Reporting systematic reviews and meta-analyses (PRISMA) and observational studies (STROBE)
ty
Patient Education and Counseling xxx (2013) xxxxxx
G Model
PEC-4612; No. of Pages 10
Contents lists available at ScienceDirect
Patient Education
jo ur n al h o mep ag e: w ww .e lseRosanna Stopford *, Kirsty Winkley, Khalida Ismail
Institute of Psychiatry, Kings College London, London, UK
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
2. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
3.1. Exposure measurements. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
3.2. Outcome measurement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
4. Discussion and conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
4.1. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
5. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
5.1. Practice implications. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
1. Introduction
Social support is an important explanatory variable with pro-gnostic signicance for health outcomes [13]. The self-management
of type 2 diabetes mellitus (T2DM) is cornerstone to achieving goodglycemic control and reducing the risk of developing microvascular(retinopathy, nephropathy and neuropathy) and macrovascular(cardiovascular and cerebrovascular disease) complications. Themanagement of diabetes necessitates an active role of the patient.This involves lifestyle modications such as improving diet, increasingphysical activity, self monitoring of health status (blood glucose andexamination of feet), acquisition of diabetes knowledge as well asadherence to professional advice.
Recently, there has been an increase in research into thesupportive role of healthcare professionals, diabetes education and
A R T I C L E I N F O
Article history:
Received 2 April 2013
Received in revised form 12 July 2013
Accepted 13 August 2013
Keywords:
Systematic review
Social support
Type 2 diabetes mellitus
HbA1c
A B S T R A C T
Objective: We aim to systematically review observational studies examining the association between
social support and glycemic control in adults with type 2 diabetes.
Methods: We searched MEDLINE, PsycINFO, EMBASE, Scopus, Web of Science and Sociological Abstracts
to July 2012 for observational studies investigating the association between structural or functional
aspects of social support (social networks, community ties, marital status, family support, perceived,
actual, emotional or instrumental social support) and glycemic control (HbA1c).
Results: From electronic and reference searches, 29 studies were eligible. Twenty different assessments
of social support were used. Family support and composite measures of support were most frequently
associated with reduced HbA1c. There was no evidence for a benecial effect of other support measures
on HbA1c.
Conclusion: We found marked variation in population, setting, measurement of social support and
denition of outcome, limiting the methodological validity of research. Social support may be important
in the management of type 2 diabetes, the need for consensus and standardization of measures is
highlighted.
Practice implications: The presence of informal support should be explored in routine diabetes care.
2013 Elsevier Ireland Ltd. All rights reserved.
* Corresponding author at: Kings College London, Institute of Psychiatry, Weston
Education Centre, 10 Cutcombe Road, London SE5 9RJ, United Kingdom.
Tel.: +44 0207 848 5665; fax: +44 0207 848 5668.
E-mail addresses: [email protected], [email protected]
(R. Stopford).
0738-3991/$ see front matter 2013 Elsevier Ireland Ltd. All rights reserved.http://dx.doi.org/10.1016/j.pec.2013.08.016Review
Social support and glycemic control in review of observational studiesPlease cite this article in press as: Stopford R, et al. Social support aobservational studies. Patient Educ Couns (2013), http://dx.doi.org/1pe 2 diabetes: A systematic
and Counseling
vier . co m / loc ate /p ated u co und glycemic control in type 2 diabetes: A systematic review of0.1016/j.pec.2013.08.016
R. Stopford et al. / Patient Education and Counseling xxx (2013) xxxxxx2
G Model
PEC-4612; No. of Pages 10patient participation groups in the management of T2DM; supportthat can be classied as formal. The role of more informalinterpersonal relations in diabetes care, that is, the presence orsupport provided by social networks or family members, has beenless studied. Social support comprises of structural and functionalelements [4]. These elements vary in their characteristics and intheir effects on health [5,6]. The structural aspects of support referto webs of social relationships and linkages which are bestmeasured through quantitative scoring of the size of networks orexistence of support resources (marital status, social networks andcommunity ties). Functional components (social support) areelicited from the structural basis of social relations [4]. Theexistence and quantity of social relationships do not necessarilyprovide social support, however they certainly increase thelikelihood of receiving help when needed. Social support functionsare more consistently associated with health outcomes thanstructural aspects of support [5]. However, not all support ishelpful. The term social support carries positive connotations.Social support may often be wanted, but can result in misconstruedsocial pressure, such as nagging or criticism, or unwanted(negative) outcomes [7].
In health, social support is purported to exert its inuence intwo main ways: (1) directly: providing necessary support to copewith health problems, adhere to self care-regimen and avoidpotentially negative situations (for example, economic problems)or (2) indirectly: acting as a buffer (protection) against the impactof stressful events [8].
In diabetes, both mechanistic routes of action may lead toimproved glycemic control. Social support is associated withincreased adherence to diabetes self care [915], however there isa lack of consensus as to whether this translates into improvedbiomedical outcomes. A recent meta analysis of six randomizedcontrolled trials (RCT) of formal supportive interventions (groupvisits to clinician, telephone and internet support, spouseinvolvement and family and friend support in interventions) forpatients with T2DM (pooled n = 712) tentatively reported favor-able results in diabetes self-management and biomedical out-comes [14]. Biomedical outcomes were assessed in four of the trialsand improved in two, although effects were seen in different bio-markers. HbA1c and lipids improved following group visits to theclinician [16] and BMI improved following spouse involvement indiabetes weight-management education in women only [17].Across trials, improvements were also seen in diabetes self care,quality of life and diabetes knowledge [1619].
There is some evidence to suggest that formal social support iseffective in improving glycemic control. However, RCTs articiallyintroduce social support. There is rich data available fromobservational studies which may allude to the, as yet unidentied,active ingredients of support. By using observational data tounderstand the active ingredient this can then be translated intoRCTs. Furthermore with increasing pressure on healthcaresystems, formalized support interventions are expensive toprovide, rigid and risk not engaging some individuals. On theother hand, informal support, such as that provided by signicantothers, friends and family, is free, readily available and specic tothe individual. Investigating these constructs in the context of longterm conditions such as T2DM may be important in the support ofself-management. Evidence from observational studies is the mainmethod by which to study such associations.
