Special Techniques Applicable to Bone Marrow … marrow...bone marrow trephine biopsies are stained...
39
niques that may be applied to trephine biopsy sections include: (i) a wider range of cytochemical stains; (ii) immunohistochemistry; (iii) cytogenetic and molecular genetic analysis; and (iv) ultrastruc- tural examination. Cytochemical and histochemical stains Cytochemical stains on bone marrow aspirates Perls’ stain for iron A Perls’ or Prussian blue stain (Figs 2.1 and 2.2) demonstrates haemosiderin in bone marrow macro- phages and within erythroblasts. Consequently, it allows assessment of both the amount of iron in reticulo-endothelial stores and the availability of iron to developing erythroblasts. Assessment of storage iron requires that an ade- quate number of fragments are obtained. A bone marrow film or squash will contain both intracellu- lar and extracellular iron, the latter being derived from crushed macrophages. It is usual to base assessment of iron stores mainly on intracellular iron since iron stains are prone to artefactual deposits and it can be difficult to distinguish between extra- cellular iron and artefact. Iron stores may be assessed as normal, decreased or increased, or may be graded as 1+ to 6 + as shown in Table 2.1, grades of 1+ to 3 + being considered normal. Alternatively, iron stores may be graded as 1+ to 4 + [3,4]. Examination of a Perls’ stain of a bone marrow film allows adequate assessment of erythroblast iron as long as a thinly spread area of the film is examined with optimal illumination. A proportion of normal erythroblasts have a few (one to five) fine iron-containing granules randomly distributed in TWO SPECIAL TECHNIQUES APPLICABLE TO BONE MARROW DIAGNOSIS Peripheral blood samples, bone marrow aspirates and trephine biopsy specimens are suitable for many diagnostic investigations, in addition to routine microscopy of Romanowsky-stained blood and bone marrow films and haematoxylin and eosin-stained histological sections. Some of these techniques, for example Perls’ stain to demonstrate haemosiderin in a bone marrow aspirate, are so often useful that they are performed routinely, whereas other tech- niques are applied selectively. This chapter will deal predominantly with special techniques that are applicable to bone marrow aspirates and trephine biopsy sections but reference will be made to the peripheral blood where this is the more appropriate tissue for study. Bone marrow aspirate films are stained routinely with a Romanowsky stain such as a May– Grünwald–Giemsa (MGG) or a Wright–Giemsa stain. Other diagnostic procedures that may be of use in individual cases include: (i) cytochemistry; (ii) immunophenotyping (by immunocytochemistry or flow cytometry); (iii) cytogenetic and molecular genetic analysis; (iv) ultrastructural examination; (v) culture for micro-organisms; and (vi) culture for assessment of haemopoietic progenitor cells. In most countries, histological sections cut from bone marrow trephine biopsies are stained rou- tinely with H&E. Most laboratories also use silver stains routinely to demonstrate reticulin and some employ, in addition, a Giemsa stain, a Perls’ stain or both. We recommend the routine use of H&E, Giemsa and reticulin stains. Giemsa staining per- mits the easy identification of mast cells, facilitates recognition of plasma cells and helps in making a distinction between early erythroid cells and myeloblasts. If a Giemsa stain is not performed routinely, then it is important that it is used when- ever necessary for these indications. Other tech- 51
Transcript of Special Techniques Applicable to Bone Marrow … marrow...bone marrow trephine biopsies are stained...

niques that may be applied to trephine biopsy sections include: (i) a wider range of cytochemicalstains; (ii) immunohistochemistry; (iii) cytogeneticand molecular genetic analysis; and (iv) ultrastruc-tural examination.
Cytochemical and histochemical stains
Cytochemical stains on bone marrowaspirates
Perls’ stain for iron
A Perls’ or Prussian blue stain (Figs 2.1 and 2.2)demonstrates haemosiderin in bone marrow macro-phages and within erythroblasts. Consequently, itallows assessment of both the amount of iron inreticulo-endothelial stores and the availability ofiron to developing erythroblasts.
Assessment of storage iron requires that an ade-quate number of fragments are obtained. A bonemarrow film or squash will contain both intracellu-lar and extracellular iron, the latter being derivedfrom crushed macrophages. It is usual to baseassessment of iron stores mainly on intracellular ironsince iron stains are prone to artefactual depositsand it can be difficult to distinguish between extra-cellular iron and artefact. Iron stores may beassessed as normal, decreased or increased, or maybe graded as 1+ to 6+ as shown in Table 2.1, gradesof 1+ to 3+ being considered normal. Alternatively,iron stores may be graded as 1+ to 4+ [3,4].
Examination of a Perls’ stain of a bone marrowfilm allows adequate assessment of erythroblastiron as long as a thinly spread area of the film isexamined with optimal illumination. A proportionof normal erythroblasts have a few (one to five) fineiron-containing granules randomly distributed in
TWO
SPECIAL TECHNIQUES APPLICABLETO BONE MARROW DIAGNOSIS
Peripheral blood samples, bone marrow aspirates andtrephine biopsy specimens are suitable for manydiagnostic investigations, in addition to routinemicroscopy of Romanowsky-stained blood and bonemarrow films and haematoxylin and eosin-stainedhistological sections. Some of these techniques, forexample Perls’ stain to demonstrate haemosiderinin a bone marrow aspirate, are so often useful thatthey are performed routinely, whereas other tech-niques are applied selectively. This chapter will dealpredominantly with special techniques that areapplicable to bone marrow aspirates and trephinebiopsy sections but reference will be made to theperipheral blood where this is the more appropriatetissue for study.
Bone marrow aspirate films are stained routinelywith a Romanowsky stain such as a May–Grünwald–Giemsa (MGG) or a Wright–Giemsa stain.Other diagnostic procedures that may be of use in individual cases include: (i) cytochemistry; (ii)immunophenotyping (by immunocytochemistry orflow cytometry); (iii) cytogenetic and moleculargenetic analysis; (iv) ultrastructural examination;(v) culture for micro-organisms; and (vi) culture forassessment of haemopoietic progenitor cells.
In most countries, histological sections cut frombone marrow trephine biopsies are stained rou-tinely with H&E. Most laboratories also use silverstains routinely to demonstrate reticulin and someemploy, in addition, a Giemsa stain, a Perls’ stain or both. We recommend the routine use of H&E,Giemsa and reticulin stains. Giemsa staining per-mits the easy identification of mast cells, facilitatesrecognition of plasma cells and helps in making a distinction between early erythroid cells andmyeloblasts. If a Giemsa stain is not performed routinely, then it is important that it is used when-ever necessary for these indications. Other tech-
51

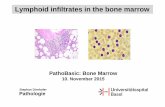
the cytoplasm (Fig. 2.3). Such erythroblasts are de-signated sideroblasts. In haematologically normalsubjects with adequate iron stores, 20–50% of bone marrow erythroblasts are sideroblasts [5–7].Examination of an iron stain allows detection notonly of an increased or decreased proportion ofsideroblasts but also of abnormal sideroblasts. Thelatter include those in which siderotic granules are merely increased in size and number and thosein which granules are also distributed abnormallywithin the cytoplasm, being sited in a ring aroundthe nucleus rather than randomly (ring sideroblasts).
52 CHAPTER TWO
Fig. 2.1 Aspirate of normal BM:bluish-black iron in macrophages in a fragment. Perls’ stain ×377.
Fig. 2.2 Aspirate of normal BM: a fragment with no stainable iron.Perls’ stain ×377.
Table 2.1 Grading of bone marrow storage iron [1,2].
0 No stainable iron1+ Small iron particles just visible in reticulum cells
using an oil objective2+ Small, sparse iron particles in reticulum cells,
visible at lower power3+ Numerous small particles in reticulum cells4+ Larger particles with a tendency to aggregate
into clumps5+ Dense, large clumps6+ Very large clumps and extracellular iron

SPECIAL TECHNIQUES 53
In certain pathological conditions, plasma cellscontain haemosiderin inclusions which are irregularin shape and relatively large. On an MGG stain theyare greenish-black (Fig. 2.4a). Their nature is con-firmed by a Perls’ stain (Fig. 2.4b). Haemosiderininclusions in plasma cells are observed mainly iniron overload (for example in haemochromatosisand transfusional siderosis) and in chronic alco-holism [8].
Problems and pitfalls
Since iron is distributed irregularly within bonemarrow macrophages, it is necessary to assess anumber of fragments before concluding that storageiron is absent or reduced. If necessary, a Perls’ staincan be performed on more than one bone marrowfilm. Stain deposit on the slide must be distin-guished from haemosiderin. Careful examinationwill show that it is not related to cells and is often inanother plane of focus.
Other cytochemical stains
Cytochemical stains are employed mainly in theinvestigation of acute leukaemia and the myelodys-plastic syndromes (MDS). In acute leukaemia theremay be numerous blast cells in the peripheral blood and it is then useful to perform cytochemicalstains on blood and bone marrow in parallel. Cyto-chemical investigation of suspected MDS should be
performed on bone marrow films since there areusually only small numbers of immature cells in theperipheral blood.
The techniques recommended for diagnosis andclassification of acute leukaemia are either myelo-peroxidase or Sudan black B staining, to identifycells showing granulocytic differentiation, plus anon-specific esterase or combined esterase stain, to identify cells showing monocytic differentiation.Enzyme cytochemistry for either α-naphthyl butyrateesterase or α-naphthyl acetate esterase is suitable asa ‘non-specific’ esterase staining method for the iden-tification of monocytic differentiation. In a combinedesterase stain either of these methods is combinedwith demonstration of naphthol AS-D chloro-acetate esterase (chloro-acetate esterase), the latterto show granulocytic differentiation. The applica-tion of these stains will be discussed in Chapter 4.
Other cytochemical stains which are occasionallyused include toluidine blue to demonstrate themetachromatic granules in basophils and mast cellsand staining of cells of mast cell lineage for ε-aminocaproate. When immunophenotyping is avail-able, periodic acid–Schiff (PAS) and acid phosphatasestains are redundant in the investigation of acuteleukaemias, although differences can be observedbetween different types of acute lymphoblasticleukaemia (ALL) and acute myeloid leukaemia(AML) [9,10]. Either a Sudan black B or a myelo-peroxidase stain should also be used in cases of suspected MDS to facilitate detection of Auer rods.
Fig. 2.3 BM aspirate from ahealthy volunteer showing anormal sideroblast. Perls’ stain×960.

Cytochemistry now has little place in the inves-tigation of lymphoproliferative disorders. However,the demonstration of tartrate-resistant acid phos-phatase activity is still of value in the diagnosis ofhairy cell leukaemia, particularly when a largepanel of appropriate immunophenotyping reagentsis not available.
Histochemical stains on trephine biopsysections
Perls’ stain for haemosiderin
Because of the irregular distribution of iron withinbone marrow macrophages, a biopsy may show the
presence of iron when none has been detected in an aspirate. Haemosiderin can often be detected,particularly when it is increased, as golden brownrefractile pigment in an unstained or H&E-stained section (Fig. 2.5). In a Giemsa-stained section it is greenish-blue (Fig. 2.6). An iron stain (Fig. 2.7)can be successfully carried out using either plastic-embedded or paraffin-embedded biopsy specimens.However, plastic-embedded specimens give more reli-able results. Decalcification of a paraffin-embeddedspecimen, whether by acid decalcification or bychelation, leads to some leaching out of iron.Plastic-embedded samples are also superior for thedetection of ring sideroblasts or other abnormalsideroblasts. These can sometimes also be detected
54 CHAPTER TWO
Fig. 2.4 BM aspirate from a patientwith chronic alcoholism showinghaemosiderin in plasma cells. (a) MGG ×960. (b) Perls’ stain ×960.(b)
(a)

Fig. 2.5 Section of BM showinghaemosiderin within macrophagesin an HIV-positive patient with iron overload. Paraffin-embedded,H&E ×376.
Fig. 2.6 Section of BM trephinebiopsy specimen showinghaemosiderin in stromalmacrophages demonstrated byGiemsa staining. A distinctiveyellow–green colour is obtainedthat is easily visible againstbackground haemopoietic cellstaining. Paraffin-embedded,Giemsa ×940.
Fig. 2.7 Section of normal BM:macrophage containing iron.Plastic-embedded, Perls’ stain ×940.
SPECIAL TECHNIQUES 55

in paraffin-embedded bone marrow fragments but not in decalcified trephine biopsy sections.However, no technique for processing and stainingof a biopsy specimen allows assessment of whethersiderotic granules are normal or decreased; thisrequires an iron stain of an aspirate. Haemosiderindeposits in plasma cells may, however, be suf-ficiently large that they can be detected on sectionsof paraffin-embedded trephine biopsy specimens(Fig. 2.8).
Practice differs between laboratories as to wheth-er a Perls’ stain for haemosiderin is performed routinely. If a bone marrow aspirate containingadequate fragments is available, then iron stainingof trephine biopsy sections is redundant. However,it may well be more efficient for organizational rea-sons to perform an iron stain routinely rather thanto perform it selectively only in those cases where itis likely to give information of specific diagnosticuse.
Problems and pitfalls
The amount of iron that is leached out when aparaffin-embedded biopsy specimen is decalcified is variable and unpredictable. The amount of stain-able iron is reduced and sometimes all stainable iron is removed. Loss of stainable iron is less with ethylene diamine tetra-acetic acid (EDTA)decalcification than with other methods. Because of the unpredictable leaching out of iron it is not
possible to quantify iron accurately on a decalcifiedbiopsy specimen. It is only possible to say that iron is present or increased but not that it is decreased or absent.
There are conflicting reports of the comparabilityof iron stains performed on aspirates and biopsyspecimens, not all of which are readily explicable by the factors already mentioned. Lundin et al. [3]found that in 8% of cases iron was detectable in a biopsy specimen and not in an aspirate and inanother 8% the reverse was true; by assessing otherfactors they were not able to establish that one orother method was more valid. Fong et al. [4] foundthat in 8% of patients iron was present in an aspirate but was not detectable in a biopsy sample;however, this was not due to the process ofdecalcification since it was noted with regard to sections of marrow fragments as well as for trephinebiopsy sections. Conflicting findings were reportedby Krause et al. [11] who found that iron wasalways detectable in a biopsy when it was present inan aspirate, but two thirds of patients with absentiron in an aspirate had detectable iron on a biopsyspecimen. It is clear that minor variations in tech-nique may be critical. Our own observations arethat when specimens are decalcified using manualprocessing techniques there may be a failure todetect iron in a trephine biopsy specimen when it isclearly present in an aspirate. Iron stains performedon aspirates and biopsies should clearly be regardedas complementary.
56 CHAPTER TWO
Fig. 2.8 Section of trephine biopsyspecimen from a child with ironoverload associated with congenitalsideroblastic anaemia showing anumber of plasma cells containinglarge haemosiderin deposits.Paraffin-embedded, Perls’ stain ×960.

