
Single Versus Double-Incision IN THIS ISSUE:...
12
1 Brought to you through a sponsorship from: IN THIS ISSUE: Single Versus Double-Incision Technique for the Repair of Acute Distal Biceps Tendon Ruptures: No Major Differences in a Randomized Clinical Trial 1 Sugar Isn’t Always So Sweet 2 A Lateral Pinning Pattern Is Preferred for Supracondylar Distal Humeral Fractures in Children 2 The Tip Apex Distance “Myth”: Not Busted 10 Is a Stiff Symphyseal Implant a Good Idea? 11 Missed Injuries in Trauma Patients 12 EDITOR Marc Swiontkowski, MD, Editor Professor Department of Surgery University of Minnesota From the publisher of The Journal of Bone & Joint Surgery © 2012 Should We Treat Acute Osteoporotic Fractures with Bisphosphonates? 3 To Remove or Not to Remove: That Is the Hardware Question 4 Gritti-Stokes Amputation Increased Rate of Walking without Assistive Devices When Compared with Transfemoral Amputation in Trauma Patients 9 Lack of Support for the Importance of Debridement Within Six Hours of Open Fractures in Meta-Analysis 10 SUMMARY OF: Grewal R, Athwal GS, Macdermid JC, Faber KJ, Drosdowech DS, El- Hawary R, King GJ. Single Versus Double-Incision Technique for the Repair of Acute Distal Biceps Tendon Ruptures: A Randomized Clinical Trial. J Bone Joint Surg Am. 2012 Jul 3;94(13):1166-74. Christian Krettek, FRACS, FRCSEd Medizinische Hochschule Hannover SUMMARY The authors of this clinical trial evaluated outcomes of the single versus double-incision techniques for acute distal biceps tendon repair. Patients who had an acute distal biceps rupture were randomly assigned to one of two groups: single-incision repair with two suture anchors (forty-seven) or double-incision repair with transosseous drill holes (forty-four). Follow-up evaluations were performed at three, six, twelve, and twenty- four months after the operation. The primary outcome was the American Shoulder and Elbow Surgeons (ASES) elbow score, whereas secondary outcomes were muscle strength; complication rates; and Disabilities of the Arm, Shoulder and Hand (DASH) and Patient-Rated Elbow Evaluation (PREE) scores. The groups did not differ signifi- cantly with regard to mean age, percentages of dominant arms affected, or Workers’ Compensation cases. The two groups did not differ with respect to their final outcomes at two years—i.e., ASES pain score (p = 0.4), ASES function score (p = 0.10), DASH score (p = 0.3), or PREE score (p = 0.4) (Table I and Fig. 1)—or with regard to isometric extension, pronation, or supination strength at more than one year. The patients in the double-incision group had only a 10% advantage in final isometric flexion strength (104% versus 94% in the single-incision group; p = 0.01). The rate of strength recovery did not differ between the groups. The patients treated with the single-incision technique had more early transient neurapraxias of the lateral antebrachial cutaneous nerve (nineteen of forty-seven versus three of forty-three in the double-incision group; p < 0.001). The authors reported four reruptures; all were related to patient noncompliance or reinjury during the early postoperative period and did not appear to be related to the fixation technique (p = 0.3). DISCUSSION This is an important study for several reasons. First, it is the first prospective randomized clinical trial that compared the outcomes of single and double-incision techniques for the repair of distal biceps tendon ruptures. It was carefully planned and well-performed. Single Versus Double-Incision Technique for the Repair of Acute Distal Biceps Tendon Ruptures: No Major Differences in a Randomized Clinical Trial doi:10.2106/JBJS.OT.L.00309
Transcript of Single Versus Double-Incision IN THIS ISSUE:...

1
Brought to you through a sponsorship from:
IN THIS ISSUE:
Single Versus Double-Incision Technique for the Repair of Acute Distal Biceps Tendon Ruptures: No Major Differences in a Randomized Clinical Trial 1
Sugar Isn’t Always So Sweet 2
A Lateral Pinning Pattern Is Preferred for Supracondylar Distal Humeral Fractures in Children 2
The Tip Apex Distance “Myth”: Not Busted 10Is a Stiff Symphyseal Implant a Good Idea? 11Missed Injuries in Trauma Patients 12
EDITORMarc Swiontkowski, MD, Editor Professor Department of Surgery University of Minnesota
From the publisher of The Journal of Bone & Joint Surgery © 2012
Should We Treat Acute Osteoporotic Fractures with Bisphosphonates? 3
To Remove or Not to Remove: That Is the Hardware Question 4
Gritti-Stokes Amputation Increased Rate of Walking without Assistive Devices When
Compared with Transfemoral Amputation in Trauma Patients 9
Lack of Support for the Importance of Debridement Within
Six Hours of Open Fractures in Meta-Analysis 10
SUMMARY OF: Grewal R, Athwal GS, Macdermid JC, Faber KJ, Drosdowech DS, El-Hawary R, King GJ. Single Versus Double-Incision Technique for the Repair of Acute Distal Biceps Tendon Ruptures: A Randomized Clinical Trial.
J Bone Joint Surg Am. 2012 Jul 3;94(13):1166-74.
Christian Krettek, FRACS, FRCSEd Medizinische Hochschule Hannover
SUMMARYThe authors of this clinical trial evaluated outcomes of the single versus double-incision techniques for acute distal biceps tendon repair. Patients who had an acute distal biceps rupture were randomly assigned to one of two groups: single-incision repair with two suture anchors (forty-seven) or double-incision repair with transosseous drill holes (forty-four). Follow-up evaluations were performed at three, six, twelve, and twenty-four months after the operation. The primary outcome was the American Shoulder and Elbow Surgeons (ASES) elbow score, whereas secondary outcomes were muscle strength; complication rates; and Disabilities of the Arm, Shoulder and Hand (DASH) and Patient-Rated Elbow Evaluation (PREE) scores. The groups did not differ signifi-cantly with regard to mean age, percentages of dominant arms affected, or Workers’ Compensation cases.
