Site Initiation Meeting – May 23, 2013 Montreal General Hospital, McGill CRP Nadine Ezer Clinical...
61
Site Initiation Meeting – May 23, 2013 Montreal General Hospital, McGill CRP Nadine Ezer Clinical Trial Monitor Roche
-
Upload
ethan-harvey -
Category
Documents
-
view
216 -
download
0
Transcript of Site Initiation Meeting – May 23, 2013 Montreal General Hospital, McGill CRP Nadine Ezer Clinical...
Site Initiation Meeting – May 23, 2013
Montreal General Hospital, McGill CRP
Nadine Ezer Clinical Trial Monitor Roche

2
JACOB Study(BO25114)
A double-blind, placebo-controlled, randomized, multicenter Phase III Study evaluating the efficacy and safety of pertuzumab in combination with trastuzumab and chemotherapy in patients with HER2-positive metastatic gastroesophageal junction and gastric cancer

3
The global statusStudy Timelines & Status
Final Protocol(27 Sep)
1st Investigator
meeting(Mar)
1st Site activation(Mar/Apr)
780 subjects recruited
FPI(Apr
2013)
LPI(May 2016)
Final Primary Analysis(Jun 2017)
2012 2014 - 2015 2016 2018 - 202220172013
LSLO
CompletedUpcomingStudy MilestonesData Point
1st Interim Safety Analysis(Oct 2013)
2nd Interim Safety Analysis(Feb 2014)
1st HA/IRB approval
(Dec)
Interim Analysis
70% OS event(Sep 2016)

4
OUR 2013 SMT (GDT) Goal for the JACOB Study
Enrollment of 110 patients of the total 780 patients required
by 31 December 2013

5
Other Teams Supporting the Study
IXRS
Central Laboratory
Central HER2 Testing

Overview of Gastric/GEJ cancer

7
Increasing incidence of adenocarcinoma of gastric cardia/GEJ• Multifactorial etiology (obesity, gastroesophageal reflux, diets high in
salted/smoked foods, FH, H. pylori, tobacco and alcohol use)• 65% diagnosed with regional/distant disease3
• Median survival < 1 year – better treatments are needed!
4th most common cancer diagnosis (1,000,000 new cases each year) 1
3rd leading cause of cancer death in males globally (700,000 deaths) 2
>70% of new cases and deaths occur in developing countries 2 –
Gastric/GEJ Adenocarcinoma
6. cardia (including gastroesophageal junction)
1. GLOBOCAN 20082. Jemal et al., CA CANCER J CLIN 2011;61:69–903. Howlader SEER data 2001-7

10
The incidence of gastric cancer is highest in Asia
Parkin DM, et al. CA Cancer J Clin 2005; 55:74–108.
Age-standardised incidence(per 100,000)
Incidence Mortality
60 50 40 30 20 10 10 20 30 40 50 60
Eastern AsiaCentral and Eastern Europe
Less developed regionsWorld
South AmericaMore developed regions
Central AmericaSouthern Europe
South-Eastern AsiaCaribbeanPolynesia
Melanesia
Northern Europe
Australia/New ZealandSouth-Central Asia
Middle AfricaEastern Africa
Northern AmericaWestern Africa
Micronesia
Western Europe
Southern AfricaNorthern Africa
Western Asia
0
Male Female

11
Gastric cancer clinical presentation/RX
Abdominal pain, weight loss, obstruction, GI bleed
Limited disease (resectable without distant mets)
• Surgical resection of primary tumor and LN with perioperative chemotherapy and XRT
Locally advanced (unresectable)/metastatic
• Chemotherapy – differs by geographic region, - usual regimens: ECF, EOF, ECX, TC
• Biologic therapy (eg. Trastuzumab, Met inhibiting agents)
• Palliative surgery (e.g. bypass)
• Palliative radiotherapy
12
HER2 positive cancer
Breast cancer 20% HER2 positive• Trastuzumab with chemotherapy improves OS in adjuvant and metastatic settings
Gastric cancer 20% HER2 positive • Trastuzumab with chemotherapy improves OS in metastatic settings (ToGA)
HER2 positive rates may be slightly lower in Asian populations (19 vs. 15%)
Different guidelines for interpreting HER2+ in gastric vs. breast cancer• Breast cancer methods result in underscoring of HER2 in gastric ca
New HER2 targeted therapies• Lapatinib: oral TKI of HER1 and HER2 approved for met breast ca
• TYTAN trial in second line HER2+ (by FISH) GC lapatinib did not prolong OS• LOGiC trial in first line HER2+ GC
• Pertuzumab: IV monoclonal antibody targets HER2• T-DM1: IV antibody drug conjugate targets HER2
Bang et al Lancet 2010 / Hofmann et al Histopath 2008 / Ruschoff et al Mod Path 2012

13
ToGA trial designPhase III, randomized, open-label, international, multicenter study
Locally Advanced (inoperable) vs. Metastatic GC vs. GEJMeasurable vs. Non-measurableECOG PS 0-1 vs. 2Capecitabine vs. 5-FU
Primary endpoint OS
a Chosen at investigator’s discretion 1 Bang et al; Abstract 4556, ASCO 2009
GEJ, gastroesophageal junctionBang Lancet 2010
5-FU or capecitabine a + cisplatin
(n=290)
RHER2-positiveadvanced GC
(n=584)5-FU or capecitabine a
+ cisplatin + trastuzumab(n=294)
3807 patients screened
810 HER2-positive
(22.1%)(IHC 3+ or FISH +)
Stratification factors

14
ToGA (BO18255)
The results of the ToGA study (Herceptin®/trastuzumab plus fluoropyrimidine-cisplatin chemotherapy) established a new standard of care for treatment of HER2 positive AGC*: Adding trastuzumab to chemotherapy prolongs survival
Median OS duration improved from 11.1 to 13.8 months in the full analysis population
Median OS duration improved from 11.8 to 16.0 months in the high HER2 overexpressing population (tumors that are IHC3+ or IHC2+/ISH+)
* AGC = Advanced Gastric Cancer Defined as Inoperable, locally advanced or metastatic gastric/GEJ adenocarcinoma

15
No.at riskF/X + C + H
F/X + C
13.8
K-M Plot of Overall Survival in ToGA Study(full analysis population)
H, Herceptin / Bang YJ., et al., Lancet 2010; 376: 687-697
Time (Months)
Even
t
1.0
0.8
0.6
0.2
0
0.4
0
294
290
36
0
0
20
43
24
10
147
117
32
4
0
4
246
223
16
71
47
24
21
14
28
12
6
2
277
266
6
209
185
8
173
143
12
113
90
14
90
64
18
56
32
22
30
16
26
13
7
30
6
5
34
1
0
HR = 0.7495% CI (0.60, 0.91)p value = 0.0046
OS13.8
Events167182 11.1
F/X + C + HF/X + C
11.1
Median

