Sonographic evaluation of breast Dr. Muhammad Bin Zulfiqar
74
Sonographic evaluation of Breast DR MUHAMMAD BIN ZULFIQAR PGR III FCPS Services institute of Medical Sciences/ Services Hospital Lahore
-
Upload
dr-muhammad-bin-zulfiqar -
Category
Health & Medicine
-
view
5.246 -
download
6
Transcript of Sonographic evaluation of breast Dr. Muhammad Bin Zulfiqar

Sonographic evaluation of Breast
DR MUHAMMAD BIN ZULFIQARPGR III FCPS Services institute of Medical
Sciences/ Services Hospital Lahore

• High Resolution Breast Sonography.
• Elastography (Shear wave elastography).
Introduction
• Breast ultrasound uses high-frequency sound waves to map the internal structures of the breast.
• Sonoelastography is a noninvasive technique of imaging stiffness or elasticity of tissues by measuring movement or transformation of tissue in response to a small applied pressure.

Introduction
• Ultrasound has high sensitivity (95.7%) and high NPV
(99.9%) in detecting breast lesions.
• Sonography is gaining popularity as a screening tool
especially in ladies below 40 years so can be regarded as
primary imaging modality of choice.
• Its role in conjunction with mammography is well
established fact now.AJR:199, November 2012 Kolb et al, Buchberger et al, and Kaplan.

Aim
• To differentiate between benign and malignant masses with confidence.

Breast Sonography

Equipment selection:
Transducer• At the minimum, a 7.5 MHz
linear array probe should be used.
• 12-14 MHz probe

Apply gentle uniform pressure with the ultrasound transducer
Increase transducer pressure for:– greater penetration– scanning the subareolar region.
Scanning is done in three directions.
1. Radial 2. Transverse 3. Longitudinal Breast USG examination is not complete until we
check axillary tail and other breast

• Localization is by the clock face.
12
3
66
39

• All macroscopic breast structures can be easily imaged with adequate sonographic equipment.
The breast can be divided into five regions • skin, nipple, subareolar tissues• subcutaneous region• parenchyma (between the subcutaneous and
retro mammary regions)• retromammary region.• Axillary tail
Sonographic Breast Anatomy

Ultrasound interpretation
• The subcutaneous fat layer is demonstrated superficially as hypoechoic tissue compared to the glandular tissue from which it is separated by a well-defined scalloped margin.
• Normal ducts are often visible, particularly in the subareolar region, as anechoic tubular structures.
• Deep to the glandular tissue, a retromammary fat layer is usually visible and, behind this, the structures of the chest wall.
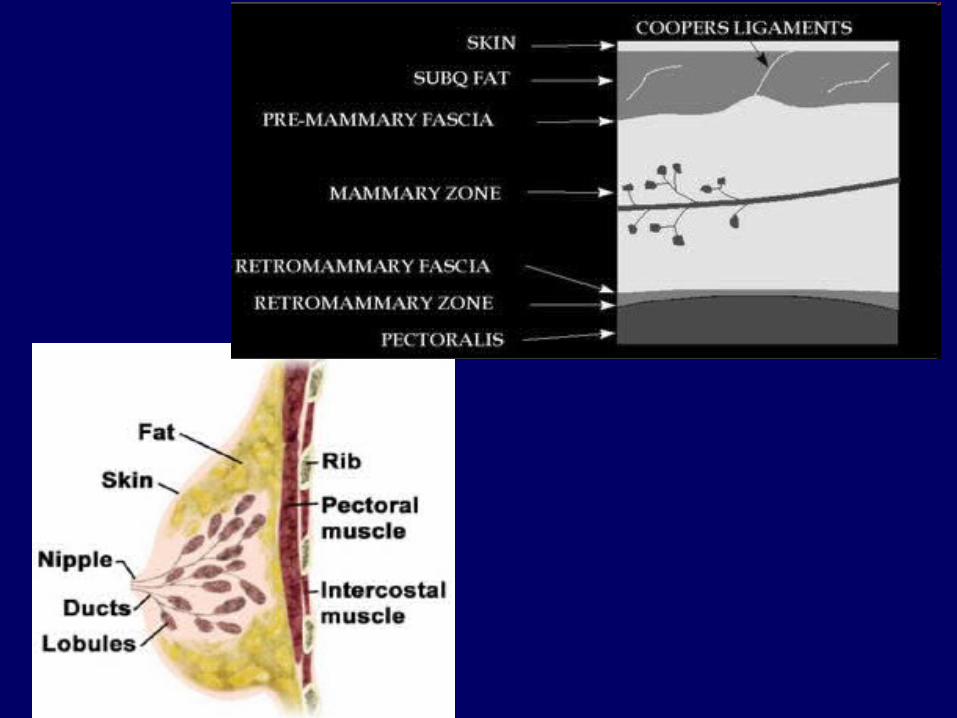

