SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN surgery ...
18
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN Lecture delivered at the Royal College of Surgeons of England on 5th October 1956 by J. J. Mason Brown, O.B.E., F.R.C.S.Ed. Lecturer in Paediatric Surgery, University of Edinburgh; Surgeon, Royal Hospital for Sick Children, Edinburgh; Paediatric Surgeon, Royal Infirmary, Edinburgh INTRODUCTION THE SUBJECT FOR a lecture such as this should fulfil certain criteria. Full accounts of the subject should not be found in standard textbooks on surgery, recent work related to it should be available for assessment and problems should still remain in order that interest may be aroused in seeking their solution. Despite the large amount of time and thought devoted to this subject, especially in recent years, problems still remain, for had this not been so it would hardly have been chosen for discussion at recent meetings, both of the British Association of Surgeons and the American Surgical Association. Types of intestinal obstruction in the newborn In the neonate, intestinal obstruction is caused by a number of different lesions and some form of classification is desirable. On a pathological basis the obstruction may be complete or incomplete. This is an unsatis- factory classification because complete obstruction can occur although there is no macroscopic organic lesion. It seems preferable to reserve the terms, complete and incomplete, to describe the disturbance of the physiology which is of greater importance. Another common classification is into intrinsic and extrinsic obstructions depending on whether the pathological lesion lies in or outwith the intestine. While intrinsic lesions tend more frequently to be complete and to date from before birth in contradistinction to extrinsic ones, which are often incomplete and may not become apparent until after birth, the main essential is to have a classification which readily brings all the causes of neonatal obstruction under review by the surgeon at operation. Unless the surgeon is aware of all the possibilities he may not be able to establish the cause of the obstruction and apply the appropriate measures for its relief. As we are dealing with the newly born baby it is justifiable to borrow a classification which some obstetricians employ in describing the factors which may be responsible for difficulties in delivery, viz., faults in the passages, faults in the passenger, faults in the powers and extrinsic factors. 280
Transcript of SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN surgery ...
SMALL INTESTINE OBSTRUCTION IN THENEWLY BORN
Lecture delivered at the Royal College of Surgeons of Englandon
5th October 1956by
J. J. Mason Brown, O.B.E., F.R.C.S.Ed.
Lecturer in Paediatric Surgery, University of Edinburgh; Surgeon, Royal Hospital forSick Children, Edinburgh; Paediatric Surgeon, Royal Infirmary, Edinburgh
INTRODUCTION
THE SUBJECT FOR a lecture such as this should fulfil certain criteria. Fullaccounts of the subject should not be found in standard textbooks onsurgery, recent work related to it should be available for assessmentand problems should still remain in order that interest may be arousedin seeking their solution. Despite the large amount of time and thoughtdevoted to this subject, especially in recent years, problems still remain,for had this not been so it would hardly have been chosen for discussionat recent meetings, both of the British Association of Surgeons and theAmerican Surgical Association.
Types of intestinal obstruction in the newbornIn the neonate, intestinal obstruction is caused by a number of different
lesions and some form of classification is desirable. On a pathologicalbasis the obstruction may be complete or incomplete. This is an unsatis-factory classification because complete obstruction can occur althoughthere is no macroscopic organic lesion. It seems preferable to reservethe terms, complete and incomplete, to describe the disturbance of thephysiology which is of greater importance.Another common classification is into intrinsic and extrinsic obstructions
depending on whether the pathological lesion lies in or outwith theintestine. While intrinsic lesions tend more frequently to be completeand to date from before birth in contradistinction to extrinsic ones, whichare often incomplete and may not become apparent until after birth,the main essential is to have a classification which readily brings all thecauses of neonatal obstruction under review by the surgeon at operation.Unless the surgeon is aware of all the possibilities he may not be able toestablish the cause of the obstruction and apply the appropriate measuresfor its relief.As we are dealing with the newly born baby it is justifiable to borrow
a classification which some obstetricians employ in describing the factorswhich may be responsible for difficulties in delivery, viz., faults in thepassages, faults in the passenger, faults in the powers and extrinsicfactors.
280
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
TABLE INEONATAL OBSTRUCTIONS IN THE SMALL INTESTINE
Fatults in the passagesC Atresia
CONGENITAL -A StenosisCystic duplication
Faults in the powers( Defects of the myenteric plexus
CONGENITAL - Pyloric stenosisLocalised spasm
from peritonitisACQUIRED Paralytic ileus ( from maternal drugs
Faults in the passengerC Meconium ileus
CONGENITAL ( Meconium plugsExtrinsic
( Adhesions and bandsAnnular pancreas
CONGENITAL Meckel's diverticulumI hernia (~~~ExternalIncarceration of hernia Internal
Errors of intestinal rotation
ACQUIRED Post-operative adhesions
Faults in the passagesCongenital atresia is the term applied to complete occlusion of the
lumen of the bowel. It varies in severity from simple occlusion by animperforate diaphragm to complete absence of varying lengths of bowel.Atresias are frequently multiple, the common sites being the duodenum,ileum and, less commonly, it is found in the jejunum and colon. Itsoccurrence in the oesophagus and ano-rectal region is, of course, beyondthe scope of our discussion.
Congenital stenosis is the term applied to an organic narrowing of asegment of the intestine which occurs most frequently in the duodenumand ileum. Because the obstruction is incomplete symptoms may notoccur in the neonatal period. Similar incomplete obstructive symptomsmay follow partial occlusion of the intestine by a perforated diaphragm.
Cystic duplications which do not communicate with the parent loopcompress the bowel and may cause simple obstruction or may be compli-cated by volvulus of the loop. These are probably most frequent in thejejunum.
Faults in the powersThese include all disorders of peristalsis.Paralytic ileus follows peritoneal infection or the exhibition of
methonium drugs to the mother. Localised intense spasm may occurand this is difficult to establish unless spasm occurs while the intestineis being examined. I have seen it in the ileum on two occasions. Defectsof the ganglion cells of the myenteric plexus are now recognised to be thecause of Hirschsprung's disease. The aganglionic segment in some casesinvolves the lower ileum as well as the rectum and colon. Pyloric stenosis
281
J. J. MASON BROWN
might be considered under this heading but as a rule symptoms do notoccur until the third week of life and most patients are brought fortreatment beyond the neonatal period.