The social determinants of biomedical outcomes in T2DM is anunderstudied area. Due to the epidemic of T2DM and its increasingsocietal and economic burden, the need to identify non pharmaco-logical, cheap and modiable targets for intervention is increasing.Our aim is to systematically review published and unpublishedliterature investigating the association between INFORMAL socialsupport and glycemic control in adults with T2DM.Please cite this article in press as: Stopford R, et al. Social support aobservational studies. Patient Educ Couns (2013), http://dx.doi.org/12. Methods
Eligible studies were those meeting the following inclusioncriteria: observational studies (case control, cohort and cross-sectional studies) of adults (18 years of age) with T2DM or noninsulin dependent diabetes, that investigated the relationshipbetween social support and glycemic control; studies with aprimary or secondary emphasis on the association between socialsupport and glycemic control; studies utilizing measures assessingstructural and functional components of (informal) social support:marital status, family support, social networks, and communityties (involvement in social structures within the community),perceived, actual, instrumental (tangible assistance) or emotionalsocial support. Terms were chosen to cover a wide range of supportmeasures from a socio-ecological perspective. Studies measuringother types of social support were excluded. Any variables focusingsolely on formal professional support, support from healthcareproviders and support from diabetes education programs werealso excluded. Studies combining type 1 and T2DM were excludedunless data for T2DM were reported or could be obtained fromrespective authors. Studies that were purely descriptive in naturewithout the use of statistical analysis were excluded as thesestudies provide no data to quantify associations between socialsupport and glycemic control.
Our main outcome measure was long term glycemic controlbased on the percentage of glycated hemoglobin (HbA1c). In type 2diabetes the National Institute for Clinical Excellence (NICE) statesthat the target HbA1c should be between 6.5% and 7.5% (42 mmol/mol and 58 mmol/mol) based on individual risk for micro- andmacro-vascular complications [20].
The search strategy included several data sources. Electronicdatabase searches were carried out on the following databases:MEDLINE (19462012), EMBASE (19472012), PsycINFO (18062012), Scopus (19602012), Web of Science (18992012) andSociological Abstracts (19522012). Searches were run on the 11thJuly 2012. The search was restricted to studies of human beings butwas not restricted by language or publication year. Any duplicateresults were combined.
To capture the broadest sample of relevant studies weused multiple search terms. The following search terms wereused for MEDLINE and adapted for the other databases: expDiabetes Mellitus, Type 2 and exp social support or (social adjsupport).mp or exp Marital Status or (marital adj status).mp orexp Spouses or (social adj network).mp. or exp Family andHbA1*.mp. or glyc?emic control.mp or A1c.mp. or GHb.mp. orGlycoh?emoglobin.mp. or Glyc* h?emoglobin.mp. and expEpidemiologic Studies/or exp Case-Control Studies/or exp CohortStudies/or case control.tw. or (cohort adj (study or studies)).tw.or Cohort analy*.tw. or (follow up adj (study or studies)).tw. or(observational adj (study or studies)).tw. or longitudinal.tw.or retrospective.tw. or cross sectional.tw. or Cross-SectionalStudies/.
The reference lists of eligible studies were hand searched foradditional studies not identied by the search. Related reviewsretrieved in the search were also checked for relevant citations. Theconference proceedings of the American Diabetes Association,Diabetes UK and the European Association for the Study ofDiabetes from July 2009 to July 2012 were searched under social,psychological and behavioral sub headings. Leading authors in theeld were contacted for additional data on published or unpub-lished studies.
The abstracts and titles of studies identied by the searchstrategy were screened for potentially relevant studies by oneauthor (RS). Manuscripts included based on their abstract wereobtained as full text documents which were screened for potentialinclusion in the review. In the case of ambiguity, the full text wasnd glycemic control in type 2 diabetes: A systematic review of0.1016/j.pec.2013.08.016
associated with increased HbA1c. Eight studies reported noassociation between marital status and HbA1c [43,4547,4951,53].
Social networks: Four studies assessed the association betweensocial network size and HbA1c. Kaplan and Hartwell found norelationship between social network size and HbA1c at baselinebut at 18 months large social network size was found to beassociated with a reduction in HbA1c in men [38]. Conversely,Rothenbacher et al. found large social networks to be associatedwith increased HbA1c [54]. Two studies reported no signicantassociation between social network size and HbA1c [39,48]. Kaplanand Hartwell and Chlebowy and Garvin utilized the Social SupportQuestionnaire which additionally measures satisfaction withnetwork support. In a prospective study of a RCT cohort, supportwas signicantly associated with lower HbA1c in males butincreased HbA1c in females. No association was seen in change inHbA1c at 18 months follow up [38]. In their cross-sectional study,Chlebowy and Garvin [39] report no signicant associationbetween satisfaction with network support and HbA1c.
Family support: Choi et al. assessed family support using theDiabetes Family Behavior Checklist-II (DFBC-II). The DFBC dietsubscale, but not the exercise subscale, was independentlyassociated with lower HbA1c [40]. A smaller study by Mayberryet al. did not nd this association [44]. Perceived family supportassessed using the Family Support Scale (FSS) was associated withlower HbA1c levels [42]. Gender differences were reported in astudy of 152 patients in Taiwan [45]. Family support (FSS) wasindependently associated with higher HbA1c in females and lower
R. Stopford et al. / Patient Education and Counseling xxx (2013) xxxxxx 3
G Model
PEC-4612; No. of Pages 10retrieved. Any discrepancies were discussed and resolved throughconsensus with the co-authors (KW and KI).
For selected studies, we coded in a standardized manner thefollowing information (when available): country, number ofparticipants, type of study, setting and sampling method, age,gender, duration of diabetes, social support measure, outcomemeasure, confounding variables and the main ndings. An attemptwas made to retrieve missing or incomplete data from studies byfax or e-mail. Odds ratios (OR) standardized beta values werereported when possible. Otherwise, other measures of associationsor values of statistical signicance of the reported association weregiven. Studies often investigated a number of explanatoryvariables and dependent variables. Only associations includingsocial support measures are reported.
