinal cord – L1) syndrome
Saddle anesthesia may be present or sens loss may range from patchy to complete transverse pattern
Weakness may be of upper motor neuron type, increased motor tone and reflexes
Sphincter control impaired – disturbance in urination/sexual dysfc
Cauda equina syndrome Saddle anesth may be present or sens loss may range from patchy to complete transverse.
Weakness may be of lower motor neuron type
Sphincter control impaired

8) All of the following result from intrinsic lesions in the spinal
cord except :
A. Multiple Sclerosis
B. Syrigomyelia
C. Myelopathy
D. Spinal epidural abscess
E. Spinal cord infarction

Nontraumatic Etiologies of Spinal Cord Dysfunction
Processes Affecting the Spinal Cord or Blood Supply Directly
Demyelination
Multiple sclerosis
Transverse myelitis
Spinal Arteriovenous Malformation/Subarachnoid Hemorrhage
Syringomyelia
Traumatic
Tumor
Idiopathic Spastic Paraparesis
HIV myelopathy
Other myelopathies
Spinal cord infarction Compressive Lesions Affecting the Spinal Cord
Spinal Epidural Hematoma
Spinal epidural abscess
Diskitis
Neoplasm
Metastatic
Primary CNS
HIV, human immunodeficiency virus; CNS, central nervous system.

9) All are true about MS except :
A. It is a demyelinating disease affecting CNS
B. Presents with patchy motor & sensory findings
C. Presents with UMN picture
D. Oligoclonal bands in CSF are significant only if present in the serum as well
E. Immunosuppresive therapy is the treatment of choice

10) All are true about Transverse Myelitis except :
A. Present with paraplegia , sensory level & sphincter disturbance
B. It is rare & progress slowly
C. Thoracic cord is affected most often & cervical rarely
D. The most essential aspect in management is to role out treatable causes
E. Steroids are of unknown benefit

11) All of the following are true about syringomyelia except ?
A. It is a condition of having a cavity lesion within the substance of the spinal cord
B. Disassociative anesthesia is the classic pattern of sensory deficit
C. CT is the diagnostic tool of choice
D. It is not necessary to perform an emergent imaging if f/u can be arranged
E. It is ass with Arnold – Chiari I Syndrom
It is treated with surgical removal If symptoms are progressive

12) Which statement is true about Spinal Epidural Hematoma ?
A. It is common with incidence of 5 per 100000 pts
B. It is not associated with anticoagulation therapy
C. Pain decreases by coughing or sneezing or straining
D. Patients usually present initialy with neurological deficit rather than pain
E. Emergent decompressive laminectomy is the treatment of choice

13) All statements are true about spinal epidural abscess Except :
A. It results from hematogenous spread of infection , mostly bacterial
B. Diabetics , IV drug users & HIV patients are at higher risk
C. Cervical site of infection predominate
D. Spread to subdural space & intraspinal area is uncommon
E. Urgent surgical consultation for decompression is required

• Urgent MRI must be done if diagnosis is suspected
•If MRI is not available, CT Myelogram should be done
• Neurological deficit rarely improve if surgical intervention is delayed more than 12
– 36 hrs after onset of paralysis
• Antibiotics : Vancomycin & Third generation Cephalosporine IV
Rifampin oral

14) All statements are true about Diskitis Except :
A. The most common causative organism is staph. Aurius
B. It is more common among pediatric age group, < 10 yrs
C. Lumbar spine is the most common site
D. Neurological deficit is common
E. Treated usually with antibiotics & surgery is often not necessary

15) All are true about spinal cord neoplasm Except :
A. Neurological symptoms caused by compression, invasion & distruction of the
myelinated tracts by the tumors
B. Metastasis is the most common spinal cord tumers
C. Lumbar region is the most affected
D. Recumbency worsen the pain
E. Severe nighttime pain is charactrestic


CONCLUSION

THANKS