Faults in the passenger
The passenger is, of course, meconium and it may be abnormally toughand tenacious in cases of congenital cystic fibrosis of the pancreas so thatthe bowel is incapable of passing it beyond the lower ileum-meconiumileus. In other cases the pancreas may be normal but obstruction occursdue to the presence of an impacted meconium plug.
Extrinsic lesions
These may be congenital or acquired or there may be a congenitalanomaly which predisposes to the development of an acquired condition,e.g., incarceration of an inguinal hernia.
External hernia, incarcerated inguinal hernia being the most common.Internal hernia.-Incarceration of diaphragmatic or peritoneal herniae
may occur.Errors of rotation of the midgut loop, which may cause duo denal
obstruction from the pressure of peritoneal bands, or from volvulus ofthe midgut loop around the duodeno-colic isthmus-volvulus neonatorum.
Congenital adhesions and bands associated with structures, such as thevitello-intestinal duct or the omphalo-mesenteric artery may causeobstruction in the neonatal period, although it is more common later ininfancy and childhood.
Annular pancreas may obstruct the duodenum in the newly born andmay be associated with atresia of the duodenum.
Coexistence of different types of obstruction
Extrinsic and intrinsic lesions may be found together and the onlysafe rule is for the surgeon to verify that the obstruction has been relievedand that no further lesion exists distal to it.
Incidence of intestinal obstruction in the newly born
The incidence of intestinal obstruction in the newly born baby hasbeen estimated to occur once in 1,500 births (Evans, 1951) while atresiaof the intestine occurs only once in 8,000 deliveries (Chisholm, et al, 1954).The increasing numbers of cases reported suggest that the condition isprobably more common than these figures indicate.
Pathological anatomy and physiologyMeconium is formed from the secretions of the alimentary tract and its
associated glands (liver and pancreas), as well as from the constituentsof the liquor amnii which the foetus swallows. Normal meconium is a
282
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
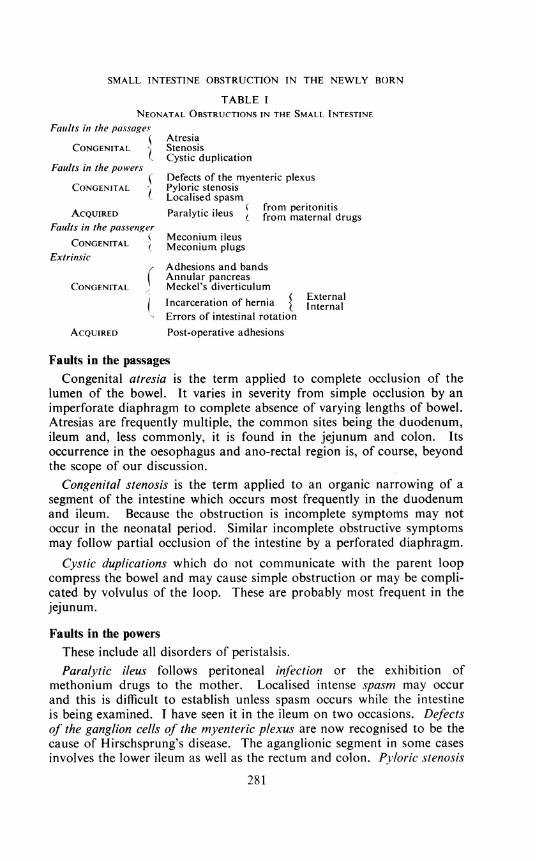
viscid semi-fluid substance, dark green to almost black in colour frombile pigments. It contains lanugo hairs and squamous epithelial cellsderived from the vernix caseosa. Normally at birth the meconium issterile and fills the greater part of the ileum and colon.When there is a complete or virtually complete obstruction, due to
atresia or to severe stenosis or meconium ileus, the effects of obstructionhave been present for a considerable time before birth and the baby isborn with a chronic foetal obstruction. Following the swallowing of air,the increased secretions, attempts at feeding the baby plus the inevitableinfection of the bowel content and the onset of fermentation in the gut,the chronic obstruction gives way to one of fulminating acuity.The evidence of chronic intra-uterine obstruction is clear, for the upper
blind loop shows marked enlargement with considerable hypertrophy of
Fig. 1. Plain radiograph three hours after birth. Complete absence of air in thesmall bowel. Intraperitoneal calcification indicative of pre-natal perforation
with meconium peritonitis.
283
J. J. MASON BROWN
its wall and with the onset of acute post-natal obstruction it becomesgreatly dilated. In some cases pre-natal abdominal distension interfereswith the delivery of the baby.
Severe obstruction arising early in intra-uterine life may result in pre-natal perforation of the bowel (Fig. 1), with the development of meconium
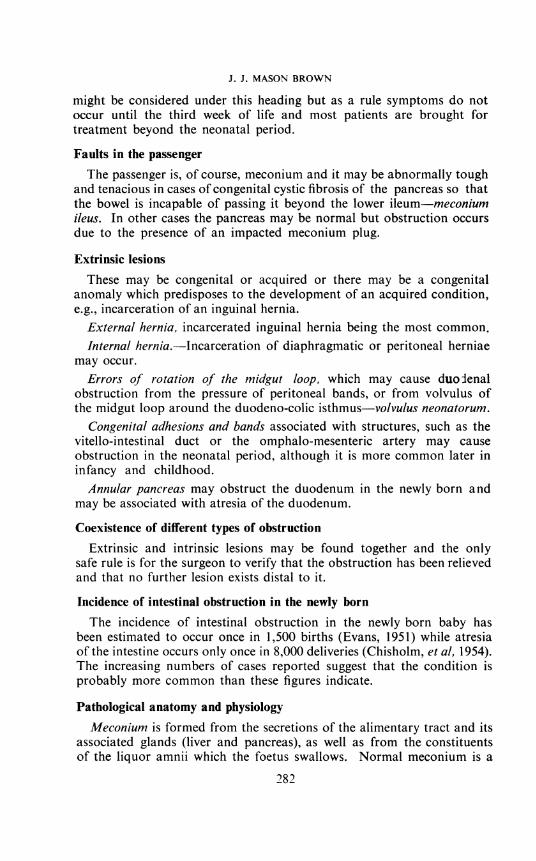
Fig. 2. Plain radiograph fourth day of life showing pneumoperitoneum frompost-natal perforation of the intestine.
peritonitis first described by Simpson (1838). Perforation of the bowelmay occur as early as the fourth month of foetal life but may also happenduring or shortly after birth (Packard and Reynolds, 1951) (Fig. 2).