Sonographic Breast Anatomy
• Skin• Subcutaneous fat• Cooper’s Ligaments• Breast parenchyma• Retromammary fat• Pectoralis muscle• Ribs• Pleura• Nipple


Cooper's ligamentskin
fibroglandular tissue

Consists of both denseconnective tissue andconnective tissue ofthe duct which can cause posterioracoustic shadowing
Nipple

Easily identified bone attenuates causing an acoustic shadow
Ribs

Tubular branchingstructures
Duct

Ultrasound showing dilated ducts (lactating)The duct appears as branching hypoechoic structure within echogenic glandular tissue.

Intramammary vessel running branching under the skin.

•Solid nodule•Ovoid•Echogenic fatty hilum
Lymph Node

INDICATIONS
• Symptomatic breast lumps in women aged less than 35 years.
• Breast lump developing during pregnancy or lactation.• Assessment of mammographic abnormality (± further
mammographic views)• Assessment of MRI or scintimammography detected
lesions.• Clinical breast mass with negative mammograms.
continued

INDICATIONS
• Breast inflammation.
• The augmented breast (together with MRI).
• Breast lump in a male (together with mammography).
• Guidance of needle biopsy or localisation.
• Follow-up of breast cancer treated with adjuvant chemotherapy.

INDICATIONS
• The original role of breast sonography is in the differentiation of cystic and solid lesions.
• Ultrasound complements both clinical examination and mammography.
• It is also successfully used as a 'second-look' procedure where an abnormality has been identified using MRI or scintimammography.
continued

INDICATIONS• Because it does not use ionising radiation, it is the
examination of choice in young women and is valuable in the assessment of the mammographically `dense' breast.
• Ultrasound plays an important role in the triple assessment of symptomatic lesions.
• Being the only `real-time' imaging modality also means it can be used to accurately localise or biopsy breast lesions.

