Sonographic and histological appearance of heel enthesopathy ...

AJR:180, April 2003
941
Sonographic Detection and Sonographically Guided Biopsy of Breast Microcalcifications
OBJECTIVE.
The purpose of this study was to evaluate the ability of sonography to de-pict and guide biopsies of mammographically suspicious microcalcifications and to reveal themammographic features and histologic outcomes of lesions amenable to sonographicallyguided biopsy.
SUBJECTS AND METHODS.
Suspicious clusters of microcalcifications without othermammographic abnormalities were evaluated on sonography before biopsy and divided intotwo groups: those with and those without microcalcifications seen on sonography. Sono-graphically detected lesions underwent sonographically guided biopsy; lesions not seen onsonography underwent mammographically guided biopsy. Imaging features and histologieswere correlated, and the positive predictive value of sonography was determined.
RESULTS.
Of 111 lesions (105 patients), 26 lesions (23%) were identified and underwentsonographically guided biopsy; 85 lesions (77%) were not identified sonographically. The diame-ters of microcalcification clusters in the sonographically identified group were significantly larger(
p
= 0.0005) and contained larger numbers of microcalcification particles (
p
= 0.038) comparedwith clusters not identified sonographically. Sonographically identified lesions were seen asmasses (77%) or dilated ducts (23%) with echogenic foci. Sonographically identified lesionswere more likely to be malignant than those not seen on sonography (69% vs 21%, respectively;
p
< 0.00002). Of 38 malignant lesions, those visible on sonography were more likely to be in-vasive than those not seen on sonography (72% vs 28%, respectively;
p
= 0.018). In malig-nant lesions undergoing core biopsy and surgical excision, the extent of disease wasunderestimated less with sonographically guided biopsy (7%, 1/15) than with stereotactic bi-opsy (33%, 5/15).
CONCLUSION.
Suspicious microcalcifications are seen infrequently on sonography (23%)but, when detected, can be successfully biopsied with sonographic guidance and more frequentlyare malignant and represent invasive cancer than those seen on mammography alone.
ammographically revealed, suspi-cious clustered microcalcifica-tions that have no associated
mammographic features are usually diagnosedby either percutaneous core needle biopsy withstereotactic guidance or at surgical excision af-ter mammographically guided wire localiza-tion. Although both techniques are successfulfor aiding in diagnosis of these lesions [1], thetechniques require mammographic compres-sion of the breast that is uncomfortable for thepatient, and they expose the breast to ionizingradiation. Many stereotactic biopsies are per-formed with the patient in a prone position,which is often considered uncomfortable andin some cases is difficult or impossible for pa-tients to tolerate. In addition, mammographic
compression can make the breast too thin to al-low successful core needle biopsy of a lesion.Finally, stereotactic biopsy equipment is ex-pensive and not universally available.
Sonography is frequently used to guidepercutaneous core biopsy or wire localiza-tion before excisional biopsy of breastmasses [1]. In general, sonographicallyguided procedures are preferred by patientsover mammographically guided proceduresbecause patients are more comfortable su-pine, the breast is not compressed, and theprocedures are often performed faster [1, 2].In addition, no ionizing radiation is used, theneedle insertion site is more flexible, and theneedle can be observed in real time withsonographically guided procedures [1, 2].
Mary Scott Soo
1
Jay A. BakerEric L. Rosen
Received August 6, 2002; accepted after revision September 18, 2002.
Presented at the annual meeting of the American Roentgen Ray Society, Seattle, April–May 2001.
1
All authors: Department of Radiology, Breast Imaging Division, Duke University Medical Center, P.O. Box 3808, Durham, NC 27710. Address correspondence to M. S. Soo.
AJR
2003;180:941–948
0361–803X/03/1804–941
© American Roentgen Ray Society
M

942
AJR:180, April 2003
Soo et al.
Recently, a study of suspicious microcalcifi-cations undergoing mammographically guidedwire localization was performed to evaluatesonographic detection of these lesions [3]. Inthis study, 45% of lesions were seen on sonog-raphy and were confirmed to be at the site ofmammographically guided wire placement[3]. Other studies have shown that sonographycan be used successfully to guide core biopsyof lesions shown on sonography to contain mi-crocalcifications [2, 4, 5]. We undertook thisstudy to determine what percentage of suspi-cious microcalcifications could be seen onsonography and then successfully sampledwith sonographic guidance; we evaluated themammographic features and histologic out-come of those lesions that were amenable tosonographically guided detection and biopsy.
