
Skeletal System Shannon Carroll, MD Suresh Agarwal, MD.
97
PROPERTIES Allow userto leave interaction: Anytime Show ‘N extSlide’Button: Show alw ays C om pletion Button Label: View Presentation
-
Upload
shyann-walston -
Category
Documents
-
view
213 -
download
0
Transcript of Skeletal System Shannon Carroll, MD Suresh Agarwal, MD.

PROPERTIESAllow user to leave interaction: AnytimeShow ‘Next Slide’ Button: Show alwaysCompletion Button Label: View Presentation

Skeletal System
Shannon Carroll, MDSuresh Agarwal, MD

Slide 3
Skeletal System
• Common Skeletal System Pathology encountered in Critical Care
• Complications of Skeletal Injury

Slide 4
Skull
www.pycomall.com/images/P/skull.jpg

Slide 5
Skull Fractures
4 Major Types
• Linear
• Depressed
• Diastatic
• Basilar

Slide 6
Linear Skull Fracture
• Most common type
• Over Lateral Convexities
• Over squamous area of temporal bone
– Damage to middle meningeal artery
– Epidural Hematoma
www.hawaii.edu/medicine/pediatrics/pemxray/v5c09h2.jpg

Slide 7
Depressed Skull Fracture
• Displaced bone fragments pushed into the cranial vault
• From blunt force by object with small surface area
• Often damages underlying brain tissue
• Complex = dura mater torn
• Contamination/Infection
• Often require surgery
anatpat.unicamp.br/minDsc35446+.jpg

Slide 8
Diastatic Skull Fracture
• Fracture causes widening of suture
• Most commonly seen in infants and small children
• Seen in adults along the lambdoid suture
Pirouzmand F, Muhajarine N. Craniofac Surg. 2008 Jan;19(1):27-36. Definition of topographic organization of skull profile in normal population and its implications on the role of sutures in skull morphology. img.medscape.com/pi/emed/ckb/radiology/336139-343764-9928.jpg

Slide 9
Basilar Skull Fracture
• From blunt force to the forehead or occiput
• Usually anterior
– Often involves cribriform plate
– Disruption of olfactory nerves
• Posterior
– Through petrous bone and internal auditory canal
– Disruption of the vestibulocochlear nerve and facial nerves
• CSF otorrhea/rhinorrhea
t0.gstatic.com/images?q=tbn:TuEw6pvP4iIG5M:http://img.medscape.com/pi/emed/ckb/neurosurgery/247017-
248108-4155.jpg

Slide 10
Basilar Skull Fracture
Raccoon Eyes
image.absoluteastronomy.com/images/encyclopediaimages/b/
bl/blackeye_pigmentation.jpg
www.itim.nsw.gov.au/images/Battle_Sign_s.jpg
Battle’s Sign

Slide 11
Vertebral Injuries
• Vertebral Column forms the Axial Skeleton
• Among All Trauma Patients
– 4.3% Cervical Spine Injury
– 6.3% Thoracolumbar Spine Injury
– 1.3% Spinal Cord Injury
www.eorthopod.com/images/ContentImages/spine/spine_thoracic/anatomy/thoracic_spine_anatomy01.jpg
Slide 12
Vertebral Injuries
7 Mechanisms of Injury
• Flexion – compression
• Axial compression
• Flexion – distraction
• Hyperextension
• Rotation
• Shear
• Avulsion

Slide 13
Cervical Spine Injuries
www.physiotherapy-treatment.com/images/human-lateral-cervical-
spine.jpg

Slide 14
Cervical Spine Injuries
• 25% Occiput to C2
• 75% C3 to C7
• Occipto-cervical subluxation
– Rare
– Usually fatal
• Fractures of the Atlas
– Pain
– Decreased mobility
• Atlanto-axial dislocation
– High risk of neurologic deficit www.springerlink.com/content/26ghau7p5nmpcjle/

Slide 15
Fractures of the Odontoid
• Apical ligament avulsion fracture
• Stable
• Minimal if any external support
img.medscape.com/pi/emed/ckb/orthopedic_surgery/1230552-1267150-
1299.jpg
Slide 16
Fractures of the Odontoid
• Waist of the odontoid
• Unstable
• Requires reduction or translation and angulation
• Requires stabilization
– Surgical
– Halo vest img.medscape.com/pi/emed/ckb/orthopedic_surgery/1230552-1267150-
1299.jpg

Slide 17
Fractures of the Odontoid
• Extends below the waist into the body of C2
• Best treated with a halo vest
• 15% incidence of nonunion with other immobilization
img.medscape.com/pi/emed/ckb/orthopedic_surgery/1230552-1267150-
1299.jpg

Slide 18
Thoracolumbar Spine Injuries
• L1 fracture 16%
• Spondylolisthesis
– Subluxation or Slip of one vertebral body on another
– Most common in lumbar spine
– Treatment
• Conservative management
• Fusion www.webinique.com/images/lumbar_spondylolisthesis_grades.
jpg

Slide 19
Spinal Instability
• Disruption of anatomic components, motion or supportive elements
• Excessive or abnormal spinal motion
• 3 Column Model
– In thoracolumbar spine
– Instability = Injury to 2 or 3 columns
www.pgblazer.com/wp-content/uploads/2009/11/three-column-concept-2.jpg

Slide 20
Spinal Instability
www.pgblazer.com/wp-content/uploads/2009/11/three-column-concept-2.jpg
• 50% Loss of Vertebral Body Height
• Angulation > 20%
• Compression Fractures
• Burst Fractures

Slide 21
Non-operative Management of Spinal Injuries
• Stable injuries
• No neurologic deficits
• Immobilization
www.alsab.ca/images/collar2.jpg

Slide 22
Spinal Immobilization
• C– spine
– Head halter
– Tongs
– Halo
images.allegrocentral.com/9E/75/J-Tongs-Traction-Tongs-557879-PRODUCT-
MEDIUM_IMAGE.jpg
www.ossur.com/lisalib/getfile.aspx?itemid=15083&proc=3

Slide 23
Spinal Immobilization
• T– and L– spine
– Bedrest
– Log rolling
– Rigid brace
www.optecusa.com/sites/default/files/imagecache/product_list/
products_01_B09.jpg

Slide 24
Operative Management of Spinal Injuries
• Spinal Fusion
– Pedicle screws and rods
• Vertebroplasty
• Kyphoplasty
www.backpain-guide.com/Chapter_Fig_folders/
Ch15_Carpentry_Folder/Ch15_Images/
15_3_Pedicle_Screws.jpg
eldoradopainmanagement.net/mediac/450_0/media/
Compression_Render_Final.jpg
www.vancouverspinedoctor.com/images/balloon_kyphoplasty.jpg

Slide 25
Cervical Spine Clearance
The NEXUS Clinical Criteria
1. Tenderness at the posterior midline of the cervical spine
2. Focal neurologic deficit
3. Decreased level of alertness
4. Evidence of intoxication
5. Clinically apparent pain that might distract the patient from the pain of a cervical spine injury
– Any of the above -> increased risk for cervical spine injury -> requires radiographic evaluation
– Sensitivity: 99.6%
– NPV: 99.9%
– Specificity: 12.9%
– PPV: 2.7%
Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set ofclinical criteria to rule out injury to the cervical spine in patients
with blunt trauma. National Emergency X-Radiography UtilizationStudy Group. N Engl J Med. 2000;343:94 –99.

