Skin and Body Membranes Human Anatomy and Physiology.
95
Skin and Body Membranes Human Anatomy and Physiology
-
Upload
georgiana-welch -
Category
Documents
-
view
236 -
download
2
Transcript of Skin and Body Membranes Human Anatomy and Physiology.

Skin and Body Membranes
Human Anatomy and Physiology

General Characteristics of Body Membranes
Cover surfaces of body/ line body cavities Form protective and often lubricating sheets
around organs 2 major groups
Epithelial Cutaneous/ Mucous/ Serous Membranes
Connective Synovial Membranes

Epithelial Membranes: covering & lining membranes
Cutaneous (skin) Mucous (lines body cavities that open to
exterior) Serous (lines body cavities closed to exterior) Remember all include both epithelial tissue
AND an underlying layer of connective tissue…so these membranes are actually simple organs
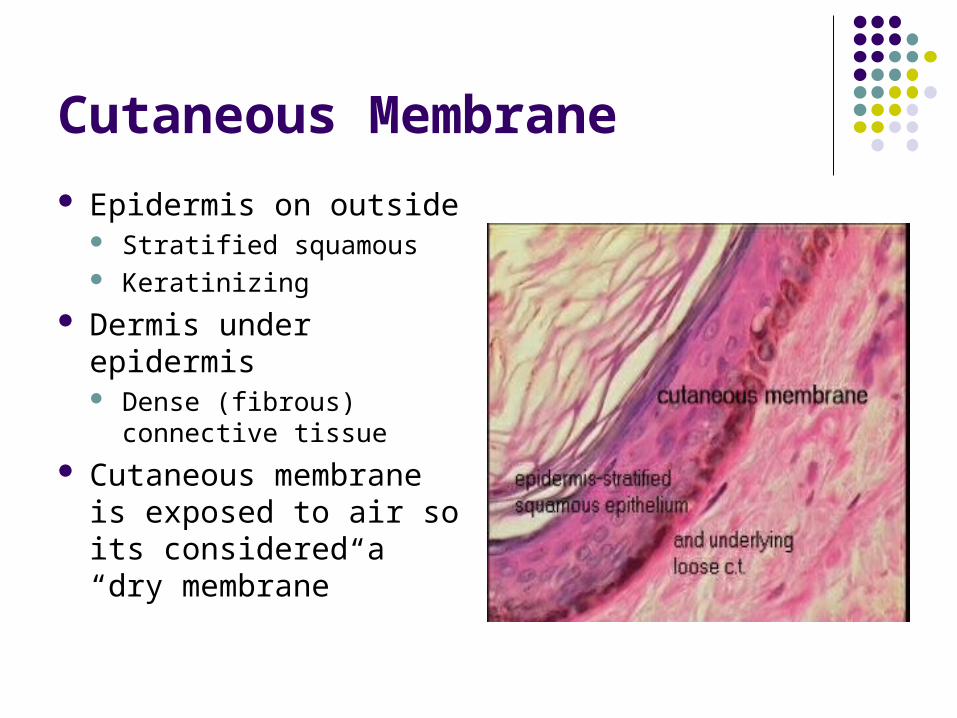
Cutaneous Membrane
Epidermis on outside Stratified squamous Keratinizing
Dermis under epidermis Dense (fibrous)
connective tissue
Cutaneous membrane is exposed to air so its considered a “dry membrane”
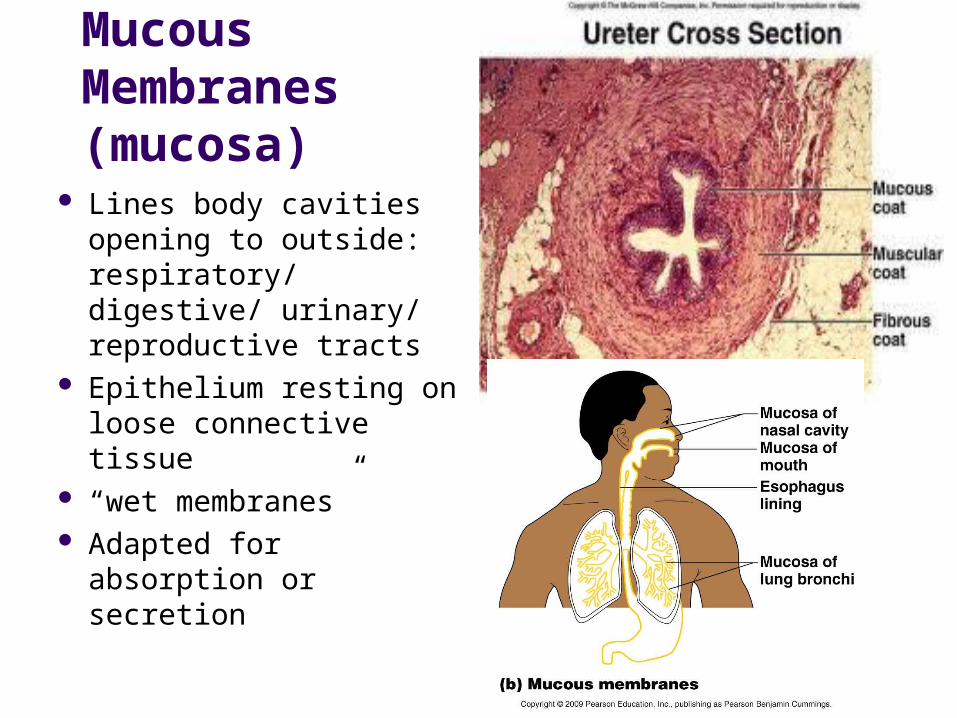
Mucous Membranes (mucosa)
Lines body cavities opening to outside: respiratory/ digestive/ urinary/ reproductive tracts
Epithelium resting on loose connective tissue
“wet membranes” Adapted for absorption
or secretion

