Smriti Hari General Secretary - International … Hari Additional Professor, Radiology All India...
63
Smriti Hari Additional Professor, Radiology All India Institute of Medical Sciences New Delhi, India General Secretary Breast Imaging Society (INDIA) [email protected]
Transcript of Smriti Hari General Secretary - International … Hari Additional Professor, Radiology All India...

Smriti Hari Additional Professor, Radiology
All India Institute of Medical Sciences
New Delhi, India
General Secretary
Breast Imaging Society (INDIA)
Breast Diseases- Diagnosis
Imaging Modalities
Mammography is the primary modality
Ultrasound
MRI
PET
Recent Advances
Digital Mammography + Tomosynthesis +CAD
US Elastography
MR Spectroscopy + DWI
Breast Specific Gamma Imaging
Mammography –Technical challenges
Inherent contrast of breast tissue low
High contrast and spatial resolution needed to detect microcalcifications(100-200µ)
Motion unsharpness
Varying ant to post thickness of breast
Radiation dose

Mammography- Equipment
High contrast resolution
Low energy (20-30 kVp) Xrays: Mo
traget, Mo, Be filters
Short exposure time
Breast compression
High spatial resolution
Small focal spot(0.3mm)
High resolution film-screen combination/
Detector
Accreditation and Quality Control is
essential
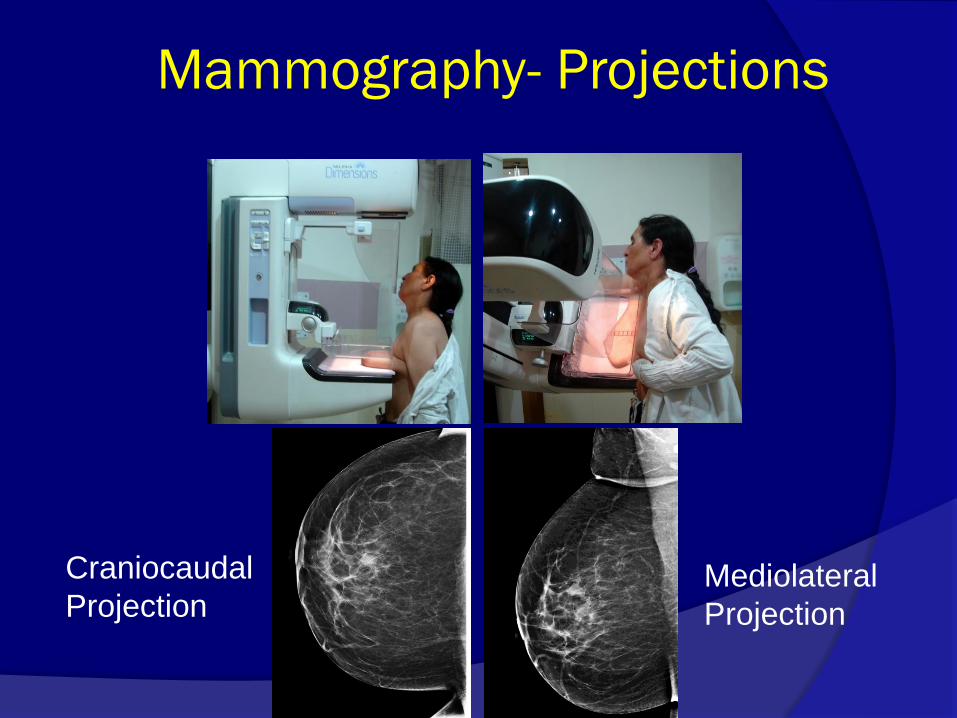
Mammography- Projections
Craniocaudal
Projection Mediolateral
Projection

Criteria for well-positioned
CC and MLO Views
Posterior Nipple Line (PNL) on CC view should be within 1cm of its length on the MLO view
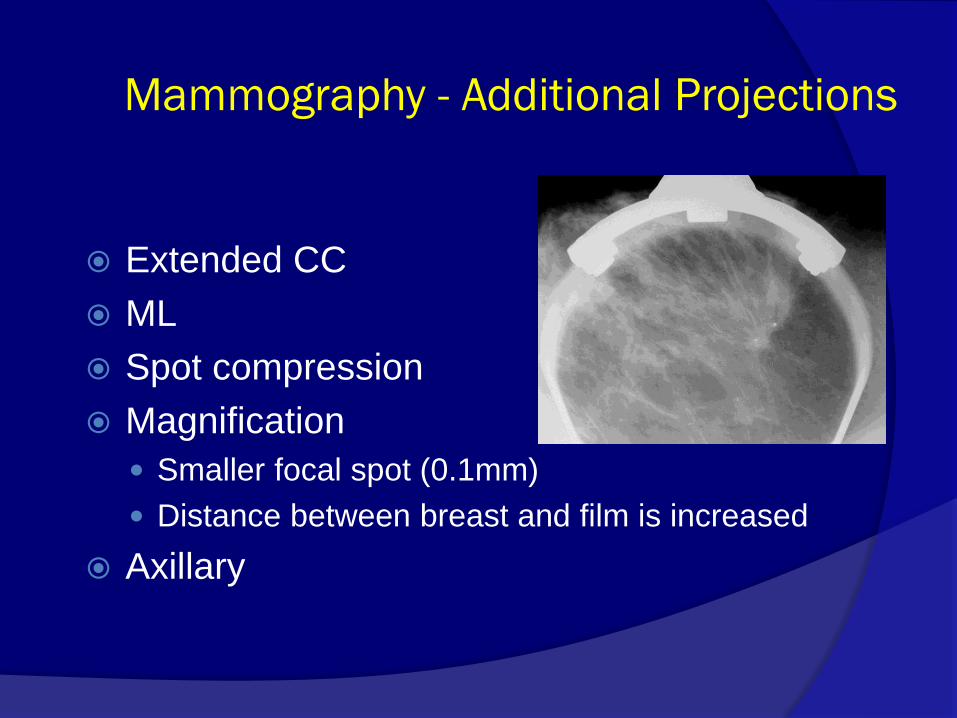
Mammography - Additional Projections
Extended CC
ML
Spot compression
Magnification
Smaller focal spot (0.1mm)
Distance between breast and film is increased
Axillary
Mammography - Indications
Screening mammography
Diagnostic mammography
Symptomatic women aged 30 years and over with
suspicion of breast cancer
Search of the occult primary
Post treatment surveillance
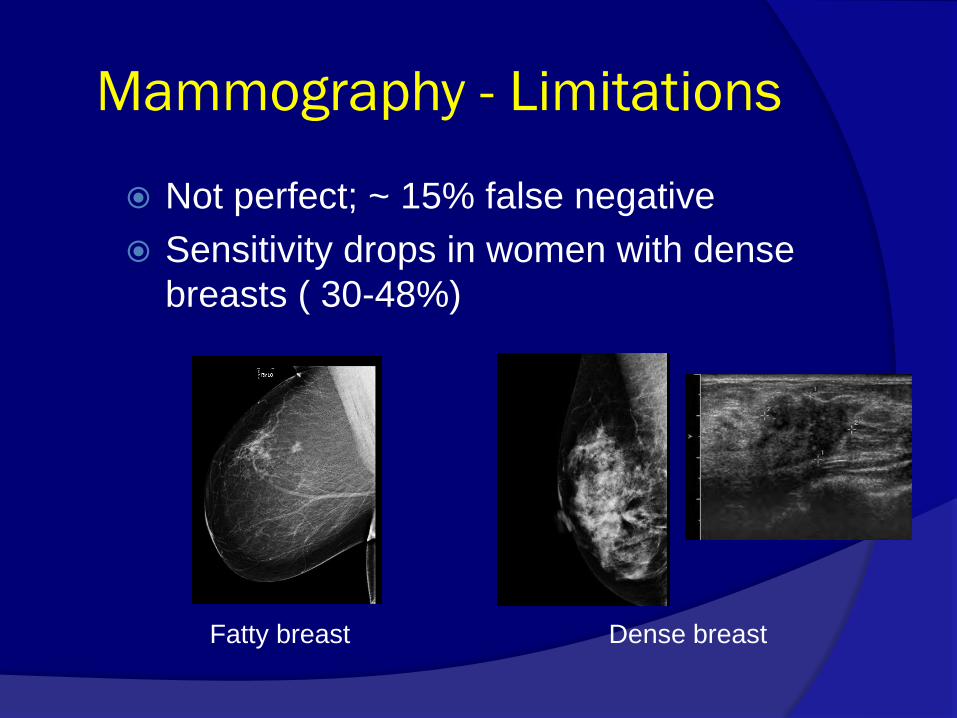
Mammography - Limitations
Not perfect; ~ 15% false negative
Sensitivity drops in women with dense
breasts ( 30-48%)
Fatty breast Dense breast
Advances in Mammography
Digital Mammography
Digital Breast Tomosynthesis
(DBT)
Computer Aided
Detectiion (CAD)
Dual Energy Mammography
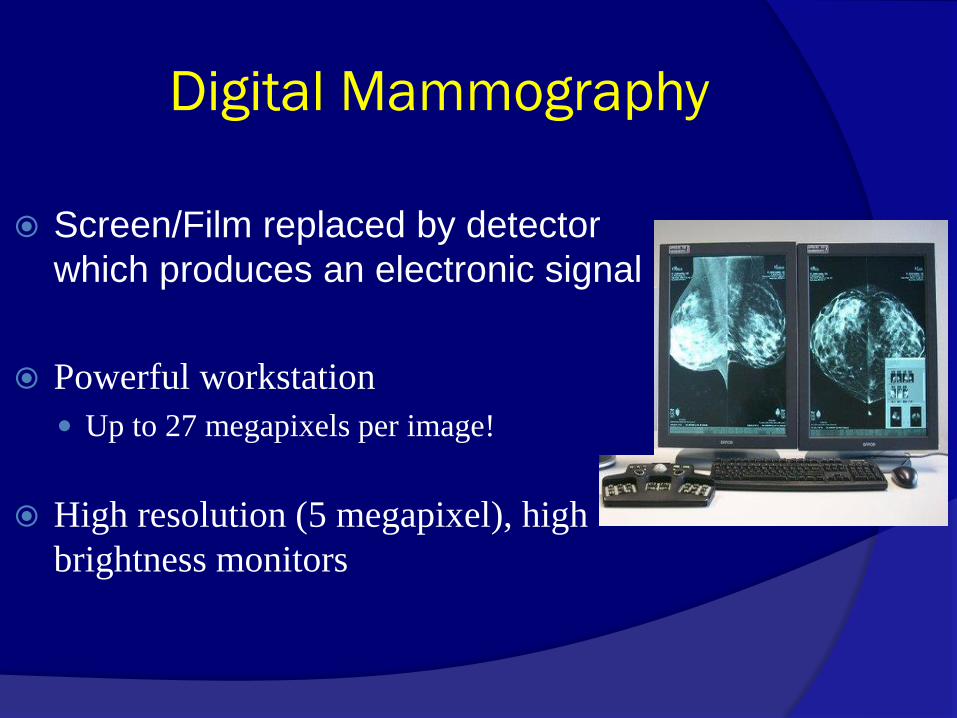
Digital Mammography
Screen/Film replaced by detector
which produces an electronic signal
Powerful workstation
Up to 27 megapixels per image!
High resolution (5 megapixel), high
brightness monitors
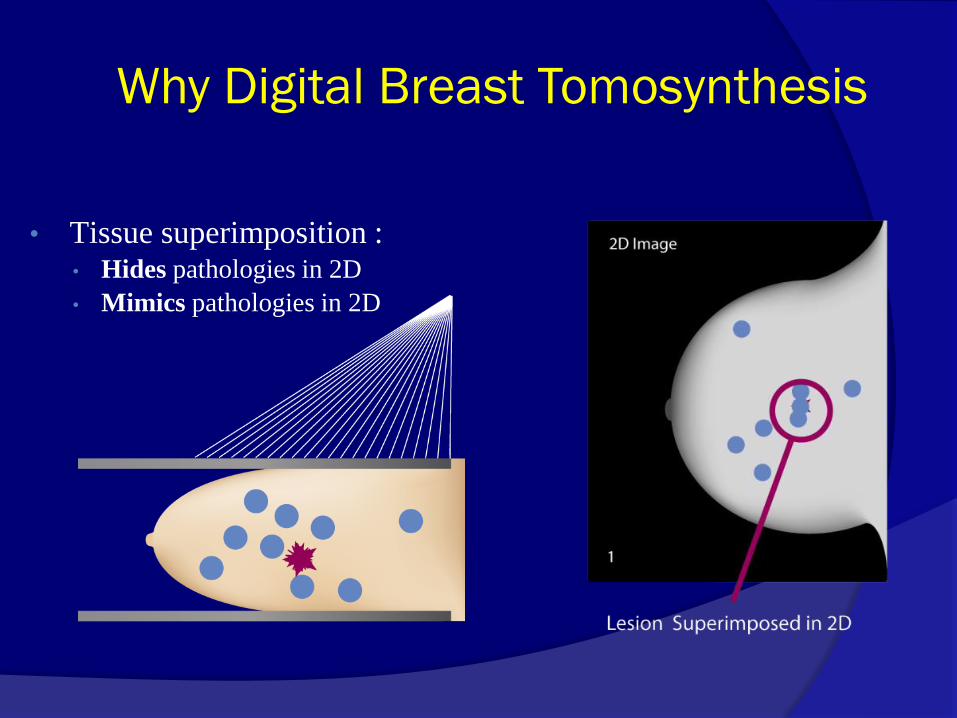
Why Digital Breast Tomosynthesis
• Tissue superimposition : • Hides pathologies in 2D
• Mimics pathologies in 2D