Subjects and Methods
During an 11-month period, 110 patients with116 suspicious groups of microcalcifications thatwere recommended for biopsy consented to enterour prospective, institutional review board–ap-proved study to determine if the suspicious micro-calcifications were visible on sonography andamenable to sonographically guided biopsy. To beinvited into the study, patients had to be scheduledfor biopsy of mammographically visible microcal-cifications without associated mammographicallyidentified masses or architectural distortions. Be-fore biopsy, sonography targeted to the site of mi-crocalcifications was performed. Each lesion wasthen placed into one of two groups after comple-tion of sonography: those with microcalcificationsdetected on sonography or those with no microcal-cifications identified on sonography. Lesions visi-ble on sonography subsequently underwentsonographically guided biopsy, with either percu-taneous core biopsy or wire localization with sur-gical excision. Specimen radiography andpostprocedure mammography were performed toconfirm that the microcalcifications were sampled.Lesions not depicted on sonography underwenteither stereotactic biopsy or mammographicallyguided wire localization with surgical excisionand specimen radiography. Four of the 110 pa-tients were excluded from the study because thesubsequent biopsy was not performed undersonographic guidance in patients in whom micro-calcifications were visible on sonography. Onepatient was excluded from those with the groupof lesions not seen on sonography because ster-eotactic biopsy could not be performed; the pa-tient chose to undergo imaging follow-up ratherthan excisional biopsy. The remaining 105 pa-tients with 111 suspicious groups of microcalcifi-cations constituted our study population.
Mammography was performed using a film-screen technique (Mammomat II, Mammomat III,Mammomat 3000, Siemens Medical Solutions, Ise-
lin, NJ; DMR Plus, General Electric Medical Sys-tems, Milwaukee, WI). Standard mediolateraloblique and craniocaudal images of the breasts wereobtained in each patient; additional spot compressionmagnification images of areas of microcalcificationswere also obtained in all except three patients.
Sonograms targeted to the site of microcalcifi-cations were obtained using high-resolutionsonography equipment (Elegra; Siemens Quan-tum, Isequah, WA) with a commercially available13.5-MHz 1.5 dimensional linear array probe. Allsonographic evaluations were performed with thepatient supine with the ipsilateral arm raised abovethe head. Images were obtained in planes radialand antiradial to the nipple in the region of themammographic microcalcifications.
Percutaneous core biopsies were performed un-der sonographic guidance for lesions visible onsonography and under stereotactic guidance for le-sions not visible on sonography using techniquespreviously described [1, 2]. For microcalcifica-tions that underwent core biopsy under sono-graphic guidance, high-resolution sonographicequipment (Siemens Medical Solutions, USA, Ise-lin, NJ) and a 13.5-MHz 1.5 dimensional linear ar-ray probe was used with either a multipassautomated gun and a 14-gauge needle (Bard, Cov-ington, GA) (
n
= 7) or a handheld vacuum-assisteddevice with an 11-gauge probe (Mammotome; Bi-opsys/Ethicon Endo-Surgery, Cincinnati, OH) (
n
=18). The choice of biopsy device was based on thepreference of the radiologist performing the proce-dure. For microcalcifications seen on mammogra-phy alone, stereotactic biopsy was performed usingeither a prone table (Stereoguide with digital spotmammography; Lorad, Danbury, CT) or an uprightadd-on stereotactic device (Senovision, DMR, Gen-eral Electric Medical Systems). For all stereotacticbiopsies, a vacuum-assisted biopsy device with an11-gauge probe was used to sample the calcifica-tions. After core biopsy in each group, specimen ra-diography was performed to confirm the presence ofmicrocalcifications, and postprocedure mammo-grams were obtained to ensure that the suspiciousgroup of microcalcifications seen on mammographywas sampled. The number of core specimens ob-tained during each biopsy was recorded and com-pared between the groups.
