Sodium and Water homeostasis
66
-
Upload
abhijit-nair -
Category
Documents
-
view
18.493 -
download
1
Transcript of Sodium and Water homeostasis


Sodium -> the most abundant cation of ECF
Sodium salts -> important part of osmotically active solutes in plasma & interstitial fluid
The amount of sodium in the body -> a prime determinant of ECF volume
The amount of sodium excreted = amount of sodium ingested over a wide range of dietary intakes allowing individuals to stay in sodium & volume balance

Regulatory systems Detects ECF volume changes Detects Sodium concentration
Modify rate of sodium
absorption/excretion
SODIUM HOMEOSTASIS

In perioperative period, adequate sodium maintenance is 1-2 meq/kg/day
Renal conservation of sodium is extraordinary
Even in profound volume depletion, urine losses may be < 1 meq/kg/day
Kidneys, Colon, sweat ducts, salivary glands control salt & water excretion &/or reabsorption : courtesy ALDOSTERONE

KIDNEY -- > Most important in homeostasis
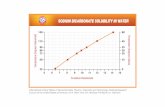
At a GFR of 125 ml/ min & serum sodium -> 145 mmol/L , kidney filters > 26 mol/ day of sodium ( 1.5 kg of NaCl )
More than 99% of filtered sodium is reabsorbed along nephrons

In KIDNEY :
Sodium is reabsorbed along different segments of nephrons :
1) PCT -> 50-75 % of filtered sodium reabsorbed via secondary active co transporters
2) Thin ascending loop of Henle doesn’t reabsorb sodium
3) Thick ascending loop of Henle reabsorbs 20-25%

4) Distal convoluted tubule: i) early DCT : 5-10% reabsorption by NaCl
co transporter ( remember THIAZIDES! ) ii) late DCT : 2-5% enters here * fine regulation, under control of
Aldosterone * here potassium sparing diuretics acts &
blocks sodium reabsorption
* Although sodium reaching here is a small fraction of filtered sodium, it is here where it is decided how much sodium will be excreted

Maintenance of a normal serum sodium concentration Control of Posm
Posm = 2 x serum sodium + glucose/20 + BUN/3
Serum sodium major determinant of Posm
Serum sodium alone provide no information about total sodium content
It only provides an estimate of relative amount of free water & sodium

Maintenance of Posm within normal limits depends on :
-> ability of kidney to excrete water, thus preventing hypo- osmolarity,
->Normal thirst mechanism with access to water to prevent hyponatremia

In presence of normal renal perfusion & intact renal function ,ADH is the principal Posm regulator
1-2% decrease in Posm -> inhibits ADH release, dilutes urine
1-2% increase in Posm -> 5-10 % decrease in blood volume or BP -> stimulates ADH release
When both Posm & BP decreases, the latter effect predominates resulting in increased ADH hypovolemia in hypovolemics

In elderly patients : Decreased GFR with age limits ability of
aged to excrete sodium prone to over expansion of ECF Hyponatremia
Impaired thirst mechanism with decreased ability to concentrate urine Hypernatremia


Hyponatremia
Na and Water deficit Water Excess Na and water excess
HypervolemicHypovolemic Euvolemic

Hyponatremia
Na and Water deficit Water Excess Na and water excess
HypervolemicHypovolemic Euvolemic
Renal LossesDiureticsMineralocorticoid deficiencyRTAKetonuriaSalt losing nephritisOsmotic diuretics
Extra-renal LossesGI lossesBurnsThird space losses eg sepsis, pancreatitis
Urinary Na > 20 mmol/L Urinary Na <10 mmol/L
Treat with Isotonic Saline

Hyponatremia
Na and Water deficit Water Excess Na and water excess
HypervolemicHypovolemic Euvolemic
Glucocorticoid deficiencyHypothyroidismSIADH
Urinary Na > 20 mmol/L
Water Restriction

Hyponatremia
Na and Water deficit Water Excess Na and water excess
HypervolemicHypovolemic Euvolemic
Nephrotic SyndromeCirrhosisCardiac Failure
Acute Renal FailureChronic Renal Failure
Urinary Na > 20 mmol/LUrinary Na <10 mmol/L
Na and Water Restriction



ADROGUE’ S FORMULA !


Maintenance a balance of water intake & output -> series of negative feedback loops involving endocrine system & autonomic system
60% of body is water
This amount of water is called TBW which remains fairly constant under normal circumstances

Water intake :- 2-2.5 lts / day ( in all forms ) Appr. 200 ml of water generated through
cell metabolism for 2.5 lts intake At the same time, water is lost through: -> Kidneys, lungs, GIT, Skin 1.5 lt as urine, 600 ml from skin, 300 ml as exhaled air ( the above two are included in insensible
losses) 100-200 ml by GIT

In healthy individuals, water homeostasis is accurately controlled, so that plasma osmolality (Posm) and its principal determinant, plasma sodium (Na) are maintained within a narrow range
This control is achieved by the close integration of water excretion and water intake
Water intake governed by -> sensation of thirst, mainly regulated by osmosensitive neurons located in the anterior hypothalamus