The bowel distal to these obstructions has never functioned ; it is thin-walled and contracted with a minute lumen and virtually no content.The colon in these cases presents the features of what is often described
284
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
as microcolon. The small amount of content has a dirty grey colour anddoes not contain either lanugo hairs or squamous epithelial cells and thisis the basis for Farber's test.
Etiology of complete atresiaSome sixteen different theories have been advanced to explain the
occurrence of intestinal atresia (O'Neill et al., 1948) but few are worthy ofconsideration. Bland-Sutton (1889) believed that such congenital lesionsoccurred at the site of major embryological events and support for thistheory is afforded by the frequency with which atresia is found in theduodenum in the region of the ampulla of Vater and at the junction of thefore and midgut loops. It does not explain the frequency of ileal atresiaexcept, possibly, at the site of origin of the vitello-intestinal duct.
In embryos of about 10 mm., i.e., about six weeks old, there is such activegrowth in length of the intestine that the midgut loop herniates throughthe umbilicus and just previous to or coincident with this increase inlength there is vigorous proliferation of the epithelial cells which actuallyocclude the lumen of the gut. This proliferative occlusion only affectspart of the intestine at any one time. Tandler (1900) described thisproliferative occlusion in the duodenum and its recanalisation by theappearance, enlargement and coalescence of vacuoles within the centralcore of cells. He concluded that duodenal atresia and stenosis resultedfrom failure of the process of vacuolation to occur. Kreuter (1909)believed that a similar process of proliferation and vacuolation occurredthroughout the small intestine but this is questioned by other embryo-logists. Madden and McCann (1956) point out that although relativelyrare atresias, stenoses and diaphragms occur in the colon which does notpass through a solid stage during development. They also suggest that:similar congenital obstructive anomalies occur in the duodenum and theaorta and the latter does not pass through a solid phase during develop-ment.As Tandler's theory does not explain the coexistence of atresias with
fistula, e.g., in the oesophagus, Aird (1939) considered that liability toatresia is a function of rapid increase in length at an early stage. It ispossible that increased longitudinal tension will result in narrowing orinterruption of the bowel. Nixon (1955), on the other hand, believes thatbecause of the structure of the wall of the atretic area, because of the almostinvariable evidence of a microscopic meconium peritonitis and because thegut shows incomplete mesenteric fixation, the causal lesion is a vascularaccident to the formed midgut loop, probably as the result of incarcerationof the physiological umbilical hernia. This theory would explain theshortening of the small intestine which is a feature of some cases of atresia.On the other hand it does not explain atresia of the duodenum, largeintestine or rectum. No theory of the etiology has yet succeeded inexplaining all the sites at which atresia occurs but this does not necessarily
285
J. J. MASON BROWN
mean that all are invalid because different factors may well be responsibleat different sites.
Clinical features of neonatal obstructionThe symptoms are vomiting and abnormalities in the passage of
meconium while the signs are distension, visible peristalsis and the findingson investigation of the rectum, vomitus and stool and the evidenceafforded by radiography. These require further consideration.
Vomiting.-Vomiting occurs in the neonatal period following intra-cranial birth injury, from infection and in prematurity but the only saferule is to investigate every case of bilious vomiting and of persistentnon-bilious vomiting immediately. The investigation does not harm thebaby and should it prove negative medical measures can be continuedconfidently in the sure knowledge that a " surgical" lesion has not beenmissed. It is only by insisting on the investigation of all cases of biliousvomiting that the diagnosis of neonatal obstruction will be madesufficiently early to give the baby a good chance of survival.
Vomiting occurs later in incomplete and in low obstructions than itdoes in complete and proximal ones and as the vast majority of obstructivelesions occur distal to the ampulla of Vater the vomitus is usually bile-stained. In some cases of atresia about ampullary level the bile duct mayenter both the upper and the lower loop and the vomitus then containsbile.
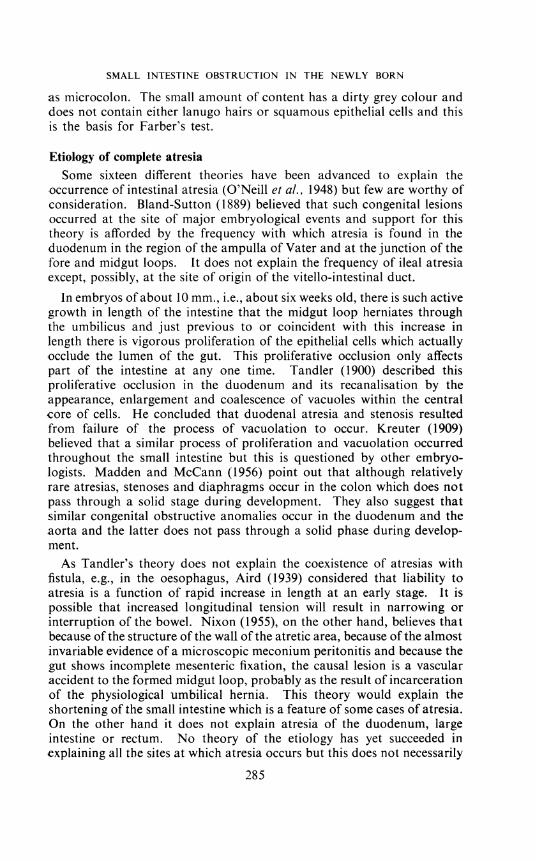
(1) (b)1Fig. 3. Antero-posterior and lateral views showing enormous distension andfluid level in dilated small bowel due to ileal atresia. (Mr. F. H. Robart's case.)
286
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
MeconiumMost (about 92 per cent.) normal babies pass meconium within the
first twenty-four hours. Any delay beyond thirty-six hours should beregarded with suspicion and the rectum should be examined. Anymeconium or material obtained should be investigated.
