Sindrome Msrfan y Ehlers Danlos

of 25
Transcript of Sindrome Msrfan y Ehlers Danlos
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
1/25
12
Ehlers-Danlos syndromes and Marfan
syndrome
Bert Callewaert MDResearch Fellow
Fransiska Malfait MD, PhDResearch Fellow
Bart Loeys MD, PhDClinical Geneticist and Senior Researcher
Anne De Paepe* MD, PhDProfessor and Head of Department
Ghent University Hospital, Centre for Medical Genetics, De Pintelaan 185, B-9000 Ghent, Belgium
Ehlers-Danlos syndromes (EDS) and Marfan syndrome (MFS) are multisystemic disorders thatprimarily affect the soft connective tissues. Both disorders have benefited from recent advancesin clinical and molecular characterization, allowing improvements in clinical diagnosis and man-agement. EDS are a heterogeneous group of conditions characterized by skin hyperextensibility,atrophic scarring, joint hypermobility and generalized tissue fragility. The current classificationproposes six subtypes based on clinical, biochemical and molecular characteristics. However, ex-amples of unclassified variants and overlap phenotypes are becoming more common. Mutationsin genes encoding fibrillar collagens or collagen-modifying enzymes have been identified in most
forms of EDS, including the classic and vascular subtypes (collagen type V and III, respectively),and the rare arthrochalasis, kyphoscoliosis and dermatosparaxis variants (type I collagen de-fects). To date, the genetic background of the hypermobility type of EDS remains unclear, al-though some new insights have been gained recently.
MFS is an autosomal-dominant disorder that affects the cardiovascular, ocular and skeletalsystem with aortic root dilation/dissection, ectopia lentis and bone overgrowth, respectively.Advances in therapeutic, mainly surgical, techniques have improved median survival significantly,yet severe morbidity and a substantial risk for premature mortality remain associated. The dis-order is caused by mutations in the FBN1 gene, encoding the microfibrillar protein fibrillin-1.Recently, new insights in the pathogenesis changed the prevailing concept of this type 1
* Corresponding author. Tel.: 32 9 332 36 03; Fax: 32 9 332 49 70.
E-mail address: [email protected] (A. De Paepe).
1521-6942/$ - see front matter 2007 Elsevier Ltd. All rights reserved.
Best Practice & Research Clinical RheumatologyVol. 22, No. 1, pp. 165189, 2008
doi:10.1016/j.berh.2007.12.005
available online at http://www.sciencedirect.com
mailto:[email protected]://www.sciencedirect.com/http://www.sciencedirect.com/mailto:[email protected] -
7/30/2019 Sindrome Msrfan y Ehlers Danlos
2/25
fibrillinopathy as a structural disorder of the connective tissue into a developmental abnormalitymanifesting perturbed cytokine signalling. These findings have opened new and unexpectedtargets for aetiologically directed drug treatments.
Key words: Ehlers-Danlos syndromes; Marfan syndrome; clinical features; molecular pathogen-esis; differential diagnosis; management.
EHLERS-DANLOS SYNDROMES
Introduction
Ehlers-Danlos syndromes (EDS) comprise a clinically and genetically heterogeneousgroup of heritable disorders of connective tissue, of which the principal clinical fea-tures are due to varying degrees of tissue fragility of the skin, ligaments, blood vessels
and internal organs. The first classical description of the syndrome in the medicalliterature is attributed to Tschernogubow, a Russian dermatologist who described itin 1891. In 1901 and 1908, respectively, it was reported by the Danish and French der-matologists Ehlers and Danlos, and in the 1930s, the condition received its eponymoustitle, and, by this, its scientific respectability. In the mid-20th Century, it was suggestedthat a genetic defect in the collagen wickerwork of the connective tissues accountedfor the phenotype, and not much later, the first genetic defect was identified as a de-ficiency of lysyl hydroxylase, a collagen-modifying enzyme. Soon thereafter, the clinicaland genetic heterogeneity of the syndrome became evident, and with the improve-ment of biochemical and molecular techniques, a range of defects in collagen proteins
and collagen-modifying enzymes were discovered in various forms of EDS. Earlydiagnosis by means of biochemical and molecular testing is now feasible for mostEDS variants, and may prove important for adequate follow-up and genetic counselling.
This chapter gives an overview of the main clinical characteristics as well as anupdate of the current insights in the molecular pathogenesis of EDS.
Epidemiology and criteria for diagnosis
The prevalence of EDS is estimated to be approximately one in 5000 births, with no racial
predisposition.1 However, the incidence rises with increased physician awareness.The first attempts to classify EDS resulted in the Berlin nosology in 1986, in which
10 subtypes were recognized.2 Elucidation of the molecular basis of several types ofEDS resulted in refinement of this classification, which led to the 1997 Villefranche no-sology.3 This classification recognizes six subtypes, based on clinical characteristics,mode of inheritance, and biochemical and molecular findings. For each subtype, majorand minor clinical diagnostic criteria were defined. The most common types are theclassic, hypermobility and vascular types, while the kyphoscoliosis, arthrochalasisand dermatosparaxis types are very rare. Over the past few years, it has become clearthat this classification remains insufficient and that many patients present with overlap-
ping forms of EDS, which cannot be classified unambiguously into one of the sixrecognized subtypes. Recent insights into the molecular and biochemical basis ofsome EDS variants call for a refinement of the Villefranche classification, which willlikely improve genetic counselling of affected families.
166 B. Callewaert et al
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
3/25
Clinical characteristics
The main clinical characteristics of EDS, which are present to varying degrees in eachsubtype, include skin hyperextensibility, delayed wound healing with atrophic scarring,
joint hypermobility, easy bruising, and generalized fragility of the soft connectivetissues.
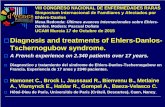
Skin hyperextensibility is characteristic for all EDS subtypes, except the vasculartype. In contrast to the skin in cutis laxa syndromes, the skin of EDS patients is hypere-lastic, which means that it extends easily and snaps back after release. The skin is oftenvery smooth and velvety to the touch. Wound healing is delayed and results in the for-mation of widened atrophic scars, so-called cigarette-paper scars, occurring mainlyover knees, elbows, shins, forehead and chin (Figure 1). In the vascular type, theskin is not hyperextensible, but thin and transparent, showing the venous patternover the chest, abdomen and extremities.
Joint hypermobility (Figure 2) is usually generalized and can vary in severity. It isgenerally assessed using the Beighton scale (Table 1). At birth, uni- or bilateral
Figure 1. Atrophic scarring on the knees in a patient with Ehlers-Danlos syndrome. On the shins, repetitive
trauma has led to haemosiderin deposition with dark and unaesthetic discolouration of the skin.
Ehlers-Danlos syndromes and Marfan syndrome 167
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
4/25
dislocation of the hip may be present. Primary muscular hypotonia may result in de-layed motor development. During childhood, complications are not frequent, but sub-luxations and dislocations may occur from young adulthood onwards, either
spontaneously or after minimal trauma. All sites can be involved, including the extrem-ities, vertebral column, costo-vertebral and costo-sternal joints, clavicular articulationsand temporomandibular joints. Other problems related to joint hypermobility are footdeformities such as congenital club foot or pes planus, joint effusions and prematureosteoarthritis. Some adults may suffer from chronic musculoskeletal pain, which is dis-tinct from the pain associated with acute dislocations. The severity of the complaints istypically greater than expected based on physical and radiological examination, and theimpact can be devastating with disruption of sleep, work, physical activities and socialrelationships.
Easy bruising is a common finding in patients with EDS, and it may even be the pre-
senting symptom in small children. It manifests as spontaneous ecchymoses, frequentlyrecurring in the same areas and causing a characteristic brownish discolouration of the
Figure 2. Joint hypermobility in Ehlers-Danlos syndrome.
Table 1. Beighton scale for joint hypermobility. A total score of at least 5 defines hypermobility.
