Skeletal Muscle Degenerative Diseases and Strategies for ...
37
Skeletal Muscle Degenerative Diseases and Strategies for Therapeutic Muscle Repair Mohammadsharif Tabebordbar, 1 Eric T. Wang, 2 and Amy J. Wagers 1, 3, ∗ 1 Department of Stem Cell and Regenerative Biology, Harvard University and Harvard Stem Cell Institute, Cambridge, Massachusetts 02138; email: [email protected], [email protected] 2 Department of Biology, Massachusetts Institute of Technology, Cambridge, Massachusetts 02139; email: [email protected] 3 Howard Hughes Medical Institute, Cambridge, Massachusetts 02138 Annu. Rev. Pathol. Mech. Dis. 2013. 8:441–75 First published online as a Review in Advance on November 1, 2012 The Annual Review of Pathology: Mechanisms of Disease is online at pathol.annualreviews.org This article’s doi: 10.1146/annurev-pathol-011811-132450 Copyright c 2013 by Annual Reviews. All rights reserved ∗ Corresponding author. Keywords myogenesis, muscular dystrophy, sarcopenia, cell therapy, gene therapy, muscle regeneration Abstract Skeletal muscle is a highly specialized, postmitotic tissue that must with- stand chronic mechanical and physiological stress throughout life to maintain proper contractile function. Muscle damage or disease leads to progressive weakness and disability, and manifests in more than 100 different human disorders. Current therapies to treat muscle degen- erative diseases are limited mostly to the amelioration of symptoms, although promising new therapeutic directions are emerging. In this review, we discuss the pathological basis for the most common muscle degenerative diseases and highlight new and encouraging experimental and clinical opportunities to prevent or reverse these afflictions. 441 Annu. Rev. Pathol. Mech. Dis. 2013.8:441-475. Downloaded from www.annualreviews.org by Harvard University on 02/02/13. For personal use only.
Transcript of Skeletal Muscle Degenerative Diseases and Strategies for ...

PM08CH17-Wagers ARI 17 December 2012 8:58
Skeletal Muscle DegenerativeDiseases and Strategies forTherapeutic Muscle RepairMohammadsharif Tabebordbar,1 Eric T. Wang,2
and Amy J. Wagers1,3,∗
1Department of Stem Cell and Regenerative Biology, Harvard University and Harvard StemCell Institute, Cambridge, Massachusetts 02138; email: [email protected],[email protected] of Biology, Massachusetts Institute of Technology, Cambridge, Massachusetts02139; email: [email protected] Hughes Medical Institute, Cambridge, Massachusetts 02138
Annu. Rev. Pathol. Mech. Dis. 2013. 8:441–75
First published online as a Review in Advance onNovember 1, 2012
The Annual Review of Pathology: Mechanisms ofDisease is online at pathol.annualreviews.org
This article’s doi:10.1146/annurev-pathol-011811-132450
Copyright c© 2013 by Annual Reviews.All rights reserved
∗Corresponding author.
Keywords
myogenesis, muscular dystrophy, sarcopenia, cell therapy, genetherapy, muscle regeneration
Abstract
Skeletal muscle is a highly specialized, postmitotic tissue that must with-stand chronic mechanical and physiological stress throughout life tomaintain proper contractile function. Muscle damage or disease leadsto progressive weakness and disability, and manifests in more than 100different human disorders. Current therapies to treat muscle degen-erative diseases are limited mostly to the amelioration of symptoms,although promising new therapeutic directions are emerging. In thisreview, we discuss the pathological basis for the most common muscledegenerative diseases and highlight new and encouraging experimentaland clinical opportunities to prevent or reverse these afflictions.
441
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
Sarcolemma:specialized cellmembrane of skeletalmuscle fibers
ECM: extracellularmatrix
Satellite cells: adultskeletal muscle stemcells located betweenthe sarcolemma andthe basal lamina
Sarcoplasm: musclefiber cytoplasm
Sarcoplasmicreticulum (SR):specializedendoplasmic reticulumof skeletal musclefibers
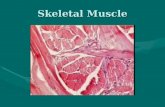
SKELETAL MUSCLE:COMPOSITION, STRUCTURE,AND FUNCTIONSkeletal muscle is composed of thousands ofmuscle fibers, which are bundled together andattached to the skeleton by tendons (Figure 1).Skeletal muscle fibers (myofibers) are multi-nucleated and form during development bythe fusion of mononucleated myoblasts. My-ofibers are surrounded by a specialized plasmamembrane, the sarcolemma, which transducessignals from motor neurons and other externalstimuli into muscle fibers. Myofibers aresurrounded by a layer of extracellular matrix(ECM) known as the basement membrane,which is composed of both an internal basallamina and an external reticular lamina (1). Thebasal lamina associates closely with the sar-colemma, providing a protective niche in whichmuscle regenerative cells (satellite cells) reside.Satellite cells are unipotent adult stem cells
Satellite cells Sarcolemma
Myofibril
Muscle fiber
I-bandH-band
Bundle of muscle fibers
A-band
Sarcomere
Myosin Actin
Z-line
M-lineT-tubulesSarcoplasmicreticulum
Figure 1Skeletal muscle structure and composition. Skeletal muscle is composed of numerous bundles of muscle fibers. Each bundle consists ofmultiple fibers, and individual fibers encompass many myofibrils. Sarcomeres are the structural units of myofibrils and are made up ofactin and myosin filaments. Abbreviation: T-tubule, transverse tubule.
that are activated in response to severe muscledamage to proliferate and differentiate, therebyforming myoblasts that can rebuild the musclethrough fusion with one another or with resid-ual myofibers. Satellite cells also possess potentself-renewal capacity, which ensures theirpersistence within the muscle and preservesthe muscle’s ability to repair after injury.
The calcium-dependent contraction ofmuscle fibers requires a specialized cytoplasm(sarcoplasm) and modified endoplasmic retic-ulum (ER) [sarcoplasmic reticulum (SR)].Transverse tubules (T-tubules) invaginatethe sarcolemma to properly transduce actionpotentials and activate the SR (Figure 1). My-ofibers contain abundant myofibrils, which actas contraction units and are surrounded by SR.Myofibrils are composed of thin myofilaments(actin) and thick myofilaments (myosin) whosecalcium-dependent movement relative to oneanother produces muscle contraction. The
442 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
Transverse tubules(T-tubules):invaginations of thesarcolemma that enterthe muscle fiberperpendicular to thelong axis of the fiber
Myofibril:contraction unit ofmuscle fiber,composed of actin andmyosin filaments
Sarcomere: structuralunit of the myofibril
DGC: dystrophin-glycoproteincomplex
Ischemia: lack ofblood supply to tissues
organization of myofilaments into myofibrilsunderlies the normally striated appearance ofskeletal muscle under light microscopy; thinfilaments make up the light band (I-band), andthick filaments make up the dark band (A-band)(Figure 1). The Z-line defines the borders ofeach sarcomere, which is the structural unit ofthe myofibril (2).
Muscle contraction is induced by depolar-ization of the sarcolemma via action potential.This depolarization opens sarcoplasmic cal-cium release channels, increasing the intracellu-lar calcium concentration and triggering actin-myosin-mediated contraction of sarcomeres.Protein assemblies known as costameres, whichconsist mainly of proteins contained withinthe dystrophin-glycoprotein complex (DGC)(3) and the integrin-vinculin-talin complex (4),transmit contraction forces from muscle fibersto the ECM and, eventually, to neighboringmyofibers. Costameres align with the Z-line ofperipheral myofibrils and physically link my-ofibrils to the sarcolemma.
SKELETAL MUSCLE INJURYAND REGENERATION
Mechanisms of Muscle Injury:Acute Muscle Damage
Acute damage to skeletal muscle can occur byphysical or chemical insult. For example, sharpor blunt trauma, or excessively hot or coldtemperatures, induces rapid myofiber necro-sis. Likewise, envenomation by snakes or beescauses acute myonecrosis. Such venoms containlow-molecular-mass myotoxins (crotamine andmyotoxin a) (5), phospholipases A2 (PLA2s)(6) and membrane-active cardiotoxins (7); beevenom alone contains melittin (8). All of thesetoxins cause depolarization and contraction ofmyofibers, and all except the low-molecular-mass myotoxins induce lysis of the sarcolemma(9). In contrast, PLA2s disrupt sarcolemmal in-tegrity by hydrolysis of glycerophospholipids.Such membrane disruption provokes calciuminflux, leading to hypercontraction, mitochon-drial calcium overload, and activation of cy-tosolic calcium-dependent PLA2s and calpains
(10). Myogenic satellite cells, nerves, and bloodvessels appear unaffected by PLA2s (10). Inaddition, the basal lamina remains intact af-ter envenomation, although some myotoxic andneurotoxic PLA2s may induce degeneration ofnerve terminals (11, 12).
Cardiotoxins are single-chain small poly-peptides that form pores in the muscle mem-brane (13). Myonecrosis induced by cardiotoxinand melittin involves rapid lysis of the sar-colemma and hypercontraction of sarcomeresfollowing calcium influx (14). Muscle necro-sis resulting from low-molecular-mass basicmyotoxins is much slower and is caused bythe induction of sodium influx via voltage-sensitive sodium channels in the sarcolemma.This sodium influx causes membrane depolar-ization, muscle contraction, and vacuolizationof the SR. Nevertheless, these myotoxins causeno apparent sarcolemma or transverse tubuledamage (15).
Ischemia/reperfusion also causes acute mus-cle damage. Prolonged periods of zero bloodflow, which occur during organ-transplantationsurgery, stroke, and hypovolemic shock, in-duce muscle dysfunction through the loss ofcellular energy supplies and accumulation ofpotentially toxic tissue metabolites. Restora-tion of blood flow is essential to the rescueof ischemic muscle; however, reactive oxygenspecies (ROS) produced during reperfusionexacerbate tissue injury by directly damagingcellular macromolecules and promoting theinfiltration of inflammatory leukocytes (16).Oxygen insufficiency during ischemia convertscellular metabolism to anaerobic pathways, ini-tiating a cascade of reactions that generate largequantities of superoxide and other free radicals(17) and increase intracellular calcium concen-trations. Calcium levels are further elevated fol-lowing reperfusion, causing the activation ofcalpain and phospholipases. These molecules,in turn, can trigger proinflammatory media-tor synthesis and leukocyte chemoattraction(18), which further damage the muscle throughrelease of reactive oxygen and proteases, com-plement activation, and increased vascular per-meability (19).
www.annualreviews.org • Skeletal Muscle Disease and Therapy 443
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
IMs: inflammatorymyopathies
Inflammation:a complex response bythe immune systemevoked by tissue injuryand often involved ininitiating the healingprocess
PM: polymyositis
sIBM: sporadicinclusion bodymyositis
NAM: necrotizingautoimmune myositis
CK: creatine kinase
Mechanisms of Muscle Injury:Contraction-Induced Damage
Contraction of skeletal muscle can cause short-ening (concentric contraction), lengthening(eccentric contraction), or no change (isomet-ric contraction) of muscle length. Concentriccontractions initiate movements, and eccentriccontractions slow or stop them. During eccen-tric contraction, the opposing force exceedsthe force generated by the muscle, leadingto its elongation. Contraction-induced injuryis most severe during eccentric contractions.Electron microscopy reveals regions of overex-tended sarcomeres or half-sarcomeres, Z-linestreaming and regional disorganization ofmyofilaments, and T-tubule damage in my-ofibers after lengthening contraction (20, 21).Weaker sarcomeres are overstretched duringeccentric contraction, and repeated overexten-sion of sarcomeres leads to their disruption.Disruption of multiple sarcomeres causesmembrane damage, beginning with tearingof T-tubules and degradation of membranecomponents involved in excitation-contractioncoupling (22). Increased intracellular calcium,promoted by damage to the SR or inductionof stretch-activated channels, further drivesmuscle contractile protein degradation, as wellas mitochondrial swelling and SR vacuolization(23). Depending on the extent of contraction-induced damage, myofiber necrosis may occur,which leads to a local inflammatory responseassociated with tissue edema and soreness.
Mechanisms of Muscle Injury:Inflammatory Myopathy
Inflammatory myopathies (IMs) representthe largest group of acquired and potentiallytreatable myopathies in people (24). Thisheterogeneous group of subacute, chronic, orsometimes acute muscle diseases commonlyinvolves muscle weakness and inflammation,revealed in muscle biopsies (25). Four differenttypes of IMs have been identified by histologi-cal, immunopathological, and clinical manifes-tations: dermatomyositis, polymyositis (PM),
sporadic inclusion body myositis (sIBM), andnecrotizing autoimmune myositis (NAM) (26).
Complement activation and the formationof membranolytic attack complexes that dam-age endothelial cells of the endomysial capillar-ies are two of the earliest events in dermato-myositis (27). Autoantibodies directed againstendothelial cells may activate the complementsystem, causing endothelial cell lysis, perivas-cular inflammation, capillary destruction, andmuscle ischemia (25). Thus, dermatomyositisdecreases capillary density in the muscle, caus-ing dilation of the remaining vessels, which at-tempt to compensate for the ischemic condi-tion (28). Complement activation also triggersthe expression of proinflammatory cytokinesand the recruitment of CD4+ T cells, B cells,macrophages, and plasmacytoid dendritic cellsto muscle (29, 30).
A common feature in the immunobiologyof PM and sIBM is the ubiquitous expres-sion of major histocompatibility complex 1(MHC-1) antigen, which is normally unde-tectable on muscle fibers (31). CD8+ cytotoxicT cells attack MHC-1-expressing myofibers,causing fiber lesions. Spike-like processes fromCD8+ cells and macrophages may also extendacross the myofiber basal lamina and com-press the fibers (32). Furthermore, perforin andgranzyme, released from CD8+ cells, promotemyofiber necrosis (33). Although there are sig-nificant immunobiological similarities betweenPM and sIBM, sIBM is additionally character-ized by the presence of a strong degenerativeprocess that involves rimmed vacuoles and in-tracellular deposition of β-amyloid and relatedmolecules (34). Other degenerative phenomenain sIBM myofibers include an induced unfoldedprotein response, lysosome and mitochondrialabnormalities, and ER stress (34).
NAM is the least understood of the IMs.Macrophages are thought to be responsible forfiber necrosis in this disease, which causes highcreatine kinase (CK) levels in patients’ blood.Neither infiltration of T cells nor expression ofMHC-1 on muscle fibers has been detected inNAM (26); however, some patients harbor au-toantibodies against signal recognition peptide,
444 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
Muscular dystrophy:a heterogeneous groupof inherited muscledegenerative diseases
which implies an antibody-mediated cause ofthe disease (35). Macrophage recruitment alsosupports antibody-dependent cell-mediated cy-totoxicity in NAM. Although there have beencases of patients with cancer or active viral in-fection (e.g., HIV), it is unclear whether NAMcan be triggered by these factors or not (24).
Mechanisms of Muscle Regeneration:Membrane Patch
Many eukaryotic cell types can repair mi-nor membrane disruptions and restore plasmamembrane integrity. Physiological disruptionsto the plasma membrane occur frequently inskeletal muscle (36), and defects in mem-
brane resealing can cause muscular dystrophy(37). The membrane repair process involvescalcium-dependent exocytosis of intracellularvesicles, such as lysosomes and enlargeosomes,which form a membrane “patch” (Figure 2)(38, 39). Dysferlin, a protein that is presentpredominantly at the muscle surface and incytoplasmic vesicles, is also a critical compo-nent in membrane repair (37); however, themechanism underlying dysferlin’s involvementin this process remains poorly understood. Dys-ferlin may function as a calcium sensor, regulat-ing vesicle-vesicle and vesicle-membrane fusionduring membrane repair (40). Dysferlin also in-teracts with annexins A1 and A2 (41). AnnexinA1 is required for membrane repair in HeLa
a b
d c
Calcium
Sarcolemma
Calpain
Annexin A1
Dysferlin
Annexin A2
SHMG53
SH
SH
SH
SH SH
SH
SH
SHS
SS
SH
S S
SHSHS S
Activatedcalpain
Cleavage?
Oxidative agents
Cytoskeleton
Figure 2Model for mechanism of membrane patching in muscle fibers. (a) In the intact muscle fiber, Mitsugumin 53 (MG53) is on sarcoplasmicvesicles in a reduced form, and the concentration of calcium in sarcoplasm is lower than in the extracellular matrix. (b) Upon membranedamage, exposure of the intracellular environment to oxidative agents leads to oxidation and oligomerization of MG53 proteins onsarcoplasmic vesicles. Increased calcium concentration around the injury site also activates calpain. Activated calpain may cleaveannexin proteins, which subsequently mediate accumulation of vesicles near the site of damage. (c) Dysferlin senses the calcium thatfloods into the fiber and triggers fusion of accumulated vesicles. Activated calpain also degrades the cytoskeleton near the damaged area,making it easier for vesicles to fuse with plasma membrane. (d ) Vesicles fuse with the sarcolemma and form a patch that seals themembrane. Abbreviation: SH, reduced sulfur moieties in MG53. Modified from Reference 262.
www.annualreviews.org • Skeletal Muscle Disease and Therapy 445
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
cells (42), but its mechanism of action is cur-rently unclear. Binding of annexins to phos-pholipids in the presence of calcium, togetherwith their ability to aggregate vesicles in vitroand interact with actin, fueled speculation abouttheir involvement in vesicle-vesicle fusion andvesicle movement (43). In addition to trigger-ing vesicle fusion, calcium influx after mem-brane injury also activates calpain, which like-wise is necessary for membrane repair (44, 45)and may mediate the disassembly of the dam-aged actin cytoskeleton through degradation ofcytoskeletal proteins such as talin and vimentin.Annexins are also proteolytic targets of calpain,and calpain-mediated cleavage of annexins maybe critical for membrane repair (46). Recently,Mitsugumin 53, a muscle-specific tripartite mo-tif family protein (TRIM72) that is present onthe sarcolemma and intracellular vesicles, wasimplicated in nucleating the assembly of therepair machinery at injury sites (47, 48). Thisprocess is independent of calcium influx andtriggered by changes in the intracellular oxida-tive environment (48). Figure 2 presents a sim-plified model of our current understanding ofmembrane patching in skeletal myofibers.
