
Social Media "The use of web-based technology to facilitate ...
117
Transcript of Social Media "The use of web-based technology to facilitate ...


Social Media
“The use of web-based technology to facilitate
interaction with others.”

ARS Question:With the exception of e-mail, how often do
you interact with peers online through social networking sites like Facebook & Twitter?
1) Always
2) Very Often
3) Sometimes
4) Rarely
5) Never

ARS Question: How likely are you to use social media to help increase public
awareness of chronic hepatitis C?
1) Very likely
2) Likely
3) Maybe
4) Probably not
5) Never

ARS Question: In patients who present with non liver related complaints, how often do you
evaluate a patient’s risk factors for chronic hepatitis C infection?
1) Always
2) Very Often
3) Sometimes
4) Rarely
5) Never
ARS Question: Among all your genotype 1 patients who are eligible for current therapy, how often are you
withholding therapy while waiting for novel drugs?
1) Always
2) Very Often
3) Sometimes
4) Rarely
5) Never

ARS Question: Among your genotype 1 patients, how
frequently will you be incorporating novel agents once they are approved?
1) Always
2) Very Often
3) Sometimes
4) Rarely
5) Never

How Will Social Media Impact Your Practice?
Bryan S. Vartabedian, MD, FAAPAssistant Professor of Pediatrics
Section of Gastroenterology, Hepatology, & NutritionBaylor College of Medicine
Houston, Texas

How Health Information Was Shared
MD
Patient
Graphic courtesy of Dr. Bryan Vartabedian.

Now Patients find each other
2000sInformation finds patients
1990sPatients find information
Long agoPatients depend on what they’re told
Evolution of Social Health
Graphic courtesy of Dr. Bryan Vartabedian.

4: Individuals – email lists3: Closed networks – MySpace, Facebook2: Open networks – blogs, feeds, YouTube1: Mainstream media – press, influencers
Armano D. Influence ripples. Available at: http://darmano.typepad.com. Accessed on: April 13, 2010.

“You don’t need to go any further doctor. Just spell
‘eosinophil’ if you would.”

CureTogether
Available at: http://www.curetogether.com. Accessed on: April 13, 2010.

• Patient to patient
• Crowdsourced data
• “Clinical trials”
CureTogether
Available at: http://www.curetogether.com/Irritable-Bowel-Syndrome/treatments/. Accessed on: April 13, 2010.

Participatory Medicine
• User-generated healthcare is shifting the balance of power from doctor to patient
• The physician encounter is evolving as a narrow, more defined element in a patient’s quest to understand what’s wrong with them

What Is Social Media?
• Content created by people using scalable online publishing technologies intended to facilitate communication and interaction
• Most often refers to activities that integrate technology, telecommunications, and social interaction, with the construction of words, pictures, videos, and audio

With permission from Solis B, et al. The conversation prism. Available at: http://www.theconversationprism.com. Accessed on: April 13, 2010.

Percentage of Adults Who Look Online for Health Information
Fox S. The social life of health information. January 14, 2009. Pew Internet & American Life Project. Available at: http://pewinternet.org/~/media//Files/Reports/2009/PIP_Health_2009.pdf. Accessed on: April 13, 2010.
61%

2005 2009
Lenhart A. Adult and Social Network Websites. January 14, 2009. Pew Internet & American Life Project. Available at: http://pewinternet.org/Reports/2009/Adults-and-Social-Network-Websites.aspx. Accessed on:April 13, 2010.
The Social Media RevolutionHow Is Its Use in Adults Growing?

US Hospitals on YouTube and Twitter
With permission from Bennett E. Hospital social network data and charts. Available at: http://ebennett.org/hsnl/data/. Accessed on: April 13, 2010.

Where Are the Doctors? The Absence of MDs in Social Media Space
• Late adopters
• Time/impatience
• Concerns over privacy, liability, and image

What Can You Do on Social Networks?
• Educate patients• Influence behavior• Promote awareness of yourself or
your hospital• Build relationships• Filter information

Armano D. Human feed. Available at: http://darmano.typepad.com. Accessed on: April 13, 2010.

Do Physicians Have an
Obligation To Be in the Online
Space?
Number of Pediatricians in the AAP
60,000
KevinMD.com. Available at: http://www.kevinmd.com/blog/2009/08/delayed-vaccine-schedule-dangerous.html. Accessed on: April 13, 2010.

Number of Members in the SSAT
2500
Number of Membersin the AASLD
3000Number of Members
in the AGA
16,000
Number of Members in the ASGE
10,000
Abbreviations: AASLD, American Society for the Study of Liver Diseases; AGA, American Gastroenterological Association; ASGE, American Society for Gastrointestinal Endoscopy; DDW, Digestive Disease Week; SSAT, The Society for Surgery of the Alimentary Tract.DDW 2010. FAQs. Available at: http://www.ddw.org/wmspage.cfm?parm1=710. Accessed on: April 13, 2010.
DDW’s 4 Sponsoring Societies

How Should Physicians Handle Patient Encounters in the
Social Media Space?
They Shouldn’t

Staying Safe on Social Networks
• Never discuss patients• Patients, boss, future employer
will read everything you write• Be nice• Don’t be anonymous

Blog
Put a stake in the ground
Graphic courtesy of Dr. Bryan Vartabedian.

Blog
Graphic courtesy of Dr. Bryan Vartabedian.
Left graphic: Kaplan Publishing. Spring 2009 Catalog. Available at: http://www.kaptest.com/pdf_files/publishing/seasonal-catalogs/KPSpring09Catalog.pdf. Accessed on: April 13, 2010. Upper right graphic: Courtesy of Dr. Bryan Vartabedian. 33 Charts blog. Available at: http://www.33charts.com. Lower graphic: Courtesy of Dr. Bryan Vartabedian. Personal Correspondence. 2010.
Visibility in Action

Armano D. Conversion. Available at: http://darmano.typepad.com. Accessed on: April 13, 2010.

The Low Rates of Chronic HCV Diagnosis and Treatment: Why and What Can We Do?
Hashem B. El-Serag, MD, MPHProfessor of Medicine
Chief, Section of Gastroenterology and HepatologyBaylor College of Medicine
Michael E. DeBakey VA Medical CenterHouston, Texas

Infected 20+ years
Overall prevalence
Past and Future US Incidenceand Prevalence of HCV Infection
Armstrong GL, et al. Hepatology. 2000;31:777-782. Graphic courtesy of the CDC.
Decline among IDUs
Overall incidence

Histologic Fibrosis Stage by Year
Num
ber
of P
erso
ns
Year
Davis GL, Alter MJ, El-Serag H, Poynard T, Jennings L . Gastroenterology 2010

Slide Not Available

Hepatitis C—Age-Adjusted Rates of Ambulatory Care Visits and Hospital Discharges with All-Listed
Diagnoses in the United States, 1979–2004
Data from National Ambulatory Medical Care Survey (NAMCS) and National Hospital Ambulatory Medical Care Survey (NHAMCS) (averages 1992-1993, 1994-1996, 1997-1999, 2000-2002, 2003-2005), and National Hospital Discharge Survey (NHDS). Everhart JE, ed. The burden of digestive diseases in the United States. 2008. NIDDK: US Government Printing Office, 2008; NIH Publication No. 09-6443.