Serous Membranes (serosa) Line body cavities that are
not exposed to outside Simple squamous
epithelium resting on thin areolar connective tissue
Occurs in pairs: parietal and visceral
Peritoneum = abdominal cavity
Pericardium = around heart
Pleura = around lungs
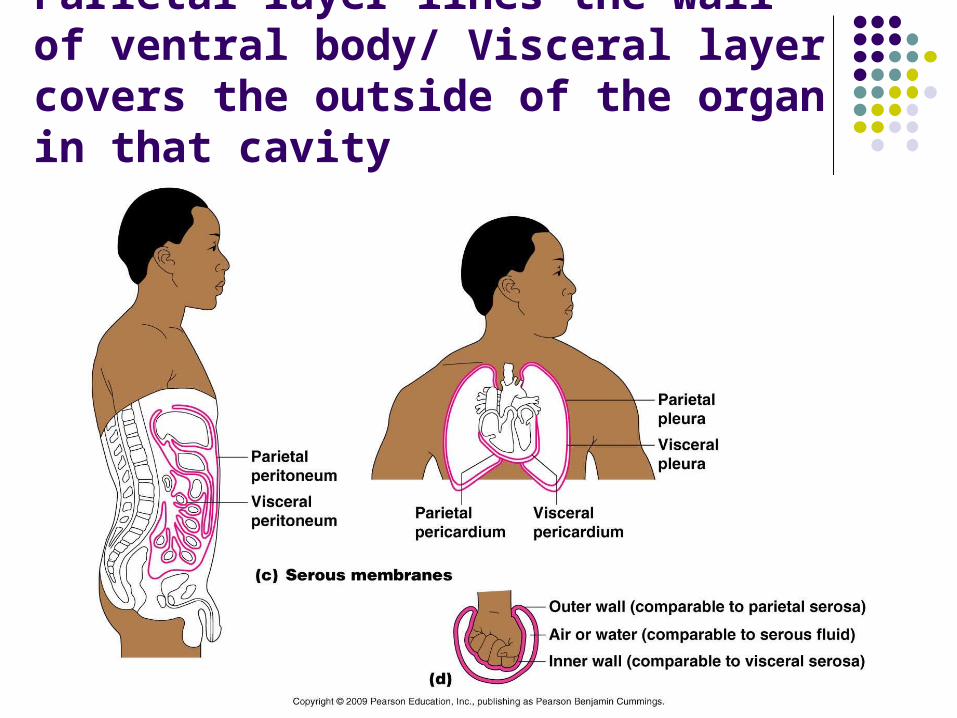
Parietal layer lines the wall of ventral body/ Visceral layer covers the outside of the organ in that cavity

Connective Tissue membranes: Synovial
No epithelial cells Soft areolar connective
tissue Line fibrous capsules
surrounding joints Cushion organs
rubbing against each other
Secrete lubricating fluid Also line bursae
The Integumentary System (your skin!)
List 4 important functions of the integumentary system, and explain how these functions are accomplished.
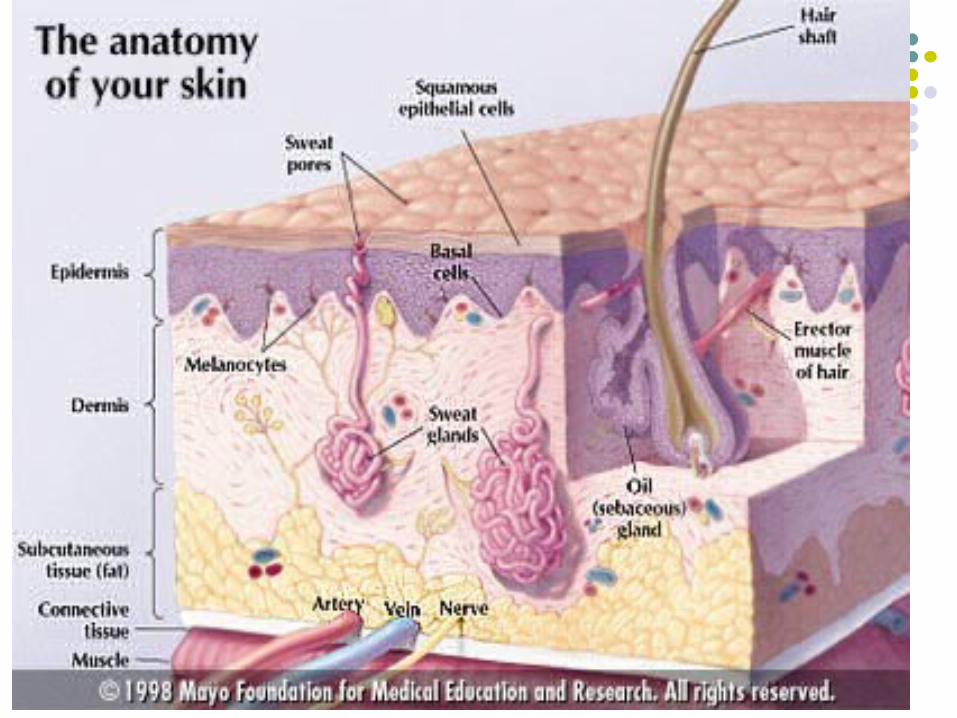
Label a diagram of the skin recognizing the following: epidermis, dermis (papillary and reticular layers), hair and hair follicle, sebaceous gland, and sweat gland
Describe the distribution and function of sebaceous glands, sweat glands and hair

The Integumentary System (continued)
Name the factors that determine skin color and describe the function of melanin
Describe syndromes/ infections/ allergic reactions in skin
Differentiate first, second and third degree burns
Explain the importance of the “rule of nines” Summarize the characteristics of basal cell
carcinoma, squamous cell carcinoma and malignant melanoma

What specifically is the integumentary system?
Cutaneous membrane
All its derivatives: Sweat glands Oil glands Hair Nails

Functions of the Skin1. Controls internal body temperature:
1. Heat loss: activates sweat glands and allows blood to flush into skin capillary beds so heat can radiate from skin surface
2. Heat retention: not allowing blood to flush to skin capillary beds
2. Aids in excretion of urea and uric acid: perspiration by sweat glands
3. Synthesizes vitamin D: modified cholesterol molecules in skin

Functions of Skin (cont.)
Protects deeper tissue from Mechanical damage: physical barrier, keratin, fat
cells, pressure receptors to stimulate movement Chemical damage: impermeable keratin,
chemoreceptors, nociceptors Bacterial damage: skin secretions Ultraviolet radiation: melanin Thermal damage: thermoreceptors/ nociceptors Desiccation: water proofing glycolipid and keratin

Integumentary system provides a wealth of sensory data
Receptors are classified by the following: Stimulus type Location Structural complexity

Classification by Stimulus Type
Mechanoreceptors—respond to touch, pressure, vibration, stretch, and itch
Thermoreceptors—sensitive to changes in temperature
Photoreceptors—respond to light energy (e.g., retina)
Chemoreceptors—respond to chemicals (e.g., smell, taste, changes in blood chemistry)
Nociceptors—sensitive to pain-causing stimuli (e.g. extreme heat or cold, excessive pressure, inflammatory chemicals)