SPECIAL TECHNIQUES 57
Reticulin and collagen stains
Histological sections, either from particle prepara-tions or trephine biopsy specimens, can be stainedfor reticulin using a silver-impregnation techniqueand also for collagen using a trichrome stain. Wehave found a Martius Scarlet Blue stain superior toa van Gieson stain for the identification of collagen.Reticulin and collagen deposition can be quant-ified as shown in Table 2.2 [12] and illustrated inFigs 2.9–2.13. The majority of haematologicallynormal subjects have a reticulin grade of 0 or 1 butoccasional subjects have a grade of 2. There is a
Fig. 2.9 Section of normal BM:reticulin grade 0, showing nostainable fibres. Plastic-embedded,Gomori’s reticulin stain ×188.
Fig. 2.10 Section of normal BM:reticulin grade 1, showing scatteredfine fibres. Plastic-embedded,Gomori’s reticulin stain ×188.
Table 2.2 Quantification of bone marrow reticulin andcollagen [12].
0 No reticulin fibres demonstrable1 Occasional fine individual fibres and foci of a fine
fibre network2 Fine fibre network throughout most of the
section; no coarse fibres3 Diffuse fibre network with scattered thick coarse
fibres but no mature collagen4 Diffuse often coarse fibre network with areas of
collagenization

Fig. 2.11 Section of normal BM:reticulin grade 2, showing a finefibre network but no coarse fibres.Paraffin-embedded, Gomori’sreticulin stain ×195.
Fig. 2.12 Section of abnormal BM:reticulin grade 3, showing thickcoarse fibres. Paraffin-embedded,Gordon and Sweet stain ×188.
Fig. 2.13 Section of abnormal BM:reticulin grade 4, showing a coarsefibre network; collagen waspresent. Paraffin-embedded,Gordon and Sweet stain ×188.
58 CHAPTER TWO

SPECIAL TECHNIQUES 59
tendency for more reticulin to be detected in iliaccrest biopsies than in sections of particles aspiratedfrom the sternum. Reticulin is concentrated aroundblood vessels and close to bone trabeculae and theseareas should be disregarded in grading reticulindeposition.
The term myelofibrosis is used to indicate deposi-tion of collagen in the marrow and sometimes alsoto indicate increased reticulin deposition. To avoidany ambiguity it is preferable to either grade retic-ulin/collagen deposition as shown in Table 2.2 or touse the term ‘reticulin fibrosis’ for grade 3 fibrosisand ‘myelofibrosis’ for grade 4. The term myeloscle-rosis has also been used in various senses; it is bestregarded as a synonym for myelofibrosis.
A reticulin stain should be performed on everytrephine biopsy specimen. It has two major roles.Firstly, increased reticulin deposition provides non-specific evidence of an abnormality of the bonemarrow. Secondly, focal abnormality in the patternof reticulin deposition can be very useful in detect-ing abnormalities that might be overlooked in an H&E-stained section. Abnormal infiltrates mayshow an associated increase in reticulin depositionor, less often, there may be a general increase inreticulin deposition but with an absence of reticulinin an area that is heavily infiltrated by non-haemopoietic cells. Focal abnormalities that may be highlighted by a localized increase in reticulin
deposition include granulomas and infiltrates ofcarcinoma or lymphoma cells.
Problems and pitfalls
To avoid confusion, pathologists should refer to re-ticulin and collagen deposition in a precise manner.Increased reticulin deposition provides evidence of a bone marrow abnormality but should not beover-interpreted since the causes are multiple. Thecauses of collagen deposition are fewer and thisabnormality is therefore of more diagnostic sig-nificance. The significance of reticulin and collagendeposition is discussed in Chapter 3 (see page 130).
Other histochemical stains
Other potentially useful histochemical stains andtheir roles in diagnosis are shown in Table 2.3. Achloro-acetate esterase (Leder) stain is illustrated in Fig. 2.14.
Problems and pitfalls
The reactivity of histochemical stains is influencedby the choice of fixative, the method of embed-ding and the process of decalcification employed.Fixation in either Bouin’s or Zenker’s solution leadsto reduced metachromatic staining of mast cells
Table 2.3 Cytochemical and histochemical stains and their indications.
Cytochemical stain Role
Chloro-acetate esterase (Leder) Identification of granulocytic differentiation and mast cells
Periodic acid–Schiff (PAS)* Staining of complex carbohydrates: identification of plasma cells and megakaryocytes (staining is variable); identification of some tumour cells; identification of fungi
Toluidine blue Identification of mast cells
Alcian blue Identification of cryptococci and some tumour cells; staining of stromal mucins
Grocott’s methenamine silver stain (GMS) Identification of fungi
Congo red stain Identification of amyloid
Ziehl–Neelsen stain (ZN) Identification of mycobacteria
Martius Scarlet Blue (MSB) Staining of collagen and fibrin/fibrinoid
* Neutrophils are also PAS-positive.

with a Giemsa stain and also reduces or abolisheschloro-acetate esterase activity. Other histochem-ical stains are satisfactory with fixation in formalinor Bouin’s or Zenker’s solution. However, it shouldbe noted that prolonged storage of formalin at highambient temperatures can lead to formic acid pro-duction; if the formalin is unbuffered, inadvertentdecalcification may occur during the process offixation with resultant adverse effects on staining.Histochemical stains are satisfactory with bothparaffin- and plastic-embedding. Acid decalcificationimpairs chloro-acetate esterase activity whereasEDTA decalcification does not. Over-exposure toEDTA reduces or abolishes Giemsa staining.
We have found that many of the proprietarycombined fixation–decalcification solutions, whichare sometimes used to achieve rapid processing,impair histochemical stains. For example, haema-toxylin staining may be impaired so that nucleardetail and cytoplasmic basophilia are not apparent.Giemsa staining may be severely impaired.
Immunophenotyping
Antigens may be expressed on the surface of cells,within the cytoplasm or within the nucleus. De-pending on the techniques applied for immunophe-notyping, there may be detection of only surfacemembrane antigens or cytoplasmic and nuclearantigens may also be detected. Detection of antigensmay be by means of polyclonal antibodies, raised
in animals such as rabbits, but increasing use isbeing made of monoclonal antibodies produced byhybridoma technology. Many monoclonal antibod-ies, reactive with lymphoid or myeloid antigens,have been characterized at a series of internationalworkshops and are described by cluster of differen-tiation (CD) numbers. A CD number refers to agroup of antibodies that recognize the same antigenand also refers to the antigen expressed. It is im-portant to note that monoclonal antibodies mayrecognize specific epitopes on antigens so that notall antibodies with the same CD number haveexactly the same reactivity with normal and abnor-mal cells. A complete list of CD numbers is given inreference 13. Some important monoclonal antibod-ies have not yet been assigned a CD number, e.g.FMC7 and DBA44.
Immunophenotyping byimmunofluorescence flow cytometry
If there are significant numbers of circulatingabnormal cells, it is most convenient to performflow cytometric immunophenotyping on a periph-eral blood sample. Otherwise this procedure can beperformed on a bone marrow aspirate or, alternat-ively, on a serous exudate, cerebrospinal fluid or a suspension of cells from a lymph node or other tissue. When peripheral blood is used, the procedurecan be applied to either a mononuclear cell prepara-tion or to whole blood in which the red cells have
60 CHAPTER TWO
Fig. 2.14 Section of trephinebiopsy specimen from a patientwith large granular lymphocyteleukaemia stained for chloro-acetate esterase. Myeloidprecursors are positive andlymphocytes are negative. Plastic-embedded, Leder’s stain ×940.

SPECIAL TECHNIQUES 61
been lysed [14]. The latter technique minimizes cellloss and potential artefacts that can be induced byexposure to Ficoll and density gradient separation.It also increases the speed and convenience of theprocedure. Choice of appropriate proprietary lysissolutions is important to avoid reduction of expres-sion of certain antigens [15].
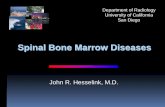
The principle of flow cytometry is that cells bear-ing specific antigens are identified by means of amonoclonal antibody (or, occasionally, a polyclonalantiserum) labelled with a fluorochrome (Fig. 2.15).The flow cytometer permits classification of cellsaccording to their light-scattering characteristicsand the intensity of their fluorescence upon activa-tion by laser light, detected after passing through anappropriate filter for the particular fluorochromeemployed. Three or more fluorochromes can beused so that the simultaneous expression of two,three or more antigens can be studied. If permeabil-ization techniques are employed, cytoplasmic andnuclear antigens can be detected as well as thoseexpressed on cell surfaces. Techniques are also avail-able for the quantification of antigen expression.
Flow cytometry immunophenotyping is appli-cable to diagnosis and classification of haematolo-gical neoplasms. When expression of three or fourantigens is assessed simultaneously it is also applica-ble to the detection of minimal residual disease.
Problems and pitfalls
Flow cytometry has the disadvantage that im-munophenotype cannot be related directly to cytol-ogy. Results must always be interpreted in the lightof the cytological features of the cells being studied.
When there are large numbers of circulating neoplastic cells, results of peripheral blood analysisare generally reliable. However, a low frequency ofabnormal cells may not be detected. When flowcytometry is performed on cell suspensions frombone marrow or other tissues, results may be mis-leading in two circumstances. Firstly, an abnormalinfiltrate may not be represented in the aspirate toany significant extent. This is often the case in follic-ular lymphoma with paratrabecular infiltration butmay also occur in any lymphoma in which reticulindeposition is increased in the infiltrated area, inter-fering with aspiration of abnormal cells. Secondly, if neoplastic cells are outnumbered by reactive cells, as in Hodgkin’s disease and in T-cell-rich B-cell lymphoma, the immunophenotyping mayrelate only to reactive T lymphocytes, not to theminor population of neoplastic cells. In both of thesecircumstances immunohistochemistry is superior.In addition, correct techniques are of critical impor-tance. For example, if gating techniques (see below)are used in order to determine the immunopheno-
CON
CO
N10
410
310
210
110
0
104103102101100
CD4
CD
810
410
310
210
110
0
104103102101100
CD3
CD
710
410
310
210
110
0
104103102101100
TCR a/b
TCR
g/d
104
103
102
101
100
104103102101100
Fig. 2.15 Scatter plot showing flowcytometry immunophenotyping ina case of T-lineage prolymphocyticleukaemia. The leukaemic cells arepositive for CD4, CD7 and TCRαβ;they are negative for CD8. (Bycourtesy of Mr R Morilla, London.)