Wire localization before surgical excision wasperformed using a 21-gauge hooked wire needle(Kopans; Cook, Bloomington, IN). For wire localiza-tions performed under sonographic guidance, high-resolution sonography equipment and a 13.5-MHz1.5 dimensional linear array probe were used to guideneedle placement. For lesions not seen on sonogra-phy, a fenestrated compression paddle with an alpha-numeric grid was used to guide needle placement.Postprocedure craniocaudal and true lateral mammo-grams were obtained after wire placement to confirmlocalization of the microcalcifications and to pro-vide the surgeon with reference images. Specimenradiography was then performed after surgical ex-cision to confirm the presence of microcalcifica-tions in the specimen.
The percentage of sonographically detected mi-crocalcification clusters was calculated. The imag-ing features of the two groups were then comparedon the basis of mammographic breast density, larg-est diameter of the group of microcalcifications,number of microcalcifications per group, microcal-cification morphology and distribution, and BreastImaging Reporting and Data System (BI-RADS) [6]final assessment category. On mammography, thesize of the group of microcalcifications was mea-sured as the greatest diameter of the group in eithermediolateral oblique or craniocaudal projections.The number of microcalcifications in each groupwas assessed on magnification images and catego-rized as fewer than 15 microcalcifications, 15–50microcalcifications, or more than 50 microcalcifica-tions. The breast density based on the four BI-RADS parenchymal patterns (predominantly fatty,scattered fibroglandular density, heterogeneouslydense, or extremely dense tissue) was recorded. Mi-crocalcification morphology was determined ac-cording to BI-RADS descriptors: pleomorphic,amorphous, fine linear-branching, round, or punc-tate. Distribution of microcalcifications was alsobased on BI-RADS descriptors: clustered, linear,segmental, or regional.
On sonography, any finding associated with themicrocalcifications was recorded, including massesor dilated ductlike structures not seen on mammog-raphy. The size of the mass or dilated duct that con-tained the microcalcifications was assessed on thebasis of the largest size measured on static images,and this size was compared with the diameters of thegroup of microcalcifications seen on mammography.
Histologic results from each core biopsy and sur-gical excision were reviewed. The positive predictivevalues of sonography and mammography for thispopulation were calculated, and the sensitivity, speci-ficity, and negative predictive value of sonographywere determined. For patients in each group under-going core biopsy of the microcalcifications followedby surgical excision, the percentage of cases in whichfinal surgical pathology results showed that the corebiopsy underestimated the disease process (e.g.,atypical ductal hyperplasia identified at core biopsybut ductal carcinoma in situ [DCIS] diagnosed at sur-gery, or DCIS identified at core biopsy but invasiveductal carcinoma diagnosed at surgery)
was com-pared between the groups.
The Fisher’s exact test, the Wilcoxon’s signedrank test, and the Mann-Whitney test were usedto compare differences between groups, and theCochran-Mantel-Haenszel statistics based on tablescores were used to test for a monotonic orderedrelationship among variables. Findings with a
p
value of less than 0.05 were considered to be sta-tistically significant.
Results
Of 111 mammographically suspicious mi-crocalcification lesions in 105 patients, 26 le-sions (23%) were identified as masses or ductswith microcalcifications and biopsied under

Sonography of Breast Microcalcifications
AJR:180, April 2003
943
sonographic guidance. In 85 lesions (77%), nomasses or microcalcifications were identifiedon sonography. One patient had one lesion seenon sonography and two lesions not seen onsonography. In no patients did findings onsonography show a suspicious mass withoutmicrocalcifications in the targeted area; how-ever, in two patients in whom sonographyshowed a mass with microcalcifications, an ad-ditional incidental mass was seen in an adjacentregion. Each mass proved to be a complicatedcyst at sonographically guided biopsy of the le-sion. In the group of patients with 26 lesionsthat underwent sonographically guided biopsy,the mean patient age was 61 years (age range,38–81 years), and in the group of patients with85 lesions that underwent mammographicallyguided biopsy, the mean patient age was 55years (age range, 39–86 years).
Table 1 lists the mammographic parenchymaldensity, mammographic features of the micro-calcifications undergoing biopsy, and the BI-RADS assessment categories for each group. Nostatistically significant difference in the breastparenchymal density was found between the twogroups (
p
= 0.951). No mass or architectural dis-tortion was identified on mammography in asso-ciation with the microcalcifications, although themicrocalcifications were often seen in a back-ground of fibroglandular density.