Classification by Location
1.Exteroceptors Respond to stimuli arising outside the body Receptors in the skin for touch, pressure, pain, and temperature Most special sense organs
2. Interoceptors (visceroceptors) Respond to stimuli arising in internal viscera and blood vessels Sensitive to chemical changes, tissue stretch, and temperature
changes
3. Proprioceptors Respond to stretch in skeletal muscles, tendons, joints, ligaments,
and connective tissue coverings of bones and muscles Inform the brain of one’s movements

Classification by Structural Complexity
1. Complex receptors (special sense organs) Vision, hearing, equilibrium, smell, and taste
(Chapter 15)
2. Simple receptors for general senses: Tactile sensations (touch, pressure, stretch,
vibration), temperature, pain, and muscle sense Unencapsulated (free) or encapsulated dendritic
endings

Unencapsulated Dendritic Endings
Thermoreceptors Cold receptors (10–40ºC); in superficial dermis Heat receptors (32–48ºC); in deeper dermis
Nociceptors Respond to:
Pinching Chemicals from damaged tissue Temperatures outside the range of thermoreceptors Capsaicin
Light touch receptors Tactile (Merkel) discs Hair follicle receptors

Table 13.1

Encapsulated Dendritic Endings
All are mechanoreceptors Meissner’s (tactile) corpuscles—discriminative touch Pacinian (lamellated) corpuscles—deep pressure and
vibration Ruffini endings—deep continuous pressure Muscle spindles—muscle stretch Golgi tendon organs—stretch in tendons Joint kinesthetic receptors—stretch in articular
capsules

Table 13.1
Skin (Integument)
Consists of three major regions1. Epidermis—superficial region
2. Dermis—middle region
3. Hypodermis (superficial fascia)—deepest region Subcutaneous layer deep to skin (not technically
part of skin) Mostly adipose tissue

Epidermis
Keratinized stratified squamous epithelium Cells of epidermis
Keratinocytes—produce fibrous protein keratin Melanocytes
10–25% of cells in lower epidermis Produce pigment melanin
Epidermal dendritic (Langerhans) cells—macrophages that help activate immune system
Tactile (Merkel) cells—touch receptors

Keratin Fibrous protein that
helps give the epidermis its protective properties
Found not only in skin, but also hair, nails, claws, horns, scales, shells, feathers, even baleen plates of whales
Strong, waterproof, contains sulfur

Melanocytes
Spider-shaped cells found in stratum basale.
Produce pigment melanin which accumulates in granules called melanosomes
Melanosomes are taken up by keratinocytes where they accumulate on the sunny side of the nucleus


Layers of the Epidermis: Stratum Basale (Basal Layer)
Deepest epidermal layer firmly attached to the dermis
Single row of stem cells Also called stratum germinativum: cells
undergo rapid division Journey from basal layer to surface
Takes 25–45 days

Figure 5.2a
Dermis
Stratum corneumMost superficial layer; 20–30 layers of deadcells represented only by flat membranoussacs filled with keratin. Glycolipids inextracellular space.
Stratum granulosumThree to five layers of flattened cells,organelles deteriorating; cytoplasm full oflamellated granules (release lipids) andkeratohyaline granules.
Stratum spinosumSeveral layers of keratinocytes unified bydesmosomes. Cells contain thick bundles ofintermediate filaments made of pre-keratin.
Stratum basaleDeepest epidermal layer; one row of activelymitotic stem cells; some newly formed cellsbecome part of the more superficial layers.See occasional melanocytes and epidermaldendritic cells.(a)

Layers of the Epidermis: Stratum Spinosum (Prickly Layer)
Cells contain a weblike system of intermediate prekeratin filaments attached to desmosomes
Abundant melanin granules and dendritic cells

Figure 5.2b
MelanocyteMelanin granule
Tactile(Merkel) cell
Sensorynerve ending Epidermal
dendritic cell
Dermis
KeratinocytesStratum corneumMost superficial layer; 20–30 layers of dead cells represented only by flat membranous sacs filled with keratin. Glycolipids in extracellular space.Stratum granulosumThree to five layers of flattened cells, organelles deteriorating; cytoplasm full of lamellated granules (release lipids) and keratohyaline granules.
Stratum spinosumSeveral layers of keratinocytes unified by desmosomes. Cells contain thick bundles of intermediate filaments made of pre-keratin.
Stratum basaleDeepest epidermal layer; one row of actively mitotic stem cells; some newly formed cells become part of the more superficial layers. See occasional melanocytes and epidermal dendritic cells.
Desmosomes
(b)

Layers of the Epidermis: Stratum Granulosum (Granular Layer)
Thin; three to five cell layers in which the cells flatten
Keratohyaline and lamellated granules accumulate

Figure 5.2a
Dermis
Stratum corneumMost superficial layer; 20–30 layers of deadcells represented only by flat membranoussacs filled with keratin. Glycolipids inextracellular space.
Stratum granulosumThree to five layers of flattened cells,organelles deteriorating; cytoplasm full oflamellated granules (release lipids) andkeratohyaline granules.
Stratum spinosumSeveral layers of keratinocytes unified bydesmosomes. Cells contain thick bundles ofintermediate filaments made of pre-keratin.
Stratum basaleDeepest epidermal layer; one row of activelymitotic stem cells; some newly formed cellsbecome part of the more superficial layers.See occasional melanocytes and epidermaldendritic cells.(a)

Layers of the Epidermis: Stratum Lucidum (Clear Layer)
In thick skin Thin, transparent band superficial to the
stratum granulosum A few rows of flat, dead keratinocytes