There is a lack of consensus regarding the optimal method ofassessing quality in observational studies [21]. All eligible studieswere included and quality was assessed. Quality was dened as thecondence that the design, conduct and analysis of each studyminimized bias in the estimation of the effect of the exposure onthe outcome. Quality assessment was based on checklist itemsfrom the prisma statement [22]. We assessed (I) description ofparticipant characteristics, (II) quality of study design, (III) methodof recruitment, (IV) validity of measures, (V) validity of outcomemeasurement and VI) controlled for confounding variables. Thequality of studies was not summarized using scores. Summaryscores are often problematic as weighting of component items anddomains are often variable and inconsistent across scales [23].Studies were considered to be of good quality if they used aprospective design, consecutive or random sampling of studyparticipants, utilized validated instruments for exposures, denedthe outcome and controlled for confounding variables.
3. Results
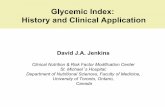
The search strategy yielded 874 studies. Reference searching,conference proceedings and expert advice identied a further 17studies and 90 studies were selected for full text review (Fig. 1).Data extraction from the full texts identied 23 studies from theelectronic database search, 4 manuscripts from the referencesearch and 2 abstracts from conference proceedings for inclusion.Reasons for exclusion from the review are shown in Fig. 1.
The studies included in the systematic review are listed inTable 1. Sixteen of the 29 studies were conducted in the UnitedStates and 4 were conducted in European countries, but not in theUK. Of the 29 studies included, the designs were: 25 cross-sectional, 3 cohort and 1 case control. The mean age of studypopulations ranged from 50.6 years to 69.2 years in the 26 studiesthat reported age, all but one study included both male and femalepopulations. Three studies did not report gender. Sample sizesranged from 53 to 2572 participants. The independent variable(social support) was assessed by self-report in all included studies.Measures of social support were varied, with little overlap acrossstudies. The most frequently used measures were multidimen-sional assessments of social support (measures that assessed morethan one component of social support) (n = 16) [2439]. Of these,13 studies generated a composite measure of social support and 3studies separated analysis by social support type [3739]. Sevenstudies investigated family support measures [4046], 10 assessedmarital status [43,4553], 5 studies assessed network size[38,39,42,48,54] and 1 assessed perceived social support [55].There were no studies that utilized measures of community ties orthat assessed stand-alone measures of actual, instrumental oremotional support although the latter were included in themeasure used by Kacerovsky-Bielesz et al. [37]. Five studies usedmore than one measure to assess social support [42,43,45,46,48].Eight studies assessed support specic to diabetes carePlease cite this article in press as: Stopford R, et al. Social support aobservational studies. Patient Educ Couns (2013), http://dx.doi.org/1[27,30,32,35,36,40,44,46] and two studies used measures of socialsupport specic to chronic disease [26,29]. We did not separateresults into functional and structural support due to heterogeneityin measurements of social support.
3.1. Exposure measurements
Marital status: Ten studies investigated the association betweenmarital status and glycemic control. Two studies report beingmarried [52] and living with a partner [48] to be independently
Titles and abstracts idened and scree ned
n = 891
Full texts retrieved for detailed review
n = 90
Excluded n = 80 1
Exclusions: n = 61
No me asure/ exc lud ed me asure of social supp ort n = 3 4No me asure of H bA1c n = 11Not m ain or seconda ry aim n = 5Combined type 1 and type 2 diab etes n = 4RCT n = 1Adolescent s n = 2Insucient data n = 2Dupli cate data n = 2
Studi es eli gible for inclusio n
n = 29
Fig. 1. Flow chart of the systematic review.nd glycemic control in type 2 diabetes: A systematic review of0.1016/j.pec.2013.08.016
Table 1Summary of studies included in the systematic review.
First author, year,
country.
Setting,
sampling
method
Sample size
(% women)
Age, mean
(SD/range)
Average duration
of diabetes years
(SD/range)
Measure of social
supportaAdjusted for
confounders
Measure of
glycemic
controlb (%)
Main ndingsc
Cross sectional study design
Mayberry, 2012,
USA
Primary care,
convenience
61 (69) 57.1 (8.6) 8.0 (6.1) Adapted version of the Diabetes
Family Behavior Checklist
(DFBC): family support in
diabetes
None HbA1c Unadjusted: no association between
DFBC and HbA1cf
Note: perceiving family members as
non supportive was associated with
poormedication adherence (r=0.44,
p7=poor control)
Unadjustede:
(1) Living with a partner was
associated with higher HbA1c
(p=0.002). Meeting with family
(p=0.9) or friends (p=0.64)>once a
month was not associated with
HbA1c.
(2) Social network function was not
associated with HbA1c (p=0.08)
Sukkarieh-Haraty,
2012, Lebanon
Outpatient,
convenience
140 (57.1) 1829=1.4%
3039=2.1%
4049=10%
5059=37.1%
6069=25%
>70=22.9%
05 years =34.3% 510
years =27.1% 1116
years =17.9% 17years =20.7%
Diabetes Care Prole: Social
support scale.
Age, sex, treatment,
diabetes associated
problems, BMI
HbA1c Social support was signicantly
associated with increased HbA1c
(beta =0.02, p=0.01).
Chew, 2011,
Malaysia
Primary care,
convenience
175 (66.3) 62.7 (10.8) 11.7 (6.7) (1) The Medical Outcomes Study
Social Support Survey: -
Structural support:
(2) number of supporters
Functional support:
(3) emotional/informational
support
(4) tangible support
(5) positive social interaction
(6) affectionate support
None HbA1c Unadjusted: no association between
social support and HbA1c.
(1) social support score (r=0.06,p=0.47)
(2) number of supporters (r=0.03,p=0.68)
(3) emotional/informational
support (r=0.06, p=0.46)(4) tangible support (r=0.03,
p=0.74)
(5) positive social interaction
(r=0.04, p=0.59)(6) affectionate support (r=0.04,
p=0.62)
Fortmann, 2011,
USA
Community,
convenience
208 (71) 50.6 (10.9) NR Chronic Illness Resource Survey
(CRIS): support received over 3
months from friends, family,
healthcare providers,
community and personal
support
None HbA1c Unadjusted: association between
CRIS and HbA1c (r=0.16, p
Table 1 (Continued )
First author, year,
country.