Thirst osmoreceptors possess an osmotic threshold, above which the sensation of thirst increases rapidly in direct proportion with Posm
Strong stimuli for water ingestion -> Hypovolaemia and hypotension detected by atrial and arterial baroreceptors
Oropharyngeal receptors &thirst regulation:-
stimulation of these receptors by water intake leads to an early satiation of thirst before Posm or plasma volume change


Disturbances of water homeostasis : i) Gain or loss of Extracellular volume, ii) Gain or loss of solute
Examples of disturbances : 1) Hypervolemia, 2) Overhydration, 3) Hypovolemia, 4) Dehydration

Hypervolemia :
Too much water & solute taken at the same time
ECF volume increases, Posm remains normal
Overhydration :
Too much water taken without solute ECF volume increases, Posm decreases as
solute is absent

Hypovolemia :
Water & solute are lost at the same time There is loss of plasma volume Posm is normal
Dehydration :
Water is lost but not the solute There is loss of volume, but as solutes are
not lost in same proportion, Posm increases

Examples :
1) Blood loss : Hypovolaemia ( water & solute loss)
2) Sweating : Dehydration ( water lost , with some solute)
3) Increased intravascular volume : Hypervolemia
( increased water & solute) 4) Polydipsia : Over hydration

Water excretion :
By kidneys :- Reabsorption, Secretion, Glomerular filtration

Kidneys -> an organ of both conservation and excretion
Conserves solutes and water needed by the body, simultaneously excretes excess solutes and metabolic wastes
The functional unit of the kidney is the nephron:
composed of a glomerulus, proximal tubule, loop of Henle, distal tubule, and collecting duct


Water excretion depends on :
hypothalamic osmoreceptors :- responds to changes in Posm
atrial and carotid bifurcation baroreceptors :- responds to changes in blood pressure or blood volume
release of the antidiuretic hormone vasopressin (VP), via the hypothalamic-neurohypophyseal axis

Absorption of 75% of filtered water :- passively in the proximal tubule along
osmotic gradients established by the active transport of solutes such as sodium, potassium, bicarbonate, amino acids, and glucose
Obligatory water reabsorption occurs in the proximal tubule regardless of the body’s actual need for water

Isotonic fluid leaves the proximal tubule to enter the descending loop of Henle
The cells of thin descending limb are highly permeable to water, with limited permeability to other molecules(sodium,urea)
Tubular fluid :increasingly concentrated in the descending limb (as water is extracted from the tubule lumen by the high interstitial osmolality)

The entire ascending limb of the loop of Henle is impermeable to water
Passive diffusion of sodium into the interstitium in the thin portion of the ascending limb, active transport of chloride and sodium occurs in the thick ascending limb
The result of the outward movement of solutes and the restricted movement of water : a decrease in the osmolality of the fluid entering the distal tubule

The primary role of the loop of Henle : to provide a hyper osmotic medullary interstitium with which urine equilibrates during its passage through the collecting duct
Medullary hypertonicity is generated and maintained by the sodium chloride pump in the thick ascending limb, passive sodium chloride transport out of the thin ascending limb, and urea transport from the inner medullary collecting duct

In the proximal part of the distal tubule; sodium, chloride and water are reabsorbed independently of the VP concentration
The adjustment of water reabsorption needed to maintain the body water balance occurs in the latter parts of the distal tubule and in the collecting duct, and depends on the release and action of the hormones aldosterone and VP

Aldosterone, as part of the renin-angiotensin system, stimulates sodium and water reabsorption, and potassium secretion
Vasopressin facilitates the diffusion of water into the interstitium, as well as the diffusion of urea in the inner medullary collecting duct
Thus, the final concentration of urine is determined by the permeability of the collecting duct to water

The discovery of the aquaporin-1 (AQP1) water channel by Agre and colleagues ,which led to the Nobel Prize in 2003, revolutionized the understanding of body fluid water regulation by the kidney
AQP2,3, and 4, along with urea and ion transporters, has allowed a much improved understanding of urinary dilution and concentration in health and disease at the cellular and molecular levels

AQP : provided a pathway for water movement across cellular membranes that could not be explained by simple diffusion through the lipid bilayers of cell membranes
AQP1: found to be expressed on the apical and the basolateral membranes of the proximal tubule and descending limb of Henle’s loop
AQP channel : not under control of vasopressin but is important in urinary concentration
Water efflux through these channels in the descending limb is an important factor in the countercurrent concentrating mechanism

AQP2, 3, and 4 expressed in the cortical and medullary collecting duct
AQP2 exclusively in the principal cells of the collecting tubule and collecting duct and is known to be regulated by arginine vasopressin (AVP)
AQP3 and 4 located on the basolateral membrane of the principal cells in the collecting duct


Thus there are four primary mechanisms regulate fluid homeostasis:
- ADH, - Thirst, - Aldosterone, - Sympathetic nervous system Out of the above 4, three mechanisms
are in the kidney


