
HCV/HIV 2013: Management of HCV in patients co-infected with HIV | PowerPoint Presentation

B. J. Dong, PharmD
April 23, 2013IAS–USA
1
Slide 1 of 66
Case 4:Management of the HIV/HCV
Coinfected Patient
IAS–USA
Betty J. Dong, PharmDProfessor of Clinical Pharmacy
University of California San FranciscoSchool of Pharmacy
AU EDITED: 04-19-13
Slide 2 of 66
Learning Objectives
• Identify the advantages of using HCV DAA in the treatment of the HIV/HCV co infected
After attending this presentation, learners will be able to:
in the treatment of the HIV/HCV co-infected patient.
• Describe interactions between ARVs and HCV DAA
• Discuss HCV DAA specific side effects and recommendations for management
Slide 5 of 66
HIV/HCV Co‐Infection• Liver disease is the leading cause of non‐AIDS related death; 66% deaths due to HCV.
• Effects of HIV on HCV infection:
– risk severe liver/cirrhosis (RR 2.07‐2.92), decompensated liver disease (RR 6 14) and HCCdecompensated liver disease (RR 6.14), and HCC
– cirrhosis/fibrosis CD4 < 350 c/mm3 (RR 1.72 ART)
– Associated with 2 fold risk for HCV death
– Potential risk of hepatotoxicity with ART
• Effects of HCV on HIV infection are less clear
JAIDS 2008;47:221; Clin Infect Dis 2008;47:1468; Ann Intern Med 2012;308:370AIDS 2008;22:1979; J Viral Hepat 2010;17:400; EuroSIDA, 13th EACS 2011, abst PS7/3
B. J. Dong, PharmD
April 23, 2013IAS–USA
2
Slide 6 of 66
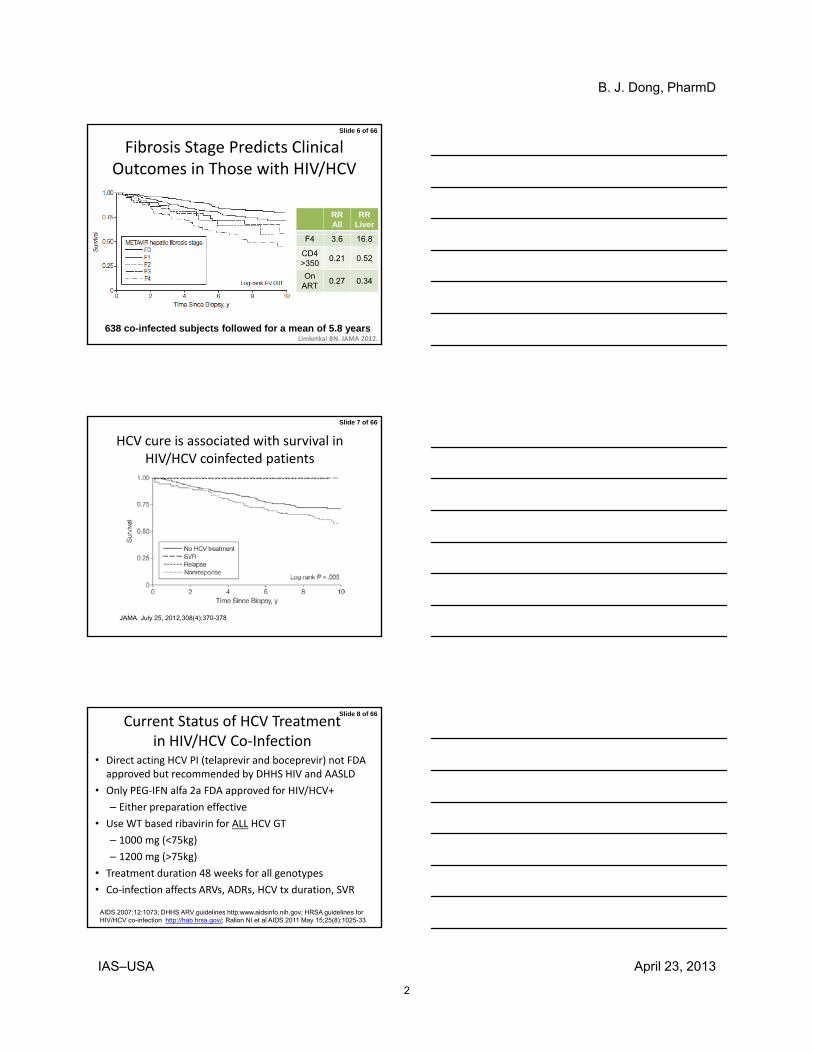
Fibrosis Stage Predicts Clinical Outcomes in Those with HIV/HCV
RRAll
RRLiver
Limketkai BN. JAMA 2012.
F4 3.6 16.8
CD4>350
0.21 0.52
OnART
0.27 0.34
638 co-infected subjects followed for a mean of 5.8 years
Slide 7 of 66
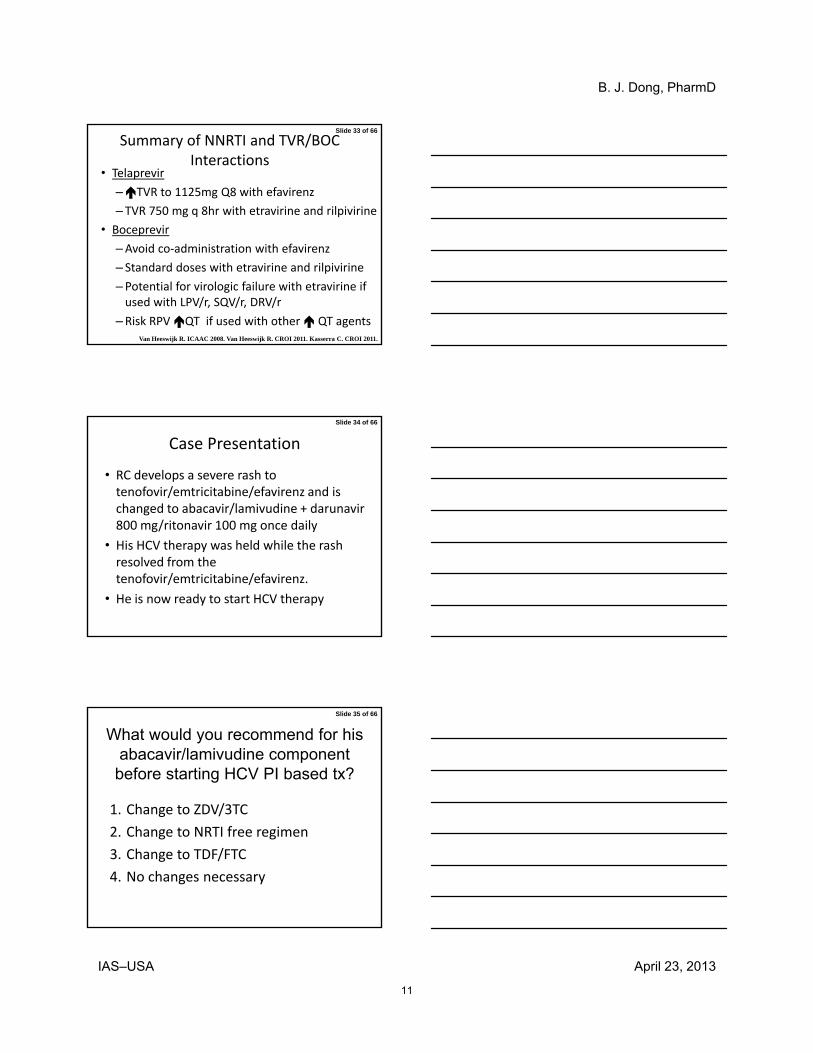
HCV cure is associated with survival in HIV/HCV coinfected patients
JAMA. July 25, 2012,308(4):370-378
Slide 8 of 66
Current Status of HCV Treatment in HIV/HCV Co‐Infection
• Direct acting HCV PI (telaprevir and boceprevir) not FDA approved but recommended by DHHS HIV and AASLD
• Only PEG‐IFN alfa 2a FDA approved for HIV/HCV+
– Either preparation effective
• Use WT based ribavirin for ALL HCV GT
– 1000 mg (<75kg)
– 1200 mg (>75kg)
• Treatment duration 48 weeks for all genotypes
• Co‐infection affects ARVs, ADRs, HCV tx duration, SVR
AIDS 2007;12:1073; DHHS ARV guidelines http:www.aidsinfo.nih.gov; HRSA guidelines for HIV/HCV co-infection http://hab.hrsa.gov/; Rallon NI et al AIDS 2011 May 15;25(8):1025-33.