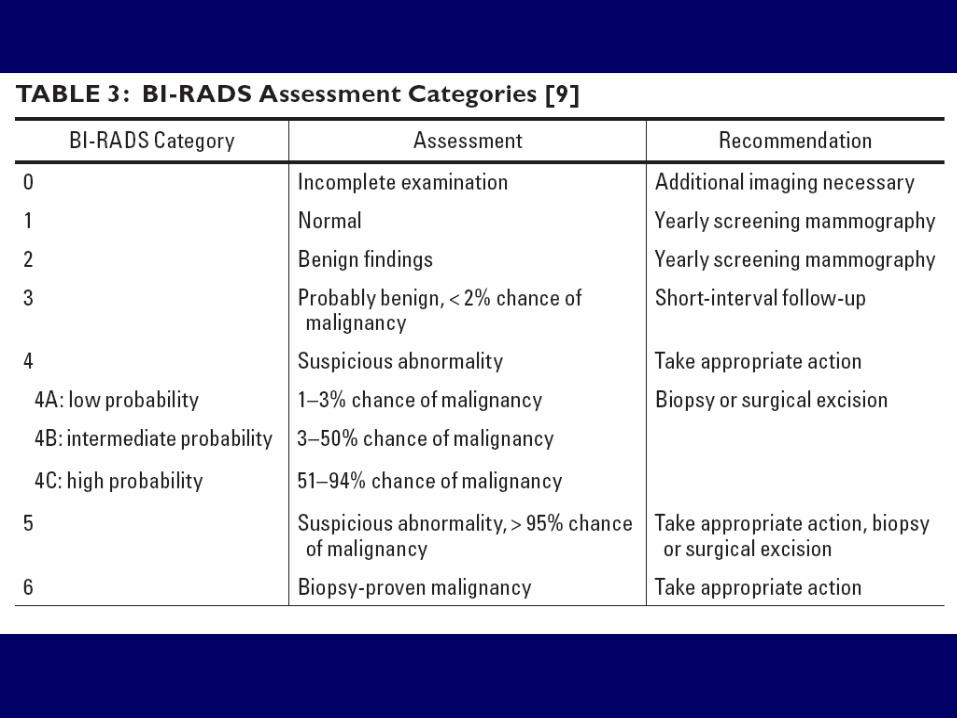
• BI-RADS assessment categories can be summarized as follows:• Category 0 - Need additional imaging evaluation• Category 1 - Negative• Category 2 - Benign finding, noncancerous• Category 3 - Probably benign finding, short-interval follow-up
suggested• Category 4 - Suspicious abnormality, biopsy considered• Category 5 - Highly suggestive of malignancy, appropriate
action needed• Category 6 – Biopsy proven cancer• Category 0 is a temporary category that means additional
imaging is needed before assigning a permanent BI-RADS assessment category.
BI-RADS

Cystic Masses of the Breast
Simple cyst or not ?
Not simple cystimaging-guided intervention is necessary to
exclude a solid mass.

Simple Cysts
• Most common masses seen at mammography.• Result from dilatation and effacement of the TDLU. • Frequently multiple and fluctuate in size on serial
examinations.

Simple Cysts
• Mammographic findings: – Circumscribed round or oval mass.
• Ultrasound: – Sonographic criteria set forth by Stavros:
• Anechoic.• Well circumscribed with a thin echogenic capsule.• Increased through-transmission.• Thin edge shadows.
– BI-RADS 2

Simple breast cyst
The first diagnostic imaging study Is mammography But ultrasound is importantTo differentiate solid from cyst

Simple Cysts
• Aspiration may be performed if :– Symptomatic.– The cyst prevents adequate compression for
mammography.
• Aspirated fluid is typically not sent for cytology except if it is bloody or the patient requests.

Complicated Cysts
• A cyst that meets all criteria of simple cyst except contains intermal echoes or fluid-fluid levels.
• Appropriate classification of complicated cyst = BI-RADS 3
– Because there is only a 0.2% chance of malignancy.
– Aspiration or short-interval follow-up should be offered.
Complex Cysts• Thick walls• Some discrete solid component
– Septa greater than 0.5 mm thick– Mural nodules.

Complicated Cyst •Breast abscess •Galactocele •Lipid cyst

Complex Cysts
Cyst with a mural nodule:– Papillary tumor.– Atypical ductal
hyperplasia.– DCIS
Complex cyst:
– Hematoma.– Galactocele.– Abscess.– Fat necrosis.– Necrotic
neoplasm.
Differential diagnosis

Simple cyst Complicated cyst Complex cyst
• Simple cyst• Galactocele• Hematoma• Oil cyst.
• Galactocele• Hematoma• Oil cyst.• Abscess.
• Galactocele• Hematoma• Fat necrosis.• Abscess.• Necrotic tumor.• Papillary tumor.• Atypical ductal
hyperplasia.• DCIS