type of a subpopulation of cells, it is essential to ensurethat the gated cells are the neoplastic population.
Caution is required in interpreting flow cytome-try findings during post-treatment follow-up ofALL. Normal immature lymphoid cells, known ashaematogones, express CD10, CD34 and terminaldeoxynucleotidyl transferase (TdT) and can thus beconfused with residual leukaemic cells [16] unlessthe strength of expression of antigens is also con-sidered. The detection of persisting cells with anaberrant combination of antigens is more reliable,as is polymerase chain reaction (PCR) analysis forrearranged immunoglobulin heavy chain (IGH) orT-cell receptor (TCR) genes (see below).
Immunocytochemistry
By convention, the term immunocytochemistryrefers to the study of the antigen expression of cellsby means of polyclonal or monoclonal antibodiesapplied to fixed cells on glass slides. The materialinvestigated may be either a blood or bone marrowfilm or a cytocentrifuged preparation of washedmononuclear cells isolated from blood or bone mar-row. The reaction of antibodies with cells carrying a specific antigen is detected by either: (i) directlabelling of the primary antibody with an enzymesuch as peroxidase or alkaline phosphatase; or (ii)an indirect method using a second, labelled anti-body that recognizes the first (e.g. a secondary antibody reactive with mouse immunoglobulinswhen the primary antibody is murine). A variety ofindirect methods are available. Indirect labellingtechniques offer the advantage of increased sensi-tivity but are more time-consuming to perform thandirect labelling.
The use of washed, separated cells in cytocentrifugepreparations is necessary for immunocytochemistryto detect surface membrane immunoglobulins,including κ and λ light chains. Plasma immunoglob-ulins interfere with the staining if blood films orfilms of bone marrow aspirates are used. For detec-tion of most other antigens, either cytocentrifugepreparations or wedge-spread films are satisfactory.If there are significant numbers of abnormal cells in the circulating blood, then a peripheral bloodsample is very satisfactory for immunocytochem-istry. Otherwise study of a bone marrow aspirate isnecessary.
Immunocytochemistry can also be used to dem-onstrate the product of an oncogene or a cancer-suppressing gene. For example, PML protein, theproduct of the gene that is rearranged and dysregu-lated in acute promyelocytic leukaemia, can be dem-onstrated with a fluorochrome-labelled monoclonalantibody and an abnormal pattern of distributioncan be shown in this type of leukaemia. Similarly, a labelled antibody can be used to demonstrateincreased expression of p53 protein when the geneis dysregulated; p53 protein is below the level ofdetection when only the wild type gene is present.
Problems and pitfalls
Immunocytochemistry has the advantage that reactivity with an antibody can be related to cellmorphology. However, it should be noted that cyto-centrifugation introduces artefactual changes, suchas nuclear lobulation. It is useful to examine anMGG-stained cytocentrifuge preparation in parallelwith the immunocytochemical stains and wedge-spread films.
Cytochemistry is slow and labour intensive andthus is not suitable for large workloads or for pro-ducing rapid results. Interpretation is subjectiveand, because only a small number of cells can beassessed, results are imprecise. Some useful anti-bodies, for example FMC7, cannot be used success-fully for immunocytochemistry although they arevery reliable with flow cytometry.
Relative advantages of flow cytometry andimmunocytochemistry
Flow cytometry has various advantages over im-munocytochemistry and is therefore the preferredtechnique where it is available as:1 it is rapid and less labour intensive;2 it permits large numbers of cells to be analysed sothat the percentage of cells bearing a specific anti-gen is estimated much more precisely and minorpopulations of cells may be identified;3 multiple directly labelled antibodies can be usedto study the co-expression of two, three or evenfour antigens;4 it is possible to ‘gate’ for cells having particularcharacteristics in order to investigate antigen expres-sion by a defined population (‘gating’ or selection of
62 CHAPTER TWO

SPECIAL TECHNIQUES 63
a subpopulation may be based on light-scatteringcharacteristics of cells or on expression of a specificantigen); and 5 the amount of antigen expressed on a specificpopulation of cells can be quantified, whereas im-munocytochemistry is not quantitative.
These advantages of flow cytometry mean that itcan be used to identify minor normal populations,such as CD34-positive haemopoietic stem cells, andminor abnormal populations showing atypical com-binations of antigen expression, as in the detectionof minimal residual disease in patients treated forhaematological neoplasms.
There are two important disadvantages of flow cyto-metry in comparison with immunocytochemistry:1 without modification, the technique detects onlysurface membrane antigens and not antigens ex-pressed within the cytoplasm or in the nucleus; and 2 cytological features of the cells studied cannot beappreciated.
The first disadvantage can be overcome readily bythe use of techniques for permeabilizing cells so thatantigens expressed in the nucleus or in the cyto-plasm can be detected. The second defect cannot beovercome easily but use of light-scattering charac-teristics of cells does at least permit a determinationof whether specific antigens are expressed on large or
small cells. Results of flow cytometry should not beinterpreted in isolation; the cytological features ofthe cells being studied must be taken into account.
Immunocytochemistry has the advantage overflow cytometry that the precise cytological featuresof cells bearing a certain antigen can be recognized.As mentioned above, however, it is very labourintensive and more time-consuming than flowcytometry and results are not quantitative. Doubleor multiple antigen combinations on individualcells cannot be demonstrated routinely. Althoughtechniques exist for sequential immunocytochem-ical staining of several antigens in the same prepara-tion, these are largely restricted to use as researchtools at present because of their practical difficulties.
Antibodies for flow cytometry andimmunocytochemistry
Antibodies to be used in flow cytometry are selecteddepending upon the purpose of the investigation.There are relatively few circumstances in which asingle antibody is used in isolation. Specific combi-nations are used for investigation of suspected acuteleukaemia or possible lymphoproliferative disor-ders. Suggested panels are provided in Tables 2.4and 2.5.
Table 2.4 Monoclonal and other antibodies useful in immunocytochemistry and flow cytometry immunophenotypingin suspected acute leukaemia.
Primary panel
For detection of myeloid differentiation CD117, CD13*, CD33, anti-MPO, CD65
For detection of B-lymphoid differentiation CD19, CD22*, CD79a
For detection of T-lymphoid differentiation CD2, CD3*, anti-TCRαβ, anti-TCRγδ
For detection of immature cells Anti-TdT (anti-terminal deoxynucleotidyl transferase), CD34, HLA-DR
Secondary panel
For further investigation of myeloid Anti-glycophorin for erythroid differentiation, CD41 (or CD61) for differentiation megakaryocyte differentiation, CD14 for monocytic differentiation,
CD11b for granulocytic or monocytic maturation
For further investigation of B-lineage CD10, cytoplasmic immunoglobulin, surface membrane differentiation immunoglobulin
For further investigation of T-lineage CD1a, CD4, CD5, CD8differentiation
* Testing is more sensitive if cytoplasmic rather than surface membrane antigen is tested for, either by ‘permeabilizing’cells or by using immunocytochemistry rather than flow cytometry.

In addition, flow cytometry can be used for:1 quantification of CD34-positive haemopoietic stemcells for stem cell harvesting and transplantation;2 quantification of CD4-positive lymphocytes forassessment of immune status in HIV infection; and3 quantification of DNA for cell cycle and ploidystudies; e.g. for detection of hyperdiploidy in ALL.
Problems and pitfalls
Because many immunophenotypic markers are notlineage-specific it is always necessary to use a panelof antibodies rather than relying on reactivity with a single antibody. Immunophenotypic markersshowing good lineage specificity include CD79a and CD79b for the B lineage, CD3 for the T lineageand myeloperoxidase for myeloid cells. However, itshould be noted that cross-reactivity of CD79a withsome cases of T-lineage ALL has been reported [17].
Immunophenotypic markers with poor lineagespecificity include TdT, HLA-DR, CD7 and CD10.
Immunohistochemistry
Immunohistochemistry refers to the demonstrationof antigens in histological tissue sections. It hasadvantages and disadvantages in relation to flowcytometry and immunocytochemistry. For prac-tical purposes, flow cytometry and immunohisto-chemistry should be regarded as complementaryinvestigations.
In flow cytometry, a wider range of antibodiescan be used and quantification of antigen expres-sion can be achieved. There is also less likelihood of non-specific staining in flow cytometry than inimmunohistochemistry. However, immunohisto-chemistry has the advantage that immunopheno-typic information can be obtained and assessed in
64 CHAPTER TWO
Table 2.5 Monoclonal and other antibodies useful in immunophenotyping suspected chronic lymphoproliferativedisorders.
Primary panel
To establish lineage A pan-B marker such as CD79a, CD19 or CD24 and a pan-T marker such as CD2 or CD3
To establish clonality of B-lineage Anti-κ and anti-λlymphoproliferative disorders and to establish the strength of expressionof surface membrane immunoglobulin
To distinguish B-lineage chronic CD79b (or CD22), CD5, CD23 and FMC7 (CLL cells are usually CD5 and lymphocytic leukaemia from other CD23 positive, CD22, CD79b and FMC7 weak or negative and show weak less common B- and T-lineage disorders expression of SmIg; the reverse pattern is usual in most types of B-lineage
NHL)
Secondary panel
For further investigation of suspected CD10 (more often positive in follicular lymphoma); CD11c, CD25, CD103 and B-lineage lymphoproliferative HC2 (for suspected hairy cell leukaemia); anti-cyclin D1 (suspected mantle disorder cell lymphoma); CD38, CD79a, CD138 and CyIg (for suspected plasma cell or
lymphoplasmacytoid neoplasm)
For further investigation of suspected CD4, CD8 (usually positive in large granular lymphocyte leukaemia), CD7 T-lineage lymphoproliferative (usually positive in T-PLL), CD25 (usually positive in ATLL); CD11b, CD16, disorder CD56, CD57 (for suspected large granular lymphocyte or NK cell
leukaemia/lymphoma)
Anti-terminal deoxynucleotidyl Recommended if it is not certain if cells are precursor lymphocytes transferase (anti-TdT) (ALL or lymphoblastic lymphoma) or mature lymphocytes
For planning of therapy CD20 (or any other antigen that may be a target of monoclonal antibody therapy)

SPECIAL TECHNIQUES 65
association with preserved information regardingthe spatial organization of labelled and unlabelledcells. Immunohistochemistry also permits assess-ment of the cytological features of cells expressingparticular antigens, in a context which is often morefamiliar than that offered by immunocytochemistry(particularly cytocentrifuge preparations, in whichsignificant morphological artefacts are induced bythe centrifugation technique itself).
Because a large number of antigens can bestained individually in adjacent thin tissue sections,the lack of easy techniques for double-staining isnot a major problem in immunohistochemistry per-formed for diagnostic and staging purposes. In acomplex infiltrate it is relatively easy to demonstratea variety of cell types differing in morphological andimmunophenotypic characteristics. For example, inT-cell-rich B-cell lymphoma, the large, neoplasticcells can be shown to have a B-cell phenotype whilethe more numerous T cells are seen to be cytologi-cally normal small lymphocytes.
Immunohistochemistry can permit the identifica-tion and characterization of an abnormal bone marrow infiltrate not represented in the patient’saspirate sample. This situation usually arises whenthere is significant reticulin fibrosis associated withan infiltrate, which hinders aspiration of cells fromthe involved area or areas of bone marrow. Suchreticulin fibrosis occurs frequently in follicular lym-phoma and almost invariably accompanies bonemarrow infiltration by Hodgkin’s disease.
When immunohistochemistry first gained wide-spread use in histopathology during the 1970s, itwas commonly assumed that decalcification, particu-larly with methods involving exposure to acids, ledto destruction of many antigens. This has proved tobe untrue and the procedure can be performed verysuccessfully with acid- or EDTA-decalcified trephinebiopsies as well as with non-decalcified samplesembedded in methacrylate resins. A few importanttechnical modifications were required to overcomethe different performance of bone marrow trephinebiopsy specimens relative to other formalin-fixedtissues. For example, early antigen retrieval tech-niques, involving tissue digestion by proteolyticenzymes to reverse protein–protein binding inducedby formalin fixation, were responsible for many initial poor results of immunohistochemistry inbone marrow trephine biopsy specimens as a conse-
quence of degradation of the antigenic target. Priorexposure to acid appears to render formalin-fixedtissue more susceptible to proteolysis and leads todegradation of some antigenic targets during incu-bation with the enzyme. In general, considerablyshortened incubation times have therefore beenfound to be beneficial with these antigen retrievalmethods. The major advance, however, has comethrough development of wet-heat methods for antigen retrieval, exposing tissue sections to acid oralkaline solutions in combination with microwaveoven or pressure cooker heating. This has been asimportant for immunohistochemistry as a generaltool in histopathology as it has been for bone mar-row trephine biopsy specimens. It has encouraged ahuge expansion in the development of new mono-clonal antibodies for diagnosis in addition to makingpossible excellent results using many existing anti-bodies that were previously unsuccessful.
The second technical modification required forsuccessful immunohistochemistry in bone marrowbiopsy specimens was necessary to minimize non-specific staining due to endogenous enzyme activity.Most methods employ indirect labelling techniqueswith either peroxidase or alkaline phosphatase con-jugated to the secondary antibody. The enzymegenerates an insoluble, coloured product from achromogenic substrate to permit visualization of theprimary antigen–antibody interaction. Cells of thegranulocyte series, particularly eosinophils, are richin endogenous peroxidase activity and bone mar-row stroma contains dendritic cells that are rich inalkaline phosphatases. When performing immuno-histochemistry on bone marrow trephine biopsyspecimens, additional steps are required to blocksuch endogenous enzyme activities and minimizenon-specific staining. To compound this problem,highly efficient amplification steps are included inmany current immunohistochemistry methods, in-creasing sensitivity by exploiting the extremely highbinding affinity of avidin or streptavidin for biotin.Endogenous biotin activity, particularly in mastcells, may also therefore require specific blockade toavoid false-positive staining.
In practice, the necessary technical modificationsare easy to incorporate to achieve excellent results inbone marrow trephine biopsy samples with a rangeof primary antibodies. While this range is somewhatlimited compared with that used in flow cytometry,

it is nonetheless extensive. Moreover, since muchbone marrow trephine biopsy immunohistochemistryis performed in the investigation of lymphoprolifer-ative disorders, it is valuable that the antibodieswhich can be used successfully are also entirelysuitable for use with other formalin-fixed tissuesamples such as biopsied lymph nodes.
Immunohistochemistry can be used to demonstratesurface membrane, cytoplasmic and nuclear anti-
gens. It can be used specifically to provide moleculargenetic information, e.g. by demonstration of theprotein product of oncogenes, such as ALK, BCL1and BCL2, or of cancer-suppressing genes, such asp53.
Tables 2.6 and 2.7 give details of useful anti-bodies for the immunohistochemical detection of antigen expression on haemopoietic and lym-phoid cells in bone marrow trephine biopsies.
66 CHAPTER TWO
Table 2.6 Antigens expressed by myeloid cells and demonstrable by immunohistochemistry in fixed, decalcified bonemarrow trephine biopsy specimens.
Antigen
CD34
CD45
Lysozyme(muramidase)
Myeloperoxidase
Alpha-1-antitrypsin
CD66e
CD68—broadspecificity
CD68—monocyterestricted
CD163
CD14
Neutrophil elastase
CD15
Comments
Endothelial cells also positive
Proteolytic pre-treatmentabolishes granulocytic andmonocytic reactivity
Many metastases of epithelialorigin also positive
Mast cells also positive
Mast cells also positive
Developing monocytes stronglypositive; macrophages weak ornegative
Promyelocytes and myelocytesstrongly positive; metamyelocytesand mature neutrophils stainweakly or are negative
Membrane and cytoplasmicstaining but membranes negativeafter proteolytic pre-treatment;expressed by neoplastic cells ofHodgkin’s disease
Specificity
Primitive haemopoieticcells
Lymphoid, granulocyticand monocytic cells
Granulocytic andmonocytic cells
Granulocytic andmonocytic cells
Granulocytic andmonocytic cells
Granulocytic cells
Granulocytic andmonocytic cells, includingosteoclasts
Monocytic cells, includingosteoclasts
Monocyte lineage cellsincluding osteoclasts
Monocytic cells
Granulocytic cells
Monocytic and granulocyticcells, especially lategranulocyte precursors
Antibody
QBEnd 10
PD7/26, RP2/18, RP2/22
Polyclonal antisera
Polyclonal antisera
Polyclonal antisera
85A12
KP1
PG-M1
10D6
NCL-CD14-223
NP57
LeuM1, BY87