• X-ray tube moves in an arc across the
breast
•
• A series of low dose images are
acquired from different angles
• Total dose approximately the same as
one 2D digital mammogram
• Projection images are reconstructed
into 1 mm slices
Reconstructed
Slices {
How Does Tomosynthesis Work?

Digital Breast Tomosynthesis
Conventional 2D Mammogram 1mm Breast Tomosynthesis slices
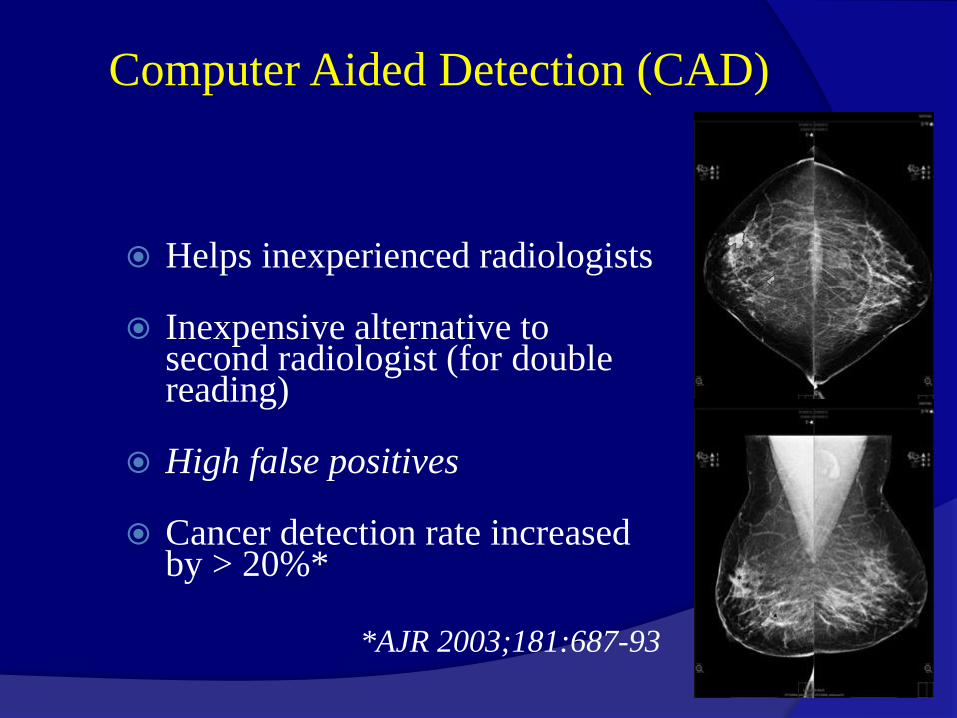
Computer Aided Detection (CAD)
Helps inexperienced radiologists
Inexpensive alternative to second radiologist (for double reading)
High false positives
Cancer detection rate increased by > 20%*
*AJR 2003;181:687-93

Mammography –Interpretation
Optimum lighting conditions
‘Back to back’ placement of films
Check for
Identification, Labelling
Radigraphic quality

Mammography Interpretation
American College of Radiology (ACR) Breast Imaging Reporting and Data System (BI-RADS)
Standardized method for describing the morphology of breast lesions and categorizing the findings in an unambiguous report
Parenchymal Density
Lexicon BI-RADS
Categories Report
Organisation
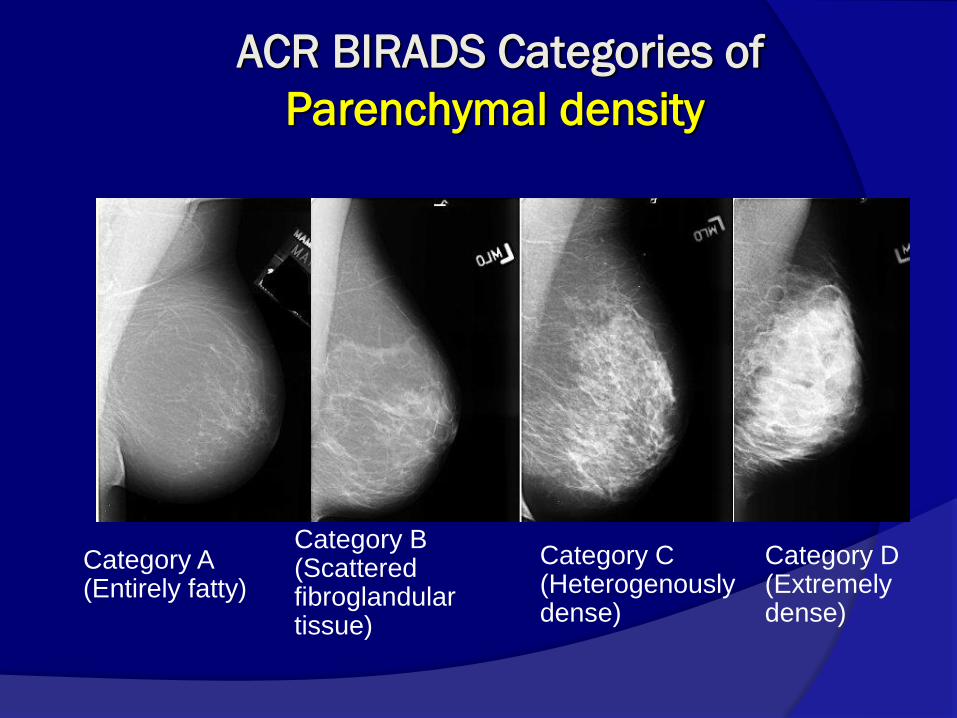
Category A (Entirely fatty)
Category B (Scattered fibroglandular tissue)
Category C (Heterogenously dense)
Category D (Extremely dense)
ACR BIRADS Categories of
Parenchymal density

Mammography-ACR BI-RADS
Lexicon
Mass
Calcification
Architectural distortion
Asymmetry
ACR BI-RADS - Mass Descriptors in
Mammography
Shape Margin
Density