B. J. Dong, PharmD
April 23, 2013IAS–USA
3
Slide 9 of 66
HCV PI Treatment Concerns During Management of HIV/HCV Co‐infected Patients
• Limited data in co‐infected patients:
– Interim TVR and BOC data presented to date
– Ongoing outcome and drug interaction studies
O l i t i iti f ARV /HCV DAA• Overlapping toxicities of ARVs/HCV DAA
• Drug‐drug interactions b/t ARVs/HCV DAA
• adherence: complex drug regimen, high pill burden, dietary requirements, longer treatment duration
• Potential for drug resistance
Slide 10 of 66
Case Study
• RC is a 58 yr old AA male co‐infected with HIV/HCV on tenofovir/emtricitabine/efavirenz
• PMH: HCV1a, depression, COPD, dyslipidemia, HIV+ d/t hemophilia, HTN, BPH, CKD Stage II
• Habits: + MJ: denies tobacco, EtOH, illicit drug use
All i NKA• Allergies: NKA
• PE: nonictericBP 125/70 P 70 Wt 158 lbs BDI 5/63COR: S1, S2, no extra heart soundslungs: clear A & Pno hepatomegaly/splenomegalyno peripheral edema
Slide 11 of 66
Laboratory Laboratory findings:findings:
•• HCV RNA HCV RNA 2 mu 2 mu IU/mLIU/mL•• AST/ALT 158/161AST/ALT 158/161•• TbilTbil 1.21.2•• Albumin 4.0Albumin 4.0
•• WBC 5.0, ANC 5.0WBC 5.0, ANC 5.0•• HgbHgb/HCT=15/45gm/HCT=15/45gm•• MCV 98 MCV 98 •• Platelet 350KPlatelet 350K
•• INR 1.2INR 1.2•• Liver U/S: no discrete Liver U/S: no discrete lesions, +corkscrewing lesions, +corkscrewing c/w cirrhosisc/w cirrhosis
•• HepHep A and B immuneA and B immune
•• BUN/BUN/SCrSCr 20/20/ScrScr 1.81.8•• CrCLCrCL: 50cc/min: 50cc/min•• CD4 390 cells/mm3CD4 390 cells/mm3•• HIV RNA 100K c/mlHIV RNA 100K c/ml•• HIV GT: no mutationsHIV GT: no mutations