Setting,
sampling
method
Sample size
(% women)
Age, mean
(SD/range)
Average duration
of diabetes years
(SD/range)
Measure of social
supportaAdjusted for
confounders
Measure of
glycemic
controlb (%)
Main ndingsc
Kim, 2010, USA NR, NR 68 NR NR Perceived spouse support Sex- others NR HbA1c Perceived spouse support was
associated with HbA1c in males but
not femalesd
Pons, 2010, USA NR, NR 698/1427 NR NR Marital status NR Categorical HbA1c
(7/>7)Marital status was not a predictor
HbA1c0.05))
KacerovskyBielesz,
2009, Austria
Outpatient,
consecutive
257 (50.97) 64 (9) 14 (9) Berlin Social Support Scales
(BSSS):
(1) emotional
(2) instrumental
(3) informational
(4) support satisfaction
Socio-demographic,
disease-specic,
clinical and
anthropometric and
psychological
measures
HbA1c (1) Emotional support was
associated with HbA1c in males
(beta =0.516, p=0.007). No
association in femalesf.
(2) Instrumental support not
associated with HbA1c in men
(beta =0.33, p=0.07) or women.f(3) Informational support was not
associated with HbA1c in menf or
women.f
(4) Support satisfaction was not
associated with HbA1c in men
(beta =0.31, p=0.054) or womenfOkura, 2009, USA Community,
convenience.
1097 (51.9) 69.2 10 years =56.4%1120 years =24.7%
21 years =18.9%
Social support subsection of the
Diabetes Care Prole: how much
patients could count on family or
friends to helpwith diabetes care
Age, sex, ethnicity,
cognitive function
education, income,
insurance status, DD,
depression,
understanding of
diabetes,
hyperglycemic
treatment, functional
limitations,
comorbidity
Categorical HbA1c
(
Table 1 (Continued )
First author, year,
country.
Setting,
sampling
method
Sample size
(% women)
Age, mean
(SD/range)
Average duration
of diabetes years
(SD/range)
Measure of social
supportaAdjusted for
confounders
Measure of
glycemic
controlb (%)
Main ndingsc
Rahman, 2008,
Malaysia
Primary care,
stratied
random
219 (59.6) 55.6 (8.55) 6 (IQR=7) Marital status Occupation,
educational level,
smoking, FH, health
center with family
medicine specialist,
FBG, Cholesterol,
Triglycerides, HDL-
cholesterol, LDL-
cholesterol, BMI, sBP,
dBP
HbA1c Being married was associated with
increased HbA1c (beta =0.93, 95%
CI =0.43, 1.44)
Howteerakul, 2007,
Thailand
Tertiary care,
convenience
243 (65.8) 60.2 (3779) Median =7 (range=140
years)
Social support scale modied
from the Michigan Diabetes Care
Prole: support from family and
friends
None Categorical HbA1c
(7=good control)Unadjusted: high social support did
not display signicantly better
HbA1c than those with low social
support (OR 1.32, 95% CI 0.74, 2.36)
Misra, 2007, USA Primary care,
convenience
180 (52) 54.8 NR Personal Resource
QuestionnairePart II (PRQ8):
perceived social support and
adequacy of support
None Categorical HbA1c
(6.5 =good control)Unadjusted: more social support
was associated with better HbA1c
(p=0.04)
Chlebowy, 2006,
USA
Outpatient,
convenience
91 (56) 54.96 (12.5) 7.1 (6.5) Social Support Questionnaire:-
(1) Number of supportive
individuals (SSQN)
(2) Satisfaction with support
(SSQS)
None HbA1c Unadjusted:
(1) SSQN and HbA1c: no associationf
(2) SSQS and HbA1c: no associationf
Whittlemore, 2005,
USA
Outpatient,
consecutive
53 (100) 57.6 (10.9) 2.7 (3.0) Diabetes self-management
assessment tool (DSMART)
subscale: condence in diabetes
self management, family/friend
and professional support
BMI HbA1c Support was a signicant predictor
of HbA1c (beta =0.41, p=0.01)
Schillinger, 2002,
USA
Primary care,
consecutive
408 (58) 58.1 (11.4) 9.5 (8.0) Adapted version of the Diabetes
Care Prole: family and friend
support with diabetes
management
Age, sex, education,
insurance, language,
diabetes education,
depression, treatment,
DD, clustering within
physicians, health
literacy
HbA1c Social support was not a predictor of
HbA1c (beta =0.0002, p=0.99).
Ilias, 2001, Greece Outpatient,
convenience
98 (26.5) 57.1 (15.3) 10.4 (6.9) (1) Family Support Scale (FSS):
perceived family support
(2) The number of family
members
None HbA1c Unadjusted:
(1) Association between FSS and
HbA1c (r=0.41, p=0.05)(2) No association between the
number of family members and
HbA1c (r=0.10, p>0.05).
Blaum, 1999, USA. Primary care,
random
393 (54) 63 (11) 8.9 (7.8) Marital status None Categorical
(HbA1c11.6 =poorcontrol)
Unadjusted: no association between
marital status and HbA1cf
Peyrot, 1999, USA Outpatient,
convenience
61 (50.5) 53.3 (0.7) 8.2 (7.0) Marital status Sex, education, DD,
BMI.
HbA1c Marital status was not a predictor of
HbA1c (beta =0.02, p>0.05)
R.
Stopford
et al.
/ Patien
t Educatio
n and
Counselin
g xxx
(2013)
xxxxxx
6 G M
odel
PEC-4612;
No.
of
Pages
10
Please
cite th
is article
in press
as:
Stopford
R,
et
al.
Socia
l su
pport
and
glycemic
contro
l in
type
2 diabetes:
A sy
stematic
review
of
observatio
nal
studies.
Patie
nt
Educ
Couns
(2013),
http
://dx.doi.o
rg/10.1016/j.p
ec.2
013.08.016
Table 1 (Continued )
First author, year,
country.
Setting,
sampling
method
Sample size
(% women)
Age, mean
(SD/range)
Average duration
of diabetes years
(SD/range)
Measure of social
supportaAdjusted for
confounders
Measure of
glycemic
controlb (%)
Main ndingsc
Dai, 1996, Taiwan Outpatient,
convenience
150 (56.7) 63.7 (7.4) 10.6 (6.7) (1) Marital status.
(2) Family support scale (FSS):
adapted from the Personal
Resources Questionnaire85
Part II: emotional support,
informational exchange,
afrmation and reciprocity.