In the group of microcalcifications seenon sonography, the mammographic diame-ters of the clusters of microcalcificationswere significantly larger than those clustersnot identified on sonography (
p
= 0.0005).The microcalcifications seen on sonographyalso had significantly more microcalcifica-tions per cluster than those not seen onsonography (
p
= 0.038). Segmentally distrib-uted microcalcifications were found only inthe group of microcalcifications seen onsonography, which was statistically signifi-cant (
p
= 0.012). There was no significantcorrelation with other morphologic featuresof the microcalcifications on mammography.
BI-RADS category 5 lesions (highly sug-gestive of malignancy) were significantlymore likely to be seen on sonography (Fig. 1)than not seen on sonography (
p
< 0.00003),with 89% (8/9) of all BI-RADS category 5 le-sions identified on sonography. BI-RADS cat-egory 4 lesions seen on sonography (Fig. 2)had a greater likelihood of being malignant(59%, 10/17) than did BI-RADS category 4 le-sions not seen on sonography (21%, 17/81).
The mammographic lesions shown onsonography were seen as echogenic fociwithin either hypoechoic (95%) or isoechoic
(5%) masses (77%), or within hypoechoic di-lated ductlike structures (23%). The mean sizeof the abnormal sonographic finding (mass orduct with microcalcifications, 16 mm) was lessthan that of the corresponding mammographicgroup of microcalcifications (23 mm), al-though the difference was not statistically sig-nificant (
p
= 0.10). Seventy-one percent ofmasses showed posterior acoustic shadowing,and 83% of these were malignant. The masseswere either irregular (89%) or lobular (11%),and either wider than tall (75%) or taller thanwide (25%). Seventy-two percent of thewider-than-tall masses, a feature that is oftenassociated with benign lesions, proved to bemalignant. However, the margin of thesemasses suggested a malignant process ineach, classified as ill-defined, angular, mi-crolobulated, or duct extension.
Of 25 core biopsies performed in thegroup of microcalcifications seen on sonog-raphy, an 11-gauge vacuum-assisted devicewas used in 18 biopsies (72%) and a 14-gauge multipass gun was used in seven biop-sies (28%). A mean of eight cores was taken,using each device. The outcome of eachsonographically guided procedure was con-sidered successful, confirmed with specimenradiographs showing microcalcifications inall cases (96%) except one. In the one lesionin which no microcalcifications were identifiedon the specimen radiograph, a large hypoechoicmass associated with the microcalcifications onsonography was successfully targeted andsampled, although microcalcifications werenot retrieved despite multiple attempts (Fig.3). Nevertheless, DCIS was confirmed athistology. In the one wire localization pro-
Note.—BI-RADS = Breast Imaging Reporting and Data Systems [6]. aSignificant difference noted between groups with p < 0.05.
TABLE 1 Mammographic Features of Microcalcifications
SizeOn Sonography
Visible Not Visible
Size of microcalcification groupsa
Mean size (mm) 23 9 Size range (mm) 3–90 2–45
Features No. % No. %
Breast parenchymal density pattern
Predominantly fatty 0 0 2 2 Scattered fibroglandular density 8 31 24 28 Heterogeneously dense 13 50 40 47 Extremely dense 5 19 19 22No. of microcalcificationsa
<15 11 42 37 4415–50 7 27 36 43>50 8 31 11 13
Distribution of microcalcifications Clustered 19 73 81 95Linear 1 4 1 1Segmentala 3 12 0 0Regional 3 12 3 4
Microcalcification morphology Punctate 1 4 8 9Round 1 4 4 5Amorphous 3 12 12 14Pleomorphic 18 69 58 68Fine linear-branching 3 12 1 1
BI-RADS assessment category 3 1 4 3 4 4 17 65 81 95
5a 8 31 1 1

944
AJR:180, April 2003
Soo et al.
cedure performed with sonographic guid-ance before surgical excision (core biopsywas never requested in this patient), micro-calcifications were identified on the speci-men radiograph.
In the group of lesions not seen on sonog-raphy, 73 (91%) of 80 attempted stereotacticcore biopsies were performed successfullyusing an 11-gauge vacuum-assisted device.More core specimens were obtained duringstereotactic biopsy of lesions in this group(range, 5–28; mean number of cores, 11)compared with the group seen on sonogra-phy and biopsied with sonographic guidance(range, 5–15; mean number of cores, 8) (
p
=0.001). Seven (9%) of 80 attempted stereo-tactically guided procedures were terminatedbecause the lesion was either too faint orsmall (size range, 2–8 mm) to be seen on thedigital monitor (
n
= 6) or because the breast
became too thin with compression to allowuse of the biopsy needle device (
n
= 1).These patients subsequently underwent sur-gical excision of the lesions.
