Sonographic Characterization of Tenosynovitis · 2016-12-30 · phasis on the change of tendon...
6
199 2 ; 28 (2) : Jou rnal of Korean R adiological Soc iety , March , 1 992 Sonographic Characterization of Tenosynovitis Gwy Suk Seo , M.D. , Hyo Keun Lim , M.D. , In Jae Lee , M.D , Kil Woo Lee , M.D. , Sang Hoon Bae , M.D. , Kyung Hwan Lee , M.D. Department of DiagnOstic RadioJogy , CoJJege o[ Medicine . HaJJym University - Abstract- Te nosynovitis of the ex tr e miti es is not uncommon but its di agnosis is not easy owing to its non-specific clinical manifestation. Thus it was b eyond the field of imaging diagnosis so fa r. Recently the development of high resolu- tion ultrasonogram has aided preop erative imaging diagnosis of tenosynovitis. Th e authors performed a retrosp ec- tive review of 27 patients who had ultraso nography due to tendon pathology(including 18 tenosynovit es) by sonographic findings and evaluating the diagnostic value of each finding. The overall diagnostic accuracy was 81.1 % a nd co mmon sonographic findings wer e focal swelling of the tendon. well-defined margin of th e le sion. prese rv ed fibrillar pattern. ec ho c hange of the lesion site and f1 uid co ll ect ion . Above al l. f1 uid collection was th e onl y statistically significant c riterion for diagnosis of tenosynovitis(p<0.05). But its sensitivity was as low as 50%. ln con - clusion the ultrasonogr a phy is us eful in diagnosis of tenosynovitis and f1 uid collection is of diagnostic value . but th e differe ntiation b etwee n nodular te nosynovitis without f1 uid coll ec tion and other benign tumor is still beyo nd the scope of ultrasonographic diagnosis ‘ Index Words: Ultrasound ‘ Te nosynovitis ‘ Tendinitis INTRODUCTION Two main categories of non-traumati c les ion of the ext re mities are infla mmatory diseases and tumorous co nditions . which are characteriz ed by quite diffe rent c1 inical manif estatio ns and which re quir e diff ere nt approach to the managemen t. And usually they co me to need medical a dvice complaining of pain or swe ll- ing which is so c ommonly an early manifestation , but non-sp ec ific. At initial period or so metimes through the whole dis ease process , diffe renti a tion betwe en the two is quite nuisant to the clinicians. As for inflam- matory diseas es , it is es pecially difficult to diagnos e a nd to differ e nti ate from others. To t he c1 ini c ians ' lu ck in ess , inflammatory condition of the tendon a nd peritendinous structures sometimes fall within the scop e of ultrasonographic examination owing to their superficial location( 1-5). In su ch a context. the authors observed co mmon findings and tried ultrasonographi c c har acte rization of te ndinou s in- flammation and discussed the rol e and limitation of ultrasonograthy in diagnosing tendinous in f1 am- m atio n. METHOD From July 1989 to Sept 199 1. twenty-seven pa- tients , who had ultrasonography and were diagnos- ed as tendon or perite ndinous pathology , were sel ecte d for a retrospective revi ew. There were 17 mal es a nd 10 females and their m ean age was 34.8(range:6-67 Yrs) . Among them 18 had tenosynovites , four had cystic tumors(two epidermal in c lusion cysts. on e ganglion. one synovial cyst )‘ Received November 29, 1991 , Accepted January 9, 1992 - 275-
Transcript of Sonographic Characterization of Tenosynovitis · 2016-12-30 · phasis on the change of tendon...

대 한 방 사 선 의 학 회 지 1992 ; 28 (2) : 27 5~28 0
Journal of Korean Radiological Society , March , 1992
Sonographic Characterization of Tenosynovitis
Gwy Suk Seo, M.D. , Hyo Keun Lim, M.D. , In Jae Lee, M.D , Kil Woo Lee, M.D. , Sang Hoon Bae, M.D. , Kyung Hwan Lee, M.D.