The two groups did not differ with respect to their final outcomes at two years—i.e., ASES pain score (p = 0.4), ASES function score (p = 0.10), DASH score (p = 0.3), or PREE score (p = 0.4) (Table I and Fig. 1)—or with regard to isometric extension, pronation, or supination strength at more than one year. The patients in the double-incision group had only a 10% advantage in final isometric flexion strength (104% versus 94% in the single-incision group; p = 0.01). The rate of strength recovery did not differ between the groups. The patients treated with the single-incision technique had more early transient neurapraxias of the lateral antebrachial cutaneous nerve (nineteen of forty-seven versus three of forty-three in the double-incision group; p < 0.001). The authors reported four reruptures; all were related to patient noncompliance or reinjury during the early postoperative period and did not appear to be related to the fixation technique (p = 0.3).
DISCUSSIONThis is an important study for several reasons. First, it is the first prospective randomized clinical trial that compared the outcomes of single and double-incision techniques for the repair of distal biceps tendon ruptures. It was carefully planned and well-performed.
Single Versus Double-Incision Technique for the Repair of Acute Distal Biceps Tendon Ruptures: No Major Differences in a Randomized Clinical Trialdoi:10.2106/JBJS.OT.L.00309

2
SUMMARY OF: Richards JE, Kauffmann RM, Zuckerman SL, Obremskey WT, May AK. Relationship of Hyperglycemia and Surgical-Site Infection in Orthopaedic Surgery.
J Bone Joint Surg Am. 2012 Jul 3;94(13):1181-6.
Sugar Isn’t Always So Sweetdoi:10.2106/JBJS.OT.L.00310
William T. Obremskey, MD, MPH Vanderbilt University Medical Center
SUMMARYThe investigators studied the effect of perioperative hyperglycemia and the risk of surgical site infection (SSI) less than thirty days postoperatively in trauma patients without diabetes. Seven hundred and ninety patients were identified. The hyperglycemic index was used as a marker for patients at risk. Overall, twenty-one thirty-day SSIs (2.7%) were noted. Of the patients, 37% had at least one glucose value of ≥200 mg/dL. Patients who had a hyperglycemic episode had an SSI risk of 4.4% versus a risk of 1.6% for patients who did not have more than one hyperglycemic value of ≥200 mg/dL. Multivariable logistic regression indicated that having two or more blood glucose levels of ≥200 mg/dL was a risk factor for thirty-day SSI with an odds ratio of 2.7. Patients with an open fracture had an increased risk of SSI as well, with an odds ratio of 3.3 After controlling for open fractures and in a multivariable regression model, the authors noted that having a hyperglycemic index of ³1.76 was a significant risk factor for SSI (odds ratio: 4.9).
DISCUSSIONGeneral surgeons, cardiac surgeons, and intensivists routinely monitor blood glucose levels for inpatients as the literature identifies hyperglycemia as a risk factor for infection and mortality (Ann Surg. 2007 Oct;246[4]:605-10; discussion 610-2, Crit Care Clin. 2001 Jan;17[1]:107-24, Am Surg. 2005 Feb;71[2]:171-4, and J Trauma. 2005 Jul;59[1]:80-3). Orthopaedic surgery is a specialty with populations at high risk for deep infection. Our patients frequently have implants, traumatized tissue, and long procedures associated with medical comorbidities. This study demonstrated increased SSI risk in adult trauma patients with perioperative hyperglycemia. Additional work should determine if the link is due to causation or if it is associated in patients who respond poorly to the stress of surgery or trauma, which increases the level of hyperglycemia. We also need to determine if improved glycemic control leads to decreased infection risk.
T.A. DeCoster, MD, and U. Modhia, MD University of New Mexico
SUMMARYThis article is a meta-analysis of the world literature on the controversial topic of lateral pinning versus cross pinning for dis-placed supracondylar humeral fractures in children. Only eighteen of more than 1800 studies met the authors’ inclusion stan-dards. They compared outcomes and complications among more than 1600 patients from the literature. The results showed that,
A Lateral Pinning Pattern Is Preferred for Supracondylar Distal Humeral Fractures in Childrendoi:10.2106/JBJS.OT.L.00304
SUMMARY OF: Woratanarat P, Angsanuntsukh C, Rattanasiri S, Attia J, Woratanarat T, Thakkinstian A. Meta-analysis of Pinning in Supracondylar Fracture of the Humerus in Children.
J Orthop Trauma. 2012 Jan;26(1):48-53.
Second, since both groups achieved favorable outcomes and reported minimal pain and disability, surgeons can select the op-erative approach that is most suited to their personal experience.
The third interesting piece information is the observation of a very low rate of heterotopic ossification, which was very mild, in each group of only 2%. This is unlike other series, in which the prevalence of heterotopic ossification has been reported to be between 5% and 10% (J Shoulder Elbow Surg. 2008 Jan-Feb;17[1 Suppl]:67S-71S, J Hand Surg Am. 2003 May;28[3]:496-502, and J Bone Joint Surg Am. 2000 Nov;82-A[11]:1575-81).
But for me, the most important message is that the use of more material and expensive implants does not necessarily mean that the outcome will be better. In this context, a comparative analysis of the operation time and total costs would have been interest-ing and valuable additional information.

3
Kyle J. Jeray, MD Greenville Hospital System University Medical Center
SUMMARYBisphosphonates prevent bone resorption with a resulting increase in bone mineral density by inhibiting osteoclastic activity; however, the effect of bisphosphonates on fracture healing is still unclear. The authors performed a prospective multicenter study looking at the use of bisphosphonates (risedronate, 35 mg weekly) in patients who had intertrochanteric hip fractures and a diagnosis of osteoporosis, but who had not been on any bisphosphonates prior to the fracture. There were three groups of thirty patients: group A started on bisphosphonates one week after surgery; group B started on bisphosphonates one month after surgery; and group C started on bisphosphonates three months after surgery. The healing times (10.7, 12.9, and 12.3 weeks in groups A, B, and C, respectively) did not differ among the three groups. The incidence of fracture complications did not differ among the groups. The authors also considered the functional outcomes at one year, and found no difference among the groups. They concluded that risedronate did not affect healing of intertrochanteric hip fractures in patients with osteoporosis.