Additional items measured
tangible aids and recuperating
atmosphere of the family.
Age, sex, education,
nance, living
arrangements, BMI,
DD, hypertension,
expectation of lial
piety, recent life stress
HbA1c (1) Marital status was not a
predictor of HbA1c (beta =0.07,
p>0.05)
(2) FSS was not a predictor of HbA1c
(beta =0.06, p>0.05)
Gender differences: increased FSS
was associated with higher HbA1c
in females (beta =0.21, p10
years =28.8%
Social support: number of people
patients can talk to about
personal problems
Age, sex, education,
MS, occupational
status, smoking status,
alcohol consumption,
PA, BMI, DD, diabetic
medication,
compliance, health
status
Categorical HbA1c
(8=poor glycaemiccontrol)
Unadjusted: more individuals in the
low social support categories had an
HbA1c8% (p=0.02)Adjusted: social support was not a
predictor of HbA1c8%f
Kaplan, 1987, USA Community,
convenience
37 (54) 52.97 (13.0) NR The Social Support
Questionnaire (SSQ):
(1) number of support persons in
network (SSQ-N).
(2) Satisfaction with support
(SSQ-S)
Sex HbA1c (1) No association between SSQ-N
and HbA1c at baseline.
At 18months: SSQ-Nwas associated
with change in HbA1c in males
(r=0.3, p0.05).
(2) Association between SSQ-S and
HbA1c in males (r=0.36, p
R. Stopford et al. / Patient Education and Counseling xxx (2013) xxxxxx8
G Model
PEC-4612; No. of Pages 10HbA1c in males. Three studies reported no signicant associationbetween family support and HbA1c [41,43,46].
Perceived social support: Kim found perceived spousal support tobe independently associated with reduced HbA1c in male, but notfemale, patients [55].
Multifaceted measurements: Five (out of 13) studies found socialsupport to be independently associated with HbA1c. Okura et al.found low and intermediate support (assessed using the subsec-tion of the Diabetes Care Prole (DCP)) to be independentlyassociated with higher HbA1c [30]. Similarly, Whittemore et al.found increased social support (measured using the supportsubscale of the DSMART) to be independently associated withlower HbA1c in a female sample [32]. Kacerovsky-Bielesz et al.assessed four dimensions of social support using the Berlin SupportScales [37]. Increased emotional support was independentlyassociated with increased HbA1c in men only. No associationwith HbA1c was seen on other dimensions of social support(instrumental, informational or satisfaction). In unadjustedanalysis, Misra and Lager report greater social support (assessedusing the Personal Resource Questionnaire-II), to be associatedwith lower HbA1c [28]. Similarly, Fortmann et al. utilized 13 itemsfrom the Chronic Illness Resource Survey (CRIS) to assess supportreceived over the previous three months [26]. In unadjustedanalysis, increased social support was associated with lowerHbA1c. Self-management and depression mediated this relation-ship. Sukkarieh-Haraty reported a signicant association in theopposite direction. Social support (measured using the DCP) wasindependently associated with increased HbA1c [36].
No associations were observed in 9 studies when measuringsocial support using the following measures: Social Support Scalefor Patients with chronic disease [29], adapted questions from theDiabetes Care Prole [35], The Social Support Survey [25] the SocialSupport Scale modied from the Michigan Diabetes Care Prole[27] or The Interpersonal Support Evaluation List (ISEL) [31].
3.2. Outcome measurement
Glycemic control: The measure of glycemic control was HbA1c inall studies. Sixteen studies collected venous or capillary bloodsamples to assess HbA1c. Eight studies recorded HbA1c frommedical records [28,29,35,44,45,4951]. Two studies used selfreported HbA1c [48,55], 1 study obtained HbA1c values from hometest kits [30], and 1 study used the mean value of the 3 most recentHbA1c results over 3 years [25]. One study reported no informationas to how HbA1c was obtained [54]. Ten studies measured HbA1ccategorically. The denition of poor glycemic control variedbetween studies ranging from >6.5% (42 mmol/mol) [28] to11.6% (102 mmol/mol) [47]. The remainder of studies (n = 19)examined HbA1c as a continuous variable.
Quality assessment: All but one study [53] adequately describedparticipant characteristics. Two studies included in this systematicreview used a prospective design [29,38] with a mean follow upperiod of 15 months. Two of the included studies used randomsampling methods [47,52] and 5 used consecutive sampling[32,35,37,51,54]. Of the 23 studies using questionnaires to assesslevels of social support, 9 studies [30,35,36,4143,46,54,55](including 2 conference abstracts) did not report any informationabout the reliability or the validity of the social support measures.The remainder of studies assessed marital status only (n = 6). Onestudy did not report how HbA1c was measured [54]. Sixteenstudies controlled for confounding variables when assessing theassociation between social support and glycemic control. In 5additional studies, adjusted analysis was conducted, but socialsupport was not entered due to insignicant associations betweensocial support and glycemic control in unadjusted analysis[27,41,43,46,47]. There were no studies included in this reviewPlease cite this article in press as: Stopford R, et al. Social support aobservational studies. Patient Educ Couns (2013), http://dx.doi.org/1that assessed all 6 quality criteria, 4 studies met 5 out of 6 qualitycriteria [37,38,51,52].
4. Discussion and conclusion
4.1. Discussion
We conducted a systematic review of published and unpub-lished observational studies examining the association betweensocial support and HbA1c in adults with T2DM. There is someevidence for a benecial effect of social support (family supportand multi dimensional assessments of social support) on glycemiccontrol. There was limited evidence that being married or livingwith a partner was associated with worse glycemic control. Themajority of statistical associations in the review were notsignicant.
In keeping with the social support literature, this review notedgender differences in the association between social support andglycemic control. However, there was a lack of consensus acrossstudies regarding the direction of this relationship. In prospectiveanalysis, men with larger social networks displayed a greaterreduction in HbA1c than women [38], Similarly, in cross sectionalanalysis, family support was associated with reduced HbA1c inmales, but increased HbA1c in females [45]. The lack of genderspecic analyses may have obscured any effect of social support onglycemic control. Informal support seeking is often different inmales and females. Females seek and receive more support fromfriends and extended family, males often seek and receive moresupport from their spouse [38]. Females may also be moresusceptible to the stresses of their social relations. The associationbetween being married and poor glycemic control in two studieswas surprising due to a consistently reported protective effect ofmarriage [2,56], particularly in males [57]. Failure to acknowledgethese sex differences may have masked any association.