Slide 26
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for identifying cervical spine injuries following trauma. 2009.

Slide 27
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for identifying cervical
spine injuries following trauma. 2009.

Slide 28
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for
identifying cervicalspine injuries following trauma. 2009.
Slide 29
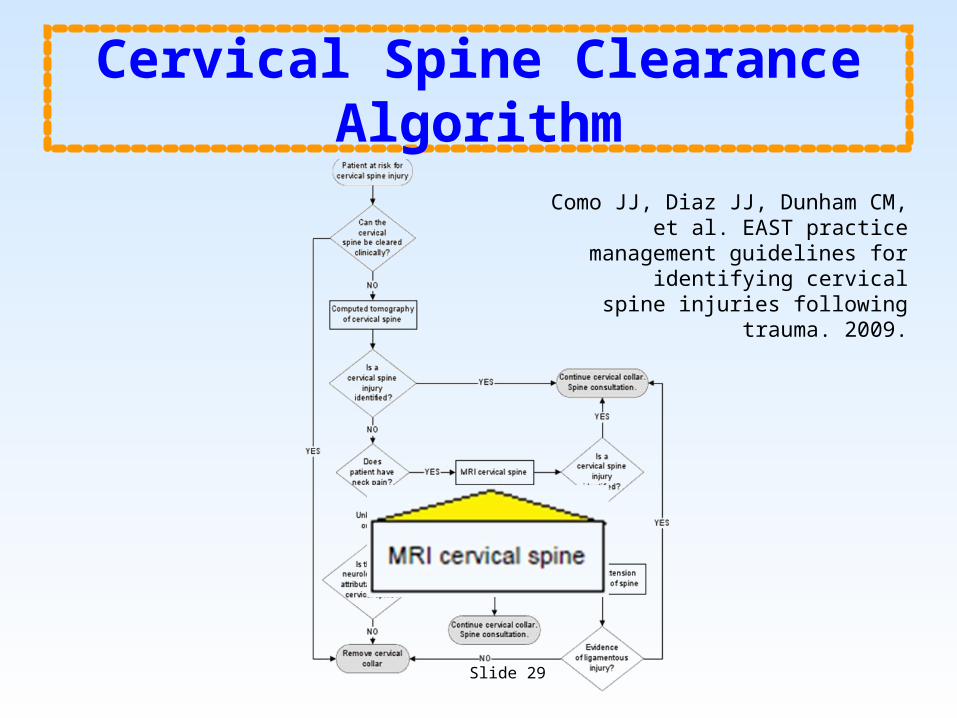
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for
identifying cervicalspine injuries following trauma. 2009.

Slide 30
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines
for identifying cervicalspine injuries following trauma. 2009.

Slide 31
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for
identifying cervicalspine injuries following trauma. 2009.

Slide 32
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for
identifying cervicalspine injuries following trauma. 2009.

Slide 33
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for
identifying cervicalspine injuries following trauma. 2009.

Slide 34
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines
for identifying cervicalspine injuries following trauma. 2009.

Slide 35
Cervical Spine Clearance Algorithm
Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for
identifying cervicalspine injuries following trauma. 2009.

Slide 36
Chest Wall
www.chelseagoodchild.com/images/portfolio/traditional/Rib_cage.jpg

Slide 37
Rib Fractures
• Overall mortality = 12%
• High-Energy Injuries:
– 1st or 2nd rib fractures
– Multiple rib fractures
– Scapula Fracture
• Rib Fractures in the Elderly (>65)
– 2 – 5 x greater risk of morbidity/mortality
– 19% Increase in mortality per rib fx
– 27% Increase in pneumoniaimage.wetpaint.com/image/1/
XOMgDfktBYZImgBWx3Xc2g171569/GW537H600
Slide 38
Rib Fractures
• Treatment = Analgesia
– PCA
– Rib Blocks
– Epidural
– Intercostal/ IntrapleuralCatheter
www.learningradiology.com/caseofweek/caseoftheweekpix2009-340/cow353-1lg.jpg

Slide 39
Flail Chest
• 2 ribs fractured in 2 locations
• Significant morbidity from underlying pulmonary contusions
• “Pendelluft”
• Treatment:
– Supplemental O2
– Analgesia
– Pulmonary Toilet
– ?Endotracheal Intubation
– ?Surgical Stabilizationupload.wikimedia.org/wikipedia/
commons/3/39/Flail_chest_mechaincs.jpg
Paradoxical Motion

Slide 40
Surgical Stabilization
• Studies suggest
– Quickly restores normal chest wall mechanics
– Less pain
– Decreased mortality
– Decreased mechanical ventilation needs
– Shorter hospital stays
– Decreased long term morbidity
www.acuteinnovations.com/files/ribloc-overview1.20090316-
1712.jpg
Gasparri MG, Almassi GH, Haasler GB (2003) Surgical management of multiple rib
fractures. Chest 124:295S

Slide 41
Suggested Indication for Surgical Treatment of Rib Fractures
• Flail chest
• Reduction of pain and
• disability
• Chest wall deformity/defect
• Symptomatic rib fracture non-union
• Thoracotomy for other indications
Raminder Nirula1, Jose J. Diaz Jr.2, Donald D. Trunkey3 and John C. Mayberry3. Rib
Fracture Repair: Indications, Technical Issues, and Future Directions. World Journal
of Surgery 2009; 33(1): 14-22

Slide 42
Sternal Fractures
• “Steering Wheel Syndrome”
• Possible Associated Injury = Blunt Cardiac Injury
• Most Common Associated Injuries:
– Rib fractures
– Long bone fractures
– Head injuries
• Treatment:
– Rest
– Analgesia
– Monitor for EKG changes
radiographics.rsna.org/content/21/5/1257/F42.medium.gif

Slide 43
Scapula Fractures
• From high energy trauma
• Rarely occur as an isolated injury
• Management:
– Sling
– Pendulum exercises at 3 weeks
– Strengthening at 6 weeks
www.eorthopod.com/sites/default/files/images/
adult_shoulder_fx_type_scapular_blade.jpg