SPECIAL TECHNIQUES 67
Antigen
Calprotectin(previously called calgranulin)
Eosinophil major basic protein
Mast cell tryptase
CD117
CD1a
Glycophorin A(α-sialoglycoprotein)
Glycophorin C(β-sialoglycoprotein)
Spectrin
Haemoglobin A
An epitope on the ABO blood group H glycoprotein
CD61
CD42b
Von Willebrand factor(previously known as Factor VIII-related antigen)
Comments
Macrophages weakly stained ornegative
Avoidance of problems withdiffusion of reaction product andnon-specific background stainingneeds careful pre-treatment
The antibody is not sufficientlysensitive in fixed, decalcifiedtrephine biopsy sections to detecthaemopoietic progenitor cells
Few, if any, such cells are normallypresent; used in diagnosis ofLangerhans cell histiocytosis
Very early proerythroblasts notstained
Expression seen in earlierproerythroblasts than α-sialoglycoprotein; cross-reactivitywith myeloblasts is seen in somecases of AML
No commercially availableantibody at present [18]
Early erythroid precursors weak ornegative
Expressed from earliestrecognizable stages of erythroiddifferentiation; also expressed byendothelial cells, megakaryocytesand cells of some large celllymphomas
Variable staining between cells;many early or dysplasticmegakaryocytes unstained
Strong, uniform cytoplasmicstaining, including early anddysplastic forms
Strong cytoplasmic staining;variable results with early anddysplastic forms
Specificity
Late granulocyte precursorsand monocytic cells
Eosinophil granulocytes
Mast cells
Mast cells
Langerhans cells
Erythroid cells
Erythroid cells
Erythroid cells
Haemoglobinizederythroid cells
Erythroid cells
Megakaryocytes
Megakaryocytes
Megakaryocytes
Antibody
Mac387
BMK13
AA1
57A5D8
MTB1, JPM30
JC159, BRIC101
Ret40f
Polyclonal antisera
Polyclonal antisera
BNH9
Y2/51
MM2/174
F8/86 and variouspolyclonal antisera
Table 2.6 (cont’d)

68 CHAPTER TWO
Table 2.7 Antigens expressed by lymphoid cells (B, T and NK lineages) and demonstrable by immunohistochemistry infixed, decalcified bone marrow trephine biopsy specimens.
Antigen Antibody Specificity Comments
CD45 PD7/26, RP218, Lymphoid, granulocytic Proteolytic pre-treatment minimizesRP2/22 and monocytic cells granulocytic and monocytic staining
Terminal NPT26 Primitive lymphoid cells In addition to ALL, up to 15% of AMLdeoxynucleotidyl and some primitive are positivetransferase (TdT) myeloid cells
CD10 56C6 Subsets of B cells Expressed in common and pre-B ALL, Burkitt’s lymphoma and follicle centre cell lymphoma; also expressed by a subset of marrow stromal cells
CD20 L26 Most B cells Some early B-lineage lymphoid cells and cells showing plasmacytic differentiation are negative
CD79a Mb1, HM47/A9, Most B cells Includes early B-lineage lymphoid cells andJCB117 those with plasmacytic differentiation; may
be negative in non-secretory myeloma; megakaryocytes are weakly positive
CDw75 LN1 B cells Preferential staining of large, transformed B cells (e.g. centroblasts and immunoblasts)
CD45RA 4KB5 B cells and a subset Small, mature B cells stain preferentiallyof T-lineage lymphoid cells
Immunoglobulin Polyclonal Plasma cells Expression by other B cells usually too weak light chains— antisera are to be detected; excessive background κ and λ usually used staining may occur due to plasma
immunoglobulins within the tissue
Immunoglobulin Polyclonal Plasma cells Expression by other B cells usually too weak heavy chains antisera are to be detected; excessive background —γ, α, µ, ε, δ usually used staining may occur due to plasma
immunoglobulins within the tissue
Rough endoplasmic VS38c Plasma cells Osteoblasts and a subset of stromal cells reticulum-associated also stainantigen (p63)
CD138 (syndecan) B-B4 Plasma cells Some carcinomas and large cell NHL are positive
CD38 AT13/5 Plasma cells Also expressed by thymocytes, early B cells, germinal centre B cells and some erythroid cells and neutrophils
Unclustered DBA44 B cells Relative specificity for hairy cell leukaemia; red cell membranes and some macrophages may also stain
Tartrate-resistant 9C5 and 14G6 Hairy cell leukaemia Mast cells, Langerhans cells, macrophages acid phosphatase and osteoclasts also stain [19]
CD23 1B12 Subset of B cells Small lymphocytic lymphoma/CLL positive; mantle cell, lymphoplasmacytoid and folliclecentre cell lymphomas negative

SPECIAL TECHNIQUES 69
CD5 4C7 Subset of B cells, Small lymphocytic lymphoma/CLL andmost T cells mantle cell lymphoma positive;
lymphoplasmacytoid and follicle centre cell lymphomas negative
BCL2 Bcl-2/100/D5, I24 T cells, mantle zone B Non-neoplastic germinal centre cells are lymphocytes and follicle negative; other B-cell lymphomas and some centre cell lymphoma haemopoietic cells are positive; it is difficult
to interpret positive staining in the bone marrow
Cyclin D1 DCS-6, P2D11F11 Mantle cell lymphoma Apoptotic nuclei and some endothelial (nuclear expression) cell nuclei are positive; immunostaining is
technically difficult
CD2 AB75 Most T cells Also expressed by some monocytes
CD3 CD3-12 and Most T cells More specific than CD2; the monoclonal polyclonal antibody is superior in performance to antisera polyclonal antisera
T-cell receptor βF1 T cells expressing αβ The majority of CD3-positive T cells and cells β chain T-cell receptor of many T-lineage neoplasms
CD45RO—broad UCHL-1 Antigen-experienced Granulocytes, monocytes and macrophages specificity T cells (membrane are also positive (cytoplasmic expression);
expression) excessive decalcification may lead to non-specific nuclear staining
CD45RO—T-cell OPD4 Antigen-experienced Less reactivity with non-lymphoid lineage restricted T cells (membrane cells than with UCHL1
expression)
CD43 MT1, DFT1 Most T cells and a subset Strong expression by granulocytic and of B cells; lymphocytic monocytic cellslymphoma/CLL and mantle cell lymphoma are usually positive; follicular lymphoma, lymphoplasmacyticlymphoma and marginal zone lymphomas are negative
CD4 1F6 T-cell subset There is often poor localization of reaction product to individual cells; macrophages are also positive
CD8 4B11 T-cell subset
CD56 1B6 Natural killer cells and Nerve fibres, neuro-ectodermal tumours, some cytotoxic T cells some leukaemic myeloblasts and cells
of some cases of multiple myeloma are positive
CD57 Leu7, NC1 Natural killer cells and Nerve fibres and neuro-ectodermal tumours some cytotoxic T cells are positive
Table 2.7 (cont’d)
Antigen Antibody Specificity Comments

Immunohistochemical stains are illustrated in Figs 2.16–2.19. Monoclonal antibodies useful in the detection of micro-organisms are shown inTable 3.1 and those for use in the diagnosis of non-haemopoietic malignancy in Table 10.1.
Problems and pitfalls
Antigen cross-reactivity between cell types. Antigencross-reactivity between different types of cell is a significant problem in immunohistochemistry
70 CHAPTER TWO
CD30 BerH2 Reed–Sternberg cells and Plasma cells and some erythroid precursors mononuclear Hodgkin’s positive if proteolytic pre-treatment is used; cells, cells of anaplastic wet-heat antigen retrieval is preferred; large cell lymphoma and some carcinomas, especially embryonal, some other pleomorphic are positivelarge cell lymphomas
CD15 LeuM1, BY87 Neoplastic cells in classical Granulocytic and monocytic cells positive, Hodgkin’s disease (but may particularly late granulocyte precursors be negative in up to 15% of cases of Hodgkin’s disease including lymphocyte-predominant)
Epithelial GP1.4 Cells of anaplastic large Some plasma cells are positive; neoplastic cells membrane antigen cell lymphoma in some cases of Hodgkin’s disease and many
carcinomas are positive; some cases of anaplastic large cell lymphoma are negative
Anaplastic lymphoma- ALK-1 Cells of anaplastic large More likely to be positive in childhood than associated kinase cell lymphoma adult cases
Ki67 antigen Ki67, MM1, Proliferating cells Useful for assessing grade of lymphoma from MIB-1 (nuclear expression) infiltrates in bone marrow; proliferating
haemopoietic cells are also positive
Table 2.7 (cont’d)
Antigen Antibody Specificity Comments
Fig. 2.16 Section of trephinebiopsy specimen from a patientwith a myelodysplastic syndromeshowing elastase-positivegranulocyte precursors. Paraffin-embedded, immunoperoxidasetechnique with anti-elastase McAb NP5 ×960.

Fig. 2.17 Section of trephinebiopsy specimen from a patientwith M6 AML showingerythroblasts, one of which isbinucleated. Paraffin-embedded,immunoperoxidase technique withantiglycophorin antibody McAbRet40f ×940.
Fig. 2.18 Section of trephinebiopsy specimen from a patientwith a myelodysplastic syndromeshowing a cluster ofmegakaryocytes. Paraffin-embedded, immunoperoxidasetechnique with CD61 McAb ×940.
Fig. 2.19 Section of trephinebiopsy specimen showingpericapillary plasma cells. Paraffin-embedded, immunoperoxidasetechnique with McAb VS38c ×940.
SPECIAL TECHNIQUES 71

(Fig. 2.20). There is a tendency to regard antigen ex-pression as being lineage-specific, whereas expressionis more accurately considered as lineage-associatedor lineage-restricted. Many antigens familiar in the context of expression by T cells, B cells or bothin lymphoid tissues are also expressed by myeloidlineages. This is particularly the case with T-cell-associated antigens, which are widely expressed bycells of granulocytic and monocytic lineages. CD43should be avoided as a T-cell marker in bone marrow because of extensive cross-reactivity of thistype. Antibodies reactive with CD45RO should beselected with care; the clone OPD4 stains T cellspreferentially, with little granulocytic and mono-cytic reactivity, while UCHL-1 often stains cells ofthe latter types strongly. Expression of CD45RO bygranulocytes and monocytes can be distinguishedfrom that shown by T cells since the former is cytoplasmic, whereas T cells show membrane stain-ing. Bone marrow stromal macrophages expressCD4 and, because of the poor localization of a ratherweak signal that is often seen with the currentlyavailable antibody, accurate assessment of CD4-positive T cells may not be possible. Monoclonalantibodies reactive with CD3 are currently the bestand most specific T-cell markers for use with bonemarrow trephine biopsy sections.
For B cells, CD79a is probably the best antigenictarget but some antibody clones cross-react withvascular smooth muscle and megakaryocytes; thesereactivities rarely cause problems in interpretation.
In our experience, many bone marrow B cells appearnegative or react only weakly for CD20; both CD79aand an alternative B-cell marker, 4KB5 (CD45RA),show consistently more small B cells than doesCD20 both in normal bone marrow and in low gradelymphoproliferative disorders. For this reason, tre-phine biopsy immunostaining for assessment ofCD20 expression for therapeutic purposes shouldnot, at present, be regarded as reliable if a negativeresult is obtained. It should be noted that L26, theCD20 monoclonal antibody used to detect reactivityin trephine biopsy specimens, detects an intracellu-lar epitope, whereas the monoclonal antibody usedfor therapy reacts with a surface membrane epitope.Antibodies directed against CD5 and BCL2 reactwith T cells as well as subsets of normal and neo-plastic B cells; results should be interpreted withcare in bone marrow lymphoid infiltrates, in whichnon-neoplastic T cells frequently predominate.
The specificity of CD45 antibodies for lymphoidcells can be improved if myeloid reactivity is reducedby proteolysis (performed as for antigen retrieval).Antibodies reactive with CD30 may cross-react withplasma cells and, depending on fixation, with eryth-roid cells. Expression in these cell types is cytoplas-mic rather than Golgi- or membrane-associated as inReed–Sternberg cells or cells of anaplastic large celllymphoma. This cross-reactivity is unlikely to causedifficulty in the interpretation of possibly lymphoidinfiltrates. However, it can be abolished by use of wetheat for antigen retrieval, rather than proteolysis.
72 CHAPTER TWO
Fig. 2.20 BM trephine biopsysection from a patient with diffuselarge B-cell lymphoma; there is heavy interstitial lymphoidinfiltrate with lymphoma cellsshowing moderate activity forCD79a (clone Mb1), whereas threemegakaryocytes show strong cross-reactivity. Immunoperoxidase,CD79a ×188.