Of the 26 lesions identified on sonographythat subsequently underwent sonographi-cally guided biopsy, 18 (69%) were malig-nant and eight (31%) were benign.Therefore, a positive finding on sonographyin the setting of mammographically suspi-cious microcalcifications had a positive pre-dictive value of 69% for identifyingcarcinoma. For suspicious microcalcifica-tions with a negative finding on sonography,mammography had a much lower positivepredictive value (21%) in our study. Of the18 malignant lesions in the group shown onsonography, 17 initially underwent core bi-opsy before definitive therapy. Of the 17 le-sions sampled with core biopsy, two patients
diagnosed with DCIS did not undergo surgi-cal excision during the study period becauseof other serious medical problems in one andthe initiation of neoadjuvant chemotherapyin another who had presented with ipsilateralmetastatic axillary lymph nodes positive foradenocarcinoma. The follow-up in this pa-tient occurred at an outside facility. Of theremaining 15 malignant lesions that wereinitially sampled with core biopsy, the extentof disease was underestimated at initial corebiopsy in one case (7%) of atypical ductalhyperplasia that was upgraded to DCIS at ex-cision (Table 2).
Of 85 lesions (80 patients) that were notidentified on sonography, 18 (21%) were ma-lignant and 67 (79%) were benign. This find-ing resulted in a negative predictive value forsonography of 79%. Of the 18 malignant le-sions, 16 diagnostic stereotactic core biop-
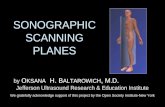
Fig. 1.—75-year-old woman with invasive ductal carcinoma in right breast.A, Spot magnification mammogram shows linear and branching microcalcifications highly suggestiveof malignancy. B, Sonogram of region of microcalcifications shows enlarged hypoechoic duct (arrowheads) with in-ternal echogenic microcalcifications (arrows). On sonographically guided core biopsy (not shown),microcalcifications in duct were targeted. C, Specimen radiograph from core biopsy shows microcalcifications (arrows) in specimens.
BA
C

Sonography of Breast Microcalcifications
AJR:180, April 2003
945
sies were attempted initially before definitivetherapy. Fifteen were successful, and onewas canceled because the breast became toothin with compression to allow use of the bi-opsy needle device. Of the 15 lesions thatwere initially sampled with stereotactic corebiopsy, the extent of disease was underesti-mated at initial core biopsy in five (33%), in-cluding two cases of atypical ductalhyperplasia that were upgraded to DCIS andthree cases of DCIS that were upgraded toinvasive ductal carcinoma at excision.
Overall, sonography showed a sensitivityof 50% and a specificity of 89% for detectingcarcinoma in cases of suspicious microcalci-fications. Lesions identified on sonographywere significantly more likely to be malig-nant than those not seen on sonography(69% vs 21%, respectively;
p
< 0.00002). Ofall malignant lesions, those seen on sonogra-phy were significantly more likely to be inva-sive than those not seen on sonography (72%vs 28%, respectively;
p
= 0.018). Less under-estimation of disease occurred in the group
of lesions biopsied under sonographic guid-ance compared with the group biopsied un-der stereotactic guidance, although thisdifference did not achieve statistical signifi-cance (
p
= 0.17).
Discussion
In the past decade, great strides have beenmade in improving resolution and contrast inbreast sonography, allowing better and morefrequent visualization of breast microcalcifi-cations [2, 3, 7, 8]. When they are detected,breast microcalcifications are seen on sonog-raphy as distinct echogenic specular reflec-tors, contrasting with a backgroundhypoechoic mass or ductlike structure thatincreases microcalcification conspicuity [2,3]. In our study, we found these same sono-graphic features to be present in lesions de-tected on sonography. Less commonly,microcalcifications can appear as broaderechogenic regions without a significant asso-ciated mass or duct [2]. On sonography, de-
tection of microcalcifications, which waspreviously limited to mammographicallyguided techniques, provides the opportunityfor biopsy of these lesions under sono-graphic guidance [2].