Efficacy of Peginterferon + Ribavirin in Achieving Sustained Virologic Response (SVR)
1. Manns M, et al. Lancet. 2001;358:958-965. 2. Fried M, et al. N Engl J Med. 2002;347:975-982. 3. Kamal SM, et al. Hepatology. 2007;46:1732-1740. 4. Khuroo MS, et al. Aliment Pharmacol Ther. 2004;20:931-938. 5. Conjeevaram H, et al. Gastroenterology. 2006;131:470-477.
Category SVR (%)
Overall 54–561,2
Genotype 1 42–461,2
Genotype 2/3 76–821,2
Genotype 4 58–772–4
African American 285
Cirrhosis 43–441,2

Tolerability
Adherence
Provider experience
Supportive medical team
Treatment Factors
Host FactorsIL28B gene polymorphism
Not African American
Immunocompetent
Lean, non-diabetic, insulin sensitive
Young, good renal function, minimal comorbid illness
Virus FactorsGenotype 2/3
Low viral load
Rapid virologic response
HCV Patients Most Likely to Achieve SVR

El-Serag HB. Gastroenterology. 2007;132:8-10.
Treatment of HCV
Efficacy x Access x Correct Diagnosis x Recommendation x
Acceptance x Adherence
Efficacy in clinical trials and research centers
Effectiveness in community
practice

Efficacy and EffectivenessA Demonstration of the Multiplicative
Effect of Factors
Efficacy of Rx “X”
60%
Access x 80%
Correct diagnosis
x 85%
Recommend x 85%
Acceptance x 85%
Adherence x 70%
Effectiveness of Rx “X”
= 21%
El-Serag HB. Gastroenterology. 2007;132:8-10.
Efficacy of Rx “Y”
80%
Access x 80%
Correct diagnosis
x 85%
Recommend x 85%
Acceptance x 85%
Adherence x 70%
Effectiveness of Rx “Y”
= 28%
Efficacy of Rx “X”
60%
Access x 90%
Correct diagnosis
x 90%
Recommend x 90%
Acceptance x 90%
Adherence x 80%
Effectiveness of Rx “X” modified
= 32%
Example 1: Rx “X”
Example 2: Rx “Y”
Example 3: Rx “X” Modified

Awareness of HCV Infection Among HCV-Infected Persons
Colvin HM, Mitchell AE, eds. Hepatitis and liver cancer: a national strategy for prevention and control of hepatitis B and C. Institute of Medicine. Washington, DC: The National Academies Press, 2009.

Receipt of Treatment
Predictors of Treatment
DemographicsGenotype, viral loadCirrhosis diagnosis
ALT, Hct, Plt, WBC, CrComorbidity
HIV diagnosisInsurance
Patient factors
Provider specialtyHCV experience Continuity
Facility factors
Provider factors
Graphic courtesy of Dr. Hashem El-Serag.

Eligibility and Acceptability of HCV Treatment
• 4084 HCV+ patients in VA Multicenter Study 12/99–12/00
• Eligibility – 32% by standard criteria, 41% by treating physician
– Predictors of noneligibility Ongoing substance abuse OR 17.68 Comorbid medical disease OR 9.62 Psychiatric disease OR 9.45 Advanced liver disease OR 8.43
• Acceptability – 76% of eligible patients
– Reasons for nonacceptance Defer Rx until better therapies 50%
Concerns regarding side effects 22%
• Treatment completion rates
– ~50% of those treated (~8% of all patients)Bini E, et al. Am J Gastroenterol. 2005;100:1772-1779.

Treatment Outcomes Retrospective Observational Cohort
Completed treatment
Achieved SVR
48-week treatment for genotype 1, 24-week treatment for genotype 2/3.
Backus LI, et al. Hepatology. 2007;46:37-47.
N = 5944

Antiviral Therapy for HCV per Year Actual, 2002–2007
Projected, Through 2014
Volk ML, et al. Hepatology. 2009;50:1750-1755.
Actual
Projected

Underutilization and Disparity
Clinical appropriateness and patient preferences
Healthcare system: access, legal, and regulatory issues
Discrimination, bias, uncertainty
Under-utilization
and DisparityP
erc
en
t
Graphic courtesy of Dr. Hashem El-Serag.

Su
rve
y R
esp
onse
s
Refused treatment
Did not f/u with clinician
Received treatment
Clinician did not recommend treatment
Unaware of diagnosis
Reasons for Lack of Treatment Among Respondents to the NHANES Hepatitis C
Follow-Up QuestionnaireN = 133
Abbreviation: NHANES, National Health and Nutrition Evaluation Survey.Volk ML, et al. Hepatology. 2009;50:1750-1755.

Summary
• HCV prevalence peaked in 2001 at 3.6 million persons
• Number and proportion of HCV patients with cirrhosis, decompensation, and HCC will increase for at least another 10–15 years
• Age of persons with complications will rise
• Will antiviral therapy change the future?
– Eradication of HCV stops progression, eliminates the risk of liver failure, and reduces HCC risk Requires therapeutic intervention before onset of advanced
fibrosis
Requires identification of infected cases

Summary
• Clinical effectiveness is dependent on several factors in addition to clinical efficacy– HCV diagnosis
– Referral to specialists
– Treatment of comorbidities
– Adherence to treatment

Institute of Medicine Report Underlying Factors
• Lack of knowledge and awareness about chronic viral hepatitis among
Colvin HM, Mitchell AE, eds. Hepatitis and liver cancer: a national strategy for prevention and control of hepatitis B and C. Institute of Medicine. Washington, DC: The National Academies Press, 2009.
• Insufficient understanding about the extent and seriousness of this public health problem
Healthcare and social service
providers
Healthcare and social service
providersAt-risk populationsAt-risk populations
Policy makers and
the public
Policy makers and
the public

Inadequate surveillance systems
underreport acute and chronic infections
At-risk people do not know they are at risk or how to avoid being
infected
At-risk people may not have access to preventive services
Institute of Medicine Report Consequences
People with chronic HCV infection do not
know they are infected
Many clinicians do not know how to screen
people for risk factors or manage those who are
infected
HCV-infected people often have inadequate
access to testing, social support, and medical management services
Colvin HM, Mitchell AE, eds. Hepatitis and liver cancer: a national strategy for prevention and control of hepatitis B and C. Institute of Medicine. Washington, DC: The National Academies Press, 2009.