Distension
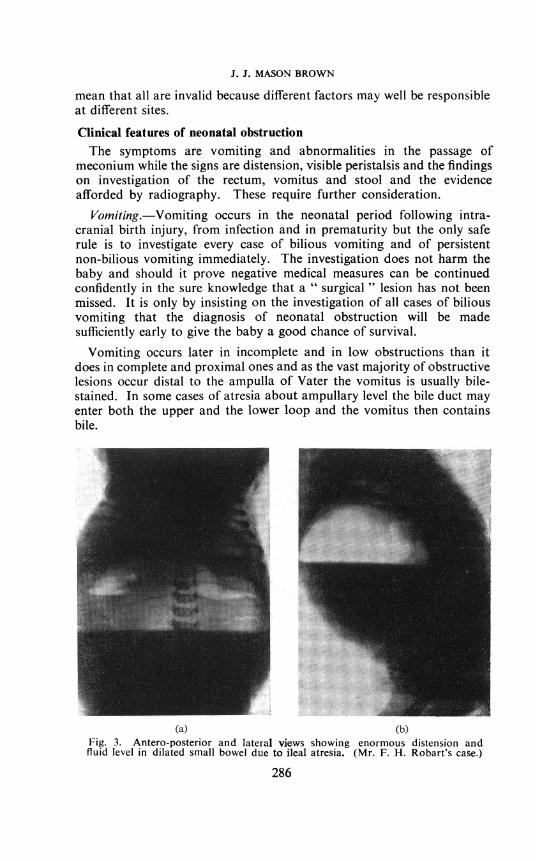
In high complete obstructions the baby may vomit so readily that thereis no obvious distension. In other cases and in the more chronic in-complete obstructions there may be obvious distension of the stomachand/or duodenum with visible peristalsis. In obstruction at a lower levelthere may be enormous distension of the proximal loop of bowel (Fig. 3)and this may be so great that it is mistaken for generalised distension.
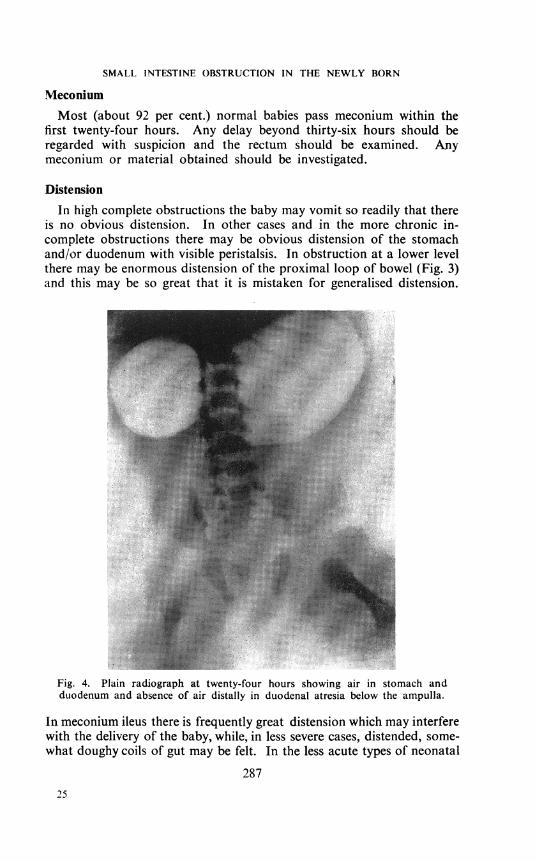
Fig. 4. Plain radiograph at twenty-four hours showing air in stomach andduodenum and absence of air distally in duodenal atresia below the ampulla.
In meconium ileus there is frequently great distension which may interferewith the delivery of the baby, while, in less severe cases, distended, some-what doughy coils of gut may be felt. In the less acute types of neonatal
28725
J. J. MASON BROWN
obstruction due to Hirschsprung's disease affecting a short segmentthere is sometimes distension and visible peristalsis of the transversecolon.
Rectal examination excludes all types of ano-rectal atresia, reveals thecontracted empty rectum of Hirschsprung's disease or of completeobstruction at a higher level in which latter it is often followed by thepassage of small amounts of greyish-white material.
RadiologyWhile the diagnosis of neonatal obstruction may be made on clinical
grounds radiography is invaluable. The normal baby begins to swallowair immediately after birth and each breath allows more air to enter theoesophagus and stomach so that air passes into the small intestine atone to three hours, is closely packed in the small bowel at eight hoursand is usually seen radiologically in the colon within twelve to eighteenhours after birth (Wasch and Marck, 1948). On the plain radiographthe signs of obstruction are progressively dilating bowel with clear areas
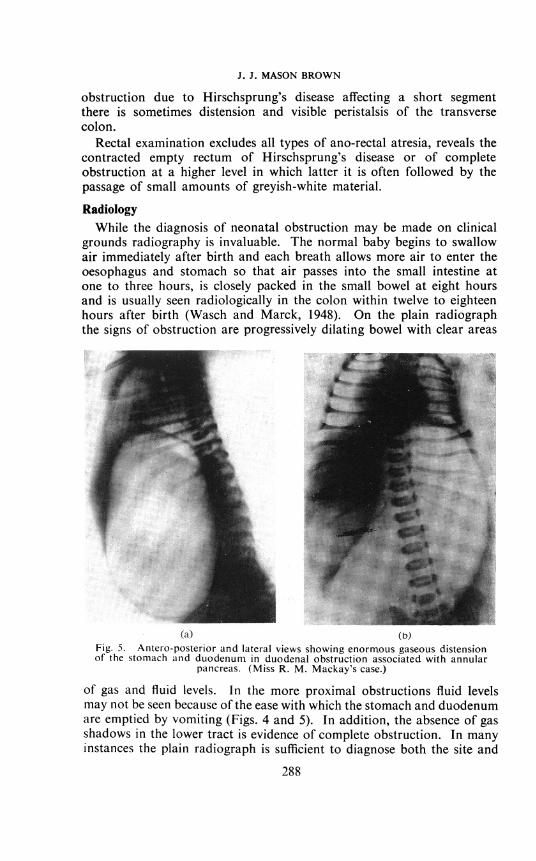
(a) (b)Fig. 5. Antero-posterior and lateral views showing enormous gaseous distensionof the stomach and duodenum in duodenal obstruction associated with annular
pancreas. (Miss R. M. Mackay's case.)