16
No.at riskFC + H
FC
K-M Plot of Overall Survival in ToGA Study(High HER2 overexpressors = IHC3+ or IHC2+/FISH+)
H, Herceptin / Bang YJ., et al., Lancet 2010; 376: 687-697
Time (Months)
Even
t
1.0
0.8
0.6
0.2
0
0.4
0
228
218
36
0
0
20
39
20
10
122
96
32
4
0
4
196
170
16
65
39
24
20
11
28
11
3
2
218
198
6
170
141
8
142
112
12
100
75
14
84
53
18
51
28
22
28
13
26
12
4
30
5
3
34
1
0
HR = 0.6595% CI (0.51, 0.83)
OS16.0
Events120136 11.8
FC + HFC
Median
16.0
11.8

17
Evidence that pertuzumab + trastuzumab are more active than either agent alone
Pertuzumab has a different mechanism of action and a different binding site on the HER2 receptor than trastuzumab
Additive activity in pre-clinical animal models• Breast cancer• Gastric cancer
Activity seen in phase II/III studies in HER2 positive BC• BO17929 (phase II – 2nd line MBC)• NEOSPHERE (phase II – EBC)• CLEOPATRA (phase III – 1st line MBC)

18
Pertuzumab (Perjeta)
An IgG1 (k) humanized monoclonal antibody
Produced in CHO (Chinese Hamster Ovary) cell cultures
Targets the HER2 receptor extra-cellular domain (sub-domain II)
Adams CW et al. Cancer Immunol Immunother 2006

19
Pertuzumab and trastuzumabbind different epitopes on HER2
• Inhibits ligand-independent HER2 signalling• Prevents HER2 ECD shedding• Activates ADCC
• Inhibits ligand-dependent HER2 signalling• Inhibits HER2 hetero-dimerization • Activates ADCC• Non-competitive with trastuzumab
due to different binding domain on HER2 receptorHubbard SR Cancer Cell 2005; Molina MA et al. Cancer Res 2001;Junttila TT et al. Cancer Cell 2009; Scheuer W et al. Cancer Res 2009;Franklin MC et al. Cancer Cell 2004; Agus DB et al. Cancer Cell 2002
pertuzumab
trastuzumab dimerization domain
Trastuzumab-HER2 complex Pertuzumab-HER2 complex

20
Patients treated with pertuzumab and trastuzumab until progression of disease or unmanageable toxicityIf docetaxel discontinued, treatment with pertuzumab and trastuzumab may continue
CLEOPATRA: Study Design: Registration Trial for Pertuzumab in Metastatic Breast Cancer
Pivotal CLEOPATRA trial: Multicenter, randomized, double-blind, placebo-controlled, Phase III study in patients with HER2+ metastatic breast cancer (mBC)
Placebo + trastuzumab (q3w)
Docetaxel (q3w)Minimum of 6 cycles
(n=406)
(n=402)
1:1‡ Docetaxel (q3w) Minimum of 6 cycles
Pertuzumab + trastuzumab (q3w)
20
q3w = every 3 weeks. * HER2 overexpression was defined as IHC 3+ or FISH amplification ratio ≥2.0. IHC 3+ is defined as uniform, intense membrane staining in >10% of tumor cells. † Patients with prior adjuvant or neoadjuvant therapy were required to have a disease-free interval of ≥12 months to be eligible for enrollment in the trial. ‡ Randomization was stratified by prior treatment status (de novo or prior adjuvant/neoadjuvant therapy) and geographic region (Europe, South America, and Asia).
Patients with HER2+,* locally recurrent, unresectable, or mBC previously untreated with a biologic or chemotherapy for metastatic disease† (n=808)

21
CLEOPATRA: Primary Endpoint1
Prog
ress
ion-
free
sur
viva
l (%
) 100
80
60
20
0
Time (Months)
40
Patients at riskPertuzumab+T+D
Placebo+T+D
Progression-Free Survival (PFS): A hazard ratio (HR) of 0.62 describes 38% reduction in risk of disease progression or death
* Stratified by prior treatment status and geographic region.Source: 1. PERJETA™ (pertuzumab) full prescribing information. Genentech, Inc., June 2012.
0
402
406
40
0
0
20
83
42
10
267
209
35
0
0
5
345
311
15
139
93
25
32
17
30
10
7
Pertuzumab +trastuzumab + docetaxel
Placebo + trastuzumab + docetaxel
HR = 0.62*95% CI (0.51, 0.75)p value = <0.0001
18.5
12.4