D epartment of DiagnOstic RadioJogy, CoJJege o[ Medicine. HaJJym University
- Abstract-
Tenosynovitis of the extremities is not uncommon but its diagnosis is not easy owing to its non-specific clinical
manifestation. Thus it was beyond the field of imaging diagnosis so fa r. Recently the development of high resolu
tion ultrasonogram has aided preoperative imaging diagnosis of tenosynovitis. The authors performed a retrospec
tive review of 27 patients who had ultrasonography due to tendon pathology(including 18 tenosynovites) by obseπing
sonographic findings and evaluating the diagnostic value of each finding. The overall diagnostic accuracy was 81.1 %
and common sonographic findings were focal swelling of the tendon. well-defined margin of the lesion. preserved
fibrillar pattern. echo change of the lesion site and f1uid collection . Above al l. f1uid collection was the only
statistically significant criterion for diagnosis of tenosynovitis(p<0.05). But its sensitivity was as low as 50%. ln con
clusion the ultrasonography is useful in diagnosis of tenosynovitis and f1uid collection is of diagnostic value . but
the differentiation between nodular tenosynovitis without f1uid collection and other benign tumor is still beyond
the scope of ultrasonographic diagnosis ‘
Index Words: Ultrasound ‘ Tenosynovitis ‘ Tendinitis
INTRODUCTION
Two main categories of non-traumatic lesion of the
extremities are infla mmatory diseases and tumorous
conditions. which are characterized by quite different
c1inical manifestations and which require different
approach to the management. And usually they come
to need medical a dvice complaining of pain or swell
ing which is so commonly an early manifestation , but
non-specific . At initial period or sometimes through
the whole disease process , differentia tion between the
two is quite nuisant to the clinicians. As for inflam
matory diseases , it is especially difficult to diagnose
a nd to differentiate from others. To the c1 inic ians'
luckiness , inflammatory condition of the tendon a nd
peritendinous structures sometimes fall within th e
scope of ultrasonographic examination owing to their
superficial location( 1-5) . In such a context. the
authors observed common findings and tried
ultrasonographic characterization of tendinous in
flammation and discussed the role and limitation of
ultrasonograthy in diagnosing tendinous in f1am
m ation .
METHOD
From July 1989 to Sept 199 1. twenty-seven pa
tients , who had ultrasonography and were diagnos
ed as tendon or peritendinous pathology , were
selected for a retrospective review. There wer e 17
males a nd 10 fem a les and their m ean age was
34.8(range:6-67 Yrs) . Among them 18 had
tenosynovites , four h ad cystic tumors(two epidermal
inc lusion cysts. one ganglion. one synovial cyst)‘
이 논문은 1991년 11월 29일 접수하여 1992년 1월 9일에 채택되었음
Received November 29, 1991, Accepted Janua ry 9, 1992
- 275-

Journal of Korean Radi이 ogical Society 1992 ; 28 (2) : 275~28D
three had tendon rupture and one had a s이id tumor.
Of all , twelve cases(six tenosynovites and six others)
were confirmed by operation and the others were
diagnosed on a clinical basis including labüratory fin
dings and aspiration cytology. The sonographic
equipment we used were SSD-630(Aloka , Tokyo ,
Japan) and UM-4(ATL , Bothell , USA) with a 5.0 or
7 .5 MHz linear probe designed for small body part in
vestigations.
We observed ultrasonographic findings with em
phasis on the change of tendon size , outer margin of
the lesion , fibrillar pattern ofthe tendon at lesion site ,
echo texture of the lesion , and presence of calcificai
tion or focal fluid collection. And then we evaluated
the significance of individual sonographic feature in
a statistical method using the Chi-square test with
Yates correction
RESULT
The commonest location of tenosynovitis was the
flexor or extensor tendon of the hand and wrist follow
ed by the Achilles tendon , peroneus tendon , and the
quadriceps tendon in decreasing order of frequen
cy(Table 1).
The clinical manifestations are listed in Table 2.
Focal swelling and pain are the major complaints and
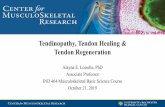
Fig. 1. A transverse sonogram of the thumb shows swollen tendon and anechoic f1uid collection surrounding the tendon(arrow).
Fig. 2. The fibrillar pattern of the Achilles tendon is preserved(arrow) even in the inflammed area(arrow).
as many as seven patients were presented with overt mass. History of trauma was noted in four patients.
The ultrasonographic findings were as follows :
Table 1. Location of the Lesion in Tenosynovitis Group focal swelling of the tendon (Fig. 1) was found in 15
Location
Finger , Hand Achilles Peroneus Quadriceps Popliteal fossa
Number (%)
11 (6 1.1)
3 (1 6.7) 2 (1.1)
1 (5.6) 1 (5.6)
cases , the margin of the tendon was well defined in
11 cases , but ill-defined in seven cases. the fibrillar
pattern of the tendon was preserved(Fig. 2) in 13
cases, partially disrupted in four cases and complete
ly lost in one case(In this case, sonographic diagnosis
was erroneous) . Ten lesions showed different echo
texture from the remaining portion of the tendon ,
Table 2. Clinical Manifestations in Tenosynovitis Group six of them were hypoechoic and four were mixed
Manifestation
Focal swelling Pain Mass Limitation of motion Trauma association
Number (%)
9 (50 .0) 7 (38 .9) 7 (38.9) 1 (5 .6) 4 (5.6)
echogenic. Of nine cases with fluid collection(Fig. 3) ,
regional focal fluid collection in three cases and dif
fuse collection paralleling the tendon course in six
was found. Totally three cases had calcification(Fig.