of gas and fluid levels. In the more proximal obstructions fluid levelsmay not be seen because of the ease with which the stomach and duodenumare emptied by vomiting (Figs. 4 and 5). In addition, the absence of gasshadows in the lower tract is evidence of complete obstruction. In manyinstances the plain radiograph is sufficient to diagnose both the site and
288
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
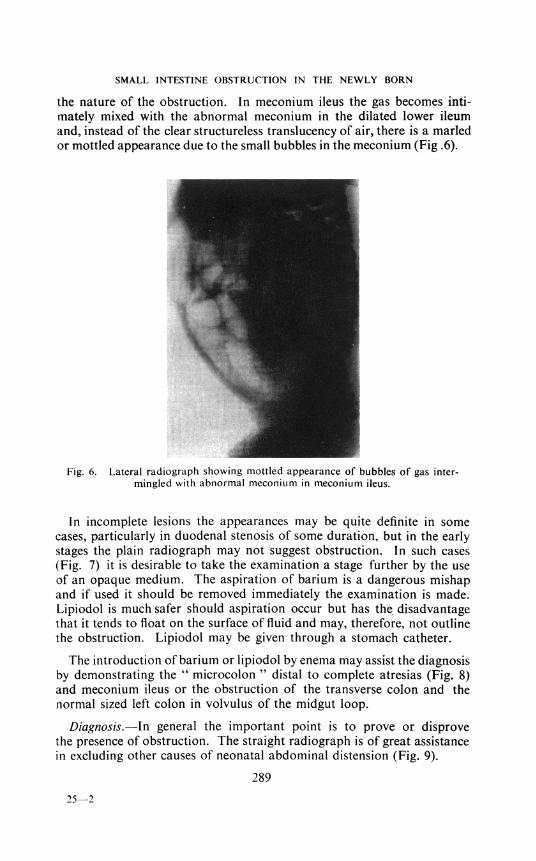
the nature of the obstruction. In meconium ileus the gas becomes inti-mately mixed with the abnormal meconium in the dilated lower ileumand, instead of the clear structureless translucency of air, there is a marledor mottled appearance due to the small bubbles in the meconium (Fig .6).
Fig. 6. Lateral radiograph showing mottled appearance of bubbles of gas inter-mingled with abnormal meconium in meconium ileus.
In incomplete lesions the appearances may be quite definite in somecases, particularly in duodenal stenosis of some duration, but in the earlystages the plain radiograph may not suggest obstruction. In such cases(Fig. 7) it is desirable to take the examination a stage further by the useof an opaque medium. The aspiration of barium is a dangerous mishapand if used it should be removed immediately the examination is made.Lipiodol is much safer should aspiration occur but has the disadvantagethat it tends to float on the surface of fluid and may, therefore, not outlinethe obstruction. Lipiodol may be given through a stomach catheter.
The introduction of barium or lipiodol by enema may assist the diagnosisby demonstrating the " microcolon " distal to complete atresias (Fig. 8)and meconium ileus or the obstruction of the transverse colon and thenormal sized left colon in volvulus of the midgut loop.
Diagnosis.-In general the important point is to prove or disprovethe presence of obstruction. The straight radiograph is of great assistancein excluding other causes of neonatal abdominal distension (Fig. 9).
289
25-2
J. J. MASON BROWN
TreatmentPreoperative.-A catheter is inserted into the stomach and aspirationi
is maintained. Polythene tubing, or a fine cannula is inserted into thesaphenous vein at the ankle for the rapid correction of the fluid deficit
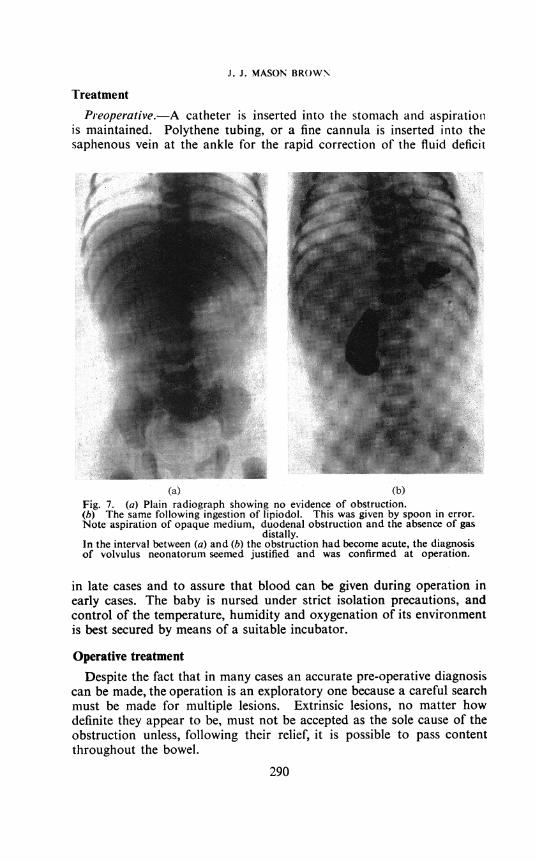
(a) (b)Fig. 7. (a) Plain radiograph showing no evidence of obstruction.(b) The same following ingestion of lipiodol. This was given by spoon in error.Note aspiration of opaque medium, duodenal obstruction and the absence of gas
distally.In the interval between (a) and (b) the obstruction had become acute, the diagnosisof volvulus neonatorum seemed justified and was confirmed at operation.
in late cases and to assure that blood can be given during operation inearly cases. The baby is nursed under strict isolation precautions, andcontrol of the temperature, humidity and oxygenation of its environmentis best secured by means of a suitable incubator.
Operative treatment
Despite the fact that in many cases an accurate pre-operative diagnosiscan be made, the operation is an exploratory one because a careful searchmust be made for multiple lesions. Extrinsic lesions, no matter howdefinite they appear to be, must not be accepted as the sole cause of theobstruction unless, following their relief, it is possible to pass contentthroughout the bowel.
290
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
The exposure must be generous by a long transverse or paramedianincision. The surgeon must not potter about with fingers or hand insidethe abdomen trying in vain to elucidate the pathology but should deliverthe intestine for complete examination.
