Skeletal muscle must watch
74
SKELETAL MUSCLE Smoking is injurious to health Rakesh kumar 1
-
Upload
rakesh89540 -
Category
Education
-
view
224 -
download
0
Transcript of Skeletal muscle must watch
1
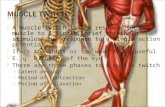
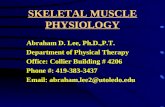
SKELETAL MUSCLE
Smoking is injurious to health
Rakesh kumar
2
Introduction Classification Microscopic structure Physiology Applied Anatomy References
Protocol
3 Introduction
MUSCULUS = LITTLE MOUSE
Muscle tissue is the one of the basic tissues of the body.
Responsible for movement .
Composed of differentiated cells containing contractile proteins(actin, myosin etc.)
4 Muscles – machines - chemical energy - mechanical energy.
40-50% of the body mass.
Attaches to bone, skin or fascia
Developed from MESODERM except a)Arrector pili b)Muscles of iris c)Myoepithelial cells of sweat ,salivary and lacrimal glands -
ECTODERM
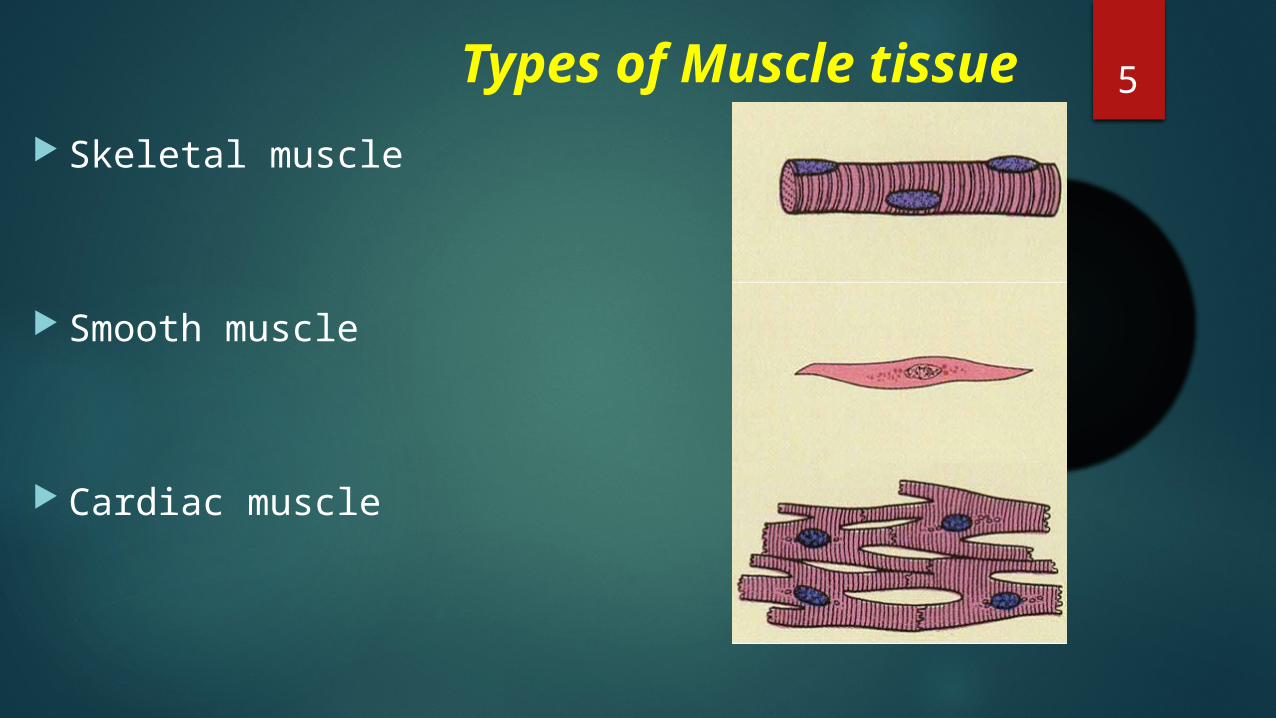
5 Types of Muscle tissue Skeletal muscle
Smooth muscle
Cardiac muscle
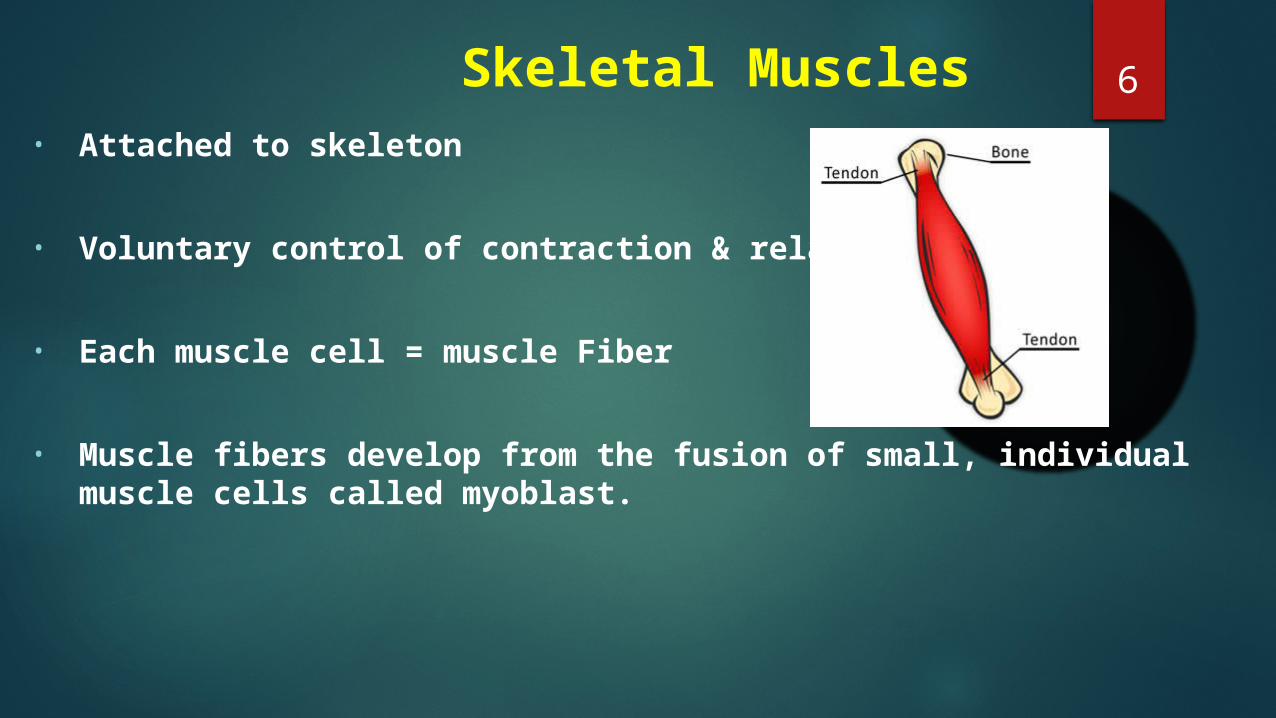
6 Skeletal Muscles• Attached to skeleton
• Voluntary control of contraction & relaxation
• Each muscle cell = muscle Fiber
• Muscle fibers develop from the fusion of small, individual muscle cells called myoblast.
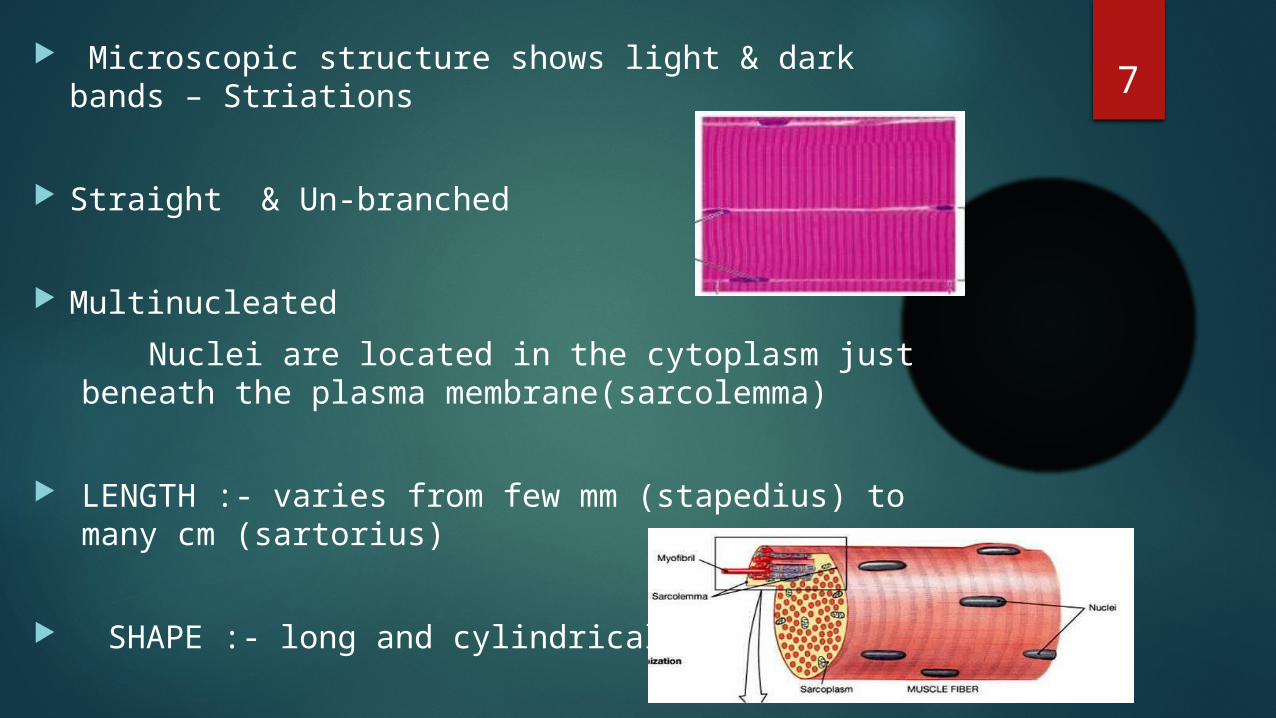
7 Microscopic structure shows light & dark bands –
Striations
Straight & Un-branched
Multinucleated Nuclei are located in the cytoplasm just beneath the
plasma membrane(sarcolemma)
LENGTH :- varies from few mm (stapedius) to many cm (sartorius)
SHAPE :- long and cylindrical
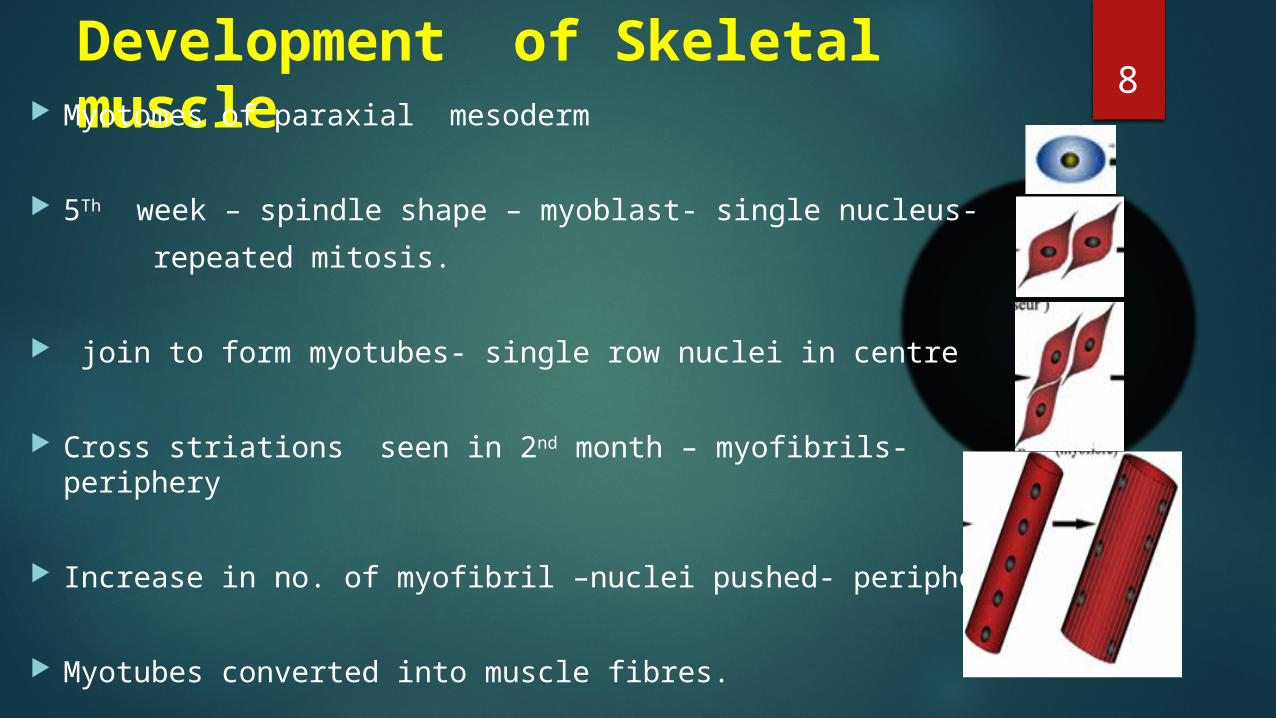
8Development of Skeletal muscle Myotomes of paraxial mesoderm
5Th week – spindle shape – myoblast- single nucleus- repeated mitosis.
join to form myotubes- single row nuclei in centre
Cross striations seen in 2nd month – myofibrils-periphery
Increase in no. of myofibril –nuclei pushed- periphery
Myotubes converted into muscle fibres.
