Sonographic diagnosis of abdominal wall relaxation
4
Sonographic Diagnosis of Abdominal Wall Relaxation Michael Mu ¨ ller, MD, Son Ngoc Truong, MD, Volker Schumpelick, MD Department of Surgery, University Hospital RWTH Aachen, Pauwelsstrasse 30, Aachen 52074, Germany Received 4 June 1998; accepted 15 October 1998 ABSTRACT: Purpose. We report our experience using sonography to diagnose abdominal wall relaxation. Methods. All patients with abdominal wall abnor- malities from 1996 through 1997 underwent clinical and sonographic examination. Sonographic criteria for abdominal wall relaxation were continuity of the fascia (no gap), identification of all muscle layers, and decreased muscle thickness on the affected side. Fifty controls with no abdominal wall abnormalities were also examined for comparison. Results. We sonographically diagnosed 5 cases of abdominal wall relaxation in 625 patients examined. The diagnosis in these 5 cases was confirmed by MRI. Muscle thickness on the affected side decreased by a mean of 38% ± 6% compared with muscle thickness on the unaffected side and was significantly different (p < 0.0001) from the mean muscle thickness seen in the controls. Conclusions. Sonography enabled the diagnosis of abdominal wall relaxation with the advantages of sav- ing time and money and not requiring use of a con- trast medium. Based on our results, we recommend sonography as the first-line imaging modality in the diagnosis of abdominal wall relaxation. © 1999 John Wiley & Sons, Inc. J Clin Ultrasound 27:183–186, 1999. Keywords: abdominal wall relaxation; ultrasonogra- phy; magnetic resonance imaging I n most cases, abnormalities of the abdominal wall are easily evaluated because of their su- perficial location, and a correct diagnosis can be made on the basis of medical history, symptoms, and physical examination. However, abdominal wall relaxation, which occurs most commonly af- ter surgery on the kidneys 1 or aorta and iliac ves- sels 2 via a lateral retroperitoneal approach, can be clinically misinterpreted as an incisional her- nia because of the scar and abdominal wall bulg- ing. Sonography allows easy access to the differ- ent soft tissue layers of the abdominal wall, but to our knowledge, the diagnosis of abdominal wall relaxation by sonography has not been reported. We report our experience using sonography to di- agnose abdominal wall relaxation in cases in which clinical findings were ambiguous. PATIENTS AND METHODS From 1996 to 1997, we sonographically examined all patients who were referred to our surgical de- partment for the evaluation and treatment of ab- dominal wall abnormalities, regardless of the clinical diagnosis. Before sonographic examina- tion, all patients were asked about their symp- toms and physically examined. Informed consent was obtained from all participants in the study. Real-time sonography in transverse and longitu- dinal planes was performed with a CS 9400 ultra- sound scanner (Hitachi, Tokyo, Japan) and a 7.5- MHz linear-array transducer while the patient was in supine and standing positions. Blood ves- sels were verified by color duplex scanning. To distinguish hernias from abdominal wall relax- ation, dynamic studies were obtained while the patient performed Valsalva’s maneuver, coughed, and/or strained. Generally, in hernias, the hernial sac increases in size or changes location when the patient coughs or bears down. 3 We measured the thickness of abdominal muscles on both the affected and unaffected sides and compared these measurements with those of muscles on the right and left abdominal sides in a control group of 50 healthy subjects with no ab- dominal wall abnormalities. Criteria for the sono- Correspondence to: M. Mu ¨ ller © 1999 John Wiley & Sons, Inc. CCC 0091-2751/99/040183-04 VOL. 27, NO. 4, MAY 1999 183
Transcript of Sonographic diagnosis of abdominal wall relaxation

Sonographic Diagnosis of AbdominalWall Relaxation
Michael Muller, MD, Son Ngoc Truong, MD, Volker Schumpelick, MD
Department of Surgery, University Hospital RWTH Aachen, Pauwelsstrasse 30, Aachen 52074, Germany
Received 4 June 1998; accepted 15 October 1998
ABSTRACT: Purpose. We report our experience usingsonography to diagnose abdominal wall relaxation.