22
CLEOPATRA: Confirmatory interim analysis of overall survival (OS IA2)
Ove
rall
surv
ival
(%)
100
80
60
20
0
Time (Months)
40
Patients at riskPtz + T + D
Pla + T + D
D, docetaxel; OS, overall survival; Pla, placebo; Ptz, pertuzumab; T, trastuzumabS Swain, San Antonio Breast Cancer Symposium (SABCS), 2012 (Abstract #P5-18-26)
Pertuzumab + T + D: 113 events;median not reached
Placebo + T + D: 154 events; median 37.6 months
0
402
406
55
0
0
20
317
285
10
371
350
35
84
67
5
387
383
15
342
324
25
230
198
30
143
128
HR = 0.6695% CI (0.52−0.84)p value = 0.0008
40
33
22
45
9
4
50
0
0
Stopping boundary for concluding statistical significance at this interim analysis was p≤0.0138
Median follow-up: 30.0 months, n=267 OS events
23
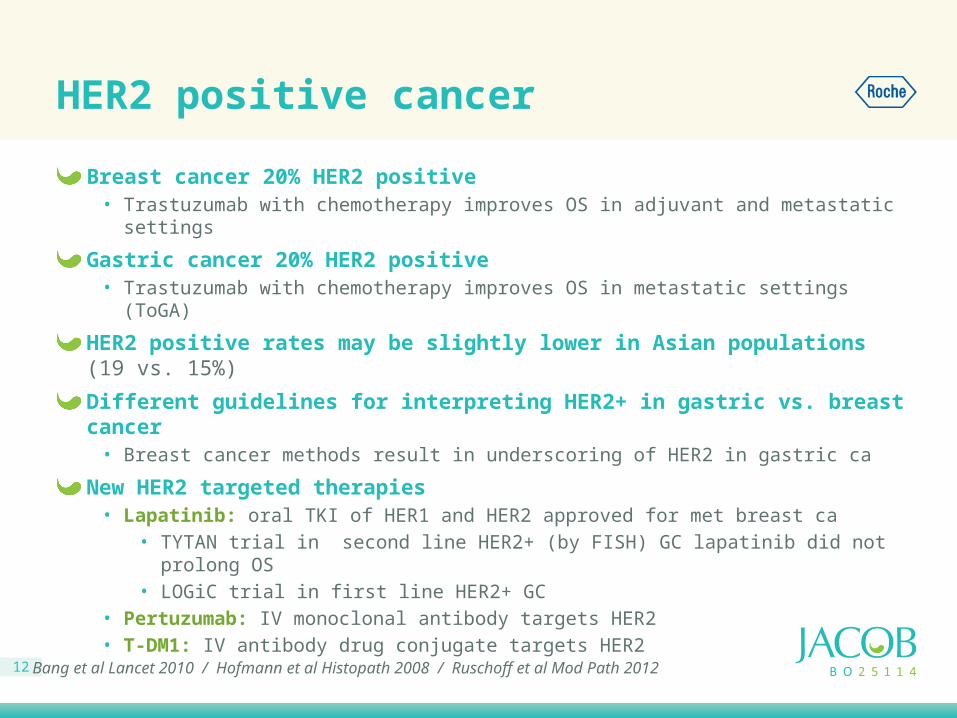
CLEOPATRA: Adverse events (all grades)≥25% incidence or ≥5% difference between arms
Adverse event, n (%) Placebo + trastuzumab + docetaxel (n=397)
Pertuzumab + trastuzumab + docetaxel (n=407)
Diarrhea 184 (46.3) 272 (66.8)Alopecia 240 (60.5) 248 (60.9)Neutropenia 197 (49.6) 215 (52.8)Nausea 165 (41.6) 172 (42.3)Fatigue 146 (36.8) 153 (37.6)Rash 96 (24.2) 137 (33.7)Decreased appetite 105 (26.4) 119 (29.2)Mucosal inflammation 79 (19.9) 113 (27.8)Asthenia 120 (30.2) 106 (26.0)Peripheral edema 119 (30.0) 94 (23.1)Constipation 99 (24.9) 61 (15.0)Febrile neutropenia 30 (7.6) 56 (13.8)Dry skin 17 (4.3) 43 (10.6)

24
Perjeta/Pertuzumab 1st Line MBCApprovals as of 16 May 2013
Country Approval
United States 08 Jun 2012
Switzerland 14 Aug 2012
Mexico 26 Sep 2012
Macau 03 Dec 2012
Uruguay 26 Dec 2012
Kosovo 20 Jan 2013
Georgia 21 Jan 2013
Aruba 31 Jan 2013
Kuwait 6 Feb 2013
Country Approval
Israel 12 Feb 2013
European Union 4 Mar 2013
Iceland Mar 2013
Canada 14 Apr 2013
Russia 16 Apr 2013
Argentina 25 Apr 2013
Norway Apr 2013
Luxemburg Apr 2013
Australia 5 May 2013

25
Rationale for a Phase III study of pertuzumab in HER2-positive gastric cancer
Preclinical data show that pertuzumab increased the activity of trastuzumab in HER2-positive gastric cancer xenograft models
HER2-positive gastric/GEJ cancer (ToGA): clinical evidence that HER2-targeted therapy extends survival
In HER2-positive mBC: CLEOPATRA study confirmed improved efficacy of combined HER2-directed therapy with docetaxel
Large safety database showing good tolerability across multiple indications , includes data with capecitabine and platinum
Plan → Phase III trial in advanced gastric/GEJ cancer.
• But what dose Pertuzumab in aGC ?

26
JOSHUA BP27836: Phase IIa study rationale
Determine pertuzumab dose in HER2 positive advanced GEJ/gastric cancer
Achieve PK clinical target for minimum pertuzumab concentration of 20 g/ml in >90% of patients
• Same clinical target concentration as in HER2-positive breast cancer
Move to Phase III with dose modeled from Phase IIa data

27
JOSHUA: Study design, Phase IIa trial
Estimate minimum (trough) serum pertuzumab concentration to identify a steady state of ≥20 g/ml in 90% of patientsSafety and tolerability
HER2-positiveinoperable locally
advanced or recurrent and/or metastatic GEJ/GC
(IHC3+ or IHC2+ and FISH+; ECOG PS 0 or 1)
Primary objectives:
Arm APertuzumab 840 mg,
then 420 mg + X + cisplatin x6 q3w
+ trastuzumabn=15
ECOG PS, Eastern Cooperative Oncology Group performance status; FISH, fluorescence in situ hybridisation; GC, gastric cancer; GEJ, gastroesophageal junction; IHC, immunohistochemistry; PD, progressive disease; pK, pharmacokinetics; X, capecitabine
Arm BPertuzumab 840 mg
+ X + cisplatin x6 q3w + trastuzumab
n=15
Dose selection for Phase III
study based on PK modelling

