
South Asian Clinical Toxicology Research Collaboration Paraquat Poisoning Lessons from a Large...
39
South Asian Clinical Toxicology Research Collabor Paraquat Poisoning Lessons from a Large Cohort Indika Gawarammana (MD, FRCPE, PhD) Department of Medicine and South Asian Clinical Toxicology Research Collaboration Faculty of Medicine- University of Peradeniya Sri Lanka
-
Upload
nathan-mckenzie -
Category
Documents
-
view
224 -
download
3
Transcript of South Asian Clinical Toxicology Research Collaboration Paraquat Poisoning Lessons from a Large...
South Asian Clinical Toxicology Research Collaboration
Paraquat PoisoningLessons from a Large
Cohort
Indika Gawarammana(MD, FRCPE, PhD)
Department of Medicine and South Asian Clinical Toxicology Research Collaboration
Faculty of Medicine- University of Peradeniya
Sri Lanka

South Asian Clinical Toxicology Research Collaboration
Paraquat- history First described in 1882 Electron donation to PQ forms a stable PQ.+
Used as an oxidation-reduction indicator Introduced as a herbicide in 1962
South Asian Clinical Toxicology Research Collaboration
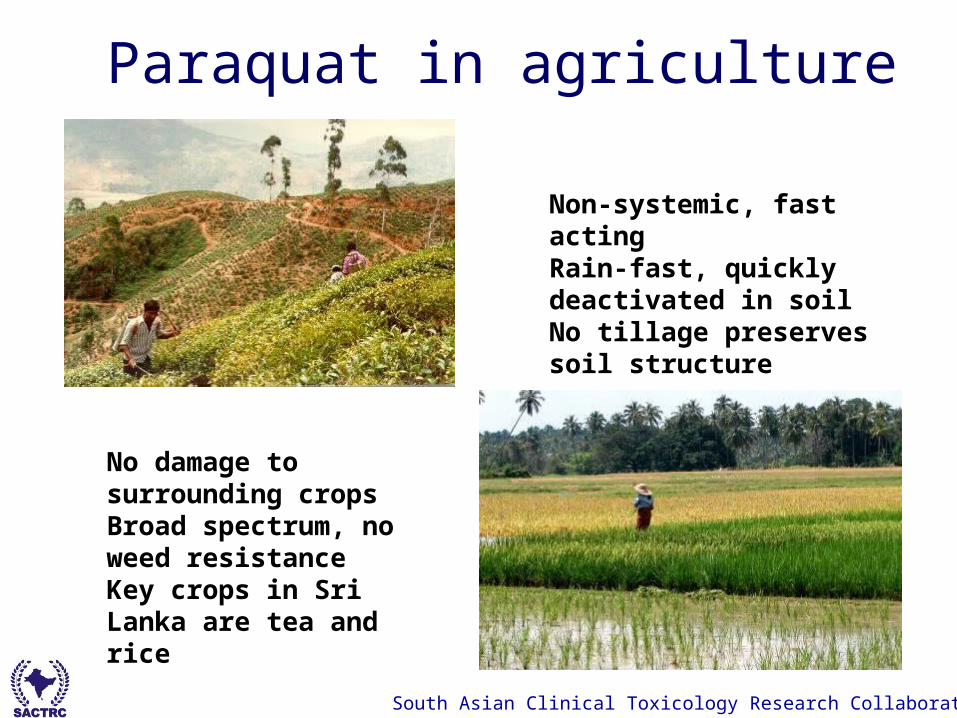
Paraquat in agriculture
Non-systemic, fast acting Rain-fast, quickly
deactivated in soil No tillage preserves soil
structure
No damage to surrounding crops
Broad spectrum, no weed resistance
Key crops in Sri Lanka are tea and rice

South Asian Clinical Toxicology Research Collaboration
Paraquatproportion of death
So
Carbamates6%
Other Her-bicides
14%
Paraquat35%
Dimethoate20%
Fenthion4%
Chlorpyrifos14%
Other OP6% Carbamates
Other Herbicides
Paraquat
Dimethoate
Fenthion
Chlorpyrifos
Other OP