Mass shape
P
robabili
ty o
f m
alig
nancy
Round
Oval
Irregular
Lobulated
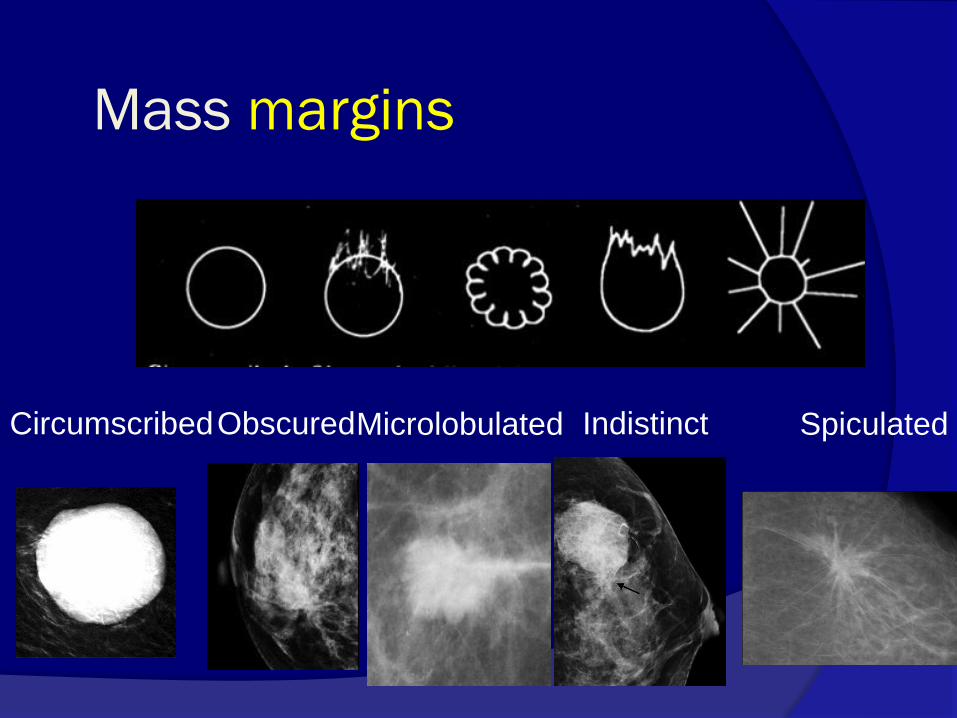
Mass margins
Circumscribed Indistinct Obscured Spiculated Microlobulated
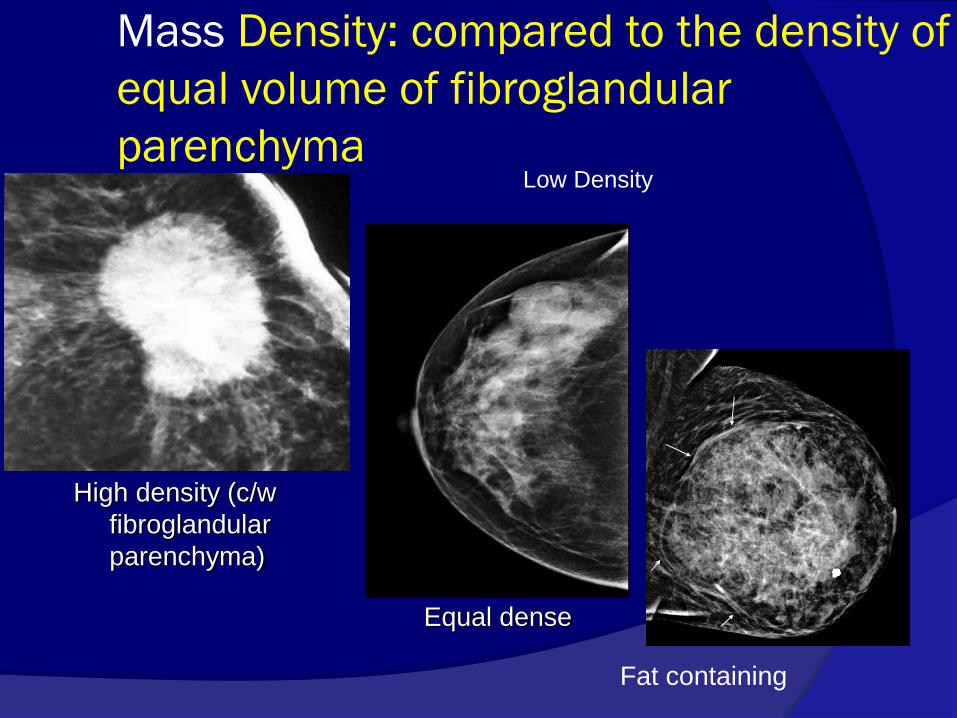
Mass Density: compared to the density of
equal volume of fibroglandular
parenchyma
Fat containing
High density (c/w
fibroglandular
parenchyma)
Equal dense
Low Density
ACR BI-RADS – Calcification
Descriptors in mammography
Morphology Number
Distribution

Calcification morphology
Typically Benign
Suspicious for
Malignancy

Typically Benign Morphology
Skin
Popcorn
Vascular
Rodlike
Round
Dystrophic
Suspicious morphology
Amorphous
Coarse hetrogenous
Fine pleomorphic
Fine linear or fine linear branching
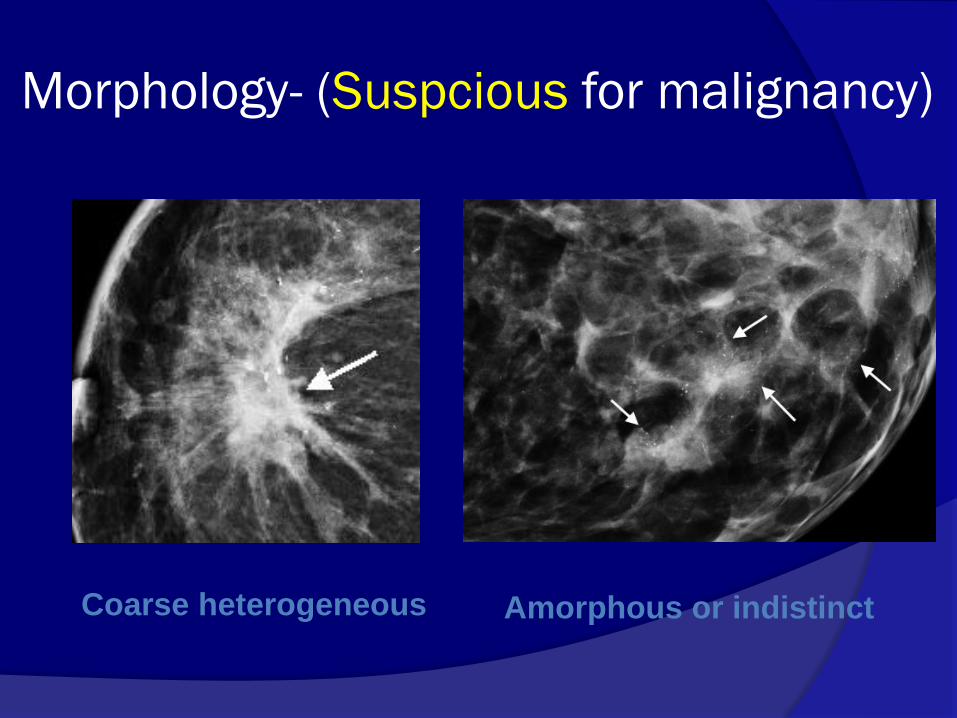
Morphology- (Suspcious for malignancy)
Coarse heterogeneous Amorphous or indistinct
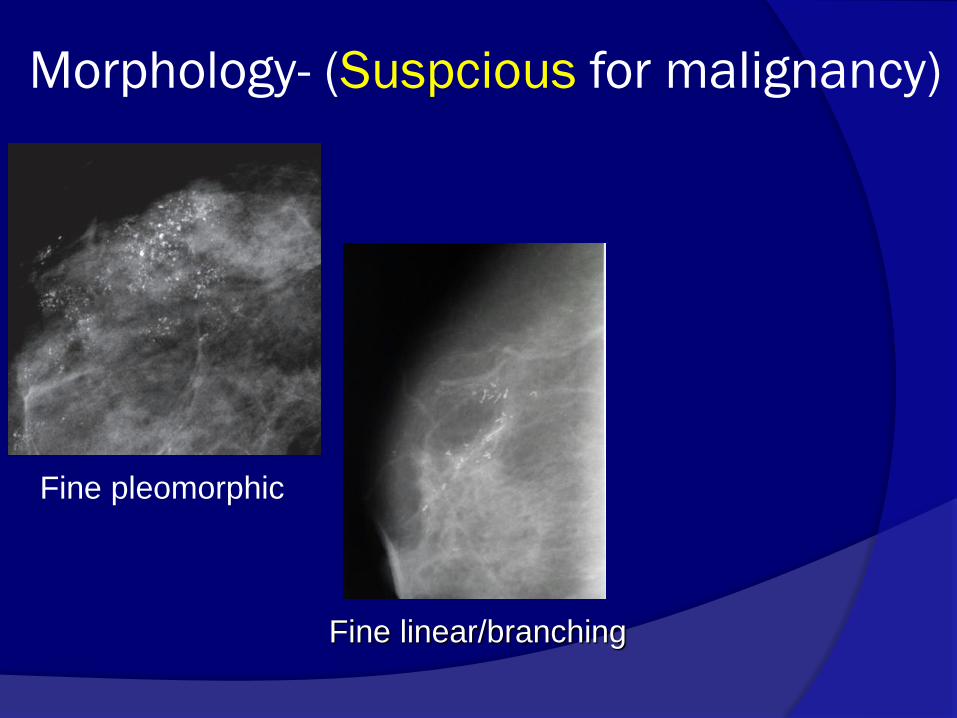
Fine pleomorphic
Fine linear/branching
Morphology- (Suspcious for malignancy)
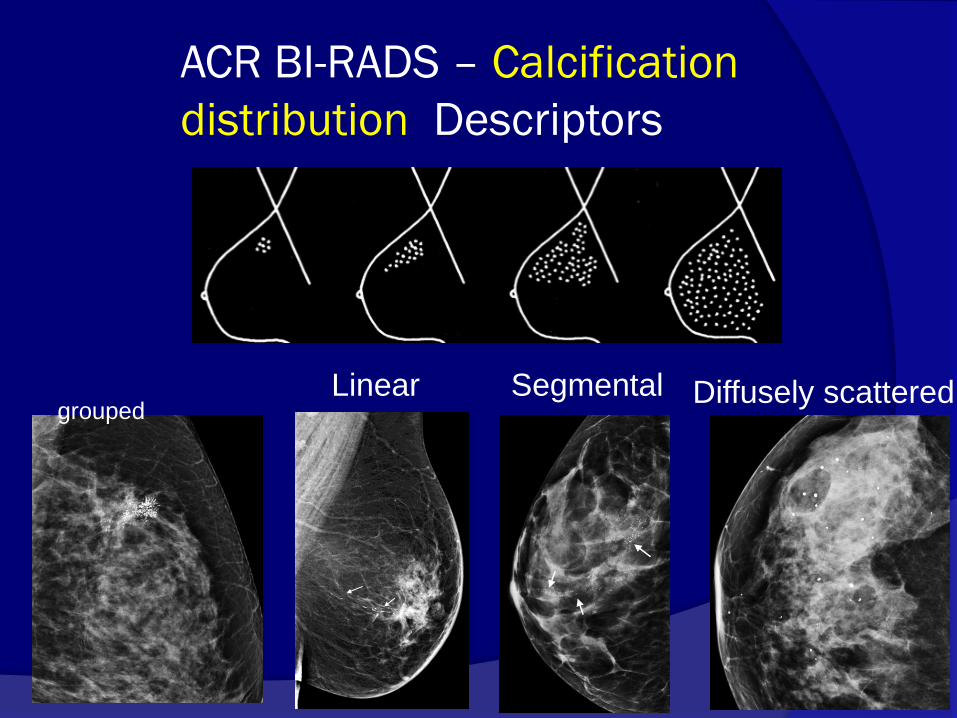
ACR BI-RADS – Calcification
distribution Descriptors
Diffusely scattered
Linear
Segmental
grouped
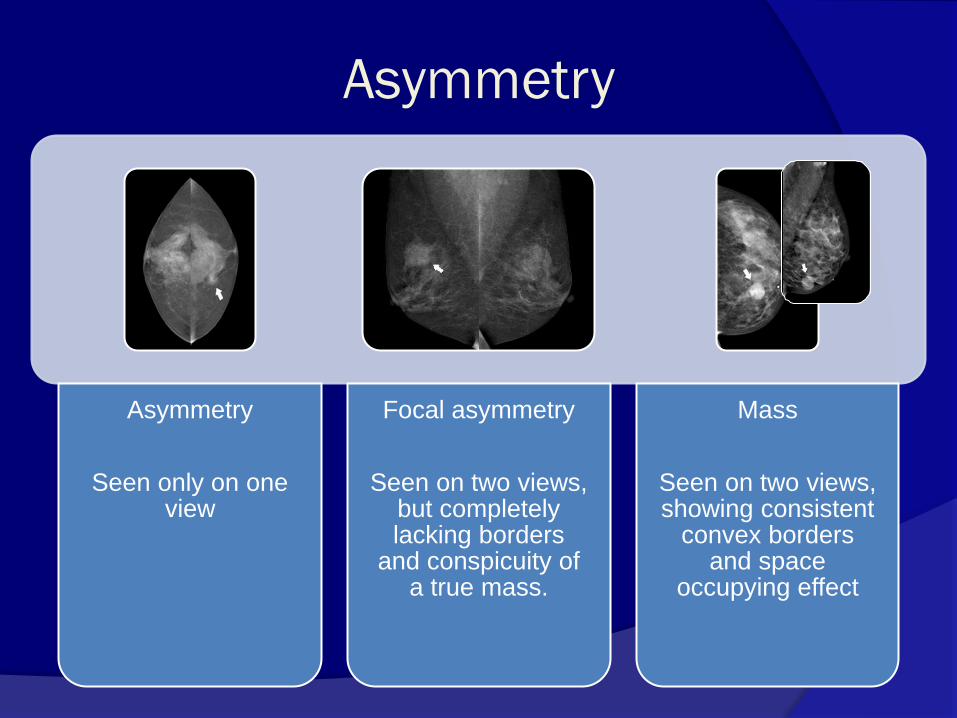
Asymmetry
Asymmetry
Seen only on one view
Focal asymmetry
Seen on two views, but completely lacking borders
and conspicuity of a true mass.
Mass
Seen on two views, showing consistent
convex borders and space
occupying effect