In our study, 23% of microcalcificationswithout other mammographic findings wereidentified on sonography, and sonographicguidance was used successfully to guide thebiopsy using core biopsy or wire localizationtechniques. Few false-positive sonograms havea specificity of 89%. The mammographic fea-tures of the microcalcifications that were mostpredictive of sonographic identification in-cluded large size of the microcalcificationgroup, large number of calcific particles in thegroup, BI-RADS category 5 lesions, and seg-mental distribution of microcalcifications.These features are consistent with a previousreport that found that the visibility of masseson sonography corresponding to areas of clus-tered microcalcifications was much higherwith highly suspicious microcalcifications,particularly those larger than 10 mm [3]. These
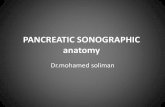
Fig. 2.—73-year-old woman with in-vasive ductal carcinoma in rightbreast.A, Spot magnification mammogramshows pleomorphic microcalcifica-tions suspicious for malignancy. B, Sonogram of region of microcalcifi-cations shows lobulated ill-definedmass (arrowheads) with associatedmicrocalcifications (arrows). C, Sonogram obtained during coreneedle biopsy shows needle (arrows)traversing mass (arrowheads).D, Specimen radiograph from corebiopsy shows microcalcification(arrow) in specimen.
BA
DC

946
AJR:180, April 2003
Soo et al.
larger, more suspicious-appearing lesionsfound on mammography in our study wereprobably more predictive that the lesion wouldbe identified on sonography because they cor-related with a greater percentage of invasivecarcinomas at histology. Invasive carcinomasoften present as hypoechoic masses on sonog-raphy that sometimes cannot be seen on mam-mography because they are obscured byregions of dense fibroglandular tissue. It islikely that the hypoechoic background pro-vided by the masses served to increase theconspicuity and detection of the internalechogenic microcalcifications in our study.Microcalcifications shown on sonographywere seen as echogenic foci in either hypo-echoic or isoechoic masses or hypoechoicductlike structures in all cases, similar to le-
sions described in previous studies [2, 3]. Eventhough sonographically depicted masses orducts containing microcalcifications tended tobe smaller than the corresponding mammo-graphic group of microcalcifications in ourstudy and the number of echogenic foci seenon sonography was less than the number ofcalcific particles seen on mammography, sono-graphically guided core biopsy was successfulin each patient, using either the 11-gaugehandheld vacuum-assisted device or the 14-gauge automated multipass gun.
On the basis of the criteria established byStavros et al. [9], the presence of microcalci-fications in a mass on sonography confers amalignant categorization; therefore, allmasses identified on sonography in our studyshowed features that would be considered
suspicious for malignancy. Most masses alsoshowed other suspicious features on the basisof criteria established by Stavros et al., in-cluding posterior acoustic shadowing; irreg-ular shape; and ill-defined, angular,microlobulated or duct-extension margins[9]. Seventy-two percent of masses classifiedas wider than tall were malignant. Widerthan tall is a feature that is often associatedwith benign lesions. However, each of thewider-than-tall lesions possessed other suspi-cious features that would prompt biopsy, re-gardless of this more benign finding.
In our study population, a positive sono-gram in the setting of mammographicallysuspicious microcalcifications had a higherpositive predictive value than did mammog-raphy of suspicious microcalcifications with
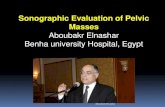
Fig. 3.—41-year-old woman with metastatic adenocarcinoma in right axillary lymph nodes andductal carcinoma in situ with necrosis in right breast.A, Sonogram obtained before biopsy of region of mammographic microcalcifications shows ill-de-fined hypoechoic mass (arrowheads) with microcalcifications (arrows) located superficially. B, Sonogram obtained during core needle biopsy shows needle (arrowheads) transversing super-ficial portion of mass, targeting microcalcifications (arrow). Microcalcifications were not seen onspecimen radiograph (not shown), and marker clip was deployed with sonographic guidance.C, Magnification craniocaudal mammogram obtained after biopsy shows residual pleomorphicmicrocalcifications (arrowheads) with adjacent marker clip (arrow) in close proximity to micro-calcifications.