South Asian Clinical Toxicology Research Collaboration
Generates free radicalsActivation of NFkB
NFkB is translocated into the nucleus, binds to promoter regionsinduces target genes involved in inflammation
South Asian Clinical Toxicology Research Collaboration
N+
N+
CH3CH3 C NN+
CH3CH3
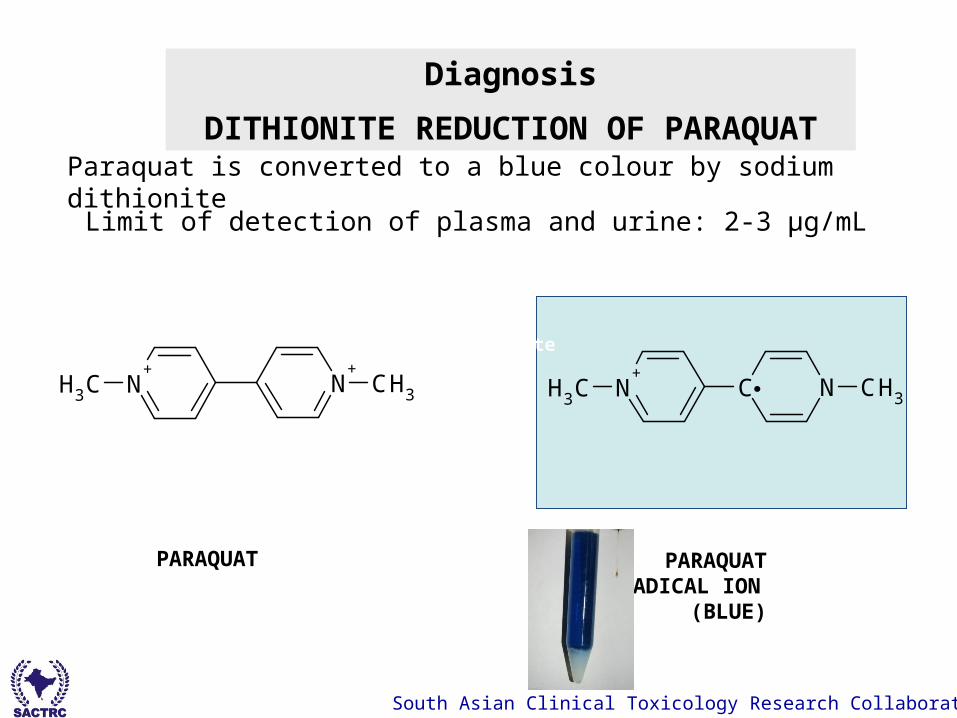
Diagnosis
DITHIONITE REDUCTION OF PARAQUAT
Sodium
dithionite
alkali
PARAQUAT PARAQUAT RADICAL ION
(BLUE)
Paraquat is converted to a blue colour by sodium dithionite
Limit of detection of plasma and urine: 2-3 µg/mL
South Asian Clinical Toxicology Research Collaboration
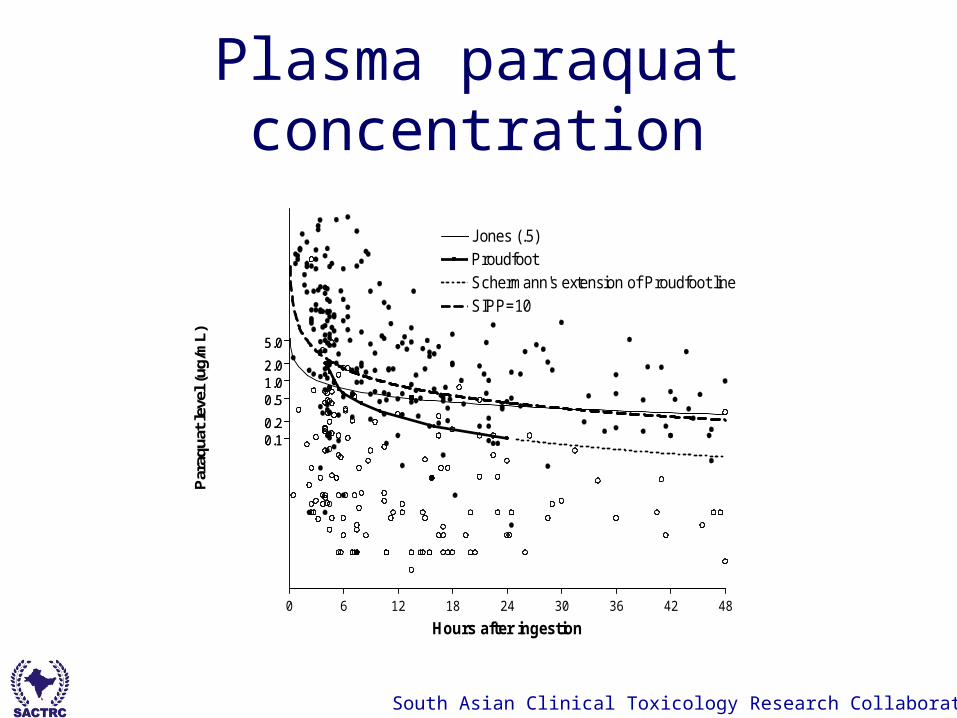
Plasma paraquat concentration
0.10.2
0.51.02.0
5.0
0 6 12 18 24 30 36 42 48
0.10.2
0.51.02.0
5.0
ProudfootSchermann's extension of Proudfoot line
Jones (.5)
SIPP=10
Hours after ingestion
Par
aqua
t le
vel (
ug/m
L)

South Asian Clinical Toxicology Research Collaboration
symptoms Nausea and vomiting in 81.6% Burning oral pain in 62.5% Odynophagia 30% Abdominal pain in 57.5% Low GCS is uncommon (8%)- but all recover
within hours