Solid Lesions
• Benign• Malignant• Indeterminate

Benign MalignantShape Oval/ellipsoid Variable
Alignment Wider than deep; aligned parallel to tissue planes
Deeper than wide
Margins Smooth/thinechogenic pseudocapsule with2-3 gentle lobulations
Irregular or spiculated; echogenic 'halo'
Echotexture Variable to intense hyperechogenicity
Low-levelMarked hypoechogenicity
Homogeneity of internal echoes
Uniform Non-uniform
Lateral shadowing
Present Absent
Posterior effect Minimum attenuation/posterior enhancement
Attenuation with obscured posterior margin
Other signs -------------- CalcificationMicrolobulationIntraductal extensionInfiltration across tissue planes and increasedechogenicity of surrounding fat

Benign Characteristics
• Round or oval shape• Smooth defined borders• Uniformly low/medium
level internal echoes• Minimal attenuation if
any• Multiple lobulations

Solid Mass - Malignant
• Irregular shape• Irregular/ill-defined
borders• Almost anechoic• Angular margin• Taller than wide

Solid Mass - Malignant
• Irregular shape• Irregular/ill-defined
borders• Almost anechoic• Angular margin• Taller than wide
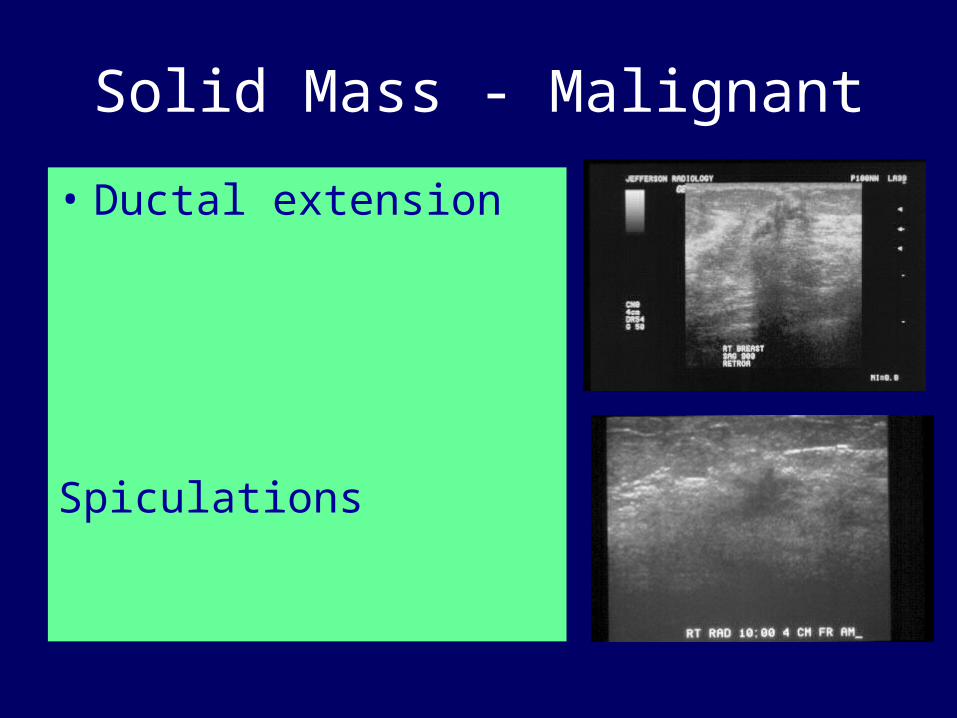
Solid Mass - Malignant
• Ductal extension
Spiculations

BIRADS II
• BI-RADS Category 2: Mass seen on mammogram proved to be a cyst.• Smooth well defined lesion in the right breast. Uniformly hypoechoic,
transverse diameter > AP, posterior acoustic enhancement, no micro/ Macro calcifications -