Mechanisms of Muscle Regeneration:Muscle Satellite Cells
Satellite cells are mononuclear cells with ahigh nucleus-to-cytoplasm ratio; they were firstidentified in electron micrographs on the ba-sis of their distinct anatomical position be-tween the sarcolemma and the basal laminaof muscle fibers (49). Satellite cells representthe endogenous source of muscle progenitorcells and account for the regenerative poten-tial of adult muscle (50). Considering the infre-quent turnover of myonuclei in adult muscle,satellite cells remain mitotically and metaboli-cally quiescent through most of life. However,satellite cells are activated after muscle injuryand in the context of chronic degenerative dis-eases (see the section titled Muscle Degenera-tive Diseases) (51–53). Damage to skeletal mus-cle results in the release of growth factors (GFs)and cytokines, such as hepatocyte growth fac-
tor; epidermal growth factor; platelet-derivedgrowth factor BB; and members of the insulin-like growth factor (IGF) and fibroblast growthfactor family (54, 55) from the ECM (56), my-ofibers, endothelial cells, interstitial cells (57),and leukocytes (58). Interaction among theseGFs and receptors on quiescent satellite cellstriggers satellite cell proliferation.
Quiescent satellite cells express variousproteins, including Pax7, CD34, c-met, M-cadherin, syndecan-3, and syndecan-4 (59–61),that are important for their activation and pro-liferation in response to muscle damage (62).Activated satellite cells downregulate Pax7 ex-pression and increase synthesis of the earlymyogenic regulatory factors MyoD and Myf5(63). These activated cells undergo a rapid pro-liferation stage regulated in part by Notch sig-naling (64). Notch inhibition and activationof Wnt signaling can induce the progressionof muscle satellite cells along the myogeniclineage to promote the production of fusion-competent myoblasts (65) and trigger the ex-pression of late myogenic regulatory factors,including myogenin. Fusion of terminally dif-ferentiated myoblasts into myofibers marks thefinal stage of muscle regeneration.
Efficient repair of skeletal muscle after re-peated injuries indicates that satellite cellsmust be replenished after muscle regeneration.Genetic fate-mapping studies strongly impli-cate satellite cells themselves as the endoge-nous source of such cell replacement; how-ever, the mechanisms regulating satellite cellself-renewal are not fully understood. Somereports suggest that nonrandom segregationof DNA strands or asymmetric distribution ofNumb, an inhibitor of Notch signaling, in thedaughters of dividing satellite cells (66, 67) maydrive asymmetric division of satellite cells andpreservation of the satellite cell pool. A re-cent study (68) provided evidence suggestingthat asymmetric division in satellite cells ex-pressing high levels of Pax7 causes segrega-tion of template DNA to daughter cells with amore immature phenotype, whereas daughtersinheriting newly synthesized DNA acquire amore differentiated phenotype. This study also
446 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
a Homeostasis b Degeneration
Inflammation
c Regeneration d
Damage RepairSatellite cellactivation
Musclefibers
Bloodvessel
Figure 3Mechanisms of satellite cell activation and regulation during muscle repair. (a) During homeostasis, satellite cells ( green) reside in closeassociation with muscle fibers (red ). Resting muscle also contains resident fibro-adipogenic precursors [FAPs ( purple)]. (b) Damage tomuscle induces myofiber degeneration and inflammation, beginning with infiltration by neutrophils and M1 macrophages (dark yellow)from blood vessels (red oval ). (c) During the regenerative phase, elaboration of growth factors and cytokines by muscle fibers,infiltrating M2 macrophages (light yellow) and activated FAPs ( purple with yellow border) activate satellite cells ( green with yellow border) toproliferate and differentiate to form myoblasts (orange ovals with yellow border) that exit the cell cycle and fuse with one another and withresidual myofibers to replenish myofibers as well as the satellite cell pool (d ).
FAPs:fibro-adipogenicprecursors
demonstrated that satellite cells harboring lowlevels of Pax7 exhibit random segregation ofDNA strands during mitosis (68). Myostatin,a member of the transforming growth factor(TGF)-β superfamily, may also promote satel-lite cell quiescence, given the increased percent-age of activated and proliferating satellite cellsin myostatin-null mice (69) and the involve-ment of the myostatin antagonist, follistatin, inmyoblast fusion (70). However, direct analysesof postnatal satellite cells in mice suggest thatthese cells lack expression of myostatin recep-tors and that they fail to respond to exogenousmyostatin in ex vivo proliferation assays (71).
In addition to soluble GFs and cytokines,satellite cell function is also regulated by in-filtrating and interstitial cell populations, in-cluding recruited inflammatory cells (72) andresident fibro-adipogenic precursors (FAPs)(Figure 3) (73, 74). The impact of inflamma-tory cells on muscle repair is quite complex.In the absence of any recruited immune cells,satellite cell regenerative activity appears to beblocked (72); however, as discussed above, anoverexuberant or unbalanced immune responsecan lead to myopathic tissue destruction that isnot recoverable through satellite cell–mediatedrepair processes. Neutrophils appear to be the
first immune cells recruited to damaged muscle(75). Their recruitment signals subsequent in-filtration by M1 macrophages, followed by M2macrophages (76, 77). M1 macrophages are ef-ficient inducers and effectors of inflammatoryprocesses, whereas M2 macrophages are moreoften involved in tissue repair, remodeling, andimmunoregulation (78). Both neutrophils andmacrophages participate in the clearance of my-ofiber debris at the injury site and in the produc-tion of inflammatory and immune-regulatorycytokines, but macrophages (particularly M2macrophages) appear to have an additional,unique function in directly regulating muscleregeneration through induction of satellite cellactivation and myoblast proliferation (79–81).
In addition to recruited immune cells,muscle-resident mesenchymal cells also appearto be critical for proper muscle repair. Forexample, skeletal muscle contains a uniquepopulation of Sca-1-expressing precursor cells,which can differentiate to form fibroblasts(82) and white or brown adipocytes (73, 83).Although these FAPs exhibit no intrinsicmyogenic activity, they are potent inducers ofmyogenesis by satellite cells (Figure 3) (73, 74).Intriguingly, whereas undifferentiated FAPspromote myofiber formation, the presence
www.annualreviews.org • Skeletal Muscle Disease and Therapy 447
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
of differentiated myofibers appears to inhibitFAP-mediated adipogenesis (74). Althoughthe exact mechanisms by which this functionalcross-antagonism is accomplished remain tobe determined, studies have suggested a rolefor paracrine signaling [by soluble mediatorssuch as IGF-1, Wnts, and interleukin (IL)-6]between FAPs and muscle satellite cells inthe FAP-dependent promotion of myogenesis(73). In contrast, cocultures of FAPs with dif-ferentiated myotubes implicate direct cell-cellinteraction in the inhibition of FAP-mediatedadipogenesis by muscle fibers (74). Thus, inaddition to alterations in satellite cell numberand intrinsic signaling responses, numerousnon-cell-autonomous inputs clearly influencethe extent and efficacy of satellite cell–mediatedmuscle repair.
MUSCLE DEGENERATIVEDISEASES
Genetic Diseases of Skeletal Muscle:Duchenne and Becker MuscularDystrophies
Duchenne muscular dystrophy (DMD) is themost common X-linked genetic disorder inhumans; it affects one in 3,500 males. Mostboys with DMD manifest symptoms within thefirst years of life. Progressive muscle weaken-ing delays walking and causes repeated falls,leaving patients wheelchair bound, typically by∼12 years of age. Most patients experience pre-mature death due to respiratory or cardiovas-cular failure in the second decade. Mutations inthe dystrophin gene leading to genetic frameshiftor loss of expression and complete absenceof protein function are the cause of DMD(Table 1) (84). Dystrophin extends over 2.4 Mbof the X chromosome and represents the largestgene in the human genome. Point mutations indystrophin are responsible for ∼40% of DMDcases; the remaining ∼60% are caused by largedeletions or duplications in this gene (85).
Dystrophin is a structural protein, a com-ponent of the DGC (Figure 4) (86), and anessential part of the costamere. Dystrophin’s
primary function is to link the myofiber cy-toskeleton to the ECM and thereby stabilizethe sarcolemma (87). Dystrophin binds cyto-plasmic actin through its amino terminus as wellas its rod-shaped domain, which is composedof 24 spectrin repeats and four hinge points(88). The C-terminal cysteine-rich domain ofdystrophin directly binds to transmembrane β-dystroglycan protein. β-Dystroglycan is linkedto the highly glycosylated α-dystroglycan(αDg), which completes the connection be-tween the myofiber cytoskeleton and ECMby interacting with laminin in the basal lam-ina (89). Absence of functional dystrophinprotein destabilizes the DGC, increasingthe susceptibility of dystrophic muscle fibersto contraction-induced injury (90). Increasedcytosolic calcium following mechanical stress,activation of proteases (particularly calpains),destruction of membrane constituents, and ul-timately myofiber necrosis occur frequently indystrophic muscles. Thus, satellite cells in thesepatients must support repeated rounds of re-generation in an attempt to compensate fordamage. As the disease advances, satellite cellsshow reduced capacity for muscle regenera-tion, possibly due to proliferation-induced re-ductions in telomere length (91) or damage-associated cell attrition (92). Absent an adequatemuscle regenerative response, fat and fibrotictissue replace muscle fibers, leading to furtherweakening and wasting (93).
In addition to mechanical stress, other sec-ondary mechanisms induce damage in dys-trophic muscle. Loss of functional dystrophinleads to reduced expression and mislocalizationof neuronal nitric oxide synthase (nNOS) fromthe sarcolemma (Figure 4) (94). Absence ofnNOS signaling impairs blood supply to con-tracting muscles, exposing dystrophic musclesto continuous ischemic insult (95). Various im-mune cells are also recruited to the dystrophicmuscle as a result of persistent damage; thesecells can cause secondary damage through in-flammatory responses and elaboration of ROS(96).
Like DMD, Becker muscular dystrophy(BMD) is also caused by mutations in dystrophin;
448 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
Table 1 Causative genetic lesions in inherited muscle degenerative diseases
Disease name Protein (gene); disease subtypeDuchenne muscular dystrophy(DMD) and Becker musculardystrophy (BMD)
Dystrophin (DMD)
Myotonic dystrophy (DM) Dystrophia myotonica protein kinase (DMPK); DM1Zinc-finger nuclease 9 (ZFN9/CNBP); DM2
Limb girdle muscular dystrophy(LGMD)
Myotilin (MYOT ); LGMD1ALamins A and C (LMNA); LGMD1BCaveolin-3 (CAV3); LGMD1CCalpain-3 (CAPN3); LGMD2ADysferlin (DYSF); LGMD2Bγ-Sarcoglycan (SGCG); LGMD2Cα-Sarcoglycan (SGCA); LGMD2Dβ-Sarcoglycan (SGCB); LGMD2Eδ-Sarcoglycan (SGCD); LGMD2FTelethonin (TCAP); LGMD2GTripartite motif–containing 32 (TRIM32); LGMD2HFukutin related protein (FKRP); LGMD2ITitin (TTN); LGMD2JProtein-O-mannosyltransferase 1 (POMT1); LGMD2KAnoctamin 5 (ANO5); LGMD2LFukutin (FCMD); LGMD2MProtein-O-mannosyltransferase 2 (POMT2); LGMD2NProtein O-linked mannose β1, 2-N-acetylglucosaminyltransferase (POMGnT1); LGMD2ODystroglycan (DAG1); LGMD2P
Emery–Dreifuss muscular dystrophy(EDMD)
Emerin (EMD); X-linked EDMDLamins A and C (LMNA); autosomal EDMDNesprin-1 (SYNE1)Nesprin-2 (SYNE2)
Congenital muscular dystrophy(CMD)
Fukutin-related protein (FKRP); Walker–Warburg syndrome (WWS), Fukuyama CMD, ormuscle–eye–brain disease
Like-glycosyl transferase (LARGE); WWS, Fukuyama CMD, or muscle–eye–brain diseaseFukutin (FCMD); WWS, Fukuyama CMD, or muscle–eye–brain diseaseProtein-O-mannosyltransferase 1 (POMT1); WWS, Fukuyama CMD, or muscle–eye–brain
diseaseProtein-O-mannosyltransferase 2 (POMT2); WWS, Fukuyama CMD, or muscle–eye–brain
diseaseProtein O-linked mannose β1, 2-N-acetylglucosaminyltransferase (POMGnT1); WWS,
Fukuyama CMD, or muscle–eye–brain diseaseLaminin-2 (LAMA2)Collagen type VI, subunit α1 (COL6A1); Ullrich syndrome or Bethlem myopathyCollagen type VI, subunit α2 (COL6A2); Ullrich syndrome or Bethlem myopathyCollagen type VI, subunit α3 (COL6A3); Ullrich syndrome or Bethlem myopathyIntegrin-α7 (ITGA7), Selenoprotein N1 (SEPN1); rigid spine syndromeLamins A and C (LMNA)
Facioscapulohumeral musculardystrophy (FSHD)
Double-homeobox protein 4 (Dux4); FSHD1A
www.annualreviews.org • Skeletal Muscle Disease and Therapy 449
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
Sarcoglycans BiglycanDystroglycans
Sarcospan
Laminin
Glycan moieties
Collagen
α
βδ
β
αγ
N terminus
F-actin
Dystrophin
nNOSSyntrophins
C terminus
α-Dystrobrevin
Sarcoplasm β
α
Figure 4Dystrophin glycoprotein complex (DGC). Dystrophin connects the muscle fiber cytoskeleton to the extracellular matrix (ECM) viainteraction with actin filaments in the sarcoplasm and β-dystroglycan in the sarcolemma. β-Dystroglycan interacts withα-dystroglycan, which is connected to laminin in the ECM through its glycan moieties. The sarcoglycan-sarcospan complex is also apart of DGC that includes α-, β-, γ-, and δ-sarcoglycans and sarcospan. This subcomplex is connected to the ECM throughinteraction with biglycan. Dystrophin also interacts with α-dystrobrevin and α- and β-syntrophins through its C-terminal domain.Neuronal nitric oxide synthase (nNOS) is localized to the DGC via its interaction with syntrophins.
Myotonia: theinability to relaxmuscles aftercontraction
however, Becker mutations maintain the dys-trophin reading frame. Thus, most BMD pa-tients express a partially functional dystrophinprotein, which lacks the internal spectrin re-peats but contains the critical actin-bindingand C-terminal domains (97). BMD patientsshow a milder phenotype and a more hetero-geneous clinical manifestation of the disease.Some BMD patients remain ambulatory aftertheir forties, and a few can survive more than60 years (98).
Genetic Diseases of Skeletal Muscle:Myotonic Dystrophy
Myotonic dystrophy type 1 [also known as dys-trophia myotonica type 1 (DM1)] was first de-scribed by Hans Steinert in 1909 (99). DM1affects more than 1 in 8,000 individuals world-wide but has an increased incidence (up to 1 in500) in certain populations due to founder ef-fects. DM1 is an autosomal dominant disease
caused by a trinucleotide repeat expansion inthe 3′ untranslated region (3′ UTR) of DMPKon chromosome 19 (100–102). Normal individ-uals have fewer than 30 repeats, and expansionsabove this range can initiate DM symptoms.Age of onset and disease severity appear to cor-relate with repeat expansion length. Typically,expansions greater than 1,000 repeats yield asevere congenital form of DM. DM repeats areunstable over time and across cell types, and re-peat lengths in muscle, heart, brain, and othertissues can significantly exceed those measuredin blood (103).
Although the pathognomonic symptomof DM is myotonia, or the inability to relaxmuscles after contraction, DM affects multiplebody systems and therefore is not exclusively amuscular dystrophy. Additional DM symptomsinclude muscle wasting and weakening, cardiacconduction block, smooth muscle dysfunction,so-called Christmas tree cataracts, insulinresistance, neuropsychiatric abnormalities,
450 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
hypersomnia, fatigue, sleep dysregulation, andtesticular atrophy (99). Muscle wasting oftenoccurs in the distal-to-proximal direction,first affecting hand, face, and tongue muscles,leading to grip weakness, ptosis, and speechdifficulties. Weakness of the tibialis muscleleads to foot drop, and progressive weaknessin all major skeletal muscle groups occurs overtime. Although centralized myofiber nuclei,heterogeneous fiber cross-sectional areas, andfibrosis are commonly observed, regenerationand immune cell infiltration are not; thus, thecentral nuclei are believed to reflect processesthat are unrelated to regeneration. Heartblock in DM can cause atrial fibrillation andoccasionally ventricular tachycardia, makingsudden death a significant risk for DM pa-tients; however, this risk can be mitigated bypacemakers or implantable cardioverter defib-rillators. Smooth muscle dysfunction in DMcan dysregulate gastrointestinal tract motilityand cause gallbladder dysfunction. Executivefunctioning and other central nervous systemfunctions, particularly involving the prefrontalcortex, are also especially affected in DM(99).
The penetrance of symptoms among DMpatients is so wide ranging that it has been de-scribed as the most variable disease known tomankind (99). DM exhibits genetic anticipa-tion, and its pattern of inheritance is similarto that of other microsatellite repeat diseases,such as Huntington’s disease and spinocerebel-lar ataxias. Often, entire families are diagnosedonly after a hypotonic newborn, suffering fromcongenital DM1, inspires a cascade of diagnosesup the family tree (104).