DISCUSSIONAs the rate of fragility fractures continues to rise and the number of patients being treated with bisphosphonates rises as well, the question of whether or not we should treat acute osteoporotic fractures with bisphosphonates is of increasing importance. The obvious concern is that, by suppressing the ability of bone to remodel when treated with a bisphosphonate, healing may be adversely affected. However, several animal studies have conflicting evidence. Some studies involving bisphosphonates demonstrated delays in fracture healing1-3, while others showed no effect4,5, and others even suggested enhanced fracture healing6,7. Authors of some small clinical studies have reported no adverse effects of bisphosphonates on healing8,9. Kim et al. examined the use of bisphosphonate treatment on osteoporotic fractures in a small, well-defined population. Although their numbers were small, they did perform a power analysis prior to the start of the study based on their primary end point of radiographic healing time. Based on their reported data, it appears that the clinical use of risedronate may not make a differ-ence in the time to fracture healing if risedronate is started within a week after the fracture, as compared with starting the drug after the fracture has healed. However, we need to be cautious, as this is only one small study, and it involved a single drug in the bisphosphonate class. The authors did not evaluate individuals who were already on the drug prior to fracture, which is often the case.
Ultimately, the goal of bisphosphonate treatment is to prevent secondary fractures and reduce mortality after the fragility frac-ture. The authors of this paper did not report if any additional fragility fractures occurred in the study patients, or whether there was a difference based on the time to starting the bisphosphonate. Assuming no additional fragility fractures or such time-based differences occurred, we then need to ask ourselves: what is the value of treating patients with bisphosphonates early on versus waiting three months if there is no difference in preventing additional fragility fractures?
SUMMARY OF: Kim TY, Ha YC, Kang BJ, Lee YK, Koo KH. Does Early Administration of Bisphosphonate Affect Fracture Healing in Patients with Intertrochanteric Fractures?
J Bone Joint Surg Br. 2012 Jul;94(7):956-60.
Should We Treat Acute Osteoporotic Fractures with Bisphosphonates?doi:10.2106/JBJS.OT.L.00361
with cross pinning, two extra cases of loss of fixation were prevented but five additional ulnar nerve injuries were caused per 100 patients treated. The authors, therefore, favored lateral pinning.
DISCUSSIONSupracondylar distal humeral fractures in children are common worldwide. They are classified as 13M according to the AO/OTA pediatric fracture classification. The optimal pin pattern has been controversial, with medial and lateral pins (cross pinning) and lateral pins only, being the two leading patterns. Cross pinning is thought to be mechanically superior, but it places the ulnar nerve at risk for injury. The authors confirmed these findings and quantified the comparative benefits (less loss of reduction) and complications (ulnar nerve injury). The risk of late deformity and poor function was the same for both groups. The authors also emphasized that the risk of loss of fixation with lateral pinning can be minimized with the insertion of divergent pins or three pins. When cross pinning is used, it is mechanically superior if the pins cross proximal to the fracture line and not at the fracture. Other practical factors that affect outcome, including quality of reduction, exact location of the pins within the distal and proximal fragments, and number of attempts necessary to achieve final pin position, could not be compared.

4
CONTENT IS CONTINUED ON PAGE 9
William T. Obremskey, MD, MPH Vanderbilt University Medical Center
SUMMARYWilliams et al. reported on a prospective study of sixty-nine patients who underwent elective removal of symptomatic hardware from the foot and ankle. The Short-Form McGill Pain Questionnaire was used to assess pain preoperatively and six weeks post-operatively1. The patients were also asked if they would undergo the procedure again and if they were satisfied with the results. Pain, as measured on the visual analog scale (VAS), decreased from 3.06 to 0.88. Sixty-five percent of patients had no pain at six weeks postoperatively. Ninety-one percent of patients stated that they would undergo the procedure again and were satisfied with the result.
DISCUSSIONAs health care in the United States moves towards accountable care organizations and increased scrutiny, hardware removal may be a procedure that is difficult to justify without adequate data to support patient quality-of-life and functional improvement. Hardware removal may be one of those procedures that insurance companies say is not medically necessary and is not covered under a health-care plan2. The indications and outcomes for hardware removal have not been well-documented3-8. In general, orthopaedic surgeons are well-positioned to prove and demonstrate the effectiveness (clinical and functional outcomes) of pro-cedures that we perform. Data from this article are more pieces of information that will help physicians (as opposed to adminis-trators or politicians) continue to drive medical decision-making. The authors should be commended for providing good data on a common clinical issue, as hardware removal is one of the most common procedures reported by orthopaedic surgeons who sit for Part II of their American Board of Orthopaedic Surgery (ABOS) certification.
REFERENCES1. Melzack R. The short-form McGill Pain Questionnaire. Pain. 1987 Aug;30(2):191-7.2. Böstman O, Pihlajamäki H. Routine implant removal after fracture surgery: a potentially reducible consumer of hospital resources in trauma units. J Trauma. 1996 Nov;41(5):846-9.3. Hanson B, van der Werken C, Stengel D. Surgeons’ beliefs and perceptions about removal of orthopaedic implants. BMC Musculoskelet Disord. 2008 May 24;9:73. 4. Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma. 2001 May;15(4):271-4.5. Jacobsen S, Honnens de Lichtenberg M, Jensen CM, Tørholm C. Removal of internal fixation—the effect on patients’ complaints: a study of 66 cases of removal of internal fixation after malleolar fractures. Foot Ankle Int. 1994 Apr;15(4):170-1.6. Busam ML, Esther RJ, Obremskey WT. Hardware removal: indications and expectations. J Am Acad Orthop Surg. 2006 Feb;14(2):113-20.7. Sanderson PL, Ryan W, Turner PG. Complications of metalwork removal. Injury. 1992;23(1):29-30.8. Richards RH, Palmer JD, Clarke NM. Observations on removal of metal implants. Injury. 1992;23(1):25-8.
SUMMARY OF: Williams AA, Witten DM, Duester R, Chou LB. The Benefits of Implant Removal from the Foot and Ankle.
J Bone Joint Surg Am. 2012 Jul 18;94(14):1316-20.