Joint/finding Negative Unilateral Bilateral
Passive dorsiflexion of the 5th finger> 90 0 1 2
Passive flexion of thumbs to the forearm 0 1 2
Hyperextension of the elbows beyond 10 0 1 2
Hyperextension of the knees beyond 10 0 1 2Forward flexion of the trunk with knees
fully extended and palms resting on the floor
0 Present 1
168 B. Callewaert et al
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
5/25
skin, especially in exposed areas such as shins and knees. There is a tendency towardsprolonged bleeding, e.g. following brushing of the teeth, in spite of a normal coagula-tion status.
Other manifestations of generalized tissue fragility are observed in multiple organsand include cervical insufficiency; inguinal, umbilical or other hernias; recurrent rectalprolapse in early childhood; and dehiscence of sutured incisions in skin or mucosa.
Structural cardiac malformations are uncommon in most EDS types, but mitral valveprolapse and, less frequently, tricuspid valve prolapse may occur.
The vascular type of EDS deserves special attention as this condition is associatedwith an increased risk of life-threatening complications and a decreased life expec-tancy. Patients with vascular EDS are at risk of arterial rupture which may occur spon-taneously or may be preceded by aneurysm, arteriovenous fistulae or dissection.Other complications include spontaneous rupture of the bowel, intestine or graviduterus. Patients with vascular EDS who are pregnant should be followed in a high-risk obstetric programme.
In addition to these general features, some EDS subtypes are characterized by
a number of clinical manifestations which are subtype specific, and which have beendefined in the major and/or minor criteria of the nosology, as outlined in Table 2.
Differential diagnosis
EDS shows limited overlap with other heritable disorders of connective tissue, whichcan usually be differentiated by distinctive clinical features. EDS should be distinguishedfrom Marfan syndrome (MFS), the clinical and molecular features of which are dis-cussed below. In EDS, the skin fragility is more prominent, and joint hypermobility
is usually more severe. Although patients with the kyphoscoliosis type of EDS, and oc-casionally patients with the hypermobility type of EDS, can present with a marfanoidhabitus, the association with ectopia lentis and/or aortic dilatation or aneurysm isstrongly suggestive for MFS.
There is considerable clinical overlap between the vascular type of EDS and Loeys-Dietz syndrome type 2, a recently identified aortic aneurysm syndrome that will bediscussed in more detail below and which is caused by mutations in the genes codingfor transforming growth factor-beta (TGFb) receptor 1 and 2 (TGFBR1 or TGFBR2).4
The hyperextensible skin in EDS should be distinguished from the skin laxity ob-served in cutis laxa and De Barsy syndromes, in which the redundant skin hangs in
loose folds and only returns very slowly to its former position. In these syndromes,the skin is not fragile and wound healing is normal.
EDS should also be distinguished from occipital horn syndrome (OHS), character-ized by the presence of occipital horns; distinctive wedge-shaped calcifications at thesites of attachment of the trapezius muscle and the sternocleidomastoid muscle to theoccipital bone. Occipital horns may be clinically palpable or observed on skull radio-graphs. Individuals with OHS also have lax skin and joints, bladder diverticulae, inguinalhernias and vascular tortuosity. There is no easy bruising or fragility of the skin. Theserum concentrations of copper and ceruloplasmin are low. This X-linked condition isallelic with Menkes disease and is caused by mutations in a copper transporter protein
encoded by ATP7A.5
Joint hypermobility may be the presenting feature in some other rare genetic con-ditions, such as pseudo-achondroplasia or Larsen syndrome, which present with otherdistinctive symptoms, and in which the typical EDS skin features are absent. Distal joint
Ehlers-Danlos syndromes and Marfan syndrome 169
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
6/25
Table 2. Updated Ehlers-Danlos syndrome (EDS) nosology. The presence of more than one cardinal feature is h
of EDS, while the additional features contribute to the diagnosis of the specific subtype.
Clinical subtype Clinical manifestations Gene defect Pr
Cardinal features Additional features
Classic (AD) Skin hyperextensibility
Widened atrophic
scarring
Smooth and velvety
skin
Joint hypermobility
Easy bruising
Molluscoid
pseudotumours
Subcutaneous
spheroids
Muscular hypotonia
Complications of
joint hypermobility
Surgical complications Positive family history
COL5A1 non-
functional allele
Mutation (mis-sense,
exon-deletion) in
COL5A1 or COL5A2
Fu
of
Unknown U
Classic-like (AR) Skin hyperextensibility
Easy bruising
Joint hypermobility
Smooth and velvety
skin
Complications of
joint hypermobility
Homozygous or
compound heterozygous
mutations in TNX-B
C
of
Hypermobility (AD) Generalized joint
hypermobility
Mild skin involvement
(mild skin
hyperextensibility, mildatrophic scarring,
soft skin)
Recurring joint
dislocations
Chronic joint pain
Positive family
history
TNX-B non-functional
allele
Mis-sense mutation in
TNX-B
Sy
on
of
St
ofCOL5A1 non-functional
allele
Fu
of
Unknown
One locus on
chromosome 8p21
U
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
7/25
Vascular (AD) Excessive bruising
Thin, translucent skin
Arterial/intestinal/
uterine fragility
or rupture
Characteristic facial
appearance
Acrogeria
Early-onset varicose
veins
Hypermobility
of small joints
Tendon and muscle
rupture
Arteriovenous or
carotid-cavernous
sinus fistula
Pneumo(haemo)thorax
Positive family history,
sudden death in close
relative(s)
COL3A1 mutation
COL3A1 non-functional
allele
St
of
Sy
on
of
pr
Vascular-like (AD) Skin hyperextensibility
Atrophic scarring
Easy bruising Arterial rupture
Thin, translucent skin
Joint hypermobility
Complications ofjoint hypermobility
Positive family
history
COL1A1 mis-sense
mutation
R
in
do
Osteopenia
Arterial rupture
COL1A1 mis-sense
mutation
R-
in
do
Cardiac valvular
(AR)
Severe cardiac valvular
disease
Skin hyperextensibility
Joint hypermobility
Atrophic scarring
Easy bruising
Blue sclerae
Increased bone
fragility
Homozygous or
compound heterozygous
mutations in COL1A2
C
of
ch
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
8/25
Table 2 (continued)Clinical subtype Clinical manifestations Gene defect Pr
Cardinal features Additional features
Kyphoscoliotic
(AR)
Severe muscular
hypotonia at birth
Generalized joint laxity
Kyphoscoliosis at birth
Scleral fragility and
rupture of the globe
Tissue fragility,
including atrophic
scars
Easy bruising
Arterial rupture
Marfanoid habitus
Microcornea
Osteopenia
Homozygous or
compound heterozygous
mutations in LH-1
(PLOD1)
D
ly
Unknown U
EDS/OI overlap
syndrome (AD)
Joint hypermobility
Mild skin involvement
Blue sclerae
Increased bone fragility
Easy bruising
Recurring joint
dislocations
Kyphoscoliosis
Chronic joint pain
Arterial rupture
Positive family
history
Mutation (exon-deletion,
mis-sense) in COL1A1 or
COL1A2 encoding the
most
amino-terminal part (w
first 80e100 amino acids)
of type I collagen triple
helical domain
St
of
N
le
pr
pr
Arthrochalasis (AD) Severe generalized
joint hypermobility withrecurrent subluxations
Congenital bilateral
hip dislocation
Skin hyperextensibility
Widened, atrophic
scars
Easy bruising
Muscular hypotonia Kyphoscoliosis
Mild osteopenia
Mutation leading to
deletion of exon 6 ofCOL1A1 or COL1A2
Lo
-Nsit
or
ch
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
9/25
Dermatosparaxis
(AR)
Severe skin
fragility
Sagging, redundant
skin
Excessive bruising
Characteristic facies
(oedema of eyelids,
downslanting palpebral
fissures, epicanthic
folds, blue sclerae,
gingival hyperplasia,
micrognathia)
Postnatal growth
deficiency, short
hands and feet
Umbilical hernia
Delayed closure
of fontanelles
Soft, doughy
skin texture
Premature
rupture of
membranes
Progressive cigarette-
paper scar formation
Progressive generalized
joint hypermobility,
delayed gross motor
development
Increased palmar
wrinkling
Bladder rupture
Rupture of diaphragm
ADAMTS-2 Pr
N
IP, inheritance pattern; AD, autosomal dominant; AR, autosomal recessive; PLOD 1, procollagen-lysine 2-
OI, osteogenesis imperfecta; HPLC, high-performance liquid chromatography; SDS-PAGE: sodium-dodecyl poly
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
10/25
hyperextensibility in combination with proximal contractures and generalized muscleweakness is the hallmark of severe congenital muscular dystrophy, known as Ullrichdisease or scleroatonic muscular dystrophy.6 The finding of excessive distal joint laxityis striking and often raises EDS as a diagnostic consideration. This condition, which canbe inherited autosomal dominantly or recessively, results from mutations in the genesencoding type VI collagen.79
Molecular pathogenesis
EDS is extremely heterogeneous at both the clinical and the molecular level. Abnor-malities in the expression or structure of the fibrillar collagen types I, III and V, aswell as enzymatic abnormalities in the post-translational modification and processingof these collagens, have been identified in a number of EDS subtypes.
