Solitary cystic mediastinal lymphangioma · 2013-02-18 · Solitary cystic mediastinal lymphangioma...
3
Solitary cystic mediastinal lymphangioma To the Editor: Solitary cystic mediastinal lymphangioma (CML) is a very uncommon benign vascular tumour developed from lympha- tic vessels. Cystic lymphangioma is a cyst caused by a congenital malformation of the lymphatic vessels and can affect any site in the body, but ,1% of lymphangiomas are mediastinal [1] and pulmonary lesions are even less common. They are most often located in the anterior mediastinum. We report a case of anterior CML in a 16-yr-old male, with a short review of the literature. A 16-yr-old male was admitted to the Thoracic Oncology unit (Ho ˆ pital Nord, Marseilles, France) for recurrent left pleural effusion. The patient reported a 6-month history of chest pain and dyspnoea with hyperthermia. An initial diagnosis of left empyema was suspected. It was managed by iterative thoracentesis with saline pleural lavages, antibiotics and physiotherapy. On admission, physical examination was unremarkable except for left-sided dullness on percussion. The patient was afebrile. Chest radiography revealed a large basal opacity of the left lung silhouetting out the heart and diaphragm. Initially, this opacity was thought to represent a recurrent pleural effusion (fig. 1a). Computed tomography scans revealed a cystic lesion in the left basithoracic and anterolateral pleura with smooth borders measuring 63690 mm (fig. 1b). No other intra- or extrapulmonary cystic lesions were found. With a presumptive diagnosis of a pleuropericardial cyst, video-assisted thoracic surgery was performed. Cytology and bacteriology were performed. The cyst contained serous fluid and had no connection or adhesion to adjacent organs, and was vascularised by small vessels from the mediastinal parietal pleura. Resection of the mass was performed. Histologically, the cyst wall was fibrous and lined by smooth muscle cells and by a single layer of flattened endothelial cells (fig. 2a). The margins of the resection were free from tumour. The lack of red blood cells in the cyst contents excluded haemangioma (fig. 2b and c). The final histological diagnosis was cystic lymphangioma. The post- operative clinical course was satisfactory, without complica- tions and without recurrence, as documented by repeat computed tomography after 43 months of follow-up. We hereby report the incidental finding of a solitary pleural- based pulmonary lymphangioma of the anterior mediastinum. CML is a rare benign vascular tumour that represents 0.7–4.5% of mediastinal tumours [1, 2]. More than 90% of CML is found in the first 2 yrs of life, 60% before the age of 5 yrs and only exceptionally in adulthood. To our knowledge, only few cases have been reported [1–4]. It has been described in cases of chromosomal and Mendelian abnormalities such as Turner syndrome, Down syndrome, and trisomy 13 and 18. CMLs are haemodynamically inactive, mature tumours with a low potential for carcinogenesis [1, 5]. Cystic lymphangiomas were first described by Wernher in 1843 [6]. The first case of chest wall lymphangioma was reported in 1973 [6]. Cystic lymphangioma is a congenital malformation that probably results from sequestration of lymphatic tissue that fails to communicate with the rest of the lymphatic system [1, 7]. The symptoms are based on the size and location, and vary widely, ranging from an acute mass syndrome to chest pain or local complication (rupture, infection, cystic haemorrhage or superior vena cava syndrome) [8]. Others have implicated specific factors such as infection, tumour or trauma [9]. According to the classification by Landing and Farber [10], lymphangiomas are classified into three types including: simple or capillary lymphangioma, cystic lymphangioma, and cavernous lymphangioma. Capillary lymphangiomas a) b) FIGURE 1. a) Chest radiography showing a large basal opacity of the left lung silhouetting out the heart border and left hemidiaphragm, causing mediastinal shift. b) Chest computed tomography showing an anterolateral fluid collection located in the base of the left lung with smooth borders measuring 63690 mm and causing regional atelectasis. c EUROPEAN RESPIRATORY REVIEW VOLUME 22 NUMBER 127 91
Transcript of Solitary cystic mediastinal lymphangioma · 2013-02-18 · Solitary cystic mediastinal lymphangioma...