Asymmetry needs further
evaluation if -
Corresponds with clinical abnormality
New development
Associated with calcification, architectural distortion
Special views to exclude true mass or architectural
distortion. Comparison to old mammograms if available, short
interval follow-up if not If special views show mass like character, or if the
area can be palpated - biopsy
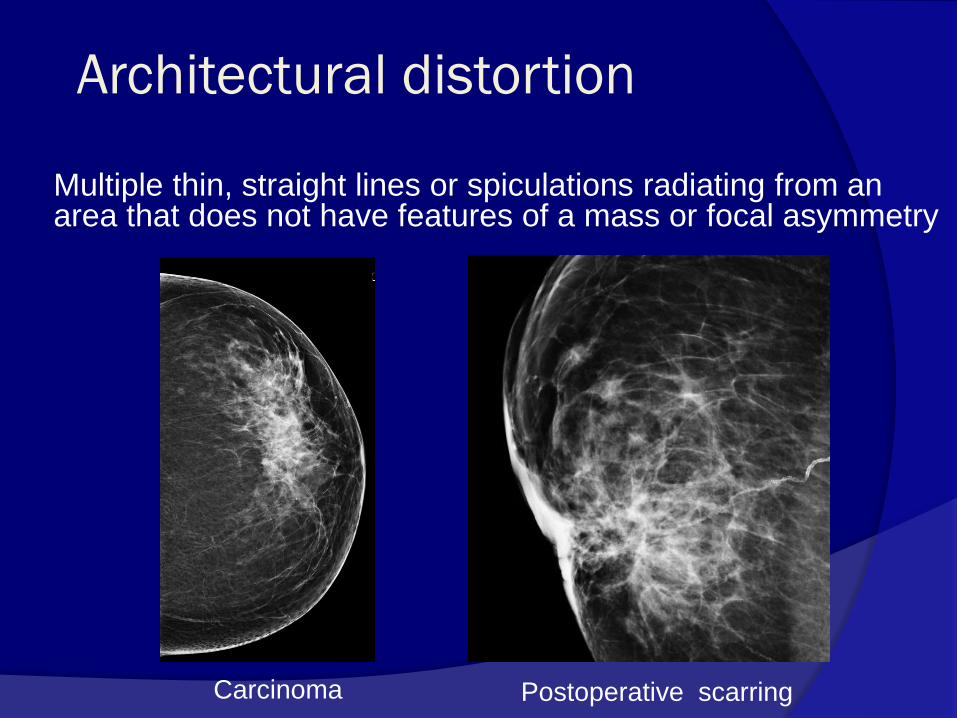
Architectural distortion
Multiple thin, straight lines or spiculations radiating from an
area that does not have features of a mass or focal asymmetry
Postoperative scarring Carcinoma
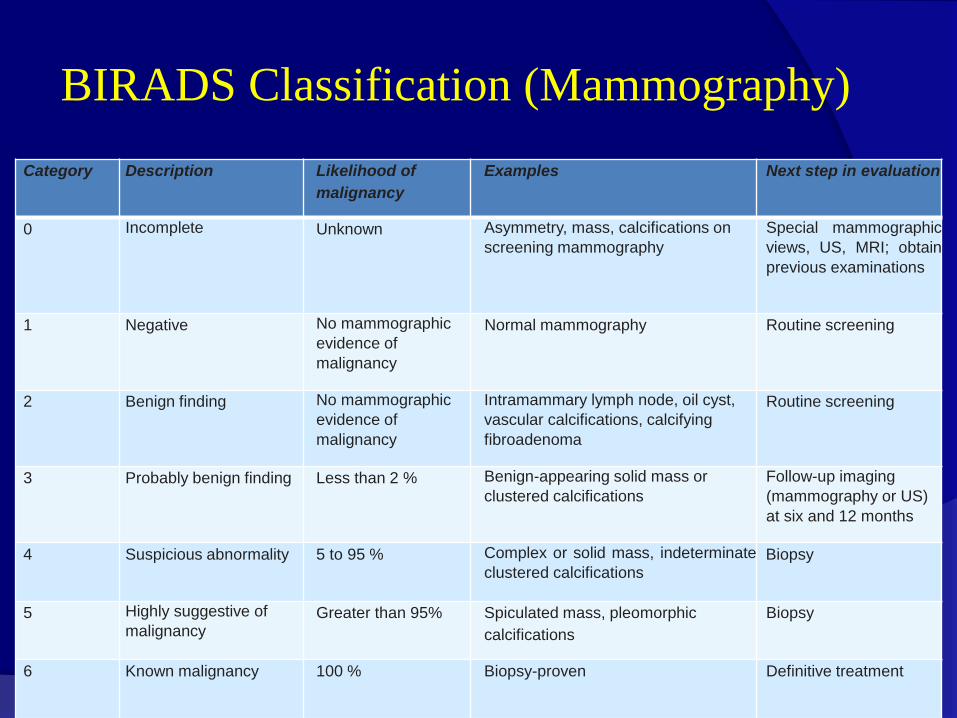
BIRADS Classification (Mammography)
Category Description Likelihood of
malignancy
Examples Next step in evaluation
0 Incomplete Unknown Asymmetry, mass, calcifications on
screening mammography Special mammographic
views, US, MRI; obtain
previous examinations
1 Negative No mammographic
evidence of
malignancy
Normal mammography Routine screening
2 Benign finding No mammographic
evidence of
malignancy
Intramammary lymph node, oil cyst,
vascular calcifications, calcifying
fibroadenoma
Routine screening
3 Probably benign finding Less than 2 % Benign-appearing solid mass or
clustered calcifications Follow-up imaging
(mammography or US)
at six and 12 months
4 Suspicious abnormality 5 to 95 % Complex or solid mass, indeterminate
clustered calcifications Biopsy
5 Highly suggestive of
malignancy Greater than 95% Spiculated mass, pleomorphic
calcifications
Biopsy
6 Known malignancy 100 % Biopsy-proven Definitive treatment
Management of BIRADS 3 lesions
Short interval follow-up mammography every 6
months for 2 years (watchful waiting)
95%, no growth, bx is avoided
2-3 %, a benign process grows, and requires bx to establish its nature
1-2 % are cancer, growth is seen on follow-up, and bx initiates treatment. Although some time is lost in the process, the cancers found at follow-up are usually still small and curable.