B. J. Dong, PharmD
April 23, 2013IAS–USA
4
Slide 12 of 66
What would you treat first, HIV or HCV?
1.HIV
2.HCV
3.Does not matter
4.Don’t know
Slide 13 of 66
HIV or HCV Treatment First?
• Timing of the initiation of HCV and ART
–ART first to CD4 count (CD4 with HCV tx) and achieve undetectable HIV VL
–ART X 6‐12 mo if CD4 <200 cells/mm3:
– SVR if CD4 > 350
– HIV RNA by ART may also HCV RNA and SVR
Slide 14 of 66
What would you tell RC about the SVR reported with a HCV DAA/PEGIFN/RBV
regimen for a patient such as him
1. 35‐45%
2 46 55%2. 46‐55%
3. 56‐64%
4. 65‐80%
5. 81‐90%

B. J. Dong, PharmD
April 23, 2013IAS–USA
5
Slide 15 of 66
Efficacy of PegIFN + RBV in HCV/HIV‐Coinfected Patients
44-49.6
(%)
All patients
GT1 HIV/HCV co-infected patients
60
100
80
1.Torriani F, et al. N Engl J Med. 2004;351:438-450. (Apricot) 2. Chung R, et al. N Engl J Med. 2004;351:451-459.(ACTG) 3. Carrat F, et al. JAMA. 2004;292:2839-2848. (RIBAVIC) 4. Laguno M, et al.AIDS. 2004;18:F27-F36 (BARCELONA). Nunez M et al. AIDS Hum Res Retroviruses 2007;23:972-(PRESCO)
PegIFN alfa-2a +RBV 800[1]
PegIFN alfa-2a +RBV 600-1000[2]
PegIFN alfa-2b + RBV 800[3]
Peg IFN alfa-2b +Wt based RBV 800-1200[4-5]
40
29 27
14
27
17
38-35SV
R
0
20
40
Slide 16 of 66
Telaprevir/PR for Treatment Naïve HCV GT 1 HIV negative and positive patients (SVR12)
75 74
44 45
60
80
0
20
40
HIV negative HIV positive
HCV PI + PR
PR48
.Sulkowski et al JID 2013;207 (S1):S26; Jacobson et al. New Eng J Med 2011
Slide 17 of 66
Boceprevir/PR for Treatment Naïve HCV GT1 HIV negative and positive patients (SVR 12)
6662
60
80
38
29
0
20
40
HIV negative HIV positive
HCV PI + PR
PR48
.Sulkowski et al JID 2013;207 (S1):S26; Poordad et al. New Eng J Med 2011

B. J. Dong, PharmD
April 23, 2013IAS–USA
6
Slide 18 of 66
On treatment responses to TVR based HCV treatment similar in HIV/HCV co‐infected and HCV mono‐infected
• N=33 co‐infected and 117 mono‐infected
• Median CD4 489, 81% (25/310 HIV VL<LLQ/D)
• Undetectable HCV VL (co‐infected vs. mono‐infx)
– Wk 4 42.4% vs. 43.6% (p=1.00)
– Wk 12 72.7% vs 65.8% (p=0.532)
– Wk 24 72.7% vs 58.1% (p=0.16)
– EOT 63.6% vs 51.2% (p=0.24)
Martel-Laferriere et al. CROI 2013, abst 679
Slide 19 of 66
ANRS: TVR/IFN/RBV in HIV/HCV Co‐infection with Prior PR Failures (n=69)
%
80%
100%
Overall
Fibrosis 3‐ 4
Null Responders with Cirrhosis Excluded
Cotte, et al. CROI 2013, Abstract 36;
0%
20%
40%
60%
EVR16
prior null
partial
Relapse
Breakthrough
TDF/FTC +ATV/r 49%EFV 19%RAL 17%
Slide 20 of 66
ANRS: BOC/IFN/RBV in HIV/HCV Co‐infection with Prior PR Failures (n=64)
• Null responders with cirrhosis excluded• PR failures: relapse 31.3%; breakthrough 7.8%; partial response 28.1%, null response 32.8%
• TDF or ABC + FTC/3TC + ATV/r or RAL
Poizot-Martin, et al. CROI 2013, Abst 37
0
20
40
60
80
100
EVR 16 (%)
6373
38
53
70
All
F4 (N=11)
Prior null resp (N=21)
ATV/r
RAL