To Remove or Not to Remove: That Is the Hardware Questiondoi:10.2106/JBJS.OT.L.00313
REFERENCES1. Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005 Mar;90(3):1294-301. Epub 2004 Dec 14.2. Li J, Mori S, Kaji Y, Mashiba T, Kawanishi J, Norimatsu H. Effect of bisphosphonate (incadronate) on fracture healing of long bones in rats. J Bone Miner Res. 1999 Jun;14(6):969-79.3. Li C, Mori S, Li J, Kaji Y, Akiyama T, Kawanishi J, Norimatsu H. Long-term effect of incadronate disodium (YM-175) on fracture healing of femoral shaft in growing rats. J Bone Miner Res. 2001 Mar;16(3):429-36.4. Bauss F, Schenk RK, Hört S, Müller-Beckmann B, Sponer G. New model for simulation of fracture repair in full-grown beagle dogs: model characterization and results from a long-term study with ibandronate. J Pharmacol Toxicol Methods. 2004 Jul-Aug;50(1):25-34.5. Munns CF, Rauch F, Zeitlin L, Fassier F, Glorieux FH. Delayed osteotomy but not fracture healing in pediatric osteogenesis imperfecta patients receiving pamidronate. J Bone Miner Res. 2004 Nov;19(11):1779-86. Epub 2004 Aug 23.6. Amanat N, Brown R, Bilston LE, Little DG. A single systemic dose of pamidronate improves bone mineral content and accelerates restoration of strength in a rat model of fracture repair. J Orthop Res. 2005 Sep;23(5):1029-34. Epub 2005 Apr 19.7. Goodship AE, Walker PC, McNally D, Chambers T, Green JR. Use of bisphosphonate (pamidronate) to modulate fracture repair in ovine bone. Ann Oncol.1994;5 Suppl 7:S53-5. 8. Adolphson P, Abbaszadegan H, Bodén H, Salemyr M, Henriques T. Clodronate increases mineralization of callus after Colles’ fracture: a randomized, double-blind, placebo-controlled, prospective trial in 32 patients. Acta Orthop Scand. 2000 Apr;71(2):195-200.9. Rozental TD, Vazquez MA, Chacko AT, Ayogu N, Bouxsein ML. Comparison of radiographic fracture healing in the distal radius for patients on and off bisphosphonate therapy. J Hand Surg Am. 2009 Apr;34(4):595-602.
A D V E R T I S E M E N T
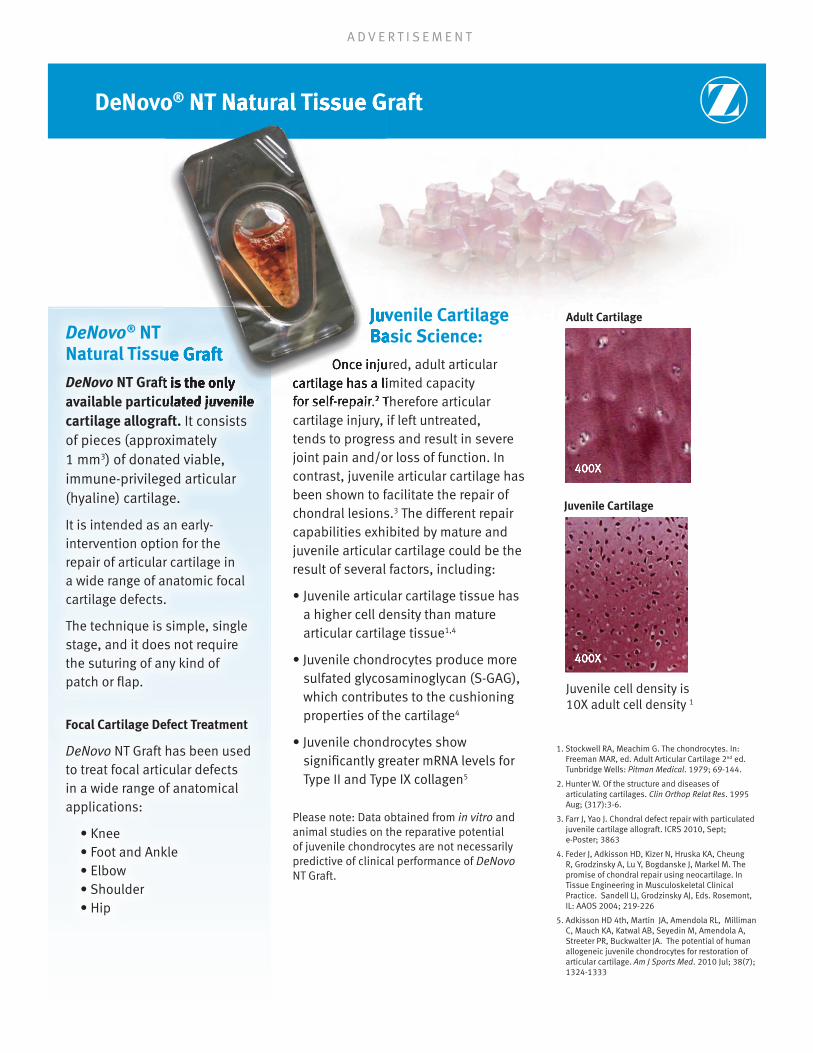
DeNovo® NT Natural Tissue Graft
Juvenile Cartilage
Adult Cartilage
Juvenile cell density is 10X adult cell density 1
Juvenile Cartilage Basic Science:
Once injured, adult articular cartilage has a limited capacity for self-repair.2 Therefore articular cartilage injury, if left untreated, tends to progress and result in severe joint pain and/or loss of function. In contrast, juvenile articular cartilage has been shown to facilitate the repair of chondral lesions.3 The different repair capabilities exhibited by mature and juvenile articular cartilage could be the result of several factors, including:
•Juvenilearticularcartilagetissuehasa higher cell density than mature articular cartilage tissue1,4
•Juvenilechondrocytesproducemoresulfated glycosaminoglycan (S-GAG), which contributes to the cushioning properties of the cartilage4
•Juvenilechondrocytesshowsignificantly greater mRNA levels for Type II and Type IX collagen5
Please note: Data obtained from in vitro and animal studies on the reparative potential of juvenile chondrocytes are not necessarily predictive of clinical performance of DeNovo NT Graft.
1. Stockwell RA, Meachim G. The chondrocytes. In: Freeman MAR, ed. Adult Articular Cartilage 2nd ed. Tunbridge Wells: Pitman Medical. 1979; 69-144.