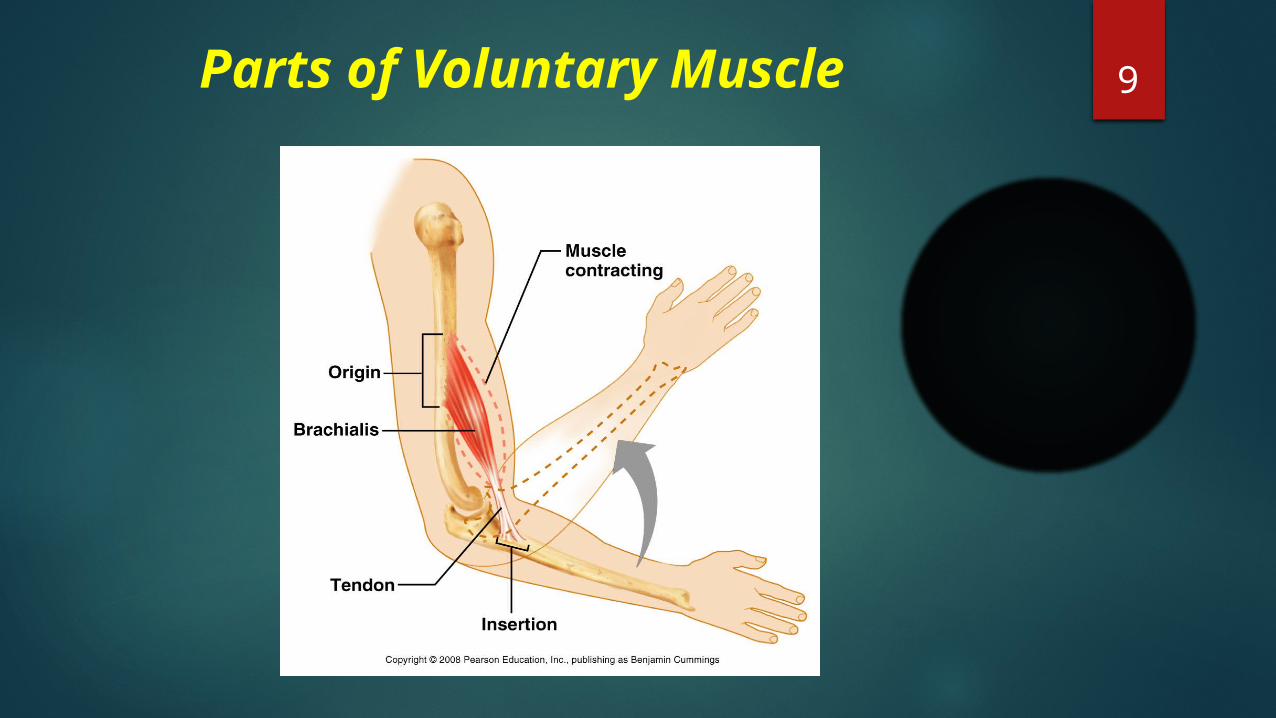
9 Parts of Voluntary Muscle
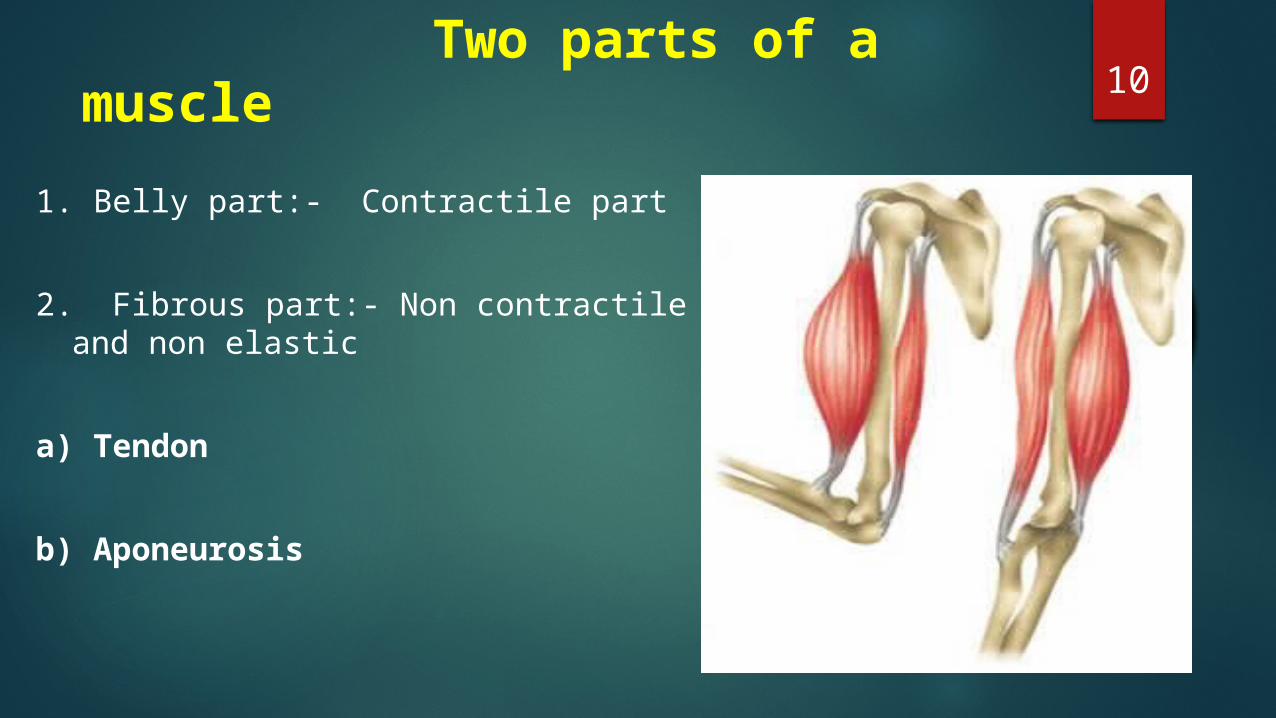
10 Two parts of a muscle
1. Belly part:- Contractile part
2. Fibrous part:- Non contractile and non elastic
a) Tendon
b) Aponeurosis
11 Classification According to colour
According to Insertion of muscle
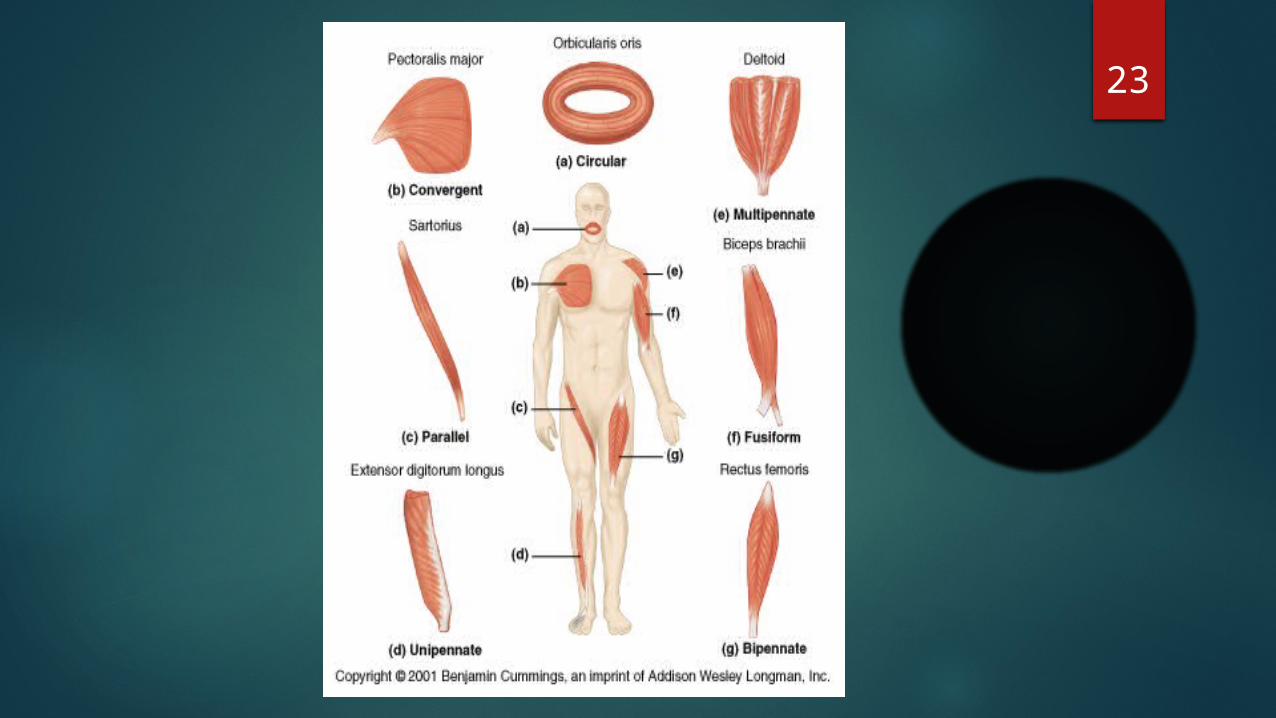
According to direction of muscle fibre - Parallel - Pennate - Spiral - Cruciate
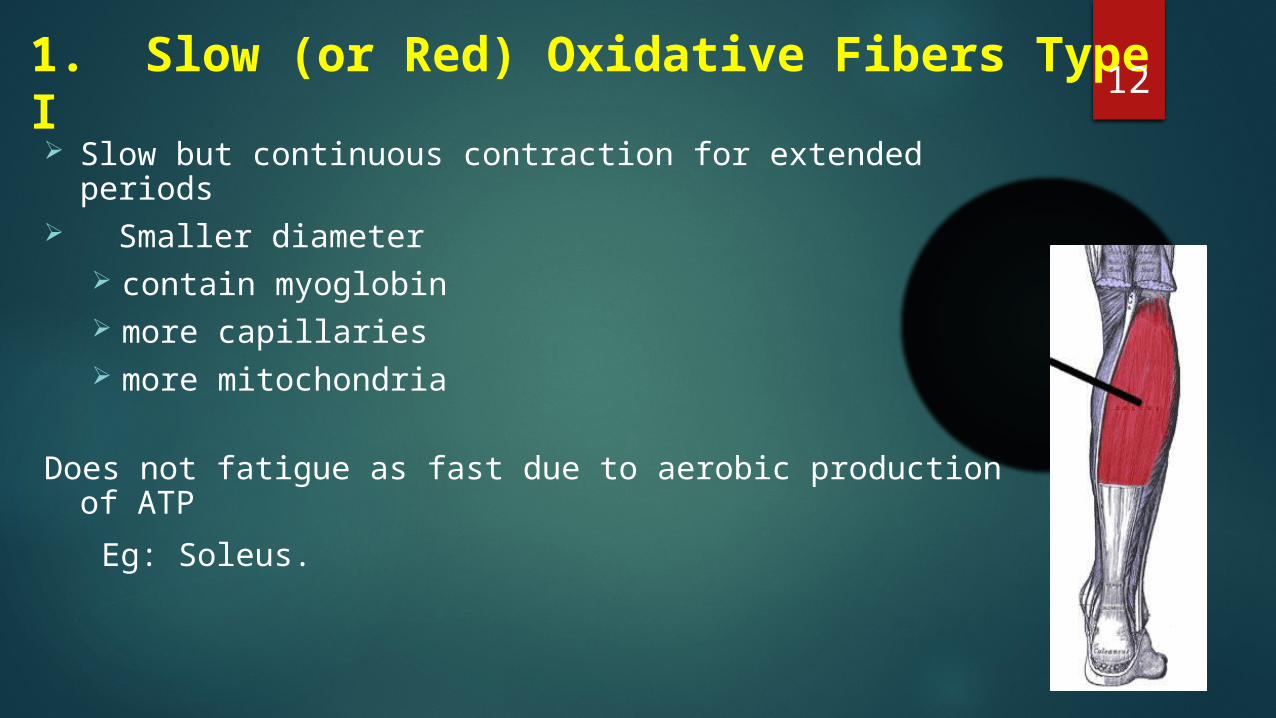
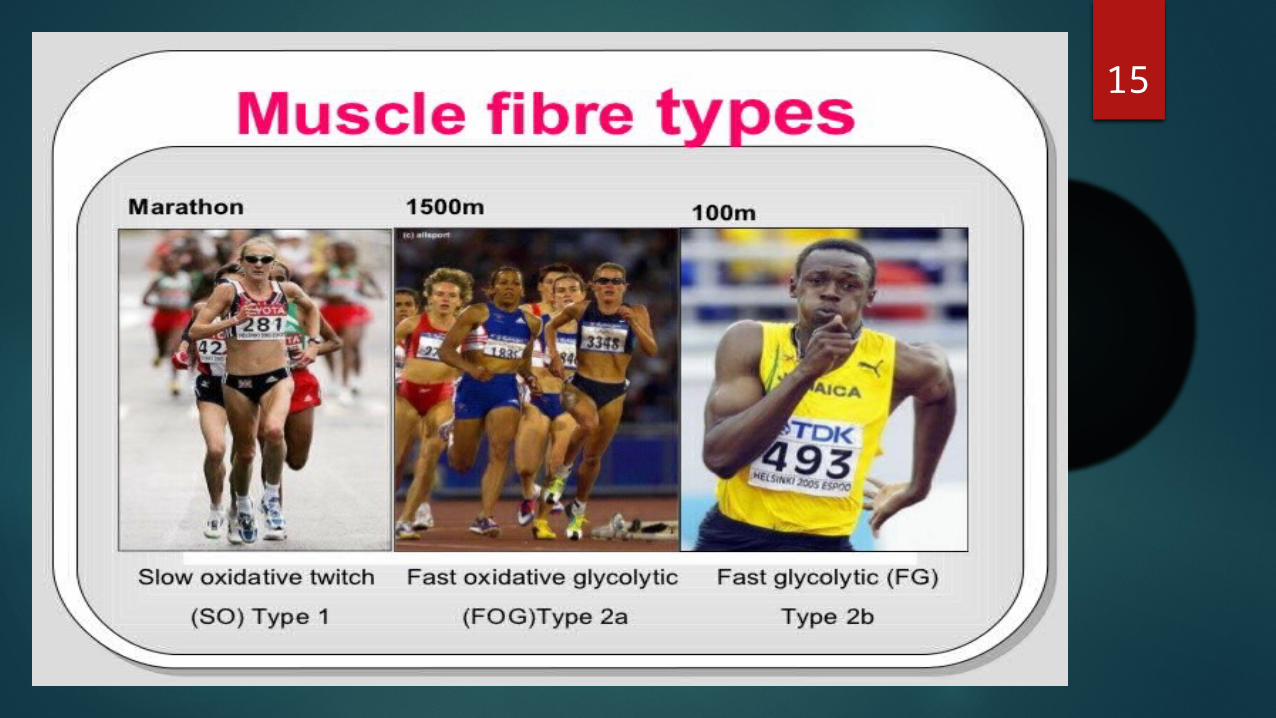
121. Slow (or Red) Oxidative Fibers Type I Slow but continuous contraction for extended periods
Smaller diameter
contain myoglobin more capillaries more mitochondria
Does not fatigue as fast due to aerobic production of ATP Eg: Soleus.
132. Fast (Red) Oxidative Fibers Type IIaHave attributes in between fast and slow
types
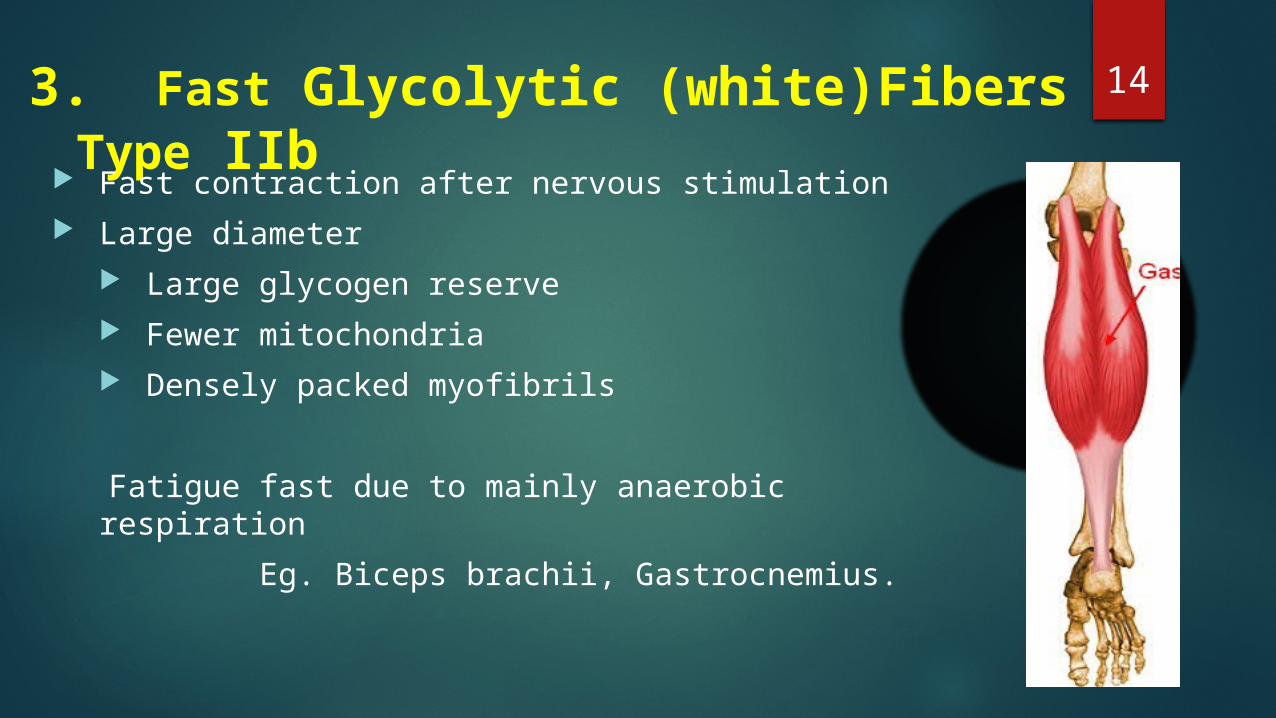
143. Fast Glycolytic (white)Fibers Type IIb
Fast contraction after nervous stimulation Large diameter
Large glycogen reserve Fewer mitochondria Densely packed myofibrils
Fatigue fast due to mainly anaerobic respiration Eg. Biceps brachii, Gastrocnemius.
15
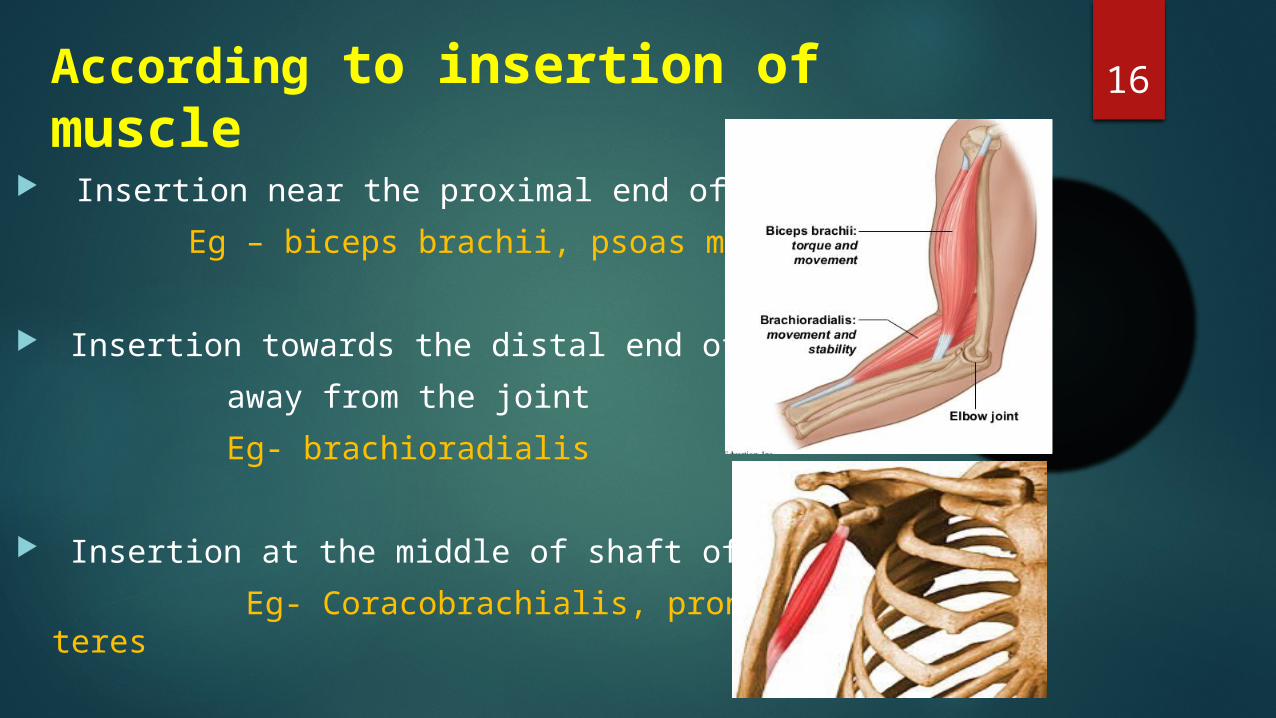
16According to insertion of muscle
Insertion near the proximal end of bone Eg – biceps brachii, psoas major
Insertion towards the distal end of bone, away from the joint Eg- brachioradialis
Insertion at the middle of shaft of bone Eg- Coracobrachialis, pronator teres
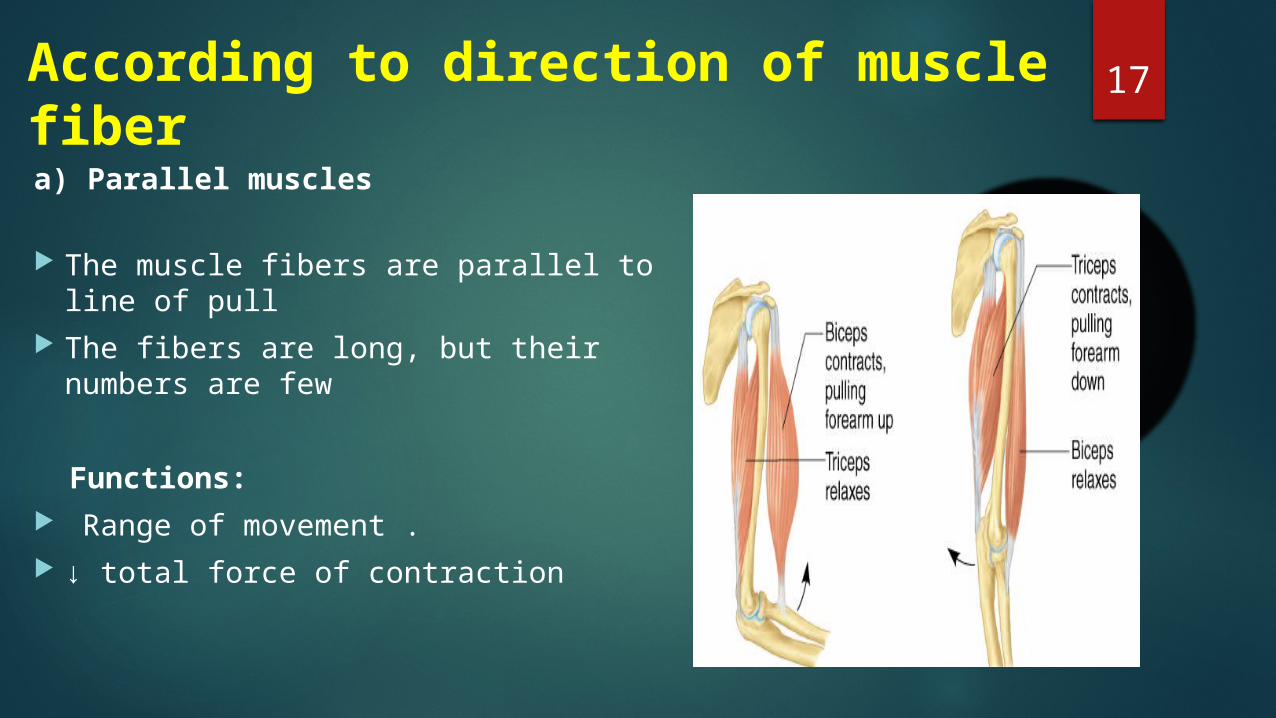
17According to direction of muscle fibera) Parallel muscles
The muscle fibers are parallel to line of pull
The fibers are long, but their numbers are few
Functions: Range of movement . ↓ total force of contraction