BIRADS III
• BIRADS 3 refers to a lesion that is probably benign. There is an 1.5 cm mass on mammogram. US was recommended and showed a solid, well-circumscribed parallel mass suggesting a probably benign lesion.
Fibroadenoma
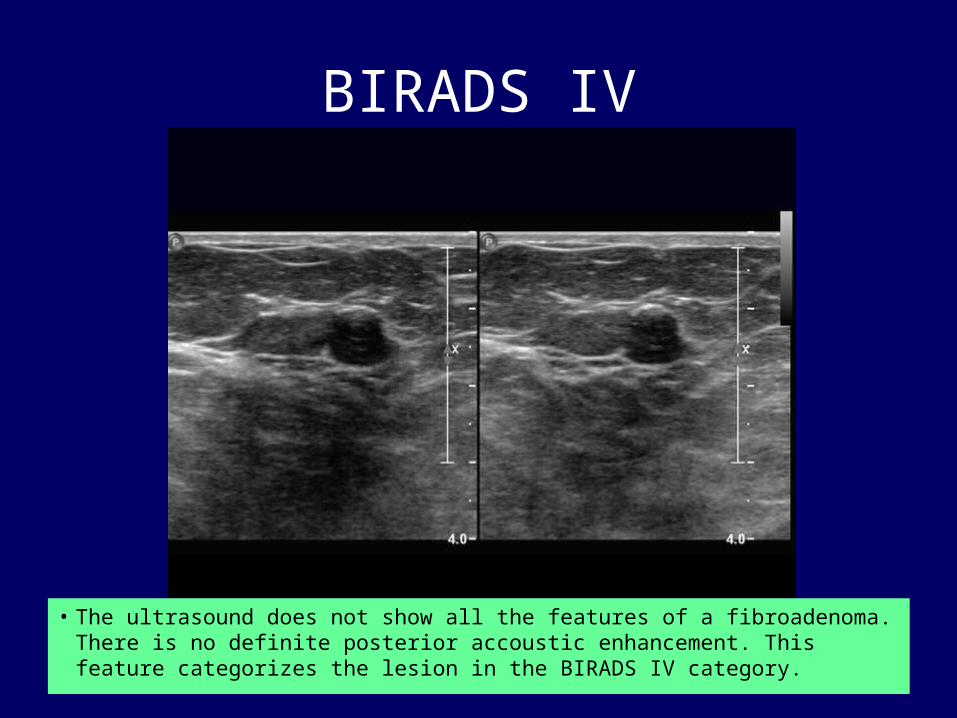
BIRADS IV
• The ultrasound does not show all the features of a fibroadenoma. There is no definite posterior accoustic enhancement. This feature categorizes the lesion in the BIRADS IV category.
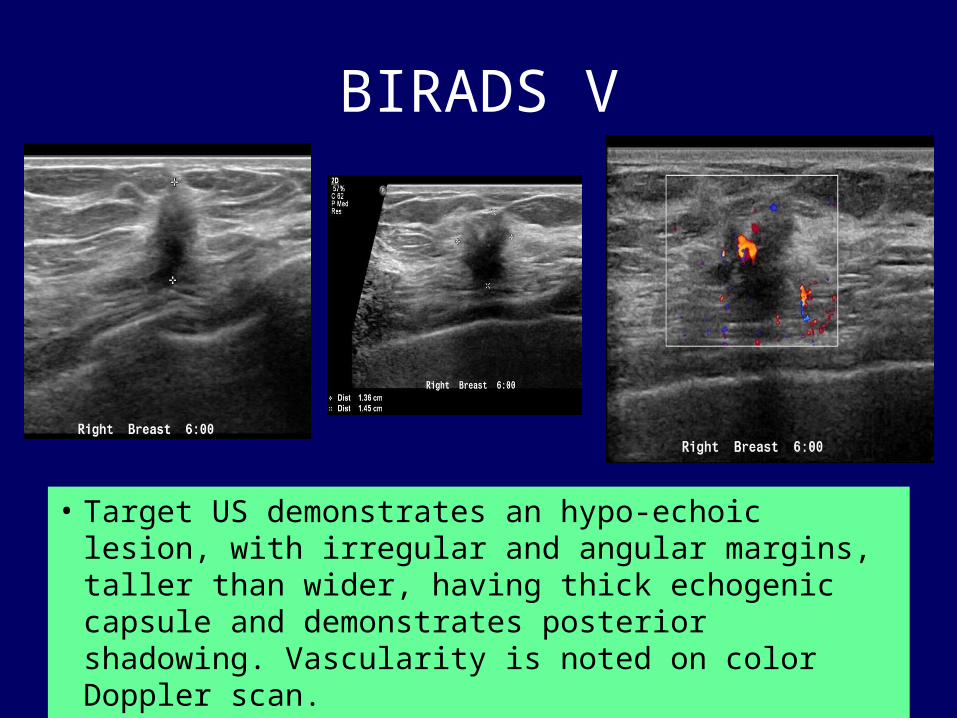
BIRADS V
• Target US demonstrates an hypo-echoic lesion, with irregular and angular margins, taller than wider, having thick echogenic capsule and demonstrates posterior shadowing. Vascularity is noted on color Doppler scan.