Methods. All patients with abdominal wall abnor-malities from 1996 through 1997 underwent clinicaland sonographic examination. Sonographic criteriafor abdominal wall relaxation were continuity of thefascia (no gap), identification of all muscle layers, anddecreased muscle thickness on the affected side. Fiftycontrols with no abdominal wall abnormalities werealso examined for comparison.
Results. We sonographically diagnosed 5 cases ofabdominal wall relaxation in 625 patients examined.The diagnosis in these 5 cases was confirmed by MRI.Muscle thickness on the affected side decreased by amean of 38% ± 6% compared with muscle thicknesson the unaffected side and was significantly different(p < 0.0001) from the mean muscle thickness seen inthe controls.
Conclusions. Sonography enabled the diagnosis ofabdominal wall relaxation with the advantages of sav-ing time and money and not requiring use of a con-trast medium. Based on our results, we recommendsonography as the first-line imaging modality in thediagnosis of abdominal wall relaxation. © 1999 JohnWiley & Sons, Inc. J Clin Ultrasound 27:183–186, 1999.
Keywords: abdominal wall relaxation; ultrasonogra-phy; magnetic resonance imaging
In most cases, abnormalities of the abdominalwall are easily evaluated because of their su-
perficial location, and a correct diagnosis can bemade on the basis of medical history, symptoms,and physical examination. However, abdominalwall relaxation, which occurs most commonly af-ter surgery on the kidneys1 or aorta and iliac ves-sels2 via a lateral retroperitoneal approach, can
be clinically misinterpreted as an incisional her-nia because of the scar and abdominal wall bulg-ing. Sonography allows easy access to the differ-ent soft tissue layers of the abdominal wall, but toour knowledge, the diagnosis of abdominal wallrelaxation by sonography has not been reported.We report our experience using sonography to di-agnose abdominal wall relaxation in cases inwhich clinical findings were ambiguous.
PATIENTS AND METHODS
From 1996 to 1997, we sonographically examinedall patients who were referred to our surgical de-partment for the evaluation and treatment of ab-dominal wall abnormalities, regardless of theclinical diagnosis. Before sonographic examina-tion, all patients were asked about their symp-toms and physically examined. Informed consentwas obtained from all participants in the study.Real-time sonography in transverse and longitu-dinal planes was performed with a CS 9400 ultra-sound scanner (Hitachi, Tokyo, Japan) and a 7.5-MHz linear-array transducer while the patientwas in supine and standing positions. Blood ves-sels were verified by color duplex scanning. Todistinguish hernias from abdominal wall relax-ation, dynamic studies were obtained while thepatient performed Valsalva’s maneuver, coughed,and/or strained. Generally, in hernias, the hernialsac increases in size or changes location when thepatient coughs or bears down.3
We measured the thickness of abdominalmuscles on both the affected and unaffected sidesand compared these measurements with those ofmuscles on the right and left abdominal sides in acontrol group of 50 healthy subjects with no ab-dominal wall abnormalities. Criteria for the sono-
Correspondence to: M. Muller
© 1999 John Wiley & Sons, Inc. CCC 0091-2751/99/040183-04
VOL. 27, NO. 4, MAY 1999 183

graphic diagnosis of abdominal wall relaxationwere no discontinuity of the aponeurosis (ie, fas-cial gap), visualization of all muscle layers of theabdominal wall, and decrease in muscle thicknessof the affected side compared with the unaffectedside.
Sonographic diagnoses of abdominal wall re-laxation were confirmed by MRI (1.5-T SP 63Magnetom; Siemens, Erlangen, Germany). Sta-tistical comparisons were done with a single-tailed t-test. A p value below 0.05 was consideredstatistically significant.
RESULTS
Among the 625 patients examined, 577 patients(92%) were diagnosed as having an abdominalwall hernia and 5 patients (1%) as having ab-dominal wall relaxation. Sonography revealed li-poma in 23 patients (4%) and metastasis in 8 pa-tients (1%), and these diagnoses were confirmedby histologic examination of surgically resectedspecimens. The remaining 12 patients (2%) hadvarious pathologic conditions.