Although only considered in two studies, temporality may be animportant factor when considering social support in long termconditions. We cannot infer causality in cross sectional designs, butprospective designs may also be problematic as a bi directionalassociation between social support and glycemic control may exist.Elevated HbA1c may well result in increased social support. Thismay be particularly true with functional support where elevatedHbA1c may result in help seeking and receipt of support; elevatedHbA1c is less likely to result in structural measures such asmarriage. In order to optimally investigate this association, aprospective cohort design is needed to measure multiple dimen-sions of social support at the time of diagnosis and the change insocial support over time. These studies will allow us to furtherallude to the active component of social support and to thedirectionality of the association.
Associations between social support and glycemic controlvaried depending on the measurement of social support. Multidi-mensional assessments of social support may better represent thecomplex multi-factorial nature of social support and the multipleand interacting components that inuence health. In accordancewith previous research, composite measures were more predictiveof biomedical outcomes than less complex measures [6]. Further-more, the consistent association between social support and healthin the wider literature may indicate that our review failed to detectthe active component(s) of social support, crucial for its effectivefunctioning.
In T2DM, improvements in self-management, psychologicalfunctioning and biomedical outcomes are seen following formal-ized support interventions; support provided, for the most part, bystrangers [14]. Naturally occurring relationships (e.g. friends andfamily) may exert a greater inuence on health than supportprovided by health care professionals [6] or strangers [58].nd glycemic control in type 2 diabetes: A systematic review of0.1016/j.pec.2013.08.016
R. Stopford et al. / Patient Education and Counseling xxx (2013) xxxxxx 9
G Model
PEC-4612; No. of Pages 10Evidence provided in this systematic review is based entirely onnaturally occurring (informal) social relationships. Such supportmay be more prominent in the life of an individual than organizedsupport sessions, and able to exert a greater and sustainedinuence. This said, the utilization of naturally occurring socialrelationships (spousal support and family and friend support) informalized interventions found mixed results [14]. Spousalsupport was benecial for obese women with T2DM whenattending diabetes education programs [17] but in a similar study,attendance of culturally tailored education with family or friendsoffered no improvement in glycemic control when compared toattending alone [59].
We expect that social support may vary across the course ofdisease, perhaps being benecial only when individuals are in needand receptive to aid. This may, in part, explain the consistentrelationship between social support and mortality seen in theliterature [6]. In T2DM we may expect social support to be morerelevant with disease progression. Most of the studies includedrelatively healthy individuals, not experiencing life threateningconditions or end stage diabetes complications. The majority ofstudies recruited patients from primary care and outpatientsettings; these individuals may have sufcient social supportand there may be a bias against patients lacking social support whomay not be attending clinics. This may lead to an underestimationof the effect of social support. Illness may also result in poorer ormore restricted social relations as a result of physical connementor disability. Sampling from community ambulatory clinics mayexclude such individuals.
There is also a tendency to assume that all social relationshipsare supportive, but the notion that support impacts negativelyupon health outcomes, including chronic disease self-manage-ment, has been previously reported [15]. Our review did not takeinto account the quality of relationships. Negative support(hostility, criticism and harassment) can be counterproductiveand more predictive of outcomes than positive aspects of socialrelationships [7].
There is evidence that social support may be a clinicallyrelevant factor on the pathway to glycemic control. Four studies(two not included in the review) document evidence for an indirectassociation between social support and HbA1c, mediated by selfefcacy, adherence [34,44], self care behaviors [26,33] anddepression [26]. Many studies statistically adjusted for establishedrisk factors. This may underestimate the effect of social support onglycemic control, since there is evidence that at least some of theimpact of social support on HbA1c is mediated by these factors.
One of the strengths of conducting systematic reviews is thatfuture designs may be improved by highlighting the limitations ofexisting research. This systematic review, although inconsistent inndings, highlights important conceptual and methodologicalbarriers when reviewing the expansive and heterogeneous socialsupport literature.
Concerns relate to the use of non standardized measurementsof social support with varying validity and reliability. A multitudeof social support measures exist with no gold standard assess-ment tool available. In 30 studies, 21 different measures of socialsupport were used. The heterogeneity between measures posesproblems when comparing and reporting studies. The need tostandardize social support measures is necessary for the (a)progression of the evidence base (b) communication to stake-holders of diabetes care and (c) development of interventions.Social risk factors are challenging to measure and validate asconstructs are often difcult to dene and quantify [60]. In socialepidemiology research in chronic disease, we may need to usequalitative research to identify important forms of support and theconditions under which it is delivered to inform the developmentof standardized measures. It is important to establish whether aPlease cite this article in press as: Stopford R, et al. Social support aobservational studies. Patient Educ Couns (2013), http://dx.doi.org/1valid standardized measure assesses what it is designed to indiverse populations. In health disparities research, standardizedmeasures may sometimes not be appropriate across cultural andsocial domains. Less rigid, semi-structured interviews may befavorable when studying a construct such as social support. Theseoften take into account gender and cultural variations whilstacknowledging there is something fundamental about socialsupport regardless of these factors.
There was also high variability across studies in the measure-ment and denition of HbA1c, particularly amongst studies usingcategorical measures of HbA1c. Measuring HbA1c categorically isnowadays less seen in the diabetes literature. HbA1c is measuredon a continuum to internationally accepted measures (IFCC) [61].The denition of poor glycemic control ranged from 6.5% to 11.5%(48 mmol/mol to 102 mmol/mol) across studies irrespective ofnational guidelines. This makes comparisons across studiesparticularly difcult and reduces the probability of identifyingtrends in the literature.
5. Conclusion
The ndings of this systematic review indicate tentativeevidence for a potentially important role for informal supportsources in glycemic control in individuals with T2DM. There isneed for consensus and standardization of social support measuresto build an evidence base from the literature.
5.1. Practice implications
The multiple resources for social support should be openlydiscussed with patients in healthcare settings. Males and femalesmay utilize and benet from social support in different ways andthis must be taken into consideration. Physicians should exploreinformal support sources if a patient is struggling with their selfcare. Diabetes care teams could encourage informal and availablesocial support from family members before more formal supportinterventions are implemented.