Mutations in the COL5A1 and COL5A2 genes, encoding the a1- and the a2-chains oftype V collagen, respectively, are found in approximately 50% of individuals with the
classic type of EDS. Type V collagen is a minor fibrillar collagen which co-assembleswith type I collagen, and acts as a regulator of collagen fibril diameter through the re-tention of a non-collagenous amino-terminal domain of the proa1(V)-collagen chain. Inapproximately one-third of all classic EDS patients, the disease is caused by a mutationleading to a non-functional COL5A1 allele, resulting in a diminished amount of type Vcollagen that is available for collagen fibrillogenesis. In a smaller proportion of patients,a mutation in COL5A1 or COL5A2 is found, resulting in the production of a structurallyaltered and functionally defective type V collagen protein.10 The relatively low detec-tion rate for mutations in the COL5A1/A2 genes suggests genetic heterogeneity for thiscondition, and this hypothesis is supported by several other findings. First, mutations
in a non-collagenous protein, tenascin-X, leading to a complete lack of serum tenascin-X, have been shown to cause an autosomal-recessive phenotype with great similaritiesto classic EDS, but without atrophic scars.11 Tenascin-X is a large extracellular matrixprotein that is thought to play an important role in the regulation of collagen deposi-tion by dermal fibroblasts.11 Second, linkage studies have excluded the COL5A1 and/orthe COL5A2 gene in at least three pedigrees with classic EDS.12,13 Third, features ofclassic EDS are found in patients with other variants of EDS. For example, a subgroupof patients with the classic EDS phenotype has been observed who, in adult life, devel-oped severe cardiac valvular problems, and in whom a complete deficiency of the proa2-chain of type I collagen has been identified. This autosomal-recessive condition has been
termed the cardiac valvular subtype of EDS.1416 Classic EDS features were also ob-served in a number of children with non-glycine substitutions in the type I collagen triplehelical domain.17 Recent observations showed that this phenotype evolves to a vascularEDS-like phenotype in adult life, with increased risk for spontaneous arterial rupture.18
To date, little is known regarding the genetic defects underlying the hypermobilitytype of EDS, which is by far the most common subtype. In this subtype, considerablevariability in clinical presentation, between as well as within families, hampers the useof genetic linkage studies, although some new insights on the genetic background ofthis condition have emerged recently. Family studies show that a phenotypic contin-uum may exist between classic and hypermobile EDS, and therefore, haplo-
insufficiency of the COL5A1 gene may be found in patients with the hypermobilitytype of EDS, despite the fact that the skin is not severely affected. In a small subset ofpatients with hypermobile EDS (5%), diminished levels of tenascin-X, due to heterozygousmutations in the TNX-B gene, have been identified.19 In the vast majority of patients,
174 B. Callewaert et al
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
11/25
however, no molecular defects have been identified in this gene or in any of the fibrillarcollagen-encoding genes. The authors performed a genome-wide linkage scan ina three-generation family with the hypermobility type of EDS with at least 13 affectedindividuals, and were able to identify a new locus on chromosome 8p21 for this con-dition (Malfait et al, submitted).
The vascular type of EDS results from mutations in the COL3A1 gene, encoding the
pro-a1-chain of type III collagen. A wide spectrum ofCOL3A1 mutations has been iden-tified, the majority of which are point mutations leading to substitutions for the oblig-atory glycine in the triple helical region of the collagen molecule.1,20
Whereas defects in the genes encoding type I collagen generally result in differentforms of osteogenesis imperfecta, one specific class of mutations, affecting either theCOL1A1 or the COL1A2 gene, leads to loss of the cleavage site for the enzyme procol-lagen type I amino-proteinase. As a result, the aminopropeptide of either thepro-a1(I)- or the pro-a2(I)-collagen chain is not cleaved from the triple helical domain,resulting in elongation of the collagen chains and disturbed fibrillogenesis. This givesrise to the arthrochalasis type of EDS. It has recently been shown that some mutations
in the most amino-terminal part of type I collagen also interfere with removal of theN-terminal propeptide, despite the fact that they leave the N-proteinase cleavage siteintact. These mutations result in a distinct EDS/OI overlap phenotype, characterizedby features of both EDS and osteogenesis imperfecta21,22 (Malfait et al, submitted).
Finally, homozygous or compound heterozygous mutations in genes encoding en-zymes involved in collagen biosynthesis have been documented in several autoso-mal-recessive forms of EDS. Homozygous mutations in PLOD1 (procollagen-lysine,2-oxoglutarate 5-dioxygenase or lysyl-hydroxylase-1) are found in patients with thekyphoscoliotic type of EDS. Lysyl hydroxylase-1 is required for the hydroxylation ofspecific lysine residues to hydroxylysines, which act as precursors for the cross-linking
process that is essential for the tensile strength of collagen. A deficient activity of pro-collagen-N-proteinase due to mutations in the ADAMTS-2 gene encoding this enzymeis responsible for the dermatosparaxis type of EDS.23,24
With the recent identification of new EDS subtypes and the elucidation of their un-derlying molecular defects, it becomes clear that the Villefranche nosology needs up-dating. Table 2 gives a summary of current knowledge on the clinical characteristics ofthe different EDS variants, their inheritance patterns, their underlying genetic defects,and appropriate genetic tests.
The role of other genes in the pathogenesis of EDS
Various members of an expanding family of secreted proteoglycans, the small leucine-rich proteoglycans (SLRPs), have been shown to interact directly with fibrillar collagens,thereby modulating fibril formation, growth and morphology in vitro. Their importancein regulating fibrillogenesis has become clear from studies of SLRP-deficient mice, someof which have clinical and ultrastructural features resembling human EDS.2528 OnlyDCN, the gene encoding decorin, has been linked to a human disorder, congenitalstromal dystrophy of the cornea, although no signs of generalized connective tissuefragility were observed in affected individuals.29,30
Guidelines for management
No causal therapy is available for EDS; however, a series of preventive guidelines areapplicable to all forms of EDS. These guidelines, although not evaluated in large series
Ehlers-Danlos syndromes and Marfan syndrome 175
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
12/25
of patients with EDS, are based on common sense and clinical experience, and are gen-erally promoted by experts in the field of EDS.
Children with pronounced skin fragility should wear protective pads or bandagesover the forehead, knees and shins in order to avoid skin lacerations. Dermal woundsshould be closed without tension, preferably in two layers. Deep stitches should beapplied generously. Cutaneous stitches should be left in place twice as long as usual,
and additional fixation of adjacent skin with adhesive tape can help to prevent stretch-ing of the scar.
Patients with pronounced bruising are advised to avoid contact sports and heavyexercise. Protective pads and bandages can also be useful in the prevention of bruisesand haematomas. Supplementation of ascorbic acid, a cofactor for cross-linking of col-lagen fibrils, can ameliorate the tendency towards bruising in some patients.