South Asian Clinical Toxicology Research Collaboration
“Paraquat Tongue”
South Asian Clinical Toxicology Research Collaboration
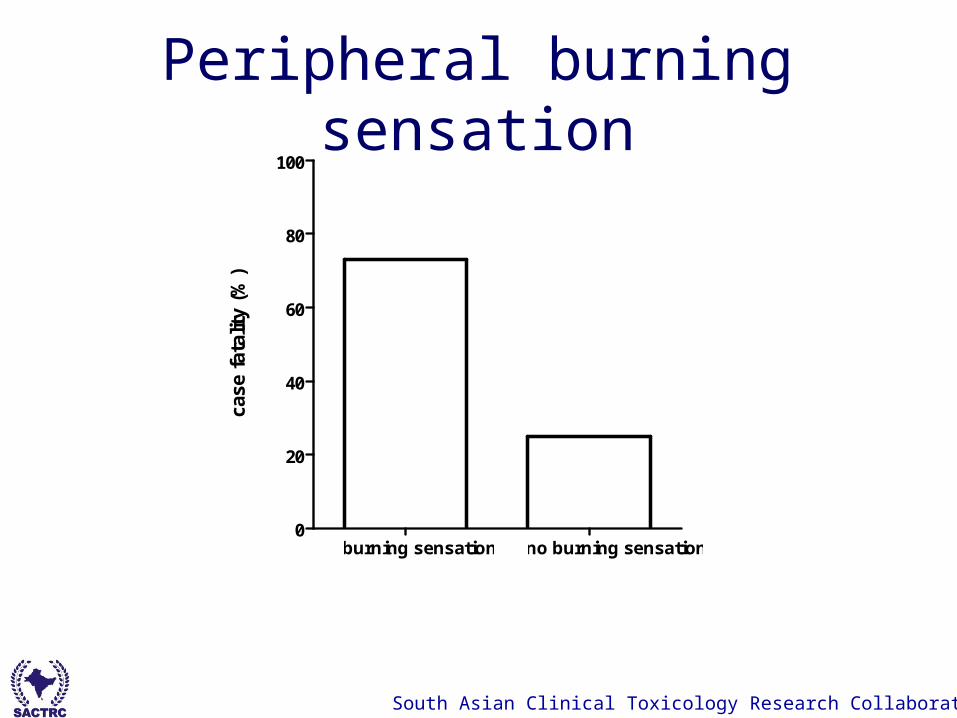
Peripheral burning sensation
burning sensation no burning sensation0
20
40
60
80
100
case
fat
alit
y (%
)
73%- median time to death36 hrs
25%- median time to death50hrs

South Asian Clinical Toxicology Research Collaboration
Proportion of deaths- volume of ingestion
Log Rank (Chi square 79.69, p<0.0001)
0 5 10 15 20 25 300.0
0.5
1.0
5-15 mls
15-50mls
>50mls
time since ingestion (days)
Pro
po
rtio
n d
ecea
sed

South Asian Clinical Toxicology Research Collaboration
Case fatality– 73.9% (95% CI 69-78).
Median time to death– 1.53 days (IQR 0.5-3.7).

South Asian Clinical Toxicology Research Collaboration
Clinical course Severe toxicity = rapid death from MOF Others= slow death over days due to hypoxia

South Asian Clinical Toxicology Research Collaboration
Respiratory rate
survivors
South Asian Clinical Toxicology Research Collaboration
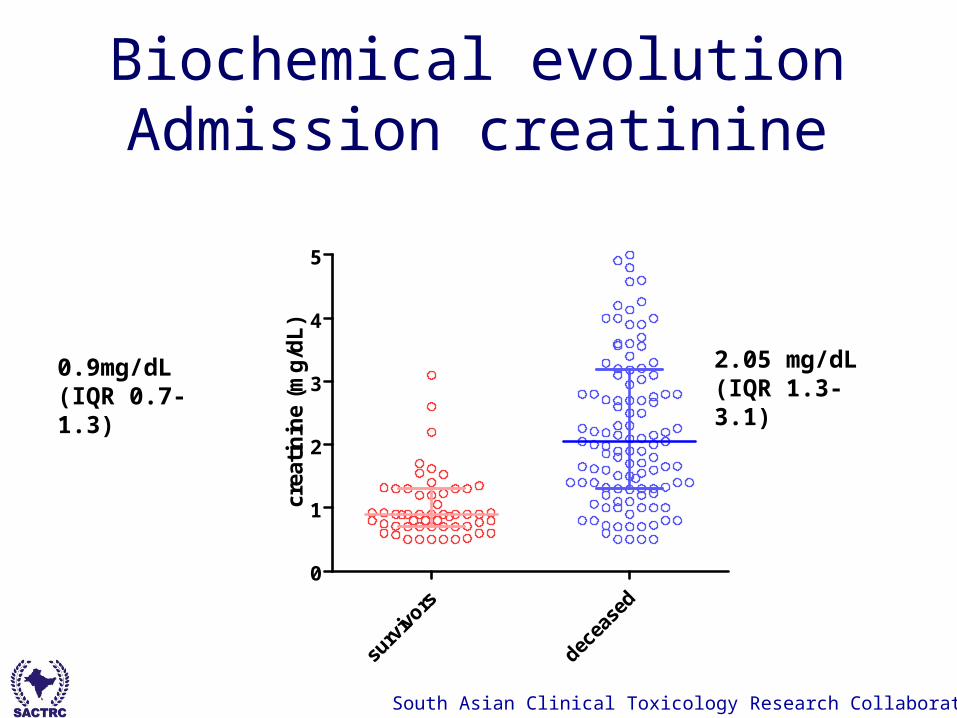
Biochemical evolutionAdmission creatinine
surv
ivors
decea
sed
0
1
2
3
4
5
crea
tin
ine
(mg
/dL
)
2.05 mg/dL (IQR 1.3-3.1)
0.9mg/dL (IQR 0.7-1.3)

South Asian Clinical Toxicology Research Collaboration
EvolutionSurvivors
0 1 2 3 4 50
2
4
6
8
10
Normal range
mean
days since ingestion
creatin
ine (m
g/d
L)
Deaths
0 1 2 3 4 50
2
4
6
8
10
Normal range
mean
days since ingestion
creatin
ine (m
g/d
L)