References
[1] Marmot M. Social determinants of health inequalities. Lancet 2005;365:1099104.
[2] Cohen S. Social relationships and health. Am Psychol 2004;59:676.[3] Uchino BN. Social support and health: a review of physiological processes
potentially underlying links to disease outcomes. J Behav Med 2006;29:37787.
[4] Lin N, Ye X, Ensel WM. Social support and depressed mood: a structuralanalysis. J Health Soc Behav 1999;40:34459.
[5] Uchino BN. Understanding the links between social support and physicalhealth: a life-span perspective with emphasis on the separability of perceivedand received support. Perspect Psychol Sci 2009;4:23655.
[6] Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: ameta-analytic review. PLoS Med 2010;7:e1000316.
[7] Clark NM, Nothwehr F. Self-management of asthma by adult patients. PatientEduc Couns 1997;32:S520.
[8] Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. PsycholBull 1985;98:310.
[9] Tang TS, Brown MB, Funnell MM, Anderson RM. Social support, quality of life,and self-care behaviors among African Americans with type 2 diabetes.Diabetes Educ 2008;34:26676.
[10] Garay-Sevilla ME, Nava LE, Malacara JM, Huerta R, de Leon JD, Mena A, et al.Adherence to treatment and social support in patients with non-insulindependent diabetes mellitus. J Diabet Complications 1995;9:816.
[11] Sherbourne CD, Hays RD, Ordway L, DiMatteo MR, Kravitz RL. Antecedents ofadherence to medical recommendations: results from the Medical OutcomesStudy. J Behav Med 1992;15:44768.
[12] Pham DT, Fortin F, Thibaudeau MF. The role of the health belief model inamputees self-evaluation of adherence to diabetes self-care behaviors. Dia-betes Educ 1996;22:12632.
[13] Schiotz ML, Bogelund M, Almdal T, Jensen BB, Willaing I. Social support andself-management behaviour among patients with Type 2 diabetes. Diabet Med2012;29:65461.nd glycemic control in type 2 diabetes: A systematic review of0.1016/j.pec.2013.08.016
[14] van Dam HA, van der Horst FG, Knoops L, Ryckman RM, Crebolder HFJM, vanden Borne BHW. Social support in diabetes: a systematic review of controlledintervention studies. Patient Educ Couns 2005;59:112.
[15] Gallant MP. The inuence of social support on chronic illness self-manage-ment: a review and directions for research. Health Educ Behav 2003;30:17095.
[16] Trento M, Passera P, Tomalino M, Bajardi M, Pomero F, Allione A, et al. Groupvisits improve metabolic control in type 2 diabetes: a 2-year follow-up.Diabetes Care 2001;24:9951000.
[17] Wing RR, Marcus MD, Epstein LH, Jawad A. A family-based approach tothe treatment of obese type II diabetic patients. J Consult Clin Psychol1991;59:156.
[18] Keyserling TC, Samuel-Hodge CD, Ammerman AS, Ainsworth BE, Henrquez-Roldan CF, Elasy TA, et al. A randomized trial of an intervention to improveself-care behaviors of African-American women with type 2 diabetes impact
[37] Kacerovsky-Bielesz G, Lienhardt S, Hagenhofer M, Kacerovsky M, Forster E,Roth R, et al. Sex-related psychological effects on metabolic control in type 2diabetes mellitus. Diabetologia 2009;52:7818.
[38] Kaplan RM, Hartwell SL. Differential effects of social support and socialnetwork on physiological and social outcomes in men and women with TypeII diabetes mellitus. Health Psychol 1987;6:387.
[39] Chlebowy DO, Garvin BJ. Social support, self-efcacy, and outcome expecta-tions: impact on self-care behaviors and glycemic control in Caucasian andAfrican American adults with type 2 diabetes. Diabetes Educ 2006;32:77786.
[40] Choi S, Rankin S. Glucose control in korean immigrants with type 2 diabetes.West J Nurs Res 2009;31:34763.
[41] DuVal TM, Rothberg M, Welch G, Friderici J, Luciano G. Correlation of socialdistress and A1C. J Gen Intern Med 2011;26:S205.
[42] Ilias I, Hatzimichelakis E, Souvatzoglou A, Anagnostopoulou T, Tselebis A.Perception of family support is correlated with glycemic control in Greekswith diabetes mellitus. Psychol Rep 2001;88:92930.
[43] Thaneerat T, Tangwongchai S, Worakul P. Prevalence of depression, hemoglo-
R. Stopford et al. / Patient Education and Counseling xxx (2013) xxxxxx10
G Model
PEC-4612; No. of Pages 10on physical activity. Diabetes Care 2002;25:157683.[19] Gilden JL, Hendryx MS, Clar S, Casia C. Diabetes support groups improve health
care of older diabetic patients. J Am Geriatr Soc 1992;40:14750.[20] McIntosh A, Hutchinson A, Home PD, Brown F, Bruce A, Damerell A, et al.
Clinical guidelines and evidence review for Type 2 diabetes: blood glucosemanagement. Shefeld: ScHARR, University of Shefeld; 2001.
[21] Sanderson S, Tatt ID, Higgins JP. Tools for assessing quality and susceptibilityto bias in observational studies in epidemiology: a systematic review andannotated bibliography. Int J Epidemiol 2007;36:66676.
[22] Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items forsystematic reviews and meta-analyses: the PRISMA statement. Ann InternMed 2009;151:2649.
[23] Juni P, Altman DG, Egger M. Systematic reviews in health care: assessing thequality of controlled clinical trials. Brit Med J 2001;323:42.
[24] Huang MF, Courtney M, Edwards H, McDowell J. Factors that affect healthoutcomes in adults with type 2 diabetes: a cross-sectional study. Int J NursStud 2010;47:5429.
[25] Chew BH, Khoo EM, Chia YC. Social support glycemic control in adult patientswith type 2 diabetes mellitus. Asia Pac J Public Health 2011. http://dx.doi.org/10.1177/1010539511431300 [published online December 23, 2011].
[26] Fortmann AL, Gallo LC, Philis-Tsimikas A. Glycemic control among Latinoswith type 2 diabetes: the role of social-environmental support resources.Health Psychol 2011;30:2518.