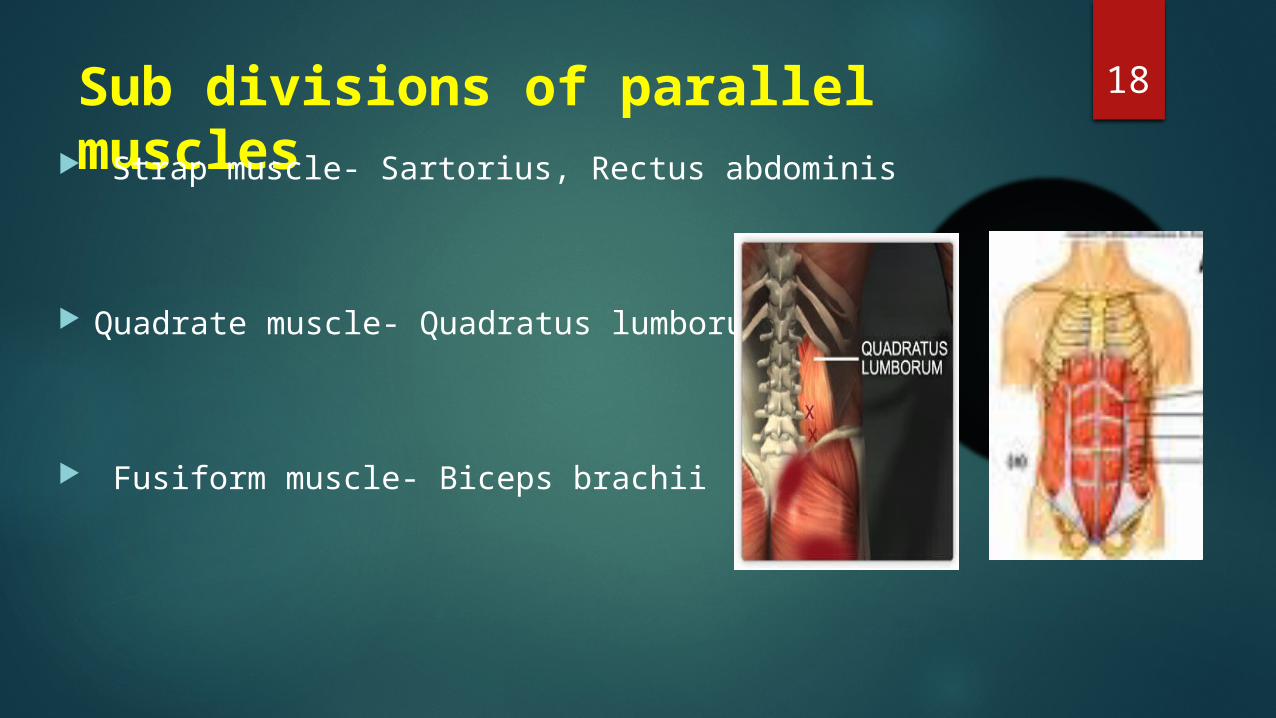
18Sub divisions of parallel muscles Strap muscle- Sartorius, Rectus abdominis
Quadrate muscle- Quadratus lumborum
Fusiform muscle- Biceps brachii
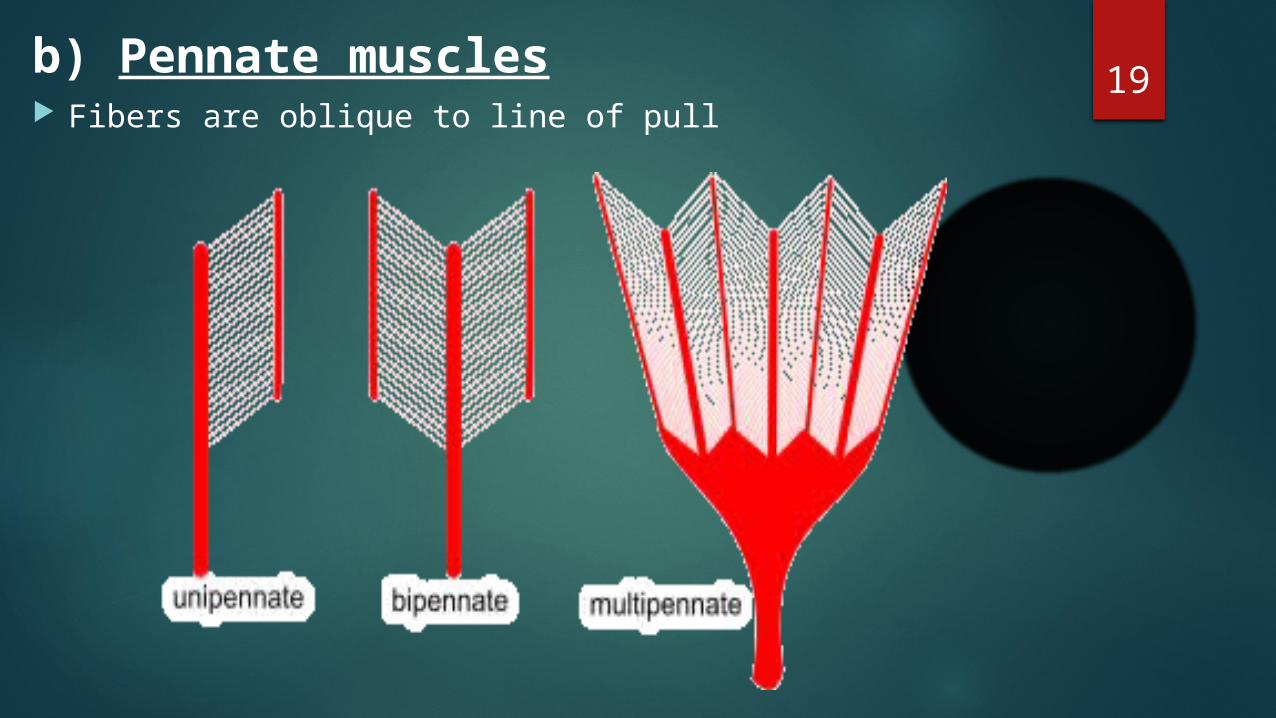
19b) Pennate muscles Fibers are oblique to line of pull
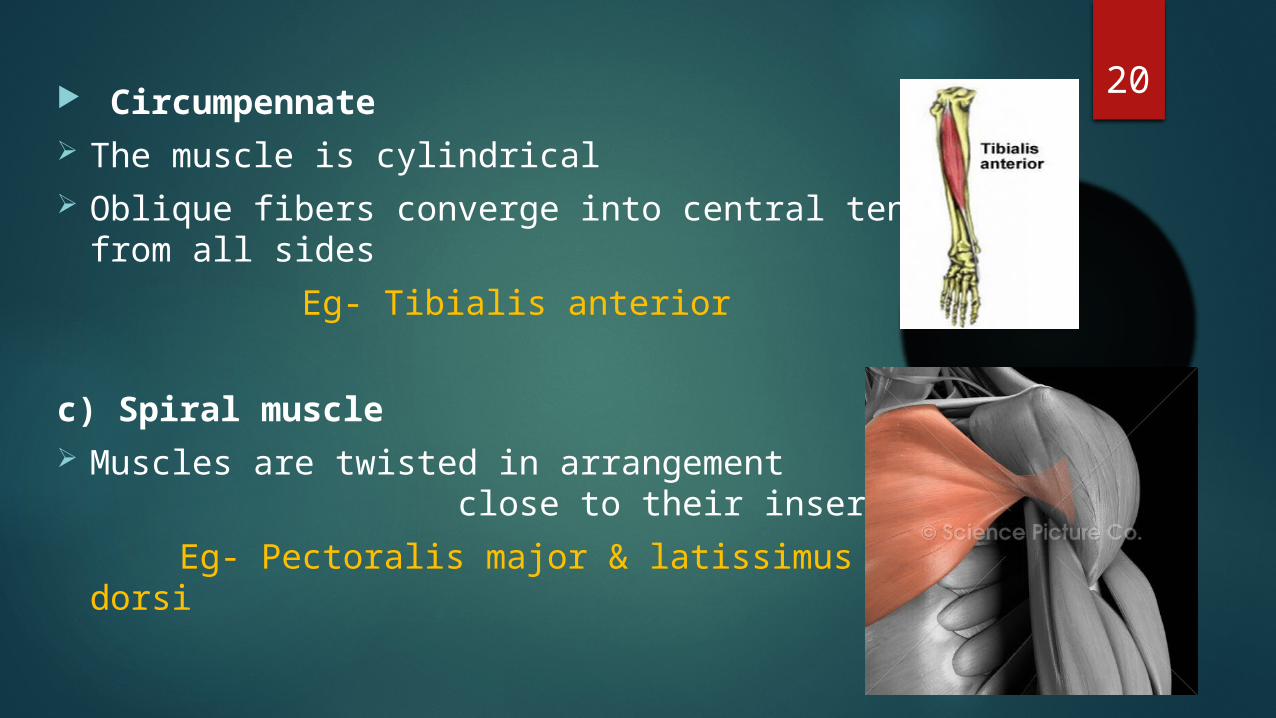
20 Circumpennate The muscle is cylindrical Oblique fibers converge into central tendon
from all sides Eg- Tibialis anterior
c) Spiral muscle Muscles are twisted in arrangement
close to their insertion Eg- Pectoralis major & latissimus dorsi
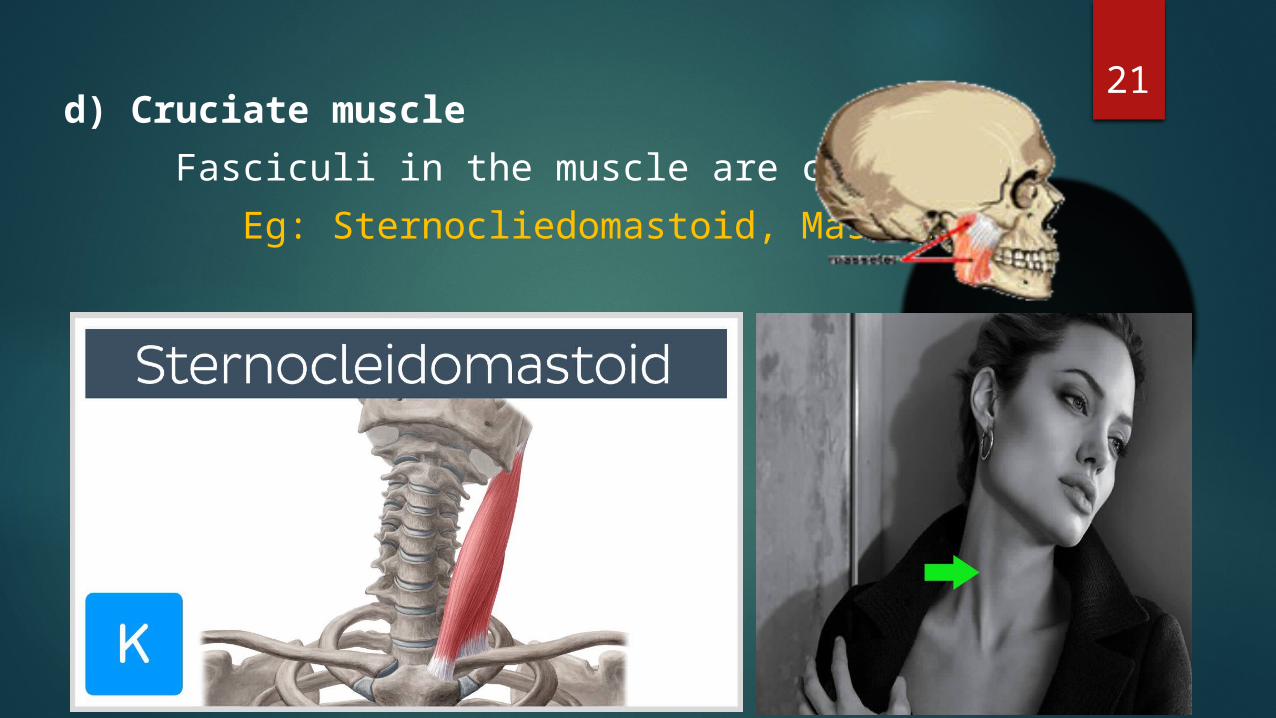
21d) Cruciate muscle Fasciculi in the muscle are crossed Eg: Sternocliedomastoid, Masseter
22
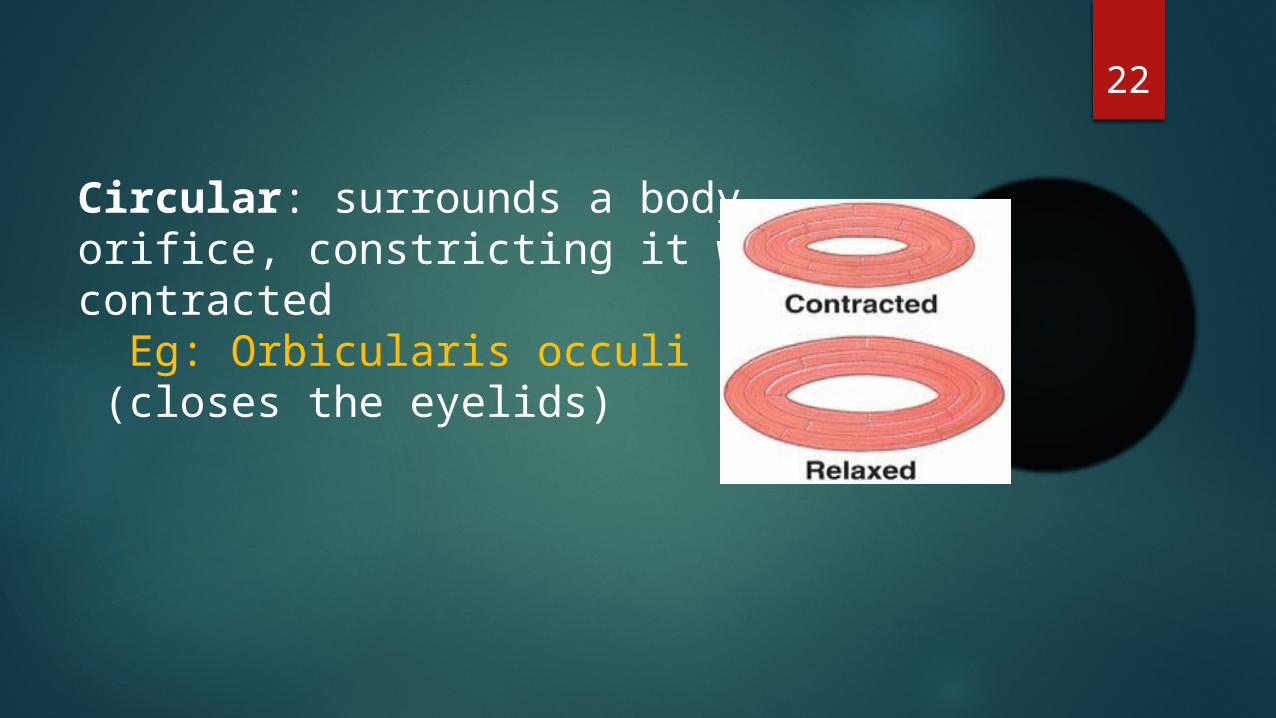
Circular: surrounds a bodyorifice, constricting it whencontracted Eg: Orbicularis occuli (closes the eyelids)
23
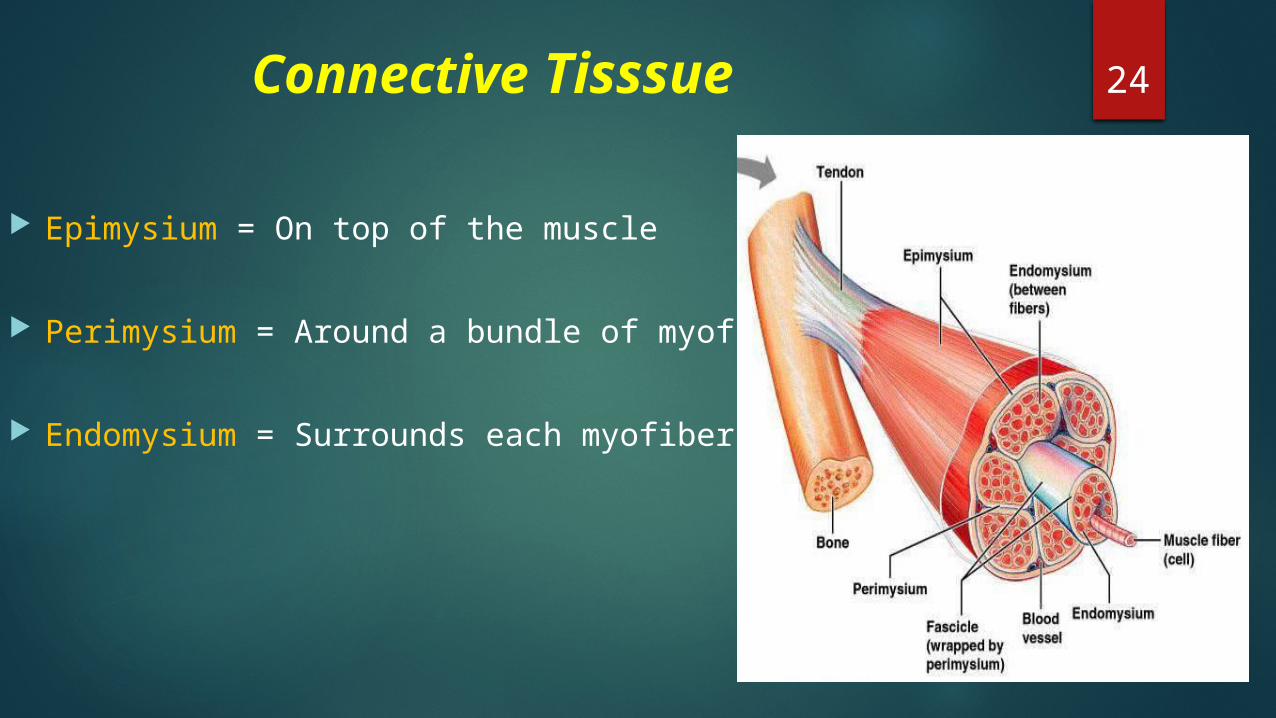
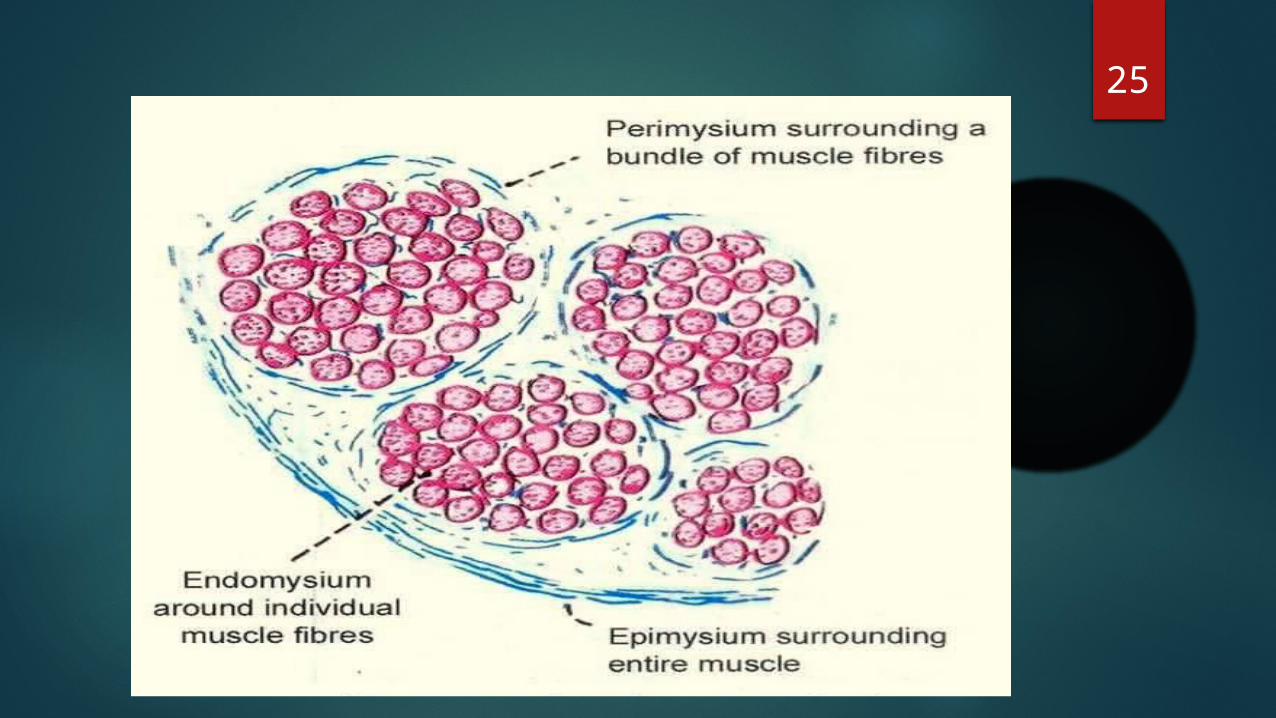
24 Connective Tisssue
Epimysium = On top of the muscle
Perimysium = Around a bundle of myofibers
Endomysium = Surrounds each myofiber
25
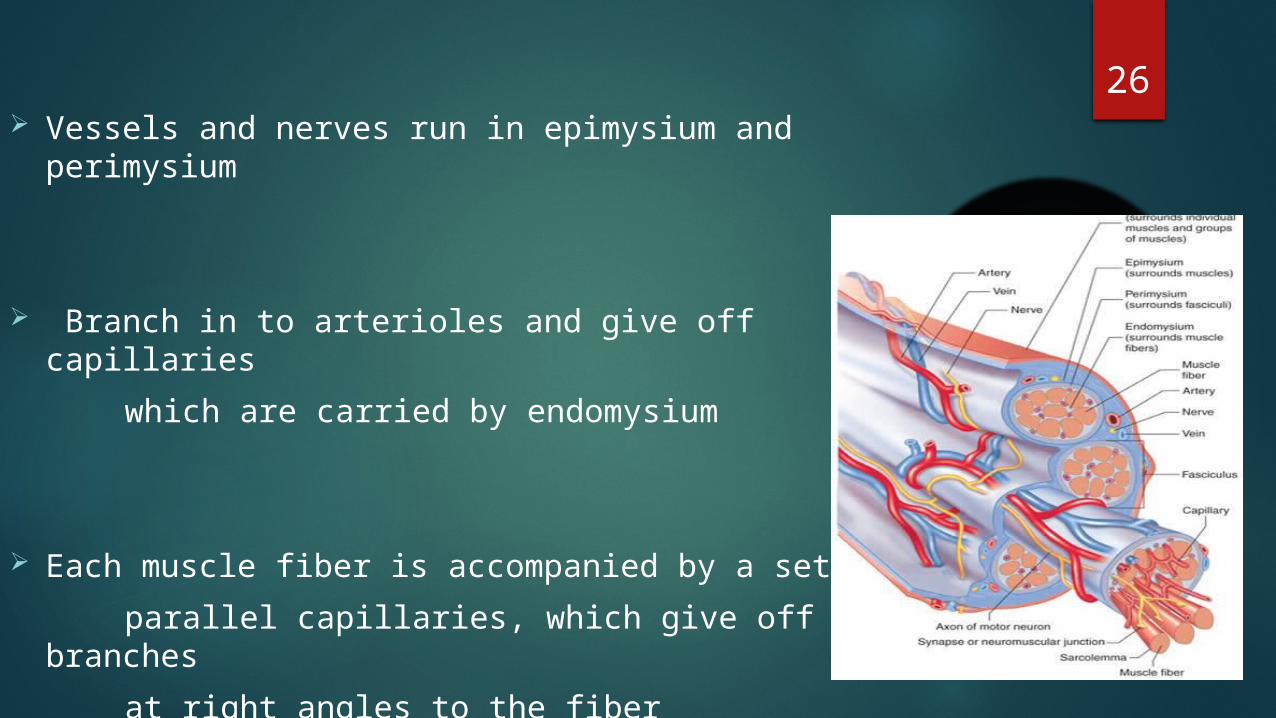
26 Vessels and nerves run in epimysium and perimysium
Branch in to arterioles and give off capillaries which are carried by endomysium
Each muscle fiber is accompanied by a set of parallel capillaries, which give off side branches at right angles to the fiber
27• Epimysium consists mainly type I collagen fibers
• Perimysium contain type I and III collagen fibers
• Endomysium contain type III and IV collagen fibers
• Collagen IV is associated with the basal lamina that invests each muscle fiber
• All these connective tissue layers extend beyond the muscle belly to form the tendons, aponeurosis and fascia.