2. Hunter W. Of the structure and diseases of articulating cartilages. Clin Orthop Relat Res. 1995 Aug; (317):3-6.
3. Farr J, Yao J. Chondral defect repair with particulated juvenile cartilage allograft. ICRS 2010, Sept; e-Poster; 3863
4. Feder J, Adkisson HD, Kizer N, Hruska KA, Cheung R, Grodzinsky A, Lu Y, Bogdanske J, Markel M. The promise of chondral repair using neocartilage. In Tissue Engineering in Musculoskeletal Clinical Practice. Sandell LJ, Grodzinsky AJ, Eds. Rosemont, IL: AAOS 2004; 219-226
5. Adkisson HD 4th, Martin JA, Amendola RL, Milliman C, Mauch KA, Katwal AB, Seyedin M, Amendola A, Streeter PR, Buckwalter JA. The potential of human allogeneic juvenile chondrocytes for restoration of articular cartilage. Am J Sports Med. 2010 Jul; 38(7); 1324-1333
400X400X400X
400X400X400X
DeNovo® NT Natural Tissue Graft
DeNovo NT Graft is the only available particulated juvenile cartilage allograft. It consists of pieces (approximately 1 mm3) of donated viable, immune-privileged articular (hyaline) cartilage.
It is intended as an early-intervention option for the repair of articular cartilage in a wide range of anatomic focal cartilage defects.
The technique is simple, single stage, and it does not require the suturing of any kind of patch or flap.
Focal Cartilage Defect Treatment
DeNovo NT Graft has been used to treat focal articular defects in a wide range of anatomical applications:
•Knee •FootandAnkle •Elbow •Shoulder •Hip
DeNovo® NT Natural Tissue Graft
Juvenile Cartilage Basic Science:
Once injured, adult articular cartilage has a limited capacity cartilage has a limited capacity for self-repair.2 Therefore articular
Natural Tissue Graft
NT Graft is the only available particulated juvenile

A D V E R T I S E M E N T
• Mini-open surgical technique available for the knee• Arthroscopically assisted surgical technique
available for the ankle
Click Here for Surgical Technique Videos!
Compare/Contrast with Contemporary Treatment Options
Additional Publications Bonner patellar case report published, J Knee Surg, Oct 2010. Case report on patient #1, with follow-up MRI at 21 months, demonstrating filled defect, resolution of subchondral edema, and patient’s return to full function.
Farr poster publication (study pts), Barcelona ICRS 2010. Dr. Farr’s subset of the ongoing 25-patient, multi-center prospective study, with the first 9 patients reaching up to 18 months post-op and demonstrating significant improvements in clinical outcomes over the pre-op baseline data.MRI data indicate good defect filling, and no revisions performed to date.
Hatic and Berlet review, Foot & Ankle Spec, Dec 2010. Discussion of DeNovo NT use and technique in osteochondral lesions of the talus.
Ng podiatric arthroscopy technique poster, ACFAS 2011. Case review of an osteochondral defect of the talus treated with DeNovo NT using an arthroscopically-assisted surgical technique.Patient returned to full unrestricted activity at 6 months post-op and was 16 months post-op at the time of the poster publication and remained very satisfied with the surgery.
Mariash podiatric case review poster, ACFAS 2011. Case review of an osteochondral defect of the talus treated with DeNovo NT using an open technique. 15-month MRI images suggested positive filling of the defect and no instability of the graft.
Farr Chondral Defect Repair of the Knee, Cartilage, July 2011. Case review of 4 patients with chondral lesions on the femoral condyle and/or trochlea treated with DeNovo NT. Patients are a subset of ongoing 25-patient, multi-center prospective study. Evaluation at 24 months post-op showed improved clinical outcomes and MRI data suggests good and persistent defect filling.
Farr poster publication (study pts), Montreal ICRS 2012.12-month MRI images for 24 of the 25 patients enrolled in prospective, single-arm study. The majority of repair tissue was shown to be well-integrated and percent fill with repair tissue was also good with 89% of lesions demonstrating >75% fill. MRI results are consistent with improved clinical outcomes as compared to baseline.
Adams Treatment of OC lesions in the talus, Tech Foot Ankle Surg, June 2011. Article provides a brief review of surgical treatment options for symptomatic lesions and the particulated juvenile cartilage allograft transplantation technique for OC lesions of the talus.
6. Knutsen G, Drogset JO, Engebretsen L, Grontvedt T, Isaksen V, Ludvigsen TC, Roberts S, Solheim E, Strand T, Johanson O. et al. A randomized trial comparing autologous chondrocyte implantation with microfracture. Findings at five years. J Bone Joint Surg Am. 2007 Oct; 89(10):2105-12. 7. Asik M, Citfci F, Sen C, Erdil M, Atalar A. The microfracture technique for the treatment of full-thickness articular cartilage lesions of the knee: Midterm results. Arthroscopy. 2008 Nov; 24(11):1214-20.
Email questions to [email protected]
© 2012 Zimmer, Inc. All rights reserved
DeNovo® NT Graft Single Stage Procedure
Cartilage Defect Treatment Options Surgery Typical Lesion Size Tissue Characteristics
DeNovo NT GraftSingle Stage
Under 5cm2 and up to 10cm2
Juvenile hyaline cartilage implanted
ACITwoStage
5-10 cm2
Adult chondrocytes implanted; Equivalent clinical outcome to microfracture6
Osteochondral Autograft
Single Stage
1-3 cm2 Patient’s own tissue; Donor site morbidity
MicrofractureSingle Stage
1-3 cm2 No tissue implanted; Fibrous repair tissue7
DebridementSingle Stage
Variable No tissue Implanted
Osteochondral Allograft
Single Stage
5-10 cm2 Donated tissue - not juvenile; Limited supply
• Simple fixation with fibrin adhesive• No need to harvest and sew a periosteal flap• No donor site morbidity
to see how you compare to other subscribers on the treatment of cartilage lesions.

A D V E R T I S E M E N T
Check out our 3D Surgery
Highlight Programs: Cover the design rationale and science around the product as well as a top-level overview of the surgical technique.
Interactive Techniques: Combining robust interactivity, 3D animation, video, and audio to create an in-depth look at the safe and effective use of Zimmer products.
Conceptual Orthopaedic Programs: Grounded in sound instructional principles, combined with highly interactive exercises.
Surgical Videos (also in 3D): The Zimmer Institute’s surgical video library provides videos of actual surgeries performed by our faculty. Recorded from an educational perspective, and segmented by the surgical steps for easier viewing.
Access an online library of self- paced courses and videos on your laptop or mobile device.