Layers of the Epidermis: Stratum Corneum (Horny Layer) 20–30 rows of dead, flat, keratinized
membranous sacs Three-quarters of the epidermal thickness Functions
Protects from abrasion and penetration Waterproofs Barrier against biological, chemical, and physical
assaults
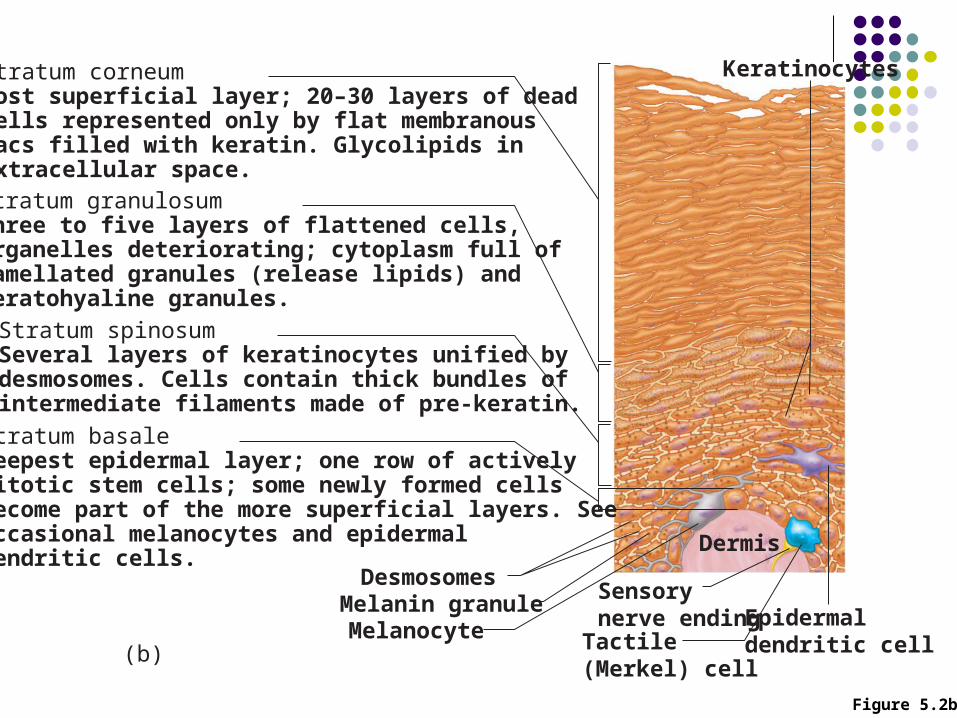
Figure 5.2b
MelanocyteMelanin granule
Tactile(Merkel) cell
Sensorynerve ending Epidermal
dendritic cell
Dermis
KeratinocytesStratum corneumMost superficial layer; 20–30 layers of dead cells represented only by flat membranous sacs filled with keratin. Glycolipids in extracellular space.Stratum granulosumThree to five layers of flattened cells, organelles deteriorating; cytoplasm full of lamellated granules (release lipids) and keratohyaline granules.
Stratum spinosumSeveral layers of keratinocytes unified by desmosomes. Cells contain thick bundles of intermediate filaments made of pre-keratin.
Stratum basaleDeepest epidermal layer; one row of actively mitotic stem cells; some newly formed cells become part of the more superficial layers. See occasional melanocytes and epidermal dendritic cells.
Desmosomes
(b)

Dermis
Strong, flexible connective tissue Cells include fibroblasts, macrophages, and
occasionally mast cells and white blood cells Two layers:
Papillary Reticular

Figure 5.1
Epidermis
Hair shaft
Dermis Reticularlayer
Papillarylayer
Hypodermis(superficial fascia)
Dermal papillae
Pore
Subpapillaryvascular plexus
Appendagesof skin • Eccrine sweat gland• Arrector pili muscle• Sebaceous (oil) gland• Hair follicle• Hair rootNervous structures
• Sensory nerve fiber• Pacinian corpuscle• Hair follicle receptor (root hair plexus)
Cutaneous vascularplexus
Adipose tissue

Layers of the Dermis: Papillary Layer
Papillary layer Areolar connective tissue with collagen and
elastic fibers and blood vessels Dermal papillae contain:
Capillary loops Meissner’s corpuscles Free nerve endings Epidermal ridges lie atop deeper dermal papillary
ridges to form friction ridges of fingerprints

Figure 5.4a
Friction ridges
(a)
Openings ofsweat gland ducts

Figure 5.4b
(b)
Layers of the Dermis: Reticular Layer
Reticular layer ~80% of the thickness of dermis Collagen fibers provide strength and resiliency Elastic fibers provide stretch-recoil properties
Collagen fibers arranged in bundles form externally invisible cleavage (tension) lines
Incisions made parallel to cleavage lines heal more readily
Skin Color
Three pigments contribute to skin color:1. Melanin
Yellow to reddish-brown to black, responsible for dark skin colors
Produced in melanocytes; migrates to keratinocytes where it forms “pigment shields” for nuclei
Freckles and pigmented moles Local accumulations of melanin
2. Carotene Yellow to orange, most obvious in the palms and soles
3. Hemoglobin Responsible for the pinkish hue of skin

Erythema
Redness of the skin caused by
embarrassment, fever, hypertension, inflammation, allergy…or even massage, acne medicine, waxing, lyme disease
30-50% erythema of unknown cause

Pallor or Blanching
Caused by fear, anger, certain emotional stress
Often a symptom of anemia or low blood pressure
Raynaud’s syndrome
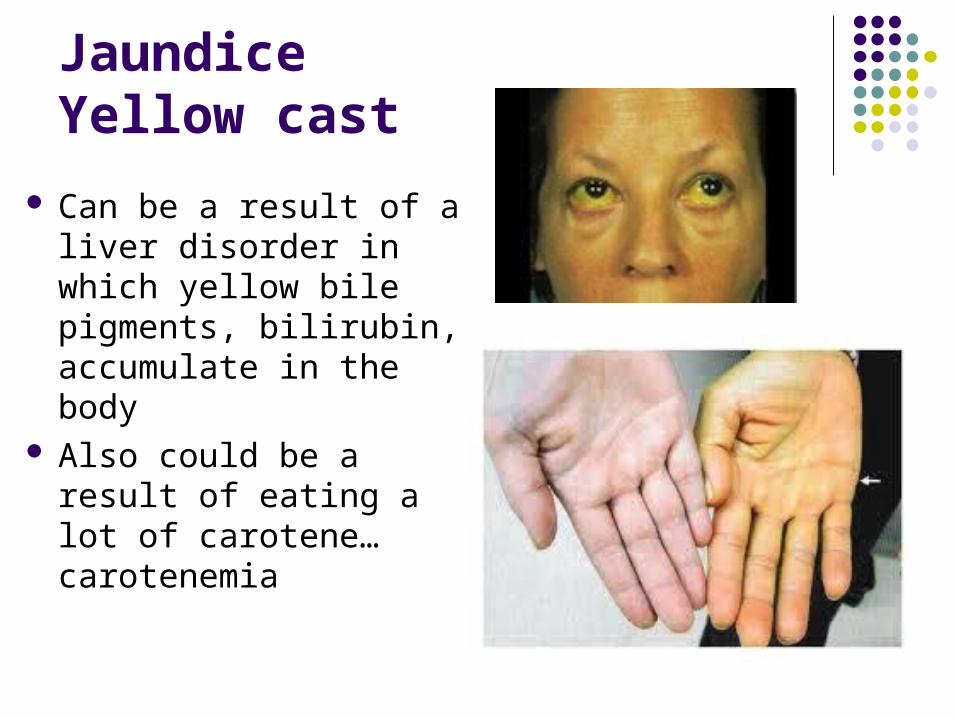
JaundiceYellow cast
Can be a result of a liver disorder in which yellow bile pigments, bilirubin, accumulate in the body
Also could be a result of eating a lot of carotene…carotenemia