Haploinsufficiency of the DMPK protein,observed in DM1 patient tissue, was initially hy-pothesized to play a central role in DM1 patho-genesis, and epigenetic effects of expanded re-peats on the expression of neighboring geneswere also proposed to play a role (Figure 5).Yet, mice lacking DMPK develop only minorcardiac and muscle defects later in life, dis-tinct from those observed in DM1 patients(105). Discovery of a second type of myotonicdystrophy, DM2, caused by a tetranucleotide
(CCUG) repeat expansion in the first intronof the CNBP gene on chromosome 3q21, pro-vided critical clues about molecular pathogen-esis in DM (106). DM2 is estimated to accountfor less than 10% of all DM cases. Althoughthe phenotype of DM2 patients is not identicalto that of DM1 patients (muscle wasting occursin a proximal-to-distal fashion, and symptomsare generally more mild than in DM1), DM2patients also experience myotonia, cataracts,frontal balding, insulin resistance, and execu-tive functioning difficulties, among other symp-toms. The discovery of DM2, combined withthe observation that nuclei of DM1 and DM2cells contain CUG- or CCUG-rich RNA foci(107, 108), shifted the focus of investigatorsfrom cis to trans mechanisms, and to a modelin which the pathogenic molecule may be theexpanded CUG- or CCUG-containing RNA(Figure 5).
Transgenic mice expressing CUG repeatsin the 3′ UTR of an unrelated gene (humanskeletal actin) in a muscle-specific fashion ex-hibit myotonia, centralized muscle nuclei, andheterogeneous myofiber cross-sectional areas(109). Members of the Muscleblind-like fam-ily of RNA-binding proteins (MBNLs) bind toCUG repeat RNA in a length-dependent fash-ion, and MBNL1 knockout mice exhibit my-otonia and centralized muscle nuclei (110, 111).Furthermore, the introduction of exogenousMBNL1 protein by an adeno-associated virus(AAV) into the muscle of CUG repeat–carryingmice significantly rescued myotonia (112).
The MBNLs were first discovered inDrosophila, where their loss results in defectsin eye and muscle development (113). MBNLscan both repress and activate alternative mRNAsplicing, and their endogenous binding se-quences are similar to those of CUG or CCUGsequences (114). For example, aberrant in-clusion of exon 7a of the chloride channel1 (CLCN1) gene, which contains a prema-ture stop codon and normally is repressed byMBNL, causes degradation and loss of CLCN1at the sarcolemma, leading to myotonia(Figure 5) (115). Loss of MBNLs appears toaccount for ∼80% of the splicing changes in
www.annualreviews.org • Skeletal Muscle Disease and Therapy 451
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
DMPK genomic locus
CLCN1 pre-mRNA
GU C GU C GU C GU C GU C GU C GU C GU C GU C
C UGC UGC UGC UGC UGC UGC UGC UGC UG
(CTG)80–2,500+)80 2,5
DMPK mRNA
Exon 7a
Nonsense-mediated decay,loss of CLCN1, myotonia
Somatic instability
AAAAA...Gppp
MBNLs
Nuclear retention of DMPK mRNA,sequestration of MBNLs,disruption of MBNL-mediatedRNA processing in the nucleus
Stable mRNA,CLCN1
Disruption of MBNL functionsin the cytoplasm
PKC activation,hyperphosphorylation of CELFs,disruption of CELF-mediatedRNA processing in the nucleus
CELFs
Disruption of CELF functionsin the cytoplasm
P–P–
P–
P–
P–
P–
Figure 5Molecular pathogenesis in myotonic dystrophy (type 1). CTG repeat expansions at the DMPK locus are transcribed into RNA andform intranuclear foci with Muscleblind-like family of RNA-binding proteins (MBNLs), leading to nuclear retention of DMPKmessenger RNA (mRNA). MBNLs, which normally regulate precursor mRNA (pre-mRNA) splicing, cannot bind to their normaltargets, causing aberrant alternative splicing patterns and downstream phenotypic consequences, such as myotonia. Through anindependent pathway, CELF proteins are hyperphosphorylated via protein kinase C (PKC) activation.
one mouse model of DM. This finding supportsthe model that expanded CUG/CCUG repeatexpression functionally sequesters MBNLs,which leads to splicing changes that cause DMphenotypes (116). Several MBNL-dependentsplicing events have been proposed to accountfor DM phenotypes, including Bin1 exon 7splicing (muscle wasting) (117), insulin recep-tor exon 11 (insulin resistance) (118), CaV1.1(muscle wasting) (119), and cardiac troponin Texon 5 (cardiac function) (120).
A separate line of investigation indicates thatoverexpression of CUG repeats may stabilize adistinct RNA-binding protein, CELF1 (121),via hyperphosphorylation by protein kinase C,which is aberrantly activated through unknownmechanisms by expanded CUG repeat expres-sion in the context of the DMPK 3′ UTR(Figure 5) (122). CELF1 is elevated in DM1patient tissues and myoblasts, and CELF1 over-expression in heart or muscle leads to cardiacdefects and muscle wasting, respectively (123),
452 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
suggesting that CELF1 activation can mediateadditional, MBNL-independent changes thatmay cause other DM1 symptoms.
Although it remains unclear exactly whichevents downstream of MBNL sequestrationcause the plethora of DM phenotypes, it hasbeen firmly established that DM is a disease ofRNA toxicity. Thus, eliminating the expandedrepeat RNA or preventing it from sequester-ing RNA-binding proteins is likely to repre-sent a viable therapeutic strategy for both DM1and DM2. Thus, similar approaches are beingpursued for both diseases, although a small butincreasingly recognized number of patients ex-perience DM symptoms in the absence of ex-panded repeats in DMPK or CNBP (124). Fur-ther investigation is needed to determine thecausative loci in this subset of patients and toevaluate whether similar molecular pathwaysmay be perturbed.
Genetic Diseases of Skeletal Muscle:Limb Girdle Muscular Dystrophies
Limb-girdle muscular dystrophy (LGMD)refers to a phenotypically related group ofdystrophies, each caused by a distinct geneticdefect. All LGMDs show progressive muscleweakness beginning from the proximal limbmuscles, elevated CK, and in some casescardiomyopathy. Disease onset varies fromearly childhood to late adulthood. LGMD maybe either autosomal dominant (LGMD1) orautosomal recessive (LGMD2) (125), and thecausative genetic defect may occur in genes en-coding DGC-associated proteins, sarcolemmalproteins, muscle fiber enzymes, sarcomericproteins, or nuclear lamina. In approximatelyone-third of LGMD patients, the mutated genehas yet to be identified. Autosomal dominantLGMD patients exhibit a milder phenotype,and the disease onset is typically in adulthood.Eight loci are known to cause LGMD1 so far,but only three genes, which encode myotilin(LGMD1A), lamins A and C (LGMD1B), andcaveolin-3 (LGMD1C), have been implicated.
Mutations in the myotilin gene are re-sponsible for LGMD1A (126). Myotilin is
localized to the Z-line and interacts withα-actinin, which cross-links actins in Z-lines(127). LGMD1A muscle biopsies analyzedby electron microscopy exhibit extensiveZ-line streaming. The mean age of onset ofLGMD1A is 27 years, and some patients showa dysarthic pattern of speech in addition to theusual LGMD features (126).
Lamins A and C are intermediate filamentproteins found in the nuclear membrane.Mutations in LMNA, which encodes lamins Aand C, cause several different muscle diseases,including hypertrophic cardiomyopathy, con-genital muscular dystrophy (CMD), familialpartial lipodystrophy, Emery–Dreifuss muscu-lar dystrophy (EDMD), and LGMD1B (125).Most LGMD1B patients exhibit cardiomyopa-thy. Skeletal myopathy is slowly progressiveand mild in these patients, and their CK levelsare slightly elevated (128). Given that laminsare expressed in most postmitotic cells, themuscle specificity of these diseases is not wellunderstood.
LGMD1C is caused by mutations in theCAV3 gene, which encodes the caveolin-3protein (129). Caveolae are membrane invagi-nations involved in localizing proteins in themembrane. Caveolin-3 is expressed in muscletissue (130) and interacts with dysferlin in thesarcolemma (131). On one hand, accumulationof dysferlin in the Golgi apparatus of cellslacking caveolin-3 led to the speculation thatcaveolin may help to transport dysferlin tothe sarcolemma (132). On the other hand, arecent report indicates that caveolin-3 mayassociate with the calcium release complexin the sarcolemma (133). CK levels typicallyare increased in LGMD1C patients, buttheir disease phenotype is generally mild andsome patients show no clinical muscle diseasesymptoms (125).
Mutations in the calpain-3 gene (CAPN3)cause LGMD2A, which accounts for 20% to40% of LGMD cases. Calpain-3 is a muscle-specific intracellular calcium–activated pro-tease associated with connectin and titin in thesarcomere (134), as well as with dysferlin (135).How mutations in calpain lead to muscular
www.annualreviews.org • Skeletal Muscle Disease and Therapy 453
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
dystrophy is poorly understood; deregulation ofsarcomere remodeling (136), membrane repair(46), cytoskeleton–membrane interaction andcytoskeleton structure (137, 138), and apoptoticcell death (139) have been proposed as potentialmechanisms.
LGMD2B is a type of dysferlinopathy inwhich defective membrane repair may lead toextensive myonecrosis. Dysferlin is a 230-kDatransmembrane protein and, as discussedabove, has been implicated in membranepatching (37). Dysferlin-deficient cells inpatients and mouse models show accumulationof submembranous vesicles and membranediscontinuities, implicating a defect in vesicle-membrane fusion (140, 141). Impaired fusionand differentiation of dysferlin-null myoblastsin vitro further support a role for this proteinin myogenesis (142). Interestingly, recent dataindicate that genetic manipulations that correctdefects in membrane resealing in certain assaysmay be insufficient to correct muscle pathologyin dysferlin-deficient mice, raising the possi-bility that additional pathological mechanismsmay contribute to this disease (143). Mutationsin dysferlin can cause LGMD2B, Miyoshi my-opathy (MM), or distal myopathy with onsetin the anterior tibial muscles (144). LGMD2Bpatients exhibit proximal myopathy and sub-stantially elevated CK levels, and disease onsetusually occurs in the patients’ twenties. Anadditional symptom in LGMD2B that distin-guishes it from the other LGMDs is infiltrationof inflammatory immune cells into muscle(145). Interestingly, identical mutations cancause LGMD2B or MM symptoms, which sug-gests that genetic modifiers or environmentalfactors may influence disease pathology (146).
The sarcoglycans are N-glycosylated trans-membrane proteins that form a heterote-trameric glycoprotein subcomplex within theDCG (147). Six sarcoglycan proteins have beencloned thus far, and the major proteins exist-ing in the muscle sarcolemma are the α-, β-,γ-, and δ-sarcoglycans. Mutations in the γ-, α-, β-, and δ-sarcoglycans cause LGMD2C, -D,-E, and -F, respectively. Defects in any ofthe sarcoglycans, except γ-sarcoglycan, desta-
bilize the entire DCG, which suggests thatthe α-, β-, and δ-sarcoglycans are closely as-sociated (148, 149). Loss of dystrophin alsoleads to the disappearance of sarcoglycan sub-units from DGC, but mutations in sarcoglycangenes do not interfere with the localization ofdystrophin. Sarcoglycanopathies usually have achildhood onset and greater severity than thatof other LGMDs. Cardiomyopathy is presentin all sarcoglycanopathies, although it is rarerin LGMD2D (150).
The sarcomeric proteins telethonin and titinare mutated in LGMD2G and LGMD2J, re-spectively. Titin is an enormous protein thatspans half the length of the sarcomere and pro-vides a scaffold for myofibrils. Telethonin is asubstrate of titin kinase, which binds to its Nterminus and provides spatially defined bind-ing sites for sarcomeric proteins to help as-semble the sarcomere (151). LGMD2H resultsfrom deficient sarcomere recycling. TRIM32,the gene responsible for LGMD2H, encodesan ubiquitin ligase that marks sarcomeric pro-teins for degradation by the proteasome (152).Recently, a putative calcium-activated chloridechannel, Anoctamin 5 (ANO5), was identifiedas the defective gene in LGMD2L. This reportalso suggests that ANO5 may function in thedysferlin-dependent muscle membrane repairpathway (153).
Mutations in proteins involved in dys-troglycan glycosylation are known to causeCMDs, Walker–Warburg syndrome (WWS),or muscle–eye–brain disease. Nonetheless, spe-cific mutations in some of these genes, includ-ing FKRP (LGMD2I), POMT1 (LGMD2K),fukutin (LGMD2M), POMT2 (LGMD2N),and POMGnT1 (LGMD2O), can also causeLGMD (154). LGMD2P, another type ofLGMD, is caused by disruption of dystrogly-can (DAG1).
Genetic Diseases of SkeletalMuscle: FacioscapulohumeralMuscular Dystrophy
Facioscapulohumeral muscular dystrophy(FSHD) is the third most common form of
454 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
muscular dystrophy and was first described in1884 (155). FSHD patients typically experiencesymptoms first in the skeletal muscles of theface (facio), scapula (scapulo), and upper arms(humeral) but ultimately develop progressivemuscle weakness throughout the body (155).Like myotonic dystrophy, FSHD is inheritedin an autosomal dominant fashion, but thegenetics of the disease have proven challengingto unravel. More than 95% of FSHD casesare associated with deletion of the tandemlyrepeated D4Z4 units at the subtelomericregion of chromosome 4q35 (FSHD1) (156).Other, rarer forms of FSHD also exist, butthe genetic bases for these variants either aredissimilar to FSHD1 or remain unclear.
Whereas normal individuals have 11–100D4Z4 repeats at the end of chromosome4, FSHD1 patients have 10 or fewer (157).Translocations between these repeat units anda similar repeating unit on the subtelomericregion of chromosome 10q occur frequently.Although contractions occur within the 10q re-peats, these never lead to FSHD (157). A partic-ular polymorphism found exclusively on chro-mosome 4, downstream of the last repeatingDUX4 unit, is essential for manifestation ofFSHD1, which explains why 10q contractionsfail to cause disease. This polymorphism en-codes a polyadenylation signal that stabilizesDUX4 transcripts that normally would be de-graded (158). Thus, aberrantly stabilized ex-pression of DUX4 may be the causative eventin FSHD pathogenesis.
Overexpression of DUX4 in various celltypes leads to apoptosis, but aberrant DUX4expression has been reported in only a mi-nority of cells. Yet, several DUX4 transcrip-tional targets appear to be robustly upreg-ulated in FSHD muscle relative to controlmuscle, suggesting that relatively restrictedDUX4 misexpression can lead to widespreadchanges in gene expression, possibly throughthe release of secreted factors and immunomod-ulators (159). Proposed strategies for mitigat-ing FSHD pathology include downregulationor repression via a dominant negative splice iso-form of aberrant DUX4 expression (159).
Genetic Diseases of Skeletal Muscle:Emery–Dreifuss Muscular DystrophyEDMD is caused by mutations in nuclear mem-brane proteins. EDMD can be X-linked orautosomal; it causes progressive muscle weak-ness, contractures, and cardiac defects (160).X-linked EDMD was mapped to the emeringene (EMD) (161), and mutations in LMNA andin the nesprin-1 and nesprin-2 genes (SYNE1and SYNE2) cause autosomal dominant andautosomal recessive EDMD, respectively(Table 1) (162–164). Emerin localizes to theinner nuclear membrane and interacts directlywith nuclear lamin proteins (Figure 6) (165).Emerin also binds to barrier-to-autointegrationfactor (BAF), and BAF oligomers directly as-sociate with chromatin (166). Furthermore,nuclear lamins are indirectly linked to the actincytoskeleton via SUN and nesprin proteins(167). Thus, emerin, lamin, nesprin, and othernuclear proteins are considered to be involvedin organizing chromatin structure, therebyproviding a scaffold for proteins involvedin gene regulation and linking the nuclearskeleton to the cytoskeleton. Both lamin andemerin are expressed in all tissues, and theparticular impact of mutations in these geneson skeletal muscle is not well understood. Onehypothesis (the mechanical-stress hypothesis)holds that contraction-induced forces towhich striated muscles are specifically exposedcause myonuclear damage and ultimatelydeath in muscle cells with defective nuclearmembrane proteins (168). Another hypothesis(the gene-expression hypothesis) suggests thatLMNA and EMD mutations alter specificchromatin sites, thereby deregulating muscledifferentiation, mechanotransduction, andapoptosis-associated genes. Of course, thesetwo hypotheses are not mutually exclusive;defects in nuclear membrane proteins maycause both increased sensitivity to contractionforce and aberrant gene expression.
Genetic Diseases of Skeletal Muscle:Congenital Muscular DystrophiesInfants with hypotonia, muscle weakness,histological manifestation of dystrophic
www.annualreviews.org • Skeletal Muscle Disease and Therapy 455
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
Actin filaments
Outer nuclear membrane
Inner nuclear membrane
Nesprin
SUN dimer
Nuclear lamin
BAF complex
Emerin
Chromatin
Figure 6Nuclear matrix proteins involved in Emery–Dreifuss muscular dystrophy. Emerin acts as a bridge between chromatin and the nuclearlamin. Nuclear lamin interacts with the SUN dimer, which is indirectly linked to the actin cytoskeleton via nesprin. Thus, mutation ofany of these genes interrupts the normal linkage between the cytoskeleton and the nuclear matrix. Abbreviation: BAF, barrier-to-autointegration factor.
myopathy, and delayed motor developmentare diagnosed with CMD. CMDs are a genet-ically heterogeneous group of neuromusculardisorders that vary widely in severity. In someforms of CMD, neurologic features result ininvolvement of the eye and brain as well. Onthe basis of the genes found to be mutated inCMD patients thus far, and the function oftheir protein products, CMDs can be classifiedinto five groups. The first and most-studiedgroup is caused by abnormalities in the glyco-sylation state of the αDg protein (169). αDgundergoes extensive O-linked glycosylation,and defects in protein glycosylation interferewith its interaction with laminin (170), therebydisrupting the link between the myofibercytoskeleton and the ECM. Mutations insix genes (LARGE, fukutin, FKRP, POMT1,POMT2, and POMGnT1) cause reduced αDgglycosylation in CMD patients (171). POMT1,POMT2, and POMGnT1 are enzymes re-
sponsible for transferring O-mannosyl glycansto αDg. LARGE, fukutin, and FKRP may alsobe involved in αDg glycosylation; however,a detailed understanding of their mechanismof action is lacking (172). Mutations in thesegenes can lead to WWS, Fukuyama CMD,or muscle–eye–brain disease, according to theseverity of the effect on αDg glycosylation.