Solitary cystic mediastinal lymphangiomaTo the Editor:
Solitary cystic mediastinal lymphangioma (CML) is a veryuncommon benign vascular tumour developed from lympha-tic vessels. Cystic lymphangioma is a cyst caused by acongenital malformation of the lymphatic vessels and canaffect any site in the body, but ,1% of lymphangiomas aremediastinal [1] and pulmonary lesions are even less common.They are most often located in the anterior mediastinum. Wereport a case of anterior CML in a 16-yr-old male, with a shortreview of the literature.
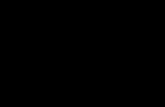
A 16-yr-old male was admitted to the Thoracic Oncology unit(Hopital Nord, Marseilles, France) for recurrent left pleuraleffusion. The patient reported a 6-month history of chest painand dyspnoea with hyperthermia. An initial diagnosis of leftempyema was suspected. It was managed by iterativethoracentesis with saline pleural lavages, antibiotics andphysiotherapy. On admission, physical examination wasunremarkable except for left-sided dullness on percussion.The patient was afebrile. Chest radiography revealed a largebasal opacity of the left lung silhouetting out the heart anddiaphragm. Initially, this opacity was thought to represent arecurrent pleural effusion (fig. 1a). Computed tomographyscans revealed a cystic lesion in the left basithoracic andanterolateral pleura with smooth borders measuring63690 mm (fig. 1b). No other intra- or extrapulmonary cysticlesions were found. With a presumptive diagnosis of apleuropericardial cyst, video-assisted thoracic surgery wasperformed. Cytology and bacteriology were performed. Thecyst contained serous fluid and had no connection or adhesionto adjacent organs, and was vascularised by small vessels fromthe mediastinal parietal pleura. Resection of the mass wasperformed. Histologically, the cyst wall was fibrous and linedby smooth muscle cells and by a single layer of flattenedendothelial cells (fig. 2a). The margins of the resection werefree from tumour. The lack of red blood cells in the cystcontents excluded haemangioma (fig. 2b and c). The finalhistological diagnosis was cystic lymphangioma. The post-operative clinical course was satisfactory, without complica-tions and without recurrence, as documented by repeatcomputed tomography after 43 months of follow-up.
We hereby report the incidental finding of a solitary pleural-based pulmonary lymphangioma of the anterior mediastinum.CML is a rare benign vascular tumour that represents 0.7–4.5%of mediastinal tumours [1, 2]. More than 90% of CML is foundin the first 2 yrs of life, 60% before the age of 5 yrs and onlyexceptionally in adulthood. To our knowledge, only few caseshave been reported [1–4]. It has been described in cases ofchromosomal and Mendelian abnormalities such as Turnersyndrome, Down syndrome, and trisomy 13 and 18. CMLs arehaemodynamically inactive, mature tumours with a lowpotential for carcinogenesis [1, 5].
Cystic lymphangiomas were first described by Wernher in 1843[6]. The first case of chest wall lymphangioma was reported in1973 [6]. Cystic lymphangioma is a congenital malformation that
probably results from sequestration of lymphatic tissue that failsto communicate with the rest of the lymphatic system [1, 7]. Thesymptoms are based on the size and location, and vary widely,ranging from an acute mass syndrome to chest pain or localcomplication (rupture, infection, cystic haemorrhage or superiorvena cava syndrome) [8]. Others have implicated specific factorssuch as infection, tumour or trauma [9].
According to the classification by Landing and Farber [10],lymphangiomas are classified into three types including:simple or capillary lymphangioma, cystic lymphangioma,and cavernous lymphangioma. Capillary lymphangiomas
a)
b)
FIGURE 1. a) Chest radiography showing a large basal opacity of the left lung
silhouetting out the heart border and left hemidiaphragm, causing mediastinal shift.
b) Chest computed tomography showing an anterolateral fluid collection located in
the base of the left lung with smooth borders measuring 63690 mm and causing
regional atelectasis. cEUROPEAN RESPIRATORY REVIEW VOLUME 22 NUMBER 127 91

consist of dilatation of capillary-sized lymphatic vessels, whichare connected to a normal lymphatic network. The cavernousvariant contains dilated lymphatic sinuses in an activelygrowing lymphoid stroma, which are also connected to normallymphatics. Cystic lymphangioma is characterised by multiplelarge cyst-like spaces lined by flat endothelial cells that may beempty or filled with clear proteinaceous or chylous fluidcontaining lymphocytes and, sometimes, red blood cells [3, 11].