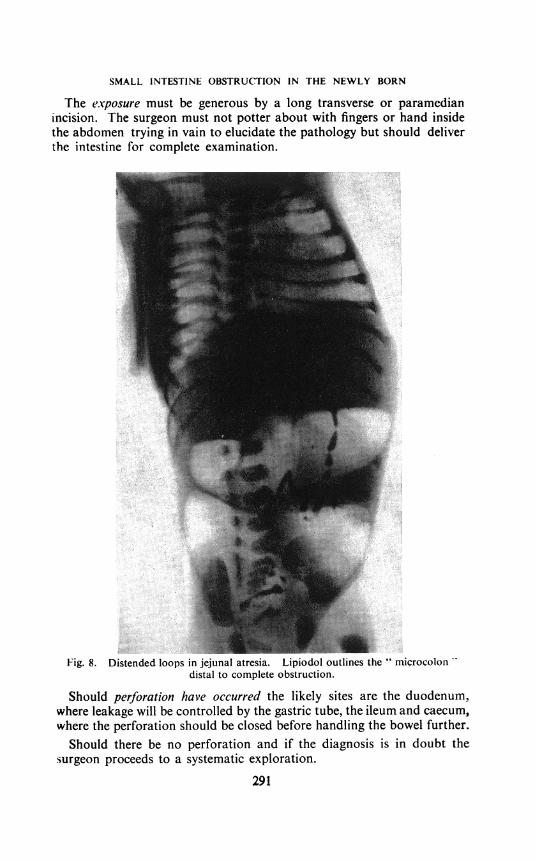
Fig. 8. Distended loops in jejunal atresia. Lipiodol outlines the " microcolon 'distal to complete obstruction.
Should perforation have occurred the likely sites are the duodenum,where leakage will be controlled by the gastric tube, the ileum and caecum,where the perforation should be closed before handling the bowel further.Should there be no perforation and if the diagnosis is in doubt the
surgeon proceeds to a systematic exploration.291
J. J. MASON BROWN
If the transverse colon is not visible and somewhat distended anddiscoloured coils of small gut appear to fill the whole abdomen there isvolvulus of the midgut loop (Glover and Barry, 1949). The gut is deliveredand the volvulus is undone by counter clockwise rotation. Attention is
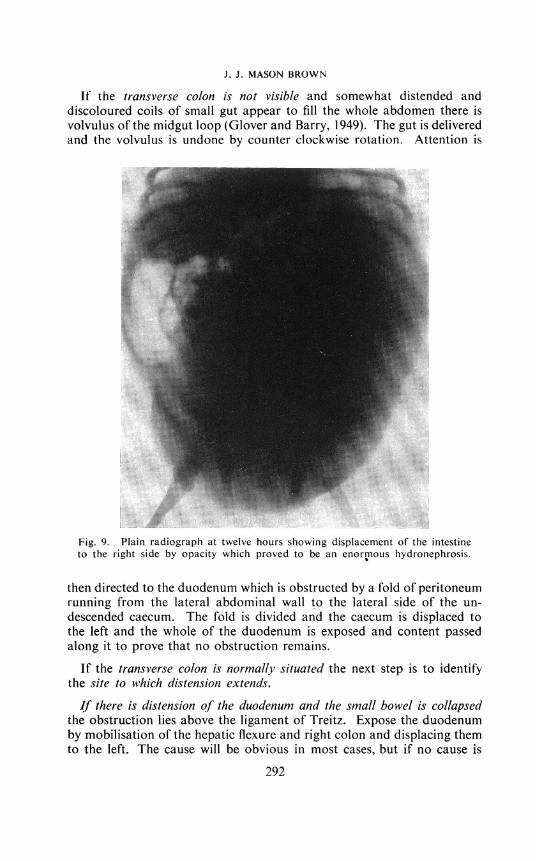
Fig. 9. Plain radiograph at twelve hours showing displacement of the intestineto the right side by opacity which proved to be an enormous hydronephrosis.
then directed to the duodenum which is obstructed by a fold of peritoneumrunning from the lateral abdominal wall to the lateral side of the un-descended caecum. The fold is divided and the caecum is displaced tothe left and the whole of the duodenum is exposed and content passedalong it to prove that no obstruction remains.
If the transverse colon is normally situated the next step is to identifythe site to which distension extends.
If there is distension of the duodenum and the small bowel is collapsedthe obstruction lies above the ligament of Treitz. Expose the duodenumby mobilisation of the hepatic flexure and right colon and displacing themto the left. The cause will be obvious in most cases, but if no cause is
292
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
found the gastric tube shold be persuaded past the pylorus lest a diaphragmbe missed.
If the upper small bowel is distended and the lower collapsed the lesionis in the jejunum or upper ileum. If the small bowel is mostlv distendedand the caecum is minute the lesion is in the lower ileum.
If the proximal colon is distended and the distal colon collapsed the lesionlies in the colon. If the greater part of the colon is distended the lesionlies in the anus, rectum or sigmoid. Ano-rectal atresia should have beendiagnosed before operation, while the apparent absence of an organiclesion is indicative of the functional obstruction of Hirschsprung's disease.The treatment of these lesions is beyond the scope of this lecture.
In all cases the appropriate treatment is carried out. Yes, but what isit ?
Meconiuni ileus is recognised by the beaded appearance of the lowestileal loop containing small firm nodules of meconium and the enormousdistension of the loop above it with doughy abnormal meconium. Thismore proximal loop is very heavy and may undergo volvulus. The onlypossible relief in these severe cases is by the removal of the bulk of theabnormal meconium. This may be done by multiple enterotomies(Hiatt and Wilson, 1948) or, better, by the passage of as much content aspossible into the dilated loop which is then resected, leaving a doublebarrelled enterostomy (Gross, 1953). Post-operatively the clearance of thebowel is assisted by the introduction of pancreatin or peroxide (Olimand Ciuti, 1954) into the enterostomy and the giving of pancreatin bymouth.
Operations for atresiaOperation has established that there is atresia of the duodenum with
the usual gross disparity in size between the upper and distal loops. Ifthe obstruction is proximal to the ampulla of Vater gastro-jejunostomy isadvisable while if it lies distal to the ampulla of Vater the alternatives areduodeno-duodenostomy or duodeno-jejunostomy.
In acute intestinal obstruction it is usually advisable to do the minimumprocedure which will relieve the obstruction. In the neonate, however,it is better to go beyond this and to relieve the obstruction, restore thecontinuity of the gut and bring about an early return of normal intestinalfunction.