The second group of CMDs results fromdefects (a) in genes encoding the ECM pro-teins laminin-211/merosin (LAMA2) and colla-gen type VI (COL6A1, COL6A2, and COL6A3)or (b) in ITGA7 (which encodes integrin-α7, themerosin receptor) present on the sarcolemma(173). These genetic defects also disrupt theassociation between the fiber contraction ma-chinery and the basal lamina. Allelic mutationsin each of the genes encoding different sub-units of collagen type VI (COL6A1, COL6A2,and COL6A3) can cause severe Ullrich CMDor mild Bethlem myopathy.
456 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
Sarcopenia:age-related decline inmuscle mass andstrength
The third group of CMDs includes a rare au-tosomal recessive disease caused by abnormal-ities in the ER protein Selenoprotein N1. Themolecular mechanism behind this type of CMDis poorly understood; however, this selenium-containing glycoprotein may be involved inprotein posttranslational modification, given itslocalization to the ER. Evidence also supportsa role for Selenoprotein N1 in protecting mus-cle from oxidative stress (174) and in support-ing myogenesis in early development (175). Arelatively new study demonstrated that, in ad-dition to LMNA’s previously reported role inLGMD2G and EDMD, defects in this genemay cause the fourth type of CMD (176). An-other recent case report described a new typeof CMD in which a mutation in a 12-year-old French boy in the gene encoding sarcom-eric protein telethonin (TCAP), associated pre-viously with LGMD2G (177), caused muscleweakness and mildly delayed motor develop-ment during infancy that progressed over thefirst decade of life (178).
Sarcopenia
Sarcopenia, the progressive loss of skeletal mus-cle mass and strength as a result of advancingage, is a present and growing global health con-cern; it affects ∼25% of individuals older than70 and 40% of individuals older than 80. In-dividuals suffering from sarcopenia experiencedecreased independence, including a progres-sive loss of the ability to perform normal activ-ities of daily living and a significantly reducedquality of life. The underlying molecular mech-anisms that contribute to the onset and progres-sion of sarcopenia remain ill defined. Studieshave implicated an increase in chronic inflam-mation, both systemically and in the muscle tis-sue itself; alterations in metabolic processes thatlead to increased insulin resistance and acti-vation of catabolic pathways; accumulation ofgenotoxic DNA damage; mitochondrial dys-function and oxidative stress; loss of motorneurons leading to motor-unit remodeling anddenervation-induced atrophy; and deficits insatellite cells that impair the normal muscleregenerative response (reviewed in References
179 and 180). Strategies to reverse sarcopeniahave focused largely on behavioral interven-tions. Introduction of resistance or endurancetraining slows sarcopenia in elderly subjects, en-hancing muscle function and even increasingthe apparent content of muscle satellite cells(181). Hormone therapy also has proven effec-tive in some instances, which has prompted theinitiation of large-scale human trials to evaluatethe impact of testosterone supplementation onmuscle function. Finally, studies aimed at un-derstanding the age-related decline in muscleregenerative potential implicate both local in-fluences [including Notch signaling (182) andTGF-β (183)] and systemic influences (184,185). Results from these studies could eventu-ally be translated into pharmacological inter-ventions to boost muscle repair potential in el-derly individuals.
THERAPEUTIC POSSIBILITIESFOR MUSCLE WASTINGDISEASES
Current treatment options for musculardystrophy are disappointingly limited andfocus mainly on managing symptoms andsuppressing the immune and inflammatoryresponse (186, 187). Therapeutic approachesthat aim instead to cure these disorders havebeen a subject of research for many decades andcan be grouped broadly into two categories onthe basis of their strategic approach. The firstcategory seeks to repair or replace the mutatedgene, whereas the second aims to reduce theimpact of the mutation by activating alterna-tive pathways or intervening downstream tocorrect the pathological consequences. Eachof these strategies presents unique advantagesand challenges, and past experiences havehelped inform and focus the direction of futureresearch and the design of future clinical trials.Here we discuss several promising therapeuticavenues, including cell transplantation, genesupplementation or correction, and oligonu-cleotide and small-molecule delivery, eachof which has been considered as a basis forcurative treatment of muscle disease.
www.annualreviews.org • Skeletal Muscle Disease and Therapy 457
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
Therapeutic Possibilities:Cell Transplantation
Because satellite cells represent a robust and ex-clusive source of new myofibers during normalmuscle regeneration, these cells and theirderivatives have long been considered attrac-tive targets for cell-replacement therapy inmuscle. In this approach, cells from an unaf-fected donor, or gene-corrected autologouscells (see the section titled Therapeutic Possi-bilities: Gene Supplementation or Correction),could be infused into patients, where theywould presumably produce donor-engraftedmuscle fibers carrying the normal allele ofthe affected gene, thereby reconstituting genefunction. Indeed, this strategy of precursor celltransplantation has been successful in the treat-ment of some hematopoietic disorders, whereinbone marrow transplantation now representsa relatively common (although certainly notrisk-free) clinical intervention. However, limi-tations in the numbers of satellite cells that canbe obtained from human muscle, and the lackof viable methods to expand these cells ex vivo,have thus far restricted clinical application ofthis approach and have simultaneously spurredconsideration of alternative sources of cellsfor transplantation. Early clinical trials eval-uated the efficacy of transplanted myoblasts,generated by long-term culture from explantsof donor muscle and injected directly into themuscle. However, these trials yielded largelydisappointing results (188), perhaps due to sig-nificant cell loss upon transplantation, causedby the death of up to 90% of the transferred cellswithin days of transplantation (189). Progressin the ability to isolate and expand primitivesatellite cells, which may show enhancedsurvival ability after transplantation (92), willprobably be essential in reinvigorating thisconceptually attractive therapeutic approach.Also, such enhancements in satellite cell acqui-sition should be coupled with improvementsin cell-delivery strategies, given that satellitecells cannot currently be delivered systemicallyand do not migrate far from the site of intra-muscular injection. These limitations pose a
daunting challenge for the delivery of donorcells to affected muscles throughout the body.
In addition to satellite cells, non–satellitecell populations that reside in muscle have beenconsidered as alternative cell-therapy vehicles.Particularly encouraging (190) have been stud-ies in dog models with cultured mesangioblasts,which may be related to blood vessel–associatedpericytes (191), and exhibit broad differentia-tion potential in culture, including productionof cells expressing markers of the skeletal mus-cle, smooth muscle, and vascular lineages (191–193). Trials are ongoing to assess the efficacyof these cells in human patients. An attractiveattribute of mesangioblasts, as well as the prob-ably related populations of CD133+ (194) andmuscle-derived “side-population” cells (195),for cell therapy is their apparent ability to homefrom the circulation into dystrophic muscle tis-sue (190 196), which allows them to be deliv-ered via vascular, rather than intramuscular, in-jection. Similar promise for vascular deliveryof muscle regenerative cells was excited by ob-servations that transfusion of donor bone mar-row cells may lead to detectable contributionsof these cells in skeletal myofibers (197, 198);however, further evaluation of such approachesindicated that the rate of engraftment was farbelow that predicted to be necessary for ther-apeutic effect (82, 199). Indeed, in a DMDpatient who received a bone marrow trans-plant for coincident severe combined immun-odeficiency, although evidence of rare donorcell engraftment in muscle was found, no im-provement in dystrophic phenotype could beattributed to the transplanted cells (200).
In an effort to overcome the pervasivelimitations in obtaining adequate numbersof immunologically matched donor cellswhen working with adult somatic cells formuscle regenerative medicine, several groupshave attempted to derive engraftable muscleprecursor cells from pluripotent stem cellsources. Such cells, including embryonic stemcells (ESCs), derived from human embryos,and induced pluripotent stem cells (iPSCs),derived by transcription factor–dependent “re-programming” of differentiated somatic cells,
458 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
ZFN: zinc-fingernuclease
can be propagated indefinitely in culture andcan, in principle, differentiate into any cell typein the body (201, 202). Thus, a robust strategyfor producing muscle precursors from thesecells would provide an inexhaustible sourceof donor cells for transplant. Moreover, whencoupled with gene-correction strategies, iPSCsgenerated in a patient-specific manner wouldproduce immunologically matched donor cellsthat could eliminate, or at least reduce, thethreat of graft destruction due to recognitionby the host immune system. However, a majorchallenge in realizing the potential of pluripo-tent stem cells for skeletal muscle therapy hasbeen the difficulty of deriving fully mature,“adult” somatic cells from ESCs or iPSCs (203).Nonetheless, important advances have beenmade, including the demonstration that tran-sient induction of the satellite cell–associatedtranscription factors Pax3 and Pax7, or cellsorting with satellite cell–specific surface mark-ers, in differentiating mouse ESCs or iPSCs canpromote the recovery of myogenic precursors,which have been successfully engrafted inmodels of DMD and FSHD (204–208).
Therapeutic Possibilities: GeneSupplementation or Correction
Rather than relying on transplanted cells as ve-hicles for complementing defective alleles inmuscular dystrophy patients, some investiga-tors in the area of muscle regenerative medicinehave focused instead on achieving direct genetherapy in affected muscle fibers through ex-ogenous delivery of a normal copy of the mu-tated gene or, more recently, by introductionof genome-modifying nucleases that may en-able in situ gene repair. Most gene-deliveryapproaches have employed recombinant viralvectors, particularly adenoviruses, because theycan carry very large inserts (a significant chal-lenge when attempting genetic complementa-tion of the largest gene in the human genome!),and AAVs, because of their relatively highefficiency of transduction in skeletal muscleand their low immunogenicity (187). However,even AAVs are susceptible to antiviral host im-
mune responses, which may necessitate hostimmunosuppression and can prevent repeatedgene-delivery attempts (186). Attempts havealso been made to produce pared-down ver-sions of dystrophy genes (e.g., mini- and mi-crodystrophin) that could provide at least par-tial restoration of gene function and enablepackaging of target sequences into AAV, aswell as retro- or lentiviral vectors (186). Finally,strategies that may support the transfer of en-tire regions of the human chromosome, includ-ing those areas that encompass the human dys-trophin gene and its regulatory elements, havebeen pursued using human artificial chromo-somes, which can be introduced into target cellsand maintained episomally to support tissue-specific expression of the exogenous gene (209).
A second and emerging approach in thegene therapy realm has been to attempt directcorrection of the mutated allele(s) in the pa-tient’s own cells. This process could, in theory,be accomplished in situ or by genetic modifi-cation in autologous somatic cells or patient-specific iPSCs, which would otherwise be ge-netically matched to individual patients andcould be transplanted therapeutically to restoregene function in patient muscles. Early effortstoward this goal have employed site-specificzinc-finger nucleases (ZFNs), which are exper-imentally engineered DNA-binding proteinsthat are modified by fusion to the Fok1 nucle-ase domain. Site-specific nuclease activity, di-rected by the ZFN DNA-binding domain, isused to induce a strand break in the target ge-nomic sequence, which can then be repaired bynonhomologous end joining or, in the case oftherapeutic gene correction, by homologous re-combination with a normal donor sequence togenerate a gene-corrected allele. However, de-spite more than 15 years of development and re-cent progress in the application of some of thesetechnologies in clinical trials aimed at suppress-ing HIV-1 in vivo, ZFNs remain cumbersometo design and employ, due in part to the contextspecificity of ZFN sequences, nonspecific DNAbinding that can lead to off-target gene cleav-age, and a relative stranglehold on the tech-nology by a single biotech company that has
www.annualreviews.org • Skeletal Muscle Disease and Therapy 459
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
TALEN:transcriptionactivator–like effectornuclease
limited ZFNs’ availability and greatly increasedtheir cost for research and clinical studies (210).Happily, the emergence of a related technol-ogy, based on DNA-binding virulence factorsproduced by plant pathogens, may circumventthese obstacles. Transcription activator–like ef-fector nucleases (TALENs), like ZFNs, exhibitsequence-specific binding to target DNA se-quences; yet, unlike ZFNs, TALENs appear tobe considerably more approachable in designand may show greater efficacy with lower cel-lular toxicity (210).
However, in all of these approaches, a per-sistent concern even with the use of autologouscells is that the ectopic or induced expressionof a gene not normally present in patient cellscould provoke an autoimmune response, whichwould lead to clearance of the gene-correctedcells. Indeed, some studies have supported theidea that induced expression of dystrophin canstimulate both humoral and cellular immuneresponses (211). Overcoming such immunolog-ical barriers represents a significant challengefor the future of gene-therapy approaches indystrophic disease.
Therapeutic Possibilities:Recombinant Protein Administration
Different groups have attempted direct admin-istration of a few recombinant proteins to ame-liorate DMD symptoms, mostly in the mdxmouse model of the disease. IGF-I is a hormoneproduced by many different tissues, includingskeletal muscle, and is elevated in dystrophicmuscle (212). IGF-I is implicated in stimula-tion of satellite cell proliferation and differenti-ation during muscle regeneration, growth, andhypertrophy (213). Administration of recom-binant IGF-I protein to mdx mice reportedlyincreases the resistance of the extensor digito-rum longus and soleus muscles to fatigue (214).In addition, mdx mice treated with recombi-nant IGF-I showed increased resistance of thediaphragm muscle to fatigue and enhanced spe-cific force output compared with untreated con-trols (215). IGF-I administration also increasedmuscle force–producing capacity and size inlaminin-deficient mice (216).
Proteins inhibiting myostatin also havebeen reported to ameliorate symptoms whenadministered to mdx mice. Myostatin (GDF8)is a member of the TGF-β superfamily anda negative regulator of muscle growth. Muta-tions in myostatin cause increased muscle massin mice (217), cattle (218), and humans (219).Delivery of a monoclonal antibody againstmyostatin into mdx mice resulted in increasedbody weight, muscle mass, and strength;however, resistance to contraction-inducedinjury was not improved according to ex vivoevaluations (220). Another study used a myo-statin propeptide to inhibit myostatin in mdxmice and reported improvements in musclesize and strength but not in susceptibilityto eccentric contraction–induced damage(221). However, systemic or intramuscularinjection of laminin-111 into mdx mice wasreported to prevent exercise-induced muscledamage, increase the expression of integrin-α7as part of the costamere, and reduce serumCK to normal levels (222). Laminin-111 alsoreportedly enhances myoblast transplantationinto immunodeficient mdx mice when used asa coadjuvant (223).
Utrophin is the autosomal homolog ofdystrophin, and these two proteins share sig-nificant structural similarities (224). Utrophinis upregulated in mdx mice, and utrophinoverexpression both prevents and amelioratesdisease symptoms in dystrophic mice (225,226). Systemic injection of a recombinantTAT-μ-utrophin protein [a truncated formof utrophin that lacks parts of the internalrod-shaped domain and is conjugated to thearginine-rich TAT (transactivator of transcrip-tion) cell–penetrating peptide] into mdx miceresulted in improved histopathology, increasedspecific force production, and reduced forcedrop after eccentric exercise (227). TAT-μ-utrophin also improved pathophysiologywhen administered to dystrophin/utrophindouble-knockout mice (228).
A recent report suggests that recombi-nant human biglycan (rhBGN) may upregulateutrophin in the sarcolemma in mdx mice (229).Biglycan is an ECM protein that binds αDg and
460 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
α- and γ-sarcoglycans and is both critical fortimely muscle regeneration (230) and impor-tant for neuromuscular junction stability (231).Mdx mice treated with rhBGN also upregulatedsome DGC components, and interestingly,muscles from these mice showed a reduced dropin force after multiple rounds of eccentric con-tractions in vitro, which suggests increased re-sistance to contraction-induced injury.
Therapeutic Possibilities:Oligonucleotide-MediatedApproachesOligonucleotide-mediated approaches for themuscular dystrophies offer the advantage ofspecificity for targets and for mechanismsof action, whether based on RNA interfer-ence (RNAi), antisense, splicing modulation, orsteric hindrance (Figure 7). Oligonucleotides
Dystrophin pre-mRNA(DMD patient missing exon 50)
Splice-switching oligonucleotides
Antisense (steric blocking)
Antisense (gap-mers)
46 47 4948 51 52
Nonsense-mediated decay of mRNA,no dystrophin protein produced
Restoration of reading frame,truncated functional dystrophin protein producedfrom stable mRNA
51
AVI-4658splice site-switching oligonucleotide
DMPK mRNA
AAAAA...Gppp
Release of MBNLs
CAGCAGCAGCAG
AAAAA...Gppp
Antisense (CAG)n oligonucleotide
DMPK mRNA
AAAAA...
Gppp
CAGCAGCAGCAG
DNA
Modified bases
RNase H AAAAA... AAAAA...
Degradation of CUG repeatsand DMPK mRNA
Antisense gap-mer
50
Without AVI-4658
With AVI-4658
Figure 7Oligonucleotide-mediated therapeutic approaches for muscular dystrophies. Aside from RNA interference–mediated approaches, atleast three major oligonucleotide-based approaches are under active investigation; these approaches include splice-site modulation,antisense via steric blocking, and antisense via gap-mer function. Several of these approaches have been effective in clinical andpreclinical studies of Duchenne muscular dystrophy (DMD) and dystrophia myotonica type 1. Abbreviations: MBNL, Muscleblind-likefamily of RNA-binding protein; mRNA, messenger RNA; pre-mRNA, precursor mRNA.
www.annualreviews.org • Skeletal Muscle Disease and Therapy 461
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
have been used in the context of DMD to altersplice site usage in order to modulate the dys-trophin open reading frame (232); positive re-sults have recently been obtained in the clinic.These antisense oligonucleotides are basicallydesigned to mask the splice site for mutatedor additional exons, thereby removing theseexons from the messenger RNA and creat-ing an internally deleted protein that maintainsits crucial N- and C-terminus-associated func-tions. Such shortened forms of dystrophin arefound in BMD patients, whose disease is usuallymuch milder than DMD. Phosphorodiamidatemorpholino oligomer (PMO) and 2′-O-methyl-phosphorothioate (2′OMP) are two types of an-tisense oligonucleotides that have been used inDMD exon skipping studies and clinical trials.Both PMO and 2′OMP contain modificationsthat make them more biologically stable and re-sistant to nucleases. 2′OMPs designed to targetexon 23 of the DMD gene in mdx mice restoreddystrophin expression in skeletal muscle wheninjected intramuscularly (233) or intravascu-larly (234). This promising result led to test-ing of a 2′OMP targeting exon 51 of the DMDgene (PRO051) in clinical trials. Intramuscu-lar injection of PRO051 resulted in dystrophinexpression in 64% to 97% of muscle fibers atlevels between 17% and 35% of normal fibers(235). A Phase I/II clinical trial for PRO051has also been performed by subcutaneous in-jection of the compound in patients; the injec-tions led to the expression of dystrophin in adose-dependent manner without apparent ad-verse effects (236). A Phase III clinical trial ofPRO051 is under way.