Slide 44
Indications for Surgical Repair of Scapula Fractures
• If it is one of multiple shoulder fractures
• Displaced fracture of the glenoid neck
• Displaced fracture of the glenoid fossa
• Significant disruption of superior shoulder suspensory complex
www.ncbi.nlm.nih.gov/bookshelf/picrender.fcgi?
book=physmedrehab&part=A3412&blobname=ch4f4-30.jpg
Slide 45
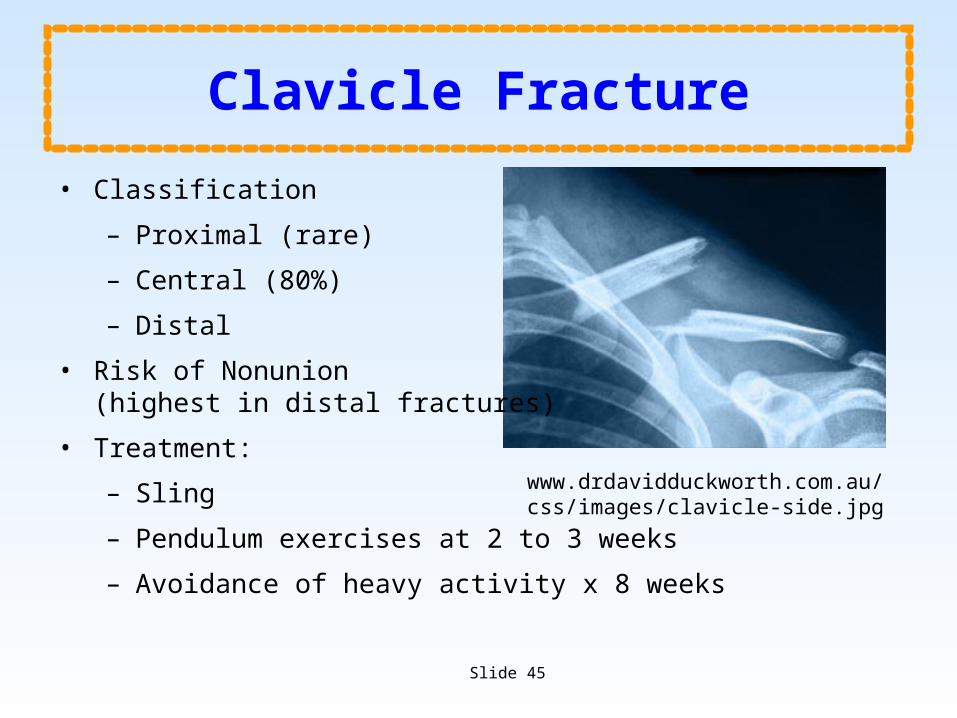
Clavicle Fracture
• Classification
– Proximal (rare)
– Central (80%)
– Distal
• Risk of Nonunion (highest in distal fractures)
• Treatment:
– Sling
– Pendulum exercises at 2 to 3 weeks
– Avoidance of heavy activity x 8 weeks
www.drdavidduckworth.com.au/css/images/clavicle-side.jpg

Slide 46
Clavicle Fractures
• Indications for surgical fixation:
– Distal clavicle
– Middle clavicle with >2cm of shortening
– Open
– Symptomatic Nonunions
– Associated neurovascular injury
– Complex injuries of the shoulder
• Surgical Procedure
– Screw and Plate Fixation
– Intramedullary implants
assets.sbnation.com/assets/161691/
clavicle_fracture_surgery_photo.gif
images.google.com/imgres?imgurl=http://
assets.sbnation.com/assets/161691
images.google.com/imgres?imgurl=http://assets.sbnation.com/
assets/161691

Slide 47
Pelvis
www.exchange3d.com/cubecart/images/uploads/aff973/Pelvis///Pelvis_thumb01.jpg

Slide 48
Pelvic Fractures
• Most Common Etiologies
– Motorcycle collisions
– Pedestrian v. Motor vehicle
– Fall > 15 feet
– Motor vehicle collision
• Mortality
– 7-14%
– 30% w/ severe or open fractures
– Most deaths due to other traumatic causes
• Concomitant Injuries in >90% of patients with pelvic fractures
• Most deaths due to:
– Head Injury
– Non-pelvic hemorrhage
– Lung Injury
– Thromboembolic Events
– MSOF
Slide 49
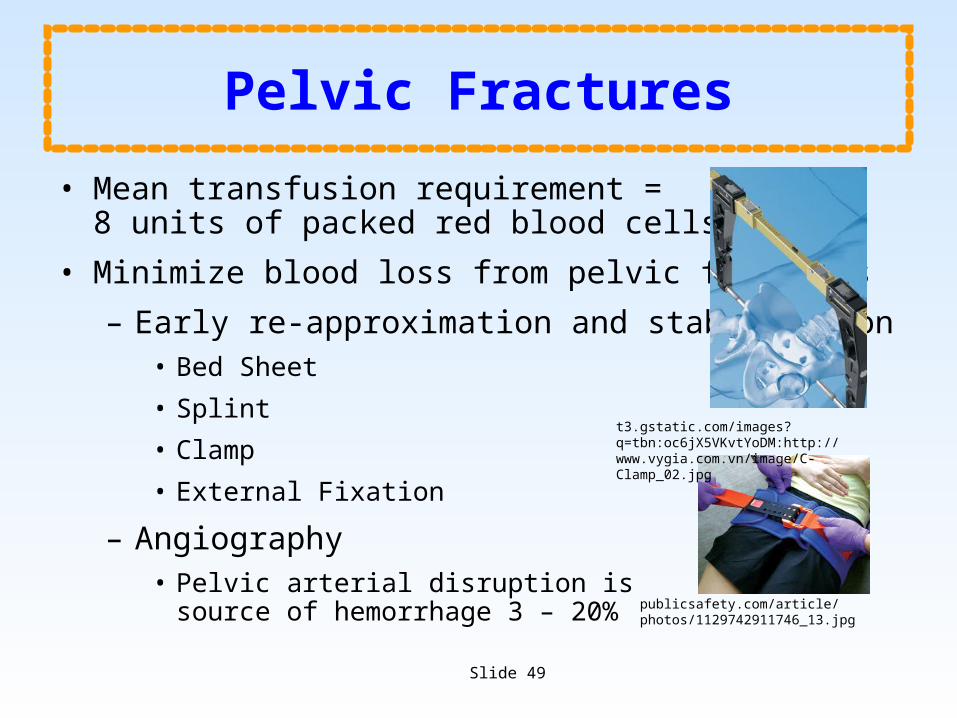
Pelvic Fractures
• Mean transfusion requirement = 8 units of packed red blood cells
• Minimize blood loss from pelvic fractures
– Early re-approximation and stabilization• Bed Sheet
• Splint
• Clamp
• External Fixation
– Angiography• Pelvic arterial disruption is
source of hemorrhage 3 – 20%
t3.gstatic.com/images?q=tbn:oc6jX5VKvtYoDM:http://www.vygia.com.vn/image/C-Clamp_02.jpg
publicsafety.com/article/photos/1129742911746_13.jpg