B. J. Dong, PharmD
April 23, 2013IAS–USA
7
Slide 21 of 66
Which HCV DAA is Associated with Higher SVR for HIV/HCV Co‐infected Patients?
1. Telaprevir
2. Boceprevir
3. Both are reported to be equivalent
4. No head to head comparison data to determine this
Slide 22 of 66
Telaprevir Outperformed Boceprevir in Retrospective Analysis
• No head‐to‐head trials of TVR vs BOC
• Retrospective analysis of all treated patients at 3 clinics, n = 106
TVR i t d ith hi h RVR BOC• TVR associated with higher RVR vs. BOC
– Irrespective of HIV status
• Reduced BOC response particularly in patients with prior IFN experience and GT1a
Benito, et al Abstract 676, CROI 2013
Slide 23 of 66
Triple Combination TVR HCV Therapy Exhibits Higher Early Antiviral Potency than
with BOC Regardless HIV Status
• N=274 (68 BOC, 206 TVR) international sites– 29% vs 23% IL28B CC
– 95% advanced liver cirrhosis vs 66% (p< 0.001)
– HIV co‐infection (12 vs 18%)
• Results: RVR 84% TVR vs 60% BOC– TVR strongest predictor RVR (OR 5.3) p < 0.0001
– Baseline HCV RNA 0.44 p=0.03
– GT 1b OR 2.3 (p=0.05)
– No effect from HIV infection
Benito JM et al CROI 2013, Abst 676

B. J. Dong, PharmD
April 23, 2013IAS–USA
8
Slide 24 of 66
In our HIV+ pt receiving efavirenz/TDF/FTC, which telaprevir
dose would you recommend?
1. 750 mg q 8hr
2. 750 mg q 12hr
3. 1125 mg q 12hr
4. 1125 mg q 8hr
5. 1500 mg q 8hr
Slide 25 of 66
Telaprevir and EFV
1000
2000
3000
4000
TVR 750 mg q8h (n=20, reference)
TVR 1500 mg q12h + E/T (n=16)TVR 1125 mg q8h
+ E/T (n=15)
TV
R c
once
ntra
tion
(ng/
mL)
TVR doseEffect of EFV/TDF on TVR
Cmin Cmax AUC8h
750 mg q8h 0.53 0.80
1125 mg q8h 0.75 (0.66–0.86) 0.86 (0.76–0.97) 0.82 (0.73–0.92)
1500 mg q12h 0.52 (0.42–0.64) 0.97 (0.88–1.06) 0.80 (0.73–0.88)*
Van Heeswijk R. ICAAC 2008. Van Heeswijk R. CROI 2011.
0
0 2 4 6 8 10 12
+ E/T (n=15)
Time (hours)
*Average steady state plasma concentration (Cssaverage)
Slide 26 of 66
Effect of Nonnucleosides on Telaprevir (TVR) Pharmacokinetics
% Change in TVR PK TVR Cmin
TVR Cmax
TVR AUC*
ff f
• TVR to 1125 mg q 8hr minimized efavirenz intx• No significant changes in TVR PK with ETR or RPV
CROI 2011, Abst 119; CROI 2011 Abst 629;
Effect of ART on Telaprevir 750 mg tid exposures
EFV with 1125 mg q 8hr TVR ‐25 ‐14 ‐18
EFV 600 mg daily ‐47 ‐9 ‐26
ETR 200 mg bid ‐25 ‐10 ‐16
RPV 25 mg daily ‐13 ‐5 ‐8
Kakuda TN et al Abstr O-18; Barcelona 2012

B. J. Dong, PharmD
April 23, 2013IAS–USA
9
Slide 27 of 66
Effect of Telaprevir (TVR) on NNRTI Levels
% Change in NNRTI PK Parameter
NNRTI Cmin
NNRTI Cmax
NNRTI AUC*
Eff t f T l i 750 8h
• No significant reduction in ETR levels • RPV levels (risk QTc prolongation?)
Van Heeswijk R et al, CROI 2011, Abst 119; Garg V et al, CROI 2011 Abst 629;
Effect of Telaprevir 750 mg q8hr on NNRTI exposuresEFV ‐2 ‐16 ‐7
EFV with 1125 mg Q 8hr TVR ‐10 ‐24 ‐18
ETR 200 mg bid ‐3 ‐7 ‐6
RPV 25 mg daily +93 +49 +78
Kakuda TN et al Abstract O-18; Barcelona, Spain 2012
Slide 28 of 66Telaprevir (TVR) Administration (TVR) and Missed Dosages
• TVR: 375 mg tablets: total 6 tabs/day
– 750 mg Q 8 hr (2 tabs/dose q 8hr)
– 1125 mg (3 tabs/dose) bid
• (OPTIMIZE): comparable SVR12 73% (q 8r) vs 74% (q 12 hr)
– 1125 mg q 8hr with efavirenz
– Within 20‐30 minutes of 20 gm fat meal
– What to do about missed doses
• If miss within 4 hr of missed dose, take ASAP w/ food.
• If > 4 hrs, do not take missed dose, resume dosing
Slide 29 of 66
OPTIMIZE: BID Dosing Noninferior to TID Dosing of TVR in Tx‐Naive GT1
Patients
73 7478 81
59 58
TVR q8hr + pegIFN/RBVTVR BID + pegIFN/RBV
2 (
%)
100
80
60
• Adverse events similar between treatment arms
Buti M, et al. AASLD 2012. Abstract LB-8.
270/371
274/369
209/268
213/264
61/103
61/105
n/N =
Bridging Fibrosisor Cirrhosis
No, Minimal, orPortal Fibrosis
Overall
SV
R1
2
40
20
0