In children with hypotonia and delayed motor development, a physiotherapeuticprogramme is important. Non-weight-bearing muscular exercise, such as swimming,is useful to promote muscular development and coordination. Sports with heavy jointstrain, such as contact sports, are discouraged. Anti-inflammatory drugs may relieve
joint pain; however, it is wise to refrain from drugs that interfere with platelet function,such as anti-inflammatory drugs and acetylsalicylic acid, in patients with pronouncedbruising. In these instances, the use of paracetamol is preferred.1
Patients with mitral valve prolapse and regurgitation require antibiotic prophylaxisfor bacterial endocarditis. A baseline echocardiogram with aortic diameter measure-ment is recommended before 10 years of age, with follow-up studies timed accordingto whether an abnormal measurement is found.
For the vascular and vascular-like types of EDS, some prophylactic measures are ofparticular importance. Due to the pronounced vascular and tissue fragility, it is pru-dent for individuals with these conditions to avoid contact sports or isometric exer-
cises (weightlifting), and to refrain from drugs that interfere with platelet functionand anti-coagulation. Invasive vascular procedures such as arteriography and catheter-ization should also be avoided because of the risk for life-threatening vascular rup-ture.31,32 Surgical interventions are generally discouraged because of increasedvascular fragility, and conservative therapy is recommended. If surgery is unavoidable,manipulation of vascular and other tissues should be done with extreme care.Although no effective preventive treatment yet exists in vascular EDS, the use ofb-blockers is now under study.
Finally, emotional support and behavioural and psychological therapy can be usefulin all subtypes of EDS in order to facilitate the process of coping with the drawbacks of
the condition. In this respect, joining a patient support group can be beneficial.
MARFAN SYNDROME
Introduction
Over 100 years ago, the French paediatrician Antoine-Bernard Marfan described a 5-year-old girl, Gabrielle, with long slender digits, long bone overgrowth and musclehypoplasia.33 Since then, clinical research has further delineated this condition and iden-
tified it as a systemic disorder of the connective tissue, with severe manifestations inthe cardiovascular, ocular and skeletal system impelling a multidisciplinary approachfor both diagnosis and management. Since the identification of FBN1 as the causalgene, ongoing research is unravelling the pathophysiology underlying the pleiotropic
176 B. Callewaert et al
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
13/25
manifestations observed in MFS. Recent insights in the pathogenesis have changed theprevailing concept of this type 1 fibrillinopathy as a structural disorder of the connectivetissue into a developmental abnormality manifesting perturbed cytokine signalling, andopening new and unexpected targets for drug treatments.
Epidemiology and criteria for diagnosis
MFS occurs worldwide with an estimated incidence of one in 5000, affecting bothsexes equally.34 The disease demonstrates autosomal-dominant inheritance withhigh penetrance and marked inter- and intrafamilial variability. MFS is caused by muta-tions in the FBN1 gene, encoding an important extracellular matrix protein, fibrillin-1.The clinical and molecular diagnosis of MFS can be hampered by several factors. First,MFS is a clinically evolving phenotype that is not always easily recognizable at a youngage, especially in the absence of a familial history. Second, although the major symp-toms comprise the ocular and cardiovascular system, the diagnosis is often triggered
by skeletal involvement that, at the mild end of the spectrum, overlaps with normalvariation. Third, although most, if not all, patients harbour mutations in the FBN1gene, a diagnostic molecular test is neither commonly nor rapidly available.
In 1986, a first set of clinical criteria was defined by expert opinion in the Berlinnosology.2 With the discovery of the molecular basis of MFS in 1991 identifyingFBN1 mutations as the underlying cause of the disease35, it became clear that morestringent criteria were needed to avoid the danger of overdiagnosis. In 1996, theseshortcomings were addressed in the revised Ghent nosology, which also acknowl-edged the contribution of molecular analysis to the diagnosis.36 In the Ghent nosology,major and minor criteria in the skeletal, ocular, cardiovascular, dural, integument and
pulmonary systems have been defined. The major manifestations include a combinationof four out of eight major skeletal features, ectopia lentis, aortic root dilatation/dissec-tion, dural ectasia and a positive familial history and/or presence of an FBN1 mutation.The diagnosis of MFS in a sporadic patient requires major involvement of at least twodifferent organ systems and minor involvement of a third system. In the presence of anFBN1 mutation known to cause MFS or a positive familial history, one major and oneminor system involvement is sufficient to make the diagnosis. This nosology stressesthat a family history is only contributory as a major criterion when a first-degree rel-ative is diagnosed independently on the basis of clinical criteria alone. In the absence ofa family history, molecular confirmation of an FBN1 defect also constitutes a major
criterion.The Ghent criteria have proven to work well, and with improving techniques, mo-
lecular confirmation of the diagnosis is possible in over 90% of MFS patients.37 How-ever, these diagnostic criteria define an entity within the wider clinical spectrum oftype 1 fibrillinopathies and, as such, the diagnosis is what we define it to be. Therefore,a few drawbacks should be considered in a new nosology. For example, it is of concernthat in the absence of aortic dilation, patients may carry the diagnosis as a social stigmarestricting their career aspirations and possibilities towards life insurance rather thanas a guarantee for optimal medical care. A new expert panel on Marfan nosology iscurrently addressing this issue by making the criteria more patient centred and evi-
dence based. Although the use of major and minor organ involvement is helpful, severalhinge points within the Ghent nosology have not been validated. Moreover, they do notnecessarily make a fundamental difference in patient management. For example, does thepresence of dural ectasia ever make a difference in the diagnostic decision-making
Ehlers-Danlos syndromes and Marfan syndrome 177
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
14/25
process, and does it carry predictive value towards the development of aortic rootdilatation?
Also, there is a clear need for better definitions of ectopia lentis syndrome, mitralvalve prolapse, myopia, mild non-progressive aortic root dilation, and marfanoid skel-etal and skin features (MASS phenotype), and mitral valve prolapse syndrome. Finally,the criteria should be complemented with management and follow-up guidelines for
patients that do not yet fulfill the diagnostic criteria.Unavoidably, in some cases, FBN1 mutation analysis will remain helpful, especially in
families with marked intrafamilial variability, in children that present with evolvingMarfan phenotypes and in the context of prenatal or pre-implantation diagnosis38, al-though it remains difficult, if not impossible, to predict severity on the basis of a mu-tation alone. Since mutation screening is expensive, time consuming and hasincomplete mutation detection rates, advantages and disadvantages have to be consid-ered for each patient.
Clinical characteristics
Skeletal system
Long bone overgrowth contributes to the most striking observations in MFS, leadingto disproportionately long limbs and anterior chest deformities due to rib overgrowth.Other major manifestations include arachnodactyly, elbow contractures, scoliosis orspondylolisthesis, protrusio acetabulae (detected by x-ray) and calcaneal displacementresulting in pes planus with hindfoot valgus. Arachnodactyly is often a subjective findingbut requires the thumb sign (when the fully adducted thumb extends beyond the ulnarborder of the palm) and wrist sign (when the distal phalanges of the thumb and fifth
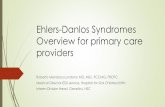
finger fully overlap when grasping the contralateral wrist). Patients may present withtypical facial characteristics including downslanting palpebral fissures, enophthalmia,retrognathia and a high arched palate with tooth crowding. Joint hypermobility maypredispose to ligamentous injury, dislocations, chronic joint pain and premature ar-throsis. Other troublesome locomotor symptoms include muscle hypoplasia and my-algia, resulting in fatigue and spinal pain. These symptoms increase with age and affectup to 98% of adult patients.39 It has been suggested that MFS patients have more frac-tures due to osteopenia, but this remains to be confirmed (Figure 3).