Slide 50
Pelvic Compression Fracture Vectors
• Lateral Compression
• Anterior-Posterior Compression
• Vertical Shear
images.google.com/imgres?imgurl=http://www.aofoundation.org/AOFileServerSurgery/
MyPortalFiles%3FFilePath%3D/Surgery/en/_img/surgery/01-Diagnosis/61/62-A1-xrays-

Slide 51
Lateral Compression Fracture
• Impact to lateral side of pelvic ring
• Shortens diameter across pelvis/decreases volume of pelvis
• Little risk of vascular or ligamentous injury
www.eorthopod.com/content/adult-pelvis-fractures-types

Slide 52
Anterior-Posterior Compression Fractures
• “Open Book”
• Mechanisms:
– Direct Impact to the Iliac Spines
– Transmitted through the femurs
• Can have ligamentous injury without fracture
• Increases diameter/volume of pelvis
• Significant risk of bleeding
• Unstable
www.eorthopod.com/sites/default/files/images/adult_pelvis_fx_causes06.jpg

Slide 53
Vertical Shear Pelvic Fractures
• Mechanism: Fall/Jump landing on straight leg
• Disruption of ligaments:
– Symphyseal
– Sacrospinous
– Sacrotuberous
– SI
– Increases Diameter/Volume of Pelvis
• Less bleeding than A-P fractures, but still significant risk
www.eorthopod.com/content/adult-pelvis-fractures-types

Slide 54
Upper Extremity
www.buyamag.com/graphics/arm_ue200.jpg

Slide 55
Shoulder Fractures/Dislocations
• Acromioclavicular dislocation
– “Shoulder Separation”
– Mechanism: fall onto acromion
– Involved ligaments:• Acromioclavicular ligament
• Coracoclavicular ligament
– Complications:• Risk of Brachial Plexus Injury
• Risk of Subclavian Vessel Injury
– Treatment: Sling
www.jurewitz.com/upload/shoulder_acromioclavicular_separ
ation_intro01.jpg

Slide 56
Shoulder Fractures/Dislocations
• Floating Shoulder
– Glenoid neck fracture + Clavicle fracture
– Glenohumeral joint without attachment to the rest of the skeleton
– Usually requires surgical fixation of one of the elements (clavicle)
Low CK, Lam AWM. Results of fixation of clavicle alone in managing floating shoulder. Singapore Med .
2000;4(19):452-453.

Slide 57
Shoulder dislocation
• Anterior (85-95%)
– Risk of axillary nerve injury
– Treatment: Closed Reduction
• Posterior
– Mechanisms: Seizures, Electrocution
– Risk of axillary artery injury
– Treatment: Closed Reduction
http://www.sports-injury-info.com/image-files/shoulder-dislocation.jpg
www.eorthopod.com/images/ContentImages/shoulder/shoulder_dislocation/shoulder_dislocation_anatomy12.jpg

Slide 58
Humerus FracturesProximal Humerus Fractures
• Concomitant injuries:
– Rotator cuff injuries
– Shoulder dislocation
• Risk of peripheral nerve injuries
• Risk of axillary artery injury
• Nondisplaced Fractures
– Sling for a short period
– Early Range Of Motion
• Displaced Fractures
– With impaction of humeral head: Nonop
– Most 2 Part Fractures: Closed reduction w/ percutaneous fixation
– Most 3 Part Fractures: ORIF
www.shouldersurgeon.com/graphics/
4_parts_prox_humerus.jpg

Slide 59
Humerus Fractures
• Midshaft Humerus Fractures
– Radial Nerve Injury• 12% of Humeral Shaft Fractures
• with fractures of the distal 1/3 of the Humerus
• Runs in the spiral groove
• 70% resolve w/ conservative management
• Splint wrist and digits
– Nondisplaced: Sling
– Displaced: • Reduction with long arm cast for gravity traction
• Fracture Brace
• Plate and Screw Fixation
• Intramedullary Nailing
www.eorthopod.com/sites/default/files/images/adult_humeral_fx_brace.jpg

Slide 60
Humerus Fractures
Supracondylar Humerus Fractures
• Almost always require ORIF
• Volkmann’s Contracture
– Supracondylar Humerus Fracture
– Anterior interosseus artery is occluded
– After reduction, perfussion is restored
– Reperfussion injury leads to Flexor Compartment Syndrome
www.unboundedmedicine.com/wp-content/Volkman.jpg
Slide 61
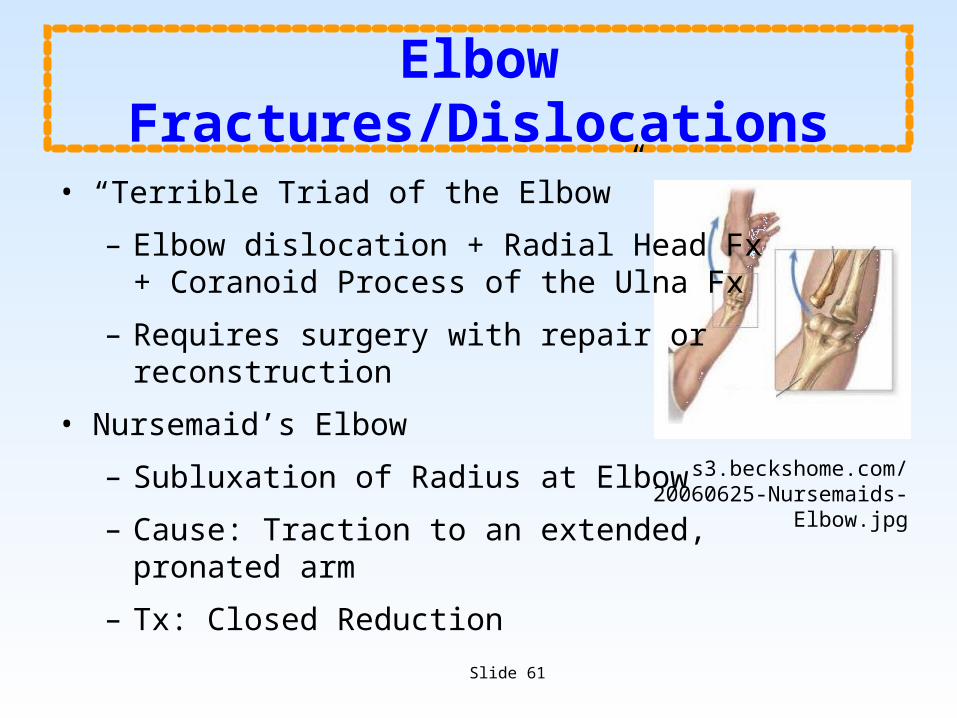
Elbow Fractures/Dislocations
• “Terrible Triad of the Elbow”
– Elbow dislocation + Radial Head Fx+ Coranoid Process of the Ulna Fx
– Requires surgery with repair or reconstruction
• Nursemaid’s Elbow
– Subluxation of Radius at Elbow
– Cause: Traction to an extended, pronated arm
– Tx: Closed Reduction
s3.beckshome.com/20060625-Nursemaids-Elbow.jpg