The E-Learning experience complements the institute’s extensive hands on professional education programs that are dedicated to keep you up-to-date on the latest products and surgical techniques.
Log on to learn more, view surgeon-to-surgeon training opportunities and register online for all Zimmer Institute courses and events.
Click here to visit zio.zimmer.com
UPCOMING COURSES:
November 17, 2012
Cadaveric Resident Shoulder CourseDallas, Texas
Contact your local sales representative to register
The Zimmer Institute’s medical education curriculum is now available at a time and place that works for you!
A D V E R T I S E M E N T
Our curriculum supplements residency programs’ ACGME core competency curriculum by meeting select requirements from a practice management perspective.
There are 12 basic and advanced modules that cover a range of topics, which are critical to residents and fellows business of medicine training. Examples of course objectives include:
– Explore Practice Options
– Analyze an Employment Contract
– Recognize Red Flags During Negotiations
– Understand and Define Recommended Insurance
– Decipher Reimbursement and Financial Reports
BeyondTheExamRoom.com is offered at no cost due to grants provided by our inaugural sponsor, Zimmer, Inc. Beyond the Exam Room sponsors do not contribute to or influence content.
BeyondTheExamRoom.com
An online, e-Learning course that aims to provide a foundation for physicians
Residents and fellows are able to use the modules at any time, at no cost. This is achieved through scholarships provided by our partners and sponsors. Program Administrators are also given a user ID in order to track and evaluate resident and fellow participation. Reports on module completion and passage rate are available for review.
To register your residency program, please contact: Ebony Halliburton, Beyond The Exam Room Residency Coordinator
Career and Professional Development Business Fundamentals and Practice Management Fiscal Literacy
IF Design.Solutions.
Beyond The Exam Room Logo Concepts
Creative date
12.22.11
Final
GrayscaleBalck and White
Reverse
WatermarkGrayscale
WatermarkCMYK
Four Color Process100% Cyan
PantoneProcess Cyan
100% Black
NOTE:All Greyscales are
percentages of Black
9
Christian Krettek, FRACS, FRCSEd Medizinische Hochschule Hannover
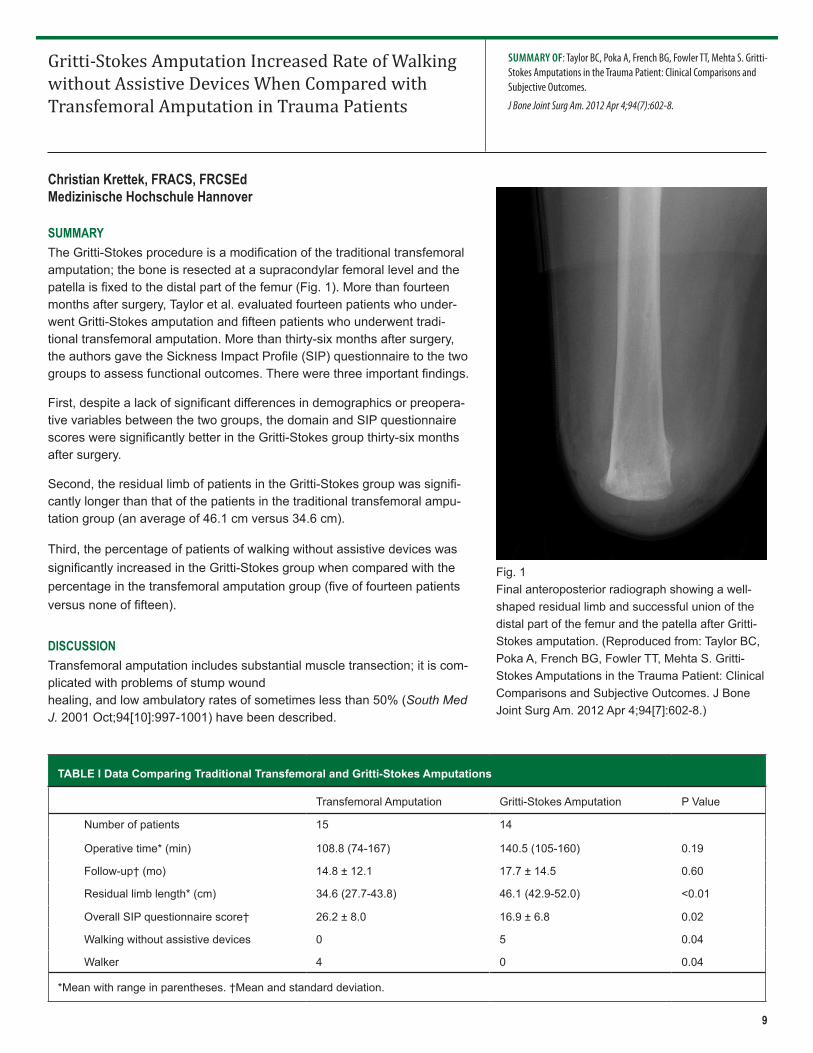
SUMMARYThe Gritti-Stokes procedure is a modification of the traditional transfemoral amputation; the bone is resected at a supracondylar femoral level and the patella is fixed to the distal part of the femur (Fig. 1). More than fourteen months after surgery, Taylor et al. evaluated fourteen patients who under-went Gritti-Stokes amputation and fifteen patients who underwent tradi-tional transfemoral amputation. More than thirty-six months after surgery, the authors gave the Sickness Impact Profile (SIP) questionnaire to the two groups to assess functional outcomes. There were three important findings.
First, despite a lack of significant differences in demographics or preopera-tive variables between the two groups, the domain and SIP questionnaire scores were significantly better in the Gritti-Stokes group thirty-six months after surgery.
Second, the residual limb of patients in the Gritti-Stokes group was signifi-cantly longer than that of the patients in the traditional transfemoral ampu-tation group (an average of 46.1 cm versus 34.6 cm).
Third, the percentage of patients of walking without assistive devices was significantly increased in the Gritti-Stokes group when compared with the percentage in the transfemoral amputation group (five of fourteen patients versus none of fifteen).
DISCUSSIONTransfemoral amputation includes substantial muscle transection; it is com-plicated with problems of stump wound healing, and low ambulatory rates of sometimes less than 50% (South Med J. 2001 Oct;94[10]:997-1001) have been described.