B. J. Dong, PharmD
April 23, 2013IAS–USA
10
Slide 30 of 66
In our HIV+ pt receiving efavirenz/TDF/FTC, what happens if boceprevir is used instead?
1. Better choice since no interaction
2. EFV toxicity d/t EFV levels
3. BOC failure d/t BOC levels
4. Risk of both EFV and BOC failure
5. Unclear, since data not available
Slide 31 of 66Boceprevir (BOC) and NNRTIs• Avoid with EFV; Cmin BOC
• Can co‐administer with ETR and RPV.
• Monitor for RPV induced QT
% Change in BOC PK Cmax AUC Cmin
Efavirenz ‐8 ‐19 ‐44
Rilpivirine ‐2 ‐6 +4
Hammond KP et al. J Acquir Immumn Defic Syndro 2013; 62:67-73; Kasserra C, et al. CROI 2011. Abstr 118.
p
Etravirine +10 +10 ‐12
Effect of boceprevir on NNRTI exposure
Tenofovir +32 +5 No data
Efavirenz +11 +20 No data
Etravirine 200 mg bid ‐24 ‐23 ‐29
Rilpivirine 25 mg daily +15 +39 +51
Slide 32 of 66
Pharmacokinetic Interaction Between Boceprevir and Etravirine in HIV/HCV SeronegativeVolunteers.Hammond, Kyle;
lf lWolfe, Pamela; Burton, James; Predhomme, Julie; RN, MS; Ellis, Christine; Ray, Michelle; Bushman, Lane; Kiser, JenniferJAIDS 62(1):67‐73, January 1, 2013.
B. J. Dong, PharmD
April 23, 2013IAS–USA
11
Slide 33 of 66
Summary of NNRTI and TVR/BOC Interactions
• Telaprevir
–TVR to 1125mg Q8 with efavirenz
– TVR 750 mg q 8hr with etravirine and rilpivirine
• Boceprevirp
–Avoid co‐administration with efavirenz
– Standard doses with etravirine and rilpivirine
–Potential for virologic failure with etravirine if used with LPV/r, SQV/r, DRV/r
–Risk RPV QT if used with other QT agentsVan Heeswijk R. ICAAC 2008. Van Heeswijk R. CROI 2011. Kasserra C. CROI 2011.
Slide 34 of 66
Case Presentation
• RC develops a severe rash to tenofovir/emtricitabine/efavirenz and is changed to abacavir/lamivudine + darunavir 800 mg/ritonavir 100 mg once daily800 mg/ritonavir 100 mg once daily
• His HCV therapy was held while the rash resolved from the tenofovir/emtricitabine/efavirenz.
• He is now ready to start HCV therapy
Slide 35 of 66
What would you recommend for his abacavir/lamivudine component
before starting HCV PI based tx?
1. Change to ZDV/3TC
2. Change to NRTI free regimen
3. Change to TDF/FTC
4. No changes necessary

B. J. Dong, PharmD
April 23, 2013IAS–USA
12
Slide 36 of 66
Abacavir Reducing Efficacy of HCV Treatment
• Inhibitory competition b/t ABC and RBV (guanosine analogues)
Retrospective Abacavir Non‐ABC P‐values
SVR rates SVR rates
n=256 29% 45% 0.02
• Conclusions:
– Retrospective analysis of small data sets
– ABC did not SVR w/ wt‐based RBV
– ABC appropriate to use if benefits > risks
Antivir Ther. 2008;13(3):429-37, J Antimicrob Chemother 2008;62:1365.;
RBV >13.2 mg/kg/day 31% 38% 0.4
RBV<13.2 mg/kg/day 20% 52% 0.03
n=244 46.2% 46.7% <0.05
Slide 37 of 66
Adriana A et al CROI 2013, abstr 538
Conclusions:• ABC did not alter RBV or
RBV=TP concentrations.• ABC can be co-
administered safely to HIV/HCV co-infected pts
Slide 38 of 66
What would you recommend for the ritonavir boosted darunavir component
before starting a telaprevir based treatment
1. Increase DRV/r to 600/100 mg BID.
2 Ch DRV/ t RAL 800 d il2. Change DRV/r to RAL 800 mg daily.
3. Change DRV/r to ATV/r
4. Stop all ART during the HCV PI treatment.
5. Continue his once daily DRV/r.

B. J. Dong, PharmD
April 23, 2013IAS–USA
13
Slide 39 of 66Effects of HIV Protease Inhibitors on Telaprevir (TVR) Pharmacokinetics
%Change in TVR PK Parameter TVR Cmin
TVR Cmax
TVR AUC*
• Atazanavir/r had minimal effect on TVR PK• Avoid co-administration w/ other HIV PI: TVR levels
CROI 2011, Abst 119; CROI 2011 Abst 629;
ATV/RTV ‐15 ‐21 ‐20
DRV/RTV ‐32 ‐36 ‐35
FPV/RTV ‐30 ‐33 ‐32
LPV/RTV ‐52 ‐53 ‐54
RTV 100 mg bid ‐32 ‐15 ‐24
Kakuda TN et al Abstract O-18; Barcelona 2012
Slide 40 of 66
Mean TVR PK Profiles
TVR alone
n=14 n=17 n=16 n=20
3000
on
(n
g/m
L)
LPV ATV DRV fAPV
0 2 4 6 8 0 2 4 6 8
van Heeswijk R. CROI 2011.AUC = area under the curve
AUC 54% AUC 20% AUC 32%AUC 35%
TVR + ARV
n=12 n=14 n=11 n=18
Time (hours)
0
1000
2000
TV
R c
on
cen
trat
i
0 2 4 6 8 0 2 4 6 8
42% 15%
32% 30%
Slide 41 of 66
Effect of Telaprevir (TVR) on HIV PI
%Change in ARV PKParameters
ARV Cmin
ARV Cmax
ARV AUC*
•ATV/r w/ potential for bilirubin• DRV/r, FPV/r, LPV/r: avoid co-administration
Van Heeswijk R et al, CROI 2011, Abst 119; Garg V et al, CROI 2011 Abst 629;
ATV/RTV +85 ‐15 +17
DRV/RTV ‐42 ‐40 ‐40
FPV/RTV ‐56 ‐35 ‐47
LPV/RTV +14 ‐4 +6
Kakuda TN et al Abstract O-18; Barcelona, Spain 2012