Albinism
Absence of pigment in the skin, hair and eyes.
Melanocytes are present but melanin not produced because of missing or disabled enzyme

Black and Blue marksBruising
Bruise can also be called a contusion
Where blood has escaped from the circulation and clotted beneath the skin
Mild Hematoma

Cyanosis
When hemoglobin is poorly oxygenated both the blood and often the skin appear blue
Skin become cyanotic during heart failure and severe respiratory disorders
Not as evident in darker skinned people

Blue Fugates of Troublesome Creek, Kentucky
Genetic Disorder that was amplified in a small Appalachain community from a French descendant
Form of hemoglobin, methemoglobin cannot be recycled back into hemoglobin because of an enzyme deficiency

Part 2 Skin Appendages Compare the structure and locations of sweat
and oil glands and their secretions. Compare and contrast eccrine and apocrine
glands. List the parts of a hair follicle. Describe
functional relationship of arrector pili muscles to the hair follicle.
Name the regions of a hair and explain the basis of hair color.
Describe the structure of nails.

Sweat Glands
Two main types of sweat (sudoriferous) glands
1. Eccrine (merocrine) sweat glands—abundant on palms, soles, and forehead
Sweat: 99% water, NaCl, vitamin C, antibodies, dermcidin (microbe killing peptide), metabolic wastes (urea, uric acid and ammonia)
pH from 4-6 Ducts connect to pores Function in thermoregulation

Multicellular Exocrine Glands
Multicellular exocrine glands are composed of a duct and a secretory unit
Classified according to:Duct type (simple or compound) Structure of their secretory units
(tubular, alveolar, or tubuloalveolar)

Figure 4.5
Compound duct structure(duct branches)
Simple tubular
ExampleIntestinal glands
Simple branchedtubular
ExampleStomach (gastric)glands
Compound tubular
ExampleDuodenal glands of small intestine
Compound alveolar
ExampleMammary glands
Simplealveolar
ExampleNo importantexample in humans
Simple branchedalveolar
ExampleSebaceous (oil)glands
Compoundtubuloalveolar
ExampleSalivary glands
Tubularsecretorystructure
Alveolarsecretorystructure
Surface epithelium Duct Secretory epithelium
Simple duct structure(duct does not branch)
Modes of SecretionMerocrine
Products are secreted by exocytosis (e.g., pancreas, sweat and salivary glands)
HolocrineProducts are secreted by rupture
of gland cells (e.g., sebaceous glands)
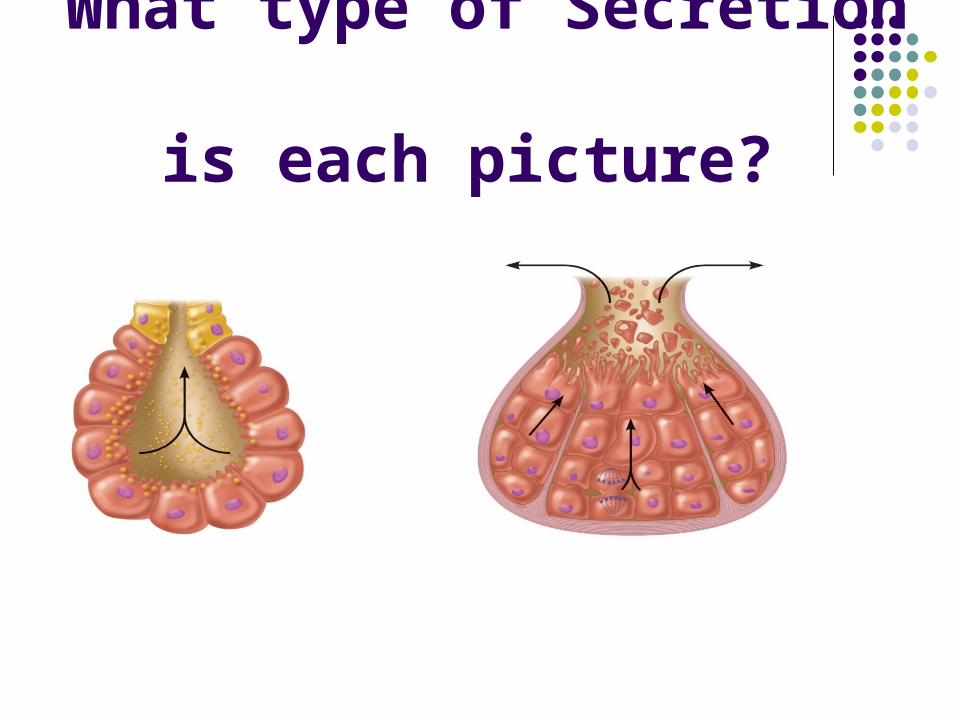
What type of Secretion is each picture?

Eccrine Sweat Glands are also called merocrine sweat glands
Sweating is regulated by the sympathetic division of the autonomic nervous system
Major role is to prevent overheating of body Heat induced sweating begins on forehead
and spreads inferiorly over body Emotionally induced sweating begins on
palms, soles and axillae then spreads to other areas of body
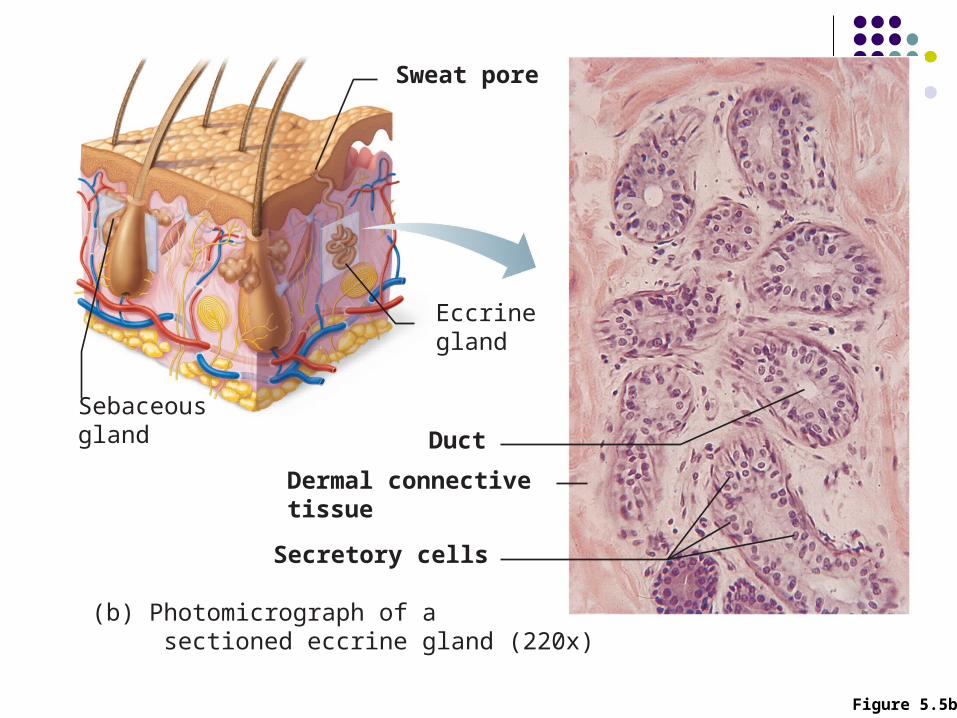
Figure 5.5b
(b) Photomicrograph of a sectioned eccrine gland (220x)
Secretory cells
Dermal connectivetissue
Duct
Sebaceousgland
Sweat pore
Eccrinegland