SUMMARY OF: Taylor BC, Poka A, French BG, Fowler TT, Mehta S. Gritti-Stokes Amputations in the Trauma Patient: Clinical Comparisons and Subjective Outcomes.
J Bone Joint Surg Am. 2012 Apr 4;94(7):602-8.
Gritti-Stokes Amputation Increased Rate of Walking without Assistive Devices When Compared with Transfemoral Amputation in Trauma Patientsdoi:10.2106/JBJS.OT.L.00330
TABLE I Data Comparing Traditional Transfemoral and Gritti-Stokes Amputations
Transfemoral Amputation Gritti-Stokes Amputation P Value
Number of patients 15 14
Operative time* (min) 108.8 (74-167) 140.5 (105-160) 0.19
Follow-up† (mo) 14.8 ± 12.1 17.7 ± 14.5 0.60
Residual limb length* (cm) 34.6 (27.7-43.8) 46.1 (42.9-52.0) <0.01
Overall SIP questionnaire score† 26.2 ± 8.0 16.9 ± 6.8 0.02
Walking without assistive devices 0 5 0.04
Walker 4 0 0.04
*Mean with range in parentheses. †Mean and standard deviation.
Fig. 1Final anteroposterior radiograph showing a well-shaped residual limb and successful union of the distal part of the femur and the patella after Gritti-Stokes amputation. (Reproduced from: Taylor BC, Poka A, French BG, Fowler TT, Mehta S. Gritti-Stokes Amputations in the Trauma Patient: Clinical Comparisons and Subjective Outcomes. J Bone Joint Surg Am. 2012 Apr 4;94[7]:602-8.)

10
Thomas A. DeCoster, MD University of New Mexico
SUMMARYThe authors of this meta-analysis of the importance of time to operative debridement of open fractures with regard to infection rate identified sixteen high-quality studies, which included more than 3500 patients, and found that debridement within six hours was no better than debridement after six hours. The authors cautioned that timely operative debridement is warranted and future studies are necessary to determine what time lag may be associated with an increased infection rate. Dr. Jason Calhoun provid-ed additional perspective in an invited commentary on this article in the online version of The Journal of Bone and Joint Surgery.
DISCUSSIONThe “within six hours” rule for operative debridement of open fractures has been an orthopaedic principle for decades and has been incorporated into trauma system standards worldwide without much scientific data to support it (J Orthop Trauma. 2008 Nov-Dec;22[10 Suppl]:S133-4). Recently, researchers have questioned this principle, and data reported from the last ten years (including data from my own institution) (Orthopedics. 2008 Dec;31[12]) have not supported it. I agree with Dr. Calhoun’s recom-mendations. Surgeons and institution personnel who closely monitor their open-fracture infection rates should investigate and report important time parameters and consider the new Orthopaedic Trauma Association (OTA) open-fracture classification as a guide (J Orthop Trauma. 2010 Aug;24[8]:457-64). Others should probably continue their current practice and monitor future literature for evidence-based guidelines on optimal timing of debridement for open fractures.
SUMMARY OF: Schenker ML, Yannascoli S, Baldwin KD, Ahn J, Mehta S. Does Timing to Operative Debridement Affect Infectious Complications in Open Long-Bone Fractures? A Systematic Review.
J Bone Joint Surg Am. 2012 Jun 20;94(12)1057-64.
Lack of Support for the Importance of Debridement Within Six Hours of Open Fractures in Meta-Analysisdoi:10.2106/JBJS.OT.L.00327
William T. Obremskey, MD, MPH Vanderbilt University Medical Center
SUMMARYDe Bruijn et al. challenged one of the well-established “myths” of orthopaedic trauma. They attempted to assess the validity of the tip apex distance (TAD) as a predictor of intertrochanteric screw cutout in stable and unstable fractures. In 1997, Baumgaert-
SUMMARY OF: De Bruijn K, den Hartog D, Tuinebreijer W, Roukema G. Reliability of Predictors for Screw Cutout in Intertrochanteric Hip Fractures.
J Bone Joint Surg Am. 2012 Jul 18;94(14):1266-72.
The Tip Apex Distance “Myth”: Not Busteddoi:10.2106/JBJS.OT.L.00312
In knee disarticulation amputation, the patella is maintained and the patellar tendon is sutured to the cruciate ligaments. The remaining large bulbous femoral condyles allow excellent weight-bearing, but without surgical modification there can be is-sues with skin breakdown and prosthetic fitting (South Med J. 2001 Oct;94[10]:997-1001). Other studies have demonstrated major reamputation rates between 9% and 17% (Prosthet Orthot Int. 1979 Apr;3[1]:15-9, J Bone Joint Surg Am. 2000 Nov;82-A[11]:1571-4, Ann R Coll Surg Engl. 1987 Jan;69[1]:1-4, and J Bone Joint Surg Am. 1988 Jun;70[5]:746-50).
The Gritti-Stokes technique does not involve major muscle transection and does not have the problems related to large bulbous femoral condyles. Despite several limitations (a small sample size and retrospective analysis), this is an important study; for the first time it showed that Gritti-Stokes amputation in a trauma population was not only safe and beneficial, but also had several important functional advantages when compared with transfemoral amputation (Table I).

11
Adam J. Starr, MD UT Southwestern Medical Center
SUMMARYIn this retrospective review, Moed and colleagues polled ten busy centers regarding failures of locked symphyseal plates and received responses from three surgeons, who reported a total of six cases. The total number of operations performed could not be reliably calculated, so the frequency of failure could not be determined. The failures followed one of two pathways. Half of the implants failed due to bone resorption at the screw-bone interface or due to gradual loosening and minor (10 to 12-mm) asymp-tomatic gapping at the symphysis. These failures were thought to be similar to the loosening sometimes seen with nonlocking plate-and-screw constructs. The other half of the implants failed in an early, abrupt fashion, with complete unilateral screw pull-out from bone, or breakage of screws at the screw-plate interface. Investigation of the three abrupt cases showed that, in one of them, malalignment of the screws with the threaded holes during screw insertion may have led to the failure.
The authors concluded that failure mechanisms of the design-specific symphyseal locked plates included failure modes seen with nonlocked and locked plates in other settings, and noted that specific indications for the use of locked plates in the pelvis remain to be determined.
