Single-stage tracheal resection for severe tracheal stenosis in older children
6
International Journal of Pediatric Otorhinolaryngology (2004) 68, 1—6 Single-stage tracheal resection for severe tracheal stenosis in older children Diego Preciado, Robin T. Cotton, Michael J. Rutter* Division of Pediatric Otolaryngology/Head and Neck Surgery, Cincinnati Children’s Hospital Medical Center, 3333 Burnet Avenue, Cincinnati, OH 45215, USA Received 16 July 2003; accepted 31 August 2003 KEYWORDS Tracheal resection; Tracheal stenosis; Tracheal stent Summary Objective: While tracheal resection for management of tracheal stenosis is an effective technique that has been well described in adults, the results in children have been less encouraging, as children tolerate anastomotic tension less well than adults. We describe our current technique for the management of severe tracheal stenosis in older children. Methods: Four teenagers, 16—17 years of age, presented with severe tracheal stenosis. A 16-year-old girl had sustained tracheal stenosis fol- lowing prolonged intubation, and presented with a severe Grade III stenosis having had 25 endoscopic procedures, and a failed resection at another institute. Two 17-year-old boys and a 17-year-old girl presented with Grade IV stenosis at the suprastomal area following previous intubation injuries. All four children had an identical procedure with tracheal resection over a Hood tracheal stent. Results: All four children were extubated in the operating room. Chin-to-chest sutures were removed between 7 and 10 days, as was the Hood stent. All four are currently asymptomatic with no airway stenosis. Conclusions: Although tracheal resection for tracheal stenosis in children is associated with a higher failure rate than is seen in the adult population, even severe stenosis and long segment resection may achieve excellent results. We feel that important factors influencing outcome in this series included anastomosis to an intact cricoid ring, and support of the anastomosis with a tracheal stent. © 2003 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Cricotracheal or tracheal resection is becoming the procedure of choice for the management of severe acquired tracheal and subglottic stenosis in children [1,2]. It offers the advantage of recon- structing the airway with well vascularized, rigid trachea. Despite this, the management of severe tracheal and subglottic stenosis in children con- Presented December 2002 at the Society for, Ear, Nose, and Throat Advances in Children, Atlanta, GA. ∗ Corresponding author. Tel.: +1-513-636-4356; fax: +1-513-636-2886. E-mail address: [email protected] (M.J. Rutter). tinues to be challenging. Due to a smaller airway diameter, and to worse tolerance of anastamotic tension [3,4], pediatric tracheal procedures have been generally less successful than those in adults [5]. In most cases, the severity of pre-operative subglottic or tracheal obstruction predicates mul- tiple surgical treatment stages with placement of suprastomal stents or T-tubes. Laryngotracheal stenosis in children most com- monly involves the subglottis, as it is uncommon to find pediatric patients where the stenotic seg- ment is isolated to the high trachea, sparing the cricoid cartilage. In children with purely tracheal stenosis, tracheal resection with primary anas- tomosis to an intact cricoid cartilage seems to 0165-5876/$ – see front matter © 2003 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijporl.2003.08.054
-
Upload
diego-preciado -
Category
Documents
-
view
212 -
download
0
Transcript of Single-stage tracheal resection for severe tracheal stenosis in older children

International Journal of Pediatric Otorhinolaryngology (2004) 68, 1—6
Single-stage tracheal resection for severe trachealstenosis in older children�
Diego Preciado, Robin T. Cotton, Michael J. Rutter*
Division of Pediatric Otolaryngology/Head and Neck Surgery, Cincinnati Children’s HospitalMedical Center, 3333 Burnet Avenue, Cincinnati, OH 45215, USA
Received 16 July 2003; accepted 31 August 2003
KEYWORDSTracheal resection;Tracheal stenosis;Tracheal stent