The JACOB Study (BO25114):
Rationale of Study Design and Protocol Overview
29
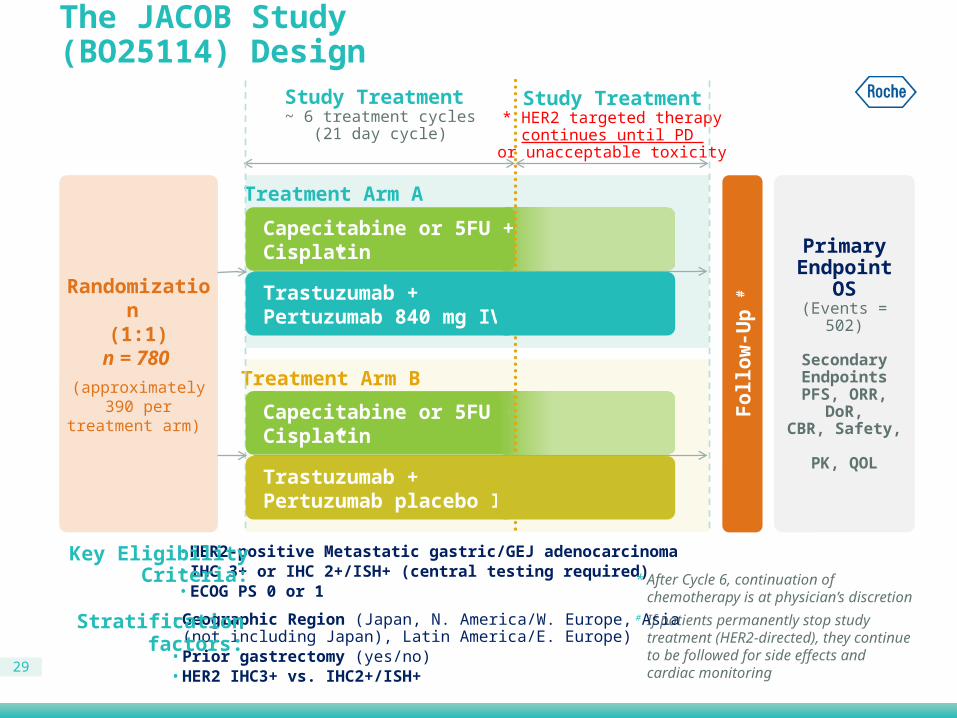
The JACOB Study (BO25114) Design
Randomization (1:1)
n = 780 (approximately
390 pertreatment arm)
Follo
w-U
p #
Study Treatment ~ 6 treatment cycles
(21 day cycle)
Study Treatment* HER2 targeted therapy
continues until PD or unacceptable toxicity
• HER2-positive Metastatic gastric/GEJ adenocarcinoma• IHC 3+ or IHC 2+/ISH+ (central testing required)• ECOG PS 0 or 1
Key EligibilityCriteria: * After Cycle 6, continuation of chemotherapy
is at physician’s discretion
Primary Endpoint
OS(Events = 502)
Secondary Endpoints
PFS, ORR, DoR,CBR, Safety,
PK, QOL
Treatment Arm A
Treatment Arm B
Capecitabine or 5FU + Cisplatin
Capecitabine or 5FU + Cisplatin
Trastuzumab + Pertuzumab 840 mg IV Q3W
Trastuzumab + Pertuzumab placebo IV Q3W
*
*
# If patients permanently stop study treatment (HER2-directed), they continue to be followed for side effects and cardiac monitoring
• Geographic Region (Japan, N. America/W. Europe, Asia (not including Japan), Latin America/E. Europe)• Prior gastrectomy (yes/no)• HER2 IHC3+ vs. IHC2+/ISH+
Stratificationfactors:

30
JACOB: Study endpoints
PrimaryOverall survival (15.0 vs. 19.3 mos, HR 0.78)
SecondaryPFS, ORR, duration of objective response, clinical benefit rateSafetyPKQoL
ExploratoryBiomarkers • Tumor tissue: HER receptor status, ERCC1, PTEN, PI3K, MET• Blood: HER2 ECD, HER ligands, anti-therapeutic antibody
ORR, objective response rate; PFS, progression-free survival; pK, pharmacokinetics; QoL, quality of life

31
JACOB: Biomarker Analyses Overview
* Minimum of 15 slides to be sent if country or site regulations do not allow shipment of a tumor block
Patient selection(Block/partial block*)
Exploratory BM Research(Block/partial block*)
RCR(Roche clinical repository, optional)
Central confirmation of HER2 (prospectively)
• IHC• ISH
• Serum • Plasma• Whole blood
sample for DNA extraction
• c-MET• ERCC1• PTEN• PIK3CA mutations• HER2/3 mRNA• HER3 protein
Biomarker analysis and sampling strategy in JACOB

32
JACOB: Statistical assumptions
Hazard ratio 0.78
Number of patients 780
Number of events for 80% power 502
Median OS: control vs. experimental arm, months 15 vs. 19.3 (Δ=4.3)
Minimum detectable difference at 80% power 0.8372.9 months
Enrollment*, months 38
Expected availability of OS data†, months 55 ~ Q4 2017
* Assuming a 5% withdrawal rate within 55 months† Clinical cut-off from EAST plus 2 monthsOS, overall survival

33
JACOB: Interim Analyses
Safety:Monthly review of AEs first six months
Regular safety monitoring reviews (approximately every 6 months)
Two formal interim safety analyses• After 50 patients have been enrolled and followed up for at least 2 months• After 100 patients have been enrolled and followed up for at least 4 months
Efficacy:One interim analysis of OS after 351 deaths have occurred

34
JACOB: Target Study Population
Approximately 780 patients with histologically confirmed metastatic GEJ/GC who have received no prior treatment for metastatic disease• Measurable or non-measurable evaluable (RECIST 1.1)
• ECOG PS 0 or 1
• Baseline LVEF ≥ 55% (MUGA or echocardiogram)
• Life expectancy ≥ 3 months
HER2 positive (IHC3+ or IHC2+/ISH+) tumor by central laboratory testing

35
Definition of HER2 positivity in JACOB
HER2 positivity isdefined as:
IHC 3+ (regardless of ISH results)
IHC 2+ if confirmed by a positive ISH result (cut-off for ISH ratio: 2.0 HER2/CEP17)
For IHC testing, the cut-off as approved by FDA in context of ToGA will apply
35
Screening population
IHC test
IHC 0 and 1+ IHC 2+ IHC 3+
Not eligible Reflex test by ISH eligible
ISH- ISH+
Not eligible eligible

36
Tissue requirements for HER2 central assessment
Tumor blocks preferred (submission of slides should be an exception!) Cutting at central lab ensures higher quality and higher level of
standardization and saves tissue!
If blocks not available a minimum of 15 unstained and freshly cut slides can be submitted for HER2 testing and exploratory Biomarker analyses (maximum 48hrs from slicing to shipment)Biopsy or surgical specimen of either primary or recurrent/metastatic tumor are allowed for HER2 assessment • For biopsies, ideally 6 to 8 biopsies taken from different metastatic
lesions should be submitted and assessed• Fine needle aspirates CANNOT be accepted
The fixative allowed is neutral buffered formalin (10%)