28Attachment of tendon to skeletal muscle
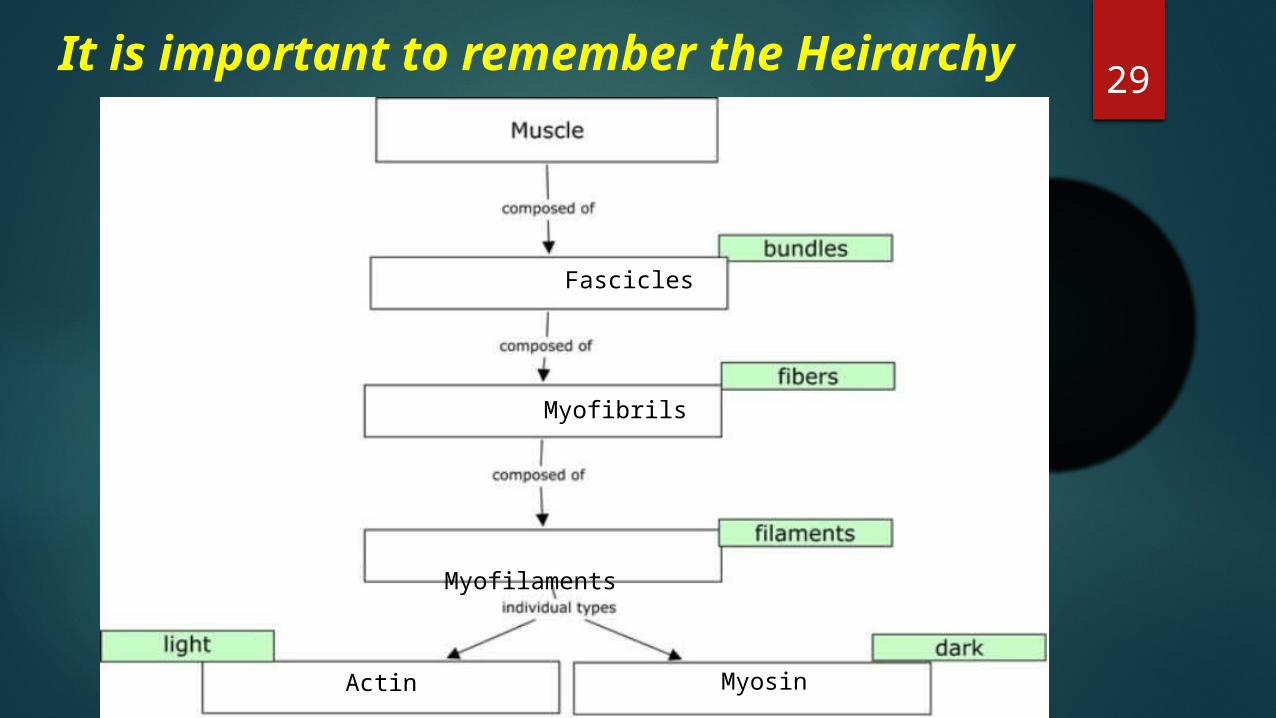
29
Fascicles
Myofibrils
Myofilaments
Actin Myosin
It is important to remember the Heirarchy
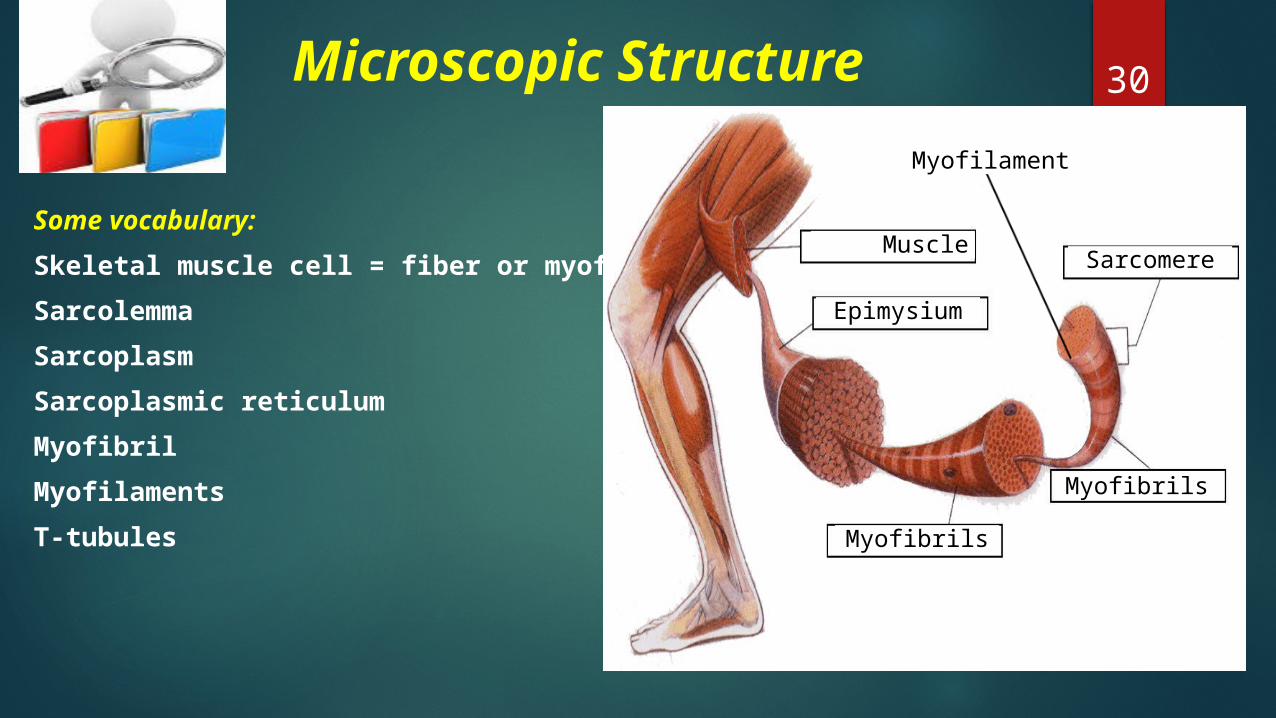
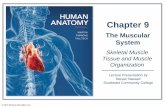
30 Microscopic Structure
Some vocabulary:Skeletal muscle cell = fiber or myofiber Sarcolemma Sarcoplasm Sarcoplasmic reticulumMyofibrilMyofilamentsT-tubules
Muscle
Epimysium
Myofibrils
Sarcomere
Myofilament
Myofibrils
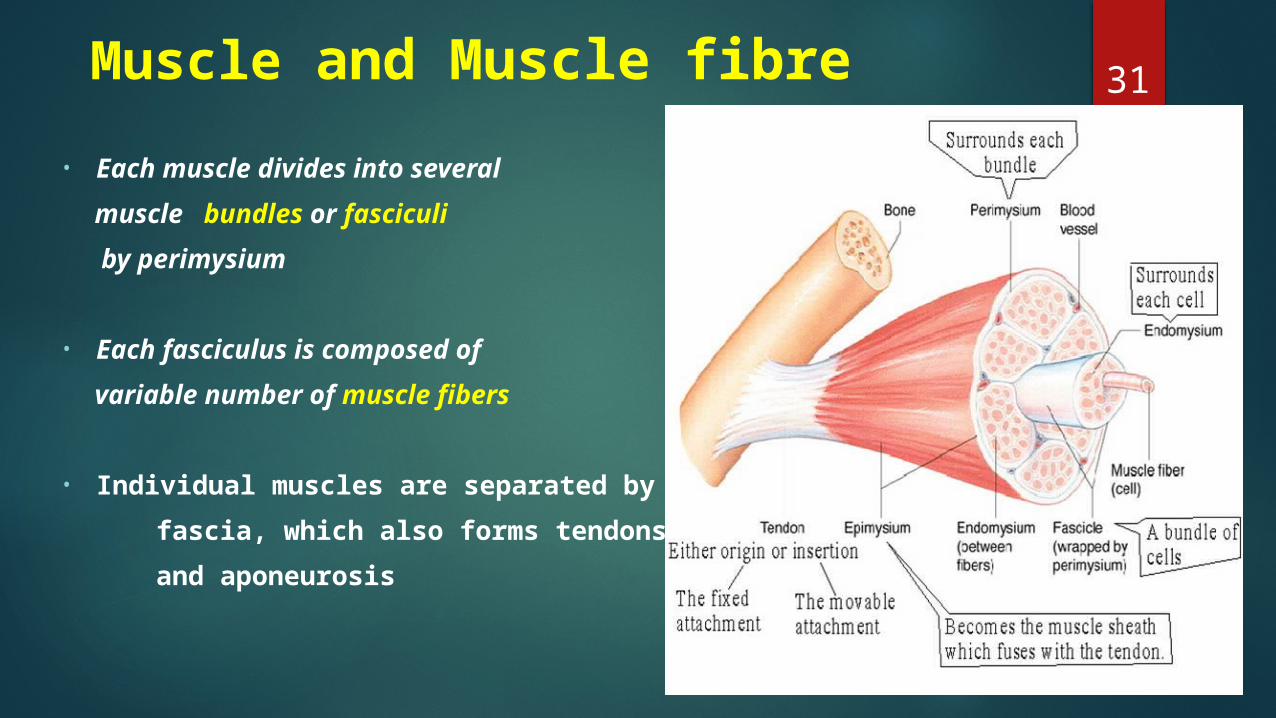
31 Muscle and Muscle fibre• Each muscle divides into several muscle bundles or fasciculi by perimysium
• Each fasciculus is composed of variable number of muscle fibers
• Individual muscles are separated by fascia, which also forms tendons and aponeurosis
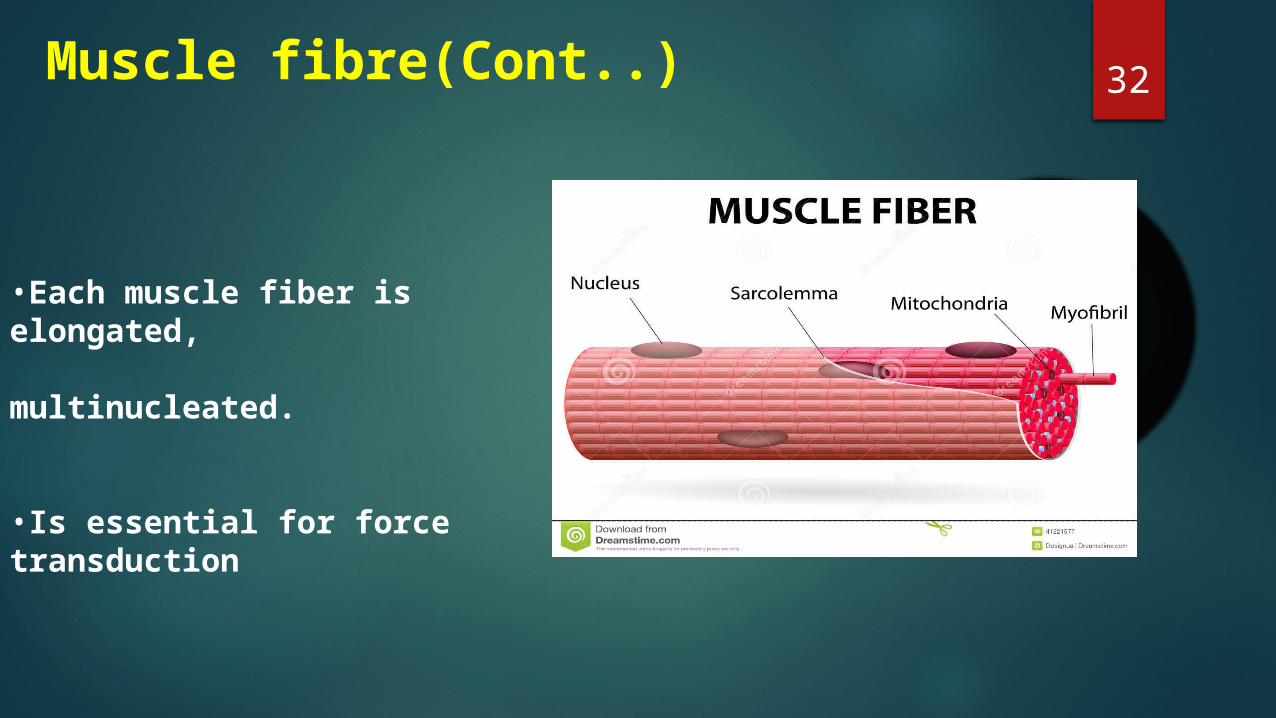
32Muscle fibre(Cont..)
•Each muscle fiber is elongated,
multinucleated.