Ocular system
Ocular lens dislocation of any degree should promptly trigger further assessment forMFS. It occurs in approximately one-half to two-thirds of all patients. Final diagnosis ofectopia lentis can only be made by slit lamp examination. High myopia, retinal detach-ment, cataract or glaucoma occur and may cause significant visual impairment or evenblindness.40
Cardiovascular system
While other systems may be severely impaired in MFS, cardiovascular pathology re-mains the leading cause of mortality and morbidity with aortic root dilatation, dissec-
tion and rupture being life-threatening manifestations. Dilatation is generally greatestat the sinuses of Valsalva. Measurements should be normalized to body surface areaand age.41 Aortic root aneurysms occur in an age-dependent manner with high vari-ability among individuals, prompting life-long follow-up. While in severe cases, the
178 B. Callewaert et al
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
15/25
onset of dilation occurs early in life, some individuals will never need aortic root re-placement. The majority of fatal events associated with untreated MFS occur in earlyadult life. However, timely recognition and appropriate medical and surgical manage-
ment of the disease increased the mean survival age to 72 years.42
The improvedlife expectancy in MFS has revealed that patients are also prone to more distally oc-curring aortic manifestations, especially after aortic root replacement, requiring ap-propriate imaging.43 Pulmonary artery diameters are significantly larger in MFS andmay become apparent before aortic root dilatation, revealing potential diagnosticvalue, especially in children.44
Two-thirds of patients have mitral valve dysfunction, with valve prolapse, insuffi-ciency and calcification often associated with myxomatous valve thickening.45 In con-trast, aortic valve insufficiency usually results from aortic root dilation. At the extremeend of presentation, infants with neonatal MFS manifest severely impaired valve dys-
function, leading to congestive heart failure, pulmonary hypertension and even earlydeath.46
Primary progressive myocardial dysfunction is usually mild, but may be aggravatedby b-adrenergic blockade or valve insufficiency.47
Figure 3. Clinical features in a 12-year-old boy with Marfan syndrome. Note the pectus excavatum and long
bone overgrowth (A); a beginning scoliosis at the onset of growth acceleration (B); and arachnodactyly and
hypermobility of the small joints (C).
Ehlers-Danlos syndromes and Marfan syndrome 179
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
16/25
Dura
Dural ectasia is a common observation, with a prevalence of up to 92% in Marfan pa-tients. It may be detected in young children.48 Unfortunately, many other conditions,including neurofibromatosis, Loeys-Dietz syndrome and EDS, manifest dural ectasia,and its precise specificity and sensitivity is not established. Moreover, it requires spe-
cific imaging of the lumbosacral region, with computed tomography (CT) or magneticresonance imaging (MRI) reducing its accessibility. In some patients, it causes discom-fort as low back pain, headaches and irradiating leg pains.49
Skin/pulmonary system
Due to low specificity, skin and pulmonary involvement are only defined as minor cri-teria. Striae distensae independent of marked weight gain or pregnancy occur in up totwo-thirds of all patients.50 Recurrent inguinal or surgical hernias are common andneed special attention. Pneumothorax, pulmonary emphysema and dysfunction, partly
due to alveolar septation defects, represent rare but disabling manifestations. Restric-tive lung disease may result from severe pectus deformities. In view of the long boneovergrowth, pulmonary function should be normalized to sitting height rather thanbody surface area.51
Differential diagnosis
The differential diagnosis of MFS is extensive, comprising other connective tissue dis-orders and metabolic diseases with skeletal, ocular and/or cardiovascular involvement(Table 3).
Cardiovascular system
As in MFS, thoracic aortic root dilatation (TAA) presenting with no or minor systemicinvolvement is progressive, and the risk for dissection or rupture depends mainly onaortic measurements. Importantly, aortic aneurysms in TAA can also occur distallyfrom the sinuses of Valsalva, requiring imaging of the entire aorta. About 20% of pa-tients with TAA have a positive family history, with predominantly autosomal-domi-nant segregation and decreased penetrance.52 Genetic mapping studies haverevealed large genetic heterogeneity in TAA53,54, and therefore it is not possible to
perform comprehensive genetic screening, mandating follow-up of first-degree familymembers. Occasional FBN1 mutations are identified in patients with TAA who oftenshow limited skeletal and skin involvement. Recently, mutations in TGFb receptor 2(TGFBR2) gene have been implicated as a rare cause (5%) in familial TAA, with morewidespread vascular disease and aneurysms and dissections of the descending aortaand middle-sized arteries.55
Bicuspid aortic valve, the most common cardiac malformation with a prevalence of12% in the general population, is frequently associated with aortic root dilation thatoften occurs above the sinuses of Valsalva. Increasing evidence suggests a common ge-netic defect underlying both the valve abnormalities and the aortic dilatation.56 Coun-
selling in first-degree relatives is complicated by incomplete penetrance of thisdominant condition.
Some EDS (as described above), mainly the vascular and kyphoscoliotic types, mayshow overlap with MFS, but can usually be differentiated on the skin findings.
180 B. Callewaert et al
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
17/25
Loeys-Dietz syndrome is a novel autosomal-dominant aortic aneurysm syndromecharacterized by the triad of hypertelorism, bifid uvula/cleft palate, and arterial tortu-osity with ascending aortic aneurysm/dissection, caused by heterozygous loss-of-func-tion mutations in the TGFBR1 or TGFBR2 gene.57 The main differences with MFS arethe absence of significant long bone overgrowth or lens dislocation, and the presenceof multiple other findings, including craniosynostosis, Chiari malformation, club feet,
patent ductus arteriosus, and aneurysms/dissection throughout the arterial tree. Incontrast to this typical presentation, referred to as Loeys-Dietz syndrome type 1,some patients show less craniofacial abnormalities but prominent skin and joint man-ifestations, more reminiscent of vascular EDS.4 This subset of patients (Loeys-Dietz
Table 3. Conditions to be considered in the differential diagnosis of Marfan syndrome.
Main feature Additional symptoms Think of . Genetic defect
Aortic root
dilation/
dissection
None or minor systemic
involvement
TAA FBN1, TGFBR1/2, other
Patent ductus arteriosus TAA/PDA MYH1, TGFBR1/2Bicuspid aortic valve BAV NOTCH1, KCNJ2, other
Thin skin, atrophic scars,
joint hypermobility
EDSIV - LDS2 COL3A1 - TGFBR1/2
Hypertelorism, bifid uvula,
cleft palate, widespread
arterial involvement
LDS1 TGFBR1/2
Ectopia lentis Stocky stature, brachydactyly WMS ADAMTS10 (AR)/FBN1 (AD)
Mental retardation,
marfanoid habitus
Homocystinuria Cystathionine beta-synthase
None or mild systemic
features
Familial EL FBN1, other
Marfanoid
habitus
Mitral valve prolapse,
stable and mild (
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
18/25
syndrome type 2) is characterized by a velvety and translucent skin, easy bruising,widened atrophic scars, uterine rupture, severe peripartal bleedings, and arterial aneu-rysm/dissections throughout the arterial circulation. Importantly, the natural history ofpatients with TGFBR1/2 mutations is far more aggressive than in MFS or even vascularEDS, with a mean age at death of 26.1 years. Aortic dissections occur in young child-hood and/or at smaller aortic dimensions (
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
19/25
Molecular pathogenesis
Fibrillin 1, the protein mutated in MFS, is a 350-kDa extracellular glycoprotein that ishighly conserved between different species. Most mutations affect predictably spacedcysteine residues in the calcium binding epidermal growth factor-like domains neededfor proper folding and stabilization of the protein. Fibrillins polymerize extracellularlyas parallel bundles of head-to-tail monomers, and form macro-aggregates, calledmicrofibrils, in association with other proteins such as latent TGFb binding proteins.Microfibrils provide force-bearing structural support and can associate with elastin toform elastic fibres providing elasticity in a time- and tissue-dependent manner.68 Fora long time, it was believed that the pathophysiology of MFS was entirely based onseverely reduced and fragmented elastic fibres in affected tissues. This observationled to the hypothesis that structural deficiency of the fibrillin-1 protein was themost important factor in the aetiology of MFS. While this hypothesis offered an ex-planation for aortic pathology, it did not reconcile the observation of other clinicalfeatures such as long bone overgrowth, thickening of the cardiac valves or musclehypoplasia.