BA
C

Sonography of Breast Microcalcifications
AJR:180, April 2003
947
a negative sonogram (69% vs 21%). Micro-calcifications detected on sonography weremore than three times as likely to be malig-nant than microcalcifications not seen onsonography, and lesions detected on sonog-raphy were also almost three times morelikely to represent an invasive cancer thanthose seen on mammography alone. Al-though the positive predictive value washigher in lesions shown on sonography, thisgroup of lesions also contained a larger num-ber of BI-RADS category 5 lesions that werealready highly suggestive of malignancy onthe basis of the mammographic interpreta-tion. In these few cases, identification of thelesion on sonography would not increase thesuspicion of the lesion. However, BI-RADScategory 4 lesions that were identified onsonography were much more likely to bemalignant than BI-RADS category 4 lesionsnot identified on sonography (Fig. 2).
Our study showed less underestimation ofdisease when core biopsy was performedwith sonographic guidance, compared withlesions undergoing stereotactically guidedbiopsy, despite the fact that smaller 14-gaugeneedles were used in sampling 28% of caseswith sonographic guidance and larger 11-gauge probes were used in all stereotacticallyguided biopsies. The smaller 14-gauge nee-dles used with the multipass automated guntechnique have previously been reported toresult in more underestimation of diseasethan the 11-gauge probes used with vacuum-assisted technique on the basis of data fromseries of stereotactic biopsy cases [10, 11].
This underestimation did not occur in ourgroup biopsied with sonography guidance.Underestimation of disease was lower in ourgroup of statistically larger lesions seen onsonography. This finding differs from that ofanother recent report suggesting that under-estimation of disease during stereotactic bi-opsy is greater in larger lesions (> 30 mm)[12]. Theoretically, the underestimation ofdisease normally caused by a sampling errorof larger heterogeneous lesions or usingsmaller 14-gauge needles could be reducedby sampling lesions with sonographic guid-ance because the hypoechoic masses or duct-like structures seen in addition to echogenicmicrocalcifications could be directly targetedin real time. In addition, a mass that was seenon sonography but not identified on mam-mography might represent the higher gradecomponent of the lesion (e.g., invasive com-ponent in a large area of DCIS), as has beensuggested in a previous report [2]. In our ste-
reotactically guided procedures, no findingother than microcalcifications was seen, andthe needle device was guided by static mam-mographic imaging rather than by real-timeimaging. However, the difference in underes-timation of disease in our study did not reachstatistical significance; therefore, evaluationwith a larger sample size would be needed tofurther investigate this theory. In addition,our study was not a randomized trial to com-pare sonographically guided biopsy with ste-reotactically guided biopsy of equal-sizedand equivalently categorized BI-RADS le-sions. This comparison is necessary to deter-mine if sonographically guided biopsy ofmicrocalcifications truly results in less un-derestimation of disease.
The obvious limitation to sonographicguidance for biopsy of microcalcifications isthat not all groups of microcalcifications canbe detected on sonography, with only 23% ofcases identified in our study. This percentageis smaller than that reported in a previousstudy of suspicious microcalcifications un-dergoing mammographically guided wire lo-calization before excisional biopsy. In thatstudy, sonography was performed before andafter wire placement with mammographicguidance, and 45% of lesions were seen onsonography [3]. The method and end point toour study differed in that we were challengedto perform sonographically guided biopsy orwire localization of the lesion detected, con-firming the lesion by specimen radiographyrather than relying on mammographicallyguided wire localization for confirmation.Lesions in our study had to be confidentlyidentified on sonography with visualizationof microcalcifications to undergo biopsywith sonographic guidance.
Another factor likely contributing to thelower detection rate was the small size (often
≤
5 mm) and faint appearance of the clustersof microcalcifications not detected on sonog-raphy. Biopsies for these lesions proved to bechallenging procedures even using the stereo-tactically guided technique because six stereo-tactically guided procedures were attemptedbut terminated as a result of lesions being toofaint to be seen on the digital monitor.
In conclusion, suspicious clustered micro-calcifications are infrequently seen on sonog-raphy. Sonography is most successful atshowing larger areas of highly suspicious mi-crocalcifications, and a positive sonogram inthe setting of mammographically suspiciousmicrocalcifications has a high specificity anda high positive predictive value for detecting
carcinoma. Biopsy of suspicious microcalci-fications under sonographic guidance is a via-ble and accurate alternative to stereotacticbiopsy for microcalcifications that are visibleon sonography. This technique has potential
Note.—IDC = invasive ductal carcinoma, DCIS = ductalcarcinoma in situ, ADH = atypical ductal hyperplasia, LCIS =lobular carcinoma in situ.
aIndicates underestimation of disease compared withsurgical excision result.