Institute of Medicine Report Recommendations
Colvin HM, Mitchell AE, eds. Hepatitis and liver cancer: a national strategy for prevention and control of hepatitis B and C. Institute of Medicine. Washington, DC: The National Academies Press, 2009.
Viral Hepatitis Services
Federally funded health insurance programs (eg, Medicare) should:
Incorporate guidelines for risk-factor screening as required component of preventive care
Surveillance
The CDC should:
Evaluate national HCV public health surveillance systemDevelop agreements with state health departments to support core HCV surveillanceSupport targeted surveillance
Knowledge & Awareness
The CDC should work with key stakeholders to:
Develop HCV educational programs for providersDevelop and evaluate innovative and effective outreach programs to 1) target at-risk populations, and 2) increase public awareness



ARS Question: How likely are you to use social media to help increase public
awareness of chronic hepatitis C?
1) Very likely
2) Likely
3) Maybe
4) Probably not
5) Never

ARS Question: In patients who present with non liver related complaints, how often do you
evaluate a patient’s risk factors for chronic hepatitis C infection?
1) Always
2) Very Often
3) Sometimes
4) Rarely
5) Never

Optimization of Interferon-Based Therapies in
Current HCV Patients–Can We Do Better?
Donald M. Jensen, MDProfessor of Medicine
Director, Center for Liver DiseasesUniversity of Chicago Medical Center
Chicago, Illinois

Why Do Current Drugs Fail?
• Viral factors1
– Viral protein products as inhibitors of innate immunity
– Viral proteins as inhibitors of adaptive responses
• Host factors– Fixed: race, genetics, age, gender
– Modifiable: body mass index, insulin resistance, steatosis1
• Treatment factors– Dose, duration, adherence, tolerability
1. Tai AW, et al. J Hepatol. 2009;50:412-420.

Baseline Predictors
• Host genetic makeup– IL28B polymorphism1
Allele on chromosome 19, rs12979860 Resides 3 kilobases upstream from the IL28B gene
encoding IFN-gamma-3 Strongly associated with rate of sustained virologic
response
– Other racial and genetic factors
• Viral factors– Genotype
– Viral load
1. Ge D, et al. Nature. 2009;461:399-401.

Importance of IL28B Polymorphisms
• C/C genotype is more common in racial groups with a higher sustained virologic response (SVR)
• C/C genotype is associated with a higher SVR compared with T/C or T/T
• IL28B polymorphisms may partially explain racial differences in antiviral response and may be a useful pretherapy tool
Ge D, et al. Nature. 2009;461:399-401.

C Allele is Associated with SVRPercentage SVR by Genotype of rs12979860
0 20 40 60 80 100
C/C
T/C
T/T
SVR
Combined
European Americans
African AmericansHispanics
N = 1,137
P = 1.37 x 10-28 vs T/T
Ge D, et al. Nature. 2009;461:399-401.
n = 70n = 14
n = 102
n = 91n = 35
n = 433
n = 186
n = 559
n = 392
n = 30
n = 336
n = 26

rs12
9798
60 C
-all
ele
Fre
qu
ency
SVR (%)
African Americans(n = 61)
Hispanics(n = 16)
European Americans(n = 271)
East Asians(n = 107)
IL28B Genetic Variation and Genotype 1 Response
Ge D, et al. Nature. 2009;461:399-401.

PEG IFN + RBV THERAPY
Treatment of Chronic HCVGenotype 1 Response Rate
Detection limit (50 IU/mL)
0
1
2
3
4
5
6
7
8
9
10
-6 0 4 8 12 16 20 24 28 32 36 40 44 48 72
Weeks
Lo
g H
CV
RN
A (
IU/m
L)
Null
88%–91%
68%–72%
27%–43%
2%–5%
SVR
Partial~29%
Stopping Rules
1
cEVRRVR~20%
2
1. Jensen DM, et al. Hepatology. 2006;43:954-960. 2. Ghany MG, et al. Hepatology. 2009;49:1335-1374. 3. Fried MW, et al. N Engl J Med. 2002;347:975-982. 4. Manns MP, et al. Lancet. 2001;358:958-965. 5. Davis GL, et al. Hepatology. 2003;38:645-652. Graphic courtesy of Dr. Donald Jensen.
pEVR
51%
Abbreviations: EVR, early virologic response; cEVR, complete EVR; pEVR, partial EVR; RVR, rapid virologic response.

Improving Current Therapy2 Goals
• Increase SVR rate– Decrease risk of hepatocellular carcinoma (HCC)1,2
– Decrease risk of decompensation3,4
– Improve fibrosis/reversal of cirrhosis4
– Improve quality of life5
• Improve adherence and tolerability
– Shorten treatment duration if RVR
– Minimize treatment-related adverse events
1. Craxi A, et al. Clin Liver Dis. 2005;9:329-346. 2. Shiratori Y, et al. Ann Intern Med. 2005;142:105-114. 3. Shiratori Y, et al. Ann Intern Med. 2000;132:517-524. 4. Poynard T, et al. Gastroenterology. 2002;122:1303-1313. 5. Foster GR, et al. J Viral Hepat. 2009;16:605-611.

Goal—Increase SVR Rate
Current options• Increase interferon and/or ribavirin dose
• Increase adherence
• Increase treatment duration
Is there evidence that these work?

Induction Dosing of InterferonInduction IFN dosing
leads to a greater number of early
responders.However, standard
dosing catches up after induction ends.
0 12 24 36 48
HC
V R
NA
neg
(%
)
Induction IFN
Std IFN
Weeks
Proportions of Patients with Undetectable HCV RNA After Starting Combination Therapy1
There is no overall SVR benefit to
induction dosing
Abbreviations: CR, conventional; HR, high-dose induction. 1. Upper right graphic with permission from Kim TH, et al. Intervirology. 2005;48:230-238. Lower left graphic courtesy of Dr. Donald M. Jensen.