Acute renal failure (ARF) : a common complication of critical illness, associated with high mortality and has a separate independent effect on the risk of death
Despite several advances in treatment and in our understanding of the pathogenesis of ARF, many aspects in this field, including fluid management remain subject to controversy, confusion and lack of consensus




optimization of the haemodynamic status
and correction of any volume deficit will have a salutary effect on kidney function
will help minimize further extension of the kidney injury and will potentially facilitate recovery from AKI with minimization of any residual functional impairment
AKI is characterized by a continuum of volume responsiveness and/or unresponsiveness

The term used nowadays are : ‘volume-responsive AKI’ and ‘volume-
unresponsive AKI’ Volume-responsive AKI was previously
called pre-renal acute renal failure (ARF). Renal hypovolaemia : the most important
cause of volume-responsive AKI, particularly in patients outside the ICU
Here, organ perfusion and renal function will improve with volume loading

In volume unresponsive AKI, renal perfusion is suboptimal despite adequate circulating volume, or even volume overload
E.g. serious congestive heart failure or diastolic dysfunction
Here, fluid loading will not result in improved kidney perfusion, and might even lead to pulmonary edema , further worsening of cardiac function ,affect organ perfusion

In still other situations, the patient may already be fluid overloaded, but the intravascular circulating volume is reduced
E.g. in sepsis, cirrhosis of liver, other diseases causing third spacing

AKI :- A complex syndrome, defined as an
abrupt change in serum creatinine &/or urine output & classified according to RIFLE ( risk, injury, failure, loss & end stage kidney disease ) criteria, further refined by AKIN ( Acute Kidney Injury Network )
• AKI is commonly & increasingly encountered in patients with critical illness
• Correct fluid therapy is the cornerstone of prevention & management of critically ill patients of AKI

Cumulative positive balance has a negative impact on outcomes
Beneficial therapeutic in established AKI: - Rapid resuscitation - Removal of stimulus contributing to AKI - Judicious avoidance of complications - Allowing time for recovery

In patients with AKI &/or oliguria, a positive fluid balance is almost universal
Payers et all, in SOAP ( Sepsis Occurance in Acutely Ill patients ) study, quoted that there is independent relation between mortality & positive fluid balance in a cohort of critically ill patients with AKI

Principles of fluid management in AKI :
Correction of hypovolemia, In presence of fluid overload -> -> Diuretics, -> Fluid restriction, ->Minimise drug infusion volumes, Closely monitor I/O, Daily weight ( if possible ), Dialysis

AIM : ISOVOLEMIA !
RULE OF THUMB : Fluid therapy should be equal to
insensible losses + output ( Urine, drains, diarrhea )
Insensible losses : 1- 10 kg -> 25 ml/kg. 10-20 kg -> 12.5 ml/kg. > 20 kg -> 5 ml/ kg.

Insensible losses increases : By 12 % for 1 degree increase above 37.5, 10-25 % if sweating, 25-50 % if hyperventilating, 25-75 % if hyper metabolic, 25 % in presence of radiant heater/
phototherapy
Insensible losses decreases in : Oedema / antidiuretic state Paralysed / deeply sedated patients Humidified atmosphere

Choice of fluid : Crystalloids, Colloids ( Starches, gelatins, albumin )
Hydroxyethylstarch (HES) : a widely used, cheap alternative to albumin
Different HES preparations available they vary with regard to : concentration, mean molecular weight (Mw), molar substitution, substitution of hydroxyethyl for hydroxyl
groups

Problems :
Renal dysfunction Interferes with coagulation Recommendation : ‘HES should be avoided in ICUs and during
the perioperative period’ (Vincent JL. Fluid resuscitation: colloids vs crystalloids.
Acta Clin Belg Suppl 2007; 62: 408–411)

A recent trial compared a ‘modern’ HES preparation with a low Mw and low molar substitution and a HA solution, in cardiac surgery patients with preoperative compromised kidney function
Result :this type of HES solution had no negative influence on kidney integrity
(Boldt J, Brosch C et al. Influence of volume therapy with a modern HES preparation on kidney function in cardiac surgery patients with compromised renal function: a comparison with human albumin. Crit Care Med 2007; 35: 2740–2746)

In the VISEP study in severe sepsis, patients were randomly given 10% pentastarch solution, a low Mw HES 200/0.5 or modified Ringer’s lactate for fluid resuscitation.
Although the mortality was not significantly different, the HES group had a significantly higher rate of AKI (34.9 versus 22.8%,) and more days on which RRT was required
(Brunkhorst FM, Engel C, Bloos F et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med 2008; 358: 125–139)

Message : Its important to distinguish between
disorders of osmoregulation & disorders of volume regulation since water & sodium balance are regulated independently
Changes in sodium concentration generally reflects disturbed water homeostasis
Alteration in sodium content manifests as ECF volume contraction or expansion

AKI is lethal, remember the situations that predisposes it & take due steps
Multidisciplinary approach ( patients safety first )