45 Y lady with palpable lump in Left
breast UOQ
Mass
Architectural distortion
Asymmetry
Calcification
Shape
Round
Oval
Irregular
Margins
Circumscribed
Microlobulated
Obscured
Indistinct
Spiculated
Density
High
Low
Isodense
BI-RADS 1
BI-RADS 2
BI-RADS 3
BI-RADS 4
BI-RADS 5
BI-RADS 6
Fatty
Breast US: Indications
Symptomatic breast lump in women aged < 30 yrs/
during pregnancy or lactation/ in a male
To assess mammographic abnormality
To assess MRI detected lesions
Palpable lump with negative mammogram
Breast inflammation
Guidance of needle biopsy or localisation
ACR BI-RADS Ultrasound Lexicon
Shape Orientation Margin
Lesion Boundary
Posterior Acoustic Features

Mass Shape
Round Oval
Irregular
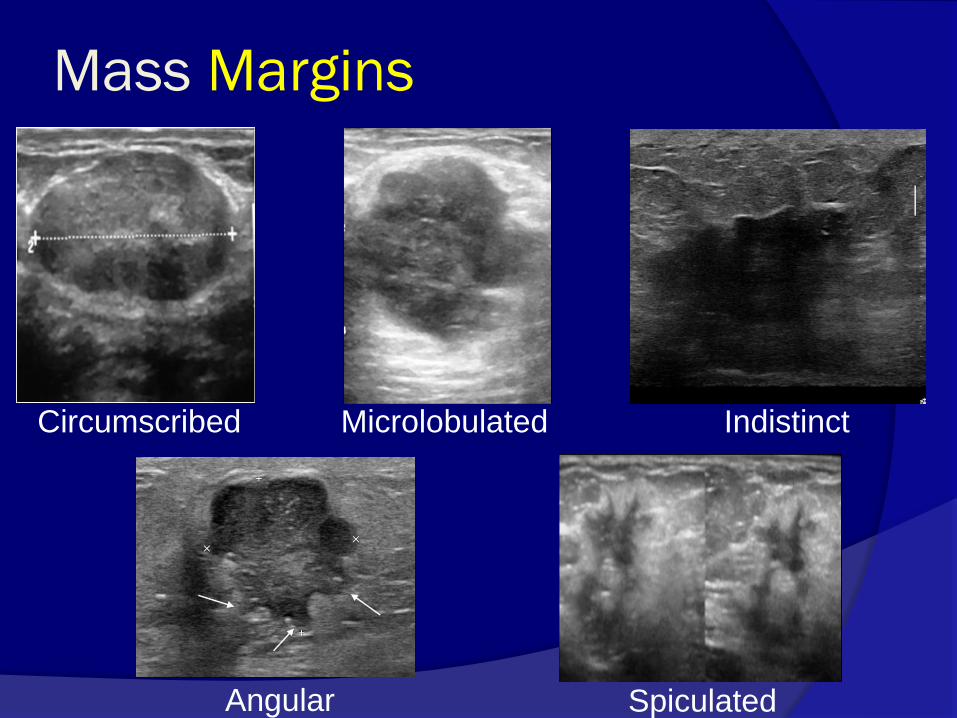
Mass Margins
Spiculated
Circumscribed
Angular
Microlobulated Indistinct
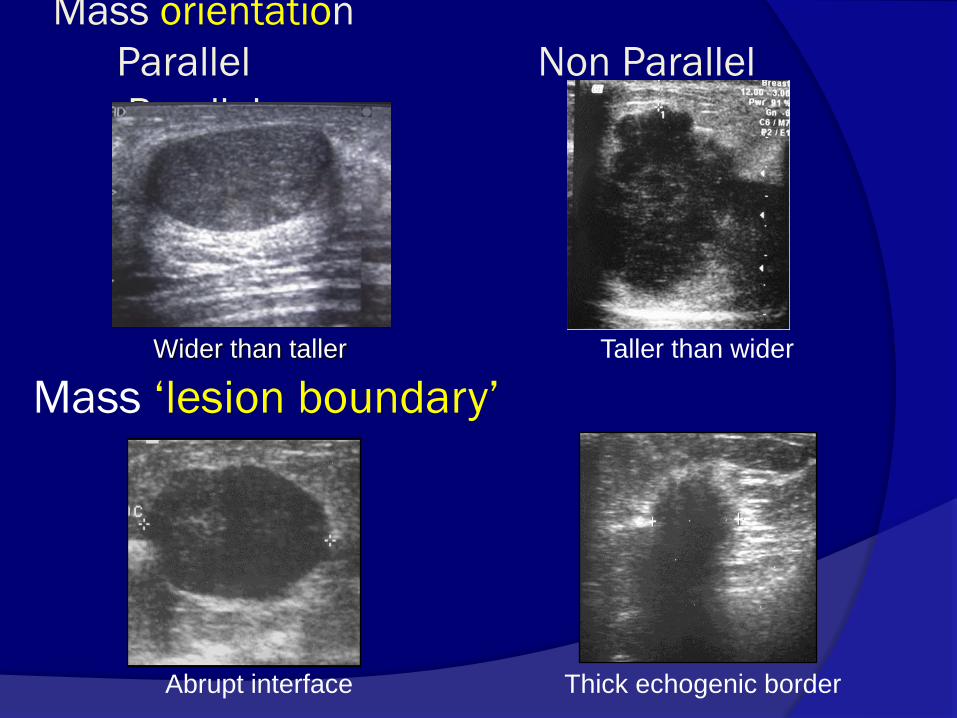
Mass orientation
Parallel Non Parallel
Parallel
Thick echogenic border
Taller than wider
Abrupt interface
Wider than taller
Mass ‘lesion boundary’

Mass echopattern
Anechoic Hypoechoic
Hyperechoic Complex Cystic /Solid
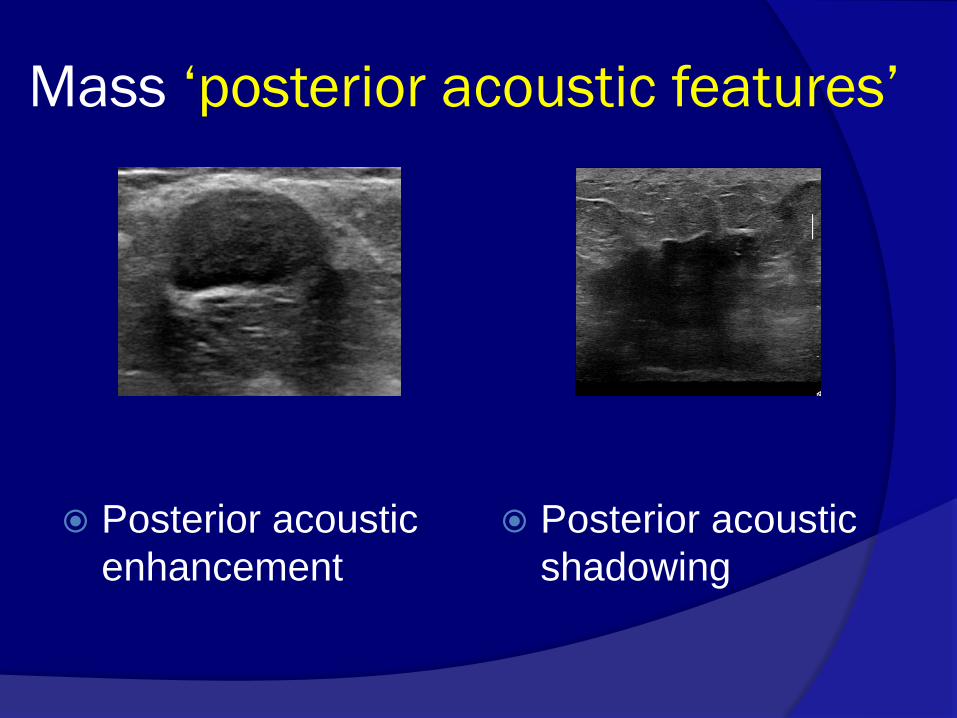
Mass ‘posterior acoustic features’
Posterior acoustic
enhancement
Posterior acoustic
shadowing
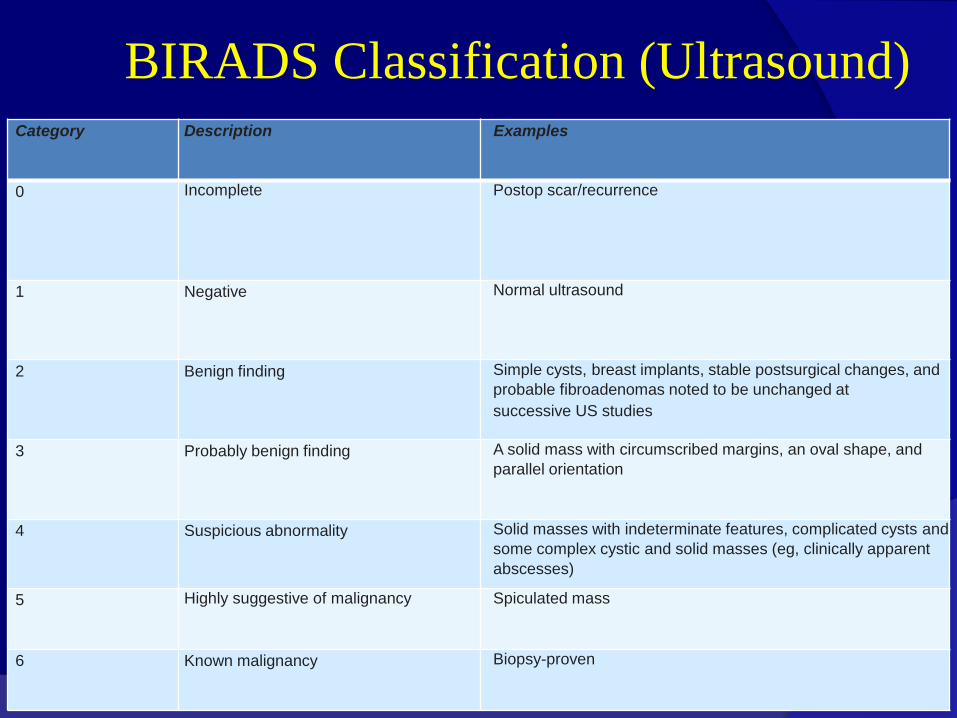
BIRADS Classification (Ultrasound) Category Description Examples
0 Incomplete Postop scar/recurrence
1 Negative Normal ultrasound
2 Benign finding Simple cysts, breast implants, stable postsurgical changes, and
probable fibroadenomas noted to be unchanged at
successive US studies
3 Probably benign finding A solid mass with circumscribed margins, an oval shape, and
parallel orientation
4 Suspicious abnormality Solid masses with indeterminate features, complicated cysts and
some complex cystic and solid masses (eg, clinically apparent
abscesses)
5 Highly suggestive of malignancy Spiculated mass
6 Known malignancy Biopsy-proven

