
Slide 1 Doxil ® (doxorubicin HCl liposome injection) Doxil in the Treatment of Advanced, Metastatic...
69
Slide 1 Doxil ® (doxorubicin HCl liposome injection) Doxil in the Treatment of Advanced, Metastatic Ovarian Cancer Oncologic Drugs Advisory Committee Meeting June 8, 1999
-
date post
21-Dec-2015 -
Category
Documents
-
view
228 -
download
3
Transcript of Slide 1 Doxil ® (doxorubicin HCl liposome injection) Doxil in the Treatment of Advanced, Metastatic...

Slide 1
Doxil®
(doxorubicin HCl liposome injection)
Doxil in the Treatment of Advanced, Metastatic Ovarian Cancer
Oncologic Drugs Advisory Committee MeetingJune 8, 1999

Slide 2
Proposed New Indication
Doxil (doxorubicin HCl liposomal injection) is indicated for:
The treatment of patients with metastatic carcinoma of the ovary who are refractory to both paclitaxel- and platinum-based chemotherapy regimens and who may also be refractory to topotecan. Refractory is defined as a patient having progressive disease while on treatment, or within 6 months of treatment.

Slide 3
Agenda
Unmet Medical Need: Maurie Markman, MD, DirectorCleveland Clinic Taussig
Cancer Center
STEALTH® Technology Frank Martin, PhD,and Doxil Pharmacology: Principal Scientist
Efficacy of Doxil: Ed Schnipper, MD, VP, Clinical Research
Safety of Doxil: Ken Cunningham, MD, VP, European Clinical
Research
Risk/Benefit: Ed Schnipper, MD, VP, Clinical Research

Slide 4
Experts Available for Questions
ConsultantsAlan Gordon, MD, Sammons Cancer Center, DallasWilliam McGuire, MD, University of MississippiFranco Muggia, MD, NYU Medical Center
Sponsor RepresentativesMartin O’Connell, PhD, Sr Dir, BiostatisticsRandy Allred, Dr PH, Dir, BiostatisticsPeter Working, PhD, VP, Nonclinical ResearchTim Sharpington, Assoc Dir, Clinical ResearchTom Tarlow, Director, Regulatory Affairs
Slide 5
Agenda
Unmet Medical Need: Maurie Markman, MD, Cleveland Clinic Taussig
Cancer Center

Slide 6
Overview of Ovarian Cancer
• 25,200 patients diagnosed in US in 1999• 14,500 deaths• 70% present with advanced disease
– Standard treatment is with platinum and paclitaxel
• Despite improvements with combination therapy– >20% fail to respond to first-line chemotherapy– 80% ultimately relapse

Slide 7
Patient Population Definitions for“second line therapy”
• Sensitive patients (those who have a durable response >6 months) likely to respond to retreatment
• Refractory patients (those who progressed while on or within 6 months of treatment) unlikely to respond
to retreatment

Slide 8
Chemotherapy Agents Approved for Second Line Treatment in Ovarian Cancer
• Paclitaxel (Taxol)• Altretamine (Hexalen)• Topotecan (Hycamtin)

Slide 9
Response Rates of Approved Agents in Second Line Treatment
Platinum/Platinum/ Platinum/ Paclitaxel/
Paclitaxel Topotecan Topotecan Agent Failure* Failure* Refractory
Topotecan 9.4% - -
Paclitaxel - 2.7% -
Altretamine - - -
* Does not necessarily meet strict definition of refractory

Slide 10
Factors Affecting Response
• Patients are less likely to respond if they:– Progress while receiving platinum therapy– Progress after receiving multiple regimens

Slide 11
Patients with Ovarian Cancer
• Relapse common• Long survival• Good Performance Status

Slide 12
Medical Need
• Need for options and alternative treatments for patients who experienced toxicity on prior therapy:– Neurotoxicity– Bone marrow toxicity– Nausea/Vomiting

Slide 13
Quality of Life
• Patients treated for long periods• Need for agents which are well tolerated and
convenient for patients

Slide 14
Agenda
Unmet Medical Need: Maurie Markman, MD, Cleveland Clinic Taussig
Cancer Center
STEALTH® Technology Frank Martin, PhD,and Doxil Pharmacology: Principal Scientist