A retrospective, multicentre study showed that in childhood,adolescence and young adults, lymphangiomas occupy cervicalor mediastinal sites in phrenic chains and are often entangled withvenous elements. This location along the pre-vascular phreniclymph nodes makes surgical dissection difficult. Entanglementwith vascular elements suggests a congenital origin [4].
In the past, lymphangiomas were distinguished from haeman-giomas by the lack of intraluminal blood. However, corebiopsies of lesion tissue using immunohistochemical andelastin staining are more useful in identifying lymphangiomasfrom other types of lesions [9].
The lymphatic nature of these lesions is sometimes difficult todemonstrate histopathologically, as it requires immunohisto-chemistry. A new monoclonal antibody, D2-40, which reacts
specifically with the lymphatic endothelium, can now be used.In this case, the endothelial-like lining cells of the cysts werepositive for D2-40, establishing the lymphatic nature of theselesions. To our knowledge, there are few reports of cases oflung solitary lymphangioma with immunohistochemical con-firmation using the monoclonal antibody D2-40 [11, 12].
The anterior mediastinal seats of our case tend towardconfusion with other tumours, such as a specifically localcongenital thymic cyst, a cyst or a bronchogenic teratoma.Similarly, a low anterior location would suggest a pleuroper-icardial cyst. The presence in the cyst walls of smooth musclecells and lymphoid nodules can rectify the diagnosis.
The treatment of choice for cystic pulmonary lymphangioma issurgical resection [1, 11, 13]. The chances of recurrence are lowif resection is complete and recurrence is common otherwise(35% versus 6% recurrence in case of complete resection) [4].
Complete resection may occasionally be difficult because ofclose proximity to vital structures [14, 15]. Other treatmentmodalities have been reported, such as marsupialisation,injection of sclerosing agents, steroids, diathermy and radio-therapy in unresectable cases, but they are generally ineffectiveand may lead to haemorrhage and infection [13].
a) b)
c)
FIGURE 2. Histopathology of a) smooth muscle cells, b) fibrous cystic walls
surrounding adjacent lymphatic and vascular structures, and c) a nonspecific
inflammatory reaction with a predominance of mononucleated lymphocytic cells.
92 VOLUME 22 NUMBER 127 EUROPEAN RESPIRATORY REVIEW

In conclusion, primary pulmonary lymphatic disorders orneoplasms are rare and are often difficult to diagnose andclassify [2]. Lymphatic abnormalities frequently mimic otherpathologic processes, particularly neoplastic processes. Theselesions are benign (as malignant change has not beendocumented) but tend to infiltrate surrounding tissues [8].Provided that the tumour is completely resected, recurrencesare rare. We believe this case adds a significant contribution tothe literature due to its rarity and unusual location.
Nataliya Khobta*, Pascale Tomasini*,#, Delphine Trousse#,",
Fabien Maldonado+, Pascal Chanez#,1 and Philippe Astoul#,e
*Dept of Multidisciplinary Oncology and Therapeutic
Innovations, Assistance Publique - Hopitaux de Marseille,
Hopital Nord, "Dept of Thoracic Surgery, Assistance Publique
- Hopitaux de Marseille, Hopital Nord, 1Dept of Ambulatory
Platforms in Pneumology, Assistance Publique - Hopitaux de
Marseille, Hopital Nord, eDept of Thoracic Oncology, Pleural
Diseases and Interventional Pulmonology, Assistance Publique
- Hopitaux de Marseille, Hopital Nord, and #Aix-Marseille
Universite, Marseilles, France. +Division of Pulmonary and
Critical Care Medicine, Mayo Clinic, Rochester, MN, USA.
Correspondence: N. Khobta, Dept of Multidisciplinary
Oncology and Therapeutic Innovations, Hopital Nord,
Universite de la Mediterranee, Chemin des Bourrely, 13915
Marseille Cedex 20, France. E-mail: [email protected]
Statement of Interest: P. Chanez has provided consultancyservices for Almirall, Boehringer Ingelheim, Centocor,GlaxoSmithKline, Merck Sharp & Dohme, AstraZeneca,Novartis, Teva, Chiesi and Schering Plough; has served onadvisory boards for Almirall, Boehringer Ingelheim, Centocor,GlaxoSmithKline, AstraZeneca, Novartis, Teva, Chiesi,Schering Plough and Merck Sharp & Dohme; has receivedlecture fees from Almirall, Boehringer Ingelheim, Centocor,GlaxoSmithKline, AstraZeneca, Novartis, Teva, Chiesi,Schering Plough and Merck Sharp & Dohme; and hasreceived industry-sponsored grants from Almirall,Boehringer Ingelheim, Centocor, GlaxoSmithKline,AstraZeneca, Novartis, Teva, Chiesi and Schering Plough.