Challenges in assigning Final category
Age of the patient Palpable probably
benign lesions
Abscess /
Hematoma
Differing categories
on various imaging
modalities
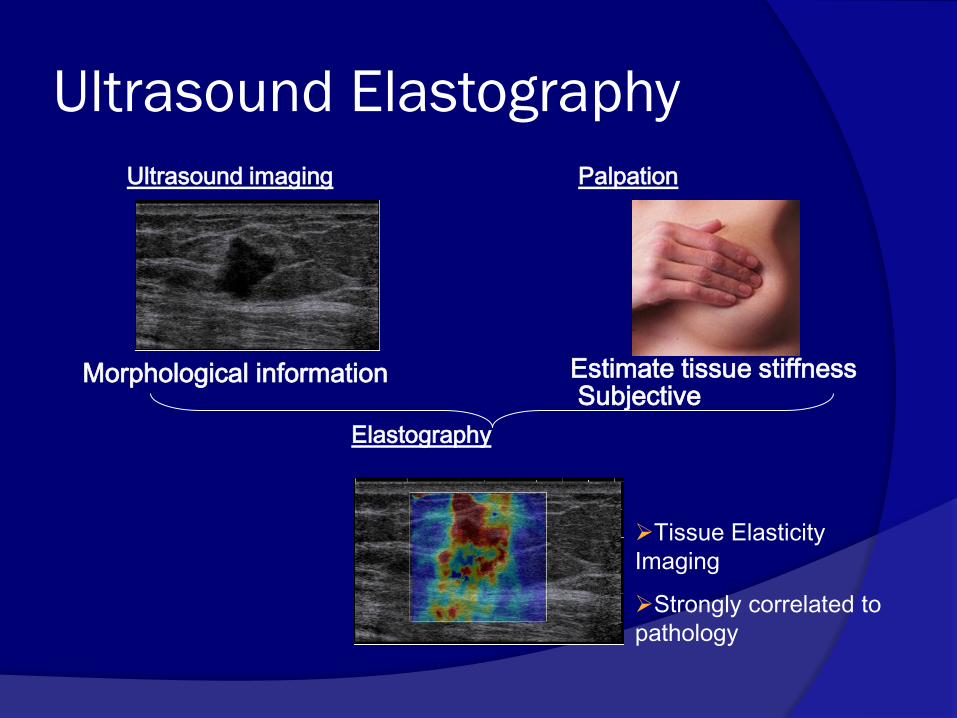
Ultrasound imaging Palpation
Morphological information Estimate tissue stiffness Subjective
Tissue Elasticity
Imaging
Strongly correlated to
pathology
Elastography
Ultrasound Elastography
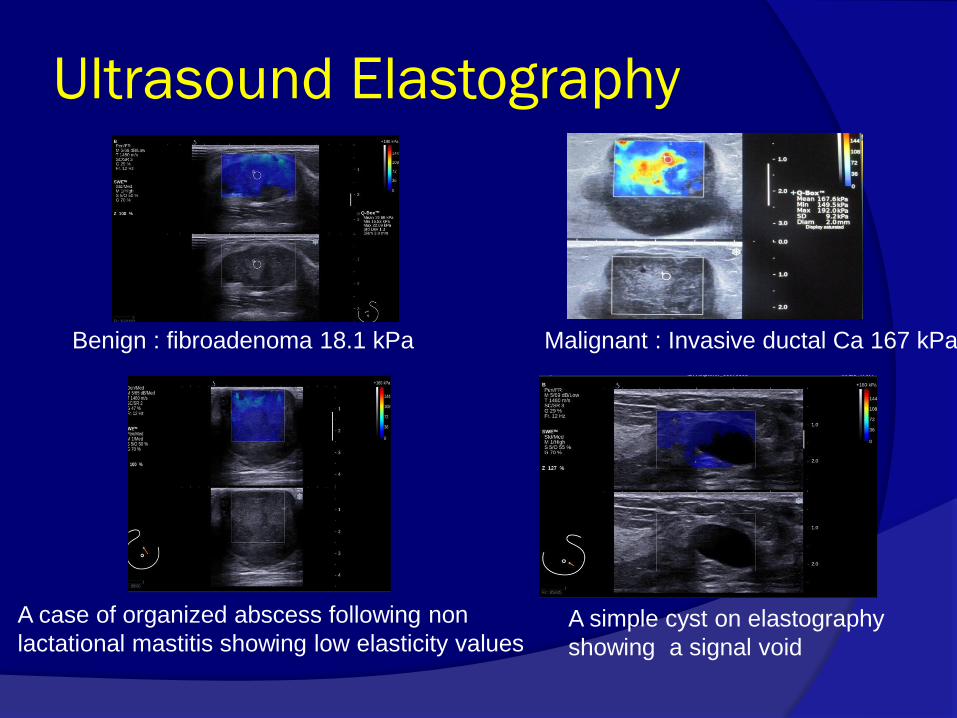
Benign : fibroadenoma 18.1 kPa Malignant : Invasive ductal Ca 167 kPa
Ultrasound Elastography
A case of organized abscess following non
lactational mastitis showing low elasticity values A simple cyst on elastography
showing a signal void
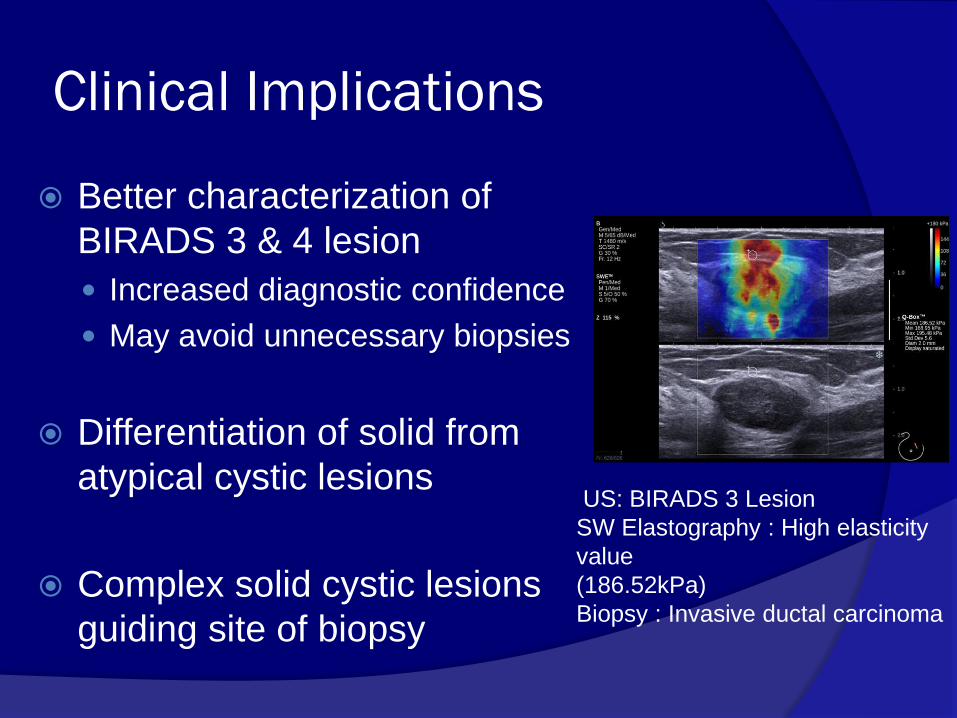
Clinical Implications
Better characterization of
BIRADS 3 & 4 lesion
Increased diagnostic confidence
May avoid unnecessary biopsies
Differentiation of solid from
atypical cystic lesions
Complex solid cystic lesions
guiding site of biopsy
US: BIRADS 3 Lesion
SW Elastography : High elasticity
value
(186.52kPa)
Biopsy : Invasive ductal carcinoma
Breast MRI
Well established adjunctive modality
Dedicated breast coils
Standardized protocols and ACR reporting lexicon
MR compatible needles
Enough literature available
Sensitivity high, Specificity moderate
Current Indications of MRI
Screening Women at a high risk of breast cancer
Diagnosis Equivocal mammogram / US
Occult breast primary in pts with axillary metastases
Staging Extent of cancer, Multifocal/ Multicentric/ Contralateral
Chest wall invasion
Infiltrating lobular cancer
Treatment Early assessment of response to NACT
Residual disease after completion of NACT
Differentiation of recurrence/ postop scar
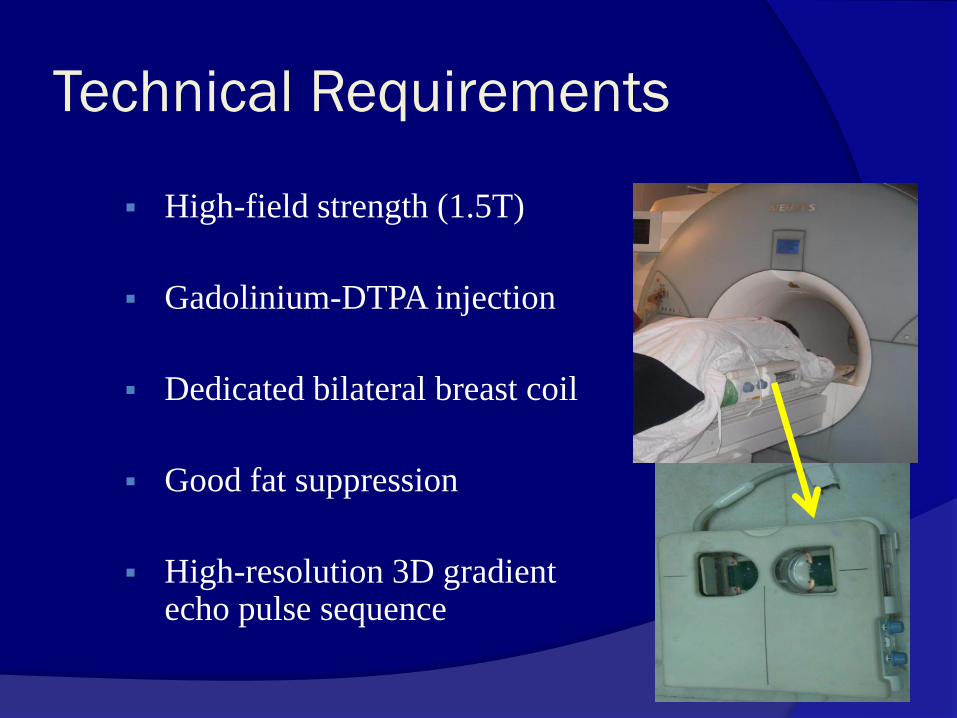
Technical Requirements
High-field strength (1.5T)
Gadolinium-DTPA injection
Dedicated bilateral breast coil
Good fat suppression
High-resolution 3D gradient echo pulse sequence
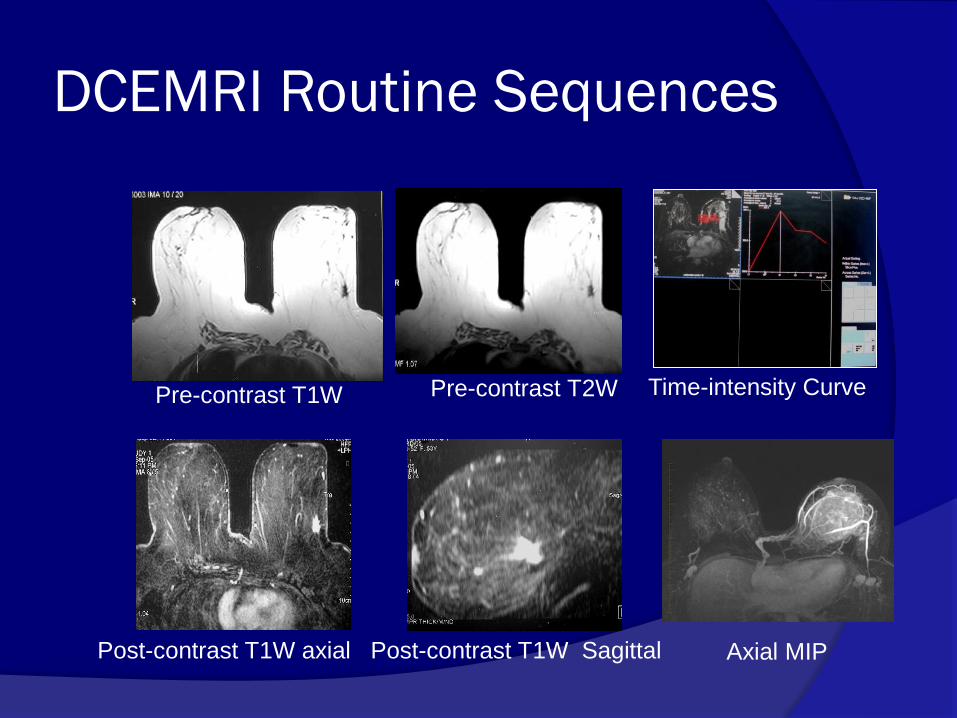
DCEMRI Routine Sequences
Pre-contrast T1W Pre-contrast T2W
Post-contrast T1W axial Post-contrast T1W Sagittal Axial MIP
Time-intensity Curve