Duodeno-jejunostomy fulfils the first two requirements but even anadequate anastomosis fails to function for some days and the feedingof the baby must be begun. The difficulty may be overcome by duodeno-jejunostomy plus:
(a) The passage of the gastric tube through the pylorus and the anasto-mosis into the jejunum. This may be technically difficult.
293
J. J. MASON BROWN
(b) The stomach tube is left in situ for aspiration. A gastrostomy ismade but the catheter is passed through the anastomosis and isused for feeding (Ehrenpreis and Sandblom, 1949).
(c) The procedure is similar to (b) except that a jejunostomy is madefor feeding purposes in place of the gastrostomy.
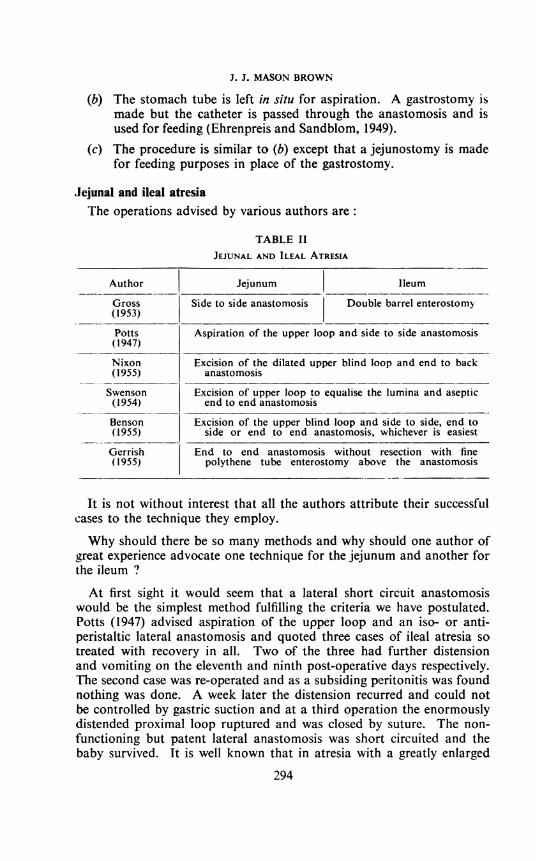
Jejunal and ileal atresiaThe operations advised by various authors are:
TABLE IIJEJUNAL AND ILEAL ATRESIA
Author Jejunum Ileum
Gross Side to side anastomosis Double barrel enterostomy(1953)
Potts Aspiration of the upper loop and side to side anastomosis(1947)
Nixon Excision of the dilated upper blind loop and end to back(1955) anastomosis
Swenson Excision of upper loop to equalise the lumina and aseptic(1954) end to end anastomosis
Benson Excision of the upper blind loop and side to side, end to(1955) side or end to end anastomosis, whichever is easiest
Gerrish End to end anastomosis without resection with fine(1955) polythene tube enterostomy above the anastomosis
It is not without interest that all the authors attribute their successfulcases to the technique they employ.
Why should there be so many methods and why should one author ofgreat experience advocate one technique for the jejunum and another forthe ileum ?
At first sight it would seem that a lateral short circuit anastomosiswould be the simplest method fulfilling the criteria we have postulated.Potts (1947) advised aspiration of the upper loop and an iso- or anti-peristaltic lateral anastomosis and quoted three cases of ileal atresia sotreated with recovery in all. Two of the three had further distensionand vomiting on the eleventh and ninth post-operative days respectively.The second case was re-operated and as a subsiding peritonitis was foundnothing was done. A week later the distension recurred and could notbe controlled by gastric suction and at a third operation the enormouslydistended proximal loop ruptured and was closed by suture. The non-functioning but patent lateral anastomosis was short circuited and thebaby survived. It is well known that in atresia with a greatly enlarged
294
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
proximal loop patent lateral anastomoses do not function in most casesand the obstruction persists.
Nixon believes that this is due to leaving the blind loop in situ. Byingenious experiments he has shown that the dilated and hypeltrophiedloops do not function adequately at the reduced pressure which followsrelief of the obstruction. Contrariwise Gerrish has shown that the blindloop may safely be left if the end to end anastomosis is protected by theuse of a fine plastic tube enterostomy above it. He places the blame onthe lateral anastomosis but many single successful cases have beenrecorded following its employment and Gross advises it for jejunal atresiaalthough he recommends double barrel enterostomy for ileal atresia.
Technically, lateral anastomosis is the easiest procedure and it is alsoclaimed that it is better because it gives a wider stoma than end to endunion. This claim is invalid because in atresia the anatomical size of thestoma is not important, for its physiological size initially can be no greaterthan the lumen of the contracted bowel distal to it. It is true that thecalibre of the distal bowel will become rapidly normal if there is satis-factory function at the anastomosis. Clawson (1953) has focused attentionon this subject in a paper entitled " Side to Side Anastomosis, a Physio-logically Unsound Procedure." As long ago as 1888, Senn describedlateral ileal anastomosis in dogs in which the upper blind loop containedstagnant faeces, hair and straw. Bayliss and Starling (1899) and Cannonand Murphy (1906) pointed out that division of the circular muscle inlateral anastomosis prevented the satisfactory contraction above and therelaxation below on which the propulsion of the intestinal content depends.In animals end to end anastomoses functioned without stasis while side toside anastomoses did not. Fifty years ago Cannon and Murphy summedup as follows " improvements in modern surgery have made the dangers ofend to end anastomosis so minimal that there is no longer a place for side toside anastomosis.'"
Quite apart from the inefficiency of lateral anastomosis Clawson hasdrawn attention to a later complication by recording the case of a boy,aged four years, who had nine inches of ileum resected for angioma andlateral anastomosis. Ten years later he complained of cramps, tiredness,nausea, distension and attacks of diarrhoea. He failed to gain weight andbecame anaemic. The upper blind loop was dilated and showed micro-scopic evidence of ulceration. Resection of the anastomosis and end toend union was followed by complete cure. The only surprising pointis that it took ten years for the symptoms to arise, for previously Irecorded (Mason Brown, 1952) a similar but more severe syndromefollowing lateral anastomosis after resection of an intussusceptionand since then have had a second case three years after lateral anas-tomosis for the relief of ileal atresia. Both my patients had the symptomsalready mentioned and, in addition, persistent occult blood in the stool
295
J. J. MASON BROWN
and very severe anaemia. Ulceration was present in both the upper andlower blind loops which were distended and so enlarged that it seemedlikely that they had continued to grow with the child. Both were curedby excision of the anastomosis and end to end union.