•Is essential for force transduction
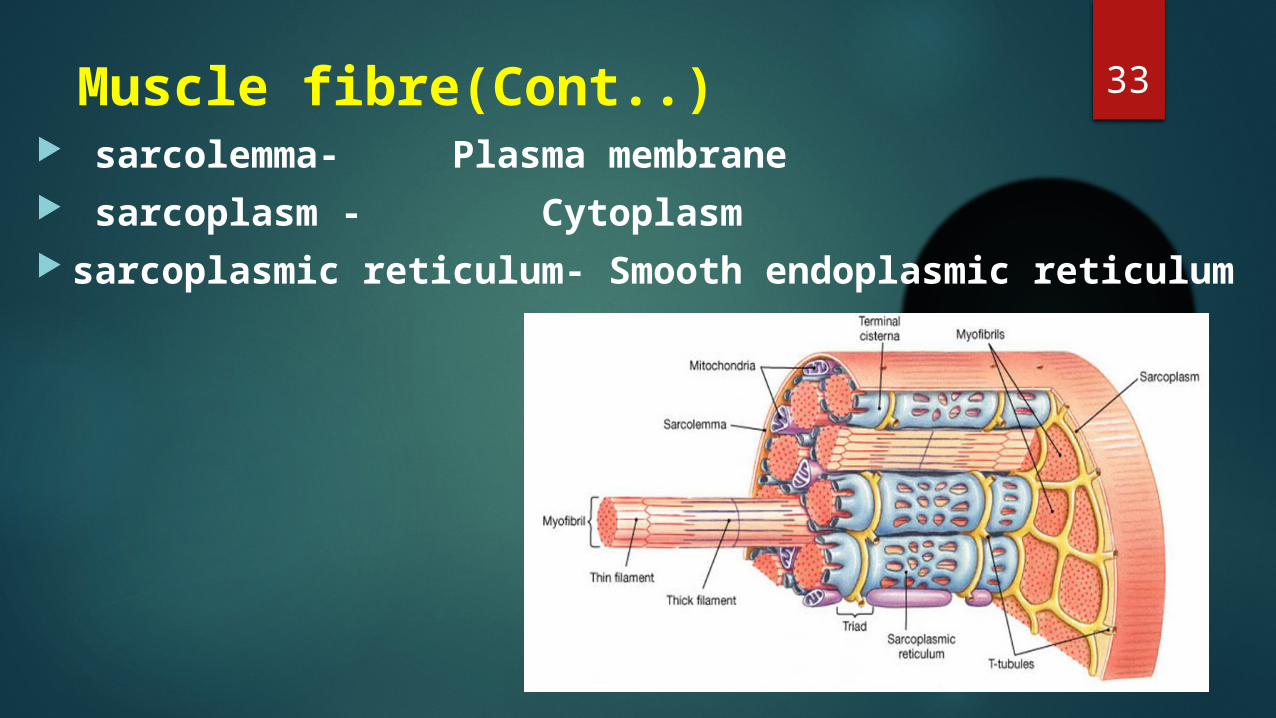
33Muscle fibre(Cont..) sarcolemma- Plasma membrane sarcoplasm - Cytoplasm sarcoplasmic reticulum- Smooth endoplasmic reticulum
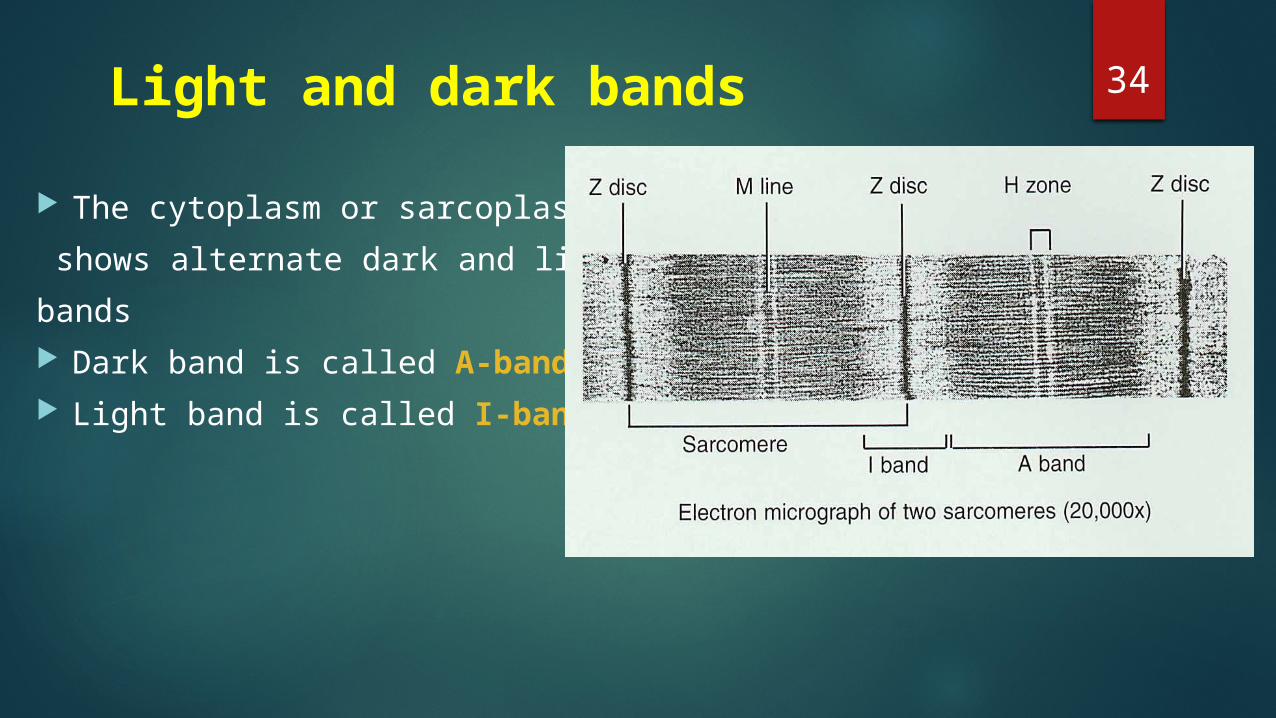
34 Light and dark bands
The cytoplasm or sarcoplasm shows alternate dark and light bands Dark band is called A-band Light band is called I-band
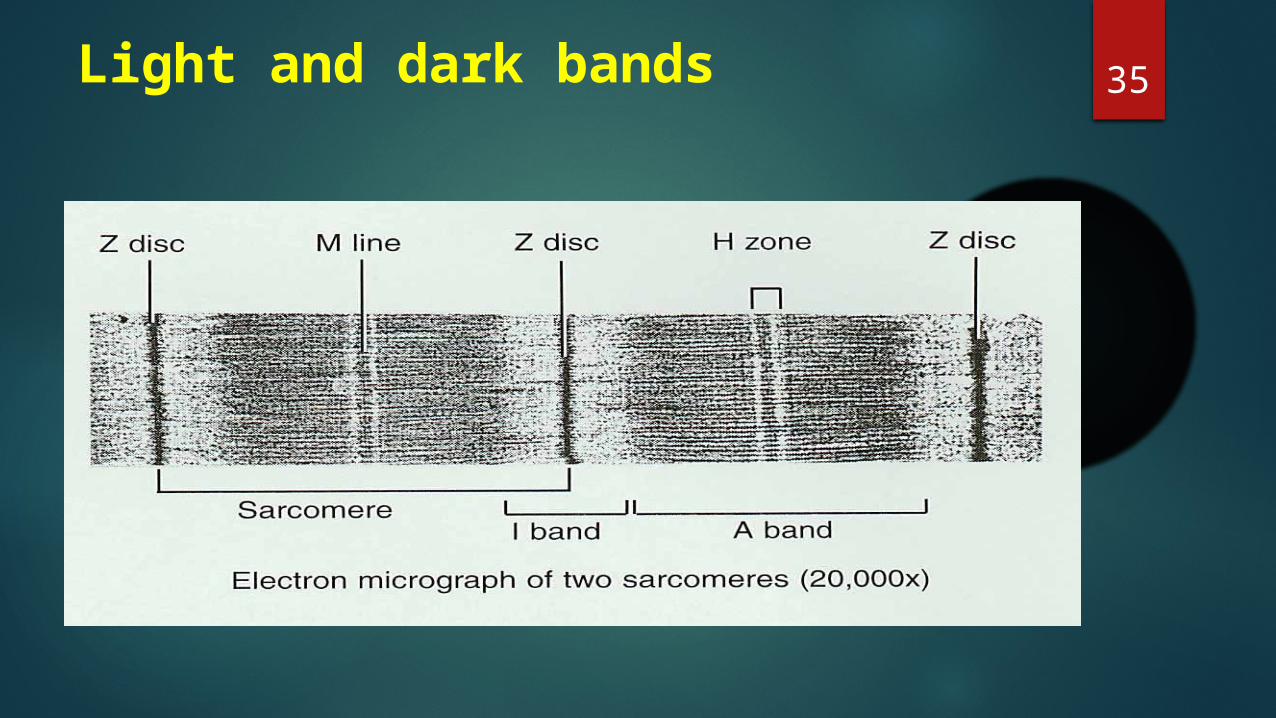
35Light and dark bands
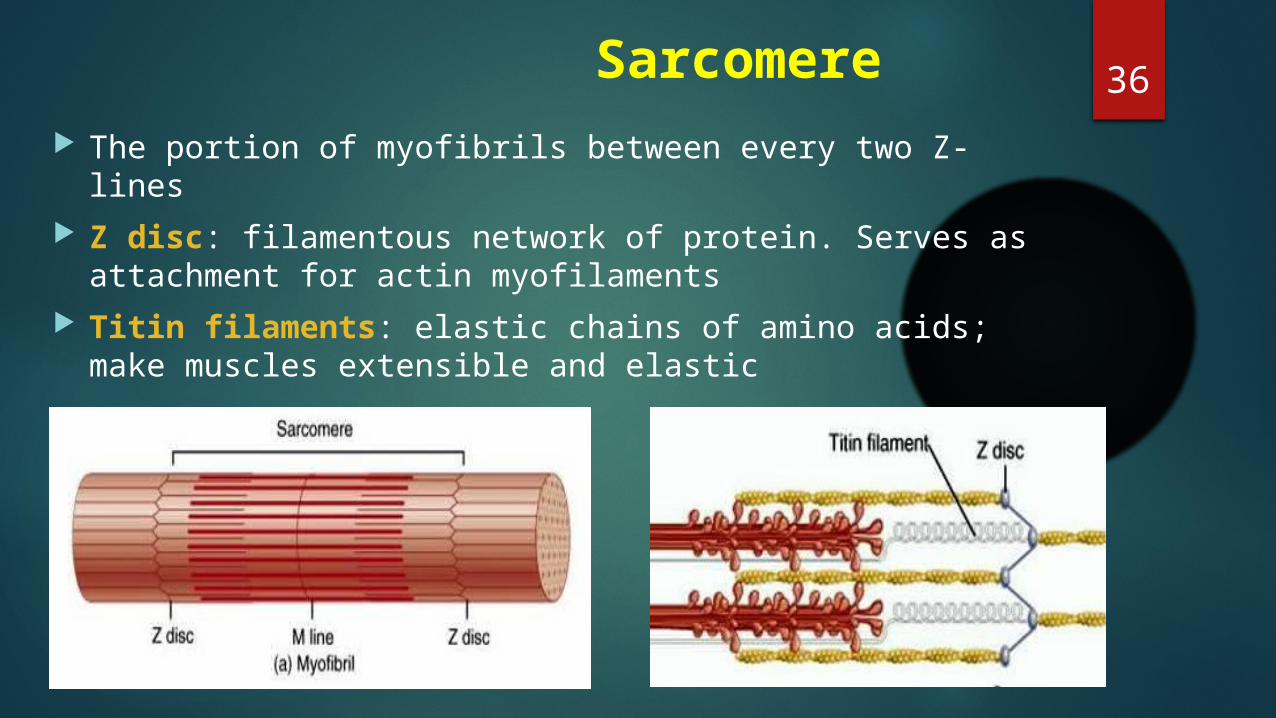
36 Sarcomere The portion of myofibrils between every two Z-lines Z disc: filamentous network of protein. Serves as
attachment for actin myofilaments Titin filaments: elastic chains of amino acids; make
muscles extensible and elastic
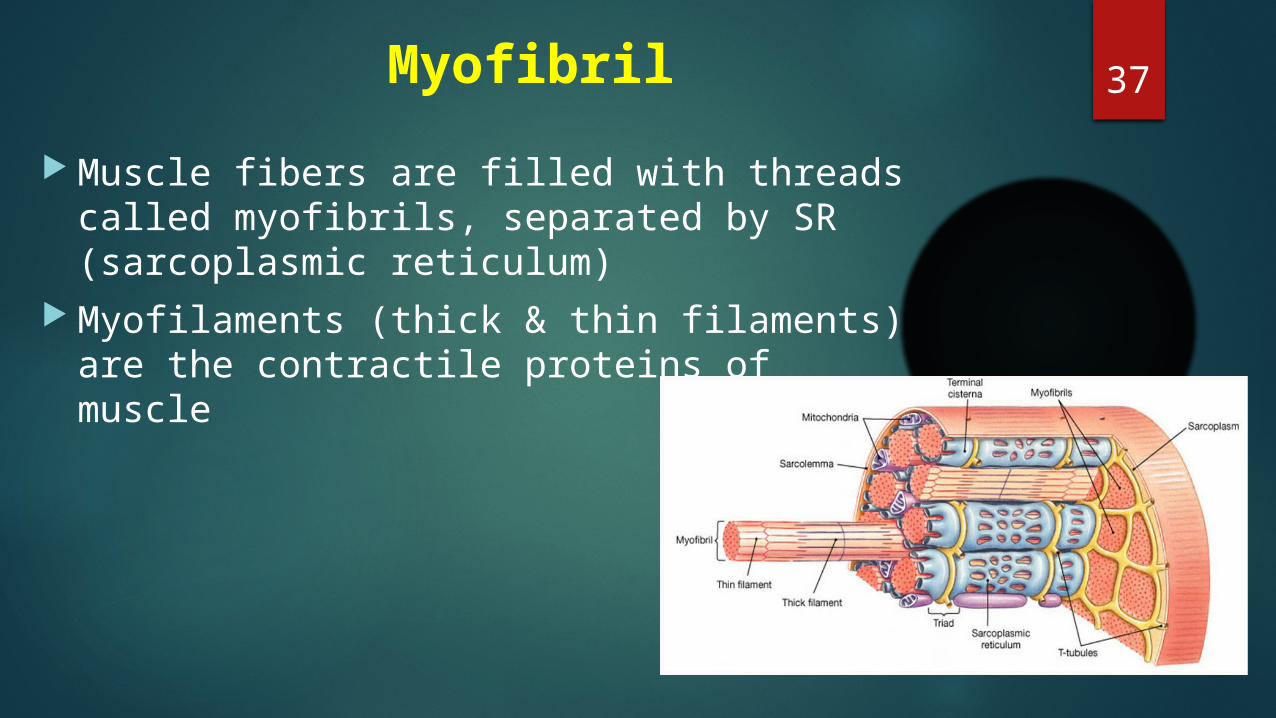
37Myofibril Muscle fibers are filled with threads called
myofibrils, separated by SR (sarcoplasmic reticulum)
Myofilaments (thick & thin filaments) are the contractile proteins of muscle
38
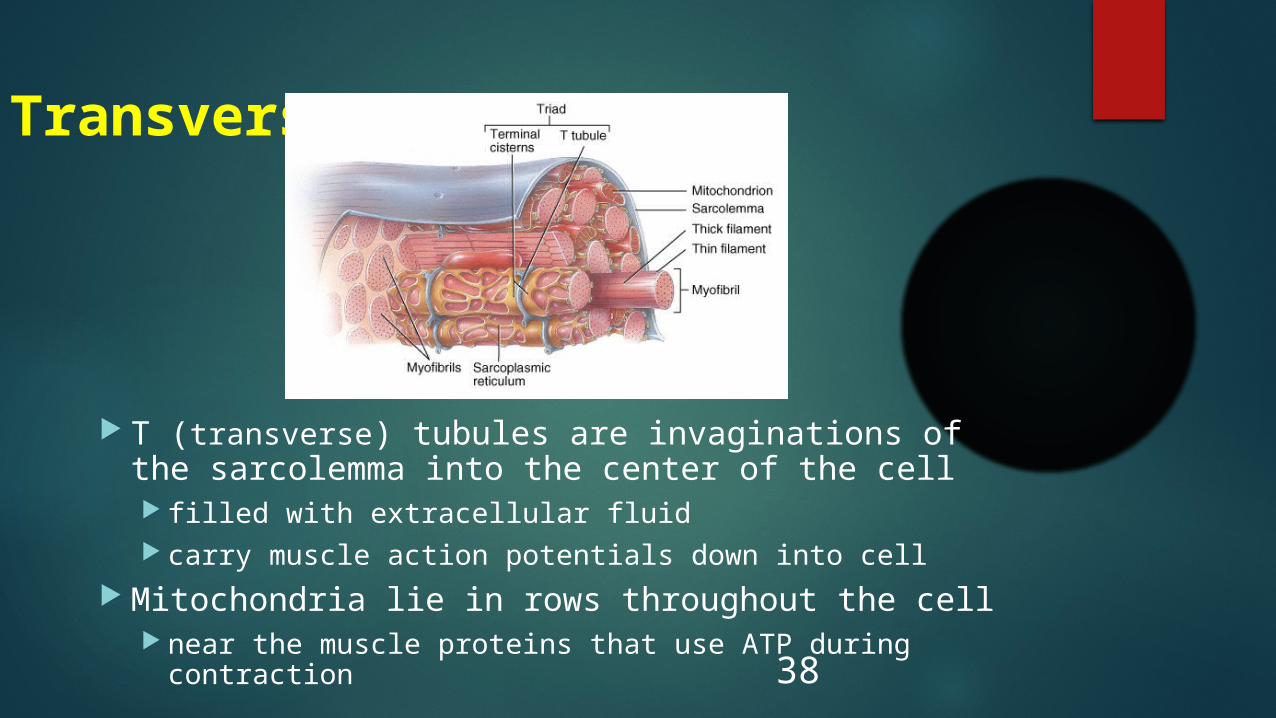
Transverse Tubules
T (transverse) tubules are invaginations of the sarcolemma into the center of the cell filled with extracellular fluid carry muscle action potentials down into cell
Mitochondria lie in rows throughout the cell near the muscle proteins that use ATP during contraction
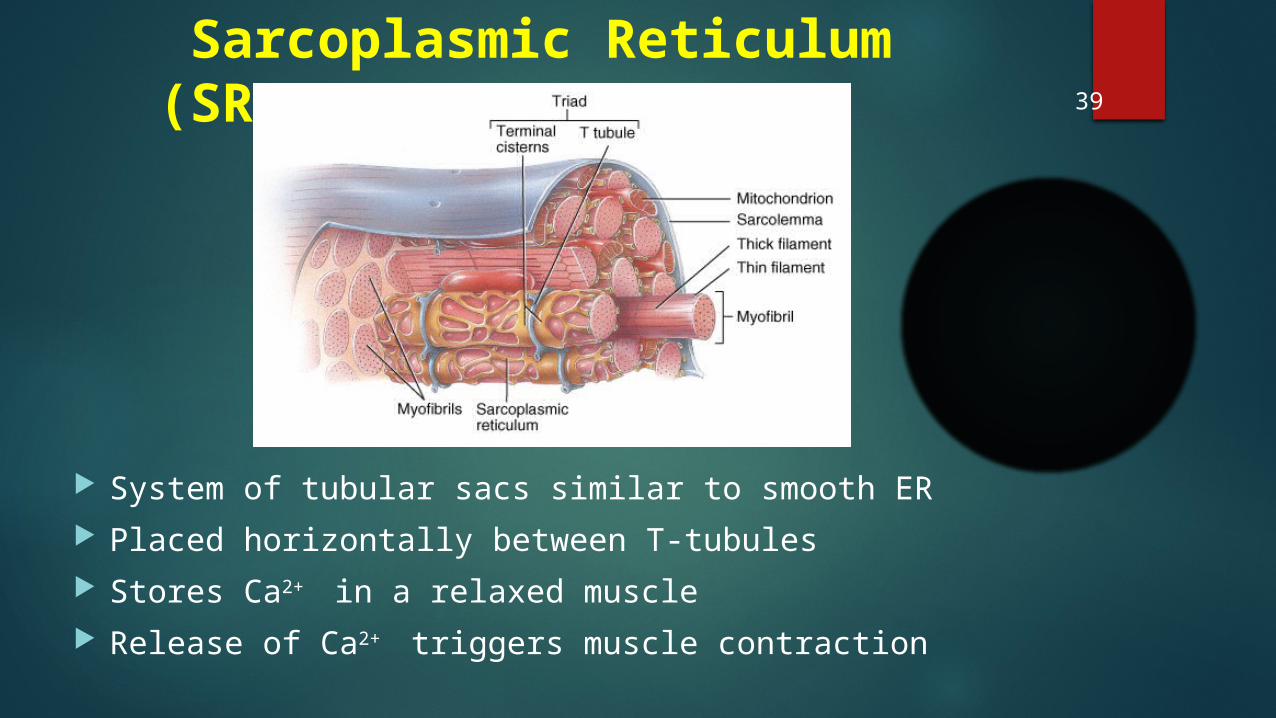
Sarcoplasmic Reticulum (SR)
System of tubular sacs similar to smooth ER Placed horizontally between T-tubules Stores Ca2+ in a relaxed muscle Release of Ca2+ triggers muscle contraction
39
40 Proteins of Muscle Myofibrils are built of 3 kinds of protein
Contractile proteins myosin and actin
Regulatory proteins which turn contraction on & off troponin and tropomyosin
Structural proteins which provide proper alignment, elasticity and extensibility
titin, myomesin, nebulin and dystrophin
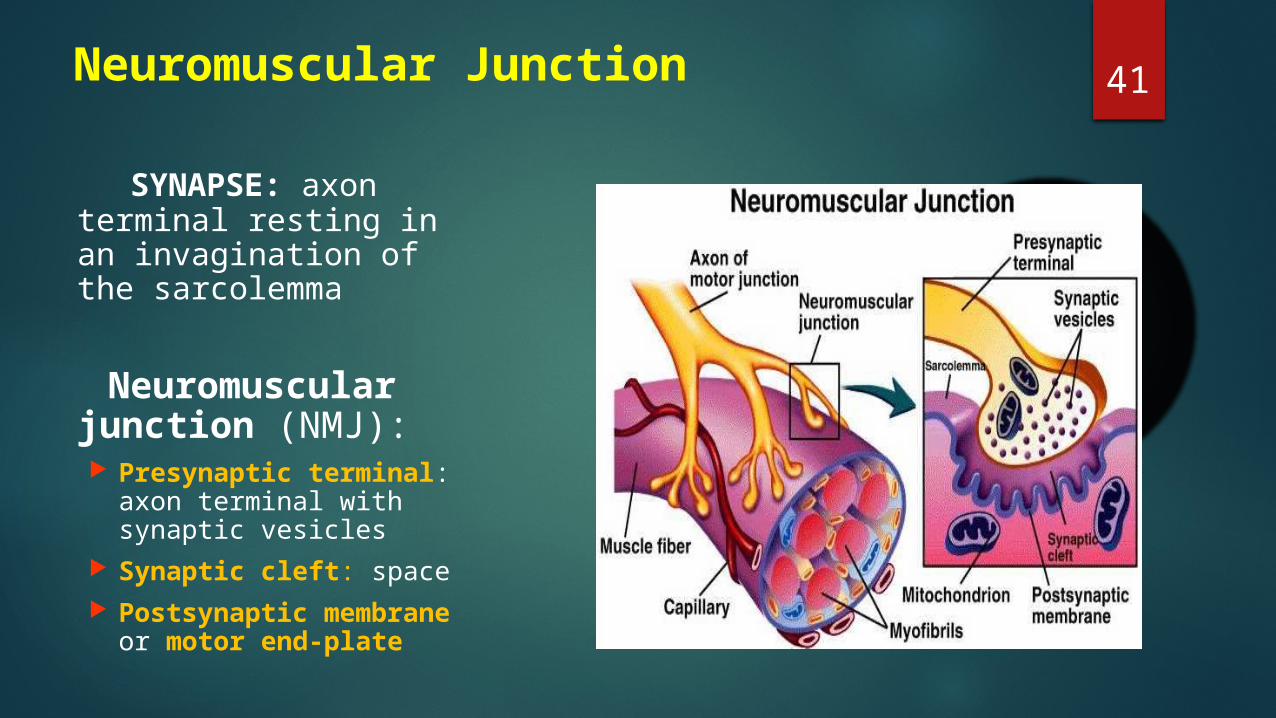
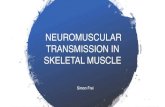
41Neuromuscular Junction
SYNAPSE: axon terminal resting in an invagination of the sarcolemma