Provenance: Submitted article, peer reviewed.
Acknowledgments: The authors would like to acknowledgeM-J. Payan (Hopital Nord, Marseilles, France) for her expertinterpretation of the histopathology specimens.
REFERENCES1 Minato H, Kaji S, Kinoshita E, et al. Solitary intrapulmonary cystic
lymphangioma in an infant: a case report with literature review.Pathol Res Pract 2006; 2010: 851–856.
2 Green NA, Diaz MC. Pulmonary lymphangioma in a 14-month-old. Pediatr Emerg Care 2011; 27: 52–54.
3 Riquet M, Briere J, Le Pimpec-Barthes F, et al. Les lymphangiomeskystiques du cou et du mediastin: existe-t-il des formes acquises?A propos de 37 cas [Cystic lymphangioma of the neck andmediastinum: are there acquired forms? Report of 37 cases]. Rev
Mal Respir 1999; 16: 71–79.
4 Boateng P, Anjum W, Wechsler AS. Vascular lesions of themediastinum. Thorac Surg Clin 2009; 19: 91–105.
5 Torcasio A, Veneroso S, Amabile MI, et al. Cystic hygroma of thebreast: a rare lesion. Tumori 2006; 92: 347–345.
6 Zakaria RH, Barsoum NR, El-Basmy AA, et al. Imaging ofpericardial lymphangioma. Ann Pediatr Cardiol 2011; 4: 65–67.
7 Cheng LH, Wells FC. A multidisciplinary approach to recurrentcervico-thoracic cystichygroma in an adult. Br J Oral MaxillofacSurg 2004; 42: 66–68.
8 Weissferdt A, Moran CA. Primary vascular tumors of the lungs: areview. Ann Diagn Pathol 2010; 14: 296–308.
9 Benninghoff MG, Todd WU, Bascom R.; Incidental pleural-basedpulmonary lymphangioma. J Am Osteopath Assoc 2008; 108: 525–528.
10 Balakrishnan A, Bailey CM. Lymphagioma of the tongue. Areview of pathogenesis, treatment and the use of surface laserphotocoagulation. J Laryngol Otol 1991; 105: 924–929.
11 Copcland J, Muller KM, Muller AM. Pulmonary haemangio-lymphangioma – a new entity of pulmonary vascular tumours?Histopathology 2008; 52: 527–529.
12 Nakajima J, Goto A, Takamoto S, et al. Invasive lymphangioma ofthe lung manifesting as a large pulmonary mass with hemoptysis:report of a case. Surg Today 2007; 37: 418–422.
13 Celikten A, Melek H, Citak N, et al. Minimally invasive excision ofmultiple cystic lymphangiomas of the mediastinum: a case report.Thorac Cardiovasc Surg 2010; 58: 498–500.
14 Limmer S, Krokowski M, Kujath P. Pulmonary lymphangioma.Ann Thorac Surg 2008; 85: 336–339.
15 Singh O, Singh Gupta S, Upadhyaya VD, et al. Cystic lymphan-gioma of the breast in a 6-year-old boy. J Pediatr Surg 2009; 44:2015–2018.
DOI: 10.1183/09059180.00002212
Pulmonary toxicity after long-term treatment with
lenalidomide in two myeloma patientsTo the Editor:
A white male was diagnosed with immunoglobulin G k-chainmultiple myeloma at age 63 yrs. He initially received acombination of thalidomide, doxorubicin and dexamethasonewith concomitant radiotherapy (30 Gy) to the dorsal vertebrae.The first course of this combination was complicated by
profound pancytopenia and lobar pneumonia with severe
sepsis in the setting of neutropenia, leading to the discontinua-
tion of thalidomide because of concerns regarding haematolo-
gical toxicity. The pneumonia was not microbiologically
documented but considered as being probably of bacterial
origin given the clinicoradiological presentation and a satisfying cEUROPEAN RESPIRATORY REVIEW VOLUME 22 NUMBER 127 93