B. J. Dong, PharmD
April 23, 2013IAS–USA
14
Slide 42 of 66
Impact of telaprevir on HIV PIsLPV/r ATV/r
AUC AUC 17%
n=19
n=11
n=12 n=7
4000
8000
12000
LP
V c
on
cen
tra
tio
n (
ng
/mL
)
AT
V c
on
cen
trat
ion
(n
g/m
L)
4000
3000
2000
1000
PI alonePI + TVR
PI alonePI + TVR
82%14%
van Heeswijk R. CROI 2011.
0 2 4 6 8 10 12 0 2 4 6 8 10 12
DRV/r fAPV/r
AUC 47%AUC 40%
n=20n=16
n=11n=18
Time (hours)
00 2 4 6 8 10 12 0 6 12 18 24
Time (hours)
0
Time (hours)
DR
V c
on
cen
tra
tio
n (
ng
/mL
)
6000
4000
2000
0
AP
V c
on
cen
tra
tio
n (
ng
/mL
)
Time (hours)
4000
3000
2000
1000
0
PI alonePI + TVR
PI alonePI + TVR
42% 56%
Slide 43 of 66
Effects of Raltegravir on Telaprevir PK
RAL AUC 31% and Cmin 78%
van Heeswijk et al., ICAAC, Chicago, Sept. 17-20, 2011
Slide 44 of 66Drug‐Drug Interactions: Boceprevir (BOC) and HIV PIs
• HIV protease inhibitors: avoid co‐administration% Change in BOC PK BOC Cmax BOC AUC BOC Cmin
Atazanavir/r ‐7 ‐5 ‐18
Darunavir/r ‐25 ‐32 ‐35
L i i / 50 45 57
Hammond KP et al. J Acquir Immun Defic Syndro 2013; 62:67-73; Hulskotte EGJ et al CID 2013;56:718-26
Lopinavir/r ‐50 ‐45 ‐57
% Change in ARV PK ARV Cmax ARV AUC ARV Cmin
Atazanavir/ritonavir ‐36 ‐44 ‐59
RTV100 mg daily ‐27 ‐36 ‐45
Darunavir/ritonavir ‐36 ‐44 ‐59
RTV 100 mg BID ‐13 ‐27 ‐45
Lopinavir/ritonavir ‐30 ‐34 ‐43
B. J. Dong, PharmD
April 23, 2013IAS–USA
15
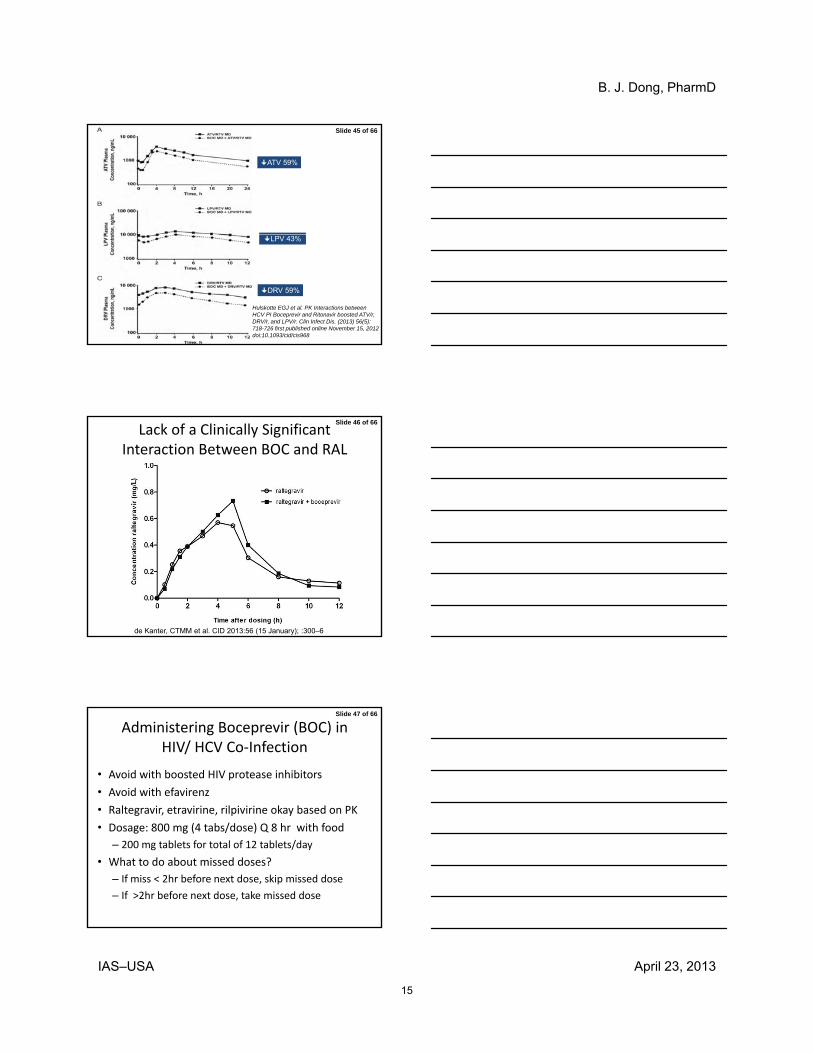
Slide 45 of 66
ATV 59%
Hulskotte EGJ et al. PK Interactions between HCV PI Boceprevir and Ritonavir boosted ATV/r, DRV/r, and LPV/r. Clin Infect Dis. (2013) 56(5): 718-726 first published online November 15, 2012 doi:10.1093/cid/cis968
LPV 43%
DRV 59%
Slide 46 of 66
Lack of a Clinically Significant Interaction Between BOC and RAL
de Kanter, CTMM et al. CID 2013:56 (15 January); :300–6
Slide 47 of 66
Administering Boceprevir (BOC) in HIV/ HCV Co‐Infection
• Avoid with boosted HIV protease inhibitors
• Avoid with efavirenz
• Raltegravir, etravirine, rilpivirine okay based on PK
• Dosage: 800 mg (4 tabs/dose) Q 8 hr with food
– 200 mg tablets for total of 12 tablets/day
• What to do about missed doses?
– If miss < 2hr before next dose, skip missed dose
– If >2hr before next dose, take missed dose