Structure of Doxil
DoxorubicinDoxorubicin
Lipid Membrane Lipid Membrane (Phospholipid +(Phospholipid +
Cholesterol)Cholesterol)
Polyethylene Polyethylene GlycolGlycol
85-100 nm85-100 nm
Slide 16
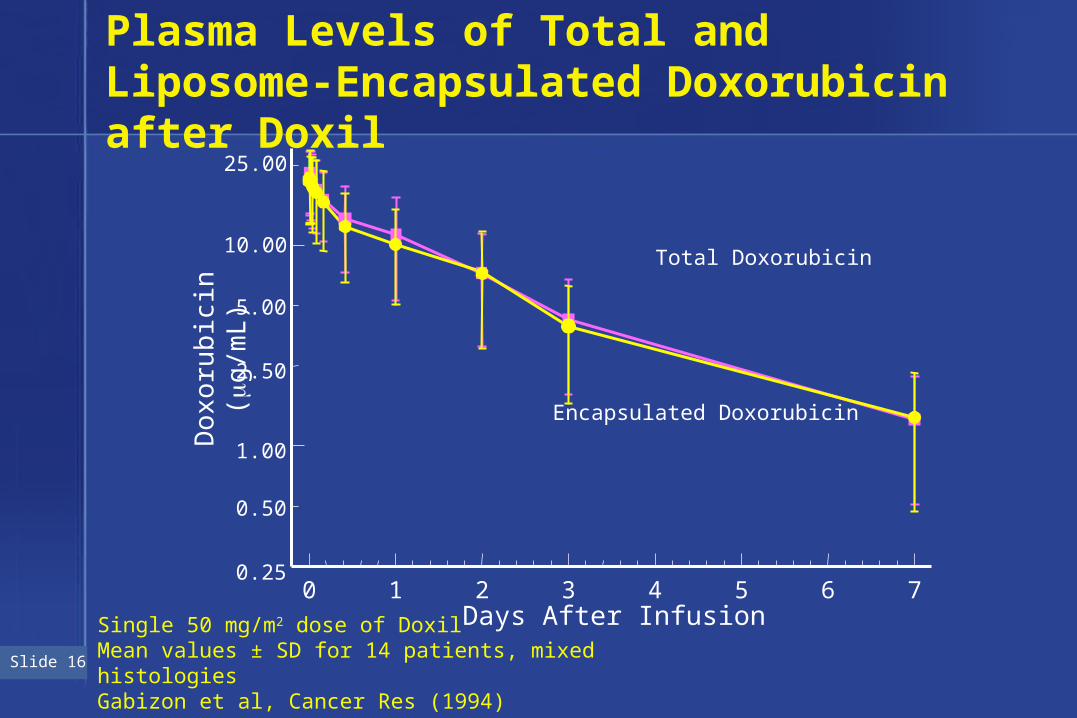
Plasma Levels of Total and Liposome-Encapsulated Doxorubicin after Doxil
Days After Infusion0 1 2 3 4 5 6 7
0.25
0.50
2.50
5.00
25.00
1.00
10.00Total Doxorubicin
Encapsulated Doxorubicin
Do
xoru
bic
in (g
/mL
)
Single 50 mg/m2 dose of DoxilMean values ± SD for 14 patients, mixed histologiesGabizon et al, Cancer Res (1994)

Slide 17
Doxorubicin Levels in Prostate Carcinoma Xenograft
Vaage J, et al. Cancer, 1994
µg
Dru
g/gm
Tum
or
Hours100 150 20050
Doxil
Adriamycin
4
6
8
2
0
Doxil AUC = 919
Adriamycin AUC = 36.5
Slide 18
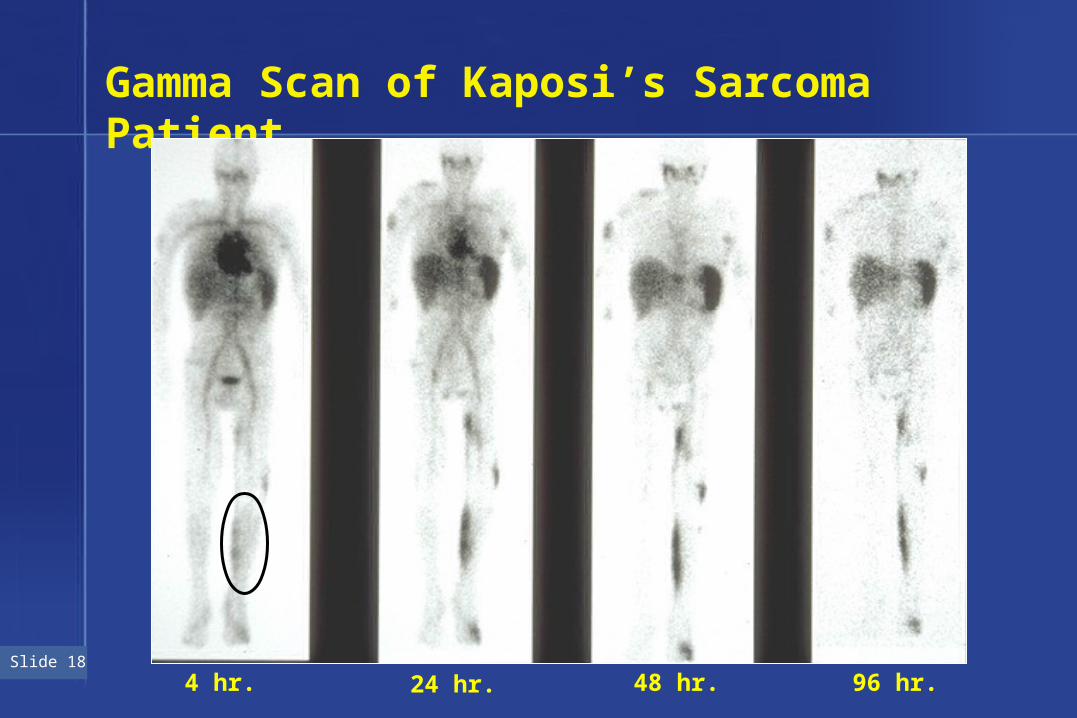
Gamma Scan of Kaposi’s Sarcoma Patient
4 hr. 24 hr. 48 hr. 96 hr.
Slide 19
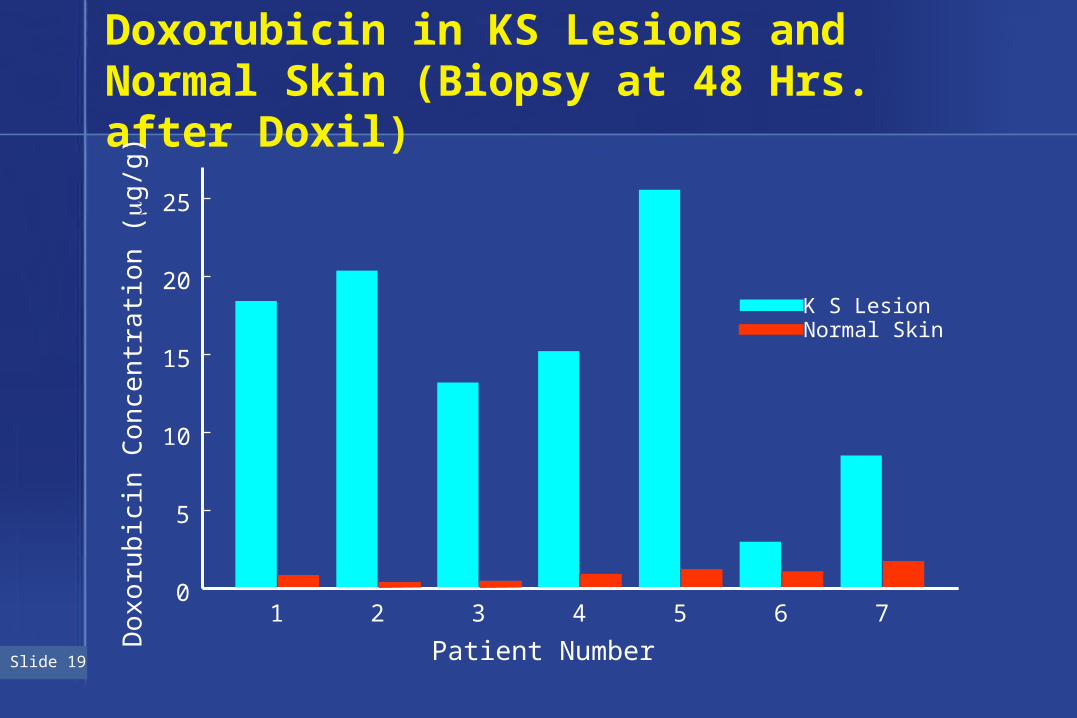
Doxorubicin in KS Lesions and Normal Skin (Biopsy at 48 Hrs. after Doxil)
1 2 3 4 5 6 7
0
5
10
15
20
25
Do
xoru
bic
in C
on
cen
tra
tion
(g
/g)
Patient Number
K S LesionNormal Skin