37
JACOB: Exclusion criteria
Cancer-Related Exclusion Criteria1. Previous systemic cytotoxic chemotherapy for advanced (inoperable or metastatic) disease
2. History of exposure to the following cumulative doses of anthracyclines:a) Epirubicin > 720 mg/m2
b) Doxorubicin or liposomal doxorubicin > 360 mg/m2
c) Mitoxantrone > 120 mg/m2 and idarubicin > 90 mg/m2
d) Other (e.g., other anthracycline greater than the equivalent of 360 mg/m2 of doxorubicin)e) If more than one anthracycline has been used, then the cumulative dose must not exceed the equivalent of 360 mg/m2 of
doxorubicin
3. Evidence of disease progression documented within 6 months after completion of prior neoadjuvant and/or adjuvant cytotoxic chemotherapy or radiotherapy for gastric/GEJ adenocarcinoma
4. Previous treatment with any HER2-directed therapy, at any time, for any duration
5. Previous exposure to any investigational treatment within 30 days before the first dose of study treatment
6. Radiotherapy within 30 days before the first dose of study treatment (within 2 weeks if given as palliation to peripheral bone metastases, if recovered from all toxicities)
7. History or evidence of brain metastasis
8. Clinically significant active GI bleeding (Grade ≥ 2 according to CTCAE v4.03)
9. Residual toxicity resulting from previous therapy, e.g., hematologic, cardiovascular, or neurologic toxicity that is Grade ≥ 2 (according to CTCAE v4.03). Alopecia is permitted
10. Other malignancy (in addition to GC) occurring within 5 years before enrollment, except for carcinoma in situ of the uterine cervix or squamous or basal cell carcinoma of the skin that has been previously treated with curative intent
1. Previous systemic cytotoxic chemotherapy for advanced (inoperable or metastatic) disease
2. History of exposure to the following cumulative doses of anthracyclines:a) Epirubicin > 720 mg/m2
b) Doxorubicin or liposomal doxorubicin > 360 mg/m2
c) Mitoxantrone > 120 mg/m2 and idarubicin > 90 mg/m2
d) Other (e.g., other anthracycline greater than the equivalent of 360 mg/m2 of doxorubicin)
e) If more than one anthracycline has been used, then the cumulative dose must not exceed the equivalent of 360 mg/m2 of doxorubicin
3. Evidence of disease progression documented within 6 months after completion of prior neoadjuvant and/or adjuvant cytotoxic chemotherapy or radiotherapy for gastric/GEJ adenocarcinoma
4. Previous treatment with any HER2-directed therapy, at any time, for any duration

38
JACOB: Exclusion criteria
Clinical Laboratory Exclusion Criteria (must be confirmed within 7 days before first dose of study treatment)11. Absolute neutrophil count (ANC) < 1.5 109/L
12. Platelet count < 75 109/L
13. Hemoglobin < 9.0 g/dL
14. Creatinine clearance < 60 mL/min/1.73 m²
15. Serum bilirubin (total) > 1.5 ULN of laboratory normal range; in case of known Gilbert’s disease a total bilirubin of 2 ULN is permitted
16. AST, ALT, and alkaline phosphatase (ALP) parameters:a) In patients with no liver and no bone metastases
i. AST or ALT > 1.5 × ULN, and ALP > 2.5 × ULNii. AST or ALT > 2.5 × ULN
b) In patients with liver metastases and no bone metastasesi. AST or ALT > 5 × ULN, and ALP > 2.5 × ULN
c) In patients with liver metastases and bone metastasesi. AST or ALT > 5 × ULN, and ALP > 10 × ULN
d) In patients with bone metastases and no liver metastasesi. AST or ALT > 1.5 × ULN, and ALP > 10 × ULN
17. Serum albumin < 25 g/L
18. Serum pregnancy test positive in a female patient of childbearing potential

39
JACOB: Exclusion criteria
General Exclusion Criteria
19. Documented history of congestive heart failure of any New York Heart Association (NYHA) criteria
20. Angina pectoris requiring treatment
21. Myocardial infarction within the past 6 months before the first dose of study treatment
22. Clinically significant valvular heart disease or uncontrollable high-risk cardiac arrhythmia, i.e., atrial tachycardia with a heart rate > 100/min at rest, significant ventricular arrhythmia (ventricular tachycardia) or higher-grade AV-block (second degree AV-block Type 2 [Mobitz 2] or third degree AV-block)
23. History or evidence of poorly controlled arterial hypertension (systolic blood pressure > 180 mmHg or diastolic blood pressure > 100 mmHg)
24. Baseline LVEF value < 55%, assessed by echocardiogram [ECHO], MUGA scan, or cardiac MRI
40
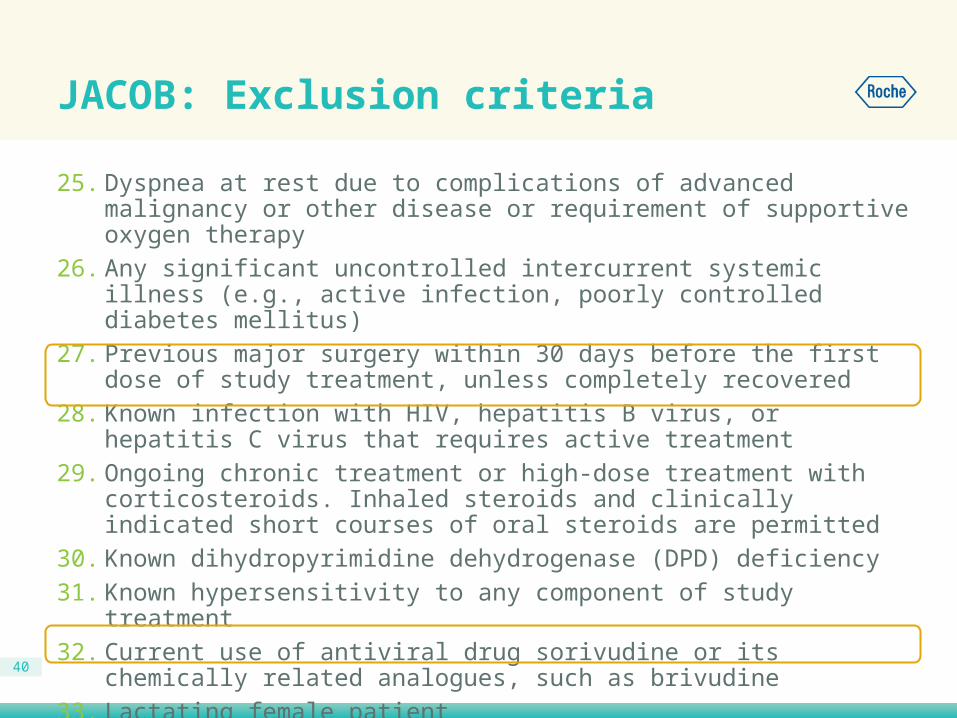
JACOB: Exclusion criteria
25. Dyspnea at rest due to complications of advanced malignancy or other disease or requirement of supportive oxygen therapy
26. Any significant uncontrolled intercurrent systemic illness (e.g., active infection, poorly controlled diabetes mellitus)
27. Previous major surgery within 30 days before the first dose of study treatment, unless completely recovered
28. Known infection with HIV, hepatitis B virus, or hepatitis C virus that requires active treatment
29. Ongoing chronic treatment or high-dose treatment with corticosteroids. Inhaled steroids and clinically indicated short courses of oral steroids are permitted
30. Known dihydropyrimidine dehydrogenase (DPD) deficiency31. Known hypersensitivity to any component of study treatment32. Current use of antiviral drug sorivudine or its chemically related analogues, such as
brivudine33. Lactating female patient34. Any patient unwilling or unable to use adequate contraceptive measures