Slide 62
Forearm Fractures
• Monteggia Fracture
– Proximal Ulna Fracture + Radial Head Dislocation
– Treatment ORIF
• Galezzi Fracture-Dislocation
– Complex disruption of the distal radioulnar joint + Unstable radius fracture
– Surgical repair is almost always necessary
www.wheelessonline.com/images/i1/mont1.jpg
www.learningradiology.com/caseofweek/caseoftheweekpix2/
cow157lg.jpg

Slide 63
Forearm Fractures
• Night-stick Fracture
– Isolated Ulnar Shaft Fracture
– Nondisplaced: Long arm cast for short period, then functional bracing
– Displaced: Compression Plating
• Colles Fracture
– Fall on outstretched, extended wrist
– Distal Radius Fracture
– Treatment: Closed Reduction
• Greenstick fracture
– Partially through bone
– Opposite side of bone bent
www.wheelessonline.com/image4/i1/nght1.jpg
z.about.com/d/orthopedics/1/0/2/1/fxapcolles.jpg
www.medscape.com/content/2002/00/44/65/446548/art-ar446548.fig10.jpg

Slide 64
Scaphoid Fracture
• ½ of all isolated carpal bone fractures
• Fracture locations:
– Waist (75%)
– Proximal Pole (20%)
– Distal Pole (5%)
– Blood supply from the ligaments at the distal pole
• Snuff Box tenderness
• Risk of Avascular Necrosis
• Operative Repair
– Open Screw Placement
– Percutaneous Screw Placement
• Cast to elbow
patientsites.com/media/img/1225/wrist_scaphoid_fracture_intro01.jpg

Slide 65
Finger/Thumb Fractures
• Rolando fracture
– T- or Y-shaped
– Thumb metacarpal base
– Difficult to manage
• Phalangeal fractures
– Usual treatment: Buddy taping or splint immobilization
– Intra-articular invovlement:
• Closed reduction
• Fixation with percutaneous screws
• Fixation with Kirschner wires
radiographics.rsnajnls.org/content/vol20/issue3/images/
large/g00mc20l25x.jpeg

Slide 66
Lower Extremity
files.turbosquid.com/Preview/Content_2009_07_13__17_30_11/leg_bones.jpgf1dbe04a-ce4d-4150-
9fc1-0fb1043c8a87Large.jpg

Slide 67
Femur Fracture
• Present in about 15% of seriously injured trauma patients
• 8-10% Bilateral
• Mortality
– Unilateral = 10-12%• 20% in patients > 65 years old
– Bilateral = 26-33%
– 90% due to concomitant injuries
• Decreased complications with surgical fixation within 24 hours

Slide 68
Hip Fractures
• 50% over 85years
– 6 month mortality of 20%
• Preoperative Management of Unstable Fxs
– Buck’s Traction
– Skeletal Tractionwww.lancastergeneralcollege.edu/content/upload/
AssetMgmt/images/College/conferences/Ortho_Traction_in_OrthopedicCare.pdf

Slide 69
Hip Fractures
Femoral Neck Fractures
• Intracapsular
– High risk of Avascular Necrosis and Nonunion
– Intracapsular hematoma also may compromise perfusion
– Surgical emergency in young people
– Treatments:
• Internal fixation
• Hip arthroplasty
• Extracapsular
– Dynamic Hip Screw (DHS)
– Early weight bearing/Rehabwww.orthomeditec.com/images/
dynamichipscrew.jpg

Slide 70
Hip Fractures
• Trochanteric Fractures
– More stable than femoral neck fractures
– Require ORIF• Early Ambulation/Rehab
• Subtrochanteric Fractures
– High risk of failure of surgical fixation
– Treatments:• ORIF
• Closed Reduction and Intramedullary Nailing
• Indirect reduction with blade-plate /screw-plate fixation

Slide 71
Hip Dislocations
• Reduction within 6 to 8 hours is crucial
• Posterior (85-95%)
– Leg internally rotated and adducted
– Risk of sciatic nerve injury
– Treatment: Closed Reduction
• Anterior
– Leg externally rotated and abducted
– Risk of femoral artery injury
– Treatment: Closed Reduction i21.photobucket.com/albums/b286/flagady15/Bones/hip-fig1.jpg
chestofbooks.com/health/anatomy/Human-Body-Construction/images/Fig-515-Posterior-luxation-of-
the-hip-produced-by-rotati.jpg

Slide 72
Femoral Shaft Fractures
• Blood loss up to 1500 – 2000cc
• Important to reduce fracture and maintain alignment early
• Closed Reduction and Reamed, Interlocking Intramedullary Nail
• Ex-fix with Intramedullary Nail
– Days 5 to 10
• Associated Complications:
– Fat Embolism Syndrome
– Acute Lung Injury/ARDS
nyic.stemlegal.com/wp-content/uploads/2009/01/femur-nailing.jpg

Slide 73
Patella Fractures
• Mechanism: Direct blow to flexed knee
• Nondisplaced: Long leg cast
• Comminuted:
– Open reduction and internal fixation
• Lag screws
• Tension Banding
– Partial or total Patellectomy
www.cahnlitigation.com/toetheslab/images/Post%20Images/fracture_of_patella_2.JPG
www.aofoundation.org/AOFileServerSurgery/
MyPortalFiles?
www.aofoundation.org/AOFileServerSurgery/MyPortalFiles?FilePath=/Surgery/en/_img/surgery/05-RedFix/34/P90-
tension-band-wiring/33_P90_i480L_C11_patella.jpg

Slide 74
Knee Dislocation
• May involve:
– Patello-femoral joint
– Tibio-femoral joint
• Usually Lateral
– Hemarthrosis or Effusion develops
– May be recurrent
– Treatment:• Closed Reduction
• Knee immobilization for 4 to 6 weeks
• Complete Knee Dislocation:
– Anterior or Posterior
– Need angiogram to assess for Popliteal Artery injury
www.ajronline.org/content/vol186/issue3/images/large/00_04_0756_04b_cmyk.jpeg