SPECIAL TECHNIQUES 73
Endothelial cell expression of CD34 can mimicreactivity in haemopoietic cells if tiny capillaries are viewed in cross-section. However, the granularnature of haemopoietic cell CD34 expression can bedistinguished from the homogeneous pattern seenin endothelium.
Problems relating to fixation and decalcification. Use ofproprietary combined fixative–decalcifier solutionscan lead to extensive loss of immunoreactivitywithin tissues, as can excessive decalcification byEDTA. Even in optimally fixed and decalcified tissues, some antigens are difficult to demonstrate.Cyclin D1 and CD4 are problematical in this regardwith currently available monoclonal antibodies.Non-specific nuclear staining may occur with avariety of antibodies in tissues that are poorly fixed,excessively decalcified or both. In our experience,the antibodies UCHL-1 (CD45RO), Ber-H2 (CD30)and NB84 are particularly prone to this problem.
Technical problems due to endogenous enzyme activityand non-specific antibody binding. Endogenous enzymeactivity and non-specific antibody binding can bothlead to technical problems. When immunostain-ing trephine biopsy sections with detection systemsbased on horseradish peroxidase, particular atten-tion must be paid to blockade of endogenous per-oxidase activity. Granulocytes express abundantperoxidase activity that is not destroyed by fixationor processing. Use of methanolic hydrogen peroxideis satisfactory but longer incubation (e.g. 30 minutes,compared with 15 minutes for most other tissues) is helpful. Because the solution oxidizes rapidly,replacement with freshly prepared methanol/H2O2
at intervals during incubation is helpful. Addition of sodium azide to the final chromogenic substrateprovides additional peroxidase blockade in difficultcases.
When using an alkaline phosphatase–anti-alkaline phosphatase detection system, there israrely any problem from endogenous alkaline phosphatase activity, since the enzyme is largelydestroyed during processing. A weak backgroundblush may be seen in some cases, due to residualactivity in stromal cells. This can be inhibited byadding levamisole to the chromogenic substrate.
Occasionally, endogenous biotin expression cancause non-specific staining when avidin–biotin or
streptavidin–biotin detection systems are used. Thisis found particularly when using antibody AA1 todemonstrate mast cell tryptase. Such activity can beblocked by sequential incubation of sections withsaturating solutions of avidin and biotin prior toimmunostaining.
Non-specific binding of antibodies to proteinresidues in the tissue, which may be a particularproblem with polyclonal antisera, can be blocked bypre-incubation of sections with bovine serum albu-min or normal human serum. Background serumstaining with anti-immunoglobulin light and heavychain antibodies may be reduced by use of wet heat methods for antigen retrieval rather than proteolysis.
Problems of interpretation. Other problems in inter-pretation can occur. As mentioned above, im-munostaining for antigens such as CD4 and cyclinD1 can be suboptimal and results need to be inter-preted with care. Positive controls, with knownreactivity, should always be performed to ensurethat the technique has worked satisfactorily. It may be necessary to repeat the staining in somecases. It should be noted that cyclin D1 expressionin mantle cell lymphoma is nuclear (and only a pro-portion of cells are positive). This nuclear stainingshould not be confused with non-specific weakcytoplasmic staining that is sometimes observed inother neoplastic lymphocytes.
Expression of CD5 by neoplastic B cells in chroniclymphocytic leukaemia (CLL) and mantle cell lymphoma is much weaker than the constitutiveexpression of this antigen by T cells. For this reason,it is important to ensure that the dilution of theantibody used is optimal for the detection of weaklyexpressed antigens on neoplastic cells. Similarly, itis important to use for comparison a positive controlthat represents one of these lymphomas, rather thannormal tissue. The detection of neoplastic B cells inCD5-immunostained bone marrow trephine biopsysections requires careful evaluation of sections sincesuch cells are often present among a backgroundpopulation that contains numerous, strongly stained,non-neoplastic T cells.
Detection of BCL2 expression by cells in B-celllymphoid infiltrates in bone marrow is seldom use-ful because of the abundance of non-neoplastic,BCL2-positive T cells, the rarity of follicle formation

and the positive reactions that can be observed notonly in follicular lymphoma but also in other B-celllymphomas.
Cytogenetic analysis
Specific, non-random chromosomal abnormalitiesare a common finding in haematological neoplasmsand often play a central role in pathogenesis. Inaddition, some haematological neoplasms are de-fined more precisely by the presence of specificchromosomal abnormalities than by haemato-logical or histological features. For example, aspecific subtype of AML, which can be designatedM4Eo/inv(16)(p13q22)/CBFβ-MYH11 fusion AML,is better defined by the presence of inversion ofchromosome 16 than by the cytological or histolog-ical features of acute myelomonocytic leukaemiawith eosinophilia. The presence of certain chromo-somal abnormalities also offers prognostic informa-tion. For example, in AML, the presence of t(8;21)(q22;q22), t(15;17)(q22;q21) or inv(16)(p13q22) isindicative of a better prognosis. Cytogenetic analy-sis can also help in distinguishing a neoplastic froma reactive process, as when the demonstration of aclonal cytogenetic abnormality provides evidencethat a case of ‘idiopathic’ hypereosinophilic syn-drome is actually eosinophilic leukaemia.
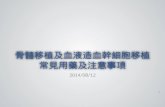
Classical cytogenetic analysis can be performedonly on cell suspensions such as those obtained fromperipheral blood or bone marrow [20]. Cytogeneticanalysis for investigation of suspected haematolog-ical neoplasms involves the examination of meta-phase spreads which can be prepared from blood or from bone marrow aspirates either as directpreparations, in tumours with a high proliferativefraction, or after a preliminary period of culture eitherwith or without mitogens. Cells are arrested in meta-phase by exposure to a spindle poison such as col-cemid. After cell lysis the chromosomes are visualizedwith stains such as Giemsa or quinacrine mustard (a fluorescent agent). Individual chromosomes areidentified by their size, by the position of the cen-tromere and by their banding pattern (the sequenceof light and dark bands apparent after staining). The findings may be illustrated by a karyogram, anordered array of chromosomes (Fig. 2.21). Alterna-tively, they may be expressed as a karyotype. Forexample, the karyotype 47,XY,+8 [18], 46,XY [2]from the bone marrow of a male patient indicatesthe presence of a clone of cells with trisomy 8; of the20 metaphases examined, two were normal.
Cytogenetic analysis has a major role in haemato-logical diagnosis. Applications include:1 confirmation of diagnosis, e.g. by demonstrationof t(15;17)(q22;q21) in M3 variant AML;
74 CHAPTER TWO
Fig. 2.21 A karyogram showingt(11;14)(q13;q32) in mantle celllymphoma. (By courtesy of Dr Fiona Ross, Salisbury.)

SPECIAL TECHNIQUES 75
2 detection of chromosomal rearrangements thatare indicative of good or bad prognosis and shouldbe considered in the choice of treatment, e.g.demonstration of hyperdiploidy, indicative of goodprognosis in ALL;3 confirmation of a neoplastic process when this is otherwise difficult, e.g. in the hypereosinophilicsyndrome or in lymphocytosis with large granularlymphocytes;4 monitoring treatment, e.g. by estimation of thenumber of Philadelphia chromosome-positive meta-phases when a patient with chronic granulocyticleukaemia is being treated with interferon;5 post-transplant monitoring, e.g. by study of sexchromosomes in a sex-mismatched allogeneic stemcell or bone marrow transplant recipient;6 diagnosis of therapy-related AML and MDS (seeChapter 4); and7 confirmation of a constitutional abnormality thatmay underlie the development of a haematologicalmalignancy, e.g. detection of trisomy 21 in a childwith acute megakaryoblastic leukaemia in whomDown’s syndrome is suspected, or demonstration ofsensitivity to clastogenic agents, confirming a diag-nosis of underlying Fanconi’s anaemia in a patientpresenting with AML.
Problems and pitfalls
Metaphase spreads in leukaemias are often of poorquality so that the characterization of an abnormal-ity can be difficult. In addition, some specific chro-mosomal rearrangements, e.g. t(12;21)(p12;q22) in ALL, are difficult to detect by karyotypic ana-lysis while others are impossible; for these rear-rangements, molecular genetic techniques arerequired.
Cytogenetic analysis fails or yields too few meta-phases for adequate analysis in a proportion of casesof acute leukaemia. Inappropriate techniques maymean that there is selection for residual normalcells, e.g. if direct examination rather than prelimi-nary culture is used for the investigation of acutepromyelocytic leukaemia.
When there is only partial replacement of themarrow by a neoplastic clone, e.g. in the MDS, acytogenetically abnormal clone may be present butmay not be identified if insufficient metaphases areexamined.
In some slowly growing tumours it is not possibleto obtain suitable metaphase preparations and meta-phases may represent residual normal cells ratherthan neoplastic cells. This is often the case, for ex-ample, in CLL.
Molecular genetic analysis
Cytogenetic analysis has been part of the diagnosticassessment of haematological neoplasms for manyyears. More recently, techniques such as Southernblot analysis and PCR have allowed molecular geneticevents associated with such chromosomal abnor-malities to be studied. These techniques have alsoled to the detection of additional genetic abnormal-ities in haematological diseases. They are being usedincreasingly for diagnosis and follow-up of patientson a routine basis.
In addition, molecular genetic analysis can be usedto establish clonality; this is particularly valuable inlymphoid neoplasms, where antigen receptor generearrangements provide unique clonal markers forneoplastic cell populations. Molecular genetic tech-niques are most readily applicable to peripheralblood or bone marrow aspirates but modified tech-niques suitable for application to trephine biopsiesare being developed currently.
New concepts with regard to somatic hypermuta-tion of antigen receptor (IGH and TCR) variableregion genes in lymphoid cell maturation are emer-ging currently from molecular genetic analysis.Knowledge of such mechanisms in T-cell matura-tion is much less advanced than it is for the B-celllineage. Basic understanding of the somatic mutationprocesses underlying affinity maturation of immuno-globulin molecules, which occur within germinalcentres, allows distinction between lymphomasderived from pregerminal centre (non-mutated),germinal centre (hypermutated with evidence ofongoing acquisition of additional mutations) andpostgerminal centre (hypermutated with no ongo-ing mutation) lymphoid cells. For example, sub-categories of CLL have been described which differby virtue of showing pregerminal centre (60%) and postgerminal centre (40%) patterns of IGHhypermutation.
Molecular analysis can also be used to identifyviral DNA or RNA in blood or bone marrow (seeChapter 3).

Fluorescence and other in situ hybridizationtechniques
In situ hybridization (ISH) is a molecular genetictechnique although it can also be regarded as anextension of conventional cytogenetics. It is basedon the hybridization of a labelled probe to inter-phase nuclei or metaphase spreads. The techniquecan employ fluorescence microscopy (fluorescencein situ hybridization or FISH), enzymatic methods[21,22] or a radioactive label. Probes, consisting ofsynthetic DNA in various forms, visualized with theaid of fluorochromes, enzymes or radio-isotopes,can be used to detect numerical abnormalities ofchromosomes or the presence of various chromoso-mal rearrangements. Target DNA may be identifiedby means of a probe conjugated to a fluorochrome.Alternatively, binding of the probe to target DNAcan be identified by means of hybridization of theprimary probe to complementary bases in a secondcomplementary probe that also contains a reportermolecule [20]. Following stringency washes per-formed to remove excess probe, binding of the probeto its target DNA is detected by means of complex-ing of the reporter molecule in the second probewith a reporter-binding molecule conjugated eitherto a fluorochrome or to an enzyme such as perox-idase or alkaline phosphatase. By using differentfluorochromes or two enzymes it is possible to iden-tify simultaneously multiple (typically two or three)different specific DNA sequences in a single prep-aration of cells. Direct fluorescence methods aremore rapid than indirect and give less non-specificbackground staining, whereas indirect fluorescencemethods generally give a stronger signal. Enzymaticmethods are currently less used but have the advan-tage that a fluorescence microscope is not needed.
Fluorescence and other ISH techniques are ap-plicable to: (i) films of blood or bone marrow cells;(ii) imprints of trephine biopsy specimens; (iii) cytocentrifuge preparations; and (iv) films of cellsthat have been cultured with or without mitogens.These techniques have the particular advantageover classical cytogenetic analysis that they can be applied not only to metaphase spreads but also tointerphase nuclei. Chromosome abnormalities cantherefore be detected in neoplastic cells that do notreadily enter mitosis, such as the neoplastic cells ofCLL and multiple myeloma. In addition, ISH can be
applied to blood or bone marrow films previouslystained with a Romanowsky stain or by immunocyto-chemistry, thus permitting correlation of cytologicaland immunophenotypic features with karyotypicinformation. Obviously, unlike cytogenetic analy-sis, ISH permits visualization of only restricted areasof individual chromosomes rather than giving aglobal view of the entire chromosome complementwithin a cell.
The probes most often employed in ISH techniquesare: (i) repetitive sequence centromeric probes (avail-able for all chromosomes and applicable to cells ininterphase or metaphase); (ii) whole chromosomepaints (available for all chromosomes but appli-cable only to cells in metaphase); and (iii) specificsequence probes, including those identifying onco-genes, cancer-suppressing genes and the break-points of recurring translocations (applicable to cellsin interphase or metaphase).
Numerical abnormalities of chromosomes can bedetected either with centromeric probes or withwhole chromosome paints. When such probes areused, normal cells have two separate fluorescentsignals. If there is an abnormality of chromosomenumber, the number of signals will vary. For ex-ample, in trisomy 12, FISH with a centromeric probefor chromosome 12 shows three signals per cellwhereas, in monosomy 7, FISH with a centromericprobe for chromosome 7 shows only one signal percell (Fig. 2.22). If using centromeric probes, ratherthan whole chromosome paints, care must be takenin making assumptions that gain or loss of a signalrepresents gain or loss of an entire chromosome target.
Several strategies can be used for detecting specifictranslocations or other rearrangements. Use of asingle probe spanning a specific chromosomal break-point is useful when multiple chromosomal partnerscan disrupt a gene of interest, as is the case withMLL and BCL6. When both partner chromosomesare predictable a variety of techniques can be used.Whole chromosome paints can be used for the twochromosomes of interest. Alternatively, two probescan be selected which bind to specific oncogenes orbind to the two chromosomes of interest at a siteclose to the expected breakpoint. The two probesare labelled with different fluorochromes. In normalcells there will be two separate signals of differentcolours whereas, in cells in which a translocation
76 CHAPTER TWO