41
Contraception
For women of childbearing potential and male participants with partners of childbearing potential: Agreement to use one highly effective form of contraception or two effective forms of non-hormonal contraception by the patient and/or partner while on study treatment and for 6 months after stopping study treatment:
Highly effective (any one)• True abstinence• Male sterilization• Tubal ligation• Combined hormonal contraceptives
Effective (any two)• IUD/IUS• Condom with spermicidal foam/gel/film/cream/suppository• Occlusive cap (diaphragm or cervical/vault cap) with
spermicidal foam/gel/film/cream/suppository
42
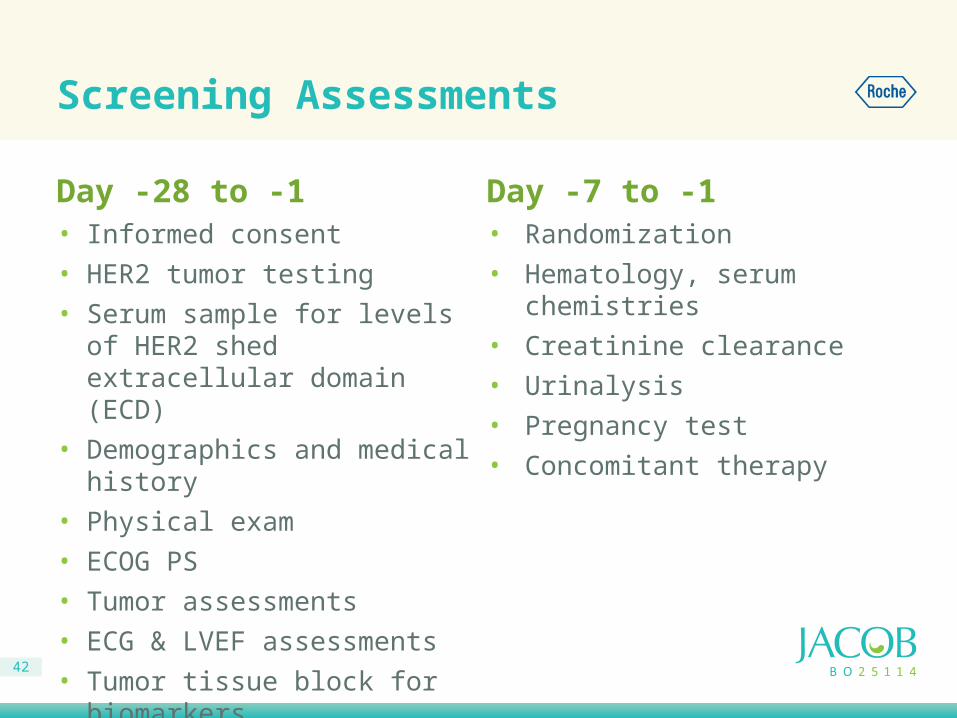
Screening Assessments
Day -28 to -1• Informed consent• HER2 tumor testing• Serum sample for levels of HER2
shed extracellular domain (ECD)• Demographics and medical history • Physical exam• ECOG PS• Tumor assessments• ECG & LVEF assessments• Tumor tissue block for biomarkers• Concomitant therapy
Day -7 to -1• Randomization• Hematology, serum chemistries• Creatinine clearance • Urinalysis• Pregnancy test• Concomitant therapy

43
JACOB: Study treatment
All agents will be given on the same day in the following order(pertuzumab/placebo → trastuzumab → chemotherapy)
Chemotherapy backbone will be administered on a 3-weekly schedule
• Capecitabine 1000 mg/m2 taken orally twice daily for 14 days then7 days off q3w
OR• 5-Fluorouracil 800 mg/m2/24 hours given intravenously by continuous
infusion for 120 hours (Days 1−5) q3w
• Cisplatin 80 mg/m2 intravenously (Day 1) q3w
• Pertuzumab 840 mg or placebo q 3 weeks• Trastuzumab 8 mg/kg initial dose, followed by 6 mg/kg q3w
with
with

44
Incomplete dose:If patient receives 50-75% of dose, the remainder should be given during the same treatment cycle, preferably before day 15 (Section 4.3.1.4.1 for details)
Administration guidelines for pertuzumab and trastuzumab
Administration Time (minutes)
Observation Time (minutes)
First dose
Pertuzumab/placebo 60 60
Trastuzumab 90 60
All later doses
Pertuzumab/placebo 30 30
Trastuzumab 30 30

The JACOB Study (BO25114):
Safety Monitoring

46
Overview of Safety Monitoring
Upfront discussion of diarrhea management and anti-diarrheal medicines prescribed
C1 Day 7 safety check (by phone) ** please document in source !
AE grading using CTCAE version 4.03• Progressive disease is not an AE
47
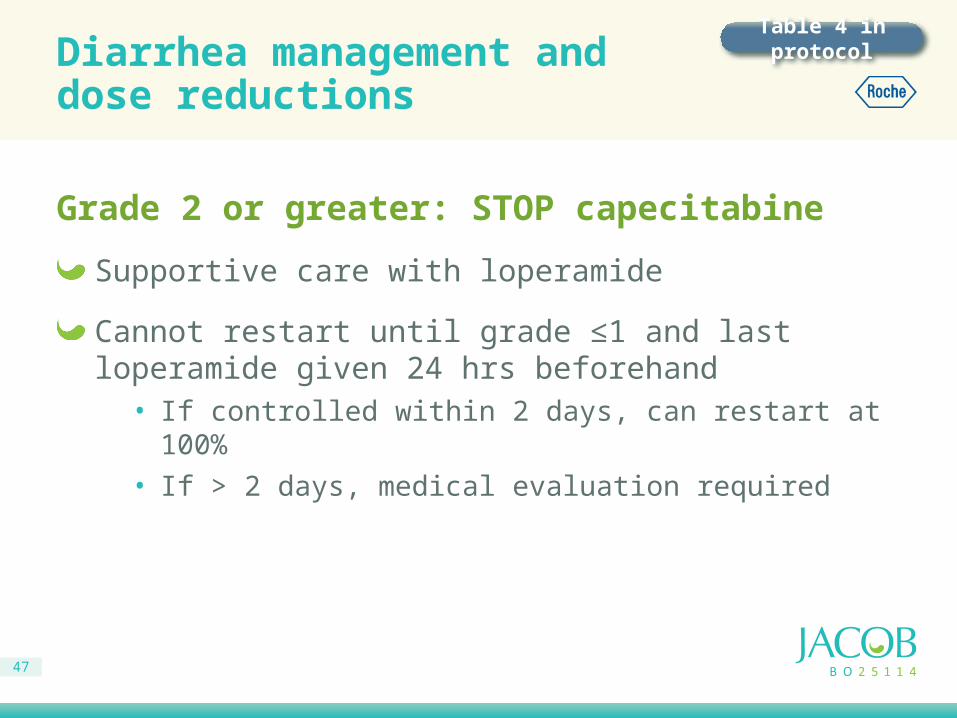
Diarrhea management anddose reductions
Grade 2 or greater: STOP capecitabine
Supportive care with loperamide
Cannot restart until grade ≤1 and last loperamide given 24 hrs beforehand• If controlled within 2 days, can restart at 100%• If > 2 days, medical evaluation required
Table 4 in protocol