Sweat Glands (cont.)2. Apocrine sweat glands—confined to axillary and
anogenital areas Sebum: sweat + fatty substances and proteins so
secretion is yellow or whitish Ducts connect to hair follicles Functional from puberty onward (as sexual scent
glands?)/ basis of body odor Also merocrine glands as opposed to other apocrine
glands (3rd type of gland not seen in humans) Specialized apocrine glands
Ceruminous glands—in external ear canal; secrete cerumen…ear wax!
Mammary glands
Sebaceous (Oil) Glands
Widely distributed, large on face, neck and upper chest
Most develop from hair follicles Become active at puberty Sebum
Oily holocrine secretion Bactericidal Softens hair and skin

Figure 5.5a
(a) Photomicrograph of a sectioned sebaceous gland (220x)
Sebaceousgland duct
Hair inhair follicle
Secretory cells
Dermalconnectivetissue
Sebaceousgland
Sweatpore
Eccrinegland

What is Acne?
Whitehead: When a sebaceous gland duct is blocked by accumulated sebum.
If sebum oxidezes and dries: blackhead
Cradle Cap (seborrhea) is from overactive sebaceous glands
“pores” on face are external outlet of hair follicles, where sebaceous glands empty
Acne is active inflammation of sebaceous lands accompanied by “pimples” which are pustules or cysts on skin
Acne is usually caused by bacterial infection, often staphylococcus.
Hair
Functions in Humans Alerting the body to presence of insects on the skin Guarding the scalp against physical trauma, heat
loss, and sunlight As opposed to other mammal hair functions like
trapping body heat Distribution
Entire surface except palms, soles, lips, nipples, and portions of external genitalia

Hair Consists of dead keratinized cells Contains hard keratin; more durable than soft
keratin of skin (and doesn’t flake off) Three layers: medulla, cortex and cuticle Hair pigments: melanins (yellow, rust brown,
black) produced by melanocyctes at base of hair follicle amd transferred to cortical cells Gray/white hair: decreased melanin production,
increased air bubbles in shaft Red hair due to iron containing pigment
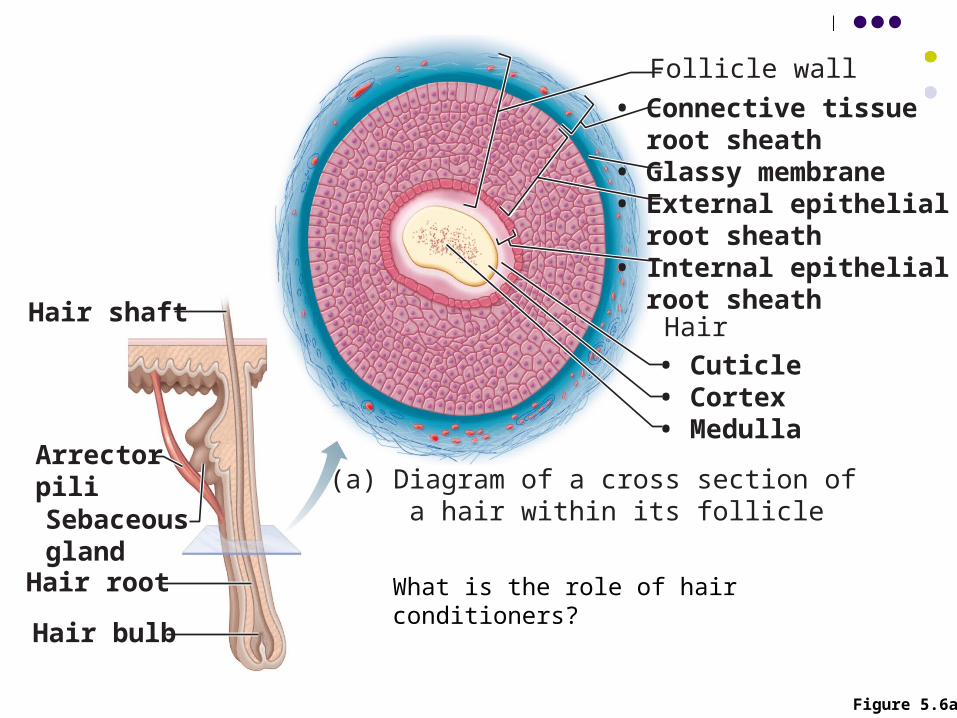
Figure 5.6a
Hair shaft
ArrectorpiliSebaceousglandHair root
Hair bulb
(a) Diagram of a cross section of a hair within its follicle
• Connective tissue root sheath• Glassy membrane• External epithelial root sheath• Internal epithelial root sheath
Follicle wall
• Cuticle• Cortex• Medulla
Hair
What is the role of hair conditioners?