SPECIAL TECHNIQUES 77
has occurred, the two colours come together on a single chromosome (Fig. 2.23). Alternatively,probes spanning the expected breakpoint on eachchromosome can be used so that, if a translocationhas occurred, the signals are split. Each abnormalchromosome then has two adjacent signals of dif-ferent colours, while the two remaining normalchromosomes have a single colour signal (Fig. 2.24);this technique is sometimes referred to as D-FISH,signifying double fusion FISH. It is also possible tocombine one probe spanning an expected break-point with another that is adjacent to the secondbreakpoint. A single probe spanning one of thebreakpoints can also be used, a split signal beingconsistent with a translocation. In this case it issometimes necessary to demonstrate that three signals represent a normal and a split signal ratherthan trisomy (Fig. 2.25). Triple colour FISH permitsthe use of a single probe identifying a sequence onone of the chromosomes implicated together withtwo separate probes identifying genes on either sideof the breakpoint on the second chromosome. Thelatter two signals are dissociated when the relevanttranslocation occurs (Fig. 2.26).
(a)
Fig. 2.23 Diagrammatic representation illustrating theprinciples of FISH, using two oncogene probes to detect atranslocation. Probes for BCR (red) and ABL (green) havebeen used. In the normal cell (left) there are four separatesignals. In the cell from a patient with t(9;22)(q34;q11)associated with chronic granulocytic leukaemia (right)there are single normal BCR and ABL signals and a doublered plus green signal where the two oncogenes have beenjuxtaposed. The red–green signal is yellow.
Fig. 2.22 Diagrammatic representation illustrating the principles of FISH, using a centromeric probe for the identificationof trisomy or monosomy. (a) Centromeric probe for chromosome 12 in chronic lymphocytic leukaemia showing fourtrisomic cells and one disomic cell. (b) Centromeric probe for chromosome 7 in myelodysplastic syndrome showing allcells to have monosomy 7.
(b)

difficult to recognize on classical cytogenetic ana-lysis if preparations are suboptimal, can be detected; 5 large numbers of cells can be scanned so that a lowfrequency abnormal population can be recognized;and6 deletion of cancer-suppressing genes or amplifica-tion of oncogenes can be demonstrated.
Fluorescent immunophenotyping and interphasecytogenetics (FICTION) is a technique combiningimmunophenotyping with FISH. It can be used, for example, to demonstrate that trisomy 12 in CLL can occur in only a proportion of the clonal lymphocytes.
A recent development of FISH is spectral karyo-typing (SKY) in which a complex panel of probesapplied simultaneously permits the identification of all chromosomes in metaphase preparations.
78 CHAPTER TWO
Fig. 2.24 Diagrammatic representation illustrating theprinciples of FISH, using two oncogene probes, both ofwhich are split in a given translocation, to detect thetranslocation. Probes spanning BCR (red) and ABL(green) have been used. In the normal cell (left) there are four separate signals. In the cell from a patient witht(9;22)(q34;q11) associated with chronic granulocyticleukaemia (right) there are single normal BCR and ABLsignals and two double red plus green signals (fusionsignals are yellow) representing BCR-ABL and ABL-BCR.
(a)
(b)
Fig. 2.25 Diagrammatic representation illustrating theprinciples of FISH, using a whole chromosome paint to detect a translocation. (a) In this case, a paint forchromosome 11 has been used. A normal cell (left) shows two signals, whereas a cell from a patient witht(11;14)(q13;q32) associated with mantle cell lymphoma(right) shows three signals representing, respectively, one normal chromosome and two signals representingthe two parts of chromosome 11 separated as a result oftranslocation. (b) To ensure that the three signals do notrepresent trisomy for chromosome 11, FISH can also beperformed with a centromeric probe for chromosome 11;since the centromere is not split in the translocation thisshows two signals in both the normal cell (left) and thecell with the translocation (right).
Probes spanning specific breakpoints are also usefulfor detecting isochromosome formation (Fig. 2.27)and chromosomal inversion. For example, inver-sion of chromosome 16 can be detected by using aprobe that spans one of the breakpoints. When apericentric inversion has occurred, the signal is splitand appears on both the long and short arms of thechromosome in a metaphase spread (Fig. 2.28).
The FISH technique can also be used to identifydeletion or amplification of chromosomal material.For example, specific probes can be used to showdeletion of a cancer-suppressing gene such as RB1or p53 or amplification of an oncogene such as MYC.
An ISH technique has the following advantagesover classical cytogenetics: 1 living cells are not required; 2 some abnormalities can be recognized in inter-phase nuclei, making the technique particularlyuseful for neoplasms, such as CLL, with a low pro-liferative rate;3 a suspected abnormality can be confirmed whenmorphology of the chromosomes is poor; 4 chromosomal rearrangements, such as inver-sion(16), which have only subtle alterations in thechromosome banding pattern and are therefore

SPECIAL TECHNIQUES 79
This technique is particularly useful for investiga-ting complex chromosomal abnormalities. Becauseexpensive equipment, reagents and software arerequired the technique is currently mainly used inresearch rather than in routine diagnosis.
Techniques for FISH are applicable to a more lim-ited extent to trephine biopsy sections, in which atpresent they are best restricted to analysis of poten-tial chromosomal gains. For mathematical reasons,analysis of chromosomal loss in tissue sections (inwhich many nuclei are only partly represented) is complex. Spatial resolution of FISH signals in histological sections is not adequate with currentmethods to permit routine application of dual colourtechniques to demonstrate translocations, althoughsplit signals from a probe spanning an expected break-point can be resolved. Some of these limitations canbe overcome by applying FISH to cytocentrifuge prep-arations from intact nuclei or whole cells extractedby proteolysis from thick sections. As for immuno-histochemistry, pre-treatments are required to unmasktarget DNA sequences. Because these vary con-siderably with different fixation and decalcification
Fig. 2.26 Diagrammatic representation of triple colourFISH, a technique used to reduce the probability of false-positive results, utilizing an ABL probe (red), a BCR probe(green) and a probe for the ASS gene (yellow) which isjust proximal to ABL. A normal cell (left) has two greenBCR signals and two fused yellow–red signals representingABL plus ASS; a cell from a patient with t(9;22)(q34;q11)has one normal BCR signal (green) and one normal ASSplus ABL signal (yellow plus red); the translocation hasseparated ASS from ABL so that there is a separate ASSsignal (yellow) and a BCR-ABL fusion signal (red plusgreen). The red–green fusion signal appears yellow.
Fig. 2.27 Diagrammatic representation of demonstrationof an isochromosome by FISH. A normal cell (left) iscompared with a cell from a patient with T-lineageprolymphocytic leukaemia showing an isochromosome of the long arm of chromosome 8. A centromeric probe(red) has been combined with a probe for the MYConcogene (green) which is located on 8q. The normal cell shows two chromosomes, each with a red signal and a green signal. The cell on the right shows, in addition, an isochromosome with two green (MYC) signals oneither side of the centromeric (red) signal.
Fig. 2.28 Diagrammatic representation of the use of FISHto demonstrate chromosomal inversion showing a normalcell (left) and a cell from a patient with M4Eo AML andinv(16)(p13q22). A chromosome paint for the short armof chromosome 16 has been used. In the normal cell thereare two chromosomes, each with a single red signal. In the cell with an inversion there is one normalchromosome (with a single signal) and one abnormalchromosome (with a split signal). The inversion ispericentric and the inverted telomeric part of the shortarm is now fused with the telomeric part of the long arm.

protocols, FISH applied to bone marrow trephinebiopsies is still predominantly a research tool.
It should be noted that ISH techniques to detectmessenger RNA (mRNA) targets can also be appliedto cytological and histological bone marrow prepa-rations. Either enzymes or fluorochromes can beused to identify the target mRNA. Double labellingwith two different fluorochromes is possible, e.g. foreither κ or λ mRNA and for either TNFα or IL-1βmRNA, in order to determine whether neoplasticlight chain-restricted plasma cells are capable ofsynthesizing these cytokines. In diagnostic practice,ISH for the detection of mRNA is useful for de-monstration of κ- or λ-expressing plasma cells (Fig.2.29) and for the detection of viral mRNA, such
as Epstein–Barr early RNA (EBER) in Epstein–Barrvirus (EBV) infection. Otherwise, its present role isin research.
Problems and pitfalls
FISH and other ISH techniques have various disadvantages:1 in any single preparation, it is only possible toidentify the specific abnormality for which relevantprobes are being employed; for example, if cells are being investigated for the presence of t(8;21),other leukaemia-associated translocations such ast(15;17) or t(9;11) will not be detected;2 secondary abnormalities are not recognized; for
80 CHAPTER TWO
Fig. 2.29 In situ hybridizationshowing (a) κ and (b) λ light chainmessenger RNA. There are onlyoccasional κ-positive cells but λ-positive cells are numerous.Paraffin-embedded,immunoperoxidase-labelledprobes ×160.
(a)
(b)

SPECIAL TECHNIQUES 81
example, if the proportion of Philadelphia-positivemetaphases were being evaluated in a case of chronicgranulocytic leukaemia, the presence of an isochro-mosome of 17q (which might be associated withimpending acute transformation) would not bedetected;3 the use of whole chromosome paints does notpermit the detection of rearrangements within asingle chromosome, such as an inversion, or smalldeletions;4 in screening for trisomies and monosomies thereare some false-positive findings, caused by accidentalco-localization of signals, so that a low frequency ofthe abnormality being sought cannot be detectedreliably; and 5 if neoplastic cells are present in the bone marrowbut cannot be aspirated because of associated fibrosis,there will be a failure to detect any relevant cytoge-netic abnormality.
The first two of these disadvantages can be cir-cumvented to some extent by the use of multicolourFISH or spectral karyotyping [21].
Southern blot analysis
In this technique DNA is extracted from a fresh,unfixed tissue sample and digested with a panel of restriction endonucleases. Sometimes, when thebone marrow is cellular, unfixed bone marrowfilms on glass slides may yield sufficient material foranalysis. The restriction endonucleases used areenzymes that recognize specific nucleotide sequencesbetween 4 and 10 base pairs in length and cut theDNA molecule wherever their target sequencesoccur. This results in DNA fragments of variablelength that can be separated, according to their size,by gel electrophoresis. These are then transferred by capillary action onto a more solid nitrocellulosemembrane to create a Southern blot. Fragmentscontaining the DNA sequences of interest can thenbe identified by hybridization with a radiolabelledDNA probe followed by autoradiography. One of themajor breakthroughs that Southern blot analysisallowed was the detection of clonality in B- and T-lymphoid neoplasms (see below). In addition, rear-rangement of a gene arising from translocation orsome other acquired chromosomal rearrangementcan be detected. This technique is used, for example,for detecting rearrangement of the MLL or BCL6 genessince rearrangement can result from a considerable
number of different translocations, not all of whichcan be detected by alternative techniques. TheSouthern blot technique is also applicable for thedetection of translocations in which there is con-siderable heterogeneity of breakpoints precludinguse of a simple PCR technique.
Southern blot analysis can be used to demonstrateclonal integration of HTLV-I proviral DNA and integration of defective HTLV-I in adult T-cellleukaemia/lymphoma [23].
Problems and pitfalls
The major drawbacks of Southern blot analysis as adiagnostic tool are the requirement for radioactivematerials, long turnaround times and the need forrelatively large quantities of DNA in the diagnosticsample, which limits the sensitivity of the method.The latter feature limits its applicability to trephinebiopsy specimens [24].
The polymerase chain reaction
The polymerase chain reaction (PCR) [25,26] is amethod of in vitro amplification of a defined DNAtarget that is flanked by regions of known sequence.The development of this technique has greatlyexpanded the diagnostic potential of moleculargenetics as a result of its ability to generate almostlimitless copies of selected target DNA sequences.The technique is 400–4000 times more sensitivethan Southern blot analysis. It consists of a repeat-ing cycle of three basic steps (denaturation, primerannealing and elongation), with each cycle potenti-ally leading to a doubling of the amount of the targetDNA sequence.
The first step (denaturation) involves heating the DNA sample to around 90°C which causes thedouble-stranded DNA molecule to separate intotwo complementary single strands. The next stage(primer annealing) requires short DNA primersequences that are complementary to the ends ofthe target DNA segment that is to be amplified. Theprimer is added to the denatured single-strandedDNA and the sample is cooled. As cooling occurs,the primers anneal (link via the complementarynucleotide sequences) to the single-stranded targetDNA. The third step (elongation) requires additionof free nucleotides to the ends of the primer DNAsegments, producing complementary copies of each