Summary Objective: While tracheal resection for management of tracheal stenosisis an effective technique that has been well described in adults, the results in childrenhave been less encouraging, as children tolerate anastomotic tension less well thanadults. We describe our current technique for the management of severe trachealstenosis in older children. Methods: Four teenagers, 16—17 years of age, presentedwith severe tracheal stenosis. A 16-year-old girl had sustained tracheal stenosis fol-lowing prolonged intubation, and presented with a severe Grade III stenosis having had25 endoscopic procedures, and a failed resection at another institute. Two 17-year-oldboys and a 17-year-old girl presented with Grade IV stenosis at the suprastomal areafollowing previous intubation injuries. All four children had an identical procedurewith tracheal resection over a Hood tracheal stent. Results: All four children wereextubated in the operating room. Chin-to-chest sutures were removed between 7 and10 days, as was the Hood stent. All four are currently asymptomatic with no airwaystenosis. Conclusions: Although tracheal resection for tracheal stenosis in childrenis associated with a higher failure rate than is seen in the adult population, evensevere stenosis and long segment resection may achieve excellent results. We feelthat important factors influencing outcome in this series included anastomosis to anintact cricoid ring, and support of the anastomosis with a tracheal stent.© 2003 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Cricotracheal or tracheal resection is becomingthe procedure of choice for the management ofsevere acquired tracheal and subglottic stenosisin children [1,2]. It offers the advantage of recon-structing the airway with well vascularized, rigidtrachea. Despite this, the management of severetracheal and subglottic stenosis in children con-
� Presented December 2002 at the Society for, Ear, Nose, andThroat Advances in Children, Atlanta, GA.
∗Corresponding author. Tel.: +1-513-636-4356;fax: +1-513-636-2886.E-mail address: [email protected] (M.J. Rutter).
tinues to be challenging. Due to a smaller airwaydiameter, and to worse tolerance of anastamotictension [3,4], pediatric tracheal procedures havebeen generally less successful than those in adults[5]. In most cases, the severity of pre-operativesubglottic or tracheal obstruction predicates mul-tiple surgical treatment stages with placement ofsuprastomal stents or T-tubes.
Laryngotracheal stenosis in children most com-monly involves the subglottis, as it is uncommonto find pediatric patients where the stenotic seg-ment is isolated to the high trachea, sparing thecricoid cartilage. In children with purely trachealstenosis, tracheal resection with primary anas-tomosis to an intact cricoid cartilage seems to
0165-5876/$ – see front matter © 2003 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijporl.2003.08.054

2 D. Preciado et al.
be an effective means of airway reconstruction[6].
We present a cohort of older children with se-vere tracheal stenosis in whom we performedsingle-stage tracheal resection, achieving extuba-tion in the immediate post-operative period. Ourapproach was based on the following concepts: (1)the preservation of an intact cricoid ring confers amore stable, rigid anastamosis, and (2) the largerairway diameter of older children provides theability to utilize large-bore indwelling Hood stentsconferring increased support to the reconstructedsite. Details of the procedure and post-operativecare are discussed.
2. Methods
Four teenagers, 16—17 years of age, presented inthe past year with severe tracheal stenosis. Threepresented with Grade IV one with Grade III purelytracheal stenosis according to the new Cotton andMyer classification scheme [7], which although de-signed to describe subglottic stenosis, is adequateto classify the patients in this series. The clinicalhistory and operative repair procedure for each pa-tient is described as follows. Follow-up has rangedfrom 1 to 6 months.
2.1. Patient histories
Case 1. A 16-year-old girl had sustained trachealstenosis following 6 days of endotracheal intu-bation secondary to a motor vehicle accident inOctober 2001. She presented with a severe GradeIII stenosis and underwent approximately 24 endo-scopic laser procedures and dilatations, followedby a tracheal resection at an outside institution,and then more endoscopic laser and dilatationprocedures. Initial evaluation at our institutionrevealed recalcitrant severe Grade III trachealstenosis. We treated her with a single-stage tra-cheal resection and placement of an indwelling,endo-luminal 14mm Hood stent. Extubation wasdone on the operative table. The stent was re-moved endoscopically on post-operative day 10.Follow-up bronchoscopies at 1 week and 1 monthafter stent removal revealed a healed anastomo-sis and a widely patent airway. She has remainedasymptomatic.