(b) Photomicrograph of a cross section of a hair and hair follicle (250x)
• Connective tissue root sheath
Follicle wall
• Cuticle
• Glassy membrane
• Cortex• Medulla
• Internal epithelial root sheath
• External epithelial root sheath
Hair
Hair shaft
ArrectorpiliSebaceousglandHair root
Hair bulb
Figure 5.6b
Hair Follicle
Extends from the epidermal surface into dermis
Two-layered wall: outer connective tissue root sheath, inner epithelial root sheath
Hair bulb: expanded deep end Hair papilla of dermal tissue protrudes into the hair
bulb Contains a knot of capillaries that provide nutrients
to growing hair

Hair Follicle
Hair follicle receptor (root hair plexus) Sensory nerve endings around each hair bulb
Stimulated by bending a hair
Arrector pili Smooth muscle attached to follicle Responsible for “goose bumps”

Figure 5.6c
Hair shaft
ArrectorpiliSebaceousglandHair root Hair bulb
(c) Diagram of a longitudinal view of the expanded hairbulb of the follicle, which encloses the matrix
• Internal epithelial root sheath• External epithelial root sheath
• Connective tissue root sheathFollicle wall
Hair matrix
MelanocyteHair papilla
Subcutaneous adipose tissue
• Medulla• Cortex• Cuticle
• Glassy membrane
Hair root

(d) Photomicrograph of longitudinal view of the hair bulb in the follicle (160x)
Follicle wall
Hair matrix
Hair papilla
Subcutaneousadipose tissue
Hair root
• Connective tissue root sheath• Glassy membrane• External epithelial root sheath• Internal epithelial root sheath
• Cuticle• Cortex• Medulla
Hair shaft
ArrectorpiliSebaceousglandHair root
Hair bulb
Figure 5.6d

Types of Hair
Vellus—pale, fine body hair of children and adult females
Terminal—coarse, long hair of eyebrows, scalp, axillary, and pubic regions (and face and neck of males)
Hair growth and density influenced by nutrition, hormones and local blood flow (that can be increased by physical irritation)

Hirsutism: excessive hairiness (particularly in women)
May result in an adrenal gland or ovarian tumor that secretes abnormally large amounts of androgens.

Types of Hair
Hair Growth Growth rate averages 2.5 mm per week Each follicle goes through growth cycles:
Growth phase (weeks to years) followed by regressive stage and resting phase (1–3 months)
Growth phase varies (6–10 years in scalp, 3–4 months in eyebrows)
During regressive stage, hair falls out. After resting phase, cycling starts again and new hair is formed to replace one that fell out
Loose an average of 90 scalp hairs daily

Hair Thinning and Baldness Alopecia—hair thinning in both sexes after age
40 True (frank) baldness
Genetically determined and sex-influenced condition Male pattern baldness is caused by follicular response
to DHT Until recently, the only cure for male pattern baldness
was to inhibit testosterone production…problems with this?
By accident, minoxidil to reduce HBP, also stimulates hair regrowth
Structure of a Nail
Scalelike modification of the epidermis on the distal, dorsal surface of fingers and toes
Made of hard keratin Each nail has free edge, body and proximal root Nail matrix at proximal root; responsible for nail
growth Normally appear pink/ region over thick nail
matrix looks like half moon (lunule)

Figure 5.7
Lateralnail fold
Lunule
Nailmatrix
Root of nail
Proximalnail fold
Hyponychium
Nail bed
Phalanx (bone of fingertip)
Eponychium(cuticle)
Bodyof nail
Free edgeof nail
(a)
(b)
Nail Basics Proximal and lateral
borders of nail are overlapped by skin folds called nail folds
Proximal nail fold is the eponychium (aka: cuticle)
Region beneath the free edge of the nail where dirt and debris accumulate is the hyponychium (quick)

Functions of the Integumentary System
1. Protection—three types of barriers Chemical
Low pH secretions (acid mantle) and defensins retard bacterial activity
Physical and Mechanical Keratin and glycolipids block most water and water-
soluble substances Limited penetration of skin by lipid-soluble substances,
plant oleoresins (e.g., poison ivy), organic solvents, salts of heavy metals, some drugs
Biological barriers Dendritic cells, macrophages, and DNA

Functions of the Integumentary System
2. Body temperature regulation ~500 ml/day of routine insensible perspiration (at
normal body temperature) At elevated temperature, dilation of dermal
vessels and increased sweat gland activity (sensible perspirations) cool the body
3. Cutaneous sensations Temperature, touch, and pain
Functions of the Integumentary System
4. Metabolic functions Synthesis of vitamin D precursor and
collagenase Chemical conversion of carcinogens and some
hormones
5. Blood reservoir—up to 5% of body’s blood volume
6. Excretion—nitrogenous wastes and salt in sweat
Part Three: Homeostatic Imbalances of Skin
Summarize the characteristics of three major skin cancers
Explain why serious burns are life threatening. Describe how to determine the extent of a burn and differentiate first, second and third degree burns.
Discuss various common homeostatic imbalances from acne to psoriasis.
ID effects of tattoo on skin
Homeostatic Imbalances of Skin: Infections & AllergiesSkin can develop more than 1000 different
conditions and ailments.Objectives:1. Describe cause of several common skin
disorders .2. Summarize the characteristics of the three
major types of skin cancers.3. Explain why serious burns are life
threatening. Describe how to determine the extent of a burn and differentiate first, second and third-degree burns.

Burns
When skin is burned, 2 life threatening problems result: body loses supply of fluids containing proteins
and electrolytes. Dehydration and electrolyte imbalance can lead to kidney shut down and circulatory shock (inadequate blood flow to body)
After 24 hours, infection is important threat…leading cause of death in burn victims.
Rule of Nines: way to determine volume of fluid lost by burns

Rule of Nines
Divides the body into 11 areas each representing 9% of total body area, with genitals accounting for remaining 1%
This is obviously only an approximation

Classification of Burns First Degree
Only the epidermis is damaged
Red and swollen Heals in 2-3 days Sunburn
Second Degree Injury to epidermis and
upper region of dermis Red, painful, blisters Care to protect from
infection
Third Degree Destroys entire thickness
of skin Full thickness burn Appears blanched (gray-
white) or blackened Nerve endings are
destroyed/ not painful Regeneration not
possible/ skin grafting necessary


Skin Cancer The single most common type of cancer in
humans 1 in 5 Americans will develop skin cancer Most important risk factor: overexposure
ultraviolet radiation in sunlight Damages DNA bases (pyrimidines: C and T) UV light disables tumor suppressor gene: p53
Most skin neoplasms are benign and do not metastasize. For example: a wart
There are three types of malignant skin neoplasms