Evidence for Increased RBV Dosing
PEG IFN -2b/RBV Registration Trial1
All genotypes
0
20
40
60
80
100
5 9 13 17 21
SV
R (
%)
RBV Dose (mg/kg)
P = .015
aP = .569; bP = .019. 1. Manns MP, et al. Lancet. 2001;358:958-965. 2. Jacobson IM, et al. Hepatology. 2007;46:971-981.
WIN-R Trial2
Genotype 1
Weight-baseda
Flat-dosingb

Importance of RBV Adherence
Adherence messages• Maintain RBV dose
>60% over entire treatment1,2
• Use 200 mg dose reduction steps1,2
• For anemia, use erythropoiesis-stimulating agents sparingly (black box warning)3-5
1. Reddy KR, et al. J Hepatol. 2009;50:402-411. 2. Reau N, et al. Am J Gastroenterol. 2008;103:1981-1988. 3. Sulkowski MS, et al. J Viral Hepat. 2004;11:243-250. 4. Afdhal NH, et al. Gastroenterology. 2004;126:1302-1311. 5. US FDA. News release. March 9, 2007.
Effect of RBV Exposure on Relapse Rate1
0
Cumulative Ribavirin Dose
10
20
30
40
50
60
70
80
Rel
apse
Rat
e (%
) >97% (n = 37)
5419 22 32
80%–97% (n = 14)
60%–80% (n = 18)
>97% (n = 37)
0%–60% (n = 13)

Extending Duration Genotype 1 with Early Virologic Response
48 weeks
72 weeks
12Week
Berg1
G1 onlyRBV 800 mg
48 724 0
29 21
Relapse
53 54
SVR
48 weeks72 weeks
Berg1
G1 onlyRBV 800 mg
HCV RNA pos at week 12; neg at week 24
64 4017 29
1. Berg T, et al. Gastroenterology. 2006;130:1086-1097. 2. Pearlman BL, et al. Hepatology. 2007;46:1688-1694. Graphic courtesy of Dr. Donald M. Jensen.
48 weeks72 weeks
Pearlman2 G1RBV 800/1400 mg
18 38 5920
HCV RNA pos at week 12; neg at week 24 P = .03 P = .004
P = .04
All patient analysis

Can We Shorten Therapy Based on an RVR
to Improve Adherence and Minimize Side Effects?

Utilizing RVR to Shorten Therapy in Genotype 1
For genotype 1, retrospective and prospective data
suggest 24 weeks of therapy may be
adequate when RVR is achieved (particularly
those with low baseline HCV RNA)1-6
1. Zeuzem S, et al. J Hepatol. 2006;44:97-103. 2. Graphic with permission from Jensen DM, et al. Hepatology. 2006;43:954-960. 3. Ferenci P, et al. Gastroenterology. 2008;135:451-458. 4. Yu ML, et al. Hepatology. 2008;47:1884-1893. 5. Zeuzem S, et al. J Viral Hepat. 2009;16:75-90. 6. Nelson DR, et al. Clin Gastroenterol Hepatol. 2009;7:397-414.
89
16
73
35
0
20
40
60
SV
R (
%)
Patients with an RVR at wk 4
88
80
23
44
100
Patients without an RVR at wk 4
n = 18 33 40 56 81 84 208 210
PEG IFN -2a/RBV2
9124 wk + RBV 800
48 wk + RBV 800
48 wk + RBV 1000/1200
24 wk + RBV 1000/1200

Utilizing RVR to Shorten Therapy in Genotypes 2 and 3
For genotype 2 or 3, conflicting clinical
trials data, but largest study to date suggests
shortening therapy may lead to greater
relapse rates1-7
1. Shiffman ML, et al. N Engl J Med. 2007;357:124-134. 2. von Wagner M, et al. Gastroenterology. 2005;129:522-527. 3. Mangia A, et al. N Engl J Med. 2005;352:2609-2617. 4. Lagging M, et al. Hepatology. 2008;47:1837-1845. 5. Dalgard O, et al. Hepatology. 2008;47:35-42. 6. Andriulli A, et al. Dig Liver Dis. 2006;38:741-748. 7. Nelson DR, et al. Clin Gastroenterol Hepatol. 2009;7:397-414.
79 78 8085 85 85
0
20
40
60
80
100
16-wk Regimen
SV
R (
%)
P = .02
Any genotypeGenotype 2
Accelerate Trial1
SVR Rates in Patients with RVR
Genotype 3
24-wk Regimen

Response-Guided TherapyA New Paradigm?
Individualized treatment based on viral kinetic measurements should….• Improve overall cost-benefit
• Improve tolerability for those with RVR
• Decrease relapse rate
Nonresponders

PEG IFN/RBV Nonresponder Clinical Trials
1. Poynard T, et al. Gastroenterology. 2009;136:1618-1628. 2. Jensen DM, et al. Ann Intern Med. 2009;150:528-540. 3. Bacon BR, et al. Hepatology. 2009;49:1838-1846.
EPIC31
476 NRs
PEG IFN -2b 1.5 mcg/kg + RBV 800–1400 mg/d x 48 wk
SVR: 6% overall 4% geno-1
REPEAT2
942 Geno-1 NRs
PEG IFN -2a 180 or 360/180 g/wk + RBV 1000–1200 mg/d x 48 or 72 wk
SVR:
7%–16%
DIRECT3
659 Geno-1 NRs
cIFN 9 or 15 g/d + RBV 1000–1200 x 48 weeks
SVR:
7%–11%
Abbreviation: cIFN, consensus interferon.

Maintenance Therapy

1. Di Bisceglie AM, et al. Hepatology. 2007;46:LB1. 2. Shiffman ML, et al. J Hepatol. 2008;48:S62. 3. Afdhal NH, et al. J Hepatol. 2008;48:S4. 4. Bruix J, et al. J Hepatol. 2009;50(suppl 1):S22.
Maintenance PEG IFN in Nonresponders3 Randomized Controlled Trials
HALT-C COPILOT Bruix, et al
No difference in clinical outcomes1
Subgroup with >4-log reduction in
HCV RNA had reduced
outcomes2
Subjects with baseline
portal hypertension had reduced
outcomes (variceal
bleeding) with PEG IFN3
In primary analysis,
maintenance was not
superior to observational
control in preventing
occurrence of clinical events4

Treat Now or Wait Until STAT-C?
• Advanced fibrosis
• Symptomatic
• Genotype 2, 3, or 4
• IL28B C/C genotype (?)
• Genotype 1 with mild histology
• PEG IFN/RBV prior nonresponders
• IL28B T/T or T/C genotype
Treat Now May Consider Waiting
Interferon and ribavirin will be required in combination with all new STAT-C agents for several years

Conclusions
• Response-guided therapy is important theme now for optimizing existing interferon/ribavirin-based therapies
• Improvements in current standard of care can be demonstrated by– Identifying likely responder populations
– Shortening treatment duration in patients with RVR and poor tolerability
– Extending treatment duration in patients with slow partial response