Case 2. A 17-year-old boy sustained trachealtrauma after a hanging suicide attempt in Decem-ber 2001. He developed progressive shortness ofbreath and was tracheotomized February 2002.Initial evaluation at our institution revealed Grade
IV stenosis. An identical reconstruction was per-formed with single-stage tracheal resection andplacement of an indwelling, endo-luminal 16mmHood stent. Extubation was again performed onthe operative table on recovery from anesthe-sia. The stent was removed endoscopically onpost-operative day 7. Follow-up bronchoscopy per-formed at 1 week after stent removal revealed ahealed anastomosis and a widely patent airway. Hehas remained asymptomatic.
Case 3. A 17-year-old boy developed trachealstenosis following a motor vehicle accident in May2002. He was endotracheally intubated for 5 daysafter the injury at which point a tracheotomywas performed during repair of multiple facialand mandibular fractures. Due to inability to de-cannulate, bronchoscopy was performed whichrevealed Grade IV tracheal stenosis. He under-went an identical procedure to the aforementionedcases. A 16mm Hood stent was used which wasremoved endoscopically on post-operative day10. Follow-up bronchoscopy performed at 1 weekand 1 month revealed a well-healed anastomo-sis and a widely patent airway. He has remainedasymptomatic.
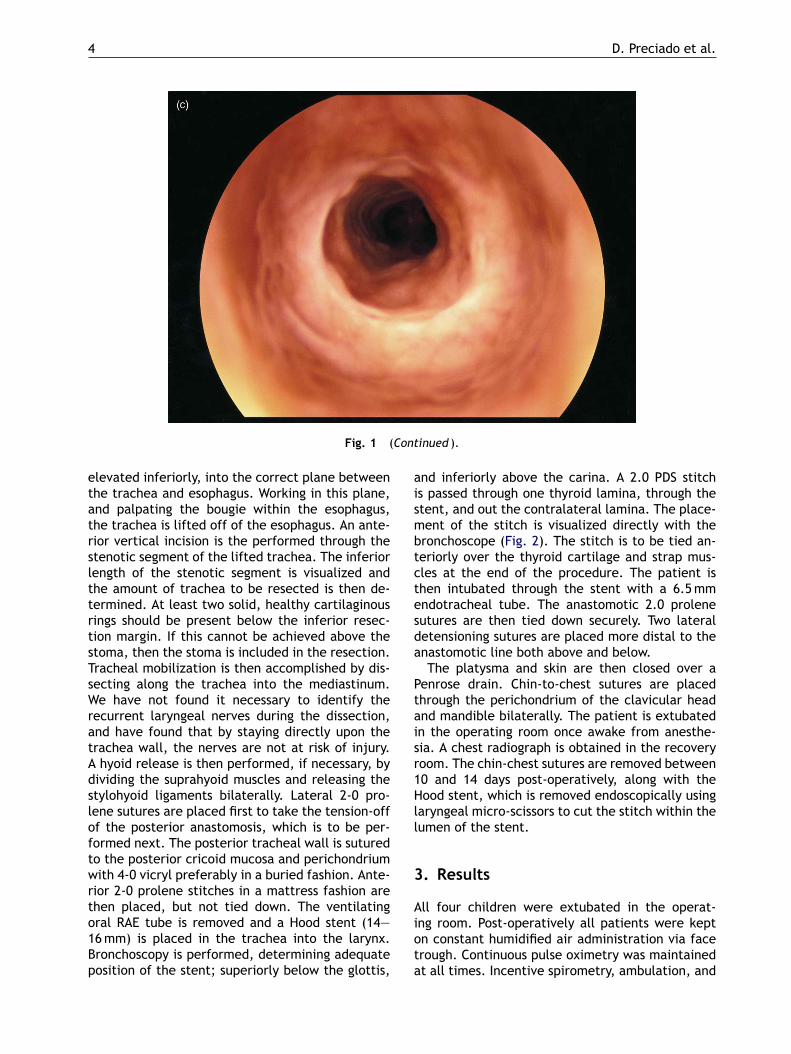
Case 4. A 17-year-old female developed trachealstenosis following endotracheal intubation for 6days secondary to a motor vehicle accident in June2002. After failing to extubate, the stenosis wasnoted and a tracheotomy was performed. Her air-way was the treated with three endoscopic laserprocedures with dilatation which unfortunatelyfailed to improve the stenosis. She was evaluated atour institution, where Grade IV stenosis was noted(Fig. 1a). She underwent an identical procedure tothe aforementioned cases. In her case, a 14mmHood stent was used which was removed endsocop-ically on post-operative day 14. Follow-up bron-choscopy at 1 week (Fig. 1b) and 6 months (Fig. 1c)after stent removal have revealed a well-healedanastomosis and a widely patent airway. She hasremained asymptomatic.