DISCUSSIONThis is an interesting, albeit small, study that demonstrated failures that were anticipated by many pelvic fracture surgeons as locked symphyseal implants were released for use. As the authors correctly noted, this small series can offer only a snapshot of potential failures. The rate of failure remains unknown. It may be that the problems with locked implants occur no more frequent-ly than those encountered with traditional, nonlocked plates. Larger series are needed.
The authors should be commended for highlighting this important topic—namely, asking what is the preferred construct for stabilization of a joint, as opposed to a fracture? Locked plating systems were designed to stabilize fractures. It has long been
SUMMARY OF: Moed BR, Grimshaw CS, Segina DN. Failure of Locked Design-Specific Plate Fixation of the Pubic Symphysis: A Report of Six Cases.
J Orthop Trauma. 2012 Jul;26(7):e71-5.
Is a Stiff Symphyseal Implant a Good Idea?doi:10.2106/JBJS.OT.L.00354
ner and Solberg reported that a tip apex difference of <2.5 cm was the measurement to attain to decrease the risk of screw cutout (J Bone Joint Surg Br. 1997 Nov;79[6]:969-71). This has surprisingly been neither challenged nor verified in the orthopae-dic trauma literature. De Bruijn et al. are to be commended on their critical analysis of their own data and their fiscal analysis that confirms that the TAD is still a valid and reproducible measurement.
DISCUSSIONThe authors retrospectively reviewed the results of the treatment of intertrochanteric fractures at their institution. Intertrochanteric hip fractures were stabilized in 290 patients, and 215 patients were suitable for the study. The authors measured the TAD of the “quadrant” of the hip where the screw was placed, and noted the fracture type and quality of reduction. Two authors measured the TAD for all these fractures. The authors used cephalomedullary nails in approximately 80% of the population and sliding hip screws in 20%. Baumgaertner and Solberg included some cephalomedullary nails in their initial study, but the principle of TAD has not been verified with sliding hip screws or cephalomedullary nails since the study’s original publication.
Sixteen patients had screw cutout. The average TAD of those who had cutout versus those who did not have cut out was 25.9 ± 8.6 mm versus 21.3 ± 6.1 mm (p = 0.005). Poor fracture reduction was also associated with a significantly higher risk of screw cutout, with an odds ratio of 5.19. Placement of the screw anterior-inferiorly and central-inferiorly resulted in a significantly decreased risk of cutout according to the odds ratio. A TAD of <20 mm was also evaluated and was not found to be significantly different than measurements of <25 mm. The authors concluded that the TAD measurement was a reliable method for reducing the risk of screw cutout in this high-risk population of elderly patients.
The authors confirmed what has always made intuitive sense to orthopaedic surgeons and residents but had not been confirmed with critical analysis.

12
SUMMARY OF: Giannakopoulos GF, Saltzherr TP, Beenen LF, Reitsma JB, Bloemers FW, Goslings JC, Bakker FC; on behalf of the REACT study group. Missed Injuries During the Initial Assessment in a Cohort of 1124 Level-1 Trauma Patients.
Injury. 2012 Sep;43(9):1517-1521. Epub 2011 Aug 4.
Missed Injuries in Trauma Patients doi:10.2106/JBJS.OT.L.00306
P.V. Giannoudis, BSc, MD, FRCS School of Medicine, University of Leeds
SUMMARYGiannakopoulos et al. wished to determine the frequency, type, and implications of missed injuries in a large cohort of trauma patients. The authors also wanted to identify the factors that contributed to the injuries being missed and in which survey or period of treatment the missed injuries were diagnosed.
The study was conducted as part of a trial to assess the effects of a strategy involving early trauma resuscitating room computed tomography (CT) scanning compared with standard diagnostic imaging of adult trauma patients. Patients with missed injuries were defined as patients in whom a new injury was diagnosed after the primary and secondary surveys. To identify potentially missed injuries, a chart review was carried out of all radiological examination reports and operation records for at least three months after the trauma. To analyze factors associated with missed injuries, two patient categories were formed: patients with and those without missed injuries. All missed injuries were classified according to the Abbreviated Injury Scale (AIS) body re-gions with the use of AIS-90.
In the group of 1124 patients, 122 injuries were missed in ninety-two patients (8.2%). The missed-injury population, compared with the population without missed injuries, had significant differences with regard to Injury Severity Scores (higher), length of intensive care unit (ICU) stays (higher), traumatic brain injuries (lower Glasgow Coma Scores), and emergency interventions and receipt of blood transfusions within twenty-four hours after admission. Patients who were directly admitted to the ICU follow-ing trauma room evaluation had the highest chance for missed injuries (odds ratio 3.2; 95% confidence interval, 2.0 to 5.1; p < 0.001). The most common anatomic regions in which the missed injuries occurred were the extremities (74.6%), thorax (8.2%), and spine (6.6%). Seventy-two missed injuries (59%) remained undetected during the tertiary survey. In total, thirty-one opera-tions were required for twenty-six missed injuries.
DISCUSSIONReasons for missing injuries during the tertiary survey could have been the presence of distracting injuries, a lowered level of consciousness, and sedative or analgesic medication. The authors suggested that the creation of a tertiary survey checklist be introduced into each trauma patient’s chart to accurately register all examinations and findings.
Limitations acknowledged for this study were the retrospective review of the radiographs, the potential of having missed undiag-nosed injuries as no autopsy reports were collected, and the fact that certain soft-tissue injuries not visible on radiographs could have been missed.
Moreover, patients younger than sixteen years of age were excluded. In addition, according to the protocol utilized, the authors used a selective CT algorithm after clinical evaluation and standard conventional radiography of the chest and pelvis. The imple-mentation of a routine CT algorithm can have a substantial added value with regard to the miss rate of injuries.
The authors concluded that a high index of suspicion remains warranted, especially for polytrauma patients.
recognized that nonlocked symphyseal plates become loose over time, due to the normal motion at the symphysis. Does a locked system, with its more rigid design, offer a theoretical benefit in joint stabilization? Should we be designing implants that employ or facilitate loosening instead of rigidity? Other parts of the body (the ankle syndesmosis comes to mind) where use of rigid implants is expected to lead to failure may offer insight. Pelvic surgeons look forward to additional data from the authors on the topic of failure after symphyseal repair.


