Slide 20
Doxil Activity in Kaposi’s Sarcoma
Doxil vs ABV
Doxil vs BV
Doxil vs Doxil + BV
N
133125
121120
6264
Response
46%25%
59%23%
79%80%
Northfelt et al, JCO (1998)
Stewart et al, JCO (1998)
Mitsuyasu et al, Proc ASCO (1997)
All PatientsPrior Adria
N
4223
Response
48%52%
Product Label
Randomized Trials
Non-comparative Results in Refractory Patients

Slide 21
Doxil Activity in Ovarian Carcinoma Xenograft (HEY)
Vaage J, et al, Cancer (1993) Days After Tumor Implantation
0 7 14 21 28 35 42 49
Me
an
Tu
mo
r V
olu
me
(m
m)3
0
20
40
60
80
100
120
140Saline control
Adriamycin(6 mg/Kg)
Doxil(6 mg/Kg)

Slide 22
Rationale for Exploring Ovarian Indication
• Preclinical activity superior to Adriamycin• Activity in heavily pretreated ovarian patients in
Phase I trial (Muggia et al, JCO 1995)
– 1 PR– 3 minor responses (CA125 , tumor shrinkage <50%)– 1 disease stabilization

Slide 23
Agenda
Unmet Medical Need: Maurie Markman, MD, Cleveland Clinic Taussig
Cancer Center
STEALTH® Technology Frank Martin, PhD,and Doxil Pharmacology: Principal Scientist
Efficacy of Doxil: Ed Schnipper, MD, VP, Clinical Research

Slide 24
Doxil Regulatory History in Ovarian Cancer
• Clinical development program initiated 8/94
• Orphan designation 11/98
• sNDA (50-718, 006) inadvanced ovarian cancer 12/98
• Priority review 3/99

Slide 25
Doxil in Refractory Ovarian Cancer
• Doxil is active
• Doxil is generally well tolerated
• Doxil is convenient

Slide 26
Program Overview
• Phase II non-comparative studies– 3 studies in relapsed or refractory ovarian cancer
• 30-22, 30-47, and 30-47E
• Phase III randomized comparative trial (study 30-49)– Doxil vs Topotecan– Second line following failure of platinum containing
regimen

Slide 27
Design of Phase II Studies
• Three multicenter non-comparative studies• All contained relapsed or refractory patients• Refractory defined as disease progression while
receiving, or within 6 months of receiving prior therapy– Plat/Pac Refractory - patients refractory to both Plat/Pac Refractory - patients refractory to both
platinum and paclitaxelplatinum and paclitaxel– Plat/Pac/Topo Refractory - patients refractory to Plat/Pac/Topo Refractory - patients refractory to
platinum, paclitaxel, and topotecanplatinum, paclitaxel, and topotecan