48
Diarrhea grades
CTCAE Grade(v. 4.03)
1 Increase of < 4 stools per day over baseline; mild increase in ostomy output compared to baseline
2 Increase of 4 – 6 stools per day over baseline; moderate increase in ostomy output compared to baseline
3Increase of >= 7 stools per day over baseline; incontinence; hospitalization indicated; severe increase in ostomy output compared to baseline; limiting self care ADL
4 Life-threatening consequences; urgent intervention indicated
49
Dose Modifications for pertuzumab and trastuzumab
No dose reduction permitted for toxicity, for either pertuzumab or trastuzumab
Treatment with either pertuzumab or trastuzumab (or both) may be delayed to assess or treat AEs• Dosing should be resumed as soon as appropriate after the AE has
improved (see protocol section 4.3.1.4.1)• Patients should be re-assessed at least weekly to determine if
treatment can be resumed
If trastuzumab dosing is delayed and ≥ 6 weeks have elapsed since the last dose, a re-loading dose of 8 mg/kg should be given as the next dose, then resume the 6 mg/kg Q3W dosing schedule• Pertuzumab, capecitabine, and cisplatin dosing should be
re-synchronized to the new schedule

50
If recovery has not occurred after a delay of 3 weeks (i.e., 6 weeks since previous chemotherapy doses), the patient should be permanently discontinued from fluoropyrimidine and cisplatin.
Dose Modifications for HematologicToxicity Due to FP Chemotherapy
ANC(x 109/L)
Platelets(x 109/L) Fluoropyrimidine/Cisplatin
≥ 1.5 and ≥ 75 100% of original doses, without delay
≥ 1.0 – < 1.5 and ≥ 75 75% of original doses, without delay
< 1.0 and/or ≥ 75
Delay for up to 3 weeks, then resume treatment if ANC ≥ 1.0 and platelets ≥ 75. If
ANC is ≥ 1.0 – < 1.5, administer 75% of original doses. If ANC is ≥ 1.5, administer
100% of original doses.If ANC < 1.0 or platelet count is < 75,
permanently discontinue fluoropyrimidine and cisplatin for unacceptable toxicity.
Table 2 in protocol
51
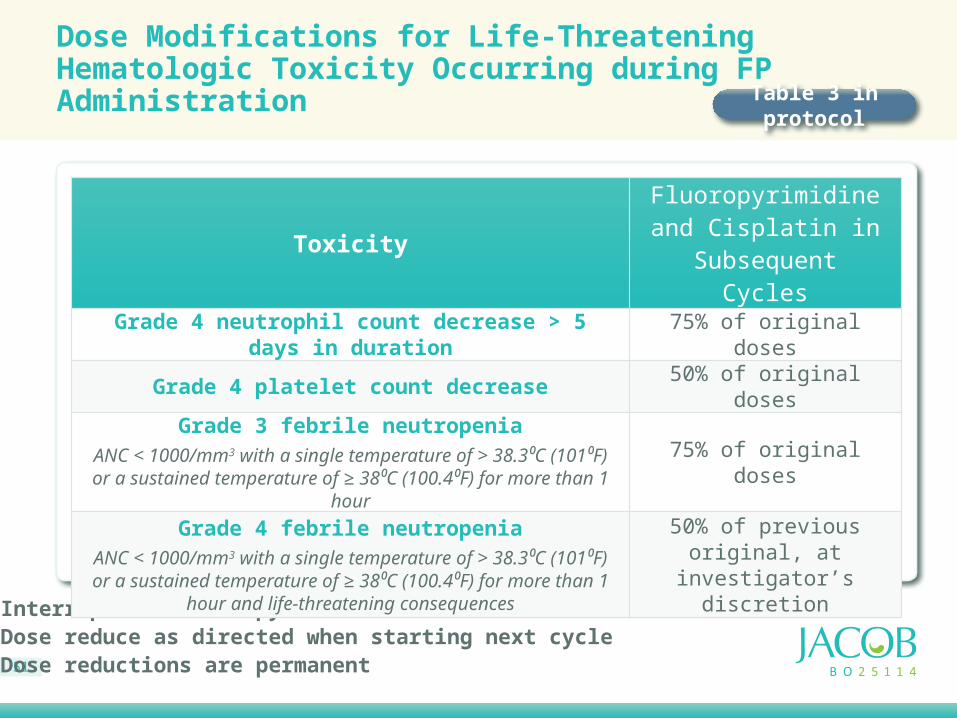
Interrupt chemotherapy Dose reduce as directed when starting next cycleDose reductions are permanent
Dose Modifications for Life-Threatening Hematologic Toxicity Occurring during FP Administration
ToxicityFluoropyrimidineand Cisplatin in
Subsequent Cycles
Grade 4 neutrophil count decrease > 5 days in duration 75% of original doses
Grade 4 platelet count decrease 50% of original doses
Grade 3 febrile neutropeniaANC < 1000/mm3 with a single temperature of > 38.3⁰C (101⁰F) or a
sustained temperature of ≥ 38⁰C (100.4⁰F) for more than 1 hour75% of original doses
Grade 4 febrile neutropeniaANC < 1000/mm3 with a single temperature of > 38.3⁰C (101⁰F) or a sustained temperature of ≥ 38⁰C (100.4⁰F) for more than 1 hour and
life-threatening consequences
50% of previous original, at investigator’s discretion
Table 3 in protocol

52
Cardiac Safety Monitoring
HER2 directed therapy has been implicated in cardiac toxicity• Pertuzumab and trastuzumab cardiac safety must be monitored
• Currently, there is no evidence for increased cardiac toxicity with pertuzumab-containing combination regimens
Regularly scheduled ECG and LVEF assessments are mandatory• Every 9 weeks while on chemotherapy treatment
• Every 12 weeks while on antibody alone treatment
• Every 6 months for 1 year after stopping study drug
• Then annually during survival follow up for up to 5 years