B. J. Dong, PharmD
April 23, 2013IAS–USA
16
Slide 48 of 66
Side Effects to HCV Direct Acting Agents: Telaprevir and Boceprevir in HIV/HCV Co‐infected Persons/ o ec ed e so s
Slide 49 of 66
Which might be most problematic in our patient taking abacavir/lamivudine +
atazanavir/r plus telaprevir/PEGIFN/ribavirin?
1. Dysgeusia
2 A t l t2. Anorectal symptoms
3. Renal failure
4. Neutropenia
5. Hypersensitivity reaction
Slide 50 of 66
TVR based HCV treatment ADRs in HIV/HCV co‐infected and HCV
mono‐infected Patients
• ADR: co‐infected mono‐infected
– Stopped 18.2% 13.7% (p=0.58)
– Severe anemia 33.3% 37.6% (p=0.69)
– Rash 15.2% 34.1% (p=0.05)
– Rectal sx 12.1% 43.6% (p=0.001)
Martel-Laferriere V, Brinkley S, Bichoupan K, Posner S, Stivalas A, Perumalswami P, Schiano T, Sulkowski M, Dieterich D, Branch A . CROI 2013, abst 679

B. J. Dong, PharmD
April 23, 2013IAS–USA
17
Slide 51 of 66
In our patient taking TVR, PEG‐IFN/RBV, what would you do for an itchy maculo‐
papular rash involving both arms
1. Start oral steroids
2. Start topical steroids
3. Stop telaprevir only
4. Stop PEG and RBV
5. Stop PEG/RBV/TVR
Slide 52 of 66
Telaprevir and Cutaneous ReactionsCutaneous
Reactions
Phase 2 Studies
(PROVE‐1,2,3)
Phase 3 Studies
(Illuminate/Advance/Realize)
Rash and/or pruritus 47‐59% 51‐60% (56%)
Grade 3 skin (severe) 4‐7% 4‐5%
Onset (days) 7‐28 16‐20
Discontinuation Rate 5‐7% 6‐6.5%
• Mechanism unclear
• Antihistamines, topical steroids for symptomatic relief
• Systemic steroids not recommended
• Close monitoring for rash progression/systemic reactions → D/C
• If no improvement within 7 days of stopping TVR, stop PEG-IFN/RBV
Dermatology 2010; 221: 303-5; NEJM 2010;362:1292; Gastro 2010;139:1412
Slide 53 of 66
Telaprevir‐Associated Rash
FDA Antiviral Drugs Advisory Committee Meeting, May 2011.
STOPTelaprevir
MonitorClosely