Slide 28
Endpoints of Phase II Studies
• Primary endpoint was response rate– All responses based on measurable disease (SWOG criteria)
– All responses confirmed
– Independent radiological review
• Secondary endpoints – Time to progression
– Duration of response
– Survival
– Safety
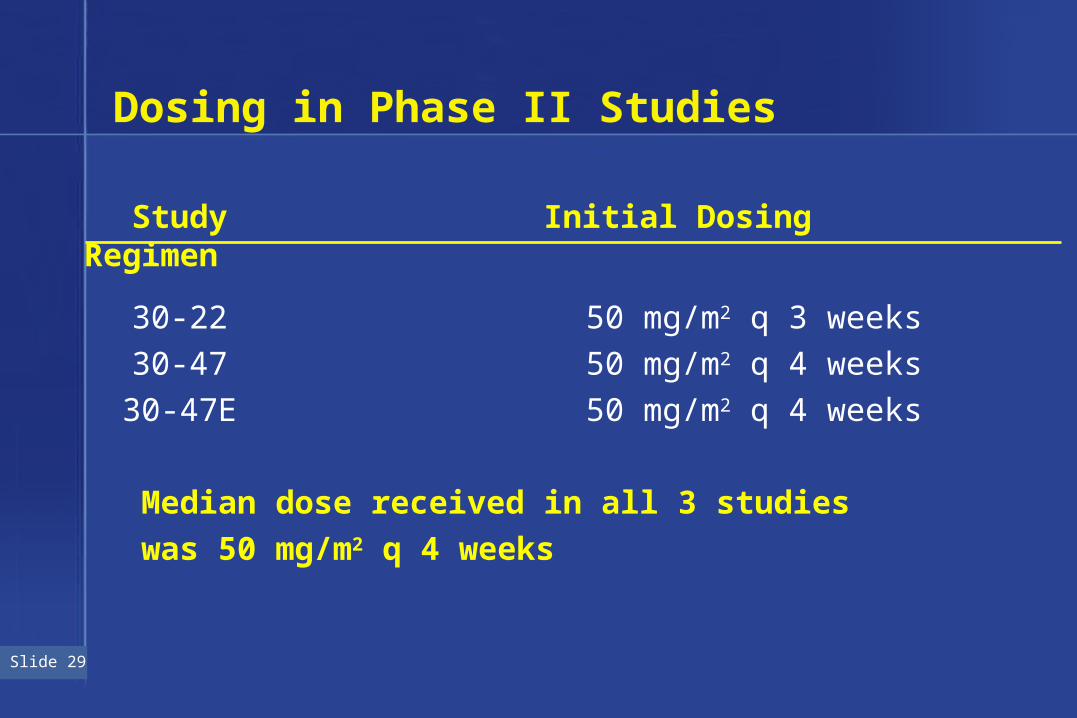
Slide 29
Dosing in Phase II Studies
Study Initial Dosing Regimen
30-22 50 mg/m2 q 3 weeks
30-47 50 mg/m2 q 4 weeks
30-47E 50 mg/m2 q 4 weeks
Median dose received in all 3 studies
was 50 mg/m2 q 4 weeks

Slide 30
Demographics of Phase II Studies
Study 30-22 Study 30-47 Study 30-47E(n = 35) (n = 89) (n = 52)
Sites 2 (US) 18 (US) 14 (Europe)
Median age 62.5 61 53.5
Patients Plat/Pac 28 49 26
refractory
Patients Plat/Pac/Topo - 33 10refractory

Slide 31
Demographics of Phase II Studies
Study 30-22 Study 30-47 Study 30-47E(n = 35) (n = 89) (n = 52)
Months from 2.1 1.7 3.7prior regimen
No. of prior regimens1 22.9% 14.6% 19.2%2 40.0% 52.8% 63.5%3 22.9% 32.6% 17.3%4 11.4% - -5 2.9% - -
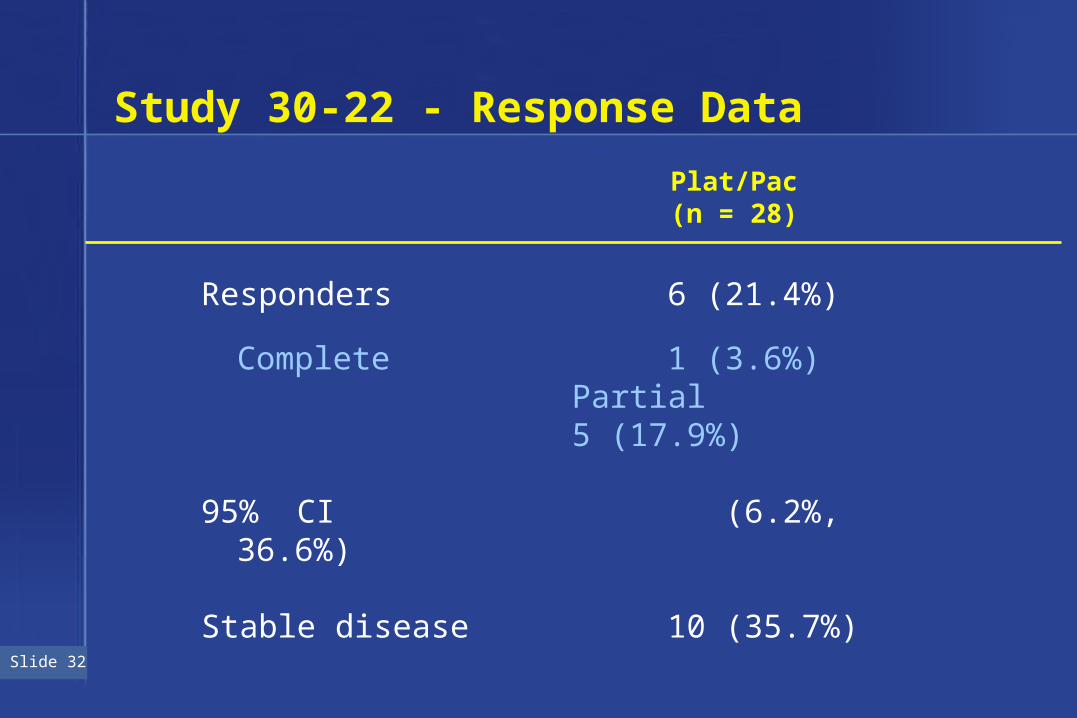
Slide 32
Study 30-22 - Response Data
Plat/Pac(n = 28)
Responders 6 (21.4%)
Complete 1 (3.6%)Partial 5 (17.9%)
95% CI (6.2%, 36.6%)
Stable disease 10 (35.7%)