South Asian Clinical Toxicology Research Collaboration
Admission WBC
0
10000
20000
30000
wh
ite
cell
cou
nt/
cmm

South Asian Clinical Toxicology Research Collaboration
>19550 <195500
20
40
60
80
100
case
fat
alit
y (%
)
OR 81, 95% CI 67-84
South Asian Clinical Toxicology Research Collaboration
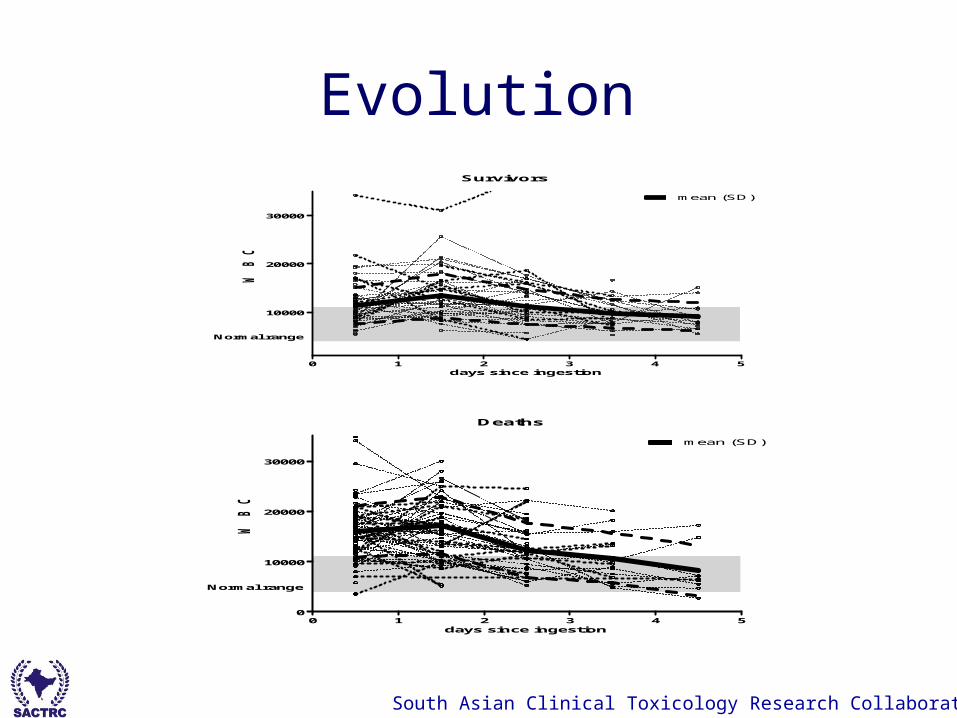
EvolutionSurvivors
0 1 2 3 4 5
10000
20000
30000
Normal range
mean (SD)
days since ingestion
WB
C
Deaths
0 1 2 3 4 50
10000
20000
30000
Normal range
mean (SD)
days since ingestion
WB
C
South Asian Clinical Toxicology Research Collaboration
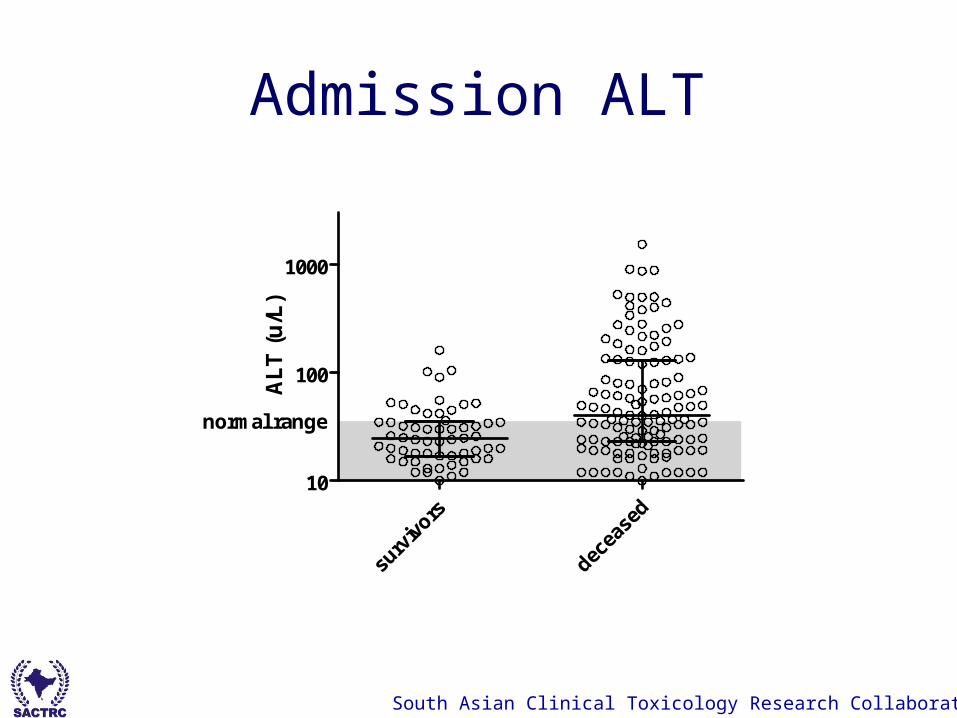
Admission ALT
10
100
1000
normal range
AL
T (
u/L
)