Details of the operative procedure performed ineach of the above cases is described as follows.
2.2. Description of surgical procedure
Microlaryngoscopy and bronchoscopy is first per-formed to confirm the stenotic pathology. Ansthe-sia and ventilation is maintained through a cut oralRing Adair Elwyn (RAE) endotracheal tube placedthrough the stoma. A shoulder roll, head ring, andesophageal bougie are placed. A horizontal incision

Tracheal stenosis in older children 3
is made, including an ellipse excision of the stomatract. The airway is then exposed in routine fashion,with the dissection exposing the hyoid, thyroid andcricoid cartilages. The trachea is skeletonized, andexposed into the anterior mediastinum. A thyroidisthmusotomy is performed and the thyroid lobesare retracted laterally with silk sutures.
Once adequate exposure is achieved, an an-terior horizontal incision is made just below the
Fig. 1 (a) Pre-operative tracheal stenosis photograph; (b) 1 week post-operative photograph; (c) 6-monthpost-operative follow-up photograph.
cricoid cartilage. The tracheal stenosis is then vi-sualized directly and confirmation that the cricoidcartilage is not involved is done. The airway inci-sion is then carried posteriorly just slightly ontothe lower border of the posterior cricoid plate.The incision is not carried through the cartilageitself. A sub-perichondrial plane of dissection isachieved and a mucosa-perichondrial flap is estab-lished along the posterior cricoid plate. This flap is
4 D. Preciado et al.
Fig. 1 (Continued ).
elevated inferiorly, into the correct plane betweenthe trachea and esophagus. Working in this plane,and palpating the bougie within the esophagus,the trachea is lifted off of the esophagus. An ante-rior vertical incision is the performed through thestenotic segment of the lifted trachea. The inferiorlength of the stenotic segment is visualized andthe amount of trachea to be resected is then de-termined. At least two solid, healthy cartilaginousrings should be present below the inferior resec-tion margin. If this cannot be achieved above thestoma, then the stoma is included in the resection.Tracheal mobilization is then accomplished by dis-secting along the trachea into the mediastinum.We have not found it necessary to identify therecurrent laryngeal nerves during the dissection,and have found that by staying directly upon thetrachea wall, the nerves are not at risk of injury.A hyoid release is then performed, if necessary, bydividing the suprahyoid muscles and releasing thestylohyoid ligaments bilaterally. Lateral 2-0 pro-lene sutures are placed first to take the tension-offof the posterior anastomosis, which is to be per-formed next. The posterior tracheal wall is suturedto the posterior cricoid mucosa and perichondriumwith 4-0 vicryl preferably in a buried fashion. Ante-rior 2-0 prolene stitches in a mattress fashion arethen placed, but not tied down. The ventilatingoral RAE tube is removed and a Hood stent (14—16mm) is placed in the trachea into the larynx.Bronchoscopy is performed, determining adequateposition of the stent; superiorly below the glottis,
and inferiorly above the carina. A 2.0 PDS stitchis passed through one thyroid lamina, through thestent, and out the contralateral lamina. The place-ment of the stitch is visualized directly with thebronchoscope (Fig. 2). The stitch is to be tied an-teriorly over the thyroid cartilage and strap mus-cles at the end of the procedure. The patient isthen intubated through the stent with a 6.5mmendotracheal tube. The anastomotic 2.0 prolenesutures are then tied down securely. Two lateraldetensioning sutures are placed more distal to theanastomotic line both above and below.