The study of fibrillin-1 mutant mouse lines that recapitulate human MFS hasrecently challenged this mechanistic view. Indeed, mouse models have shown thatstructural fibrillin-1 deficiency leads to increased activation of the sequestered cyto-kine, TGFb69,70, which has a pivotal role in development and maintenance of severaltissues. Enhanced activation of the TGFb pathway was shown to contribute to thedevelopment of emphysema, aortic aneurysms and muscle hypoplasia seen in MFS.In murine models, these changes can be effectively blocked by the administration ofTGFb antibodies.69,71,72
Further evidence of perturbed TGFb signalling in aortic aneurysm came from the
identification of the Loeys-Dietz syndrome, caused by loss-of-function mutations inthe TGFBR1 and TGFBR2 genes.57
Guidelines for management
Diagnosis and management require a multidisciplinary approach by geneticists, cardi-ologists, orthopaedic surgeons and ophthalmologists with experience in this field.73
Cardiovascular follow-up should include serial evaluation with echocardiography orCT/MRI angiography when visibility of the aortic root and ascending aorta is limited.43
Evaluation frequency should be tailored based upon aortic dimensions, the rate of aor-tic growth and family history. Beta-adrenergic blockade, titrated to physiological re-sponse, is a standard treatment to slow aortic growth, mainly by virtue of itsantihypertensive and negative inotropic effects.74 If beta-blockade is contra-indicated(asthma, Raynaud phenomenon, psoriasis, depression, fatigue), calcium antagonistsor angiotensin converting enzyme inhibitors may be used although no randomizedstudies exist. Surgical repair of the aorta is indicated once the maximal diameter ex-ceeds 5 cm in adults, when the rate of aortic growth exceeds >0.510 mm/year or inthe presence of significant aortic regurgitation. In case of proper aortic valve function,the preferred technique is the valve-sparing procedure avoiding lifelong anticoagulant
therapy, especially in females in their fertile period. Although the superiority ofthis technique in comparison with the composite graft has not been established, the10-year experience is very promising.75 After surgical repair of the aortic root, imagingof the whole aorta is warranted for timely detection of aortic graft pseudo-aneurysms,
Ehlers-Danlos syndromes and Marfan syndrome 183
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
20/25
more distally occurring aneurysms and coronary artery aneurysms.73 While most TAApatients may benefit from the same cardiovascular management guidelines as in MFS,recent studies warned about the aggressive nature of the disease in patients harbour-ing TGFb receptor mutations warranting earlier surgical repair and more extensiveimaging.4
During pregnancy, the risk for aortic complications increases with aortic root
dimensions before pregnancy, but is regarded to be low below 4 cm.73 Therefore,pregnancy should be followed intensively, with special care peripartum, througha high-risk obstetric clinic.
Orthopaedic complications mainly involve anterior chest and vertebral columndeformities that should be followed carefully, especially during and just after puberty.Since extreme pectus deformities have little impact on pulmonary function, surgery isconsidered as a cosmetic issue. Correction, preferably using the minimal invasive Nussprocedure, should not be done before the age of 11 years76, as earlier interventionmight lead to recurrent deformity due to continued rib growth. In contrast, severe(kypho-)scoliosis has a major impact on quality of life, needing surgical stabilization
as bracing often remains inadequate.77 Protrusio acetabulae is often asymptomaticin young adults, and the benefit of surgery is questioned.78 Hormone therapy isindicated if predicted final height is unacceptable.79
Diffraction anomalies due to lens subluxation, flat cornea or myopia can easily becorrected by eyeglasses or contact lenses. Lens extraction for manifest ectopia lentisor cataract severely increases the pre-existing risk for retinal detachment and glau-coma which causes significant visual impairment. Yearly examination by an experiencedophthalmologist is highly recommended for every Marfan patient.
Finally, lifestyle modifications may promote cardiovascular and psychosocial health,and prevent or relieve many locomotor inconveniences including arthrosis, fatigue,
myalgia and chronic joint pains. Patients should avoid competitive sport, straining orisometric exercise as these increase blood pressure and cause considerable dynamicstress on the aortic root. Additionally, contact sports should be avoided as thesemay precipitate aortic dissection.80 Activity guidelines are available on the NationalMarfan Foundation website (http://www.marfan.org/).
New therapeutic strategies, based upon the physiopathology in MFS, proposelosartan as an antihypertensive agent attenuating TGFb signalling. In murine models,losartan has been shown to stop aortic growth and induce regression of emphysema-tous changes in the lung, even in adult life.69,72 Currently ongoing randomized trials arefocusing on this new treatment possibility in MFS, which may also be beneficial in
related conditions.71
This beautifully illustrates how insights gained in the pathophys-iology of monogenic multisystem connective tissue disorders may lead to insights andnew treatment options for other, more common disorders.
Practice points
diagnosis of EDS is based on a combination of clinical, biochemical and ultra-structural examinations that guide molecular analysis of relevant gene(s)
in case of suspicion of vascular EDS, biochemical analysis of type III collagen
extracted from cultured skin fibroblasts is mandatory to confirm the diagnosis phenotypic overlap exists between different EDS subtypes; some form a pheno-
typic continuum
184 B. Callewaert et al
http://www.marfan.org/http://www.marfan.org/ -
7/30/2019 Sindrome Msrfan y Ehlers Danlos
21/25
ACKNOWLEDGEMENTS
The authors are indebted to Paul Coucke and Sofie Symoens for supervision of themolecular and biochemical analyses, and to Petra Van Acker and Karen Wettinck
for technical assistance. This work is supported by Grant G.0171.05 and GrantG.0094.06 from the fund for Scientific Research-Flanders (to ADP), a GOA ResearchGrant from the Ghent University (to ADP) and by the Geneskin Consortium withinthe Sixth Framework Programme of the European Commission.
several unclassified EDS phenotypes confirm wide clinical and genetic hetero-geneity within the EDS spectrum
while aortic and ocular involvement are usually the most disabling and life-threatening manifestations of MFS, the diagnosis is often triggered by skeletalabnormalities that merge with the normal population in the mild end of thespectrum
multisystem manifestations in MFS require a multidisciplinary approach fordiagnosis and management
the diagnosis of MFS still tends to stigmatize patients, and careful considerationis needed in the absence of (a familial history) aortic root dilation. Neverthe-less, aortic follow-up is always strongly advised
management guidelines in MFS are mainly based on expert opinion, and expe-rience is needed to tailor these recommendations to the individual patient
Research topics
in the classic and hypermobility types of EDS, further studies are needed to elu-cidate the underlying molecular mechanisms. The search for genetic causes ofEDS should extend beyond fibrillar collagens to other molecules that areinvolved in regulation and modulation of type I collagen fibrillogenesis
many EDS variants cannot be classified into one of the existing categories. Bet-ter insight into their phenotype, natural history and the underlying biochemical
and genetic defects will improve early recognition and diagnosis, lead to a morelogical classification and hopefully allow development of more effectivetherapies
the recent progress in identification of new molecular defects and recognitionof new EDS variants necessitates an update of the Villefranche nosology
the promising results seen in murine models for MFS treated with losartanshould be confirmed in humans with randomized clinical trials to documentcarefully the benefits and side-effects in MFS patients. These results can serveas a basic document to engage in further trials
re-evaluation of the Ghent criteria is needed after 10 years of experience in
order to define which criteria have worked well and which criteria need fur-ther evidence-based foundation
Ehlers-Danlos syndromes and Marfan syndrome 185
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
22/25
REFERENCES
1. Steinmann B, Royce P & Superti-Furga A. The Ehlers-Danlos syndrome. In Royce P & Steinmann B (eds).
Connective Tissue and its Heritable Disorders. 2nd edn. New York: Wiley-Liss, Inc., 2002, pp. 431523.
2. Beighton P, de Paepe A, Danks D et al. International nosology of heritable disorders of connective tis-
sue, Berlin, 1986. American Journal of Medical Genetics 1988; 29: 581594.
*3. Beighton P, De Paepe A, Steinmann B et al. Ehlers-Danlos syndromes: revised nosology, Villefranche,1997. Ehlers-Danlos National Foundation (USA) and Ehlers-Danlos Support Group (UK). American
Journal of Medical Genetics 1998; 77: 3137.
*4. Loeys BL, Schwarze U, Holm T et al. Aneurysm syndromes caused by mutations in the TGF-beta
receptor. New England Journal of Medicine 2006; 355: 788798.