PMOs are effective in skipping exon 23 ofthe DMD gene in mdx mice (237, 238). TheMDEX Consortium and Sarepta (formerly AVIBioPharma) tested the efficacy of a 30-mer mor-pholino (AVI-4658 or eteplirsen) in skippingexon 51 of human DMD in patients. Intra-muscular injection of AVI-4658 (239) and sys-temic delivery of the morpholino in clinicaltrials led to exon 51 skipping and expressionof dystrophin when higher morpholino doseswere used. A Phase II clinical trial for eteplirsenis now ongoing (clinicaltrials.gov identifier:
NCT01396239), and Sarepta has begun pre-clinical studies that use a drug to skip exon 50of the human DMD gene (AVI-5038).
A unique feature of DMD is the leakinessof the muscle membrane, which facilitatesdelivery of macromolecules to skeletal muscle,a challenge that must still be overcome in manyother muscular dystrophies. Exon skipping ofchloride channel exon 7a has been achievedin a mouse model of myotonic dystrophy andleads to rescue of myotonia (240). Steric block-ing approaches have also been successful inmyotonic dystrophy in displacing MBNL fromexpanded CUG repeats by targeting the RNAdirectly with CAG repeat oligonucleotides(241, 242), and RNase H–competent gap-mersare effective in degrading expanded CUGrepeat–containing transcripts (243). Still, asignificant challenge facing oligonucleotide-mediated approaches is delivery; solutionsto this problem could usher in a new era ofrational and specific therapies.
Therapeutic Possibilities:Small-Molecule Therapy
The first small molecules used to treat DMDpatients were anti-inflammatory compoundsfrom the family of glucocorticoid cortico-steroids. Deflazacort, prednisone, and pred-nisolone have been most commonly used in theclinic. In some cases, treated patients showedimproved muscle strength, prolonged ambula-tion, and slowed disease progression; however,these interventions are not a cure for the dis-ease, and major side effects, including hyperten-sion, diabetes, weight gain, and cataract, presentobstacles to their prescription (244, 245).
Approximately 10–15% of DMD cases arecaused by mutations that introduce prematurestop codons (246). Some chemicals can interactwith ribosomal subunits to cause the transla-tional machinery to skip such nonsense mu-tations by introducing an amino acid in thosepositions instead. Differences in the context ofnucleotide sequence surrounding prematureand normal stop codons allow for specificity ofaction of these compounds (247). Gentamicin,an aminoglycoside antibiotic that promotes
462 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
such ribosomal “read-through,” can inducedystrophin expression in mdx muscle to upto 20% of normal levels (248); however, thiscompound has not been effective in humantrials (249).
A high-throughput screen of ∼800,000chemicals, performed by PTC Therapeutics R©,identified ataluren (PTC-124 R©) as a compoundthat efficiently induced nonsense mutationread-through. Ataluren, which has no struc-tural similarity with aminoglycosides, restoresdystrophin expression in cultured myotubesfrom mdx mice and DMD patients. Whenadministered to mdx mice in vivo, atalurenimproved muscle-specific force and resistanceto contraction-induced injury and restoreddystrophin expression in up to 25% of fibers(250). Phase I trials of PTC-124 revealedthat the compound is well tolerated; however,three Phase II clinical trials were terminatedin March 2010 when the predeterminedprimary outcome (the 6-min walk test) was notachieved. A Phase III clinical trial (clinicaltri-als.gov identifier: NCT01247207) is currentlyrecruiting DMD and BMD participants whohave previously been exposed to ataluren.
Another small molecule, BMN-195 (SMT-C1100), emerged from a screen for chemicalsthat upregulate the expression of utrophin.Daily administration of BMN-195 to mdx miceameliorated dystrophic pathology (251), butwhen tested in a Phase I clinical trial, plasmaconcentrations of this compound failed to reachthe required level (see http://phx.corporate-ir.net/phoenix.zhtml?c = 106657&p = irol-newsArticle&ID = 1455247&highlight).However, no adverse effects were reported forBMN-195, and Summit PLC is working to geta new formulation of the compound back intoclinical trials.
Recently, Kawahara et al. (252) used a zebrafish model of DMD to screen a small-moleculelibrary to identify compounds that amelioratedystrophic pathology in newborn fish. Themost potent chemical identified in this studywas aminophylline, reported to be a nonselec-tive phosphodiesterase (PDE) inhibitor (253).Interestingly, the skeletal muscle structure of
affected dystrophin-null fish was restored af-ter treatment with aminophylline for 26 days,although no dystrophin expression was de-tected in the muscle. The mechanism underly-ing this compound’s activity is not understood,but it may relate to elevation of intracellularcyclic AMP (cAMP) levels and activation ofcAMP-dependent protein kinase (252). Theseauthors also reported that sildenafil citrate, aPDE5 inhibitor, influences muscle pathology indystrophin-null zebra fish. Sildenafil citrate waspreviously shown to reverse cardiomyopathy inmdx mice, possibly via activation of cyclic GMP(cGMP)-dependent pathways (254). Tadalafil,another PDE5 inhibitor, reportedly improvesthe histopathology of dystrophic muscle inmdx mice when administrated prenatally (255);however, existing studies on the effects of PDE5inhibitors on dystrophic muscle have evalu-ated compound administration only in the earlystages of life, and it remains unclear whetherthese molecules can reverse disease pheno-type if animals are treated after disease on-set. Both sildenafil citrate and tadalafil are inclinical trials for DMD and BMD patients(clinicaltrials.gov identifiers: NCT01350154,NCT01070511, and NCT01359670).
Small-molecule approaches for the treat-ment of myotonic dystrophy have focused pri-marily on either disrupting RNA-MBNL in-teractions or addressing symptoms of DM.Several compounds displace MBNL from ex-panded CUG repeats or suppress CUG repeat–dependent pathology (256–259), and some haveproven efficacious in animal models (257, 259).Approaches to identify these compounds in-clude the use of high-throughput screeningmethods, such as fluorescence resonance en-ergy transfer and fluorescence anisotropy. Amodular approach also has been pioneeredin which molecules that target short RNAmotifs with moderate affinity are assembledonto a peptoid-like backbone to increase affin-ity and specificity (260). Mexiletine, a USFood and Drug Administration–approved an-tiarrhythmic sodium channel blocker, has beenused to treat myotonia and other DM symp-toms (261); a clinical trial is under way to
www.annualreviews.org • Skeletal Muscle Disease and Therapy 463
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
formally investigate mexiletine’s potentiallypositive effects in this context.
CONCLUSIONS ANDPERSPECTIVES
The great variation in the etiology and pathol-ogy of skeletal muscle diseases presents manychallenges to their efficient diagnosis and treat-ment; however, recent advances show promise
for applying both patient-specific and generictherapies to ameliorate symptoms and, poten-tially, to reverse disease course. Further un-derstanding of the molecular and biochemi-cal bases for myofiber loss in these geneti-cally diverse degenerative diseases will certainlyhelp uncover new strategies for effective in-tervention to promote healthy muscle functionthroughout life.
SUMMARY POINTS
1. Damage to skeletal muscle may occur throughout life due to exercise and contraction,acute physical and chemical insult, abnormalities in the immune system, or muscle de-generative diseases.
2. Skeletal muscle has significant endogenous repair capacity, including the abilities torepair small disruptions in muscle fiber membranes and to produce new myofibers fromresident muscle stem cells following injury.
3. Muscular dystrophies include a wide range of genetic muscle degenerative diseases causedby deficiencies in stability, repair, or gene-expression regulation in muscle fibers.
4. Some muscular dystrophies arise from mutations in ubiquitously expressed genes; thereasons for the muscle specificity of these genetic disruptions remain mysterious.
5. Although most muscular dystrophies are caused by mutations in protein-coding genes,myotonic dystrophy arises from expanded nucleotide repeats in noncoding RNAs, whichcause pathological sequestration of proteins involved in mRNA splicing.
6. Current therapeutic approaches for muscular dystrophies are based on ectopic intro-duction of the normal gene, endogenous repair of the mutated gene, or amelioration ofsymptoms achieved by triggering alternative or redundant pathways.
7. High-throughput screening for therapeutically beneficial compounds has identified somesmall molecules with potential clinical applicability in muscular dystrophy patients.
8. Skipping of mutated exons in DMD has been promising, and results from clinical trialshold promise for improved therapies for many patients with relevant genetic lesions.
DISCLOSURE STATEMENT
The authors are not aware of any affiliations, memberships, funding, or financial holdings thatmight be perceived as affecting the objectivity of this review.
LITERATURE CITED
1. Sanes JR. 2003. The basement membrane/basal lamina of skeletal muscle. J. Biol. Chem. 278:12601–42. Sanger JM, Sanger JW. 2008. The dynamic Z bands of striated muscle cells. Sci. Signal. 1:pe373. Ervasti JM, Campbell KP. 1993. A role for the dystrophin-glycoprotein complex as a transmembrane
linker between laminin and actin. J. Cell Biol. 122:809–23
464 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
4. Pardo JV, Siliciano JD, Craig SW. 1983. A vinculin-containing cortical lattice in skeletal muscle: Trans-verse lattice elements (costameres) mark sites of attachment between myofibrils and sarcolemma. Proc.Natl. Acad. Sci. USA 80:1008–12
5. Ownby CL, Cameron D, Tu AT. 1976. Isolation of myotoxic component from rattlesnake (Crotalusviridis viridis) venom. Electron microscopic analysis of muscle damage. Am. J. Pathol. 85:149–66
6. Habermann E. 1972. Bee and wasp venoms. Science 177:314–227. Duchen LW, Excell BJ, Patel R, Smith B. 1974. Changes in motor end-plates resulting from muscle
fibre necrosis and regeneration. A light and electron microscopic study of the effects of the depolarizingfraction (cardiotoxin) of Dendroaspis jamesoni venom. J. Neurol. Sci. 21:391–417
8. Ownby CL, Powell JR, Jiang MS, Fletcher JE. 1997. Melittin and phospholipase A2 from bee (Apismellifera) venom cause necrosis of murine skeletal muscle in vivo. Toxicon 35:67–80
9. Harris JB, Cullen MJ. 1990. Muscle necrosis caused by snake venoms and toxins. Electron Microsc. Rev.3:183–211
10. Gutierrez JM, Ownby CL. 2003. Skeletal muscle degeneration induced by venom phospholipases A2:insights into the mechanisms of local and systemic myotoxicity. Toxicon 42:915–31
11. Harris JB, Grubb BD, Maltin CA, Dixon R. 2000. The neurotoxicity of the venom phospholipases A2,notexin and taipoxin. Exp. Neurol. 161:517–26
12. Gopalakrishnakone P, Hawgood BJ. 1984. Morphological changes induced by crotoxin in murine nerveand neuromuscular junction. Toxicon 22:791–804
13. Forouhar F, Huang WN, Liu JH, Chien KY, Wu WG, Hsiao CD. 2003. Structural basis of membrane-induced cardiotoxin A3 oligomerization. J. Biol. Chem. 278:21980–88
14. Harris JB. 2003. Myotoxic phospholipases A2 and the regeneration of skeletal muscles. Toxicon 42:933–4515. Fletcher JE, Hubert M, Wieland SJ, Gong QH, Jiang MS. 1996. Similarities and differences in mecha-
nisms of cardiotoxins, melittin and other myotoxins. Toxicon 34:1301–1116. Lewis MS, Whatley RE, Cain P, McIntyre TM, Prescott SM, Zimmerman GA. 1988. Hydrogen per-
oxide stimulates the synthesis of platelet-activating factor by endothelium and induces endothelial cell–dependent neutrophil adhesion. J. Clin. Investig. 82:2045–55
17. Ratych RE, Chuknyiska RS, Bulkley GB. 1987. The primary localization of free radical generation afteranoxia/reoxygenation in isolated endothelial cells. Surgery 102:122–31
18. Kerrigan CL, Stotland MA. 1993. Ischemia reperfusion injury: a review. Microsurgery 14:165–7519. Riedemann NC, Ward PA. 2003. Complement in ischemia reperfusion injury. Am. J. Pathol. 162:363–6720. Brown LM, Hill L. 1991. Some observations on variations in filament overlap in tetanized muscle fibres
and fibres stretched during a tetanus, detected in the electron microscope after rapid fixation. J. MuscleRes. Cell Motil. 12:171–82
21. Morgan DL, Allen DG. 1999. Early events in stretch-induced muscle damage. J. Appl. Physiol. 87:2007–15
22. Takekura H, Fujinami N, Nishizawa T, Ogasawara H, Kasuga N. 2001. Eccentric exercise-inducedmorphological changes in the membrane systems involved in excitation-contraction coupling in ratskeletal muscle. J. Physiol. 533:571–83
23. Belcastro AN, Shewchuk LD, Raj DA. 1998. Exercise-induced muscle injury: a calpain hypothesis. Mol.Cell. Biochem. 179:135–45
24. Dalakas MC. 2011. Review: an update on inflammatory and autoimmune myopathies. Neuropathol. Appl.Neurobiol. 37:226–42
25. Dalakas MC. 1991. Polymyositis, dermatomyositis and inclusion-body myositis. N. Engl. J. Med.325:1487–98
26. Dalakas MC. 2010. Inflammatory muscle diseases: a critical review on pathogenesis and therapies. Curr.Opin. Pharmacol. 10:346–52
27. Kissel JT, Mendell JR, Rammohan KW. 1986. Microvascular deposition of complement membraneattack complex in dermatomyositis. N. Engl. J. Med. 314:329–34
28. Dalakas MC. 1995. Immunopathogenesis of inflammatory myopathies. Ann. Neurol. 37(Suppl. 1):S74–8629. Arahata K, Engel AG. 1984. Monoclonal antibody analysis of mononuclear cells in myopathies. I: Quan-
titation of subsets according to diagnosis and sites of accumulation and demonstration and counts ofmuscle fibers invaded by T cells. Ann. Neurol. 16:193–208
www.annualreviews.org • Skeletal Muscle Disease and Therapy 465
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
30. Greenberg SA, Pinkus JL, Pinkus GS, Burleson T, Sanoudou D, et al. 2005. Interferon-α/β-mediatedinnate immune mechanisms in dermatomyositis. Ann. Neurol. 57:664–78
31. Emslie-Smith AM, Arahata K, Engel AG. 1989. Major histocompatibility complex class I antigen ex-pression, immunolocalization of interferon subtypes, and T cell–mediated cytotoxicity in myopathies.Hum. Pathol. 20:224–31
32. Arahata K, Engel AG. 1988. Monoclonal antibody analysis of mononuclear cells in myopathies. IV.Cell-mediated cytotoxicity and muscle fiber necrosis. Ann. Neurol. 23:168–73
33. Goebels N, Michaelis D, Engelhardt M, Huber S, Bender A, et al. 1996. Differential expression ofperforin in muscle-infiltrating T cells in polymyositis and dermatomyositis. J. Clin. Investig. 97:2905–10
34. Askanas V, Engel WK, Nogalska A. 2009. Inclusion body myositis: a degenerative muscle disease asso-ciated with intra-muscle fiber multi-protein aggregates, proteasome inhibition, endoplasmic reticulumstress and decreased lysosomal degradation. Brain Pathol. 19:493–506
35. Hengstman GJ, Vree Egberts WT, Seelig HP, Lundberg IE, Moutsopoulos HM, et al. 2006. Clinicalcharacteristics of patients with myositis and autoantibodies to different fragments of the Mi-2β antigen.Ann. Rheum. Dis. 65:242–5
36. McNeil PL, Khakee R. 1992. Disruptions of muscle fiber plasma membranes. Role in exercise-induceddamage. Am. J. Pathol. 140:1097–109
37. Bansal D, Miyake K, Vogel SS, Groh S, Chen CC, et al. 2003. Defective membrane repair in dysferlin-deficient muscular dystrophy. Nature 423:168–72
38. McNeil PL, Miyake K, Vogel SS. 2003. The endomembrane requirement for cell surface repair. Proc.Natl. Acad. Sci. USA 100:4592–97
39. Bi GQ, Alderton JM, Steinhardt RA. 1995. Calcium-regulated exocytosis is required for cell membraneresealing. J. Cell Biol. 131:1747–58
40. Glover L, Brown RH Jr. 2007. Dysferlin in membrane trafficking and patch repair. Traffic 8:785–9441. Lennon NJ, Kho A, Bacskai BJ, Perlmutter SL, Hyman BT, Brown RH Jr. 2003. Dysferlin interacts
with annexins A1 and A2 and mediates sarcolemmal wound-healing. J. Biol. Chem. 278:50466–7342. McNeil AK, Rescher U, Gerke V, McNeil PL. 2006. Requirement for annexin A1 in plasma membrane
repair. J. Biol. Chem. 281:35202–743. Gerke V, Creutz CE, Moss SE. 2005. Annexins: linking Ca2+ signalling to membrane dynamics. Nat.