TABLE 2 Core Needle Biopsy Versus Surgical Excision Results
Biopsy Core Biopsy Surgery
Sonographically guided
1 IDC IDC/DCIS2 IDC/DCIS IDC/DCIS3 IDC/DCIS IDC/DCIS4 IDC IDC/DCIS5 IDC IDC6 IDC/DCIS IDC/DCIS7 IDC/DCIS IDC/DCIS8 IDC IDC9 IDC/DCIS IDC/DCIS
10 IDC/DCIS IDC/DCIS11 IDC/DCIS IDC12 IDC IDC13 ADHa DCIS14 DCIS DCIS15 DCIS DCIS
Stereotactically guided
1 ADH Benign2 ADH Benign3 DCIS DCIS4 DCISa IDC/DCIS5 ADH LCIS6 IDC/DCIS IDC/DCIS7 DCIS DCIS8 Benign Benign9 ADHa DCIS
10 DCISa IDC/DCIS11 IDC/DCIS IDC/DCIS12 DCIS DCIS13 DCIS DCIS14 DCIS DCIS15 DCISa IDC/DCIS16 DCIS DCIS17 DCIS DCIS18 ADH Benign19 DCIS DCIS20 ADHa DCIS

948
AJR:180, April 2003
Soo et al.
for reducing patient discomfort, and furtherstudy is warranted to determine its potentialfor reducing underestimation of disease com-pared to stereotactic biopsy.
References
1. Parker SH, Burbank F. A practical approach tominimally invasive breast biopsy.
Radiology
1996
;200:11–202. Soo MS, Baker JA, Rosen EL, Vo TT. Sonograph-
ically guided biopsy of suspicious microcalcifica-tions of the breast: a pilot study.
AJR
2002
;178:1007–10153. Moon WK, Im J-G, Koh YH, Noh D-Y, Park IA.
US of mammographically detected clustered mi-crocalcifications.
Radiology
2000
;217:849–854
4. Teh WL, Wilson ARM, Evans AJ, Burrell H, Pin-der SE, Ellis IO. Ultrasound guided core biopsyof suspicious mammographic calcifications usinghigh frequency and power Doppler ultrasound.
Clin Radiol
2000
;55:390–3945. Rickard MT. Ultrasound of malignant breast mi-
crocalcifications: role in evaluation and guidedprocedures.
Australas Radiol
1996
;40:26–316. American College of Radiology.
Breast imagingreporting and data system (BI-RADS)
, 3rd ed.Reston, VA: American College of Radiology,
1998
7. Anderson ME, Soo MSC, Bentley RC, TraheyGE. The detection of breast microcalcificationswith medical ultrasound.
J Acoust Soc Am
1997
;101:29–398. Yang WT, Suen M, Ahuja A, Metreweli C. In vivo
demonstration of microcalcification in breast can-cer using high resolution ultrasound.
Br J Radiol
1997
;70:685–6909. Stavros AT, Thickman D, Rapp CL, Dennis MA,
Parker SH, Sisney GA. Solid breast nodules: useof sonography to distinguish between benign andmalignant lesions.
Radiology
1995
;196:123–13410. Liberman L, Smolkin JH, Dershaw DD, Morris
EA, Abramson AF, Rosen PP. Calcification retrievalat stereotactic, 11-gauge, directional, vacuum-as-sisted breast biopsy.
Radiology
1998
;208:251–26011. Jackman RJ, Burbank F, Parker SH, et al. Stereotac-
tic breast biopsy of nonpalpable lesions: determi-nants of ductal carcinoma in situ underestimationrates.
Radiology
2001
;218:497–50212. Brem RF, Schoonjans JM, Goodman SN, Nolten
A, Askin FB, Gatewood OMB. Nonpalpablebreast cancer: percutaneous diagnosis with 11-and 8-gauge stereotactic vacuum-assisted biopsydevices.
Radiology
2001
;219:793–796
The 2003 ARRS Annual Meeting will include a new issues forum on screening CT.