53
Algorithm for Asymptomaticdecline in LVEF
LVEF drop from baseline
LVEF ≥ 50% LVEF < 50%
LVEF drop≤ 20%
LVEF drop> 20%
LVEF drop< 10%
LVEF drop≥ 10%
CONTINUETreatment
CONTINUE Treatment and repeat LVEF in 3 weeks
HOLD Treatment and repeat LVEF in 3 weeks
Not Confirmed(LVEF drop < 10pts or
LVEF ≥ 50%)
LVEF drop CONFIRMED(LVEF drop ≥ 10pts and
LVEF < 50%)
RESUME Treatment STOP Treatment
Figure 3 of Protocol

54
Pertuzumab/Trastuzumab Cardiac Toxicity: Reporting AE/SAE
Observation How to Report Term to be Reported Grading
Asymptomatic decline in LVEF < 10% points from baseline or to an LVEF ≥ 50%
No additional reporting required, LVEF results to
be reported on eCRFN/A N/A
Asymptomatic decline in LVEF ≥ 10% points from baseline to an LVEF < 50% AE (eCRF)
“Ejection fraction
decreased”
NCI CTCAE for “ejection fraction
decreased”
Asymptomatic decline in LVEF requiring treatment or leading to discontinuation of pertuzumab/placebo and trastuzumab
AE (eCRF)“Ejection fraction
decreased”
NCI CTCAE for “ejection fraction
decreased”
Congestive heart failure (symptomatic LVSD) SAE (eCRF) “Congestive
heart failure”NCI CTCAE for “heart failure”
and NYHA Class
AE = adverse events; CTCAE = Common Terminology Criteria for Adverse Events; eCRF = electronic Case Report Form; LVEF = left ventricular ejection fraction; LVSD – left ventricular systolic dysfunction; N/A = not applicable; NCI = National Cancer Institute; NYHA = New York Heart Association; SAE = serious adverse event.Notes: Any symptomatic LVSD event must be reported as “congestive heart failure”.
Table 7 in protocol

55
LVSD Dysfunction eCRF
If a patient has a decrease in LVEF by ≥10 percentage points from baseline to an absolute value below 50% recorded in the LVEF assessment CRF, the Principal Investigator will then complete the following CRF:
Does the subject have difficulty breathing?
If yes, select all that apply:
While climbing less than 8 stair steps
While getting dressed
At rest
While lying flat
Other
Does the subject have any clinical signs that may be due to heart failure?
If yes, select all that apply:
Bilateral ankle edema
Pulmonary rales
Weight gain
Jugular venous distention
Other
58
Tumor Assessments
Measurable or non-measurable evaluable tumor (RECIST 1.1)
Baseline assessment at screening, then after every 9 weeks until progressive disease (PD) is documented
Measurable disease should be imaged using CT or MRI – use the same method throughout the study for a given patient
Report measurements of target and non-target lesions for measurable disease (per RECIST)
Report objective response (CR/PR, SD, PD) for both measurable and non-measurable evaluable disease• If PD occurs off cycle, an unscheduled Tumor Assessment
should be performed

61
Schedule for PharmacokineticSampling for Pertuzumab and Trastuzumab
Appendix 2 in protocol
Cycle 1
Cycle2
Cycle3
Cycle4
Cycle6
Cycle8 a
Post-treatment
Monitoring Visit 1 b
(28 days post
last dose)
Post-treatment
Monitoring Visit 2 c
(60-90 days post last dose)
Predose d ● ● ● ● ● ● ● ●
Postdose e ● ● ● ●
a Sample collected when on biologic therapy alone and last chemotherapy was ≥6 weeks ago. This timepoint may not coincide with Cycle 8 for all patients
b Sample collected 28 days after last administration of study
c Sample collected 60-90 days after last administration of study treatment
d Sample can be collected up to 6 hours prior to administration of the specified drug
e Sample can be collected up to 30 minutes after end of drug infusion of specified drug

62
Table 1-2 Follow-up Assessments until Death
Post-treatment Phase Monitoring d SurvivalFollow-up
TimepointPost-treatment Monitoring
Visit 2 60-90 days after
last study treatment
24 wk (±2 wk)
Every 12 weeks a (±2 wk)
ATA ●
PK sampling ●
Cardiac monitoring: LVEF b (MUGA/ECHO/MRI),ECG including cardiac
medication (start and end dates, changes in dosing)
●
Drug-related SAEs c ● ● ●
Survival assessment d ● ● ●
Post-treatment phase anticancer therapy
Information about any subsequent (post-study treatment) anticancer
therapy will be collected, including the names of all components of treatments
and start and end dates of dosing
●

63
Recruitment Challenge: High Screen Failure Rate
It is assumed that screening ineligibility rate may be ~85%
Primarily driven by requirement for HER2 positivity • ~ 22% of patients with advanced gastric cancer are HER2+
But… it’s not impossible: ToGA trial recruited successfully with a ~80% screen failure rate
Improve overall screening rates by implementing process of pre-identifying and pre-screening patients • This will help reduce screening failure rate not related to HER2
positivity• If local pre-screening HER2 result is borderline or equivocal, please still
send for central HER2 testing
Reviewing pre-screening information will help identify why potentially eligible patients are not considered for screening

64
Synergy with MetGastric study
JACOB study accepts HER2 test result from Targos and vice versa
In those MetGastric and JACOB overlapping sites (25%), screen for MetGastric study first
Where patient screened in MetGastric study has HER2 positive status:• Obtain Informed Consent for JACOB• Investigator/study nurse registers MetGastric study patient screen
number in the JACOB’s IXRS screening module• Send results transfer form with detailed patient information to Targos
→ Tissue sample will be transferred within Targos
If site is not a JACOB/MetGastric overlapping site, a referral network is recommended

65
Role and responsibility of CRC (Cardiac Review Committee)
CRC Patients with potential cardiac events (e.g. symptomatic LVSD) per investigator assessment will be reviewed by independent external Cardiac Review Committee (CRC)• CRC provides independent blinded central determination of symptomatic
declines in LVEF and definite and probable cardiac deaths for reporting to IDMC
CRCC (Duke Clinical Research Institution) is the vendor who will: Raise queries using RAVE (10 day turnaround)Request/collect source documents via emailEnsure relevant variables are cleanPrepare event packetsRecord CRC adjudicationsCoordinate CRC adjudication meetings
66
Potential source documents to be collected
Physician progress or consultation notes
Discharge summary
ECG tracing and report
ECHO/MUGA/cardiac MRI report
Chest X-ray report
Any other documents that CRCC deems necessary for case adjudication, e.g. cardiac catheterization report
• CRCC will be responsible for document translationif in language other than English

Q&A