Slide 75
Tibia-Fibula Fractures
• Proximal and Midshaft Tibia Fractures
– High risk for compartment syndrome
• Tibial Plateau Fractures
– Nondisplaced proximal tibia fractures: hinged knee brace
– Displaced/Unstable patient: External fixator
– Deformity/Instability: Surgical Repair
www.rad.washington.edu/academics/academic-sections/msk/teaching-materials/sundry-msk-
computer-programs/sundry-images-for-programs/3DCTS1_3DAP.jpg/image
Slide 76
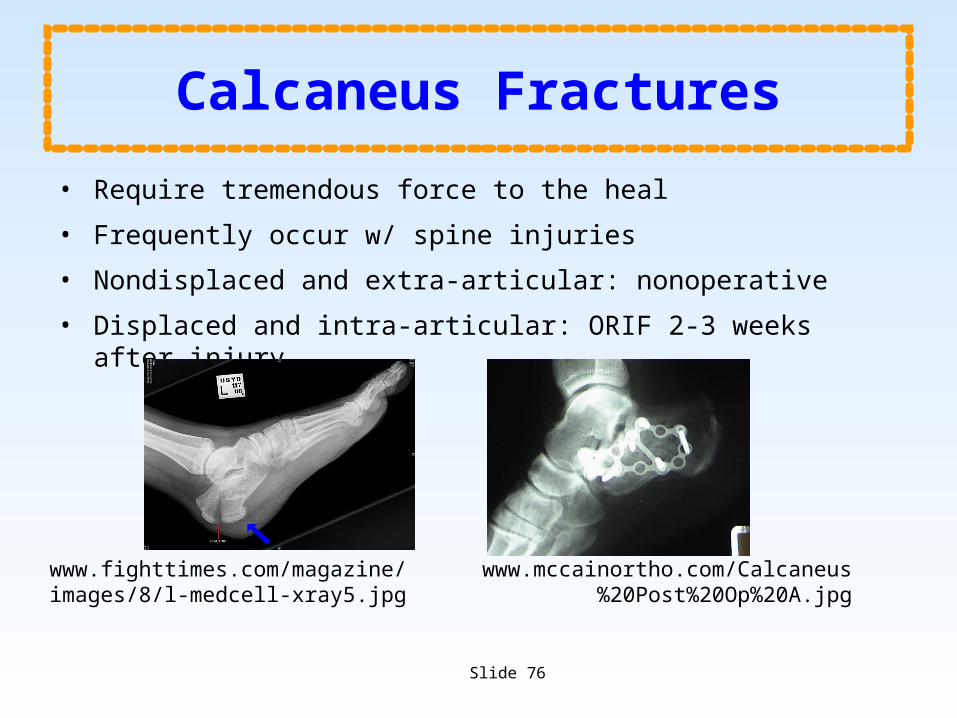
Calcaneus Fractures
• Require tremendous force to the heal
• Frequently occur w/ spine injuries
• Nondisplaced and extra-articular: nonoperative
• Displaced and intra-articular: ORIF 2-3 weeks after injury
www.fighttimes.com/magazine/images/8/l-medcell-xray5.jpg
www.mccainortho.com/Calcaneus%20Post%20Op%20A.jpg
Slide 77
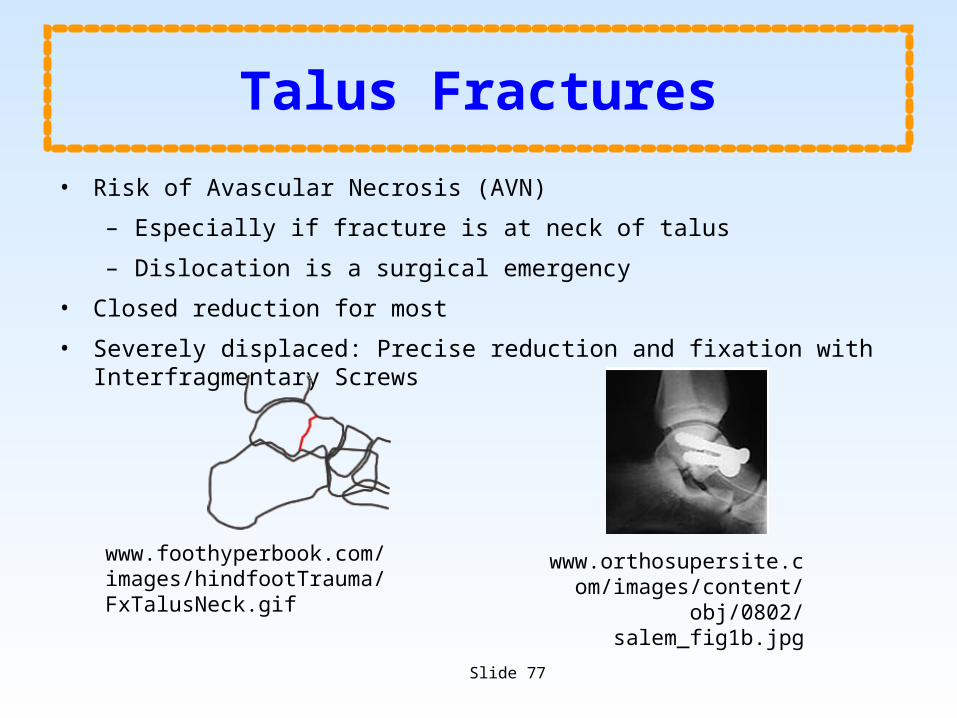
Talus Fractures
• Risk of Avascular Necrosis (AVN)
– Especially if fracture is at neck of talus
– Dislocation is a surgical emergency
• Closed reduction for most
• Severely displaced: Precise reduction and fixation with Interfragmentary Screws
www.foothyperbook.com/images/hindfootTrauma/FxTalusNeck.gif
www.orthosupersite.com/images/content/obj/0802/
salem_fig1b.jpg

Slide 78
Metatarsal Fractures
• Jones Fracture
– Mechanism: Inversion of Foot
– 5th Metatarsal
– At risk for nonunion
www.eorthopod.com/content/adult-foot-fractures-types
www.eorthopod.com/content/adult-foot-fractures-types

Slide 79
Complications of Extremity Fractures
• Infection
– Findings often appear 10-21 days after infection
– Most common organism = Staph. aureus
– Also common = Pseudomonas aeruginosa and Enterobacteriaceae
• Diagnosis
– Physical findings
– Constitutional symptoms
– Radiography• CT
• MRI
• 3-phase bone scan
• Radiolabeled WBC scan