US guided interventions in breast lesions
• Fine needle Aspiration– Cytology– Aspiration of cyst /abscess
• Core Needle Biopsy

Cyst Aspiration

US guided Biopsy
• Real-time visualization of biopsy needle • Accessibility of all areas of breast and axilla • Multidirectional sampling possible • Low cost
US guided biopsy is indicated for both palpable and non-palpable breast lesions suspicious for malignancy
Advantages

Core Biopsy Needle

Ultrasound-guided biopsy of breast lesions
• Ultrasound-guided biopsy of breast lesion. The diagnostic study (A) shows a solid lesion (calipers) suspicious for cancer. An image during the biopsy (B) shows the core biopsy needle (arrows) sampling the lesion.

Ultrasound-guided biopsy of breast lesions
• Ultrasound-guided biopsy of a solid breast mass shows biopsy needle about to enter the mass.

Elastography
• Elastography is an imaging technique to measure the stiffness of tissues.
• Images are acquired before and after soft compression of tissues and the deformation is evaluated.
• Initially elastography used manual compression and was only qualitative.
• Now techniques are available to apply a non operator dependant compression.

Elastography and US
• Elastography was developed first in the US field.
• Three step approach:– Organs mechanically stressed by either external or
internal forces.– Measurement of tissues movement induced.– Qualitative or quantitative evaluation of tissue
elastic properties from the measured displacement of tissues.
Several Approaches
• Manual compression by operator using the transducer (static elastography).
• Organ compression by heartbeat or vascular pulsations.
• Push pulse waves compression.• Supersonic shear waves.