It might be argued in these cases that the original lateral anastomosishad been life-saving and that the second operation was a small price topay for the lesser risk of a technically easier proceduie. There is ampleevidence that with rare exceptions lateral anastomosis is not effective inileal atresia although it may be successful in duodenal and jejunal atresia.
It seems certain that the difficulty arises because of the failure of theblind loop to function efficiently and for that reason Nixon and Bensonhave advised that it be excised. That the type of anastomosis is lessimportant is emphasised by Benson who performs whichever type ofanastomosis is easiest, following excision of the distended loop. Failureof the distended upper loop to function is not due to any ganglionic defectfor the ganglion cells are found to be normal in cases of atresia (Benson,1955). Barnett and Wall (1955) describe a case of megaduodenum resultingfrom the absence of para-sympathetic ganglion cells in Auerbach's plexus.This is difficult to understand for to be comparable with Hirschsprung'sdisease the defect of the plexus would require to be in the bowel distal tothe enlarged segment.
Why does function foillow vhen the blind loop is not exised in duodenalatresia ? Why has Gross been successful with lateral anastomosis alone injejunal atresia? Why has Gross been able to report such good resultsfollowing double barrel enterostomy in ileal atresia ? The only answer to allthese questions must be that provided there is adequate decompression ofthe upper loop, function will return rapidly in i. Gastric suction might beexpected to give adequate decompression in duodenal and jejunal atresiabut would not do so in ileal lesions and Gerrish has shown that theaddition of even a small tube enterostomy above the anastomosis allowseven the large ileal blind loop to regain its function.Are there any dangers apart from technical ones in adding excision of
the dilated loop to the operative procedure?The possible danger of resecting too much bowel
Potts (1955) states that in the newborn the intestine averages 305 cm.in length and the infant cannot lose more than 38 cm. and survive. Theexperimental work of Kremen, Linner and Nelson (1954) has demon-strated that excision of the upper small bowel is well tolerated but removalof the lower part produces profound nutritional disturbances. Benson(1955) in advocating resection of the upper blind loop, points out thatthe removal of 19 to 42 cm. of ileum causes diarrhoea and slow weight-gain and that 89 cm. (35 inches) of jejunum may be removed in theneonate with survival and without long-term ill effects. These figures
296
SMALL INTESTINE OBSTRUCTION IN THE NEWLY BORN
suggest that it will always be possible to resect the blind loop without thefear of serious nutritional changes.
CONCLUSIONProvided that the upper distended, loop is resected or adequately decom-
pressed, atresia can be relieved by surgical means. Satisfactory surgicaltechniques have been developed but the results of treatment of neonatalobstruction will improve only when:
All babies who vomit bile or vomit persistently are investigatedimmediatelyThe diagnosis is made befbre the 'vitality of the gut is impaired or
post-natal perforation occurs.The surgeon not only relieves the obstruction but also takes adequate
steps to exclude multiple lesions distal to it.The majority of these babies are cared for in units, the staff of which
are trained in the special care of newborn and premature infants.In the post-operative period care must be taken to control the fluid and
electrolyte therapy, the usual tendency being to over rather than undertreat these small baties.
Despite most careful treatment and even with early diagnosis there willalways be a mortality rate in these cases because of multiple intestinalanomalies or congenital defects in other systems but the prognosis insolitary lesions should be a normal expectancy of life.
REFERENCESAIRD, 1. (1939) Edilib. med. J., Trans med.-chir. Soc. Edinb. 46, 174.BARNETT, W. O., and WALL, L. (1955) Anni. Surg. 141, 527.BAYLISS, W. M., and STARLING, E. H. (1899) J. Physiol. 24, 110.BENSON, C. D. (1955) Ann. Surg. 142, 478.BLAND-SUTTON, J. (1889) Amer. J. med. Sci. 98, 457.BROWN, J. J. MASON (1952) Ediaib. med. J., Trans med.-chir. Soc. Edinb. 59, 51.CANNON, W. B., and MURPHY, F. T. (1906) Anns1. Surg. 43, 512.CHISHOLM, T. C., SPENCER, B. J., and WYATT, O. S. (1954) Pediat. Clini. N. Amer. p. 907.CLAWSON, D. K. (1953) Surgerv 34, 254.EHRENPREIS, T., and SANDBLOM, P. (1949) Acta paediat. (Uppsala) 38, 109.EVANS, C. H. (1951) Itit. Abstr. Surg. 92, 1.GERRISH, E. W. (1955) Ani7E. Surg. 142, 469.GLOVER, D. M., and BARRY, F. MCA. (1949) Ann. Surg. 130, 480.GROSS, R. E. (1953) The Surgery of Inifncley and Childhood. Philadephia, Saunders.HIATT, R. B., and WILSON, P. E. (1948) Surg. Gynec. Obstet. 87, 317.KREMEN, A. J., LINNER, J. H., and NELSON, C. H. (1954) Ann. Surg. 140, 139.KREUTER, E. (1909) Arch. clinl. Chir. 88, 303.MADDEN, J. L., and MCCANN, W. J. (1956) Int. Abstr. Surg. 103, 1.NIXON, H. H. (1955) Arch. Dik. Child/I. 30, 13.OLIM, C. B., and CIUTI, A. (1954) Anti. Surg. 140, 736.O'NEILL, J. F., ANDERSON, K., BRADSHAW, H. H., LAWSON, R. B., and HIGHTOWER, F.
(1948) Amer. J. Dis. Child. 75, 214.PACKARD, G. B., and REYNOLDS, L. E. (1951) Ann. Surg. 133, 548.POTTS, W. J. (1947) Surg. Gynec. Obstet. 85, 14.
(1955) J. Amer. Med. Ass. 157, 627.SENN, N. (1888) Ann. Surg. 7, 264.SIMPSON, J. Y. (1838) Edinb. med. surg. J. 15, 390.SWENSON, 0. (1954) Surgery, 36, 192.TANDLER, J. (1900) Morph. Jb. 29, 187.WASCH, M. G., and MARCK, A. (l948) J. Pediat. 32, 479.
297