Slide 33
Study 30-47 - Response Data
Plat/Pac Plat/Pac/Topo (n = 49) (n = 33)
Responders 9 (18.4%) 6 (18.2%)
Complete 0 1 (3.0%)Partial 9 (18.4%) 5 (15.2%)
95% CI (7.5%, 29.2%) (5.0%, 31.3%)
Stable disease 16 (32.6%) 15 (45.5%)

Slide 34
Study 30-47E - Response Data
• Refractory patients - no responders

Slide 35
Comparative Demographics ofRefractory Patients
Studies Study30-47 and 30-22 30-47E
Median CA-125 176 1005
Median bulky disease 18.84 32.35
Median duration of treatment (days) 57 29.5

Slide 36
Summary of Response Ratesin ITT Refractory Patients
CombinedStudy Plat/Pac Plat/Pac/Topo Refractory
30-22 21.4% - 21.4% 30-47 18.4% 18.2% 18.3%30-47E 0% 0% 0%
Total 14.6% 14.0% 14.4%
95% CI (7.8% - 21.4%) (3.6% - 24.3%) (8.7% - 20.1%)
(n = 103) (n = 43) (n= 146)
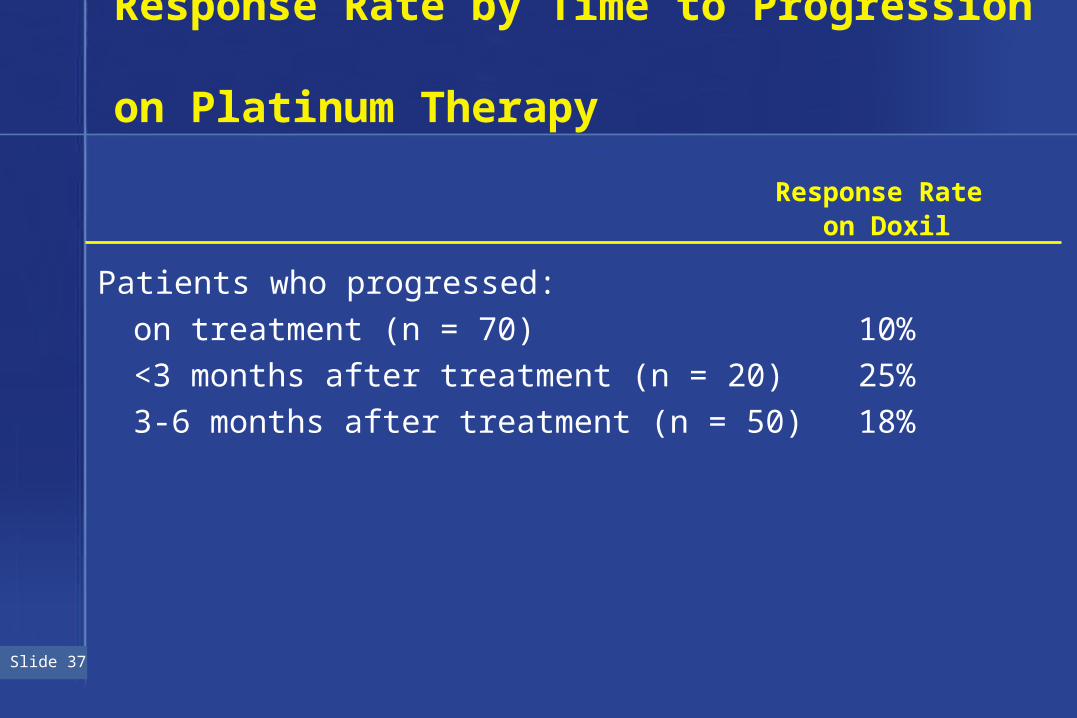
Slide 37
Response Rate by Time to Progression on Platinum Therapy
Response Rate on Doxil
Patients who progressed:
on treatment (n = 70) 10%
<3 months after treatment (n = 20) 25%
3-6 months after treatment (n = 50) 18%

Slide 38
Duration of Response
Prob
abili
ty100
80
60
40
20
00 7 14 21 28 35 42 49 56 63
Weeks Since First Dose
Median duration of response = 39.4 weeks
Combined refractory, n=21