Basal Cell Carcinoma Least malignant Most common skin
cancer/ 80% Skin cells no longer
honor boundary between epidermis and dermis/ cannot form keratin
Shiny domed shaped nodules
Slow growing Surgically removed, full
cure in 99% cases
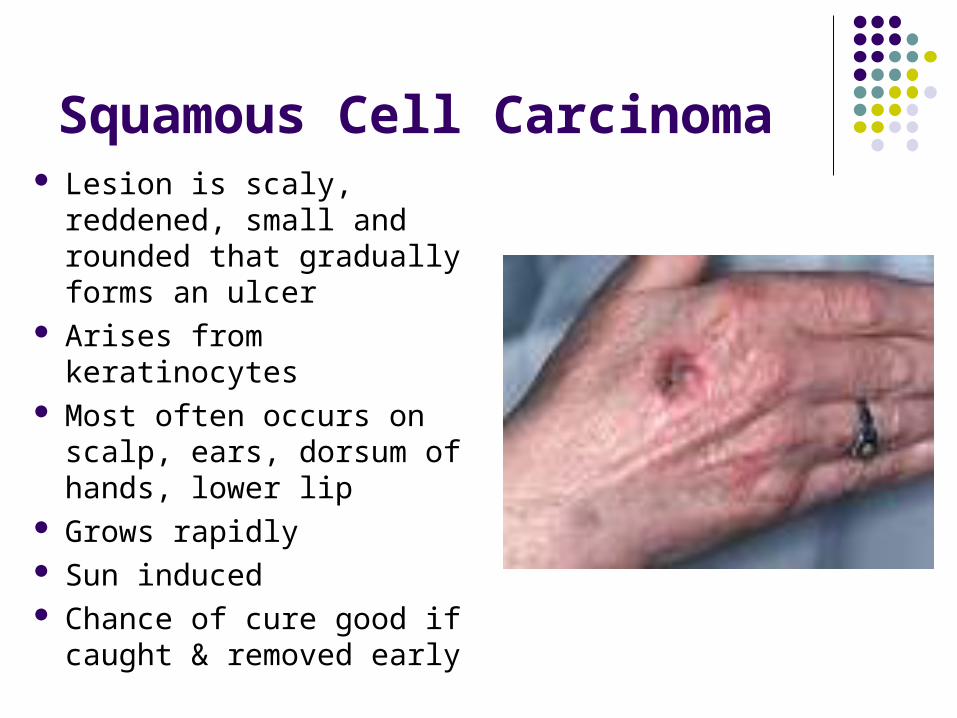
Squamous Cell Carcinoma Lesion is scaly, reddened,
small and rounded that gradually forms an ulcer
Arises from keratinocytes Most often occurs on
scalp, ears, dorsum of hands, lower lip
Grows rapidly Sun induced Chance of cure good if
caught & removed early
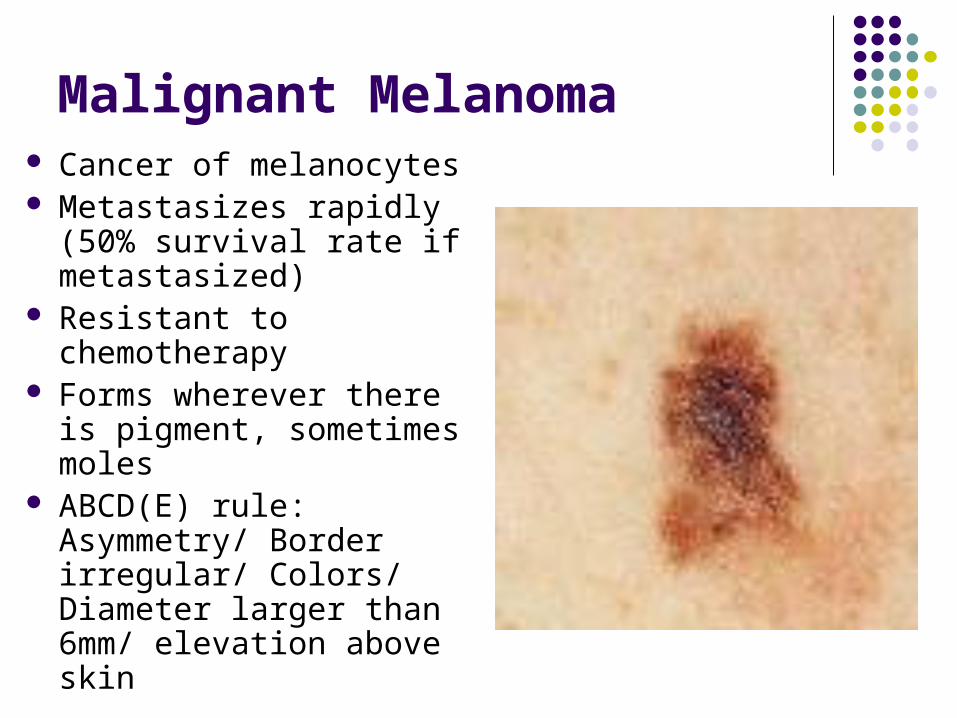
Malignant Melanoma Cancer of melanocytes Metastasizes rapidly (50%
survival rate if metastasized)
Resistant to chemotherapy Forms wherever there is
pigment, sometimes moles ABCD(E) rule:
Asymmetry/ Border irregular/ Colors/ Diameter larger than 6mm/ elevation above skin
Your epidermal cells scream for sunscreen!
Sunscreens are currently rated for their ability to prevent sunburn but not for their ability to protect against DNA damage.
SPF: Sun Protection Factor
Research = levels of radiation not strong enough to burn still affect DNA

Ultraviolet Light
UVA (ultraviolet-A): long- wave solar rays of 320-400 nanometers (billionths of a meter). Although less likely than UVB to cause sunburn, UVA penetrates the skin more deeply, and is considered the chief culprit behind wrinkling, leathering, and other aspects of "photoaging." The latest studies show that UVA not only increases UVB 's cancer-causing effects, but may directly cause some skin cancers, including melanomas.
UVB (ultraviolet-B): short-wave solar rays of 290-320 nanometers. More potent than UVA in producing sunburn, these rays are considered the main cause of basal and squamous cell carcinomas as well as a significant cause of melanoma.

Suncreens Sunblocks and sunscreens: Sunscreens chemically absorb UV rays,
sunblocks physically deflect them. Sunscreen has long blocked UVB effectively, but until recently provided less UVA protection. New ingredients such as octylcrylene and the benzophenones have improved sunscreen's defenses against shorter UVA rays, and the revolutionary chemical avobenzone (Parsol 1789) works against all UVA wavelengths.
Sunblocks have also markedly improved. New preparations such as micronized titanium dioxide are less conspicuous on the skin and offer substantial protection against both UVA and UVB.
SPF (sun protection factor): measures the length of time a product protects against skin reddening from UVB, compared to how long the skin takes to redden without protection. If it takes 20 minutes without protection to begin reddening, using an SPF 15 sunscreen theoretically prevents reddening 15 times longer -- about 5 hours. (Actually, it may take up to 24 hours after sun exposure for redness to become visible.) To maintain the SPF, reapply sunscreen every two hours and right after swimming.

Look for new DNA protecting Sunscreen Contains enzymes in
liposomes that initiate repair of DNA, particularly at the pyrimidines that have fused together.