4 ), one of which proved to be tuberculosis and the
others were diagnosed as non-tuberculous tenosy
novitis(Table 3).
- 276-

Fig. 3. Normal sized extensor tendons of the wrist are surrounded by l1uid(arrows) within common synovial sheath.
The sonographic findings of non-tenosynovitis
cases are listed on table 4
The overall diagnostic accuracy of this series was
81 . 1 % and the only single sonographic finding- l1uid
collection-was statistically significant for the
diagnosis of tenosynovitis.(p<O.05 , Table 5) Other
single findings were not statistically significant for
the diagnosis .(All P>O .25) And also no combination
of sonographic finding was significan t.
Table 3. Sonographic Findings of Tenosynovitis Group
Gwy Suk Seo , et al : Sonographic Characterization of Tenosynovitis
Fig. 4. A longitudinal sonogram of the Achilles tendon shows hypoechoic area with multiple calcific dots(arrowheads).
DISCUSSION
Many tendon abnormalities go undetected or go
neglected without call for medical advice . However ,
tendons are a very common site of injury. Inflam
matory conditions are the second most common
category of tendon abnormality. Tendons are
Patient Fibrillar* * Fluid Swelling Margin ‘ Echo*** Calcification
+ + 2
3
4
5
6
7
8
9
m U
u m M
mu
m n
mω
+
+
+
+ + +
+ +
+ +
+
+
+
+
+
+
+ + +
+
+
+ +
+
* ( +); well defined margin of tendon * *( + ); preserved fibrillar pattern of tendon * * * ( + ); change of echo texture of lesion
+ +
+
+
+ +
+
+ +
+
+ +
+ +
+ +
+ +
+ + + +
+ +
+ + + +
+ +
+
+ +
+
+
낌

Journal of Korean Radi이 ogical Society 1992 ; 28 (2) : 275~280
Table 4. Sonographic Findings of Non-Tenosynovitis Group
Calcification Fluid Echo*** Fibrillar ‘ • Margin* Swelling Patient
+ + +
+
+ + +
+
F +
+
l
2
3
4
5
6
7
8
9
+ +
+
+
+
+ +
+
+ + + +
*( +) ; well defined margin of tendon * *( +); preserved fibrillar pattern of tendon
* * • (+); change of echo texture of lesion
+
Table 5. US findings vs their Significance in Tenosynovitis
P valve specificity (e)
sensitivity (e)
False
(-) False
( + )
True (-)
True (+)
US finding
>0 .50
>0 .50
>0.75
>0.25
<0.05
>0 .50
33.3
22.2
33.3
44.4
100.0
100.0
83.3
6 1.1
72.2
55.6
50.0
16.7
3
7
5
8
9
샌
6
7
6
5
0
0
3
2
3
4
9
9
mω n
퍼 m
9
3
Swelling Margin*
Fibrillar* * Echo***
Fluid
Calcification
*( +) ; well defined margin of tendon * ‘ ( +); preserved fibrillar pattern of tendon
* * *( +) ; change of echo texture of lesion
quickly into adjacent tendinous structures especial
ly in hands where common synoviaJ sheath envelops
the deep and superficiaJ flexor tendons at the finger
leveI(6). Tenosynovitis is not only the result ofminor
or vigorous trauma. calcific deposit or infection(7.8).
but is associated with other arthritides such as
rheumatoid arthritis or tuberculosis(8). The concept
of a special form-nodular tenosynovitis is stilI under
controversy. Some regard it as a giant ceIJ tumor of
the tendon sheath and others insist it is a synovial
inflammation(6.7) .
Ultrasonographic examination has been
established method for tendon pathology but its main
application was for tumorous conditions and
traumatic ruture(l -5) . There have been only a smaIJ
number of articIes on tenosynovitis. Jeffrey. J r.
reviewed surgicaIJy confirmed acute tenosynovitis
and the sonographic finding was hypoechoic area sur
rounding the involved tendon(ll) and a case report
enveloped by a double layered synovial sheath when
they pass through an osseofibrous tunnel such as in
hands and feet(6) . So tendinous inflammation easily
develops into tenosynovitis or vice versa. It spreads
an
Fig. 5. A well-demarcated mass from the flexor tendon of the ha nd has homogeneous echogenicity and calcific foci It was misdiagnosed as benign tumor sonographically.