of the two single-stranded target DNA sequences.This is achieved using a thermostable DNA poly-merase. The strands of DNA thus generated are separated from their complementary strands by ele-vating the temperature again. The cycle is repeatedby elevating and lowering the temperature of thecontainer in which the reaction takes place. Thisprocess is performed in an automated thermalcycling instrument preset with specific temperaturesand times that are optimized for each primer pair.The cycles of denaturing, annealing and elongationare repeated 10–40 times. Amplification is initiallyexponential since each cycle doubles the amount ofDNA template present. In later cycles the rate ofincrease in the quantity of DNA is closer to linearthan to exponential. Nevertheless, very large quan-tities of the target DNA sequence are generated. Thesize of the DNA segment can be estimated by elec-trophoresis, by comparison with known standards(Fig. 2.30). The DNA generated can be directly visualized by staining with ethidium bromide andviewing under UV light. This technique has manyadvantages over Southern blot analysis for diag-nostic use, principally the short turnaround time,the lack of a requirement for radio-isotopes, the ability to amplify very small quantities of targetDNA and its applicability to fixed tissue, including
archival samples and even stained or unstainedblood or bone marrow films scraped off glass slides.Stained slides are, however, less satisfactory thanparaffin-embedded tissue because DNA degradationis greater. Techniques are available for use withdecalcified paraffin-embedded trephine biopsy speci-mens [27]; EDTA decalcification rather than formicacid decalcification is required to ensure that DNA is not degraded. The amplification achieved by PCRmakes the technique very sensitive. The DNA frag-ments produced are suitable for sequencing. Becauseof these advantages PCR, or its modification reversetranscriptase-PCR (RT-PCR), has replaced Southernblot analysis for most diagnostic applications. To distinguish it from RT-PCR, PCR is sometimesreferred to as genomic PCR or DNA-PCR.
In situ PCR is a modification of the PCR techniqueperformed on tissue sections pre-treated with a pro-teinase to facilitate entry of primers [28].
PCR can be used for investigation of clonality (byamplification of IGH or TCR genes), for detection ofrearrangement of genes resulting from acquiredcytogenetic abnormalities and for detection of bac-terial or viral sequences (for example, sequences ofMycobacterium tuberculosis in a bone marrow aspirate).
PCR can be used to demonstrate clonality of lym-phoid cells by amplification of Epstein–Barr virus
82 CHAPTER TWO
Fig. 2.30 Polyacrylamide gelstained with ethidium bromide andvisualized with ultraviolet lightshowing PCR amplification of the643 base pair BRCA1 exon 11A(top panel) and 482 base pairBRCA2 exon 11B (bottom panel).Lane 1 contains size standards andlanes 2–10 contain amplifiedsamples of DNA extracted fromEDTA-decalcified bone marrowtrephine biopsy specimens. (By courtesy of Mrs CarolineWickham, Exeter.)

SPECIAL TECHNIQUES 83
DNA. Because of a variable number of terminalrepeats in the circular episomal forms of the virus a polyclonal lymphoid population with a variety of forms of the virus can be distinguished from amonoclonal population with a single form. This can be useful for establishing clonality of EBV-inducednatural killer cell lymphomas for which there areusually no alternative techniques for demonstratingclonality.
Problems and pitfalls
Great care is required to avoid contamination during PCR analysis as even the smallest quantity of DNA with a sequence complementary to theprimers will be amplified. Meticulous technique isrequired.
Although PCR is applicable to archival material,poor preservation of DNA can lead to negativeresults [24]; amplification of a constitutional gene,for example G6PD, BCR, ABL or the β globin gene,can be used to control for DNA degradation. Pres-ervation of DNA is determined by the fixative usedand the method of processing. Formalin fixationhas been found to give optimal results but otherfixatives, e.g. B5, can be used [24]. As noted above,DNA from archival glass slides is often of inferiorquality.
Negative results can result from sampling errorwhen tissue infiltration is focal.
Variant breakpoints may be missed if appropriateprimers are not used. For example, in testing forBCL2 rearrangement in follicular lymphoma it isnecessary to screen for breakpoints in the minorcluster region (MCR) as well as the major break-point region (MBR).
In some neoplasms, PCR is an insensitive diag-nostic technique to amplify fusion genes because ofthe wide scatter of breakpoints. For example, inmantle cell lymphoma, genomic PCR detects only alittle over 50% of cases, specifically those cases witha chromosome 11 breakpoint in the major transloca-tion cluster [26].
Reverse transcriptase-polymerase chain reaction
PCR is applied to genomic DNA. Because of thepresence of introns, a gene may be very large so that
satisfactory amplification is difficult. This problemcan be circumvented by the use of mRNA as thestarting material since the introns will have beenexcised and the segment to be amplified is shorter.The mRNA must first be transcribed into comple-mentary DNA by means of reverse transcriptase.Amplification can then proceed, as in PCR of genomicDNA. RT-PCR is now very commonly employed forthe detection of leukaemia and lymphoma-relatedfusion genes.
RT-PCR can also be used for the detection of viralmRNA (see Chapter 3).
Modifications of PCR and RT-PCR techniques
Modifications of PCR and RT-PCR techniques(Table 2.8) can increase sensitivity, specificity andusefulness and permit an approximate quantifica-tion of the number of copies of the fusion gene present. Among these modifications is multiplexPCR, in which a number of sets of primers are usedto amplify simultaneously two or three differentfusion genes. This makes it possible, for example, toscreen simultaneously for the three fusion genesfound in the three subtypes of AML associated with a better prognosis: AML1-ETO, PML-RARα andCBFβ-MYH11. The development of various tech-niques for quantification of the amount of targetDNA or mRNA present means that PCR and RT-PCRare now becoming useful for the detection of minimal residual disease and for monitoring theresponse to therapy. One application of quantitativemethods is in monitoring BCR-ABL during interferontherapy or following transplantation for chronicgranulocytic leukaemia. In real-time PCR (RQ-PCR),the PCR technique results in displacement of afluorogenic product-specific probe which is degradedduring the reaction, generating a fluorescent signal.
Problems and pitfalls
RT-PCR requires intact RNA and is therefore not a suitable technique for use with most archivalmaterial. False-negative results can occur if there isdegradation of RNA and amplification of a controlmRNA sequence is therefore advised.
As for genomic PCR, the high sensitivity of thetechnique means that there is a risk of false-positiveresults if contamination is permitted to occur.

Multicentre studies have sometimes shown a highrate of false-positive reactions so that inclusion of anegative control in each assay is considered to becritical [29]. RT-PCR techniques are poorly stan-dardized and quality control is not optimal so thatdifferent laboratories produce divergent results in asignificant proportion of cases [26].
Since RT-PCR uses a small tissue sample negativeresults can occur when infiltration, e.g. of a trephinebiopsy specimen, is focal. Sometimes microscopypermits the detection of infiltration by lymphomawhen results of RT-PCR are negative [24].
It must also be noted that sensitive techniqueshave detected gene rearrangements typical ofleukaemia and lymphoma in people who do nothave an identifiable neoplastic condition. This hasbeen noted for BCR-ABL, NPM-ALK, AF4-MLL andBCL2 rearrangement, characteristic, respectively, ofchronic granulocytic leukaemia, large cell anaplasticlymphoma, acute lymphoblastic/biphenotypic leu-kaemia of infants and follicular lymphoma.
There are also problems in knowing when thedetection of minimal residual disease is clinicallysignificant. Detection of a residual clonal abnormal-ity for a year or more after cessation of treatment issometimes compatible with continued disease-free
survival. This has been noted for AML-ETO, MYH11-CBFβ, E2A-PBX and IGH gene rearrangements[26,30].
Other molecular genetic techniques
Other molecular genetic techniques are rarely usedin routine diagnosis but have research uses. Theyinclude:1 northern blot analysis for investigation of RNA; 2 western blot analysis for investigation of proteinsincluding the ‘oncoproteins’ that are the products offusion genes; 3 comparative genomic hybridization (CGH) todetect segments of chromosomes that are under- orover-represented in leukaemic cells; and 4 DNA sequencing, which is necessary for cloningof new genes.
The application of molecular genetictechniques in the investigation of leukaemiaand lymphoma
Molecular genetic techniques have two principalapplications in the investigation of haematologicalneoplasms. Firstly, they can be used to demonstrate
84 CHAPTER TWO
Table 2.8 Modifications of PCR and RT-PCR techniques.
Modification Principle
Nested PCR A second pair of primers, recognizing sequences internal to thoserecognized by the first pair, increases sensitivity and specificity
Multiplex PCR A number of pairs of primers permit the recognition of two or threeunrelated gene rearrangements in a single procedure
Quantitative PCR The PCR procedure becomes quantitative rather than merely Real-time PCR (RQ-PCR) qualitative, permitting quantification of minimal residual diseaseCompetitive PCRLimiting dilution PCRCo-amplification of target and control genes
Long-range PCR A process in which fragments up to 10 kb are generated, usingmodified polymerases
5’-RACE (rapid amplification of cDNA ends) A technique for the identification of unknown translocationpartners when one partner is well characterized but the other is not
LA-PCR (long and accurate PCR) A technique for the identification of precise translocationbreakpoints using forward primers complementary to RACE-determined gene partners and reverse primers complementary to introns of the known translocation partner

SPECIAL TECHNIQUES 85
that a monoclonal population is present and cangive information on the nature of the lymphoid cellin which a mutation occurred (see below). Secondly,they can be used to demonstrate the presence offusion genes or fusion RNA transcripts that areknown to be associated with specific neoplasms.Demonstration of clonality is mainly done by in-vestigation of IGH or TCR genes, although demon-stration of rearrangement or mutation of any genecould be used as a marker of clonality.
Detecting clonal immunoglobulin and T-cell receptor rearrangements
Clonal populations of B or T lymphocytes can bedetected by demonstrating clonal rearrangementsof IGH or TCR genes using Southern blot analysis orPCR. The basic principle underlying the technique issimilar since TCR and IGH genes are both made upof a number of variable (V), diversity (D) and joining(J) regions, present in germline DNA, which rear-range during lymphocyte development to produce afunctioning gene. During rearrangement, single V,D and J regions are combined with a constant (C)region and simultaneously nucleotides (known asN) are added and removed between the V, D and J regions. This results in a unique DNA sequence ina cell and its progeny. Rearrangement of κ and λgenes is similar but these genes lack a D region.
Using Southern blot analysis, probes that detecteither part of the IGH J region or the TCR β or γchain genes are used to detect clonal rearrange-ments. In polyclonal populations of lymphocytes,there are a large number of different rearrange-ments and no single discrete band can be visualized.In a clonal population, since all the cells share thesame rearrangement, there is a single discrete bandon electrophoresis which is separate from thegermline band.
The technique for detecting clonal rearrange-ments using PCR is somewhat different. Primerswith sequences complementary to segments of theIGH V and J regions that are relatively constant areused to amplify part of the rearranged IGH gene.Differences in the numbers of nucleotides (N)inserted between the V and J regions during re-arrangement result in multiple different sized segments of DNA being amplified in polyclonal populations, so that no discrete band is visualized.
In clonal populations, there is amplification of a single rearranged fragment which appears as a dis-crete band separate from the germline band on electrophoresis. The same principle is used to detect T-cell clones using probes complementary tosequences in the TCR γ and β chains.
Molecular genetic analysis has led to new con-cepts with regard to somatic hypermutation of anti-gen receptor (IGH and TCR) variable region genes inlymphoid cell maturation, with potential relevanceto our understanding of the origins and behaviourof all lymphomas. Knowledge of such mechanismsin T-cell maturation is much less advanced than it isfor the B-cell lineage.
Problems and pitfalls
Although PCR is more sensitive than Southern blot-ting at detecting small clonal populations, it will notdetect all rearrangements. Approximately 80% ofB-cell neoplasms will show clonal rearrangementson PCR using primers for IGH V regions, whereasthe great majority will have a rearrangementdetectable by Southern blot analysis. Hence cautionis required in interpreting negative PCR results. Thelikelihood of detecting IGH gene rearrangement byPCR varies between different types of lymphoma, inone study ranging from around 40% with follicularlymphoma to around 80% with mantle cell andsmall lymphocytic lymphomas [26]. The negativeresults in follicular and certain other lymphomasare consequent on the high rate of somatic muta-tion which is responsible for a failure of consensusprimers to bind to rearranged genes [24].
It should also be noted that rearrangement of IGHand TCR genes is not lineage-specific. Rearrangementof κ or λ light chain genes is much more specific forthe B-lymphocyte lineage than IGH gene rearrange-ment. Inappropriate gene rearrangement is quitefrequently seen in acute lymphoblastic leukaemiaand occurs, although less often, in lymphomas of mature T and B cells. In addition, IGH or TCRgene rearrangements are sometimes found in acutemyeloid leukaemia.
It is likewise important to recognize that, althoughthe detection of a clonal rearrangement usuallyindicates a neoplastic process, clonal IGH and TCRgene rearrangements have been detected in somereactive conditions.