South Asian Clinical Toxicology Research Collaboration
EvolutionSurvivors
0 1 2 3 4 50
500
1000
Normal range
mean (SD)
days since ingestion
AS
T (U
/L
)
Deaths
0 1 2 3 4 50
500
1000
Normal range
mean (SD)
days since ingestion
AS
T (U
/L
)

South Asian Clinical Toxicology Research Collaboration
Treatment Supportive care N acetylcysteine, DFO, Vitamin E Immunosuppression

South Asian Clinical Toxicology Research Collaboration
haemodialysis and haemoperfusion
lung
plasma
tissue

South Asian Clinical Toxicology Research Collaboration
Immunosuppressionpopular
Inconclusive evidence
(Eddleston M et al QJM. 2003 and Agarwal et al Singapore Med J. 2007)
South Asian Clinical Toxicology Research Collaboration Faculty of Medicine, University of Peradeniya

South Asian Clinical Toxicology Research Collaboration
RCT in Sri Lanka
Chi squared 0.74, p=0.34
0 10 20 30 40 50 60 70 80 900.0
0.5
1.0
Immunosuppression groupPlacebo group
Days post-ingestion
Fra
ctio
n s
urv
ival

South Asian Clinical Toxicology Research Collaboration
ROC curves
Area under the curve
1= perfect test

Assessment of prognosisAdmission plasma paraquat concentration
0 20 40 60 80 1000
20
40
60
80
100
AUC=0.95
100% - Specificity%
Sen
siti
vity
(%
)
0 20 40 60 80 1000
20
40
60
80
100
AUC= 0.96
100% - Specificity%
Sen
siti
vity
(%
)
Plasma paraquat SIPP score

South Asian Clinical Toxicology Research Collaboration
Number Number and % deaths
Positive test 418 251 (60%)
Negative test 149 7 (4.7%)
Semi-quantitativeUrine dithionite test

South Asian Clinical Toxicology Research Collaboration
Negative test= survival Sensitivity of 0.97 (95% CI 0.94-.98) Specificity of 0.45 (95% CI 0.4-0.5) Negative predictive value of 0.95 (95% CI
0.90-0.98)
Easy to perform, cheap Negative tests= survival Positive tests: need further evaluation

South Asian Clinical Toxicology Research Collaboration
Admission creatinine>1.26mg/dL
Sensitivity of 78% (95% CI: 69-85), specificity of 73% (95% CI: 59-84) [positive likelihood ratio 2.91]
0 20 40 60 80 1000
20
40
60
80
100
AUC=0.82
100% - Specificity%
sen
siti
vity