The platysma and skin are then closed over aPenrose drain. Chin-to-chest sutures are placedthrough the perichondrium of the clavicular headand mandible bilaterally. The patient is extubatedin the operating room once awake from anesthe-sia. A chest radiograph is obtained in the recoveryroom. The chin-chest sutures are removed between10 and 14 days post-operatively, along with theHood stent, which is removed endoscopically usinglaryngeal micro-scissors to cut the stitch within thelumen of the stent.
3. Results
All four children were extubated in the operat-ing room. Post-operatively all patients were kepton constant humidified air administration via facetrough. Continuous pulse oximetry was maintainedat all times. Incentive spirometry, ambulation, and

Tracheal stenosis in older children 5
Fig. 2 Indwelling tracheal Hood stent photograph.
Table 1 Summary of results
Patient Sex Age (years) Etiology Grade Resection SH release Stent size (mm) Stent removal
1 F 16 Intubation III 4 rings Y 14 POD 102 M 17 Hanging injury IV 3 rings N 16 POD 73 M 17 Intubation IV 6 rings Y 16 POD 104 F 17 Intubation IV 7 rings Y 14 POD 14
SH: suprahyoid; POD: post-operative day.
coughing were encouraged. Oral diet was startedon the first post-operative day. The Penrose drainwas removed on the second or third post-operativeday. Chin-to-chest sutures were removed be-tween 7 and 14 days, as was the Hood stent,endoscopically.
All patients were observed carefully for possi-ble development of impacted secretions or mucousplugging. Despite a low threshold to return to theoperating room for these reasons, it was not neces-sary in any of the patients.
Follow-up bronchoscopy was performed at thetime of stent removal did not reveal significantgranulations in any patient. It was not uncommon tofind denuded, raw mucosa at that time. All patientsremained hospitalized until their first follow-up en-doscopic evaluation, 1 week after stent removal.Follow-up has ranged from 1 to 6 months fromthat point. All four are currently asymptomaticwith no airway stenosis.Table 1 summarizes ourresults.
4. Discussion
In the past, a general reluctance had existed to per-form cricotracheal resection (CTR) in children withsevere subglottic and tracheal stenosis. This feelinghad stemmed from concern over possible injury tothe recurrent laryngeal nerves, negative effects onlaryngotracheal growth, and the overall complex-ity of the procedure. Recent series have disproventhis notion, as CTR has been performed with suc-cess in the pediatric age group [8,9]. Indeed, CTRhas become the preferred treatment method forchildren with severe type III and type IV stenosis[10,11] as long as the margin of resection is ade-quately below the free glottic edge [12]. Althoughin our experience laryngotracheal stenosis follow-ing endotracheal intubation usually manifests withextensive subglottic involvement, when the steno-sis is isolated to the upper cervical trachea, tra-cheal resection with primary anastomosis has beenthe procedure of choice [6]. Animal studies [5,13]

6 D. Preciado et al.
and long-term follow-up human series [14] have notshown interference with laryngotracheal growth ininfants and children after resection. Despite thesefacts, children do not tolerate anastomotic tensionas well as adults, and have significantly increasedproblems with dehiscence when more than 30% ofthe trachea is resected [4]. It may be that the prog-nosis of tracheal anastomotic success in children isage related. Previous series [6] from our institutionshowed that older children required no second air-way augmentation procedures after tracheal resec-tion when compared to younger children.
Our pilot series points to the feasibility of safelyperforming single-stage tracheal resection in olderchildren with severe tracheal stenosis. Multipleadvantages can be seen with this approach. Allstenotic and scarred tissue is resected, restoringa large lumen with normal mucosal lining aboveand below the anastomosis. Prolonged stentingis avoided. Immediate vocalization is achieved.Many reasons exist as to why this treatmentmethod is plausible in older children. For one,teenage childrens’ airways approximate adult size.A large-bore intraluminal stent fits in the airwayadequately, through which orotracheal intubationis possible. As compared to infants and youngerchildren, teenage airways are likely to bettertolerate anastomotic tension. Illustratively, twoof our patients required more than 30% trachealresection. Finally, the anastomosis is performedto an intact cricoid ring, which is not involvedby the stenosis. Certainly, this is a major fac-tor in tolerating increased tension and improvedsuccess.