Detection of leukaemia/lymphoma-associatedfusion genes
As discussed earlier, many haematological neo-plasms are associated with a specific non-randomchromosomal abnormality. The genes involved inmany of these rearrangements have been identi-fied, permitting the use of molecular genetic tech-niques for their detection. Some translocations canbe detected by PCR, by employing specific primerswith sequences complementary to segments of DNAthat flank the chromosomal breakpoints. The inter-vening segment across the breakpoint will only beamplified if the translocation is present. However,this technique is only applicable if the breakpointoccurs in a relatively constant position and the fusiongene is not too long. Many more translocations canbe detected by RT-PCR. Translocations that can bedetected by PCR or RT-PCR include t(9;22)(q34;q11)in chronic granulocytic leukaemia and some acutelymphoblastic leukaemias, t(14;18)(q32;q21) in fol-licular lymphoma, t(2;5)(p23;q25) in anaplasticlarge cell lymphoma and various translocations orinversions associated with acute myeloid leukaemiaincluding t(8;21)(q22;q22), t(15;17)(q22;q21) andinv(16)(p13q22).
Advantages of PCR and RT-PCR are that they givea more rapid result than conventional cytogeneticanalysis and do not require viable cells for meta-phase preparations. The highly sensitive nature ofPCR analysis also means that this technique can beused to detect very small numbers of neoplastic cells;consequently, the method can be used for the de-tection of minimal residual disease and early relapse.However, it should be noted that, using these sensitive techniques, fusion genes characteristic of leukaemia or lymphoma are sometimes detectedin normal tissues or tissues showing only reactivechanges. For example, the rearrangement charac-teristic of follicular lymphoma has been detected intonsils removed surgically for reactive conditions.
Problems and pitfalls
Disadvantages, other than the possibility of contam-inating DNA being amplified, include the fact thatnot all rearrangements can be detected. This isbecause of the necessity for a chromosomal abnor-mality to have been fully characterized so that
specific primers for each breakpoint can be designed.It should also be noted that, in contrast to standardcytogenetic analysis, molecular genetic techniquespermit the detection only of those abnormalitiesthat are being specifically sought. Nevertheless,many chromosomal rearrangements can be detectedby PCR and RT-PCR and some such rearrangementsare sufficiently common that these techniques arevery practical for the rapid and precise categoriza-tion of cases of acute leukaemia and for confirmingthe diagnosis of certain categories of lymphoma.
Ultrastructural examination
Ultrastructural examination, in which the structureof cells is studied by electron microscopy, can beapplied to peripheral blood and bone marrow but islittle used in routine diagnostic haematology. Theadvances in immunophenotyping have renderedelectron microscopy redundant in identifying M0and M7 AML. It remains of some use in identifyingsmall Sézary cells (Fig. 2.31) and in making a precisediagnosis in congenital dyserythropoietic anaemia.
Ultrastructural examination can also be appliedto trephine biopsy specimens but it is rarely neces-sary for diagnosis. It can be used for the detection of Birbeck granules for confirming the diagnosis of Langerhans cell histiocytosis but immunohisto-chemistry, including the application of a CD1amonoclonal antibody, is an alternative more readilyavailable technique that can be used for this purpose.
Bone marrow culture for assessment ofhaemopoietic progenitor cell numbers
Short- and long-term culture techniques for haemo-poietic cells have found extensive use in researchbut have only limited roles in the diagnostic assess-ment of bone marrow disorders.
Short-term culture
The major current use of short-term culture in clin-ical practice is for assessment of harvested bonemarrow or peripheral blood stem cells prior to theiruse for engraftment.
Short-term haemopoietic cultures are performedusing cells suspended at a known starting concen-tration in methyl cellulose or agar supplemented
86 CHAPTER TWO

SPECIAL TECHNIQUES 87
with culture medium, fetal bovine serum andgrowth-promoting substances such as granulocyte–macrophage colony-stimulating factor (GM-CSF),erythropoietin and thrombopoietin. They are thenincubated at 37°C for 14 days, in a humidifiedatmosphere containing 5% CO2. Depending uponthe precise conditions of the assay, multipotentialcells in the patient’s (or donor’s) sample will formcolonies containing variable proportions of differ-entiating cells of various haemopoietic lineages. Thestarting cells are seeded at a sufficiently low con-centration that individual colonies localized aroundeach single multipotential parent cell can be visual-ized separately from any neighbouring colonies.The colonies can then be counted at low powermagnification by standard light microscopy.
The most primitive multipotential cell type usu-ally assayed in such a culture system is the mixedcolony-forming unit (CFU-mix), which can gener-ate erythroid bursts and colonies of granulocyticand monocytic cells. More commonly, however,GM-CSF, in the absence of other added growth factors, is used to supplement the culture mediumand these conditions permit growth of mixed
granulocyte and monocyte colonies without anyerythroid growth. This culture system constitutesthe granulocyte–monocyte colony-forming unit(CFU-GM) assay and is the usual assay ofhaemopoietic cell growth potential in harvestedmarrow or mobilized peripheral blood stem cell collections prior to transplantation. Colony numbercorrelates only loosely with CD34-positive cellcounts in such collections. The CFU-GM providesan independent predictor of engraftment.
Occasionally, the erythropoietic potential ofprimitive haemopoietic cells requires assessment.This is done using the erythroid burst-forming unit(BFU-E) assay, in which erythropoietin is used tosupplement the culture medium in the absence of granulocyte and monocyte growth-promotingfactors. Primitive erythroid cells produce multiple,rather than single colonies, radiating as a so-called‘burst’ around the progenitor cell (BFU-E), witheach individual colony representing the offspring ofa more mature erythroid precursor, the erythroidcolony-forming unit (CFU-E). Erythroid coloniesare readily seen by light microscopy because of theorange–red colour of their cytoplasmic haemoglobin.
Fig. 2.31 Ultrastructuralexamination in Sézary syndromeshowing a Sézary cell with a highlyirregular nuclear outline. (Bycourtesy of Dr Estella Matutes,London.)

Apart from the use of culture systems as assays forpredicting haemopoietic function in transplantation,spontaneous colony formation (i.e. colony forma-tion with no growth factor supplementation) is usedby some laboratories to assist in diagnosing chronicmyeloproliferative disorders. Spontaneous mega-karyocyte colony-forming unit (CFU-Meg) activity,spontaneous BFU-E activity, or both, is demon-strable in peripheral blood or bone marrow cells frommany patients with essential thrombocythaemia.Spontaneous BFU-E also form from peripheralblood and bone marrow cells of patients with poly-cythaemia rubra vera. Blood or marrow cells fromnormal individuals and patients with reactive throm-bocytosis or secondary polycythaemia do not usu-ally show spontaneous BFU-E activity. However,they may occasionally give rise to CFU-Meg. Thispotential for false-positive results and a relativelyhigh false-negative rate in true cases of essentialthrombocythaemia and polycythaemia rubra vera,together with the cumbersome nature of the assays,have limited the diagnostic application of short-term colony-forming assays.
Long-term culture
Long-term cultures, in which haemopoietic precur-sor cells are seeded onto layers of pre-grown mar-row stroma, can potentially assess the activity ofstem cells even more primitive than those whichsurvive in short-term cultures. Assay of seeded cellsis achieved, once they have adhered to the stroma,by replacing liquid medium with methylcellulose oragar-containing semi-solid medium and assessingcolony formation as above. This system is known asthe long-term culture-initiating cell (LTC-IC) assay.It is mainly employed in research, despite its pos-sible value in predicting engraftment. Long-termcultures have also been used for ex vivo purging andexpansion of haemopoietic cells for engraftmentbut these approaches have yet to find widespreadclinical application.
Bone marrow culture for micro-organisms
Bone marrow culture for micro-organisms, forexample mycobacteria, Leishmania donovani or His-
toplasma capsulatum, can be of use in diagnosis andwill be discussed in the next chapter.
References
1 Rath CE and Finch CA (1948) Sternal marrowhemosiderin; a method for determining available ironstores in man. J Lab Clin Med, 33, 81–86.
2 Gale E, Torrance J and Bothwell T (1963) The quanti-tative estimation of total iron stores in human bonemarrow. J Clin Invest, 42, 1076–1082.
3 Lundin P, Persson E and Weinfeld A (1964) Com-parison of hemosiderin estimation in bone marrowsections and bone marrow smears. Acta Med Scand, 175,383–390.
4 Fong TP, Okafor LA, Thomas W and Westerman MP(1977) Stainable iron in aspirated and needle-biopsyspecimens. Am J Hematol, 2, 47–51.
5 Douglas AS and Dacie JV (1953) The incidence andsignificance of iron-containing granules in human erythrocytes and their precursors. J Clin Pathol, 6,307–313.
6 Bainton DF and Finch CA (1964) The diagnosis of irondeficiency anemia. Am J Med, 37, 62–70.
7 Hansen HA and Weinfeld A (1965) Hemosiderin estimations and sideroblast counts in the differentialdiagnosis of iron deficiency and other anemias. ActaMed Scand, 165, 333–356.
8 Wulfhekel U and Düllman J (1999) Storage iron inbone marrow plasma cells. Acta Haematol, 101, 7–15.
9 Hayhoe FGJ and Quaglino D. Haematological Cytochem-istry, 2nd edn. Churchill Livingstone, Edinburgh, 1988.
10 Bain BJ. Leukaemia Diagnosis, 2nd edn. BlackwellScience, Oxford, 1999.
11 Krause JR, Brubaker D and Kaplan S (1979) Com-parisons of stainable iron in aspirated and needlebiopsy specimens of bone marrow. Am J Clin Pathol, 72,68–70.
12 Bauermeister DE (1971) Quantification of bone mar-row reticulinaa normal range. Am J Clin Pathol, 56,24–31.
13 Bain BJ. Interactive Haematology Imagebank. BlackwellScience, Oxford, 1999.
14 Gratama JW, Bolhuis RLH and Van‘t Veer MB (1999)Quality control of flow cytometric immunophenotyp-ing of haematological malignancies. Clin Lab Haematol,21, 155–160.
15 Matutes E, Bain BJ, Reilly J, Barnett D and Linch D(2000) Revised guideline on immunophenotyping in acute leukaemias and chronic lymphoproliferativedisorders, in press.
16 Kallakury BVS, Hartmann D-P, Cossman J, Gooten-berg JE and Bagg A (1999) Posttherapy surveillance ofB-cell precursor acute lymphoblastic leukemia: value
88 CHAPTER TWO

SPECIAL TECHNIQUES 89
of polymerase chain reaction and limitations of flowcytometry. Am J Clin Pathol, 111, 759–766.
17 Pileri SA, Ascano S, Milani M, Visani G, Piccioli M,Orcioni CF et al. (1999) Acute leukaemia immunophe-notyping in bone-marrow routine sections. Br JHaematol, 105, 394–401.
18 Sadahira Y, Kanzaki A, Wada H and Yawata Y (1999)Immunohistochemical identification of erythroid pre-cursors in paraffin embedded bone marrow biopsy sections: spectrin is a superior marker to glycophorin. JClin Pathol, 52, 919–921.
19 Janckila AJ, Walton SP and Yam LT (1998) Speciesspecificity of monoclonal antibodies to human tartrate-resistant acid phosphatase. Biotech Histochem, 73, 316–324.
20 Fonatsch C and Streubel B. Classical and molecularcytogenetics. In: Huhn D (ed) New Diagnostic Methods inOncology and Hematology. Springer, Berlin, 1998.
21 Kearney L (1999) The impact of the new FISH tech-nologies on the cytogenetics of haematological malig-nancies. Br J Haematol, 104, 648–658.
22 Fletcher JA (1999) DNA in situ hybridization as anadjunct to tumor diagnosis. Am J Clin Pathol, 112(Suppl. 1), S11–S18.
23 Tsukasaki K, Imaizumi Y, Tawara M, Fujimoto T,Fukushima T, Hata T et al. (1999) Diversity of leukaemiccell morphology in ATL correlates with prognostic factors, aberrant immunophenotype and defectiveHTLV-1 genotype. Br J Haematol, 105, 369–375.
24 Pittaluga S, Tierens A, Dodoo YL, Delabie J and de
Wolf-Peeters C (1999) How reliable is histologic ex-amination of bone marrow trephine biopsy specimensfor the staging of non-Hodgkin lymphoma? A study of hairy cell leukemia and mantle cell lymphoma in-volvement of the bone marrow trephine specimen byhistologic, immunohistochemical, and polymerase chainreaction techniques. Am J Clin Pathol, 111, 179–184.
25 Neubauer A, Thiede C and Nagel S. Molecular biology.In: Huhn D (ed) New Diagnostic Methods in Oncology andHematology. Springer, Berlin, 1998.
26 Bagg A and Kallakury BVS (1999) Molecular pathol-ogy of leukemia and lymphoma. Am J Clin Pathol, 112(Suppl. 1), S76–S92.
27 Wickham CI, Boyce M, Joyner MV, Sarsfield P,Wilkins BS, Jones DB and Ellard S (2000) Amplifica-tion of PCR products in excess of 600 base pairs usingDNA extracted from decalcified, paraffin wax embed-ded bone marrow trephine biopsies. J Clin Pathol MolPathol, 53, 19–23.
28 Evans PAS and Morgan GJ (1999) Molecular diag-nostics in haemato-oncology. CME Bull Haematol, 2,94–99.
29 Yee K, Anglin P and Keating A (1999) Molecularapproaches to the detection and monitoring of chronicmyeloid leukemia: theory and practice. Blood Rev, 13,105–126.
30 Foroni L, Harrison CJ, Hoffbrand AV and Potter MN(1999) Investigation of minimal residual disease inchildhood and adult acute lymphoblastic leukaemia bymolecular analysis. Br J Haematol, 105, 7–24.