Slide 39
Time to Progression
Prob
abili
ty100
80
60
40
20
00 15 30 45 60 75 90 105 120
Weeks Since First Dose
Median TTP = 15.9 weeks
Combined refractory, n=146

Slide 40
Time to Progression and Time to Decrease in Karnofsky Score Combined Refractory, (n=146)
0 10 20 30 40 50 60 70 80 90 100 110
100
90
80
70
60
50
40
30
20
10
0
Time to ProgressionTime to Decrease in Karnofsky Score
Weeks Since First Dose
Pro
bab
ilit
y
Slide 40

Slide 41
Phase III Randomized Comparative Trial (Study 30-49)
• Study design– Second line study following failure of
platinum-containing regimen– Patients randomized to receive
• Doxil 50 mg/m2 q 4 weeks or
• Topotecan 1.5 mg/m2 x 5 d q 3 weeks
– Patients with measurable disease– Primary endpoint — time to progression– Secondary endpoints — response rate, duration of
response, survival, and safety

Slide 42
Study 30-49
• 90 sites in US and Europe• Target of 460 patients accrued • First planned interim analysis• 200 evaluable patients (237 ITT) with at least
6 months follow-up• Patients stratified as platinum refractory or sensitive • Subset of 81 patients met the definition of
Plat/Pac refractory
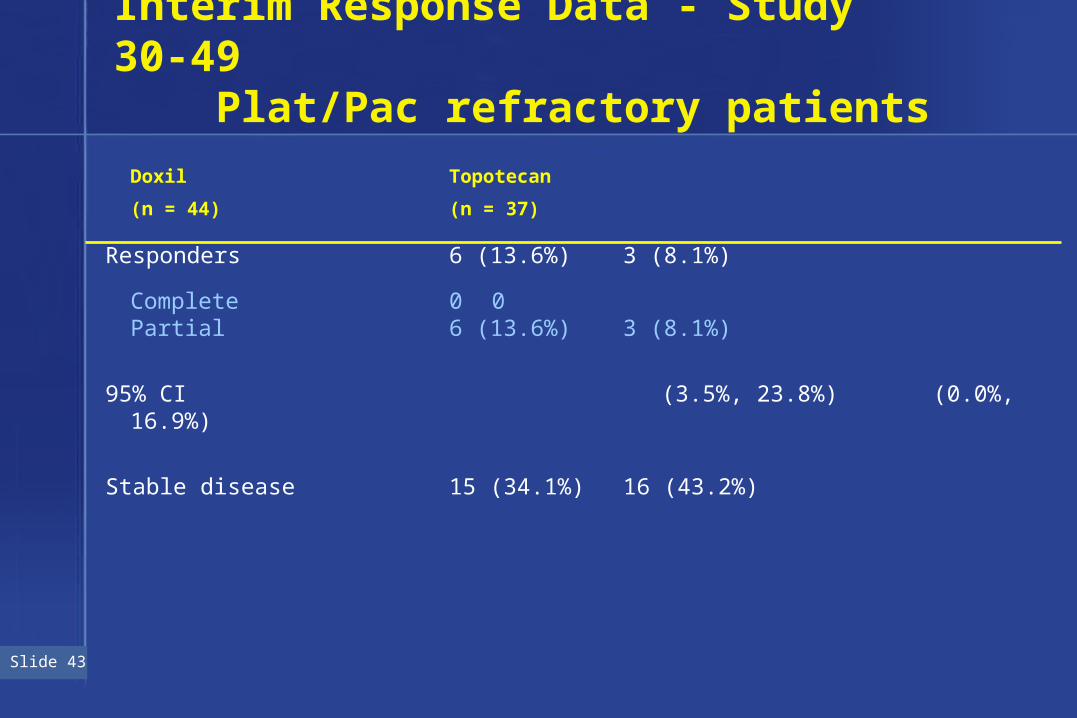
Slide 43
Interim Response Data - Study 30-49 Plat/Pac refractory patients
Doxil Topotecan
(n = 44) (n = 37)
Responders 6 (13.6%) 3 (8.1%)
Complete 0 0Partial 6 (13.6%) 3 (8.1%)
95% CI (3.5%, 23.8%) (0.0%, 16.9%)
Stable disease 15 (34.1%) 16 (43.2%)

Slide 44
Percentage Reduction in Lesion Area in Combined Refractory Patients (Studies 30-22, 30-47, 30-49, n=27)
0 2 4 6 8 10
No. of Responders
50-59
60-69
70-79
80-89
90-99
100
Per
cen
t

Slide 45
Efficacy Summary from Phase II Studies
• Response 14.4% in refractory patients
• Duration of response 39.5 weeks
• TTP 15.9 weeks

Slide 46
Agenda
Unmet Medical Need: Maurie Markman, MD, Cleveland Clinic Taussig
Cancer Center
STEALTH® Technology Frank Martin, PhD,and Doxil Pharmacology: Principal Scientist
Efficacy of Doxil: Ed Schnipper, MD, VP, Clinical Research
Safety of Doxil: Ken Cunningham, MD, VP, European Clinical
Research

Slide 47
Safety Population
• 5 studies in ovarian cancer– Total patients 408
• 16 studies in a variety of solid tumors– Total patients 772
• Kaposi’s sarcoma– Total patients 1721