ARS Question: Among all your genotype 1 patients who are eligible for current therapy, how often are you
withholding therapy while waiting for novel drugs?
1) Always
2) Very Often
3) Sometimes
4) Rarely
5) Never

How Will STAT-C Therapies Affect Future Anti-HCV Treatment Paradigms?
Ira M. Jacobson, MDVincent Astor Professor of Medicine
Chief, Division of Gastroenterology and HepatologyMedical Director of the Center for the Study of Hepatitis C
Weill Medical College of Cornell UniversityNew York, New York

Phases in the Evolution of Anti-HCV Therapy
Weisberg IW, et al. Current Hepatitis Reports. 2007;6:75-82. Graphic courtesy of Dr. Ira Jacobson.
The Empiric Phase
The Phase of
SpecificallyTargetedAntiviral Therapyfor HCV
(STAT-C)
The Final
Phase:Small
Molecule Combinations
???
The Refinement
Phase•Optimal dosing•Viral kinetics•Challengingpopulations
•Nonresponders

Emerging Anti-HCV Therapies
Genome Sequence-Based
EnzymeInhibitors Other
IFN and RBV modifications• Albinterferon• PEG IFN lambda (IL-29)• Other IFN formulations• Taribavirin (viramidine)
Immune approaches• Therapeutic vaccines• Toll-like receptor agonists• Hepatitis C immune
globulin• Monoclonal antibodies
Targeting cellular factors• Cyclophilin antagonists• Nitazoxanide• mIR-122 inhibitors• Entry inhibitors
Specifically Targeted Antiviral Therapy for HCV (STAT-C)
Abbreviations: HCV, hepatitis C virus; IFN, interferon; PEG IFN, peginterferon; RBV, ribavirin.Graphic courtesy of Dr. Ira Jacobson.
Protease
Polymerase
NS5A
RNA Interference
Antisense

Hepatitis C Virus Life Cycle
With permission from Tellinghuisen TL, et al. J Virol. 2007;81:8853-8867.

HCV Genome
With permission from Tellinghuisen TL, et al. J Virol. 2007;81:8853-8867.

Core E1 E2 P7
NS2 NS3 NS4A NS4B NS5A NS5B
Targets for Anti-HCV Drugs in Beyond Phase I Clinical Trials
5–5– –3–3
TelaprevirBoceprevirRG7227TMC 435350MK7009BI-201335BMS-650032ABT-450
BMS-790052
Active site (nucleosides)
RG7128IDX184PSI-7851
Nonnucleosides GS 9190FilibuvirABT-333ABT-072ANA598VX-222
Protease inhibitorsProtease inhibitors Polymerase inhibitors
Polymerase inhibitors
CyclophilinAntagonistsCyclophilinAntagonists
Debio 025SCY-635
NS5Ainhibitors
NS5Ainhibitors
Not all-inclusive
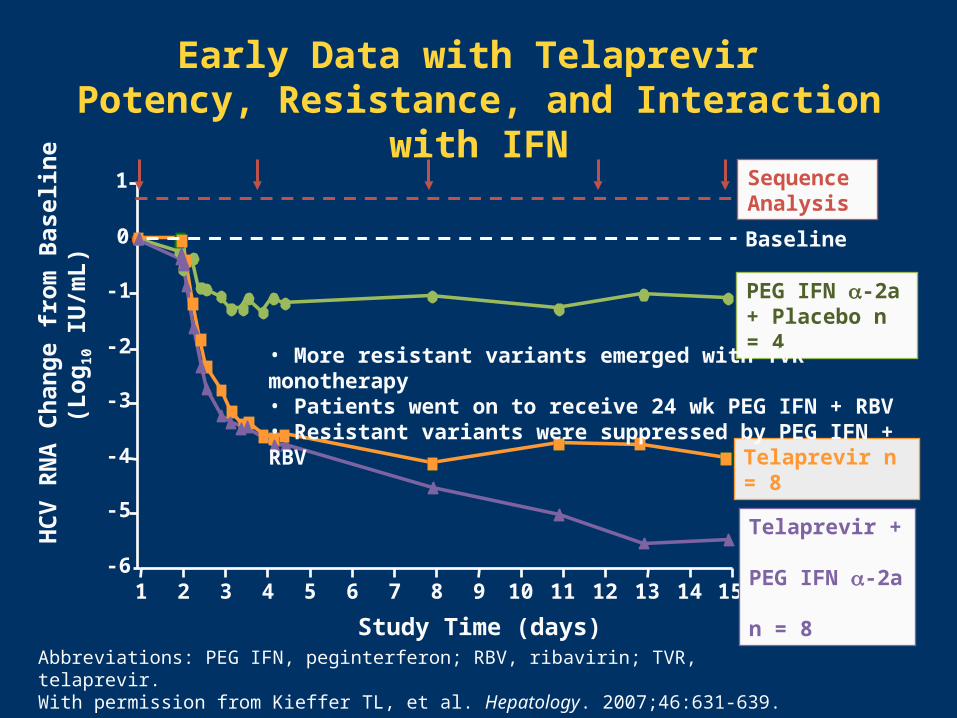
Abbreviations: PEG IFN, peginterferon; RBV, ribavirin; TVR, telaprevir.With permission from Kieffer TL, et al. Hepatology. 2007;46:631-639.
-6
-5
-4
-3
-2
-1
0
1
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Study Time (days)
HC
V R
NA
Ch
ang
e fr
om
Bas
elin
e (L
og
10 I
U/m
L)
Telaprevir n = 8
PEG IFN -2a + Placebo n = 4
Baseline
15
• More resistant variants emerged with TVR monotherapy• Patients went on to receive 24 wk PEG IFN + RBV• Resistant variants were suppressed by PEG IFN + RBV
Early Data with Telaprevir Potency, Resistance, and Interaction with IFN
Telaprevir + PEG IFN -2a n = 8
Sequence Analysis

Placebo + P + R P + R Follow-up
T + P + R Follow-up
T + P + R P + R Follow-up
T + P + R P + R Follow-up
McHutchison J, et al. N Engl J Med. 2009;360:1827-1838.
Abbreviations: R, ribavirin 1000–1200 mg/d; P, peginterferon -2a 180 µg/wk; T, telaprevir 1250 on day 1 then 750 mg q8h.
PROVE1—Telaprevir Phase IIb Study DesignUS, Genotype 1, Treatment-Naive
T12/PR24(n = 79)
T12/PR48(n = 79)
PR48 (control)(n = 75)
T12/PR12(n = 17)
240 48 7212 6036
240 48 7212 6036
Weeks
Weeks