Of the 5 patients with abdominal wall relax-ation, a typical flank bulge was seen on the rightside in 4 patients and on the left side in 1 patient(Figure 1). Four patients had previously had sur-gery on the kidneys via a typical lateral approachto the retroperitoneum, and 1 patient had previ-ously undergone surgery of a lumbar hernia withmesh implantation. All 5 patients complained of
discomfort, pain, muscle weakness, and abdomi-nal bulge on the affected side.
Sonographically, the rectus muscle on bothsides of the midline of the abdominal wall and the3 flat lateral abdominal muscles could be identi-fied. The 3 flat abdominal muscles in the flanks,ie, the oblique external, oblique internal, andtransverse muscles, were distinguished as 3 lay-ers separated by thin, highly echogenic aponeuro-ses (Figure 2). A very thin echogenic line, the peri-toneum, separated the abdominal wall from theabdominal viscera. In cases of abdominal wall re-laxation, all the abdominal wall muscle layerswere present, but they appeared thinner on theaffected side compared with the unaffected side(Figure 3). There was no discontinuity of the apo-neurosis, which remained intact during dynamicstudies.
In the patients with abdominal wall relaxation,the mean muscle thickness of all 3 abdominal lay-ers at the anterior axillary line was 13 ± 4 mm(standard deviation) on the affected side and 21 ±6 mm on the unaffected side. Direct comparison ofthe 2 sides in each patient showed a decrease inmuscle thickness of at least 33% (mean, 38% ±13%) (Table 1). The mean difference betweenmuscle thickness on the right and left sides of theabdominal wall in the control group was 5% ± 6%.The difference between these results and those ofthe 5 patients with abdominal wall relaxationwas highly significant (p < 0.0001).
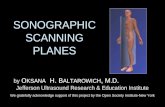
FIGURE 1. Typical abdominal bulge in a patient with abdominal wallrelaxation after surgery on the right kidney. The scar is marked byarrows.
FIGURE 2. Transverse sonogram and diagram of the normal lateralabdominal wall muscles.
MULLER ET AL
184 JOURNAL OF CLINICAL ULTRASOUND

MR images (Figure 4), showing the entire ab-dominal wall and all soft tissue layers, confirmedthe diagnosis in all 5 patients. Two patients werealso assessed by nerve conduction studies that re-vealed decreased innervation of the lateralmuscles of the abdominal wall. None of the 5 pa-tients underwent surgery for abdominal wall re-laxation.
DISCUSSION
Abdominal wall relaxation or flank bulge occursmost commonly after surgery performed via a lat-eral approach to the retroperitoneum. Repeatedcomplaints of postoperative wound complicationsand a 23% incidence of abdominal wall relaxationafter retroperitoneal surgery involving the aortaand iliac vessels have been reported in patientswhose surgery included muscle-dividing inci-sions.2 The anterolateral surgical approach to thekidney described by Guiliani in 1974 resulted in aloss of active abdominal muscle control in about
half the patients.1 However, the more recentmuscle-splitting and nerve-sparing surgical tech-niques have lowered the incidence of abdominalwall relaxation after kidney operations.
Abdominal wall relaxation is caused by muscleand fascial weakness following denervation atro-phy of a divided muscle. The denervation resultsfrom injury to the subcostal and intercostalnerves and their branches during the muscle-dividing procedure.2 Relaxation with a flankbulge occurs only when the nerves of all 3 abdomi-nal wall muscles are denervated. Experimentalresults and anatomic studies have shown that, forabdominal wall relaxation to result, the injury tothe intercostal nerve has to occur proximal to thebifurcation of the main trunk.4 Because the ma-jority of nerve bifurcations are located eitherwithin the intercostal space or at the tip of the11th rib,4 any surgical approach should avoid ex-
FIGURE 4. MR image showing right abdominal wall relaxation. Arrowpoints to the thinned muscles.