Although placement of the indwelling Hood tra-cheal stent allows for anastomotic support, sameday extubation, and immediate vocalization, thepotential for life-threatening mucous plugging is ofconcern. For this reason, all patients in our cohortwere closely monitored post-operatively, and main-tained on constant humidification. A low thresholdfor returning to the operating room to clear thestent of inspissated secretions was kept. Problemswith stent obstruction were not encountered in thisseries.
This series is limited by small numbers and limitedfollow-up periods. Initial results have been very en-couraging. Increased follow-up periods in a largergroup of teenage childrenwith tracheal stenosis willbe needed to validate our approach.
In conclusion, although tracheal resection for tra-cheal stenosis in children is associated with a higherfailure rate than is seen in the adult population,even severe stenosis and long segment resectionmay achieve excellent results. We feel that impor-tant factors influencing outcome in this series in-cluded anastomosis to an intact cricoid ring, andsupport of the anastomosis with a tracheal stent.Meticulous post-operative monitoring and care ismandatory.
References
[1] M.J. Rutter, B.E.J. Hartley, R.T. Cotton, Cricotracheal re-section in children, Arch. Otolaryngol. Head Neck Surg.127 (2001) 289—292.
[2] P. Monnier, F. Lang, M. Savary, Cricotracheal resection forpediatric subglottic stenosis, Int. J. Pediatr. Otorhinolaryn-gol. 49 (1999) S283—S286.
[3] H.C. Grillo, M. Maeda, Effect of tension on tracheal growthafter resection in puppies, J. Thorac. Cardiovasc. Surg. 65(1973) 658—668.
[4] C.D. Wright, B.B. Graham, M. Eng, et al., Pediatric trachealsurgery, Ann. Thorac. Surg. 74 (2002) 308—314.
[5] H.C. Grillo, D.M. Donahue, D.J. Mathisen, et al., Postintu-bation tracheal stenosis. Treatment and results, J. Thorac.Cardiovasc. Surg. 109 (1995) 486—493.
[6] B.J. Waitrak, R.T. Cotton, Anastomosis of the cervical tra-chea in children, Arch. Otolaryngol. Head Neck Surg. 118(1992) 58—62.
[7] C.M. Myer III, D.M. O’Connor, R.T. Cotton, Proposed gradingsystem for subglottic stenosis based on endotracheal tubesizes, Ann. Otol. Rhinol. Laryngol. 103 (1994) 319—323.
[8] Y. Stern, M.E. Gerber, D.L. Walner, R.T. Cotton, Partialcricotracheal resection with primary anstomosis in the pe-diatric age group, Ann. Otol. Rhinol. Laryngol. 106 (1997)891—896.
[9] P. Monnier, F. Lang, M. Savary, Partial cricotracheal re-section for severe pediatric subglottic stenosis: update onthe Lusanne experience, Ann. Otol. Rhinol. Laryngol. 107(1998) 961—968.
[10] B.E. Hartley, R.T. Cotton, Pediatric airway stenosis: laryn-gotracheal reconstruction or cricotracheal resection? Clin.Otolaryngol. 25 (2000) 342—349.
[11] P. Monnier, M. Savary, G. Chapius, Partial cricoid resectionwith primary tracheal anastomosis for subglottic stenosis ininfants and children, Laryngoscope 103 (1993) 1273—1283.
[12] D.L. Walner, Y. Stern, R.T. Cotton, Margins of partial crico-tracheal resection in children, Laryngoscope 109 (1999)1607—1610.
[13] B. Fearon, B.D. McMillin, Cricoid resection and thyrotra-cheal anastomosis in the growing primate, Ann. Otol. Rhi-nol. Laryngol. 94 (1985) 631—633.
[14] P. Monnier, M. Savary, G. Chapius, Partial cricoid resectionwith primary tracheal anastomosis for subglottic stenosis ininfants and children, Laryngoscope 103 (1993) 1273—1285.