Neuromuscular junction (NMJ): Presynaptic terminal:
axon terminal with synaptic vesicles
Synaptic cleft: space Postsynaptic membrane
or motor end-plate
42
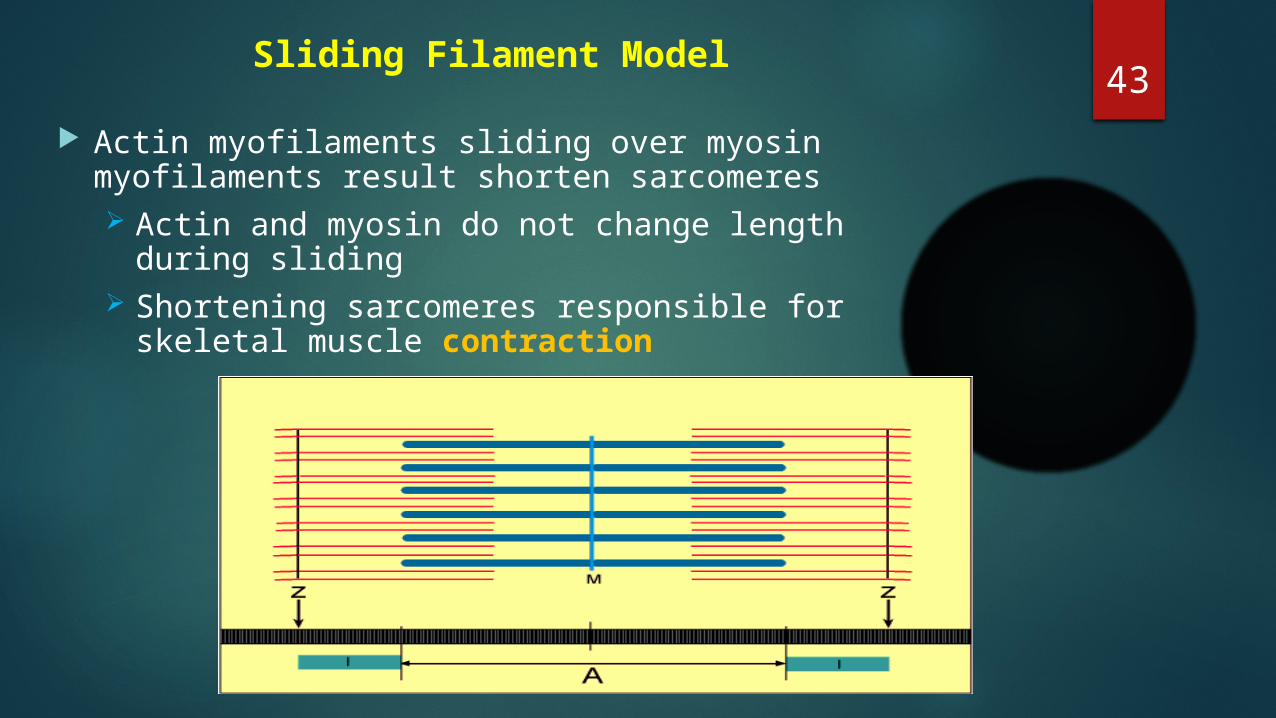
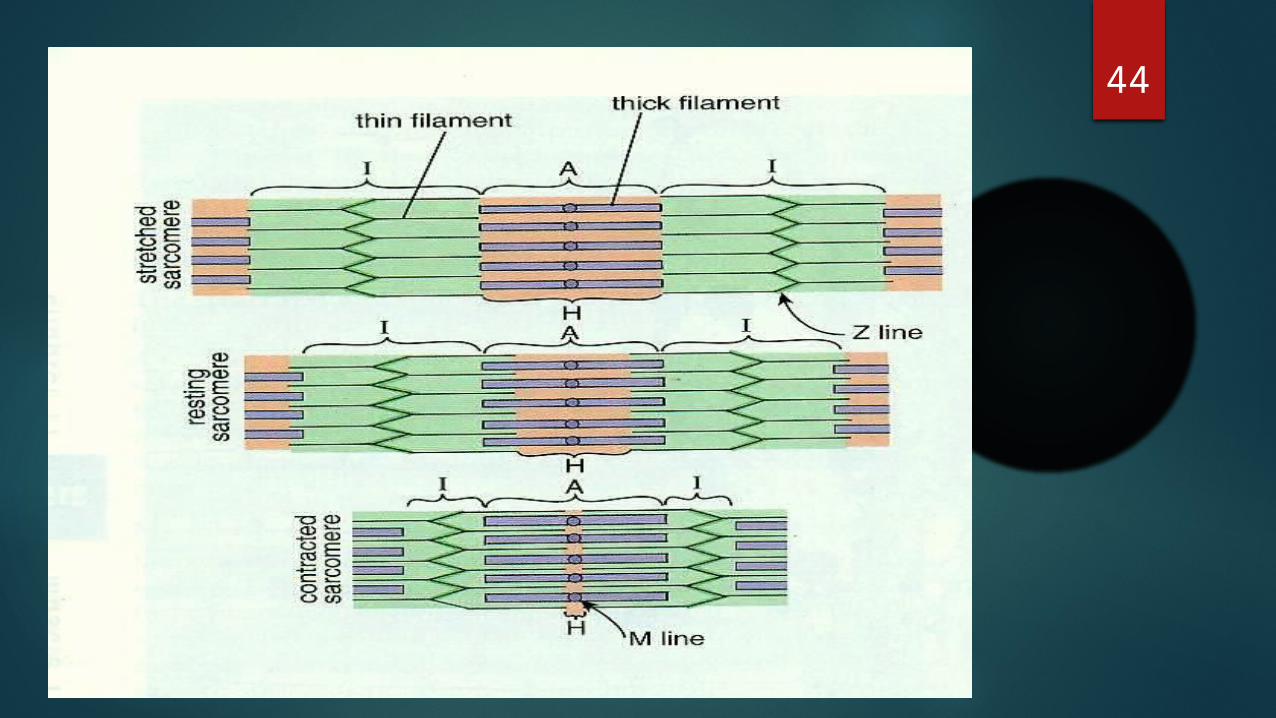
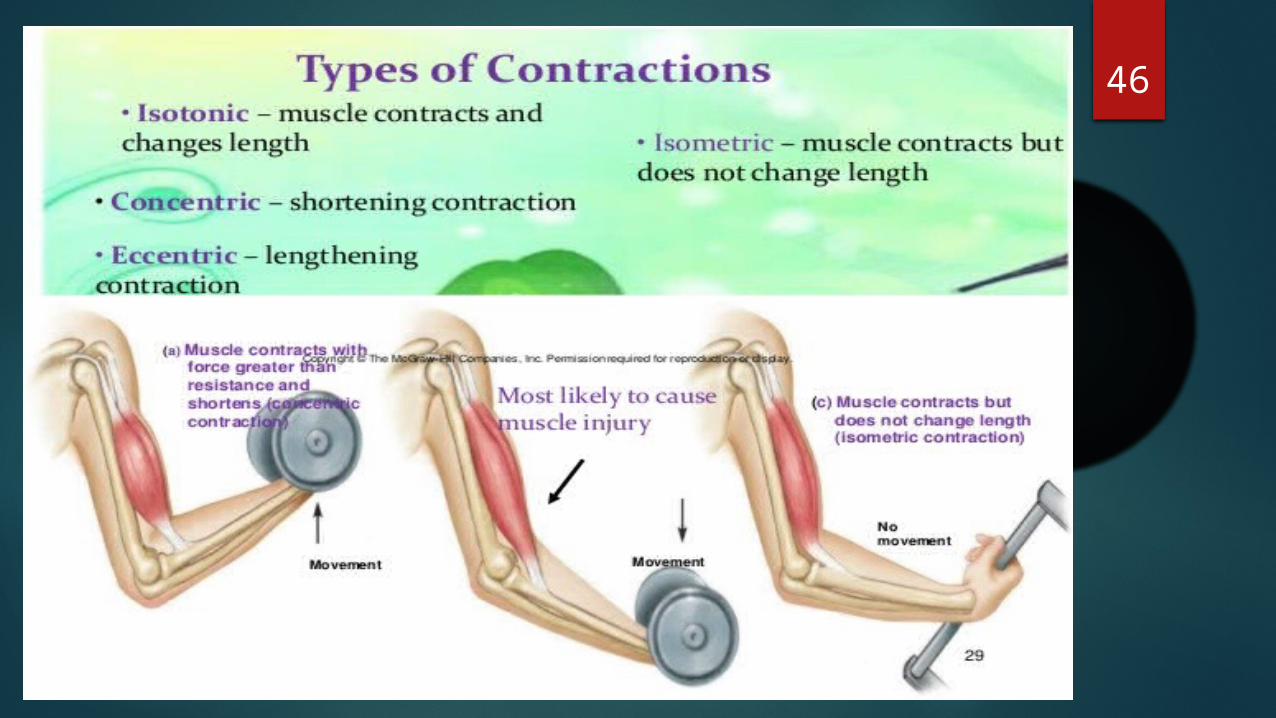
43Sliding Filament Model
Actin myofilaments sliding over myosin myofilaments result shorten sarcomeres Actin and myosin do not change length during
sliding Shortening sarcomeres responsible for skeletal
muscle contraction
44
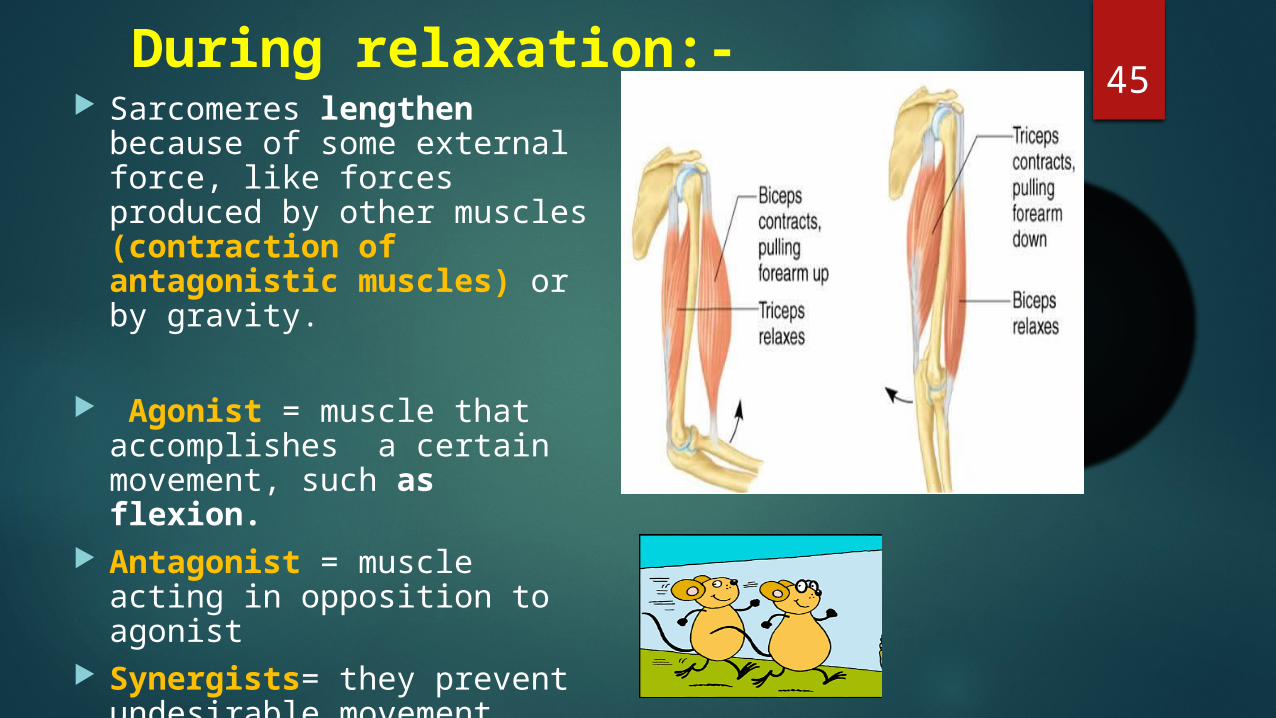
45During relaxation:-
Sarcomeres lengthen because of some external force, like forces produced by other muscles (contraction of antagonistic muscles) or by gravity.
Agonist = muscle that accomplishes a certain movement, such as flexion.
Antagonist = muscle acting in opposition to agonist
Synergists= they prevent undesirable movement
46
47 Energy Sources ATP provides immediate energy for muscle contractions. Produced from three sources Creatine phosphate
During resting conditions stores energy to synthesize ATP
ADP + Creatine phosphate------------------ Creatine + 1ATP
Anaerobic respiration Occurs in absence of oxygen and results in breakdown
of glucose to yield ATP and lactic acid Aerobic respiration
Requires oxygen and breaks down glucose to produce ATP, carbon dioxide and water
More efficient than anaerobic
(Creatine Kinase)
48Skeletal muscle: Nerve supply
Supplied by motor and sensory nerves Motor fibers: Two types
Alpha fibresThickly myelinated axons supply extrafusal
muscle fibresProduces movements(Contraction)
Gamma fibresThinly myelinated fibres which supply intrafusal
fibers of the muscle spindleMaintains the tone of the
muscle(Proprioception)Unmyelinated sympathetic fibers
Supply blood vessels
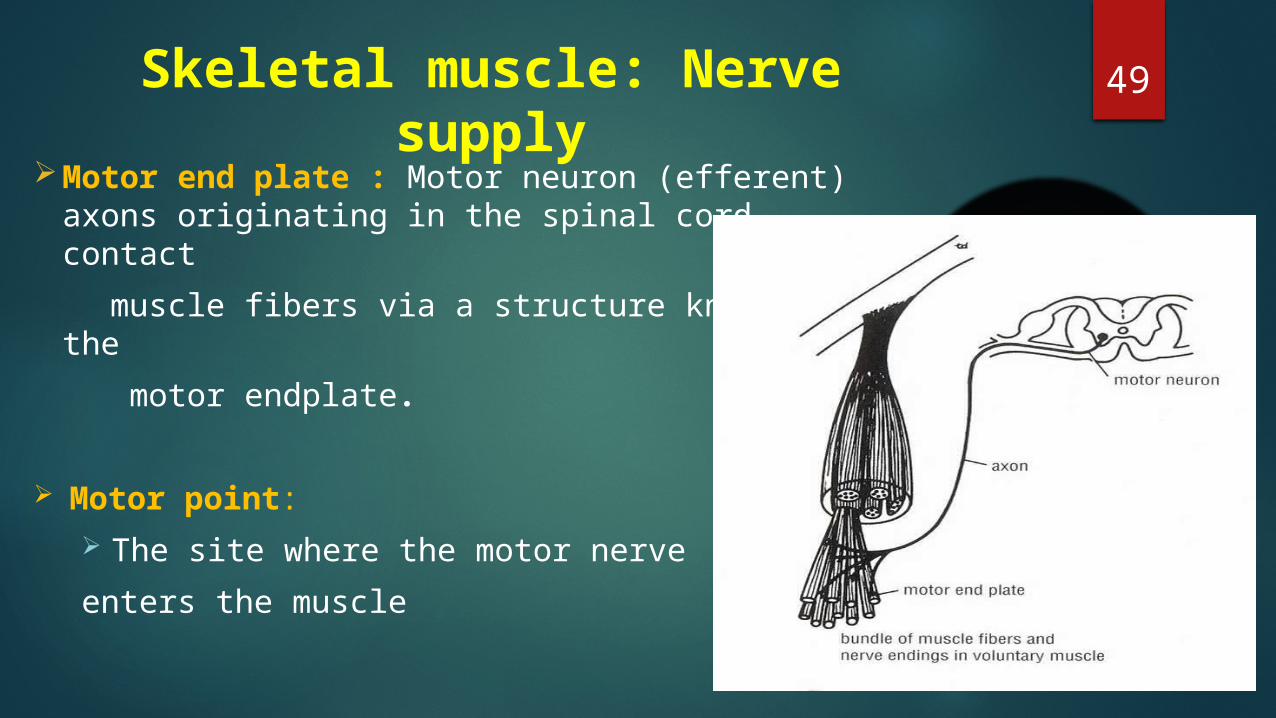
49Skeletal muscle: Nerve supply
Motor end plate : Motor neuron (efferent) axons originating in the spinal cord contact
muscle fibers via a structure known as the motor endplate.