- 278-

Gwy Suk Seo, et al : Sonographic Characterization of Tenosynovitis
by Stephenson shows peritendinous f1 uid with nor
mal tendons( 12)_ In our series , the main findings were
focal swelling of the tendon with preservation of a
fibrillar pattern , well-defined margin and f1uid collec
tion. Focal swelling and preserved fibrillar pattern is
of high sensitivity but quite non-specific. In contrast ,
f1uid collection is of statistical significance in diagnos
ing tenosynovitis
In seven cases which had initial manifestation of
palpable mass , the suspected mass proved to be
swelling of the tendon in four cases , f1uid collection
without tendon change in one case , focal swelling of
the tendon in one cases and actual mass discovery
sonographicallY in one case. The last case was
misdiagnosed preoperatively(Fig. 5) . In another case
with complete disruption of the fibrillar pattern ,
tenosynovitis could not be suggested. There were two
cases whose ultrasonographic dignosis was
tenosynovitis , but were confirmed to be fibroma and
ganglion at operation. Likewise , focal swelling
without f1uid colleciton of the tendon remains a
diagnostic pitfall , which says again that f1uid colle
tion is criterion of high specificity but low sensitivity
In conc1usion , ultrasonography is useful in
diagnosing tenosynovitis and the major specific
sonographic finding is f1uid collection. But differen
tiation between nodular tenosynovitis and benign
tumor by ultrasonography is still problematic.
REFERENCES
1. Khaleghian R. Tonkin LJ , De Geus JJ , Lee JPK.
Ultrasonic examination of the flexor tendons of th e
fingers . J Clin Ultrasound 1984;12:547-551
2. Dillehay GL , Deschler T , Rogers LF, Neiman HL.
Hendrix RW. The ultrasonographic characterization
of tendonds. Invest Radiol 1984:19:338-341
3. Fornage BD , Schernberg FL , Rilkin MD. U1trasound
exam ination of the hand. Radiology
1985: 155:785-788
4. Blei CL , Nirschl RP , Grant EG. Achilles tendon:US
diagnosis of pathologic conditions. Radiology
1986;159:765-767
5. Harcl‘e HT , Grissom LE , Finkelstein MS. Evaluation
of the musculoskeletal system with sonography.
AJR 1988: 150: 1253-1261
6. Gardner E , Gray DJ , 0 ’ Rahilly R. Anatomy. 4th Ed
Philadelphia:W B Saunders company. 1975;28-29
7. 대한정형외과학회. 정형외과학. 서울 최신의학사, 1982 : 311-315
8. Turek SL. Orthopedics. Principles and their applica
tion , vol 2. 4th Ed. Philadelphia:Lippincot t,
1984;931-932
9. Juan Rosa i. Ackermann ’s surgical pathology. vol .
7th Ed. S t. Louis:Mosby , 1989;1520-1522
10. Robbins CK. Robbins pathologic bases of disease.
4th Ed. Philadelphia:WB Saunders company ,
1989‘ 1361-1363
11. Jeffrey RB. Jr, Laing FC , Schechter WP , Markison
RE , Barton RM. Acute suppurative tenosynovitis of
th e hand :Diagnosis with US. Radiology
1987; 162:741-742
12. Stephenson CA. Seibert JJ , McAndrew MP , Glasier
CM , Leitheser RE , J r.‘ Iqbal V. Sonographic
diagnosis oftenosynovitis ofthe posterior tibial ten
don. J Clin U1trasounjd 1990;18: 114-116
- 279-

Journal of Korean Rad i이 og ica l Society 1992 ; 28 (2) : 275 "'-'280
<국문 요약 〉
사지 건초염의 초음파 진단
한럼대학교 의과대학 진단방사선과학교실
서귀숙·엄효근 ·이인재·이길우·배상훈·이경환
사지의 건염 혹은 건초염은 드물지 않은 질환이나 비특이적 임상소견으로 인하여 진단이 어렵고 과거에는 거의 영상진
단의 대상에서 제외되어 왔다. 최근 고해상력 초음파검사의 도움으로 이 질환의 수술전 영상진단이 시도되고 있는 바, 저
자들은 건 혹은 건 주위의 병변을 의심하여 초음파 검사를 하였던, 건초염 18예를 포항한 27명의 환자군을 대상으로 역행
적 연구를 시행하여 건초염의 초음파 소견을 관찰하고 각 소견의 진단적 가치에 대하여 검토하였다.
전체적인 진단율은 8L 1%였고 흔한 초음파 소견으로는 건의 국소적 종창이 있고 건의 외연이나 건 섬유의 평행한 배열
이 유지되어 있으며, 병변부위의 에코의 불규칙한 변화, 삼출액 등이 관찰되었으며 이중 단독소견으로는 삼출액만이 건초
염 진단에 、통계적으로 유의한 수치를 나타냈다(p<O.05). 건초염의 진단에 있어서 초음파 검사가 유용하며 단독 소견으로
삼출액이 진단적 가치가 있으나 그 낮은 민감도로 인하여 삼출액을 통반하지 않은 건초염과 양성 종양의 감별에는 초음파
검사만으로는 불충분하다.
- 280-