Slide 48
Drug Exposure

Slide 49
Summary of Dosing Informationfor Ovarian Patients (n = 408)
• Median cycle dose 50.0 mg/m2
• Median cycle length 29.5 days
• Cumulative dose– Median 149.8 mg/m2
– Range (24.3 - 1049.8)
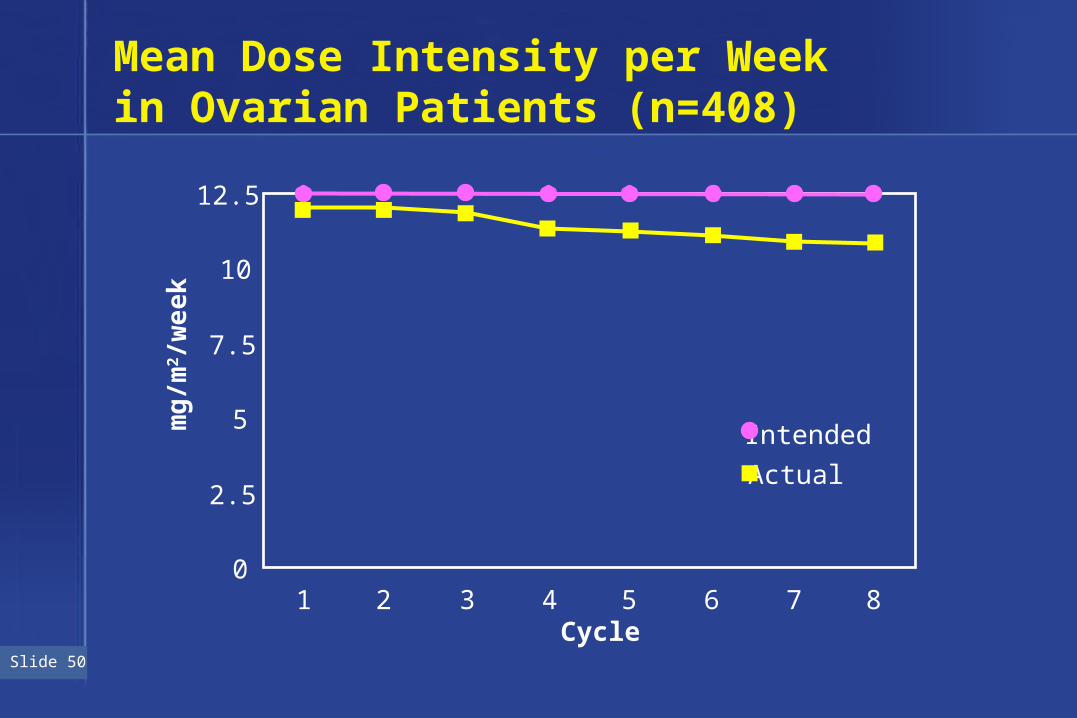
Slide 50
Mean Dose Intensity per Week in Ovarian Patients (n=408)
12.5
10
7.5
5
2.5
01 2 3 4 5 6 7 8
Cycle
IntendedActual
mg
/m2/w
eek
Slide 51
Adverse Events

Slide 52
Percent of Patients by Severity of Adverse Events (Ovarian Patients, n=396)
0
20
40
60
80
100
Grade I Grade II Grade III Grade IV Fatal
Pe
rce
nt
of
Pa
tie
nts
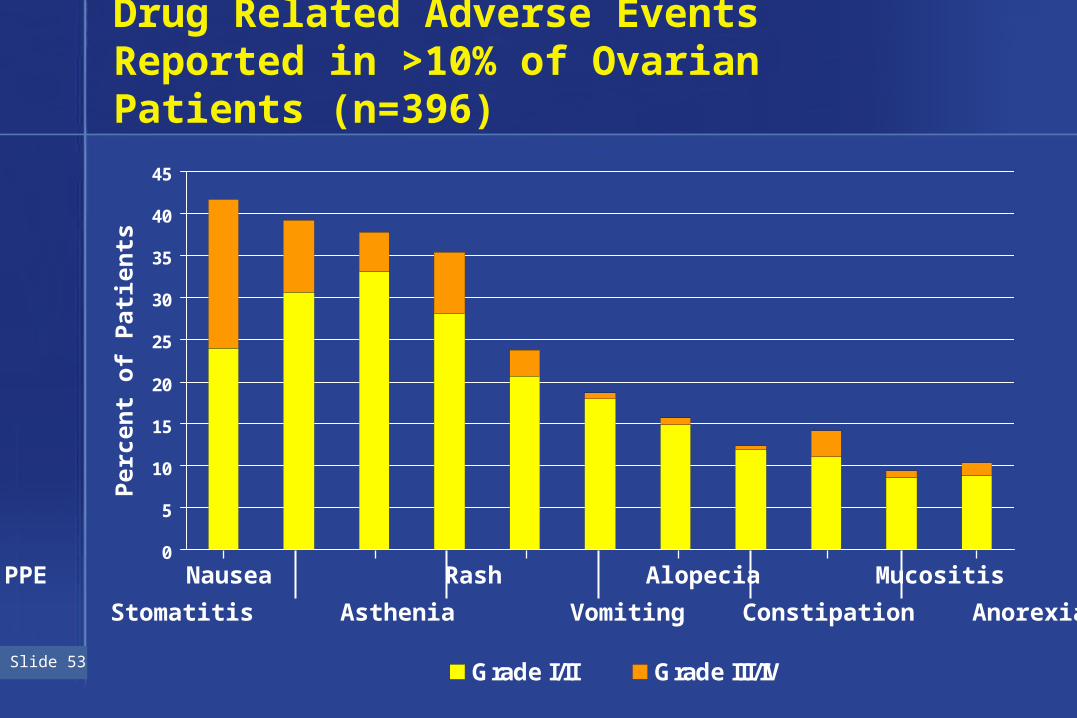
Slide 53
Drug Related Adverse Events Reported in >10% of Ovarian Patients (n=396)
0
5
10
15
20
25
30
35
40
45
Grade I/II Grade III/IV
PPE Nausea Rash Alopecia Mucositis Diarrhea
Stomatitis Asthenia Vomiting Constipation Anorexia
Per
cen
t o
f P
atie
nts