Rev. Mol. Cell Biol. 6:449–6144. Mellgren RL, Zhang W, Miyake K, McNeil PL. 2007. Calpain is required for the rapid, calcium-
dependent repair of wounded plasma membrane. J. Biol. Chem. 282:2567–7545. Howard MJ, David G, Barrett JN. 1999. Resealing of transected myelinated mammalian axons in vivo:
evidence for involvement of calpain. Neuroscience 93:807–1546. Huang Y, de Morree A, van Remoortere A, Bushby K, Frants RR, et al. 2008. Calpain 3 is a modulator
of the dysferlin protein complex in skeletal muscle. Hum. Mol. Genet. 17:1855–6647. Weisleder N, Takeshima H, Ma J. 2009. Mitsugumin 53 (MG53) facilitates vesicle trafficking in striated
muscle to contribute to cell membrane repair. Commun. Integr. Biol. 2:225–2648. Demonstrates asubstantial defect in theskeletal muscle ofmg53−/− mice inaccumulating vesicles atthe sarcolemma aftermembrane injury.
48. Cai C, Masumiya H, Weisleder N, Matsuda N, Nishi M, et al. 2009. MG53 nucleates assemblyof cell membrane repair machinery. Nat. Cell Biol. 11:56–64
49. Mauro A. 1961. Satellite cell of skeletal muscle fibers. J. Biophys. Biochem. Cytol. 9:493–9550. Goldring K, Partridge T, Watt D. 2002. Muscle stem cells. J. Pathol. 197:457–6751. Pallafacchina G, Francois S, Regnault B, Czarny B, Dive V, et al. 2010. An adult tissue-specific stem cell
in its niche: a gene profiling analysis of in vivo quiescent and activated muscle satellite cells. Stem CellRes. 4:77–91
52. Jacobs SC, Wokke JH, Bar PR, Bootsma AL. 1995. Satellite cell activation after muscle damage in youngand adult rats. Anat. Rec. 242:329–36
53. McGeachie JK, Grounds MD. 1987. Initiation and duration of muscle precursor replication after mildand severe injury to skeletal muscle of mice. An autoradiographic study. Cell Tissue Res. 248:125–30
54. Ciemerych MA, Archacka K, Grabowska I, Przewozniak M. 2011. Cell cycle regulation during prolifer-ation and differentiation of mammalian muscle precursor cells. Results Probl. Cell Differ. 53:473–527
55. Litwack G. 2011. Stem cell regulators. Preface. Vitam. Horm. 87:xxi–xxii
466 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
56. Taipale J, Keski-Oja J. 1997. Growth factors in the extracellular matrix. FASEB J. 11:51–5957. Christov C, Chretien F, Abou-Khalil R, Bassez G, Vallet G, et al. 2007. Muscle satellite cells and
endothelial cells: close neighbors and privileged partners. Mol. Biol. Cell 18:1397–40958. Tidball JG. 1995. Inflammatory cell response to acute muscle injury. Med. Sci. Sports Exerc. 27:1022–32
59. Identifies Pax7 as akey regulator of satellitecells; Pax7−/− skeletalmuscle is depleted ofsatellite cells and showsdefective postnatalmuscle growth.
59. Seale P, Sabourin LA, Girgis-Gabardo A, Mansouri A, Gruss P, Rudnicki MA. 2000. Pax7 isrequired for the specification of myogenic satellite cells. Cell 102:777–86
60. Cornelison DD, Filla MS, Stanley HM, Rapraeger AC, Olwin BB. 2001. Syndecan-3 and syndecan-4specifically mark skeletal muscle satellite cells and are implicated in satellite cell maintenance and muscleregeneration. Dev. Biol. 239:79–94
61. Beauchamp JR, Heslop L, Yu DS, Tajbakhsh S, Kelly RG, et al. 2000. Expression of CD34 and Myf5defines the majority of quiescent adult skeletal muscle satellite cells. J. Cell Biol. 151:1221–34
62. Dhawan J, Rando TA. 2005. Stem cells in postnatal myogenesis: molecular mechanisms of satellite cellquiescence, activation and replenishment. Trends Cell Biol. 15:666–73
63. Zammit PS, Golding JP, Nagata Y, Hudon V, Partridge TA, Beauchamp JR. 2004. Muscle satellite cellsadopt divergent fates: a mechanism for self-renewal? J. Cell Biol. 166:347–57
64. Conboy IM, Rando TA. 2002. The regulation of Notch signaling controls satellite cell activation andcell fate determination in postnatal myogenesis. Dev. Cell 3:397–409
65. Brack AS, Conboy IM, Conboy MJ, Shen J, Rando TA. 2008. A temporal switch from notch to Wntsignaling in muscle stem cells is necessary for normal adult myogenesis. Cell Stem Cell 2:50–59
66. Shinin V, Gayraud-Morel B, Gomes D, Tajbakhsh S. 2006. Asymmetric division and cosegregation oftemplate DNA strands in adult muscle satellite cells. Nat. Cell Biol. 8:677–87
67. Conboy MJ, Karasov AO, Rando TA. 2007. High incidence of non-random template strand segregationand asymmetric fate determination in dividing stem cells and their progeny. PLoS Biol. 5:e102
68. Shows that Pax7high
satellite cells performasymmetric celldivisions and thatdaughter cells thatretain the templateDNA strands expressstem cell markers.
68. Rocheteau P, Gayraud-Morel B, Siegl-Cachedenier I, Blasco MA, Tajbakhsh S. 2012. A subpop-ulation of adult skeletal muscle stem cells retains all template DNA strands after cell division.Cell 148:112–25
69. McCroskery S, Thomas M, Maxwell L, Sharma M, Kambadur R. 2003. Myostatin negatively regulatessatellite cell activation and self-renewal. J. Cell Biol. 162:1135–47
70. Pisconti A, Brunelli S, Di Padova M, De Palma C, Deponti D, et al. 2006. Follistatin induction by nitricoxide through cyclic GMP: a tightly regulated signaling pathway that controls myoblast fusion. J. CellBiol. 172:233–44
71. Amthor H, Otto A, Vulin A, Rochat A, Dumonceaux J, et al. 2009. Muscle hypertrophy driven bymyostatin blockade does not require stem/precursor-cell activity. Proc. Natl. Acad. Sci. USA 106:7479–84
72. Lescaudron L, Peltekian E, Fontaine-Perus J, Paulin D, Zampieri M, et al. 1999. Blood bornemacrophages are essential for the triggering of muscle regeneration following muscle transplant. Neu-romuscul. Disord. 9:72–80
73. Joe AW, Yi L, Natarajan A, Le Grand F, So L, et al. 2010. Muscle injury activates resident fi-bro/adipogenic progenitors that facilitate myogenesis. Nat. Cell Biol. 12:153–63
74. Uezumi A, Fukada S, Yamamoto N, Takeda S, Tsuchida K. 2010. Mesenchymal progenitors distinctfrom satellite cells contribute to ectopic fat cell formation in skeletal muscle. Nat. Cell Biol. 12:143–52
75. Fielding RA, Manfredi TJ, Ding W, Fiatarone MA, Evans WJ, Cannon JG. 1993. Acute phase responsein exercise. III. Neutrophil and IL-1β accumulation in skeletal muscle. Am. J. Physiol. Regul. Integr.Comp. Physiol. 265:166–72
76. Tidball JG. 2005. Inflammatory processes in muscle injury and repair. Am. J. Physiol. Regul. Integr. Comp.Physiol. 288:345–53
77. Tidball JG, Wehling-Henricks M. 2007. The role of free radicals in the pathophysiology of musculardystrophy. J. Appl. Physiol. 102:1677–86
78. Mantovani A, Sica A, Locati M. 2005. Macrophage polarization comes of age. Immunity 23:344–4679. Merly F, Lescaudron L, Rouaud T, Crossin F, Gardahaut MF. 1999. Macrophages enhance muscle
satellite cell proliferation and delay their differentiation. Muscle Nerve 22:724–3280. Cantini M, Massimino ML, Bruson A, Catani C, Dalla Libera L, Carraro U. 1994. Macrophages regulate
proliferation and differentiation of satellite cells. Biochem. Biophys. Res. Commun. 202:1688–96
www.annualreviews.org • Skeletal Muscle Disease and Therapy 467
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
81. Massimino ML, Rapizzi E, Cantini M, Libera LD, Mazzoleni F, et al. 1997. ED2+ macrophages increaseselectively myoblast proliferation in muscle cultures. Biochem. Biophys. Res. Commun. 235:754–59
82. Sherwood RI, Christensen JL, Conboy IM, Conboy MJ, Rando TA, et al. 2004. Isolation of adultmouse myogenic progenitors: functional heterogeneity of cells within and engrafting skeletal muscle.Cell 119:543–54
83. Schulz TJ, Huang TL, Tran TT, Zhang H, Townsend KL, et al. 2011. Identification of inducible brownadipocyte progenitors residing in skeletal muscle and white fat. Proc. Natl. Acad. Sci. USA 108:143–48
84. Burghes AH, Logan C, Hu X, Belfall B, Worton RG, Ray PN. 1987. A cDNA clone from theDuchenne/Becker muscular dystrophy gene. Nature 328:434–37
85. Chaturvedi LS, Mukherjee M, Srivastava S, Mittal RD, Mittal B. 2001. Point mutation and polymorphismin Duchenne/Becker muscular dystrophy (D/BMD) patients. Exp. Mol. Med. 33:251–56
86. Ervasti JM, Campbell KP. 1991. Membrane organization of the dystrophin-glycoprotein complex. Cell66:1121–31
87. Straub V, Bittner RE, Leger JJ, Voit T. 1992. Direct visualization of the dystrophin network on skeletalmuscle fiber membrane. J. Cell Biol. 119:1183–91
88. Koenig M, Kunkel LM. 1990. Detailed analysis of the repeat domain of dystrophin reveals four potentialhinge segments that may confer flexibility. J. Biol. Chem. 265:4560–66
89. Ibraghimov-Beskrovnaya O, Ervasti JM, Leveille CJ, Slaughter CA, Sernett SW, Campbell KP. 1992.Primary structure of dystrophin-associated glycoproteins linking dystrophin to the extracellular matrix.Nature 355:696–702
90. Campbell KP, Kahl SD. 1989. Association of dystrophin and an integral membrane glycoprotein. Nature338:259–62
91. Sacco A, Mourkioti F, Tran R, Choi J, Llewellyn M, et al. 2010. Short telomeres and stem cell exhaustionmodel Duchenne muscular dystrophy in mdx/mTR mice. Cell 143:1059–71
92. Cerletti M, Jurga S, Witczak CA, Hirshman MF, Shadrach JL, et al. 2008. Highly efficient, functionalengraftment of skeletal muscle stem cells in dystrophic muscles. Cell 134:37–47
93. Wallace GQ, McNally EM. 2009. Mechanisms of muscle degeneration, regeneration, and repair in themuscular dystrophies. Annu. Rev. Physiol. 71:37–57
94. Brenman JE, Chao DS, Gee SH, McGee AW, Craven SE, et al. 1996. Interaction of nitric oxide syn-thase with the postsynaptic density protein PSD-95 and α1-syntrophin mediated by PDZ domains. Cell84:757–67
95. Sander M, Chavoshan B, Harris SA, Iannaccone ST, Stull JT, et al. 2000. Functional muscle ischemia inneuronal nitric oxide synthase–deficient skeletal muscle of children with Duchenne muscular dystrophy.Proc. Natl. Acad. Sci. USA 97:13818–23
96. Spencer MJ, Tidball JG. 2001. Do immune cells promote the pathology of dystrophin-deficient my-opathies? Neuromuscul. Disord. 11:556–64
97. McNally EM, Pytel P. 2007. Muscle diseases: the muscular dystrophies. Annu. Rev. Pathol. Mech. Dis.2:87–109
98. Yazaki M, Yoshida K, Nakamura A, Koyama J, Nanba T, et al. 1999. Clinical characteristics of agedBecker muscular dystrophy patients with onset after 30 years. Eur. Neurol. 42:145–49
99. Harper PS, Van Engelen BGM, Eymard B, Wilcox DE. 2004. Myotonic Dystrophy: Present Management,Future Therapy. Oxford, UK/New York: Oxford Univ. Press. 251 pp.
100. Brook JD, McCurrach ME, Harley HG, Buckler AJ, Church D, et al. 1992. Molecular basis of myotonicdystrophy: expansion of a trinucleotide (CTG) repeat at the 3′ end of a transcript encoding a proteinkinase family member. Cell 68:799–808
101. Fu YH, Pizzuti A, Fenwick RG Jr, King J, Rajnarayan S, et al. 1992. An unstable triplet repeat in a generelated to myotonic muscular dystrophy. Science 255:1256–58
102. Mahadevan M, Tsilfidis C, Sabourin L, Shutler G, Amemiya C, et al. 1992. Myotonic dystrophy mutation:an unstable CTG repeat in the 3′ untranslated region of the gene. Science 255:1253–55
103. Ashizawa T, Dubel JR, Harati Y. 1993. Somatic instability of CTG repeat in myotonic dystrophy.Neurology 43:2674–78
468 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
104. Ashizawa T, Dubel JR, Dunne PW, Dunne CJ, Fu YH, et al. 1992. Anticipation in myotonic dystrophy.II. Complex relationships between clinical findings and structure of the GCT repeat. Neurology 42:1877–83
105. Reddy S, Smith DB, Rich MM, Leferovich JM, Reilly P, et al. 1996. Mice lacking the myotonic dystrophyprotein kinase develop a late onset progressive myopathy. Nat. Genet. 13:325–35
106. Liquori CL, Ricker K, Moseley ML, Jacobsen JF, Kress W, et al. 2001. Myotonic dystrophy type 2caused by a CCTG expansion in intron 1 of ZNF9. Science 293:864–67
107. Taneja KL, McCurrach M, Schalling M, Housman D, Singer RH. 1995. Foci of trinucleotide repeattranscripts in nuclei of myotonic dystrophy cells and tissues. J. Cell Biol. 128:995–1002
108. Davis BM, McCurrach ME, Taneja KL, Singer RH, Housman DE. 1997. Expansion of a CUG trinu-cleotide repeat in the 3′ untranslated region of myotonic dystrophy protein kinase transcripts results innuclear retention of transcripts. Proc. Natl. Acad. Sci. USA 94:7388–93
109. Demonstrates thatexpression of expandedCUG repeats outsidetheir normal DMPKcontext is sufficient toelicit myotonicdystrophy features inmice.
109. Mankodi A, Logigian E, Callahan L, McClain C, White R, et al. 2000. Myotonic dystrophy intransgenic mice expressing an expanded CUG repeat. Science 289:1769–73
110. Miller JW, Urbinati CR, Teng-Umnuay P, Stenberg MG, Byrne BJ, et al. 2000. Recruitment of humanmuscleblind proteins to (CUG)n expansions associated with myotonic dystrophy. EMBO J. 19:4439–48
111. Shows that geneticablation ofMuscleblind-likeprotein 1 reproducessome myotonicdystrophy features inmice, includingmyotonia.