Slide 80
Complications of Extremity Fractures
• Gas Gangrene
• Necrotizing fasciitis
• Treatment:
– Early wide debridement
– Antibiotics (PCN)
• Tetanus
– Highest risk w/ farming accidents
– Treatment:• Supportive
• Debridement
• Immunization
• Antibiotics
amog.com/wp-content/uploads/
2009/03/fasciitis.jpg
www.meddean.luc.edu/lumen/MedEd/mech/cases/Gram_Positive/
slide1.jpg
www2.cedarcrest.edu/academic/bio/hale/bioT_EID/lectures/tetanus-pathogen2.jpg

Slide 81
Osteomyelitis
• Acute Osteomyelitis
– Hematogenous Spread
– Contiguous Spread
• Subacute Osteomyelitis
• Chronic Osteomyelitis
ssl.gstatic.com/health/33576cb3c325418b82afc7245394d485/
ref/graphics/9712.jpg

Slide 82
Diagnosis of Osteomyelitis
• Requires 2 of the 4 following criteria:
• Purulent material on aspiration of affected bone
• Bone tissue or blood culture positive
• Localized classic physical findings of bony tenderness, with overlying soft-tissue erythema or edema
• Positive radiological imaging study www.medical-look.com/diseases_images/osteomyelitis.jpg

Slide 83
Osteomyelitis
Most Common Organisms
• Staphylococcus aureus
• Gram negative infections (vertebral bodies)
• Pseudomonas (IVDA)
• Fungal osteomyelitis (chronicallyill/TPN)
• Salmonella osteomyelitis (Sickle Cell Disease)
• Group B streptococcus (Infants 2-4 weeks old)
• Haemophilus influenzae (6 months to 4 years old)
upload.wikimedia.org/wikipedia/commons/5/59/Ostermyelitis_Tibia.jpg

Slide 84
Osteomyelitis
• Treatment:
• Surgical Debridement
• ? Limb Loss
• Antibiotics
– Broad Spectrum IV
– Tissue cultures to narrow
• Hyperbaric Oxygen for Refractory Osteomyelitis
radiographics.rsna.org/.../g07nv10c18x.jpeg
Kindwall EP. Uses of hyperbaric oxygen therapy in the 1990s. Cleve Clin J Med. Sep-Oct 1992;59(5):517-28

Slide 85
Complications of Extremity Fractures
• Fat Embolism
– Approx. 5000 deaths per year
– Classic Triad:
• Respiratory Compromise
• Change in Mental Status
• Petechiae
– Half of all cases present only with respiratory failure
– Treatment: Supportive
img.medscape.com/pi/emed/ckb/vascular_surgery/459840-459841-
460524-1723668tn.jpg
www.futurehealth.rochester.edu/dlp2/dlpdict/petechiae.jpg

Slide 86
Thromboembolism
• Virchow’s Triad:
– Hypercoagulability
– Endothelial Damage
– Venous Stasis
• More than 60% of DVTs are Asymptomatic
• PEs are the 3rd most common cause of death in trauma patients who survive past the first day
• DVT Prophylaxis:
• SCDs
• Foot pumps
– Heparin
• LMWH
• Coumadin

Slide 87
Complications of Extremity Fractures
Compartment Syndrome
• Diagnosis primarily clinical
– Pain
– Parasthesias
– Piokylothermia
– Pulseless
– Pain with passive range of motion
• Critical Pressures:
– Compartment Pressure > 30mmHg
– Diastolic BP – Compartment Pressure < 30mmHg
Slide 88
Complications of Extremity Fractures
• Rhabdomyolysis
– Treatment = aggressive IVF
• Avoid buildup of myoglobin in renal tubules
• Prevent hyperkalemia

Slide 89
Image Sources
• ajs.sagepub.com/content/32/4/1059/F1.large.jpg
• amog.com/wp-content/uploads/2009/03/fasciitis.jpg
• anatpat.unicamp.br/minDsc35446+.jpg
• assets.sbnation.com/assets/161691/clavicle_fracture_surgery_photo.gif
• chestofbooks.com/health/anatomy/Human-Body-Construction/images/Fig-515-Posterior-luxation-of-the-hip-produced-by-rotati.jpg
• Como JJ, Diaz JJ, Dunham CM, et al. EAST practice management guidelines for identifying cervical spine injuries following trauma. 2009.
• eldoradopainmanagement.net/mediac/450_0/media/Compression_Render_Final.jpg
• files.turbosquid.com/Preview/Content_2009_07_13__17_30_11/leg_bones.jpgf1dbe04a-ce4d-4150-9fc1-0fb1043c8a87Large.jpg
• Gasparri MG, Almassi GH, Haasler GB (2003) Surgical management of multiple rib fractures. Chest 124:295S

Slide 90
Image Sources• georgiahealthinfo.gov/cms/files/global/images/image_popup/
fsm7_compartmenttesting.jpg• herkules.oulu.fi/isbn9514270959/html/graphic33.png• Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule
out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography UtilizationStudy Group. N Engl J Med. 2000;343:94 –99.
• i21.photobucket.com/albums/b286/flagady15/Bones/hip-fig1.jpg• image.absoluteastronomy.com/images/encyclopediaimages/b/bl/
blackeye_pigmentation.jpg• image.wetpaint.com/image/1/XOMgDfktBYZImgBWx3Xc2g171569/GW537H600• images.allegrocentral.com/9E/75/J-Tongs-Traction-Tongs-557879-PRODUCT-
MEDIUM_IMAGE.jpg• images.google.com/imgres?imgurl=http://assets.sbnation.com/assets/161691• images.google.com/imgres?imgurl=http://www.aofoundation.org/
AOFileServerSurgery/

Slide 91
Image Sources• MyPortalFiles%3FFilePath%3D/Surgery/en/_img/surgery/01-Diagnosis/61/62-A1-
xrays-• img.medscape.com/pi/emed/ckb/orthopedic_surgery/1230552-1267150-1299.jpg• img.medscape.com/pi/emed/ckb/radiology/336139-343764-9928.jpg• img.medscape.com/pi/emed/ckb/vascular_surgery/459840-459841-460524-
1723668tn.jpg• Kindwall EP. Uses of hyperbaric oxygen therapy in the 1990s. Cleve Clin J Med. Sep-
Oct 1992;59(5):517-28• Low CK, Lam AWM. Results of fixation of clavicle alone in managing floating
shoulder. Singapore Med . 2000;4(19):452-453. • nyic.stemlegal.com/wp-content/uploads/2009/01/femur-nailing.jpg• patientsites.com/media/img/1225/wrist_scaphoid_fracture_intro01.jpg• Pirouzmand F, Muhajarine N. Craniofac Surg. 2008 Jan;19(1):27-36. Definition of
topographic organization of skull profile in normal population and its implications on the role of sutures in skull morphology.
• publicsafety.com/article/photos/1129742911746_13.jpg
www.istockphoto.com/file_thumbview_approve/843463/2/istockphoto_843463-skeleton-with-edge-of-blank-sign-includes-clipping-path.jpg