Motor point: The site where the motor nerve enters the muscle
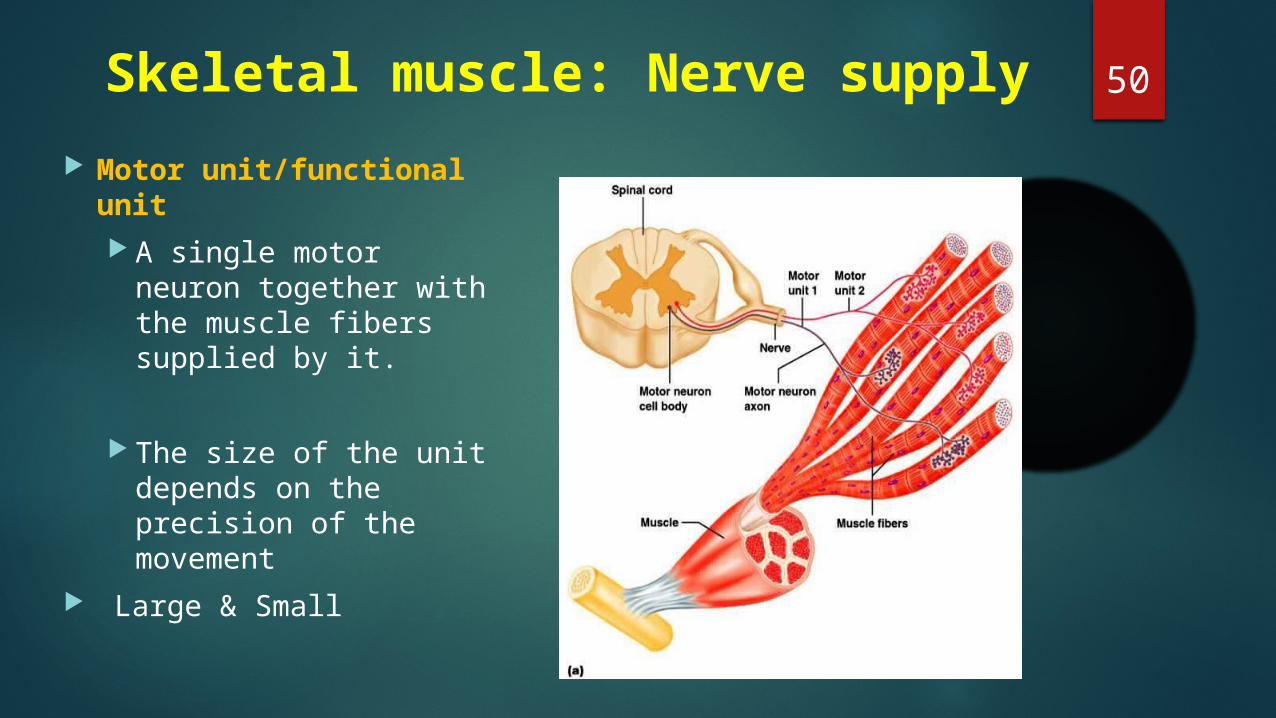
50Skeletal muscle: Nerve supply Motor unit/functional
unit A single motor neuron
together with the muscle fibers supplied by it.
The size of the unit depends on the precision of the movement
Large & Small
51 Sensory fibers
Arises from specialized endings
Muscle spindle/tendon spindle
Essential for muscle tone and body posture
Essential for coordinated voluntary movements
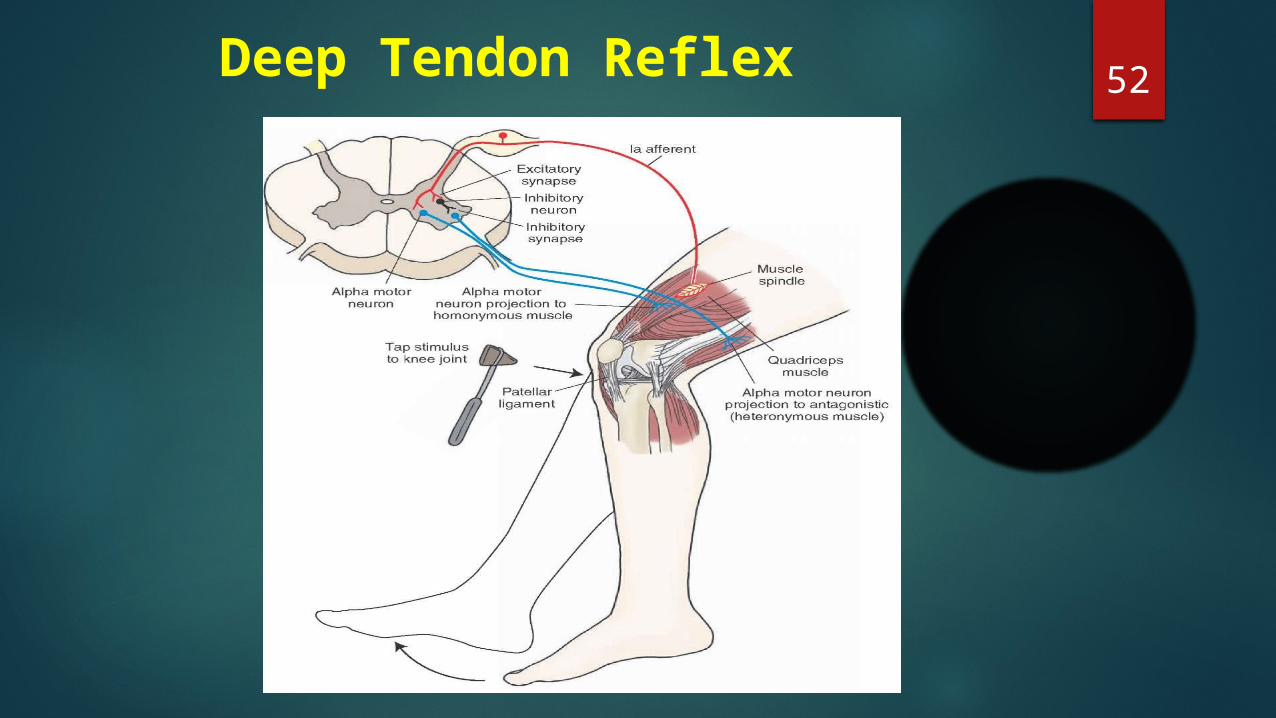
52Deep Tendon Reflex
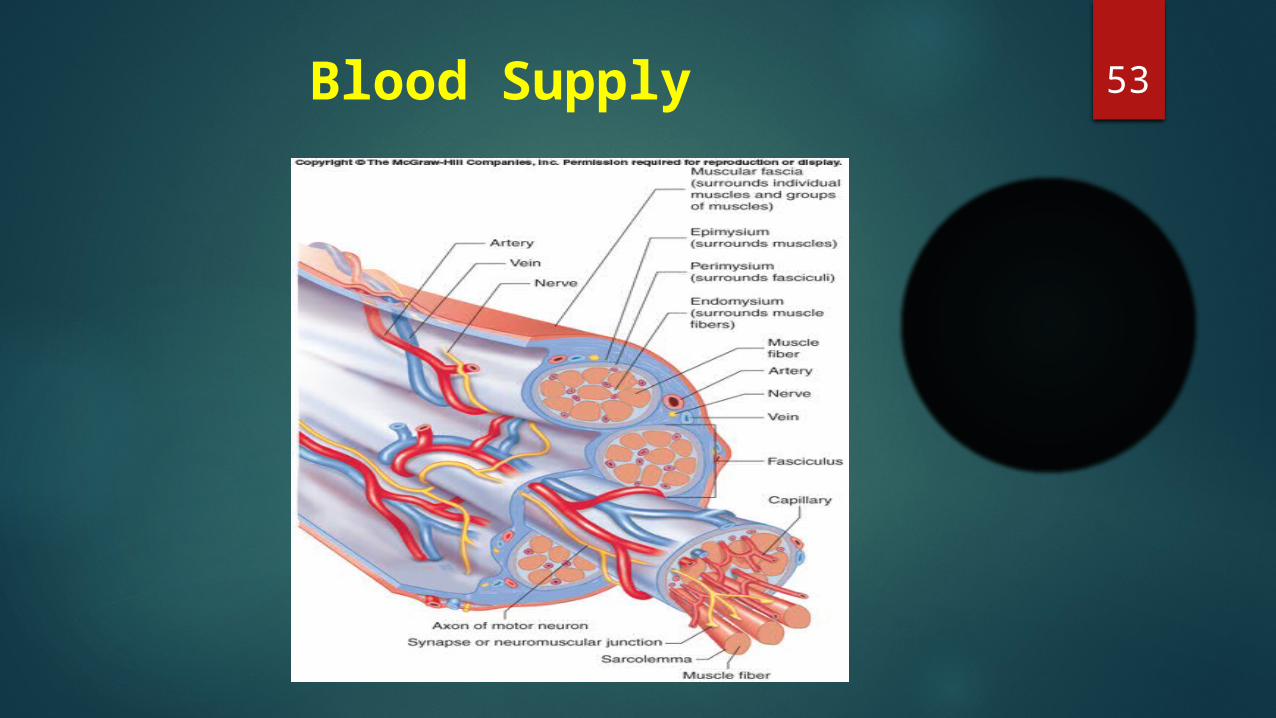
53 Blood Supply
54
Movement
Posture & Body
position
Support to Soft tissues
Joint stabilizatio
n
Body Temperatur
e
Skeletal Muscles
Functions
Facial Expression
Protection
55Properties of Muscle Tissue
Excitability Respond to chemicals released from nerve cells
Conductivity Ability to propagate electrical signals over
membrane Contractility
Ability to shorten and generate force Extensibility
Ability to be stretched without damaging the tissue
Elasticity Ability to return to original shape after being
stretched

56
APPLIED ANATOMY
57
Muscle Disorders
Trauma
Compartment syndrome
Carpal tunnelsyndromeBruises or tear
Infection
Myositis Trichinosis Fibromyalgia Tetanus
Inherited disorders
Muscular dystrophies
Tumors
MyomasSarcomas
58
Secondary Disorders
Immune problems:
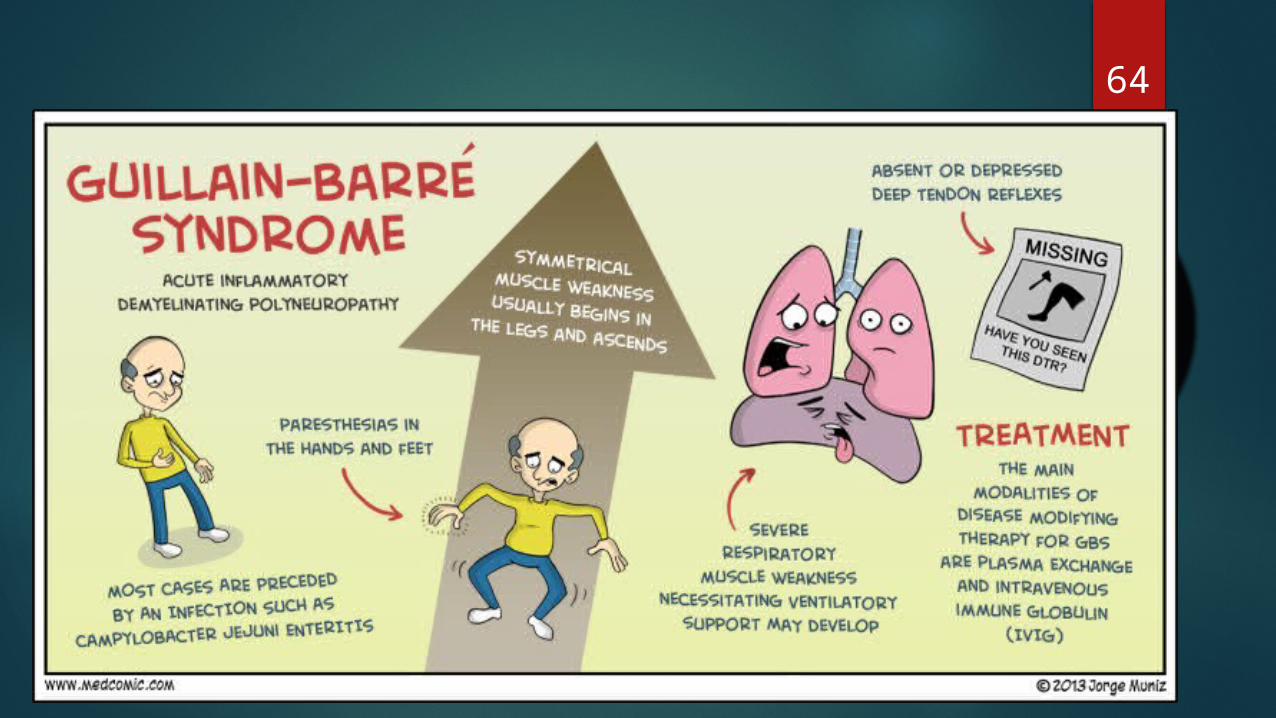
Myasthenia gravisGuilliain Barre
syndrome
Nervous system:
Botulism Poliomyelitis
Cardiovascular system:
AnemiaHeart failure
Metabolic problems:
HypercalcemiaHypocalcemia
59Fatigue Decreased capacity to work and reduced
efficiency of performance Cause - Exhaustion of Ach in motor endplate Accumulation of metabolites like lactic
acid and phosphoric acid Lack of nutrients like glucose Lack of oxygen
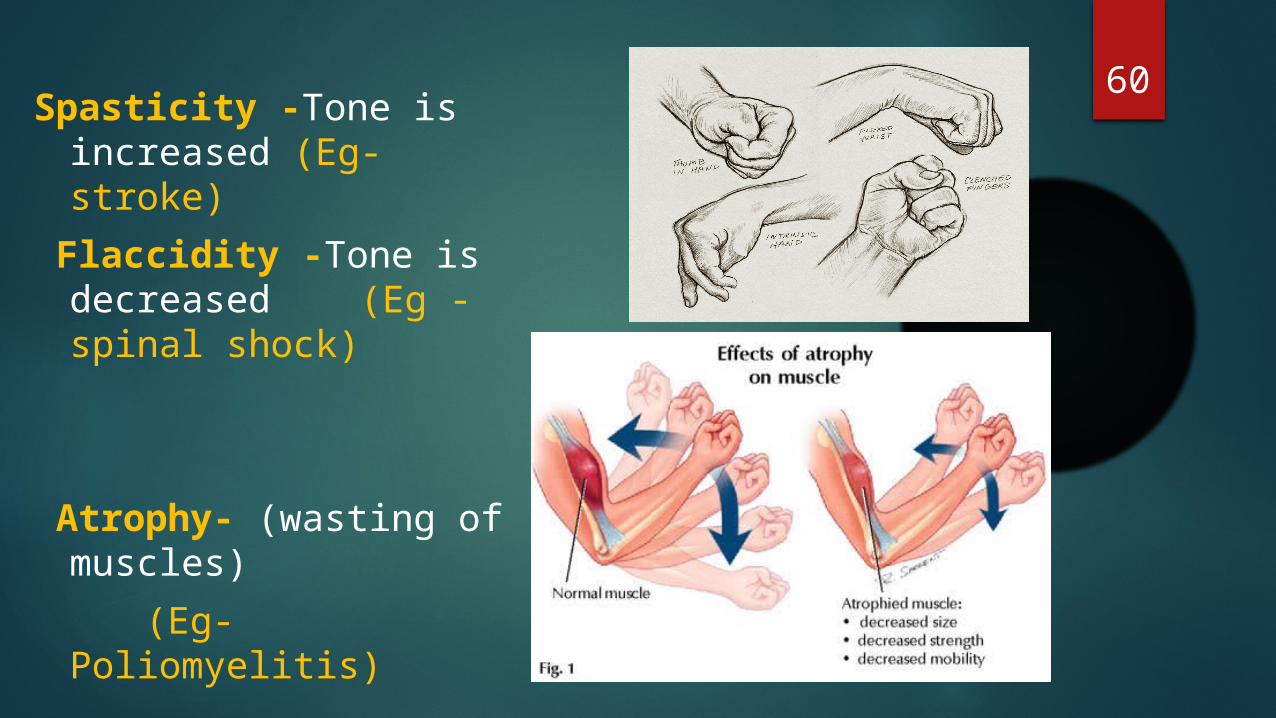
60Spasticity -Tone is increased (Eg- stroke)
Flaccidity -Tone is decreased (Eg -spinal shock)
Atrophy- (wasting of muscles)
(Eg- Poliomyelitis)
61 Hypertrophy - New muscle fibers are not
formed, Enlargement due to production of more myofibrils and cell organelles Hyperplasia –
increase in number Damage of skeletal
muscle – replaced by fibrous scar tissue
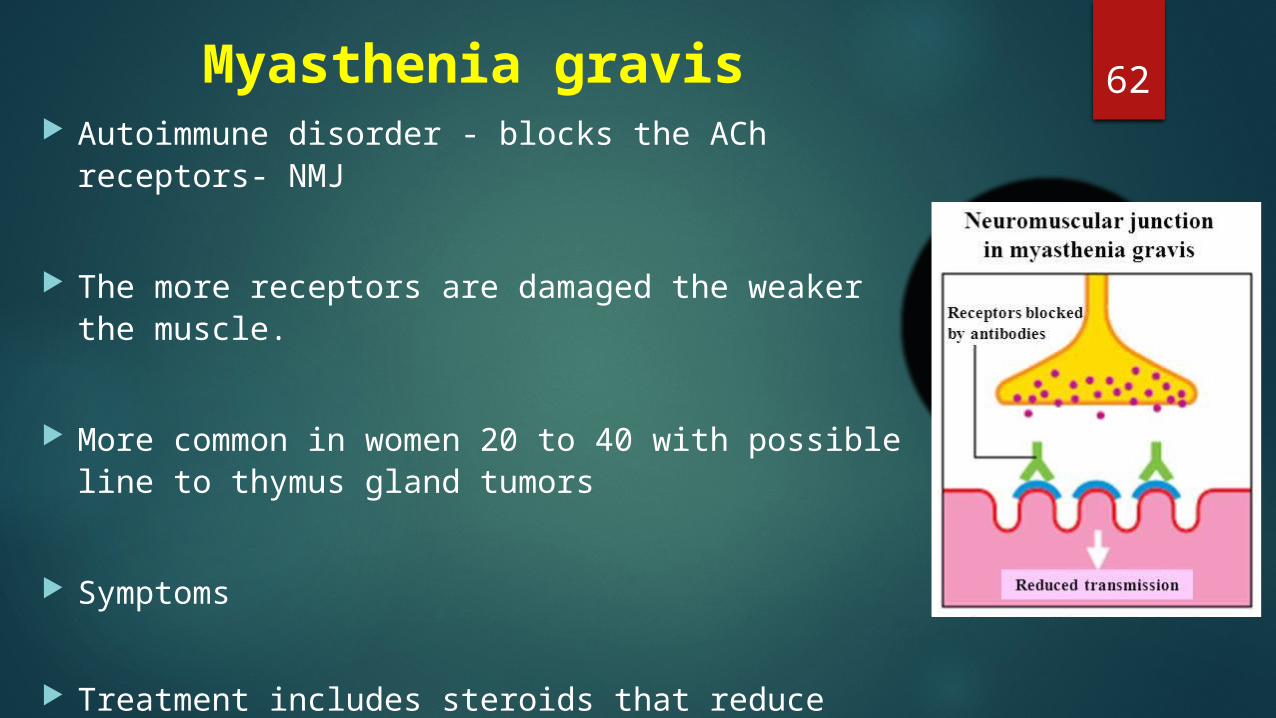
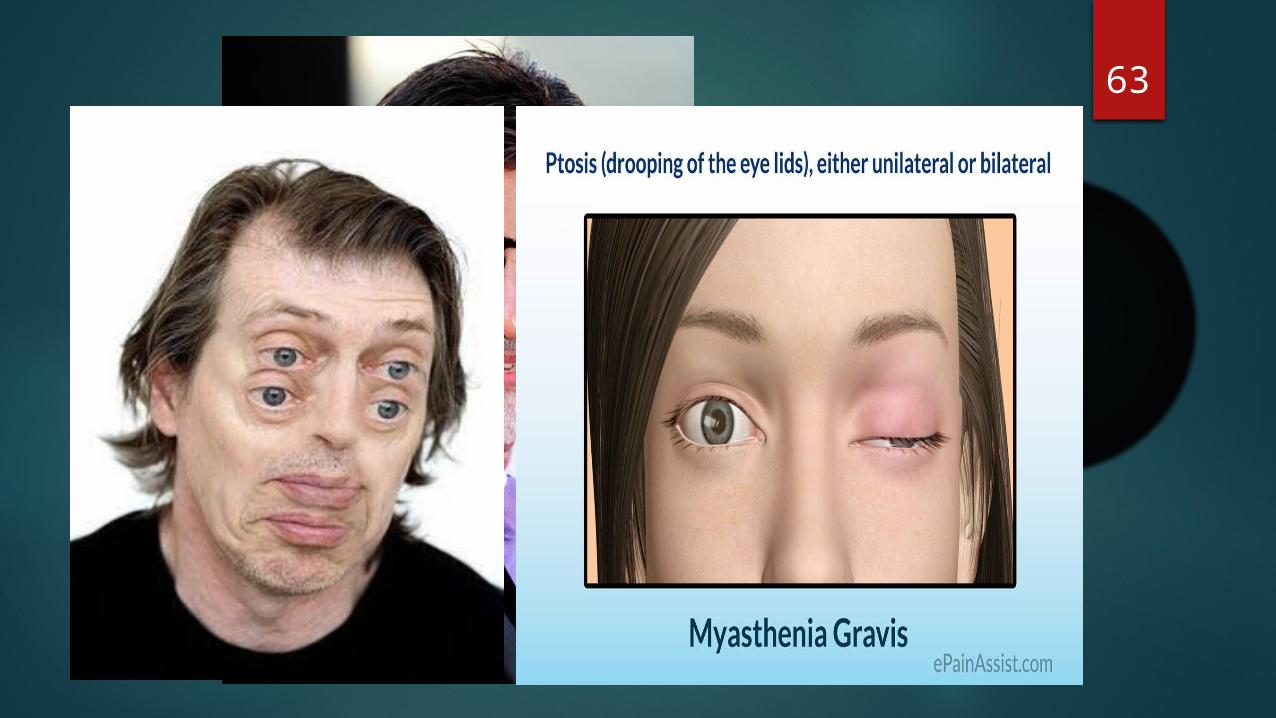
62Myasthenia gravis Autoimmune disorder - blocks the ACh receptors-
NMJ
The more receptors are damaged the weaker the muscle.