ACR BI-RADS MRI Lexicon
Focus
Mass
Morphology
Precontrast Signal intensity
Contrast kinetics
Non masslike enhancement
Distribution
Symmetry
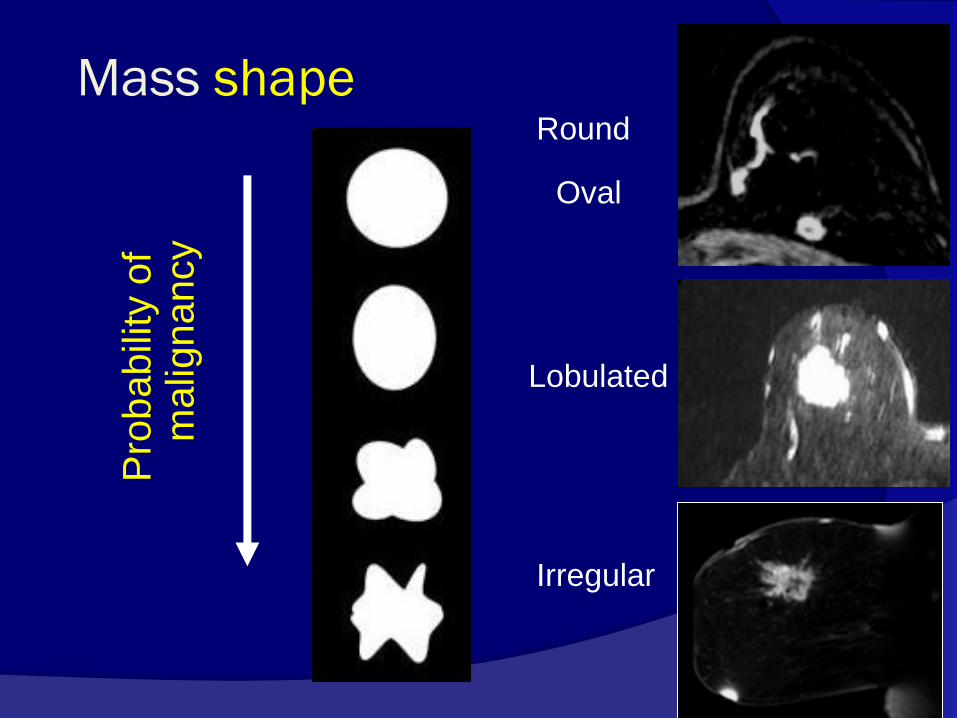
Mass shape
P
robabili
ty o
f m
alig
nancy
Round
Oval
Irregular
Lobulated
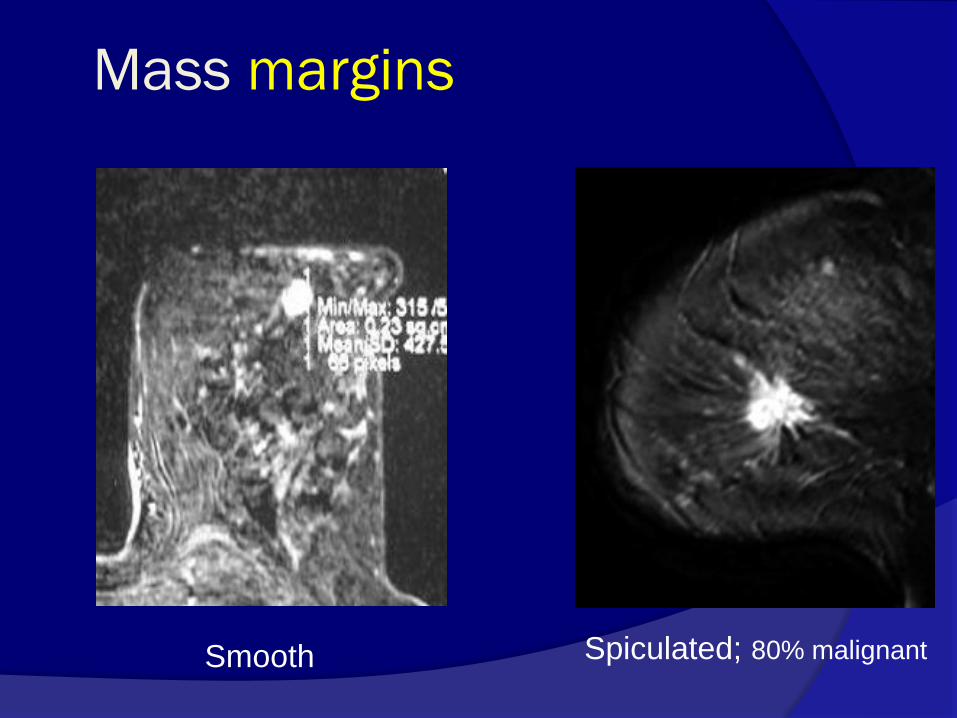
Mass margins
Smooth Spiculated; 80% malignant