Slide 92
Image Sources• radiographics.rsna.org/.../g07nv10c18x.jpeg• radiographics.rsnajnls.org/content/vol20/issue3/images/large/g00mc20l25x.jpeg• radiographics.rsna.org/content/21/5/1257/F42.medium.gif• Raminder Nirula1, Jose J. Diaz Jr.2, Donald D. Trunkey3 and John C. Mayberry3. Rib
Fracture Repair: Indications, Technical Issues, and Future Directions. World Journal of Surgery 2009; 33(1): 14-22
• s3.beckshome.com/20060625-Nursemaids-Elbow.jpg• ssl.gstatic.com/health/33576cb3c325418b82afc7245394d485/ref/graphics/9712.jpg• t0.gstatic.com/images?q=tbn:TuEw6pvP4iIG5M:http://img.medscape.com/pi/emed/
ckb/neurosurgery/247017-248108-4155.jpg• t3.gstatic.com/images?q=tbn:oc6jX5VKvtYoDM:http://www.vygia.com.vn/image/C-
Clamp_02.jpg• Textbook of Critical Care. Fink MP, Abraham E, Vincent JL, Kochanek P (ed) 5th• ed : Philadelphia : Elsevier Saunders, 2005• Trauma, 4th edMattox KL, Feliciano DV, Moore EE, eds. New York, NY: McGraw-Hill,
2000

Slide 93
Image Sources• upload.wikimedia.org/wikipedia/commons/6/61/Pulmonary_embolism.jpg
• upload.wikimedia.org/wikipedia/commons/3/39/Flail_chest_mechaincs.jpg
• upload.wikimedia.org/wikipedia/commons/5/59/Ostermyelitis_Tibia.jpg
• www2.cedarcrest.edu/academic/bio/hale/bioT_EID/lectures/tetanus-pathogen2.jpg
• www.acuteinnovations.com/files/ribloc-overview1.20090316-1712.jpg
• www.alsab.ca/images/collar2.jpg
• www.ajronline.org/content/vol186/issue3/images/large/00_04_0756_04b_cmyk.jpeg
• www.aofoundation.org/AOFileServerSurgery/MyPortalFiles?
• www.aofoundation.org/AOFileServerSurgery/MyPortalFiles?FilePath=/Surgery/en/_img/surgery/05-RedFix/34/P90-tension-band-wiring/33_P90_i480L_C11_patella.jpg
• www.backpainguide.com/Chapter_Fig_folders/Ch15_Carpentry_Folder/Ch15_Images/15_3_Pedicle_Screws.jpg

Slide 94
Image Sources• www.buyamag.com/graphics/arm_ue200.jpg• www.cahnlitigation.com/toetheslab/images/Post%20Images/
fracture_of_patella_2.JPG• www.chelseagoodchild.com/images/portfolio/traditional/Rib_cage.jpg• www.drdavidduckworth.com.au/css/images/clavicle-side.jpg• www.eorthopod.com/images/ContentImages/shoulder/shoulder_dislocation/
shoulder_dislocation_anatomy12.jpg• www.eorthopod.com/images/ContentImages/spine/spine_thoracic/anatomy/
thoracic_spine_anatomy01.jpg• www.eorthopod.com/sites/default/files/images/adult_femur_fx_intro01.jpg• www.eorthopod.com/sites/default/files/images/adult_humeral_fx_brace.jpg• www.eorthopod.com/sites/default/files/images/
adult_shoulder_fx_type_scapular_blade.jpg• www.exchange3d.com/cubecart/images/uploads/aff973/Pelvis///Pelvis_thumb01.jpg• www.fighttimes.com/magazine/images/8/l-medcell-xray5.jpg

Slide 95
Image Sources• www.foothyperbook.com/images/hindfootTrauma/FxTalusNeck.gif
• www.futurehealth.rochester.edu/dlp2/dlpdict/petechiae.jpg
• www.hawaii.edu/medicine/pediatrics/pemxray/v5c09h2.jpg
• www.istockphoto.com/file_thumbview_approve/843463/2/istockphoto_843463-skeleton-with-edge-of-blank-sign-includes-clipping-path.jpg
• www.itim.nsw.gov.au/images/Battle_Sign_s.jpg
• www.jurewitz.com/upload/shoulder_acromioclavicular_separation_intro01.jpg
• www.lancastergeneralcollege.edu/content/upload/AssetMgmt/images/College/conferences/Ortho_Traction_in_OrthopedicCare.pdf
• www.learningradiology.com/caseofweek/caseoftheweekpix2009-340/cow353-1lg.jpg
• www.learningradiology.com/caseofweek/caseoftheweekpix2/cow157lg.jpg
• www.mccainortho.com/Calcaneus%20Post%20Op%20A.jpg

Slide 96
Image Sources
• www.meddean.luc.edu/lumen/MedEd/mech/cases/Gram_Positive/slide1.jpg
• www.medical-look.com/diseases_images/osteomyelitis.jpg
• www.medscape.com/content/2002/00/44/65/446548/art-ar446548.fig10.jpg
• www.motiondust.com/visualization/pelvis.jpg
• www.ncbi.nlm.nih.gov/bookshelf/picrender.fcgi?book=physmedrehab&part=A3412&blobname=ch4f4-30.jpg
• www.nuclearonline.org/newsletter/Images/Osteo2.jpg
• www.optecusa.com/sites/default/files/imagecache/product_list/products_01_B09.jpg
• www.orthomeditec.com/images/dynamichipscrew.jpg
• www.orthosupersite.com/images/content/obj/0802/salem_fig1b.jpg
• www.ossur.com/lisalib/getfile.aspx?itemid=15083&proc=3

Slide 97
Image Sources• www.pgblazer.com/wp-content/uploads/2009/11/three-column-concept-2.jpg• www.physiotherapy-treatment.com/images/human-lateral-cervical-spine.jpg• www.pycomall.com/images/P/skeleton.jpg• www.pycomall.com/images/P/skull.jpg• www.rad.washington.edu/academics/academic-sections/msk/teaching-materials/
sundry-msk-computer-programs/sundry-images-for-programs/3DCTS1_3DAP.jpg/image
• www.springerlink.com/content/26ghau7p5nmpcjle/• www.umm.edu/spinecenter/education/images/vertebra.jpg• www.unboundedmedicine.com/wp-content/Volkman.jpg• www.vancouverspinedoctor.com/images/balloon_kyphoplasty.jpg• www.webinique.com/images/lumbar_spondylolisthesis_grades.jpg• www.wheelessonline.com/image4/i1/nght1.jpg• www.wheelessonline.com/images/i1/mont1.jpg• z.about.com/d/orthopedics/1/0/2/1/fxapcolles.jpg


