Supersonic shear waves.
• Displays elasticity maps in KiloPascals (kPa).• In the default setting, blue colors indicate
softer areas while red colors demonstrate stiffer areas.
Roles in Shear Wave Elastography
• Rule 1: upgrade BI-RADS 3 lesions with 2 suspicious SWE signs, namely not homogeneous SWE map + E max above 100 kPa.
• Rule 2: downgrade BI-RADS 4a lesions with 2 benign SWE signs, namely homogeneous SWE map + E max below 100 kPa.
• Rule 3: mix the 2 rules above: upgrade BI-RADS 3 lesions with 2 suspicious SWE signs and downgrade BI-RADS 4a lesions with 2 benign SWE signs.
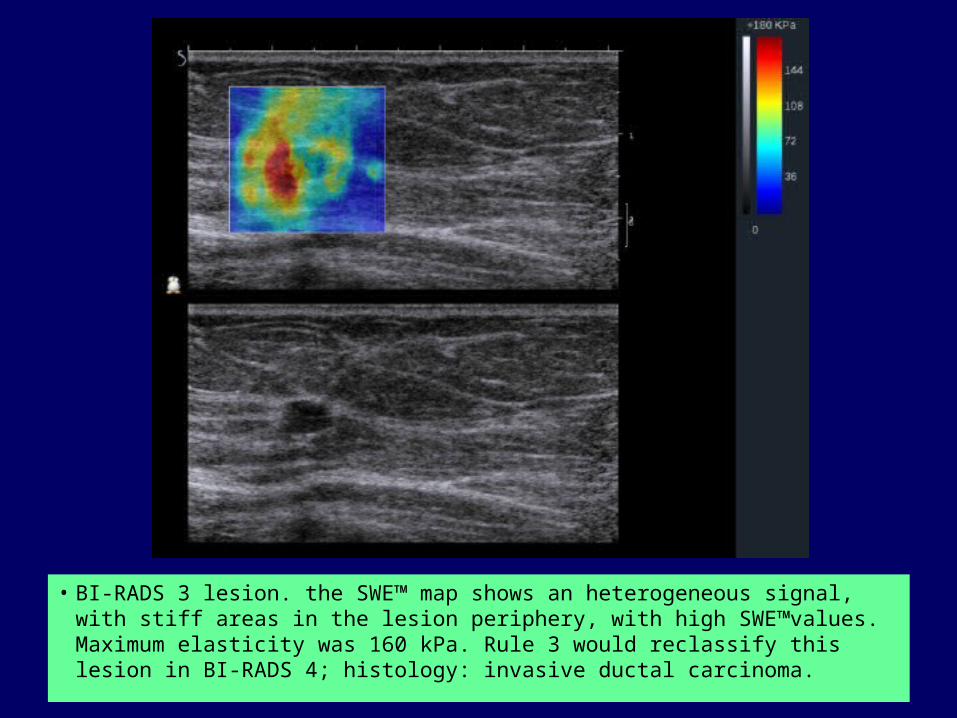
• BI-RADS 3 lesion. the SWE™ map shows an heterogeneous signal, with stiff areas in the lesion periphery, with high SWE™values. Maximum elasticity was 160 kPa. Rule 3 would reclassify this lesion in BI-RADS 4; histology: invasive ductal carcinoma.

• This BI-RADS 4 lesion showed an homogeneous SWE™ map and low SWE™ values (below 30 kPa). This lesion would be downgraded as a BI-RADS 3 according to rule 3 ; histology was a nodular adenosis.

Elastography
• Compared to gray-scale ultrasound, malignant lesions tend to be larger and more irregular on elastography likely secondary to stiff peripheral desmoplastic reaction.
• When measuring lesion size on elastography, the lesion should be measured in the exact position on both the elastogram and B-mode image.

• Heterogeneous echo texture , irregular shape and stiff color elastogram, which appears larger than the gray scale image.
• The color scale is a measure of stiffness. In these images, red indicates very stiff tissue, green/yellow indicates intermediate stiffness and blue indicates low stiffness IDC

• Benign lesions demonstrating : homogenoeus oval shape and very soft elastogram, which also appears the same size on both gray-scale and shear-wave elastography.. Clustered microcysts

FIBROADENOMA

COMPLEX CYST V/S SOLID LESIONS
• Elastography has the potential to differentiate complicated cysts form solid masses.
• Shear-wave propagation does not occur in cysts and therefore cysts should have elastography values of zero and will appear mostly black or homogeneously blue on the color overlay elastogram

Large simple cyst which shows no elasticity within the lesion and hence black

COMPLICATED CYST- HOMOGENEOUSLY BLUE

PROBLEM SOLVING• Elastography has the potential to downgrade BI-RADS 4a
lesions to BI-RADS 3, using qualitative shear-wave elastography and color assessment of lesion stiffness, oval shape and a maximum elasticity value of less than 80 kPa without a significant loss in sensitivity.
• Elastography may also be used to identify oval circumscribed cancers detected on ultrasound and may be used to upgrade a BI-RADS 3 lesion to BI-RADS 4.
• Furthermore, elastography feature analysis also has the potential to downgrade BI-RADS 3 lesion to BI-RADS 2 lesions.