South Asian Clinical Toxicology Research Collaboration
Creatinine >2.64mg/dL
(OR 16.7, 95% CI: 3.8-72, specificity: 0.96 (95% CI 0.87-0.99),
PPV 0.95 (95% CI 0.85-0.99, p<0.001).
>2.635mg/dL <2.635mg/dL0
20
40
60
80
100
case
fat
alit
y (%
)
South Asian Clinical Toxicology Research Collaboration
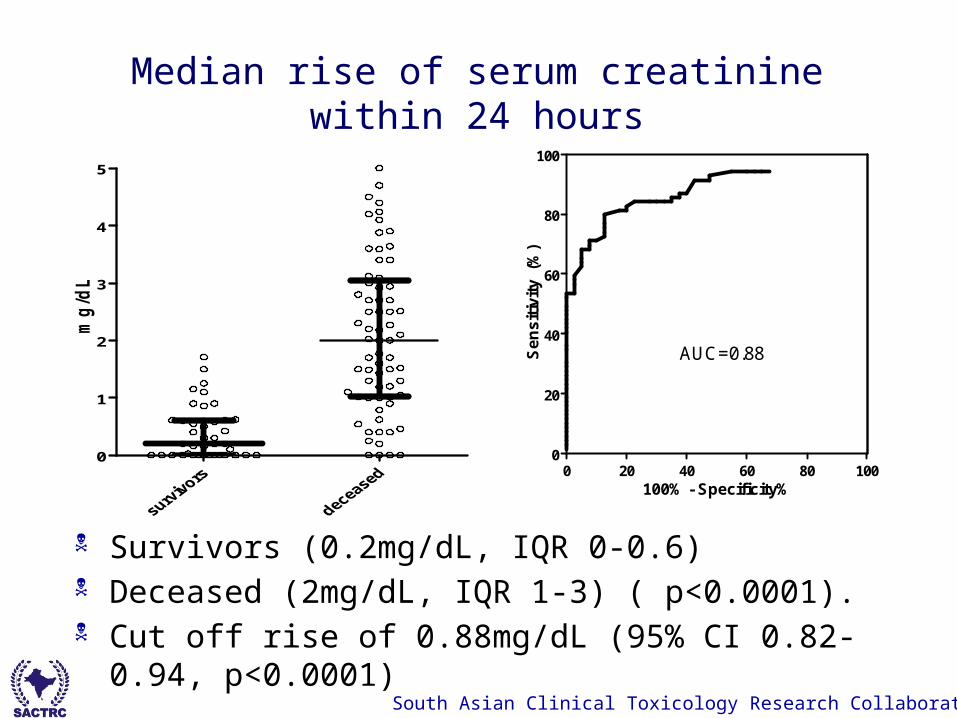
Median rise of serum creatinine within 24 hours
Survivors (0.2mg/dL, IQR 0-0.6) Deceased (2mg/dL, IQR 1-3) ( p<0.0001). Cut off rise of 0.88mg/dL (95% CI 0.82-0.94, p<0.0001)
0
1
2
3
4
5
mg
/dL
0 20 40 60 80 1000
20
40
60
80
100
AUC=0.88
100% - Specificity%
Se
ns
itiv
ity
(%
)
South Asian Clinical Toxicology Research Collaboration
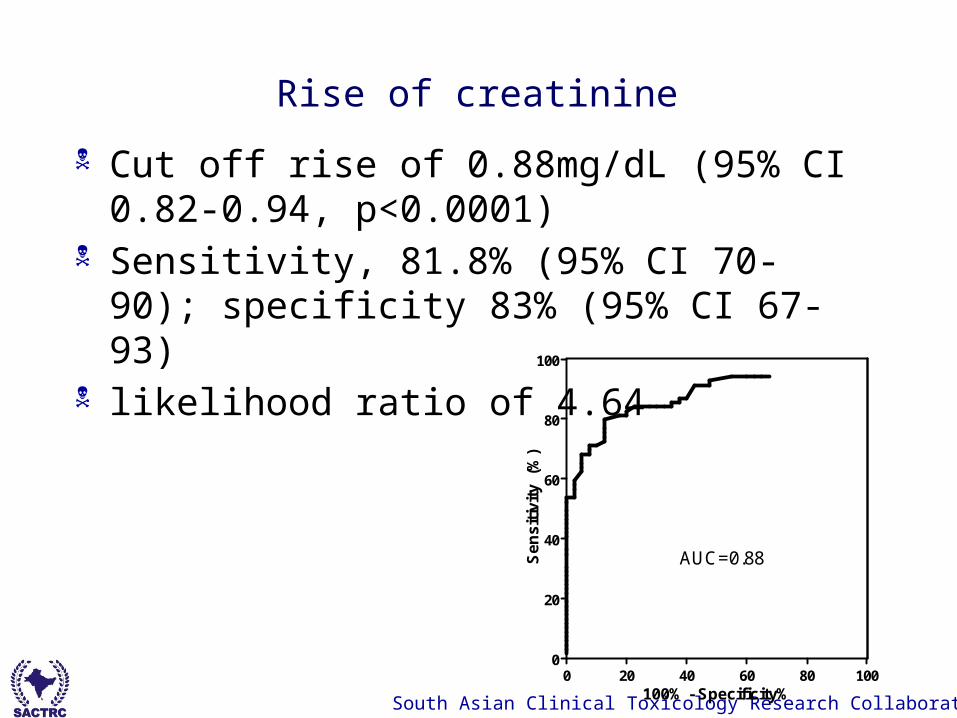
Rise of creatinine
Cut off rise of 0.88mg/dL (95% CI 0.82-0.94, p<0.0001)
Sensitivity, 81.8% (95% CI 70-90); specificity 83% (95% CI 67-93)
likelihood ratio of 4.64
0 20 40 60 80 1000
20
40
60
80
100
AUC=0.88
100% - Specificity%
Se
ns
itiv
ity
(%
)

South Asian Clinical Toxicology Research Collaboration
summary Survivors and non
survivors can be identified early
Immunosuppression does not work
Prevent access to paraquat as outcome is poor
South Asian Clinical Toxicology Research Collaboration
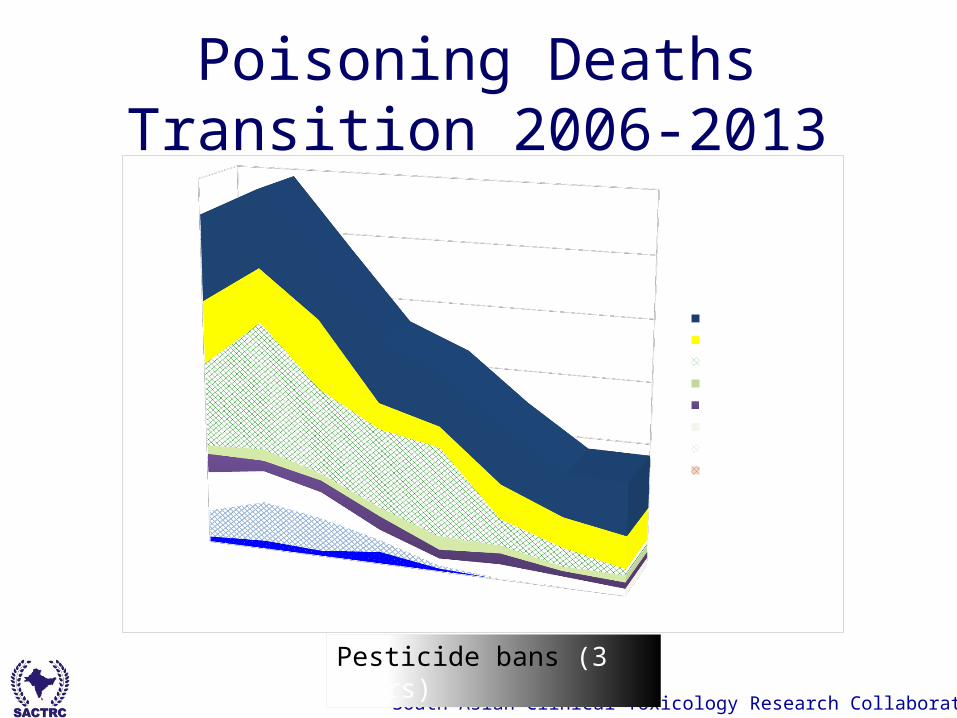
Poisoning Deaths Transition 2006-2013
20062007
20082009
20102011
20122013
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
Non Ag deathsOther PesitcidesParaquatGlyphosateCarbamatesChlorpyrifosDimethoateFenthione
Pesticide bans (3 years)