111. Kanadia RN, Johnstone KA, Mankodi A, Lungu C, Thornton CA, et al. 2003. A muscleblindknockout model for myotonic dystrophy. Science 302:1978–80
112. Kanadia RN, Shin J, Yuan Y, Beattie SG, Wheeler TM, et al. 2006. Reversal of RNA missplicing andmyotonia after muscleblind overexpression in a mouse poly(CUG) model for myotonic dystrophy. Proc.Natl. Acad. Sci. USA 103:11748–53
113. Begemann G, Paricio N, Artero R, Kiss I, Perez-Alonso M, Mlodzik M. 1997. muscleblind, a generequired for photoreceptor differentiation in Drosophila, encodes novel nuclear Cys3His-type zinc-finger-containing proteins. Development 124:4321–31
114. Pascual M, Vicente M, Monferrer L, Artero R. 2006. The Muscleblind family of proteins: an emergingclass of regulators of developmentally programmed alternative splicing. Differentiation 74:65–80
115. Charlet BN, Savkur RS, Singh G, Philips AV, Grice EA, Cooper TA. 2002. Loss of the muscle-specificchloride channel in type 1 myotonic dystrophy due to misregulated alternative splicing. Mol. Cell 10:45–53
116. Du H, Cline MS, Osborne RJ, Tuttle DL, Clark TA, et al. 2010. Aberrant alternative splicing andextracellular matrix gene expression in mouse models of myotonic dystrophy. Nat. Struct. Mol. Biol.17:187–93
117. Fugier C, Klein AF, Hammer C, Vassilopoulos S, Ivarsson Y, et al. 2011. Misregulated alternative splicingof BIN1 is associated with T tubule alterations and muscle weakness in myotonic dystrophy. Nat. Med.17:720–25
118. Savkur RS, Philips AV, Cooper TA. 2001. Aberrant regulation of insulin receptor alternative splicing isassociated with insulin resistance in myotonic dystrophy. Nat. Genet. 29:40–47
119. Tang ZZ, Yarotskyy V, Wei L, Sobczak K, Nakamori M, et al. 2012. Muscle weakness in myotonicdystrophy associated with misregulated splicing and altered gating of CaV1.1 calcium channel. Hum.Mol. Genet. 21:1312–24
120. Philips AV, Timchenko LT, Cooper TA. 1998. Disruption of splicing regulated by a CUG-bindingprotein in myotonic dystrophy. Science 280:737–41
121. Timchenko LT, Miller JW, Timchenko NA, DeVore DR, Datar KV, et al. 1996. Identification of a(CUG)n triplet repeat RNA-binding protein and its expression in myotonic dystrophy. Nucleic Acids Res.24:4407–14
122. Kuyumcu-Martinez NM, Wang GS, Cooper TA. 2007. Increased steady-state levels of CUGBP1 inmyotonic dystrophy 1 are due to PKC-mediated hyperphosphorylation. Mol. Cell 28:68–78
123. Ho TH, Bundman D, Armstrong DL, Cooper TA. 2005. Transgenic mice expressing CUG-BP1 re-produce splicing mis-regulation observed in myotonic dystrophy. Hum. Mol. Genet. 14:1539–47
124. Le Ber I, Martinez M, Campion D, Laquerriere A, Betard C, et al. 2004. A non-DM1, non-DM2multisystem myotonic disorder with frontotemporal dementia: phenotype and suggestive mapping ofthe DM3 locus to chromosome 15q21-24. Brain 127:1979–92
www.annualreviews.org • Skeletal Muscle Disease and Therapy 469
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
125. Mathews KD, Moore SA. 2003. Limb-girdle muscular dystrophy. Curr. Neurol. Neurosci. Rep. 3:78–85126. Hauser MA, Horrigan SK, Salmikangas P, Torian UM, Viles KD, et al. 2000. Myotilin is mutated in
limb girdle muscular dystrophy 1A. Hum. Mol. Genet. 9:2141–47127. Salmikangas P, Mykkanen OM, Gronholm M, Heiska L, Kere J, Carpen O. 1999. Myotilin, a novel
sarcomeric protein with two Ig-like domains, is encoded by a candidate gene for limb-girdle musculardystrophy. Hum. Mol. Genet. 8:1329–36
128. Muchir A, Bonne G, van der Kooi AJ, van Meegen M, Baas F, et al. 2000. Identification of mutations in thegene encoding lamins A/C in autosomal dominant limb girdle muscular dystrophy with atrioventricularconduction disturbances (LGMD1B). Hum. Mol. Genet. 9:1453–59
129. Minetti C, Sotgia F, Bruno C, Scartezzini P, Broda P, et al. 1998. Mutations in the caveolin-3 gene causeautosomal dominant limb-girdle muscular dystrophy. Nat. Genet. 18:365–68
130. Tang Z, Scherer PE, Okamoto T, Song K, Chu C, et al. 1996. Molecular cloning of caveolin-3, a novelmember of the caveolin gene family expressed predominantly in muscle. J. Biol. Chem. 271:2255–61
131. Matsuda C, Hayashi YK, Ogawa M, Aoki M, Murayama K, et al. 2001. The sarcolemmal proteinsdysferlin and caveolin-3 interact in skeletal muscle. Hum. Mol. Genet. 10:1761–66
132. Hernandez-Deviez DJ, Martin S, Laval SH, Lo HP, Cooper ST, et al. 2006. Aberrant dysferlin traffickingin cells lacking caveolin or expressing dystrophy mutants of caveolin-3. Hum. Mol. Genet. 15:129–42
133. Vassilopoulos S, Oddoux S, Groh S, Cacheux M, Faure J, et al. 2010. Caveolin 3 is associated with thecalcium release complex and is modified via in vivo triadin modification. Biochemistry 49:6130–35
134. Ojima K, Kawabata Y, Nakao H, Nakao K, Doi N, et al. 2010. Dynamic distribution of muscle-specificcalpain in mice has a key role in physical-stress adaptation and is impaired in muscular dystrophy. J. Clin.Investig. 120:2672–83
135. Huang Y, Verheesen P, Roussis A, Frankhuizen W, Ginjaar I, et al. 2005. Protein studies in dysfer-linopathy patients using llama-derived antibody fragments selected by phage display. Eur. J. Hum. Genet.13:721–30
136. Duguez S, Bartoli M, Richard I. 2006. Calpain 3: a key regulator of the sarcomere? FEBS J. 273:3427–36137. Taveau M, Bourg N, Sillon G, Roudaut C, Bartoli M, Richard I. 2003. Calpain 3 is activated through
autolysis within the active site and lyses sarcomeric and sarcolemmal components. Mol. Cell. Biol. 23:9127–35
138. Guyon JR, Kudryashova E, Potts A, Dalkilic I, Brosius MA, et al. 2003. Calpain 3 cleaves filamin C andregulates its ability to interact with γ- and δ-sarcoglycans. Muscle Nerve 28:472–83
139. Baghdiguian S, Richard I, Martin M, Coopman P, Beckmann JS, et al. 2001. Pathophysiology of limbgirdle muscular dystrophy type 2A: hypothesis and new insights into the IκBα/NF-κB survival pathwayin skeletal muscle. J. Mol. Med. 79:254–61
140. Piccolo F, Moore SA, Ford GC, Campbell KP. 2000. Intracellular accumulation and reduced sarcolem-mal expression of dysferlin in limb-girdle muscular dystrophies. Ann. Neurol. 48:902–12
141. Selcen D, Stilling G, Engel AG. 2001. The earliest pathologic alterations in dysferlinopathy. Neurology56:1472–81
142. de Luna N, Gallardo E, Soriano M, Dominguez-Perles R, de la Torre C, et al. 2006. Absence of dysferlinalters myogenin expression and delays human muscle differentiation “in vitro”. J. Biol. Chem. 281:17092–98
143. Lostal W, Bartoli M, Roudaut C, Bourg N, Krahn M, et al. 2012. Lack of correlation between outcomesof membrane repair assay and correction of dystrophic changes in experimental therapeutic strategy indysferlinopathy. PLoS ONE 7:e38036
144. Liu J, Aoki M, Illa I, Wu C, Fardeau M, et al. 1998. Dysferlin, a novel skeletal muscle gene, is mutatedin Miyoshi myopathy and limb girdle muscular dystrophy. Nat. Genet. 20:31–36
145. Gallardo E, Rojas-Garcia R, de Luna N, Pou A, Brown RH Jr, Illa I. 2001. Inflammation in dysferlinmyopathy: immunohistochemical characterization of 13 patients. Neurology 57:2136–38
146. Weiler T, Bashir R, Anderson LV, Davison K, Moss JA, et al. 1999. Identical mutation in patients withlimb girdle muscular dystrophy type 2B or Miyoshi myopathy suggests a role for modifier gene(s). Hum.Mol. Genet. 8:871–77
147. Sandona D, Betto R. 2009. Sarcoglycanopathies: molecular pathogenesis and therapeutic prospects.Expert Rev. Mol. Med. 11:e28
470 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
148. Vainzof M, Passos-Bueno MR, Canovas M, Moreira ES, Pavanello RC, et al. 1996. The sarcoglycancomplex in the six autosomal recessive limb-girdle muscular dystrophies. Hum. Mol. Genet. 5:1963–69
149. Hack AA, Lam MY, Cordier L, Shoturma DI, Ly CT, et al. 2000. Differential requirement for individualsarcoglycans and dystrophin in the assembly and function of the dystrophin-glycoprotein complex. J.Cell Sci. 113(Part 14):2535–44
150. Politano L, Nigro V, Passamano L, Petretta V, Comi LI, et al. 2001. Evaluation of cardiac and respiratoryinvolvement in sarcoglycanopathies. Neuromuscul. Disord. 11:178–85
151. Gregorio CC, Granzier H, Sorimachi H, Labeit S. 1999. Muscle assembly: a titanic achievement? Curr.Opin. Cell Biol. 11:18–25
152. Kudryashova E, Kudryashov D, Kramerova I, Spencer MJ. 2005. Trim32 is a ubiquitin ligase mutatedin limb girdle muscular dystrophy type 2H that binds to skeletal muscle myosin and ubiquitinates actin.J. Mol. Biol. 354:413–24
153. Bolduc V, Marlow G, Boycott KM, Saleki K, Inoue H, et al. 2010. Recessive mutations in the putativecalcium-activated chloride channel Anoctamin 5 cause proximal LGMD2L and distal MMD3 musculardystrophies. Am. J. Hum. Genet. 86:213–21
154. Nigro V, Aurino S, Piluso G. 2011. Limb girdle muscular dystrophies: update on genetic diagnosis andtherapeutic approaches. Curr. Opin. Neurol. 24:429–36
155. Tawil R, Van Der Maarel SM. 2006. Facioscapulohumeral muscular dystrophy. Muscle Nerve 34:1–15156. Wijmenga C, Frants RR, Brouwer OF, Moerer P, Weber JL, Padberg GW. 1990. Location of fa-
cioscapulohumeral muscular dystrophy gene on chromosome 4. Lancet 336:651–53157. Wijmenga C, Hewitt JE, Sandkuijl LA, Clark LN, Wright TJ, et al. 1992. Chromosome 4q DNA
rearrangements associated with facioscapulohumeral muscular dystrophy. Nat. Genet. 2:26–30158. Lemmers RJ, van der Vliet PJ, Klooster R, Sacconi S, Camano P, et al. 2010. A unifying genetic model
for facioscapulohumeral muscular dystrophy. Science 329:1650–53159. Geng LN, Yao Z, Snider L, Fong AP, Cech JN, et al. 2012. DUX4 activates germline genes, retroele-
ments, and immune mediators: implications for facioscapulohumeral dystrophy. Dev. Cell 22:38–51160. Muchir A, Worman HJ. 2007. Emery–Dreifuss muscular dystrophy. Curr. Neurol. Neurosci. Rep. 7:78–83161. Bione S, Maestrini E, Rivella S, Mancini M, Regis S, et al. 1994. Identification of a novel X-linked gene
responsible for Emery–Dreifuss muscular dystrophy. Nat. Genet. 8:323–27162. Bonne G, Di Barletta MR, Varnous S, Becane HM, Hammouda EH, et al. 1999. Mutations in the
gene encoding lamin A/C cause autosomal dominant Emery–Dreifuss muscular dystrophy. Nat. Genet.21:285–88
163. Raffaele Di Barletta M, Ricci E, Galluzzi G, Tonali P, Mora M, et al. 2000. Different mutations in theLMNA gene cause autosomal dominant and autosomal recessive Emery–Dreifuss muscular dystrophy.Am. J. Hum. Genet. 66:1407–12
164. Zhang Q, Bethmann C, Worth NF, Davies JD, Wasner C, et al. 2007. Nesprin-1 and -2 are involved inthe pathogenesis of Emery–Dreifuss muscular dystrophy and are critical for nuclear envelope integrity.Hum. Mol. Genet. 16:2816–33
165. Manilal S, Nguyen TM, Sewry CA, Morris GE. 1996. The Emery–Dreifuss muscular dystrophy protein,emerin, is a nuclear membrane protein. Hum. Mol. Genet. 5:801–8
166. Segura-Totten M, Wilson KL. 2004. BAF: roles in chromatin, nuclear structure and retrovirus integra-tion. Trends Cell Biol. 14:261–66
167. Haque F, Lloyd DJ, Smallwood DT, Dent CL, Shanahan CM, et al. 2006. SUN1 interacts with nuclearlamin A and cytoplasmic nesprins to provide a physical connection between the nuclear lamina and thecytoskeleton. Mol. Cell. Biol. 26:3738–51
168. Worman HJ, Courvalin JC. 2004. How do mutations in lamins A and C cause disease? J. Clin. Investig.113:349–51
169. Martin PT. 2007. Congenital muscular dystrophies involving the O-mannose pathway. Curr. Mol. Med.7:417–25
170. Michele DE, Barresi R, Kanagawa M, Saito F, Cohn RD, et al. 2002. Post-translational disruption ofdystroglycan-ligand interactions in congenital muscular dystrophies. Nature 418:417–22
171. Muntoni F, Brockington M, Godfrey C, Ackroyd M, Robb S, et al. 2007. Muscular dystrophies due todefective glycosylation of dystroglycan. Acta Myol. 26:129–35
www.annualreviews.org • Skeletal Muscle Disease and Therapy 471
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
172. Collins J, Bonnemann CG. 2010. Congenital muscular dystrophies: toward molecular therapeutic inter-ventions. Curr. Neurol. Neurosci. Rep. 10:83–91
173. Kaplan JC. 2008. Gene table of monogenic neuromuscular disorders (nuclear genome only). Neuromuscul.Disord. 18:101–29
174. Arbogast S, Beuvin M, Fraysse B, Zhou H, Muntoni F, Ferreiro A. 2009. Oxidative stress in SEPN1-related myopathy: from pathophysiology to treatment. Ann. Neurol. 65:677–86
175. Deniziak M, Thisse C, Rederstorff M, Hindelang C, Thisse B, Lescure A. 2007. Loss of selenoproteinN function causes disruption of muscle architecture in the zebrafish embryo. Exp. Res. 313:156–67
176. Quijano-Roy S, Mbieleu B, Bonnemann CG, Jeannet PY, Colomer J, et al. 2008. De novo LMNAmutations cause a new form of congenital muscular dystrophy. Ann. Neurol. 64:177–86
177. Moreira ES, Wiltshire TJ, Faulkner G, Nilforoushan A, Vainzof M, et al. 2000. Limb-girdle musculardystrophy type 2G is caused by mutations in the gene encoding the sarcomeric protein telethonin. Nat.Genet. 24:163–66
178. Ferreiro A, Mezmezian M, Olive M, Herlicoviez D, Fardeau M, et al. 2011. Telethonin-deficiencyinitially presenting as a congenital muscular dystrophy. Neuromuscul. Disord. 21:433–38
179. Jang YC, Sinha M, Cerletti M, Dall’osso C, Wagers AJ. 2011. Skeletal muscle stem cells: effects of agingand metabolism on muscle regenerative function. Cold Spring Harb. Symp. Quant. Biol. 76:101–11
180. Shadrach JL, Wagers AJ. 2011. Stem cells for skeletal muscle repair. Philos. Trans. R. Soc. Lond. B366:2297–306
181. Snijders T, Verdijk LB, van Loon LJ. 2009. The impact of sarcopenia and exercise training on skeletalmuscle satellite cells. Ageing Res. Rev. 8:328–38
182. Conboy IM, Conboy MJ, Smythe GM, Rando TA. 2003. Notch-mediated restoration of regenerativepotential to aged muscle. Science 302:1575–77
183. Carlson ME, Hsu M, Conboy IM. 2008. Imbalance between pSmad3 and Notch induces CDK inhibitorsin old muscle stem cells. Nature 454:528–32
184. Conboy IM, Conboy MJ, Wagers AJ, Girma ER, Weissman IL, Rando TA. 2005. Rejuvenation of agedprogenitor cells by exposure to a young systemic environment. Nature 433:760–64
185. Brack AS, Conboy MJ, Roy S, Lee M, Kuo CJ, et al. 2007. Increased Wnt signaling during aging altersmuscle stem cell fate and increases fibrosis. Science 317:807–10
186. Muir LA, Chamberlain JS. 2009. Emerging strategies for cell and gene therapy of the muscular dystro-phies. Expert Rev. Mol. Med. 11:e18
187. Partridge TA. 2011. Impending therapies for Duchenne muscular dystrophy. Curr. Opin. Neurol. 24:415–22
188. Miller RG, Sharma KR, Pavlath GK, Gussoni E, Mynhier M, et al. 1997. Myoblast implantation inDuchenne muscular dystrophy: the San Francisco study. Muscle Nerve 20:469–78
189. Tremblay JP, Guerette B. 1997. Myoblast transplantation: a brief review of the problems and of somesolutions. Basic Appl. Myol. 7:221–30
190. Sampaolesi M, Blot S, D’Antona G, Granger N, Tonlorenzi R, et al. 2006. Mesoangioblast stem cellsameliorate muscle function in dystrophic dogs. Nature 444:574–79
191. Dellavalle A, Sampaolesi M, Tonlorenzi R, Tagliafico E, Sacchetti B, et al. 2007. Pericytes of humanskeletal muscle are myogenic precursors distinct from satellite cells. Nat. Cell Biol. 9:255–67
192. Cossu G, Bianco P. 2003. Mesoangioblasts—vascular progenitors for extravascular mesodermal tissues.Curr. Opin. Genet. Dev. 13:537–42
193. Dellavalle A, Maroli G, Covarello D, Azzoni E, Innocenzi A, et al. 2011. Pericytes resident in postnatalskeletal muscle differentiate into muscle fibres and generate satellite cells. Nat. Commun. 2:499
194. Negroni E, Riederer I, Chaouch S, Belicchi M, Razini P, et al. 2009. In vivo myogenic potential ofhuman CD133+ muscle-derived stem cells: a quantitative study. Mol. Ther. 17:1771–78
195. Bachrach E, Perez AL, Choi YH, Illigens BM, Jun SJ, et al. 2006. Muscle engraftment of myogenicprogenitor cells following intraarterial transplantation. Muscle Nerve 34:44–52
196. Sampaolesi M, Torrente Y, Innocenzi A, Tonlorenzi R, D’Antona G, et al. 2003. Cell therapy of α-sarcoglycan null dystrophic mice through intra-arterial delivery of mesoangioblasts. Science 301:487–92
197. Gussoni E, Soneoka Y, Strickland CD, Buzney EA, Khan MK, et al. 1999. Dystrophin expression in themdx mouse restored by stem cell transplantation. Nature 401:390–94
472 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
198. LaBarge MA, Blau HM. 2002. Biological progression from adult bone marrow to mononucleate musclestem cell to multinucleate muscle fiber in response to injury. Cell 111:589–601
199. Sherwood RI, Christensen JL, Weissman IL, Wagers AJ. 2004. Determinants of skeletal muscle contri-butions from circulating cells, bone marrow cells, and hematopoietic stem cells. Stem Cells 22:1292–304