Mass - Internal enhancement
Homogeneous Heterogeneous Nonenhancing
septations Rim enhancement
Enhancing
septations
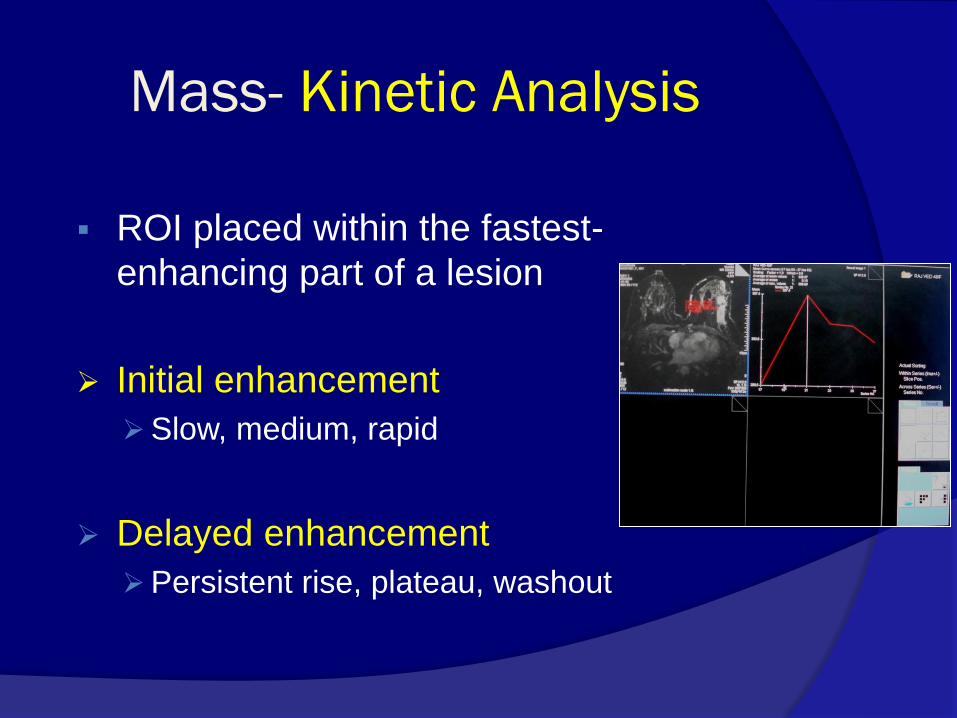
Mass- Kinetic Analysis
ROI placed within the fastest-
enhancing part of a lesion
Initial enhancement
Slow, medium, rapid
Delayed enhancement
Persistent rise, plateau, washout
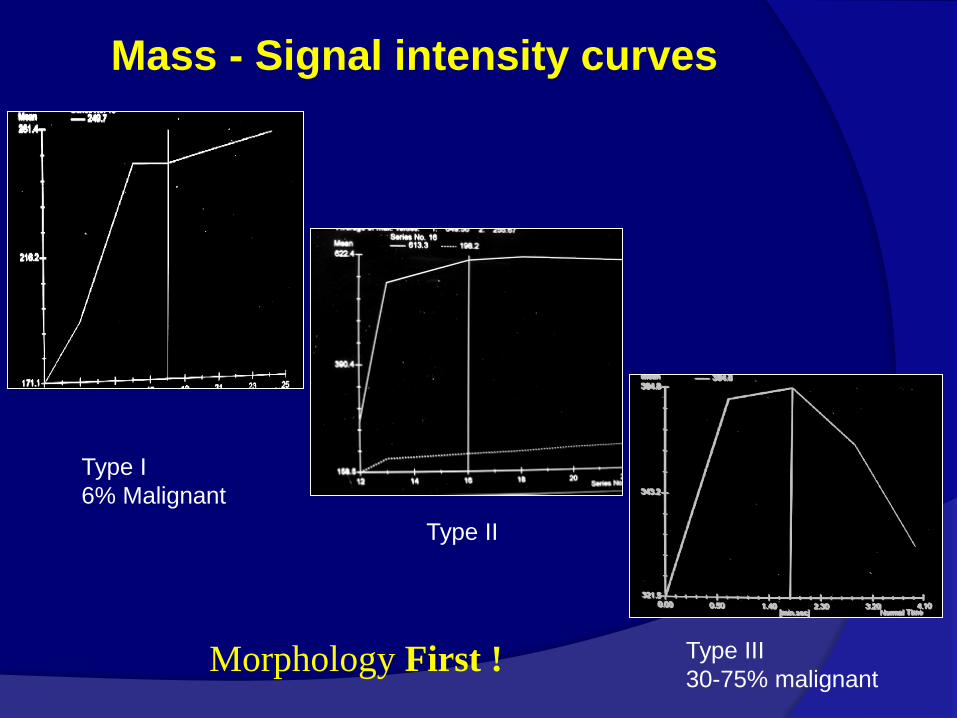
Mass - Signal intensity curves
Type I
6% Malignant
Type II
Type III
30-75% malignant Morphology First !
Non masslike enhancement
Descriptors
Distribution Internal
enhancement
Symmetry
Kinetic analysis misleading for non-mass like enhancement
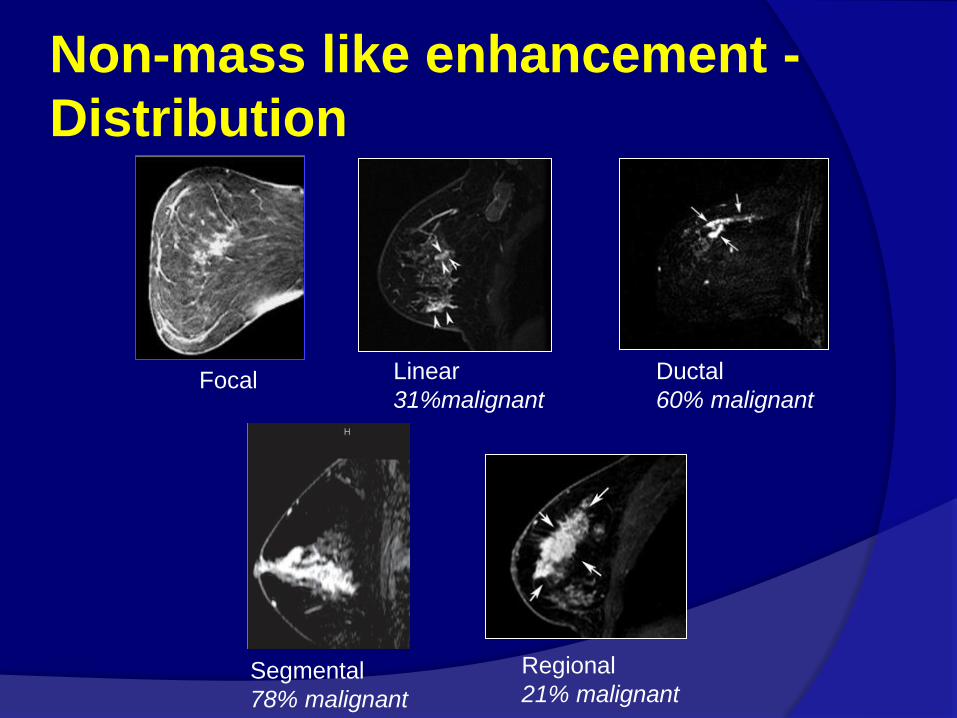
Non-mass like enhancement -
Distribution
Linear
31%malignant
Ductal
60% malignant
Segmental
78% malignant
Regional
21% malignant
Focal
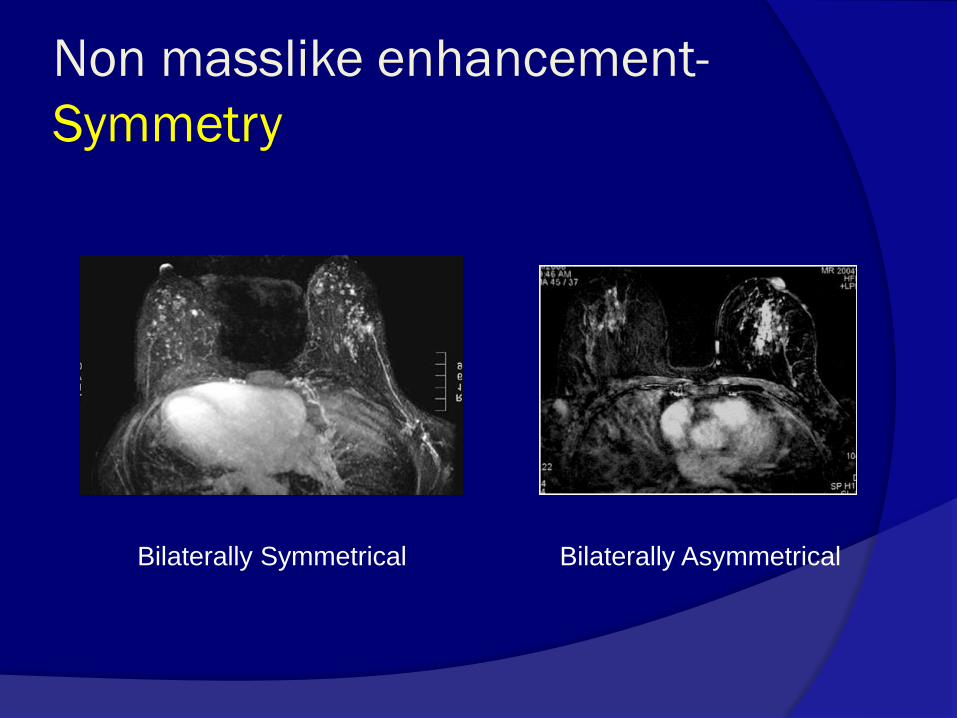
Non masslike enhancement-
Symmetry
Bilaterally Symmetrical Bilaterally Asymmetrical
Scintimammography
Breast Specific Gamma Imaging
PET

Further reading
ACR Guidelines: Breast Imaging