PROVE 1—Telaprevir + PEG IFN/RBVSVR, Intent-to-Treat Analysis, Phase II
0
20
40
60
80
100
SV
R R
ate
(%
)
41
31/75
PR 48 wk(Control)
35
6/17
T 12 wk +PR 12 wk
61
48/79
T 12 wk + PR 24 wk
67
53/79
T 12 wk + PR 48 wk
Graphic Courtesy of Dr. John McHutchison. McHutchison JG, et al. N Engl J Med. 2009;360:1827-1838.
n =
P = .02 P = .002

PROVE 1—Relapse Rates
0
10
20
30
40
50
Re
lap
se
Rat
e (
%)
23
8/35
33
3/92
6
3/51
PR 48 wk(Control)
T 12 wk +PR 12 wk
T 12 wk + PR 24 wk
T 12 wk +PR 48 wk
Denominator = number of subjects with undetectable HCV RNA at completion of assigned treatment duration. aIncludes subjects who met the RVR criterion and stopped at 12 or 24 total weeks of treatment. Graphic Courtesy of Dr. John McHutchison. McHutchison JG, et al. N Engl J Med. 2009;360:1827-1838.
1/41
TVR drives high rates of RVR and low rates of relapse
n =
a a

McHutchison JG, et al. N Engl J Med. 2009;360:1827-1838.
PROVE 1—Viral Breakthrough by Week 12
• 12/175 (7%) of telaprevir-treated patients had breakthrough– 9/12 occurred in first 4 weeks
– 3/12 occurred between weeks 5 and 12
– Only 2 breakthroughs occurred in subjects after HCV RNA became undetectable
• Telaprevir-resistant viral variants – V36M and R155K (10 patients with genotype 1a)
– A156T (1 patient with genotype 1b)
– Wild type (1 patient who missed several days)

PROVE1—Safety Data
Other TVR-related AEs: anemia, GI effects
McHutchison JG, et al. N Engl J Med. 2009;360:1827-1838. Graphic courtesy of Dr. Ira Jacobson.Abbreviations: AE, adverse event; D/C, discontinuation; GI, gastrointestinal; TVR, telaprevir.

Hezode C, et al. N Engl J Med. 2009;360:1839-1850. Graphic courtesy of Dr. Ira Jacobson.
PROVE2—SVR European, Genotype 1, Treatment-Naive
aP = .004 vs control; bP = .12 vs control; cP = .003 vs control. Abbreviations: P, peginterferon -2a 180 µg/wk; R, ribavirin 1000–1200 mg/d; T, telaprevir 1250 mg on day 1 then 750 mg q8h.
c
38/82 49/82 56/81 28/78
a b
n =
Higher relapse ratewith 12 vs 24 weeks
Impaired response, more breakthroughand more relapse
w/out RBV

C208 Study—Telaprevir q8h vs q12h and PEG IFN alfa-2a vs 2b + RBV (N = 161)
Response-Guided Therapy
Abbreviations: P, peginterferon; R, ribavirin; T, telapravir. Forns X, et al. Journal of Hepatology. 2010;52(suppl 1):S26. Graphic courtesy of Dr. Ira Jacobson.
T 750 mg q8h + P -2a 180 µg/wk + R 1000–1200 mg/d
T 750 mg q8h + P -2b 1.5 µg/kg/wk + R 800–1200 mg/d
T 1125 mg q12h + P -2a 180 µg/wk + R 1000–1200 mg/d
T 1125 mg q12h + P -2b 1.5 µg/kg/wk + R 800–1200 mg/d

T + P + R P + R Follow-up
T + P + R P + R Follow-up
T + P Follow-up
Placebo + P + R P + R Follow-up
Patients who failed previous treatment with at least 1 adequate course of PEG IFN combination with RBV defined as at least 12 weeks of therapy.
Abbreviations: R, ribavirin 1000–1200 mg/d; P, peginterferon -2a 180 µg/wk; T, telaprevir 1125 mg day 1 then 750 mg q8h.McHutchison JG, et al. N Engl J Med. 2010;362:1292-1303.
T24/P24(n = 111)
PR48(n = 114)
T12/P24(n = 115)
T24/PR48(n = 113)
240 48 7212 6036
240 48 7212 6036
Weeks
Weeks
PROVE3—Study DesignPrior Treatment Failures
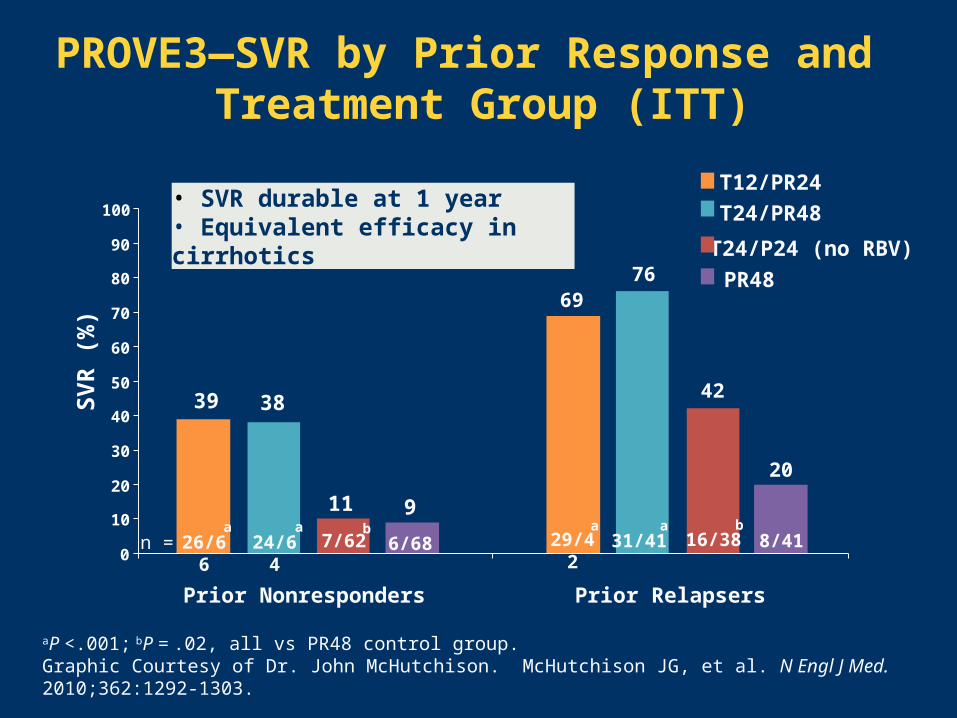
PROVE3—SVR by Prior Response and Treatment Group (ITT)
aP <.001; bP = .02, all vs PR48 control group.Graphic Courtesy of Dr. John McHutchison. McHutchison JG, et al. N Engl J Med. 2010;362:1292-1303.
Prior RelapsersPrior Nonresponders
39 38
11 9
69
42
76
0
10
20
30
40
50
60
70
80
90
100
SV
R (
%)
20
• SVR durable at 1 year• Equivalent efficacy in cirrhotics
n = 26/66 24/64 7/62 6/68 29/42 31/41 16/38 8/41
T12/PR24
T24/PR48
T24/P24 (no RBV)
PR48
a a a ab b