[27] Howteerakul N, Suwannapong N, Rittichu C, Rawdaree P. Adherence to regi-mens and glycemic control of patients with type 2 diabetes attending atertiary Hospital Clinic. Asia Pac J Public Health 2007;19:439.
[28] Misra R, Lager J. Ethnic and gender differences in psychosocial factors, gly-cemic control, and quality of life among adult type 2 diabetic patients. J DiabetComplications 2009;23:5464.
[29] Nozaki T, Morita C, Matsubayashi S, Ishido K, Yokoyama H, Kawai K, et al.Relation between psychosocial variables and the glycemic control of patientswith type 2 diabetes: a cross-sectional and prospective study. BioPsychoSocMed 2009;3:4.
[30] Okura T, Heisler M, Langa KM. Association between cognitive function andsocial support with glycemic control in adults with diabetes mellitus. J AmGeriatr Soc 2009;57:181624.
[31] Wilson W, Ary DV, Biglan A. Psychosocial predictors of self-care behaviors(compliance) and glycemic control in non-insulin-dependent diabetes melli-tus. Diabetes Care 1986;9:61422.
[32] Whittemore R, DEramo Melkus G, Grey M. Metabolic control, self-manage-ment and psychosocial adjustment in women with type 2 diabetes. J Clin Nurs2005;14:195203.
[33] Osborn CY, Bains SS, Egede LE. Health literacy, diabetes self-care, and glycemiccontrol in adults with type 2 diabetes. Diabetes Technol Ther 2010;12:9139.
[34] Nakahara R, Yoshiuchi K, Kumano H, Hara Y, Suematsu H, Kuboki T. Prospec-tive study on inuence of psychosocial factors on glycemic control in Japanesepatients with type 2 diabetes. Psychosomatics 2006;47:2406.
[35] Schillinger D, Grumbach K, Piette J, Wang F, Osmond D, Daher C, et al.Association of health literacy with diabetes outcomes. J Amer Med Assoc2002;288:47582.
[36] Sukkarieh-Haraty O, Howard E, Nemr R, Nasrallah M. The relationship be-tween diabetes self-care, psychological adjustment, social support and gly-caemic control in the Lebanese population with type 2 diabetes. Diabet Med2012;29:1078.Please cite this article in press as: Stopford R, et al. Social support aobservational studies. Patient Educ Couns (2013), http://dx.doi.org/1bin A1C level, and associated factors in outpatients with type-2 diabetes. AsianBiomed 2009;3:38390.
[44] Mayberry LS, Osborn CY. Family support, medication adherence, and glycemiccontrol among adults with type 2 diabetes. Diabetes Care 2012;35:123945.
[45] Dai Y-T. The effects of family support, expectation of lial piety, and stress onhealth consequences of older adults with diabetes mellitus. Diss Abstr Int B SciEng 1996;56:6670.
[46] Venkataraman K, Kannan AT, Kalra OP, Gambhir JK, Sharma AK, Sundaram KR,et al. Diabetes self-efcacy strongly inuences actual control of diabetes inpatients attending a tertiary hospital in India. J Community Health 2012;37:65362.
[47] Blaum CS, Velez L, Hiss RG, Halter JB. Characteristics related to poor glycemiccontrol in NIDDM patients in community practice. Diabetes Care 1997;20:711.
[48] Schiotz ML, Bogelund M, Almdal T, Jensen BB, Willaing I. Social support andself-management behaviour among patients with type 2 diabetes. Diabet Med2012;29:65461.
[49] Souza RAP, Correr CJ, Melchiors AC, Sanches AC, Wiens A, Pontarolo R.Determinants of glycemic control and quality of life in type 2 diabetic patients.Lat Am J Pharm 2011;30:8607.
[50] Peyrot M, McMurry Jr JF, Kruger DF. A biopsychosocial model of glycemiccontrol in diabetes: stress, coping and regimen adherence. J Health Soc Behav1999;40:14158.
[51] Kirk JK, Davis SW, Hildebrandt CA, Strachan EN, Peechara ML, Lord R. Char-acteristics associated with glycemic control among family medicine patientswith type 2 diabetes. N C Med J 2011;72:34550.
[52] Rahman NAA, Ismail AAS, Yaacob NA, Naing L. Factors associated with HbA1clevels in poorly controlled type 2 diabetic patients in North-East Malaysia. IntMed J 2008;15:2934.
[53] Pons G, Van Hove C, Engebretson LE, Van Houten HK, Anderson BR, VogelsangDA, et al. The role of illness perceptions in achieving diabetes outcomes. In:Abstract presented at: American Diabetes Association; 2011.
[54] Rothenbacher D, Ruter G, Saam S, Brenner H. Younger patients with type 2diabetes need better glycaemic control: results of a community-based studydescribing factors associated with a high HbA1c value. Br J Gen Pract2003;53:389.
[55] Kim YK. The associations between attachment avoidance, perceived spousalsupport, and diabetes self-care. Diss Abstr Int A Hum Soc Sci 2011;71:3438.
[56] Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health:Durkheim in the new millennium. Soc Sci Med 2000;51:84357.
[57] Umberson D. Gender, marital status and the social control of health behavior.Soc Sci Med 1992;34:90717.
[58] Edens JL, Larkin KT, Abel JL. The effect of social support and physical touch oncardiovascular reactions to mental stress. J Psychosom Res 1992;36:37181.
[59] Gilliland SS, Azen SP, Perez GE, Carter JS. Strong in body and spirit lifestyleintervention for native american adults with diabetes in New Mexico. DiabetesCare 2002;25:7883.
[60] Hidalgo B, Goodman M. Validation of self-reported measures in health dis-parities research. J Biom Biostat 2012;3:e114.
[61] Jeppsson J-O, Kobold U, Barr J, Finke A, Hoelzel W, Hoshino T, et al. ApprovedIFCC reference method for the measurement of HbA1c in human blood. ClinChem Lab Med 2002;40:7889.nd glycemic control in type 2 diabetes: A systematic review of0.1016/j.pec.2013.08.016
Social support and glycemic control in type 2 diabetes: A systematic review of observational studiesIntroductionMethodsResultsExposure measurementsOutcome measurement
Discussion and conclusionDiscussion
ConclusionPractice implications
References