5. Kaler SG, Gallo LK, Proud VK et al. Occipital horn syndrome and a mild Menkes phenotype associated
with splice site mutations at the MNK locus. Nature Genetics 1994; 8: 195202.
6. Mercuri E, Lampe A, Straub V et al. Congenital muscular dystrophy with short stature, proximal
contractures and distal laxity. Neuropediatrics 2004; 35: 224229.
7. Camacho Vanegas O, Bertini E, Zhang RZ et al. Ullrich scleroatonic muscular dystrophy is caused by
recessive mutations in collagen type VI. Proceedings of the National Academy of Sciences of the United
States of America 2001; 98: 75167521.8. Pan TC, Zhang RZ, Sudano DG et al. New molecular mechanism for Ullrich congenital muscular
dystrophy: a heterozygous in-frame deletion in the COL6A1 gene causes a severe phenotype. American
Journal of Human Genetics 2003; 73: 355369.
9. Baker NL, Morgelin M, Peat R et al. Dominant collagen VI mutations are a common cause of Ullrich
congenital muscular dystrophy. Human Molecular Genetics 2005; 14: 279293.
*10. Malfait F, Coucke P, Symoens S et al. The molecular basis of classic Ehlers-Danlos syndrome: a comprehensive
study of biochemical and molecular findings in 48 unrelated patients. Human Mutation 2005; 25: 2837.
11. Schalkwijk J, Zweers MC, Steijlen PM et al. A recessive form of the Ehlers-Danlos syndrome caused by
tenascin-X deficiency. New England Journal of Medicine 2001; 345: 11671175.
12. Greenspan DS, Northrup H, Au KS et al. COL5A1: fine genetic mapping and exclusion as candidate
gene in families with nail-patella syndrome, tuberous sclerosis 1, hereditary hemorrhagic telangiectasia,and Ehlers-Danlos Syndrome type II. Genomics 1995; 25: 737739.
13. Wenstrup RJ, Langland GT, Willing MC et al. A splice-junction mutation in the region of COL5A1 that
codes for the carboxyl propeptide of pro alpha 1(V) chains results in the gravis form of the Ehlers-
Danlos syndrome (type I). Human Molecular Genetics 1996; 5: 17331736.
14. Hata R, Kurata S & Shinkai H. Existence of malfunctioning pro alpha2(I) collagen genes in a patient with
a pro alpha 2(I)-chain-defective variant of Ehlers-Danlos syndrome. European Journal of Biochemistry
1988; 174: 231237.
15. Sasaki T, Arai K, Ono M et al. Ehlers-Danlos syndrome. A variant characterized by the deficiency of pro
alpha 2 chain of type I procollagen. Archives of Dermatology 1987; 123: 7679.
16. Schwarze U, Hata R, McKusick VA et al. Rare autosomal recessive cardiac valvular form of Ehlers-
Danlos syndrome results from mutations in the COL1A2 gene that activate the nonsense-mediatedRNA decay pathway. American Journal of Human Genetics 2004; 74: 917930.
17. Nuytinck L, Freund M, Lagae L et al. Classical Ehlers-Danlos syndrome caused by a mutation in type I
collagen. American Journal of Human Genetics 2000; 66: 13981402.
*18. Malfait F, Symoens S, De Backer J et al. Three arginine to cysteine substitutions in the pro-alpha (I)-
collagen chain cause Ehlers-Danlos syndrome with a propensity to arterial rupture in early adulthood.
Human Mutation 2007; 28: 387395.
19. Zweers MC, Bristow J, Steijlen PM et al. Haploinsufficiency of TNXB is associated with hypermobility
type of Ehlers-Danlos syndrome. American Journal of Human Genetics 2003; 73: 214217.
20. Schwarze U, Schievink WI, Petty E et al. Haploinsufficiency for one COL3A1 allele of type III procolla-
gen results in a phenotype similar to the vascular form of Ehlers-Danlos syndrome, Ehlers-Danlos
syndrome type IV. American Journal of Human Genetics 2001; 69: 9891001.21. Cabral WA, Makareeva E, Colige A et al. Mutations near amino end of alpha 1(I) collagen cause
combined OI/EDS by interference with N-propeptide processing. Journal of Biological Chemistry 2005;
280: 1925919269.
186 B. Callewaert et al
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
23/25
22. Makareeva E, Cabral WA, Marini JC & Leikin S. Molecular mechanism of alpha 1(I)-osteogenesis imper-
fecta/Ehlers-Danlos syndrome: unfolding of an N-anchor domain at the N-terminal end of the type I
collagen triple helix. Journal of Biological Chemistry 2006; 281: 64636470.
23. Colige A, Sieron AL, Li SW et al. Human Ehlers-Danlos syndrome type VII C and bovine dermatospar-
axis are caused by mutations in the procollagen I N-proteinase gene. American Journal of Human Genetics
1999; 65: 308317.
24. Colige A, Nuytinck L, Hausser I et al. Novel types of mutation responsible for the dermatosparactictype of Ehlers-Danlos syndrome (type VIIC) and common polymorphisms in the ADAMTS2 gene. Jour-
nal of Investigative Dermatology 2004; 123: 656663.
25. Danielson KG, Baribault H, Holmes DF et al. Targeted disruption of decorin leads to abnormal collagen
fibril morphology and skin fragility. Journal of Cell Biology 1997; 136: 729743.
26. Chakravarti S, Magnuson T, Lass JH et al. Lumican regulates collagen fibril assembly: skin fragility and
corneal opacity in the absence of lumican. Journal of Cell Biology 1998; 141: 12771286.
27. Takeda U, Utani A, Wu J et al. Targeted disruption of dermatopontin causes abnormal collagen fibrillo-
genesis. Journal of Investigative Dermatology 2002; 119: 678683.
28. Tasheva ES, Koester A, Paulsen AQ et al. Mimecan/osteoglycin-deficient mice have collagen fibril abnor-
malities. Molecular Vision 2002; 8: 407415.
29. Bredrup C, Knappskog PM, Majewski J et al. Congenital stromal dystrophy of the cornea caused by
a mutation in the decorin gene. Investigative Ophthalmology & Visual Science 2005; 46: 420426.
30. Rodahl E, Van Ginderdeuren R, Knappskog PM et al. A second decorin frame shift mutation in a family
with congenital stromal corneal dystrophy. American Journal of Ophthalmology 2006; 142: 520521.
31. Freeman RK, Swegle J & Sise MJ. The surgical complications of Ehlers-Danlos syndrome. American
Surgeon 1996; 62: 869873.
32. Cikrit DF, Miles JH & Silver D. Spontaneous arterial perforation: the Ehlers-Danlos specter. Journal of
Vascular Surgery 1987; 5: 248255.
33. Marfan A. Un cas de deformation congenitale des quatres membres, plus prononcee aux extremites,
caracterisee par lallongement des os avec un certain degre damincissement. Bulletins et memoires de
la Societe medicale des hopitaux de Paris 1886; 13: 220228.
34. Pyeritz R. Marfan syndrome and other disorders of fibrillin. In Rimoin DL, Conner JM & Pyeritz RE (eds).
Principles and Practice of Medical Genetics. 3rd edn. New York: Churchill Livingstone, 1997, pp. 10271066.
35. Dietz HC, Cutting GR, Pyeritz RE et al. Marfan syndrome caused by a recurrent de novo missense
mutation in the fibrillin gene. Nature 1991; 352: 337339.
*36. De Paepe A, Devereux RB, Dietz HC et al. Revised diagnostic criteria for the Marfan syndrome.
American Journal of Medical Genetics 1996; 62: 417426.
*37. Loeys B, De Backer J, Van Acker P et al. Comprehensive molecular screening of the FBN1 gene favors
locus homogeneity of classical Marfan syndrome. Human Mutation 2004; 24: 140146.
38. Loeys B, Nuytinck L, Delvaux I et al. Genotype and phenotype analysis of 171 patients referred for
molecular study of the fibrillin-1 gene FBN1 because of suspected Marfan syndrome. Archives of Internal
Medicine 2001; 161: 24472454.