South Asian Clinical Toxicology Research Collaboration
AcknowledgementsAndrew Dawson, Nick Buckley,
Michael Eddleston,
SACTRC collaborators, research team and hospital staff
University of PeradeniyaWellcome Trust & NHMRC
Syngenta
Michael Eddleston1,2,3*, Peter Eyer4, Franz Worek5, Edmund Juszczak6, Nicola Alder6, FahimMohamed2,3, Lalith Senarathna2,3, Ariyasena Hittarage7, Shifa Azher8, K. Jeganathan7,
ShalukaJayamanne8, Ludwig von Meyer9, Andrew H. Dawson3,10, Mohamed Hussain Rezvi Sheriff2,3,
Nick A.Buckley3, We thank the Directors and the medical and nursing staff of the study
hospitals for their help and support; Stuart Allen for programming; theIDMC and Professor Doug Altman for advice; Renate Heilmair, BodoPfeiffer, and Elisabeth Topoll for technical assistance; J. V. Peter for
information on the Vellore RCTs; and Allister Vale and Nick Bateman forcritical review.
Ox-Col Poisoning Study Collaborators: Darren Roberts, DamithePitahawatte, Asanga Dissanayaka, Nalinda Deshapriya, Ruwan Seneviratne,
Sandima Gunatilake, Indika Weerasinghe, Thushara Diunugala,Sriyantha Adikari, Suwini Karunaratne, Prabath Piyasena, Senarath
Angammana, Deepal Inguruwatte, Samithe Egodage, Mathisha Dissanayake,Waruna Wijeyasiri-wardene, Shammi Rajapakshe, Sidath Yawasinghe,
Bandara, Sumith Kumara, Thushita Kumara, NilumdimaWijekoon, Kusal Wijeweera, Himali Sepalika Sudusinghe, Hasantha
Ranganath, Mahi Wickramagamage, R. U. Wijesinghe, S. M. I.Senavirathne, Chinthaka De Silva, Chaminda Manamperi, T. Suhitharan,Sevana-yagam David, D. Y. Mohamed Mahir, Lakshmi Sriskandarajah,
Sellakkuddy Selva-ganesh, Chamila Bandara Herath, Kanchana Liyanage,Chinthaka Semasinghe, Pandula Illangasinghe, Gayan Wickramasinghe,Sudesh Rathnayake, Vindhya Jayasinghe, Iranga Jayasundara, Mahesh
Dahanayake, Prasanna Weerakoon, Praba W. Nanayakkara, ParamananthanSajeevan, Vethanathan Bavanthan, Janitha Kumari Illangakoon,
Chamantha Dilmini Karunarathne, Kuleesha Kodisinghe, BuddikaJeevantha Wimalarathne, Asela Udagedara, Ashoka Subasinghe, Kiloshini
Samanthi Hendawitharana, Dammika Prabath Nungamugedara, ArunaWijayanayaka, Sanjeewa Amarasinghe, Sakunthala Nilmini Liyanage,
Indika de Alwis, Thushara Priyawansha, Chathura Pallangasinghe, ShukryZawahir, Mohamed Ashrafdeen Isnan, and Syed Shahmy
Independent Data Monitoring Committee (IDMC): ProfessorMike Clarke (Director, UK Cochrane Centre, Oxford; Chair); ProfessorKeith Hawton (Department of Psychiatry, Oxford); Dr. Julian Higgins
(MRC Biostatistics Unit, Cambridge University; statistician); ProfessorSaroj Jayasinghe (Department of Clinical Medicine, Colombo, Sri Lanka);
Professor Nimal Senanayake (Department of Clinical Medicine, Peradeniya,Sri Lanka); Professor Kris Weerasuriya (WHO/SEARO, New Delhi).- Michael Eddleston, Edmund
Juszczak, Nick A Buckley, Lalith Senarathna, Fahim Mohamed, Wasantha Dissanayake, Ariyasena Hittarage,
Shifa Azher, K Jeganathan, Shaluka Jayamanne, M H Rezvi Sheriff , David A Warrell, We thank Palitha Abeykoon and Kan Tun (WHO), Lakshman Karalliedde,