FIGURE 3. (Left) Transverse sonogram of abdominal wall relaxation. (Right) The unaffected side is shown for comparison. The abdominal wallmuscles are delineated by arrowheads.
TABLE 1
Muscle Thickness in 5 Patients with Abdominal
Wall Relaxation
PatientAffected
SideUnaffected
Side Difference % Decrease
1 17 28 11 392 13 21 8 383 8 12 4 334 15 25 10 405 11 18 7 39Mean ± SD 13 ± 4 21 ± 6 8 ± 3 38 ± 3
Abbreviation: SD, standard deviation.
ABDOMINAL WALL RELAXATION
VOL. 27, NO. 4, MAY 1999 185

tension into the intercostal space because suchextension could injure the intercostal nerve.
The first step in diagnosing abdominal wall re-laxation is the clinical examination. Abdominalwall bulging is typically found, but there is nopalpable fascial gap, as is found in cases of hernia.However, in obese patients, it is difficult to dis-tinguish abdominal wall relaxation from a smallhernia. In these and other problematic cases, fur-ther diagnostic tools are required to make a cor-rect diagnosis. A correct diagnosis is essentialbecause abdominal wall relaxation needs no op-erative treatment, whereas any kind of hernia re-quires surgical repair. Additional diagnosticmethods include sonography, CT, MRI, and neu-rologic examination with nerve conduction stud-ies. Both CT and MRI show the entire abdominalwall and enable direct comparison between theaffected and unaffected sides. MRI also makes itpossible to identify the different layers of the ab-dominal wall; CT does not offer this advantage.
In our study, MRI and sonography showed ab-dominal wall relaxation equally well, althoughthe number of false-negative sonographic diag-noses is not known because MRI was done only toconfirm the cases diagnosed by sonography. Aprevious study showed that sonographic findingsprovided correct diagnoses of clinically indetermi-nate abdominal wall and inguinal abnormalitiesin 85% of cases.5 Those reported results combinedwith the results of our study indicate that sonog-raphy is an excellent tool for correctly diagnosingabdominal wall abnormalities. A 7.5-MHz trans-ducer facilitates identification of the 3 muscle lay-ers and comparison with these layers on the con-tralateral side. As an alternative to MRI for suchcases, sonography has the advantages of faster
examination, lower cost, and no risks of allergicreaction to a contrast agent. In addition, sono-graphic examination can be repeated.
Our study confirms the criteria for the sono-graphic diagnosis of abdominal wall relaxation:intact fascia, visualization of all muscle layers,and muscle thickness on the affected side that isat least a third less than that on the unaffectedside. In contrast, hernias show a discontinuity ofthe fascia with protruding hernial contents.3 Werecommend sonography as the first-line imagingmodality in the diagnosis of abdominal wall re-laxation.
REFERENCES
1. Giberti C, Martorana G, Carmignani G. The Guil-iani muscle splitting and nerve-sparing anterolat-eral transabdominal approach to the kidney. Urol-ogy 1996;47:911.
2. Honig MP, Mason RA, Giron F. Wound complica-tions of the retroperitoneal approach to the aortaand iliac vessels. J Vasc Surg 1992;15:28.
3. Truong SN, Muller M, Schumpelick V. Imagingprocedures for investigations of the abdominal walland inguinal region. In: Schumpelick V, Kings-north AN, editors. Abdominal wall: function de-fects and repair. Berlin: Springer; in press.
4. Gardner GP, Josephs LG, Rosca M, et al. The ret-roperitoneal incision: an evaluation of postopera-tive flank bulge. Arch Surg 1994;129:753.
5. Truong SN, Pfingsten F, Dreuw B, et al. Value ofultrasound in the diagnosis of undetermined find-ings in the abdominal wall and inguinal region. In:Schumpelick V, Wantz GE, editors. Inguinal her-nia repair. Proceedings of the Expert Meeting onHernia Surgery; 1994 Feb 2–5, St. Moritz. Basel:Karger; 1995. p 29–41.
MULLER ET AL
186 JOURNAL OF CLINICAL ULTRASOUND