Rollover Study (107) in Treatment Failures From Control Arms of PROVE 1/2/3
Berg T, et al. 45th EASL;April 14-18, 2010. Abstract 108.
T12/PR24T12/PR24
T12/PR48T12/PR48
49/8149/81 18/3418/34 4/244/24 15/2715/27 15/2515/25 24/2524/25 3/33/3 6/76/7 0/10/10/30/3

P + R (n = 104) Follow-up
PR P + R + B (n = 103) Follow-up
PR P + R + B (n = 103) Follow-up
P + R + B (n = 107) Follow-up
P + R + B (n = 103) Follow-up
P + R (n = 16) Follow-up
P + R-LD (n = 59) Follow-up
No Lead-in
R-LD
Control
Lead-in
Sprint 1—Boceprevir + PEG IFN -2b + RBV International, Phase II, Treatment-Naive, Geno 1
280 48 7212a 6036Weeks 4
Par
t 1
Par
t 2b
aInterim analysis; bPart 2 consisted of 75 patients in 10 US sites, 1:4 randomization. Abbreviations: B, boceprevir 800 mg TID; P, PEG IFN -2b 1.5 µg/kg/wk; R, ribavirin 800–1400 mg/d; R-LD, low-dose ribavirin 400–1000 mg/d.Kwo P, et al. J Hepatol. 2009;50:S4.

SPRINT 1—SVR 24 Rates
38
56
75
54
67
0
20
40
60
80
100
SV
R (
%)
PRB Lead-In(n = 103)
PRBNo Lead-In(n = 103)
PRBLead-In(n = 103)
PRBNo Lead-In(n = 107)
PRControl(n = 104)
Tx 28 Weeks Tx 48 Weeks
50
36
PR Control(n = 16)
PR-LD(n = 59)
Part 2Part 1
aP = 0.005; bP = 0.013; cP <.0001, compared with PR Control. Kwo P, et al. J Hepatol. 2009;50:S4.
a b c c

0
24
7
30
4
24
12
75
3
0
10
20
30
40
Breakthrough Relapse
Pe
rce
nt
PR48PRB28PR4-PRB24PRB48PR4-PRB44
Relapse and Breakthrough in SPRINT 1Reduction with Lead-in
Kwo P, et al. J Hepatol. 2009;50:S4. Graphic courtesy of Dr. Ira Jacobson.

SPRINT 1—SVR 24 in Those Who Achieved RVR
100
82
94
74
84
0
20
40
60
80
100
SV
R (
%)
PRControl(n = 104)
PRB Lead-In(n = 103)
PRBNo Lead-In(n = 103)
PRBLead-In(n = 103)
PRBNo Lead-In(n = 107)
Tx 28 Weeks Tx 48 WeeksKwo P, et al. J Hepatol. 2009;50:S4. Graphic courtesy of Dr. Paul Kwo.
32/3832/3862/6662/6632/4332/4354/6654/668/88/8

SPRINT 1—Null Responders to PEG/RBV Can Have SVR with a Protease Inhibitor
Kwo PY, et al. Hepatology. 2009;50(4 Suppl):331A.
a1 patient who was positive at wk 24 became undetectable at wk 30 onwards; b2 patients were missing PCR at wk 24, but later had undetectable PCR.
Log10 Viral Load Decrease After 4-Wk PR Lead-inLog10 Viral Load Decrease After 4-Wk PR Lead-in
aabb
PR4/PRB24PR4/PRB24
PR4/PRB44PR4/PRB44
2/72/7 5/215/21 3/103/10 8/118/11 14/2114/21 10/1210/12 11/1111/11 3/33/34/94/9 8/138/13 11/1711/17 8/108/10 11/1411/14 14/1714/17 11/1211/12 9/99/9
<0.5<0.5 0.5–<1.00.5–<1.0 1.0–<1.51.0–<1.5 1.5–<2.01.5–<2.0 2.0–<3.02.0–<3.0 3.0–<4.03.0–<4.0 ≥4.0≥4.0 Undetect-able
Undetect-able
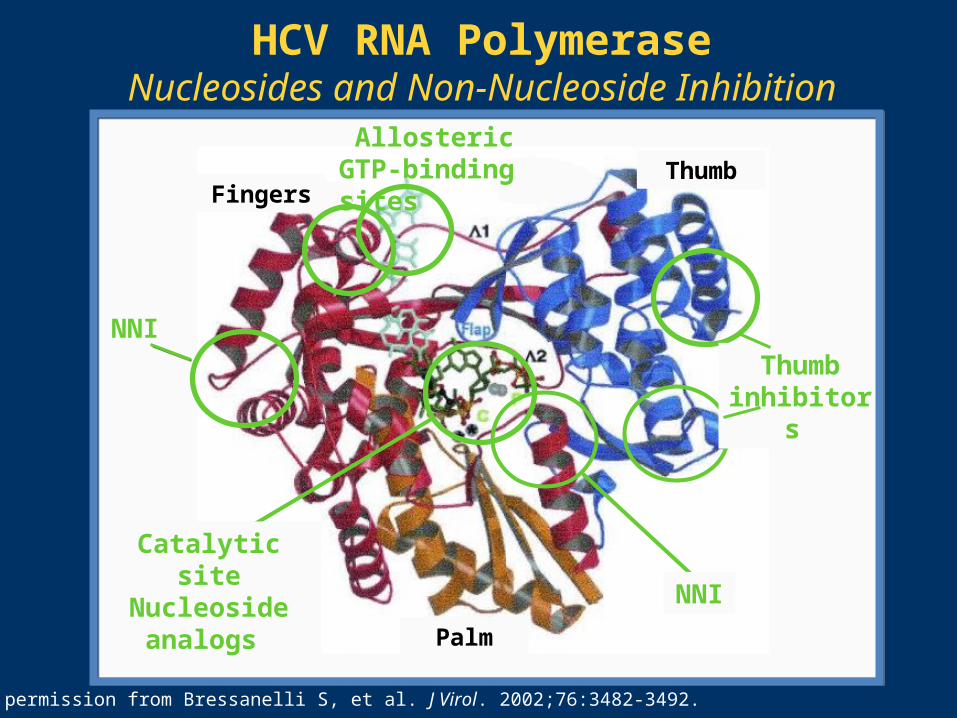
With permission from Bressanelli S, et al. J Virol. 2002;76:3482-3492.
HCV RNA PolymeraseNucleosides and Non-Nucleoside Inhibition
Thumbinhibitors
NNI
Catalytic siteNucleoside
analogs
NNI
Palm
FingersThumb
Allosteric GTP-binding sites