Slide 54
Hematologic Laboratory Data, Ovarian Patients (n=408)
Grade III Grade IV Comment
Neutropenia 19.6% 8.6% Growth Factor 4.1%
Anemia 23.5% 16.4% RBC Trans14.0%
Epo 4.3%
Thrombocytopenia 0.5% 0.7% Platelet Trans0.5%

Slide 55
Withdrawals Due to Drug-Related AEs,Ovarian Patients (n=396)
Total withdrawals 11.0%
Five most common AEs
PPE or other skin toxicity 3.5%
Cardiovascular disorder 1.0%
Stomatitis 0.8%
Asthenia 0.8%
Infusion reactions 0.5%

Slide 56
Palmar-Plantar Erythrodysesthesia (PPE)
Management

Slide 57
PPE - Grading and Management
Symptoms Dose Adjustment
Grade I Mild erythema Redose, unless previous Grade III/IV
Grade II Erythema with Delay 1-2 weeks or until desquamation resolved to Grade 0-I
Grade III Blistering Delay 1-2 weeks or untilresolved to Grade 0-I. Then redose at 75%
Grade IV Diffuse As for Grade III

Slide 58
Cardiotoxicity

Slide 59
Cardiotoxicity
• 0.8% (6/772) withdrew due to cardiotoxicity related to Doxil– 5 asymptomatic LVEF declines– 1 CHF (after 22 cycles — 944.3 mg/m2)
• 5 additional drug related cardiac events, all Grade I

Slide 60
Cardiac Safety
• Doxil PK mimics continuous infusion of doxorubicin• Preclinical - Less cardiotoxic1
• Biopsies in 10 KS patients (469 to 860 mg/m2) show minimal cardiotoxicity (Billingham scores 0-1.5; median 0.3)2
• Biopsies in 4 solid tumor patients (675 to 1680 mg/m2) show minimal cardiotoxicity (Billingham scores 0-1.5)
1 Working et al, JPET (1999)2 Berry, et al, Ann Oncol (1998)

Slide 61
Phase III Randomized Comparative Trial(Study 30-49)
• Doxil - 50 mg/m2 every 4 weeks
• Topotecan - 1.5 mg/m2 x 5 days every 3 weeks

Slide 62
Terminations and Dose Modifications(Study 30-49)
Doxil Topotecan(n = 135) (n = 132)
Patient still on study 45.2% 40.2%
Termination due to adverse events 6.7% 9.1%
Delayed, interrupted or reduced doses % Patients 44.4% 65.9% % Cycles 32.1% 49.9%

Slide 63
Percent of Patients by Severity of Adverse Events(Study 30-49)
0
20
40
60
80
100
Grade I Grade II Grade III Grade IV
Pe
rce
nt
of
Pa
tie
nts
Doxil Topotecan

Slide 64
0
10
20
30
40
50
60
70
80
Pe
rce
nt
Pat
ien
ts
Doxil’s 5 Most Frequent Drug-Related Adverse Events (Study 30-49)
Grade I, II
Grade III, IV
Doxil Topotecan
StomatitisPPE Anemia Asthenia Nausea

Slide 65
Topotecan’s 5 Most Common Drug-Related Adverse Events (Study 30-49)
0
10
20
30
40
50
60
70
80P
erce
nt
Pat
ien
ts
Neutropenia
ThrombocytopeniaAnemia
Alopecia Leukopenia
Grade I, II
Grade III, IV
Doxil Topotecan

Slide 66
Safety Summary
• Generally well tolerated
• PPE is the most common adverse event and is manageable
• Adverse event profile is predictable

Slide 67
Agenda
Unmet Medical Need: Maurie Markman, MD, Cleveland Clinic Taussig
Cancer Center
STEALTH® Technology Frank Martin, PhD,and Doxil Pharmacology: Principal Scientist
Efficacy of Doxil: Ed Schnipper, MD, VP, Clinical Research
Safety of Doxil: Ken Cunningham, MD, VP, European Clinical
Research
Risk/Benefit: Ed Schnipper, MD, VP, Clinical Research

Slide 68
Summary
• No approved therapy
• Objective response rate of 14.4%
• Duration of response of 39.4 weeks
• Generally well tolerated
• Convenient monthly dosing

Slide 69
Conclusions
• Doxil is active in patients with ovarian cancer who are refractory to platinum and paclitaxel and who may also be refractory to Topotecan
• Doxil represents a valuable addition to the treatment options for these patients









![Liposome [GoR]](https://static.fdocuments.net/doc/165x107/54f49f044a795997318b4927/liposome-gor.jpg)