ADVANTAGE
• Oval circumscribed hypoechoic mass on grey scale imaging, which has benign ultrasound features. However, elastography demonstrates a heterogeneous large and stiff elastogram.

QUANTITATIVE ASSESMENT
• Lesion stiffness can also be measured quantitatively with shear wave elastography.
• Stiffness of malignant lesions is generally greater than 80–100 kPa), while fat has relatively low elasticity values near 7 kPa and breast parenchyma have elasticity values ranging from 30-50 kPa.
• However, one must be careful when using kPa in lesion evaluation, as some soft cancers may have low kPa values between 20-80 kPa, similar to benign lesions

Pitfalls in elastography….
• Some cancers lack a significant desmoplastic reaction and may be soft, resulting in a false negative elastogram .
• With shear-wave elastography, some cancers may have a mean stiffness of less than 50 kPa
• Similarly, some benign lesions may appear stiff including hyalinized fibroadenomas, fat necrosis and fibrosis.
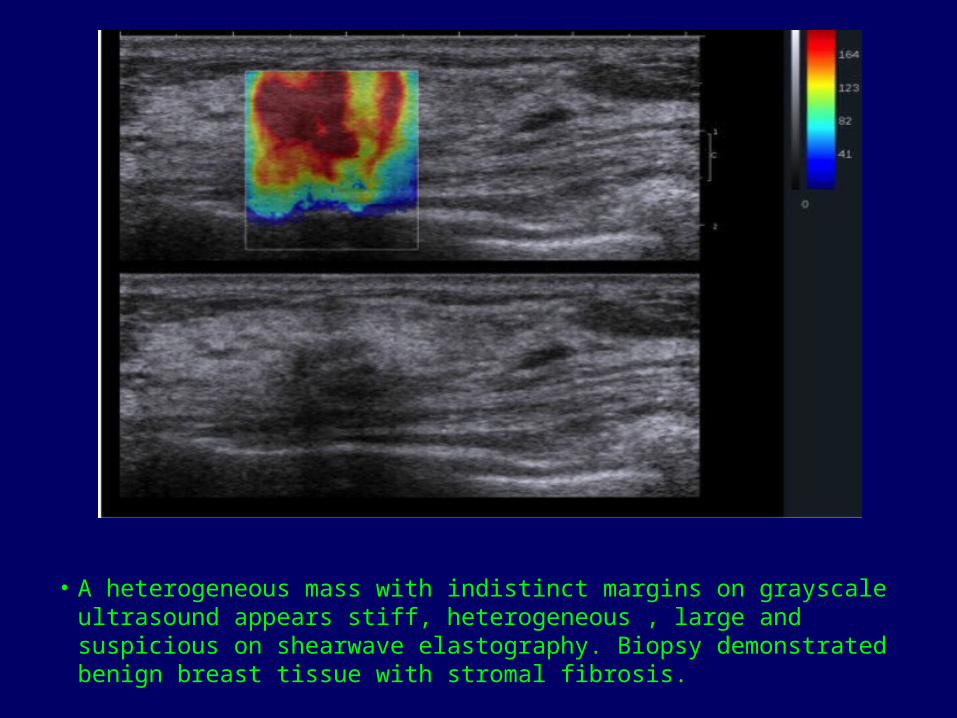
• A heterogeneous mass with indistinct margins on grayscale ultrasound appears stiff, heterogeneous , large and suspicious on shearwave elastography. Biopsy demonstrated benign breast tissue with stromal fibrosis.
Take Home Message
• To differentiate between benign and malignant masses with confidence.
• By Elastography – Downgrade BI-RADS 4a lesions to BI-RADS 3– Upgrade a BI-RADS 3 lesion to BI-RADS 4.– Downgrade BI-RADS 3 lesion to BI-RADS 2 lesions.
THANK YOU