NS5B Polymerase Inhibitor OverviewEfficacy
Many agents with antiviral activity, increased with PEG IFN + RBV
Nucleosides appear active across genotypes
Some non-nucleosides have potency gradient across genotypes and even G1 subtypes
NS5B Polymerase Inhibitor Overview Efficacy
• Phase II trials
– Nucleos(t)ide polymerase inhibitors (RG7128 + PEG FN alfa + RBV)
RVR in 85% with RG7128 + SOC vs 10% with SOC alone1
– Nonnucleos(t)ide polymerase inhibitors (filibuvir, ANA598, GS 9190, ABT-333) + PEG IFN alfa + RBV
Higher rates of RVR (40%–75%) vs SOC2,3
1. Lalezari J, et al. J Hepatol. 2008;48:S29. 2. Jacobson I, et al. J Hepatol. 2009;48:S382-S383.3. Rodriguez-Torres M, et al. Hepatology. 2009;50(4 suppl):LB6.

NS5B Polymerase Inhibitor OverviewResistance and Adverse Effects
• Differences in genetic barrier to resistance class: nucleosides have high barrier
• Resistance can be minimized by combining withPEG IFN + RBV
• Different resistance mutation patterns suggest potential for combinations of polymerase inhibitors
• Toxicity issues with earlier agents: GI effects, hepatotoxicity, hematologic toxicity, and visual disturbance
1. Shi ST, et al. Antimicrob Agents Chemother. 2008;52:675-683. 2. Lawitz E, et al. J Hepatol. 2009;50(suppl 1):S37. 3. Nelson D, et al. J Hepatol. 2008;48:S371. 4. McCown MF, et al. Antimicrob Agents Chemother. 2008;52:1604-1612. 5. Lalezari J, et al. J Hepatol. 2008;48:S29. 6. Bavisotto L, et al. Hepatology. 2007;46 (suppl 1):255A. 7. Cooper C, et al. Hepatology. 2007;46(suppl 1):LB11.

Highlights from EASL 2010Protease Inhibitors
• Good activity for telaprevir against genotype 21
– 3.7-log decline with 2 weeks of telaprevir monotherapy
1. Foster GR, et al. 45th EASL;April 14-18, 2010. Abstract 206. 2. Gane E, et al. 45th EASL;April 14-18, 2010. Abstract 144. 3. Carroll S, et al. 45th EASL;April 14-18, 2010. Abstract 128. 4. Sulkowski M, et al. 45th EASL;April 14-18, 2010. Abstract 298.
• Ritonavir boosting lowers dose needed for RG7227, a protease inhibitor2
• Development of a protease inhibitor (MK-5172) with in vitro activity against resistant variants R155K, A156T, D168V3
• Excellent activity of a protease inhibitor (BI 201335) in nonresponders to PEG IFN + RBV with low breakthrough rates4
– RVR 62%–69% with 240 mg QD or BID, with or without 3-day lead-in
– Viral rebound at 12 weeks 16%–22%
Highlights from EASL 2010NS5B and NS5A Inhibitors
• SVR data for a nucleoside (RG7128) in genotypes 2,31
– 13/20 (65%) prior treatment failures had SVR
1. Gane EJ, et al. 45th EASL;April 14-18, 2010. Abstract 143. 2. Rodriguez-Torres M, et al. 45th EASL;April 14-18, 2010. Abstract 137. 3. Jacobson I, et al. 45th EASL;April 14-18, 2010. Abstract 5. 4. Pol S, et al. 45th EASL;April 14-18, 2010. Abstract 297.
• Robust nonnucleoside with high barrier to resistance(VX-222)2
– >3-log decline in HCV RNA with 3 days of dosing
• Promise for NS5A inhibitors4
– Up to 92% RVR with BMS-790052 in dose ranging study with Peg IFN + RBV
Highlights from EASL 2010NonSTAT-C Drugs
• Intravenous silibin for partial responders1
1. Biermer M, et al. 45th EASL;April 14-18, 2010. Abstract 142. 2. Jacobson I, et al. 45th EASL;April 14-18, 2010. Abstract 6. 3. Muir A, et al. 45th EASL;April 14-18, 2010. Abstract 138. 4. Mouch SA, et al. 45th EASL;April 14-18, 2010. Abstract 204. 5. Shiffman ML, et al. 45th EASL;April 14-18, 2010. Abstract 296.
1. Biermer M, et al. 45th EASL;April 14-18, 2010. Abstract 142. 2. Jacobson I, et al. 45th EASL;April 14-18, 2010. Abstract 6. 3. Muir A, et al. 45th EASL;April 14-18, 2010. Abstract 138. 4. Mouch SA, et al. 45th EASL;April 14-18, 2010. Abstract 204. 5. Shiffman ML, et al. 45th EASL;April 14-18, 2010. Abstract 296.
• Potential role for immune stimulation (GI5005, TLR-9 agonist)2,3
• Increased SVR with vitamin D (86% vs 41%, n = 27)4
• Nitazoxanide in nonresponders (SVR 7%)5
• Cyclophilin Inhibitor Debio 025 can induce SVR ± Peg IFN after a four week course (four patients)

INFORM-1 Study—Median Change from Baseline Cohorts B–G
Abbreviation: TF, treatment failure. With permission from Gane EJ, et al. Hepatology. 2009;50(4 suppl):394A-395A.

A B C
Prevention of emergent resistance
(pre-existing or de novo)
+ +A
Profound suppression
of broad range ofviral variants,
including pre-existing
• Different drugs may contribute variably to each of these goals
• Not all components have to be STAT-C agents
Graphic courtesy of Dr. Ira Jacobson.
The Goal of IFN-Free Combination Regimens

New Anti-HCV TherapiesAnticipated Developments
• Approval of telaprevir/boceprevir seems likely in 2011• Other direct antivirals and compounds with novel
mechanisms of action in development• Response-guided therapy• Incorporation of genetic testing• Accelerated development of interferon-free
combinations• The question for clinicians: to wait or not to wait?



ARS Question: Among your genotype 1 patients, how
frequently will you be incorporating novel agents once they are approved?
1) Always
2) Very Often
3) Sometimes
4) Rarely
5) Never


