More common in women 20 to 40 with possible line
to thymus gland tumors
Symptoms
Treatment includes steroids that reduce antibodies that bind to ACh receptors and inhibitors of acetylcholinesterase
63
64
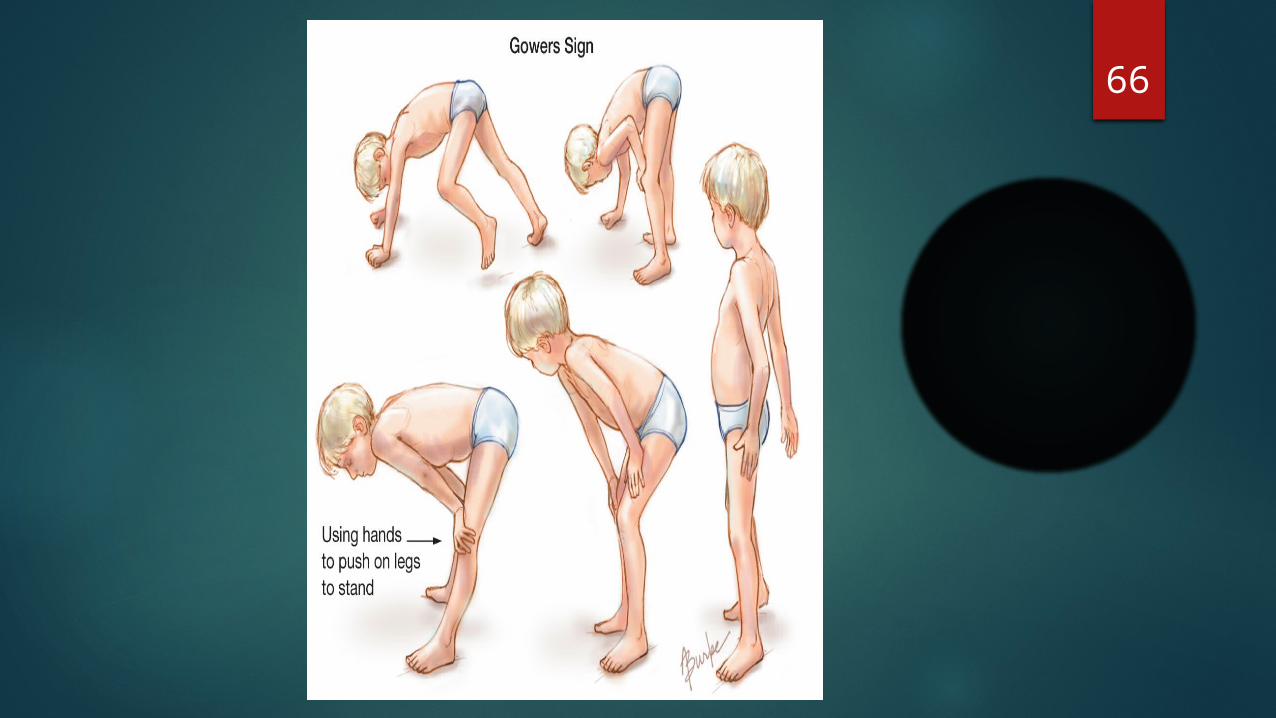
65Muscular Dystrophies Inherited, muscle-destroying diseases Sarcolemma tears during muscle
contraction X linked disease - male Appears by age 5 in males and by 12 may
be unable to walk Degeneration of individual muscle fibers
produces atrophy of the skeletal muscle
66
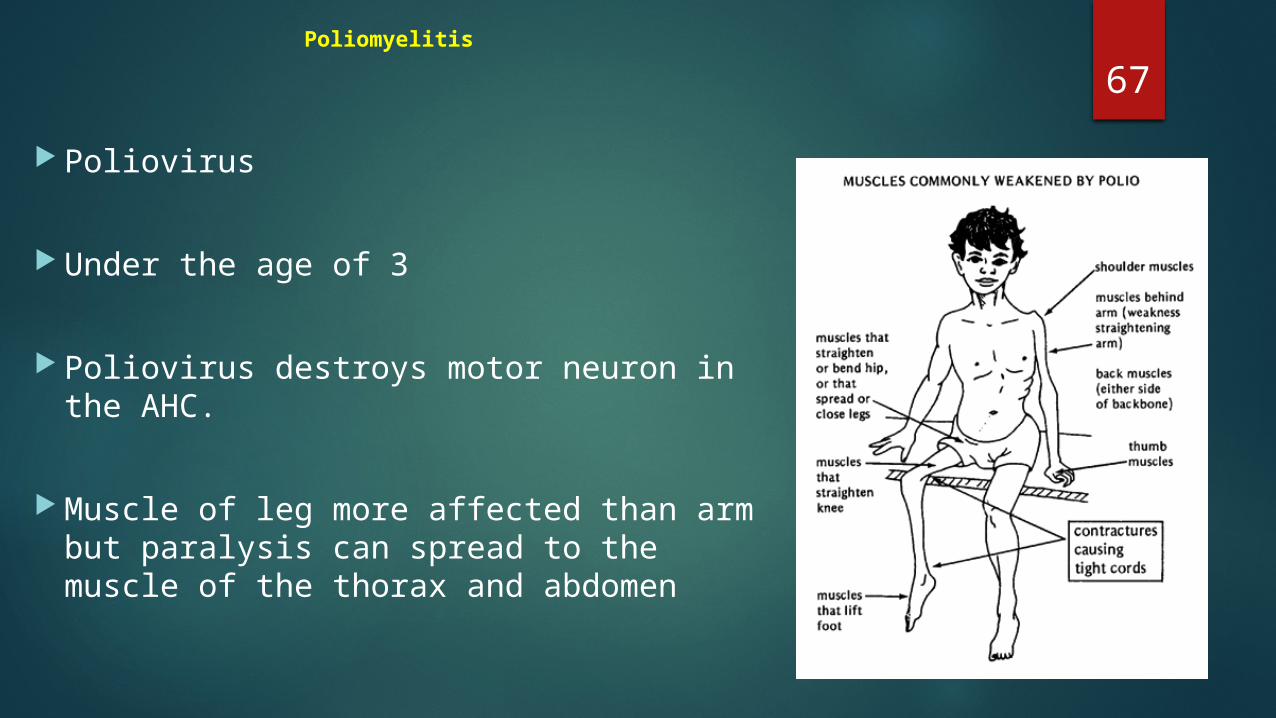
67Poliomyelitis
Poliovirus
Under the age of 3
Poliovirus destroys motor neuron in the AHC.
Muscle of leg more affected than arm but paralysis can spread to the muscle of the thorax and abdomen

68Sports Injuries 5 year study of college football players
indicate:• Mild – 73.5%• Moderate – 21.5%• Severe – 11.6%
A study of 1650 joggers running 27 miles a week reported 1819 injuries in a single year.
69Sports related conditions Bone bruise: bleeding within the periosteum
Bursitis: an inflammation of bursae
Muscle cramps: prolonged,involuntary,and painful muscular contraction
Sprains: tear or break in ligaments or tendons
Strains: tears in muscles
Tendinitis: an inflammation of connective tissue surrounding a tendon
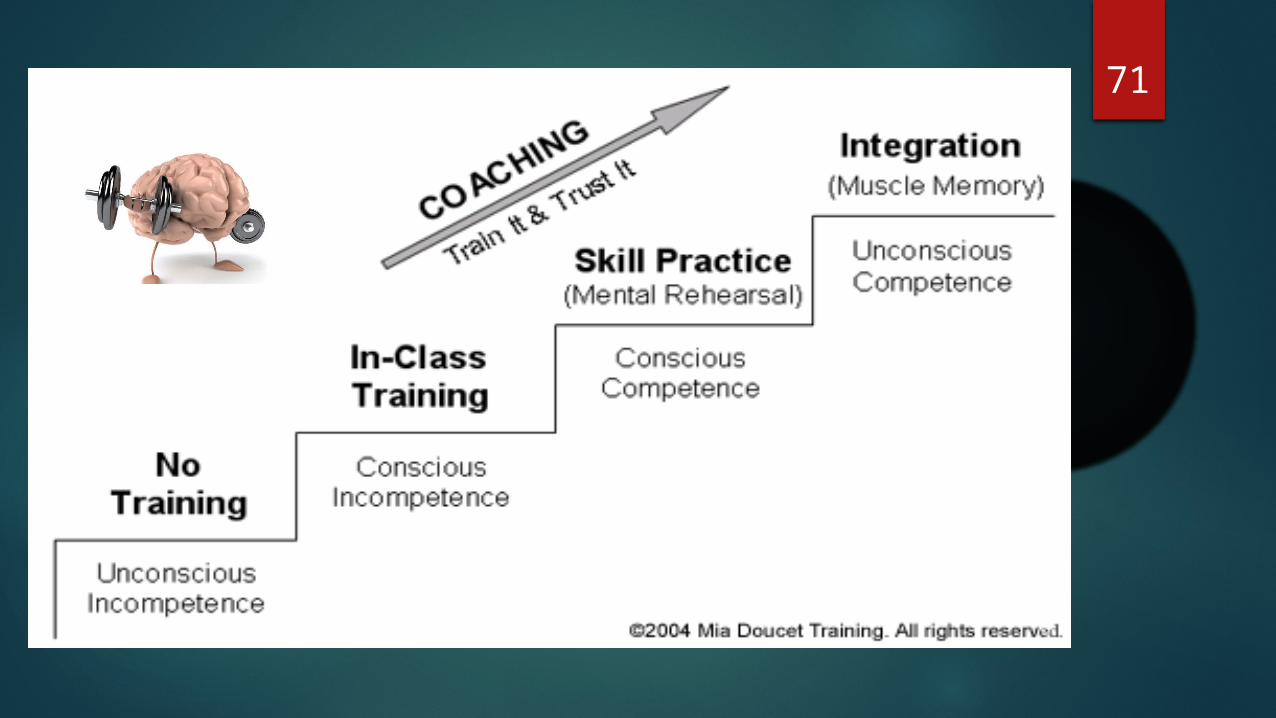
70Muscle Memory
Muscle memory is not a memory stored in your muscles,but memories stored in your brain.
Motor Learning.
Muscle Encoding.
Muscle Re-education or Rehabilitaion.
71
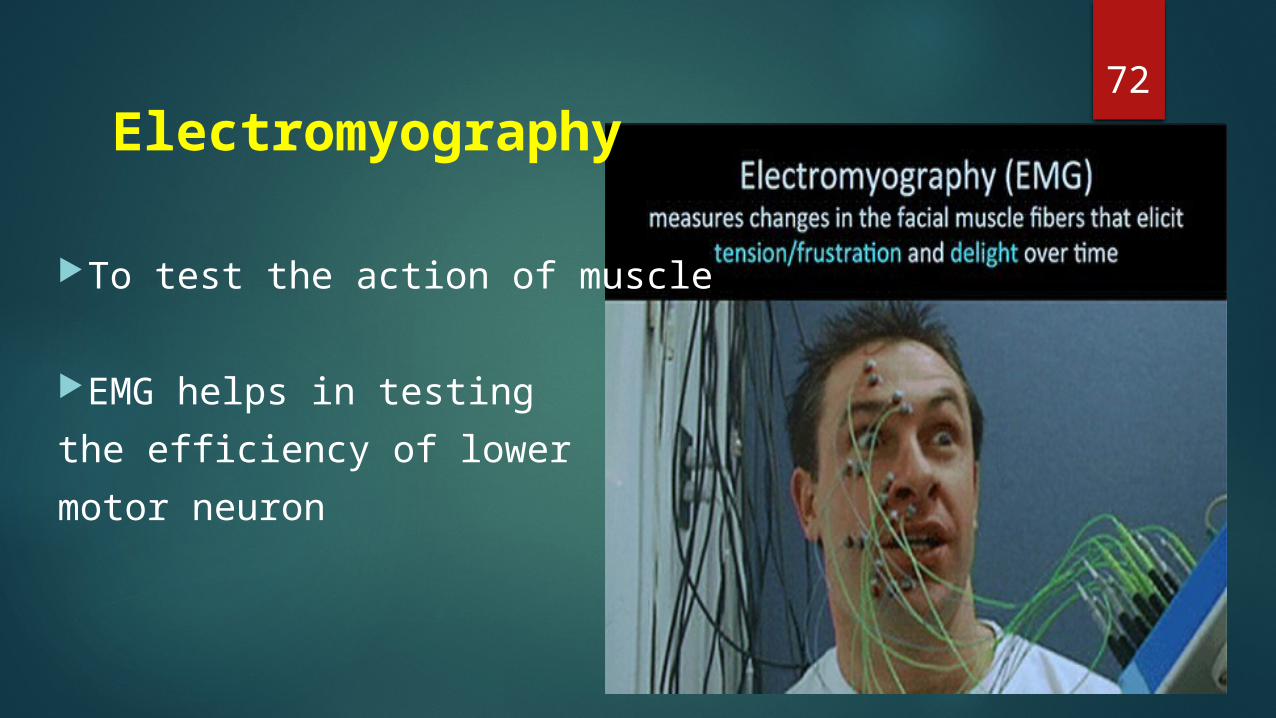
72 Electromyography
To test the action of muscle
EMG helps in testing the efficiency of lower motor neuron
REFERENCES1. Gray’s Anatomy- Susan Standring. 40th Edition. 2. Inderbir singh. Textbook of human histology with color atlas,
2006, 5th edition3. DiFiore’s , Atlas of histology, 12th edition4. Vander’s Human physiology, 12th edition5. Manipal manual of physiology,1st edition6. Principal of general anatomy A.k.datta,7th edition7. General anatomy,B D Chaurasia,4th edition8. Principles of Human Anatomy,Gerard J.Tortora/Mark T.Nielsen,
13th edition9. Gross Anatomy,Kyung Won Chung/Harold M. chung, 6th edition10. A&P ,Applications Manual ,Martini &Welch
73

74