D G S Alahakoon, and W M T B Wijekoon, and the Directors, medicaland nursing staff of the study hospitals for their help and support, the
IDMEC, Robin Ferner, and Doug Altman for advice, Geoff Isbister,Simon Thomas, Lewis Nelson, and Nick Bateman for critical review, Ly-
Mee Yu and Nicola Alder for statistical support, Shukry Zawahir, andChathura Palagasinghe for help with the fi nal patient audit; and the
Ox-Col study doctors for their work in the face of many pressures. ME is aWellcome Trust Career Development Fellow; this work was funded by
grant 063560 from the Wellcome Trust’s Tropical Interest Group to ME.The South Asian Clinical Toxicology Research Collaboration is funded by
a Wellcome Trust/National Health and Medical Research CouncilInternational Collaborative Research Grant 071669.
Ox-Col poisoning study collaboratorsDarren Roberts, Asanka Perera, Manjula Rajapakshe, K Reginald,
Sapumal Haggalla, Samantha Wijesundara, Jaya Ratnayake,S M T Bandara, Subashini Kumarasinghe, Manjula Weerakoon,
Ayanthi Karunaratne, Manonath Marasinghe, Ruwan Kumara,Sumedha Kumara, Nilan Suranga, Jamal Dean, Dharshana Fernando,
Sagara Kumara, Koshitha Gunarathne, R M Senanayake, Najeeb Khan,Kalum Dhammika, Anuradhi Weerasinghe, M S F Zanoona,
Samanmali Edirisinghe, Medhangi Karunaratne, Sampath Attapattu,Upul Hendalage, Indika Wanasinghe, Lal Bogahawattage,
SyngentaR D S M Peiris, S M Dayarathne, Gayan Costa, Chandana de Silva,Prabath Abeyrathna, Bandula Senadeera, Gayan Gunarathne,
Kusal Wijayaweera, M Senthilkumaran, Y Ruthra, K Sutharshan,Dimuth de Silva, Anjana Amarasinghe, Janaka Balasooriya,
Damithe Pitahawatte, Asangha Dissanayaka, Aravinda Perera,Nalinda Deshapriya, Suranga Gurusinghe, Ruwan Seneviratne,Saman Chandana; Mubashi Mohamed, Koshala Abeysundera,
Nasmiyar Mubarak, Lumbini de Silva, Daniel, Sandima Gunatilake,Indika Weerasinghe, Thushara Diunugala, Sriyantha Adikari,
Suwini Karunaratne, Prabath Piyasena, Senarath Angammana,Deepal Inguruwatte, Samithe Egodage, Mathisha Dissanayake,
Waruna Wijeyasiriwardene, Shammi Rajapakshe, Sidath Yawasinghe,Samanthi Bandara, Sumith Kumara, Thushita Kumara,
Nilumdima Wijekoon.Independent data monitoring and ethics committee
Mike Clarke (Director, UK Cochrane Centre, Oxford; Chair);Keith Hawton (Department of Psychiatry, Oxford); Julian Higgins (MRCBiostatistics Unit, Cambridge University; Statistician); Saroj Jayasinghe
(Department of Clinical Medicine, Colombo); Nimal Senanayake(Department of Clinical Medicine, Peradeniya); Kris Weerasuriya
(WHO/SEARO, New Delhi).
South Asian Clinical Toxicology Research Collaboration
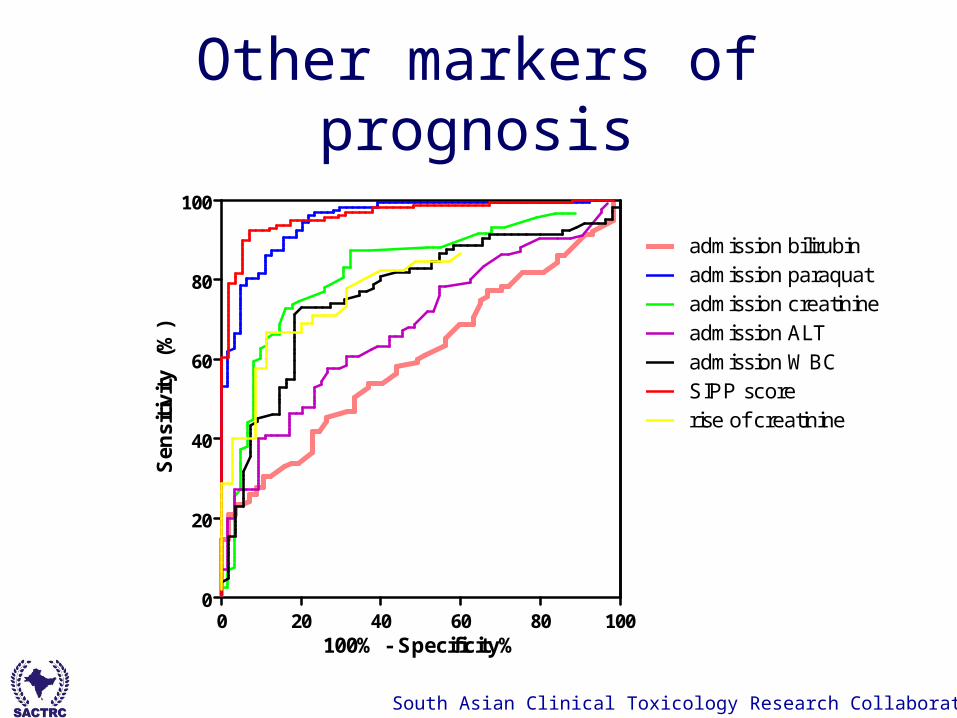
Other markers of prognosis
0 20 40 60 80 1000
20
40
60
80
100
admission paraquatadmission creatinineadmission ALTadmission WBCSIPP scorerise of creatinine
admission bilirubin
100% - Specificity%
Sen
siti
vity
(%
)

South Asian Clinical Toxicology Research Collaboration
No rise CFR 52.5%

South Asian Clinical Toxicology Research Collaboration


