200. Gussoni E, Bennett RR, Muskiewicz KR, Meyerrose T, Nolta JA, et al. 2002. Long-term persistence ofdonor nuclei in a Duchenne muscular dystrophy patient receiving bone marrow transplantation. J. Clin.Investig. 110:807–14
201. Yu J, Vodyanik MA, Smuga-Otto K, Antosiewicz-Bourget J, Frane JL, et al. 2007. Induced pluripotentstem cell lines derived from human somatic cells. Science 318:1917–20
202. Takahashi K, Tanabe K, Ohnuki M, Narita M, Ichisaka T, et al. 2007. Induction of pluripotent stemcells from adult human fibroblasts by defined factors. Cell 131:861–72
203. Rashid ST, Vallier L. 2010. Induced pluripotent stem cells—alchemist’s tale or clinical reality? ExpertRev. Mol. Med. 12:25
204. Darabi R, Baik J, Clee M, Kyba M, Tupler R, Perlingeiro RC. 2009. Engraftment of embryonic stemcell–derived myogenic progenitors in a dominant model of muscular dystrophy. Exp. Neurol. 220:212–16
205. Darabi R, Gehlbach K, Bachoo RM, Kamath S, Osawa M, et al. 2008. Functional skeletal muscle regen-eration from differentiating embryonic stem cells. Nat. Med. 14:134–43
206. Darabi R, Pan W, Bosnakovski D, Baik J, Kyba M, Perlingeiro RC. 2011. Functional myogenic engraft-ment from mouse iPS cells. Stem Cell Rev. 7:948–57
207. Darabi R, Santos FN, Filareto A, Pan W, Koene R, et al. 2011. Assessment of the myogenic stem cellcompartment following transplantation of Pax3/Pax7-induced embryonic stem cell–derived progenitors.Stem Cells 29:777–90
208. Mizuno Y, Chang H, Umeda K, Niwa A, Iwasa T, et al. 2010. Generation of skeletal musclestem/progenitor cells from murine induced pluripotent stem cells. FASEB J. 24:2245–53
209. Kazuki Y, Hiratsuka M, Takiguchi M, Osaki M, Kajitani N, et al. 2010. Complete genetic correction ofips cells from Duchenne muscular dystrophy. Mol. Ther. 18:386–93
210. DeFrancesco L. 2011. Move over ZFNs. Nat. Biotechnol. 29:681–84211. Wells DJ, Ferrer A, Wells KE. 2002. Immunological hurdles in the path to gene therapy for Duchenne
muscular dystrophy. Expert Rev. Mol. Med. 4:1–23212. De Luca A, Pierno S, Camerino C, Cocchi D, Camerino DC. 1999. Higher content of insulin-like
growth factor I in dystrophic mdx mouse: potential role in the spontaneous regeneration through anelectrophysiological investigation of muscle function. Neuromuscul. Disord. 9:11–18
213. Singleton JR, Feldman EL. 2001. Insulin-like growth factor I in muscle metabolism and myotherapies.Neurobiol. Dis. 8:541–54
214. Gregorevic P, Plant DR, Lynch GS. 2004. Administration of insulin-like growth factor I improves fatigueresistance of skeletal muscles from dystrophic mdx mice. Muscle Nerve 30:295–304
215. Gregorevic P, Plant DR, Leeding KS, Bach LA, Lynch GS. 2002. Improved contractile function of themdx dystrophic mouse diaphragm muscle after insulin-like growth factor I administration. Am. J. Pathol.161:2263–72
216. Lynch GS, Cuffe SA, Plant DR, Gregorevic P. 2001. IGF-I treatment improves the functional propertiesof fast- and slow-twitch skeletal muscles from dystrophic mice. Neuromuscul. Disord. 11:260–68
217. McPherron AC, Lawler AM, Lee SJ. 1997. Regulation of skeletal muscle mass in mice by a new TGF-βsuperfamily member. Nature 387:83–90
218. Grobet L, Martin LJ, Poncelet D, Pirottin D, Brouwers B, et al. 1997. A deletion in the bovine myostatingene causes the double-muscled phenotype in cattle. Nat. Genet. 17:71–74
219. Schuelke M, Wagner KR, Stolz LE, Hubner C, Riebel T, et al. 2004. Myostatin mutation associatedwith gross muscle hypertrophy in a child. N. Engl. J. Med. 350:2682–88
220. Bogdanovich S, Krag TO, Barton ER, Morris LD, Whittemore LA, et al. 2002. Functional improvementof dystrophic muscle by myostatin blockade. Nature 420:418–21
221. Bogdanovich S, Perkins KJ, Krag TO, Whittemore LA, Khurana TS. 2005. Myostatin propeptide-mediated amelioration of dystrophic pathophysiology. FASEB J. 19:543–49
222. Rooney JE, Gurpur PB, Burkin DJ. 2009. Laminin-111 protein therapy prevents muscle disease in themdx mouse model for Duchenne muscular dystrophy. Proc. Natl. Acad. Sci. USA 106:7991–96
www.annualreviews.org • Skeletal Muscle Disease and Therapy 473
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
223. Goudenege S, Lamarre Y, Dumont N, Rousseau J, Frenette J, et al. 2010. Laminin-111: a potentialtherapeutic agent for Duchenne muscular dystrophy. J. Am. Soc. Gene Ther. 18:2155–63
224. Tinsley JM, Blake DJ, Roche A, Fairbrother U, Riss J, et al. 1992. Primary structure of dystrophin-relatedprotein. Nature 360:591–93
225. Squire S, Raymackers JM, Vandebrouck C, Potter A, Tinsley J, et al. 2002. Prevention of pathology inmdx mice by expression of utrophin: analysis using an inducible transgenic expression system. Hum. Mol.Genet. 11:3333–44
226. Gilbert R, Nalbantoglu J, Petrof BJ, Ebihara S, Guibinga GH, et al. 1999. Adenovirus-mediated utrophingene transfer mitigates the dystrophic phenotype of mdx mouse muscles. Hum. Gene Ther. 10:1299–310
227. Sonnemann KJ, Heun-Johnson H, Turner AJ, Baltgalvis KA, Lowe DA, Ervasti JM. 2009. Functionalsubstitution by TAT-utrophin in dystrophin-deficient mice. PLoS Med. 6:e1000083
228. Call JA, Ervasti JM, Lowe DA. 2011. TAT-μUtrophin mitigates the pathophysiology of dystrophin andutrophin double-knockout mice. J. Appl. Physiol. 111:200–5
229. Amenta AR, Yilmaz A, Bogdanovich S, McKechnie BA, Abedi M, et al. 2011. Biglycan recruits utrophinto the sarcolemma and counters dystrophic pathology in mdx mice. Proc. Natl. Acad. Sci. USA 108:762–67
230. Casar JC, McKechnie BA, Fallon JR, Young MF, Brandan E. 2004. Transient up-regulation of bigly-can during skeletal muscle regeneration: delayed fiber growth along with decorin increase in biglycan-deficient mice. Dev. Biol. 268:358–71
231. Amenta AR, Creely HE, Mercado ML, Hagiwara H, McKechnie BA, et al. 2012. Biglycan is an extra-cellular MuSK binding protein important for synapse stability. J. Neurosci. 32:2324–34
232. Wilton SD, Lloyd F, Carville K, Fletcher S, Honeyman K, et al. 1999. Specific removal of the nonsensemutation from the mdx dystrophin mRNA using antisense oligonucleotides. Neuromuscul. Disord. 9:330–38
233. Lu QL, Mann CJ, Lou F, Bou-Gharios G, Morris GE, et al. 2003. Functional amounts of dystrophinproduced by skipping the mutated exon in the mdx dystrophic mouse. Nat. Med. 9:1009–14
234. Lu QL, Rabinowitz A, Chen YC, Yokota T, Yin H, et al. 2005. Systemic delivery of antisense oligori-bonucleotide restores dystrophin expression in body-wide skeletal muscles. Proc. Natl. Acad. Sci. USA102:198–203
235. van Deutekom JC, Janson AA, Ginjaar IB, Frankhuizen WS, Aartsma-Rus A, et al. 2007. Local dystrophinrestoration with antisense oligonucleotide PRO051. N. Engl. J. Med. 357:2677–86
236. Goemans NM, Buyse G, Tulinius M, Verschuuren JJG, de Kimpe SJ, van Deutekom JCT. 2009. A phaseI/IIa study on antisense compound PRO051 in patients with Duchenne muscular dystrophy. Neuromuscul.Disord. 19:659–60
237. Gebski BL, Mann CJ, Fletcher S, Wilton SD. 2003. Morpholino antisense oligonucleotide induceddystrophin exon 23 skipping in mdx mouse muscle. Hum. Mol. Genet. 12:1801–11
238. Alter J, Lou F, Rabinowitz A, Yin H, Rosenfeld J, et al. 2006. Systemic delivery of morpholino oligonu-cleotide restores dystrophin expression bodywide and improves dystrophic pathology. Nat. Med. 12:175–77
239. Reports thatintramuscular injectionof AVI-4658 had noadverse effects in DMDpatients and causedexpression ofdystrophin in injectedmuscles.
239. Kinali M, Arechavala-Gomeza V, Feng L, Cirak S, Hunt D, et al. 2009. Local restoration ofdystrophin expression with the morpholino oligomer AVI-4658 in Duchenne muscular dystro-phy: a single-blind, placebo-controlled, dose-escalation, proof-of-concept study. Lancet Neurol.8:918–28
240. Wheeler TM, Lueck JD, Swanson MS, Dirksen RT, Thornton CA. 2007. Correction of ClC-1 splicingeliminates chloride channelopathy and myotonia in mouse models of myotonic dystrophy. J. Clin. Investig.117:3952–57
241. Wheeler TM, Sobczak K, Lueck JD, Osborne RJ, Lin X, et al. 2009. Reversal of RNA dominance bydisplacement of protein sequestered on triplet repeat RNA. Science 325:336–39
242. Mulders SA, van den Broek WJ, Wheeler TM, Croes HJ, van Kuik-Romeijn P, et al. 2009. Triplet-repeat oligonucleotide-mediated reversal of RNA toxicity in myotonic dystrophy. Proc. Natl. Acad. Sci.USA 106:13915–20
243. Lee JE, Bennett CF, Cooper TA. RNase H–mediated degradation of toxic RNA in myotonic dystrophytype 1. Proc. Natl. Acad. Sci. USA 109:4221–26
474 Tabebordbar ·Wang ·Wagers
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08CH17-Wagers ARI 17 December 2012 8:58
244. Escolar DM, Scacheri CG. 2001. Pharmacologic and genetic therapy for childhood muscular dystrophies.Curr. Neurol. Neurosci. Rep. 1:168–74
245. Manzur AY, Kuntzer T, Pike M, Swan A. 2008. Glucocorticoid corticosteroids for Duchenne musculardystrophy. Cochrane Database Syst. Rev. CD003725
246. Aartsma-Rus A, Van Deutekom JC, Fokkema IF, Van Ommen GJ, Den Dunnen JT. 2006. Entries in theLeiden Duchenne muscular dystrophy mutation database: an overview of mutation types and paradoxicalcases that confirm the reading-frame rule. Muscle Nerve 34:135–44
247. Manuvakhova M, Keeling K, Bedwell DM. 2000. Aminoglycoside antibiotics mediate context-dependentsuppression of termination codons in a mammalian translation system. RNA 6:1044–55
248. Barton-Davis ER, Cordier L, Shoturma DI, Leland SE, Sweeney HL. 1999. Aminoglycoside antibioticsrestore dystrophin function to skeletal muscles of mdx mice. J. Clin. Investig. 104:375–81
249. Finkel RS. 2010. Read-through strategies for suppression of nonsense mutations in Duchenne/Beckermuscular dystrophy: aminoglycosides and ataluren (PTC124). J. Child Neurol. 25:1158–64
250. Reports thatPTC-124 restoreddystrophin productionin mdx mice and humanprimary muscle cellswith nonsensemutations in thedystrophin gene.
250. Welch EM, Barton ER, Zhuo J, Tomizawa Y, Friesen WJ, et al. 2007. PTC124 targets geneticdisorders caused by nonsense mutations. Nature 447:87–91
251. Tinsley JM, Fairclough RJ, Storer R, Wilkes FJ, Potter AC, et al. 2011. Daily treatment with SMTC1100,a novel small molecule utrophin upregulator, dramatically reduces the dystrophic symptoms in the mdxmouse. PLoS ONE 6:e19189
252. Demonstrates thataminophylline restoresthe normal structure ofskeletal muscle in azebra fish model ofDMD.
252. Kawahara G, Karpf JA, Myers JA, Alexander MS, Guyon JR, Kunkel LM. 2011. Drug screeningin a zebrafish model of Duchenne muscular dystrophy. Proc. Natl. Acad. Sci. USA 108:5331–36
253. Essayan DM. 2001. Cyclic nucleotide phosphodiesterases. J. Allergy Clin. Immunol. 108:671–80254. Adamo CM, Dai DF, Percival JM, Minami E, Willis MS, et al. 2010. Sildenafil reverses cardiac dysfunc-
tion in the mdx mouse model of Duchenne muscular dystrophy. Proc. Natl. Acad. Sci. USA 107:19079–83255. Asai A, Sahani N, Kaneki M, Ouchi Y, Martyn JA, Yasuhara SE. 2007. Primary role of functional ischemia,
quantitative evidence for the two-hit mechanism, and phosphodiesterase-5 inhibitor therapy in mousemuscular dystrophy. PLoS ONE 2:e806
256. Gareiss PC, Sobczak K, McNaughton BR, Palde PB, Thornton CA, Miller BL. 2008. Dynamic combina-torial selection of molecules capable of inhibiting the (CUG) repeat RNA-MBNL1 interaction in vitro:discovery of lead compounds targeting myotonic dystrophy (DM1). J. Am. Chem. Soc. 130:16254–61
257. Warf MB, Nakamori M, Matthys CM, Thornton CA, Berglund JA. 2009. Pentamidine reverses thesplicing defects associated with myotonic dystrophy. Proc. Natl. Acad. Sci. USA 106:18551–56
258. Arambula JF, Ramisetty SR, Baranger AM, Zimmerman SC. 2009. A simple ligand that selectively targetsCUG trinucleotide repeats and inhibits MBNL protein binding. Proc. Natl. Acad. Sci. USA 106:16068–73
259. Parkesh R, Childs-Disney JL, Nakamori M, Kumar A, Wang E, et al. 2012. Design of a bioactivesmall molecule that targets the myotonic dystrophy type 1 RNA via an RNA motif–ligand database andchemical similarity searching. J. Am. Chem. Soc. 134:4731–42
260. Pushechnikov A, Lee MM, Childs-Disney JL, Sobczak K, French JM, et al. 2009. Rational design ofligands targeting triplet repeating transcripts that cause RNA dominant disease: application to myotonicmuscular dystrophy type 1 and spinocerebellar ataxia type 3. J. Am. Chem. Soc. 131:9767–79
261. Logigian EL, Martens WB, Moxley RT IV, McDermott MP, Dilek N, et al. 2010. Mexiletine is aneffective antimyotonia treatment in myotonic dystrophy type 1. Neurology 74:1441–48
262. Han R, Campbell KP. 2007. Dysferlin and muscle membrane repair. Curr. Opin. Cell Biol. 19:409–16
www.annualreviews.org • Skeletal Muscle Disease and Therapy 475
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08-FrontMatter ARI 17 December 2012 9:46
Annual Review ofPathology:Mechanisms ofDisease
Volume 8, 2013Contents
Pathogenesis of Langerhans Cell HistiocytosisGayane Badalian-Very, Jo-Anne Vergilio, Mark Fleming,
and Barrett J. Rollins � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1
Molecular Pathophysiology of Myelodysplastic SyndromesR. Coleman Lindsley and Benjamin L. Ebert � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �21
The Role of Telomere Biology in CancerLifeng Xu, Shang Li, and Bradley A. Stohr � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �49
Chromosome Translocation, B Cell Lymphoma,and Activation-Induced Cytidine DeaminaseDavide F. Robbiani and Michel C. Nussenzweig � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �79
Autophagy as a Stress-Response and Quality-Control Mechanism:Implications for Cell Injury and Human DiseaseLyndsay Murrow and Jayanta Debnath � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 105
Pathogenesis of Antineutrophil Cytoplasmic Autoantibody–AssociatedSmall-Vessel VasculitisJ. Charles Jennette, Ronald J. Falk, Peiqi Hu, and Hong Xiao � � � � � � � � � � � � � � � � � � � � � � � � � 139
Molecular Basis of Asbestos-Induced Lung DiseaseGang Liu, Paul Cheresh, and David W. Kamp � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 161
Progressive Multifocal Leukoencephalopathy: Why Grayand White MatterSarah Gheuens, Christian Wuthrich, and Igor J. Koralnik � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 189
IgA Nephropathy: Molecular Mechanisms of the DiseaseJiri Mestecky, Milan Raska, Bruce A. Julian, Ali G. Gharavi,
Matthew B. Renfrow, Zina Moldoveanu, Lea Novak, Karel Matousovic,and Jan Novak � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 217
Host Responses in Tissue Repair and FibrosisJeremy S. Duffield, Mark Lupher, Victor J. Thannickal,
and Thomas A. Wynn � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 241
v
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.

PM08-FrontMatter ARI 17 December 2012 9:46
Cellular Heterogeneity and Molecular Evolution in CancerVanessa Almendro, Andriy Marusyk, and Kornelia Polyak � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 277
The Immunobiology and Pathophysiology of Primary Biliary CirrhosisGideon M. Hirschfield and M. Eric Gershwin � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 303
Digital Imaging in Pathology: Whole-Slide Imaging and BeyondFarzad Ghaznavi, Andrew Evans, Anant Madabhushi,
and Michael Feldman � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 331
Pathological and Molecular Advances in PediatricLow-Grade AstrocytomaFausto J. Rodriguez, Kah Suan Lim, Daniel Bowers,
and Charles G. Eberhart � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 361
Diagnostic Applications of High-Throughput DNA SequencingScott D. Boyd � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 381
Pathogenesis of the Viral Hemorrhagic FeversSlobodan Paessler and David H. Walker � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 411
Skeletal Muscle Degenerative Diseases and Strategies for TherapeuticMuscle RepairMohammadsharif Tabebordbar, Eric T. Wang, and Amy J. Wagers � � � � � � � � � � � � � � � � � � � 441
The Th17 Pathway and Inflammatory Diseases of the Intestines,Lungs, and SkinCasey T. Weaver, Charles O. Elson, Lynette A. Fouser, and Jay K. Kolls � � � � � � � � � � � � � � 477
Indexes
Cumulative Index of Contributing Authors, Volumes 1–8 � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 513
Cumulative Index of Article Titles, Volumes 1–8 � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 517
Errata
An online log of corrections to Annual Review of Pathology: Mechanisms of Disease articlesmay be found at http://pathol.annualreviews.org
vi Contents
Ann
u. R
ev. P
atho
l. M
ech.
Dis
. 201
3.8:
441-
475.
Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
Har
vard
Uni
vers
ity o
n 02
/02/
13. F
or p
erso
nal u
se o
nly.