B. J. Dong, PharmD
April 23, 2013IAS–USA
18
Slide 54 of 66
Pre‐Treatment Considerations for Telaprevir‐Associated Rash and Rectal
Symptoms • Good skin hygiene
– Emollient creams and lipid‐rich lotions
– Sunscreen avoid prolonged sun exposureSunscreen, avoid prolonged sun exposure
– Avoid hot showers and drying soaps (eg. Ivory)
• Anal itching
– Enough fat with TVR
– Sitz bath
– Tucks1. Telaprevir [package insert]. October 2012. 2. Cacoub P, et al. J Heptol. 2012;56:455-463.
Slide 55 of 66
Case Discussion
• A 32‐year‐old Ukranian female with genotype 1b HCV infection and cirrhosis (corkscrew) on ultrasounds comes for F/U after starting peginterferon alfa‐2a and ribavirin 1000 mg/day with boceprevir 800ribavirin 1000 mg/day, with boceprevir 800 mg 3 times daily after a 4‐week lead‐in.
• After one week of boceprevir, ANC is 670 cells/mm3 with no signs of infection. Platelets are down to 118K from her baseline of 250K.
Slide 56 of 66
What would you do at this time?
1. Start eltrombopag to increase her platelet count
2. Start filgrastim to reduce risk of infection
3 Start eltrombopag and filgrastim immediately3. Start eltrombopag and filgrastim immediately
4. Start prophylactic antibiotics to prevent infection
5. Reduce PEGIFN dose to 135 mcg/week and start filgrastim
6. Do nothing

B. J. Dong, PharmD
April 23, 2013IAS–USA
19
Slide 57 of 66
Eltrombopag
• FDA approved in Nov 2012 for thrombocytopenia in HCV to allow the initiation and maintenance of IFN
• Risks: hepatotoxicity, hepatic decompensation, thrombotic/ thromboembolic events
• Should not be used to normalize platelet counts; not thoroughly evaluated for safety or efficacy with protease inhibitor–based HCV therapy
• Consider if plt <20‐30K
• Must not be taken within 4 hours of any medications or products containing polyvalent cations such as antacids, dairy products, and mineral supplements
Slide 58 of 66
ENABLE 1: Eltrombopag as Adjunct Therapy for Thrombocytopenia in HCV
• Regimen: pegIFN/RBV
• In patients with baseline platelets < 75,000/mm3, 95% were eligible to start antiviral therapy with pegIFN following open‐label eltrombopag
• Eltrombopag: significantly improved response rates to HCV p g g y p ptherapy
Afdhal N, et al. AASLD 2011. Abstract LB-3.
100
80
60
40
20
0
Pat
ien
ts (
%)
RVR
17
Virologic Response (ITT)PlaceboEltrombopag
EVR cEVR ETR SVR
16
50
66
26
4237
48
14
23
P = .0064
P = .008P < .0001
P < .0001
P = .7495
Slide 59 of 66
Crystal Ball into
What Does the Future Hold?

B. J. Dong, PharmD
April 23, 2013IAS–USA
20
Slide 60 of 66
SVR12 in HIV/HCV Coinfection Treated with Simeprevir/IFN/RBV
40%
60%
80%
100%
77% 75% 80%
All
Naïve
Relapse10/13
RGT patients ONLYDoes not include cirrhotics/nulls(64% of nulls still
0%
20%
SVR 12
Relapse
Dieterich, et al. CROI 2013, Abstr154LB
(Excludes cirrhotics)
10/13 6/84/5
5% hyperbilirubinemia27% neutropenia21% anemia
responding at wk 24)
Slide 61 of 66
Faldaprevir/IFN/RBV in HIV/HCV Coinfection: EVR
80%
100%
60%
74%
82%
91% 78% naïve22% relapseF4 4%96% on ART
Dieterich, et al. CROI 2013; Abstr 40LB; Sabo Abst 35
0%
20%
40%
60%
Naïve (n=239) Relapser (n=69)
WEEK 4
WEEK 12
Slide 62 of 66
Faldaprevir Drug Interactions
• DRv/r 800/100 mg
– FDV AUC 129% and Cmin 283%
– No clinically relevant interaction on DRV/r levels
– FDV 120 mg daily with DRV/r
Ef i• Efavirenz
– FDV AUC 35% and Cmin 46%
– FDV 240 mg bid being with EFV
– No significant effects on EFV
• TDF
– FDV AUC 22% and Cmin 25%
Sabo Abst 35 CROI 2013

B. J. Dong, PharmD
April 23, 2013IAS–USA
21
Slide 63 of 66
Conclusions
• Treatments for HIV/HCV patients are evolving
• HCV DAA data suggest SVR in HIV/HCV similar to mono‐infected
• Interferon free agents under investigation but• Interferon free agents under investigation but several years before approval in HIV/HCV co‐infected
• Be mindful of HCV/HIV drug‐drug interactions and overlapping toxicities
Slide 66 of 66
Acknowledgements
Special thanks for slides:
Jennifer Kiser, PharmD, U ColoradoCharles Flexner, MD, Johns HopkinsChip Schooley, MD, Univ San Diego
![Mattias MANDORFER, M.D.1,3...been investigated in the TURQUOISE-1 study [18] in HIV/HCV-GT 1-coinfected patients, including 10% of patients with cirrhosis. Patients were randomized](https://static.fdocuments.net/doc/165x107/5f893c4d49f0f976bc6ff99f/mattias-mandorfer-md13-been-investigated-in-the-turquoise-1-study-18-in.jpg)












![Elizabeth Sherman, PharmD, AAHIVPhivaidsinstitute.med.miami.edu/documents/...HIV-HCV...• SVR rates similar to HCV monoinfected [1,2] • In HCV/HIV coinfection, treat HCV as though](https://static.fdocuments.net/doc/165x107/5fbc30e57653e03e261e9924/elizabeth-sherman-pharmd-aa-a-svr-rates-similar-to-hcv-monoinfected-12.jpg)