39. Grahame R & Pyeritz RE. The Marfan syndrome: joint and skin manifestations are prevalent and
correlated. British Journal of Rheumatology 1995; 34: 126131.
40. Maumenee IH. The eye in the Marfan syndrome. Transactions of the American Ophthalmological Society
1981; 79: 684733.
41. Roman MJ, Devereux RB, Kramer-Fox R & OLoughlin J. Two-dimensional echocardiographic aortic
root dimensions in normal children and adults. American Journal of Cardiology 1989; 64: 507512.
42. Silverman DI, Burton KJ, Gray J et al. Life expectancy in the Marfan syndrome. American Journal of
Cardiology 1995; 75: 157160.
43. Milewicz DM, Dietz HC & Miller DC. Treatment of aortic disease in patients with Marfan syndrome.
Circulation 2005; 111: e150e157.
44. De Backer J, Loeys B, Devos D et al. A critical analysis of minor cardiovascular criteria in the diagnostic
evaluation of patients with Marfan syndrome. Genetics in Medicine 2006; 8: 401408.
45. Pyeritz RE & Wappel MA. Mitral valve dysfunction in the Marfan syndrome. Clinical and echocardio-
graphic study of prevalence and natural history. American Journal of Medicine 1983; 74: 797807.
46. Sisk HE, Zahka KG & Pyeritz RE. The Marfan syndrome in early childhood: analysis of 15 patients
diagnosed at less than 4 years of age. American Journal of Cardiology 1983; 52: 353358.
Ehlers-Danlos syndromes and Marfan syndrome 187
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
24/25
47. De Backer JF, Devos D, Segers P et al. Primary impairment of left ventricular function in Marfan
syndrome. International Journal of Cardiology 2006; 112: 353358.
48. Fattori R, Nienaber CA, Descovich B et al. Importance of dural ectasia in phenotypic assessment of
Marfans syndrome. Lancet 1999; 354: 910913.
49. Foran JR, Pyeritz RE, Dietz HC & Sponseller PD. Characterization of the symptoms associated with
dural ectasia in the Marfan patient. American Journal of Medical Genetics 2005; 134: 5865.
50. Cohen PR & Schneiderman P. Clinical manifestations of the Marfan syndrome. International Journal ofDermatology1989; 28: 291299.
51. Streeten EA, Murphy EA & Pyeritz RE. Pulmonary function in the Marfan syndrome. Chest 1987; 91:
408412.
52. Biddinger A, Rocklin M, Coselli J & Milewicz DM. Familial thoracic aortic dilatations and dissections:
a case control study. Journal of Vascular Surgery 1997; 25: 506511.
53. Guo D, Hasham S, Kuang SQ et al. Familial thoracic aortic aneurysms and dissections: genetic
heterogeneity with a major locus mapping to 5q1314. Circulation 2001; 103: 24612468.
54. Vaughan CJ, Casey M, He J et al. Identification of a chromosome 11q23.2q24 locus for familial aortic
aneurysm disease, a genetically heterogeneous disorder. Circulation 2001; 103: 24692475.
55. Pannu H, Fadulu VT, Chang J et al. Mutations in transforming growth factor-beta receptor type II cause
familial thoracic aortic aneurysms and dissections. Circulation 2005; 112: 513520.
56. Braverman AC, Guven H, Beardslee MA et al. The bicuspid aortic valve. Current Problems in Cardiology
2005; 30: 470522.
*57. Loeys BL, Chen J, Neptune ER et al. A syndrome of altered cardiovascular, craniofacial, neurocognitive
and skeletal development caused by mutations in TGFBR1 or TGFBR2. Nature Genetics 2005; 37:
275281.
58. Dagoneau N, Benoist-Lasselin C, Huber C et al. ADAMTS10 mutations in autosomal recessive Weill-
Marchesani syndrome. American Journal of Human Genetics 2004; 75: 801806.
59. Faivre L, Gorlin RJ, Wirtz MK et al. In frame fibrillin-1 gene deletion in autosomal dominant Weill-
Marchesani syndrome. Journal of Medical Genetics 2003; 40: 3436.
60. Lieberman ER, Gomperts ED, Shaw KN et al. Homocystinuria: clinical and pathologic review, with
emphasis on thrombotic features, including pulmonary artery thrombosis. Perspectives in Pediatric
Pathology 1993; 17: 125147.
61. Glesby MJ & Pyeritz RE. Association of mitral valve prolapse and systemic abnormalities of connective
tissue. A phenotypic continuum. Journal of the American Medical Association 1989; 262: 523528.
62. Montgomery RA, Geraghty MT, Bull E et al. Multiple molecular mechanisms underlying subdiagnostic
variants of Marfan syndrome. American Journal of Human Genetics 1998; 63: 17031711.
63. Gupta PA, Wallis DD, Chin TO et al. FBN2 mutation associated with manifestations of Marfan syn-
drome and congenital contractural arachnodactyly. Journal of Medical Genetics 2004; 41: e56.
64. Putnam EA, Zhang H, Ramirez F & Milewicz DM. Fibrillin-2 (FBN2) mutations result in the Marfan-like
disorder, congenital contractural arachnodactyly. Nature Genetics 1995; 11: 456458.
65. Sood S, Eldadah ZA, Krause WL et al. Mutation in fibrillin-1 and the Marfanoid-craniosynostosis
(Shprintzen-Goldberg) syndrome. Nature Genetics 1996; 12: 209211.
66. Raymond FL, Tarpey PS, Edkins S et al. Mutations in ZDHHC9, which encodes a palmitoyltransferase of
NRAS and HRAS, cause X-linked mental retardation associated with a Marfanoid habitus. American
Journal of Human Genetics 2007; 80: 982987.
67. Schwartz CE, Tarpey PS, Lubs HA et al. The original Lujan syndrome family has a novel missense mu-
tation (p.N1007S) in the MED12 gene. Journal of Medical Genetics 2007; 44: 472477.
*68. Robinson PN, Arteaga-Solis E, Baldock C et al. The molecular genetics of Marfan syndrome and related
disorders. Journal of Medical Genetics 2006; 43: 769787.
69. Neptune ER, Frischmeyer PA, Arking DE et al. Dysregulation of TGF-beta activation contributes to
pathogenesis in Marfan syndrome. Nature Genetics 2003; 33: 407411.
70. Pereira L, Andrikopoulos K, Tian J et al. Targetting of the gene encoding fibrillin-1 recapitulates the
vascular aspect of Marfan syndrome. Nature Genetics 1997; 17: 218222.
71. Cohn RD, van Erp C, Habashi JP et al. Angiotensin II type 1 receptor blockade attenuates TGF-beta-
induced failure of muscle regeneration in multiple myopathic states. Nature Medicine 2007; 13: 204210.
*72. Habashi JP, Judge DP, Holm TM et al. Losartan, an AT1 antagonist, prevents aortic aneurysm in a mouse
model of Marfan syndrome. Science 2006; 312: 117121.
188 B. Callewaert et al
-
7/30/2019 Sindrome Msrfan y Ehlers Danlos
25/25
73. Ades L. Guidelines for the diagnosis and management of Marfan syndrome. Heart, Lung and Circulation
2007; 16: 2830.
*74. Shores J, Berger KR, Murphy EA & Pyeritz RE. Progression of aortic dilatation and the benefit of
long-term beta-adrenergic blockade in Marfans syndrome. New England Journal of Medicine 1994;
330: 13351341.
75. Kallenbach K, Baraki H, Khaladj N et al. Aortic valve-sparing operation in Marfan syndrome: what do
we know after a decade? Annals of Thoracic Surgery 2007; 83: S764S768. discussion S85S90.76. Lawson ML, Mellins RB, Tabangin M et al. Impact of pectus excavatum on pulmonary function before
and after repair with the Nuss procedure. Journal of Pediatric Surgery 2005; 40: 174180.
77. Jones KB, Erkula G, Sponseller PD & Dormans JP. Spine deformity correction in Marfan syndrome. Spine
2002; 27: 20032012.
78. Giampietro PF, Raggio C & Davis JG. Marfan syndrome: orthopedic and genetic review. Current Opinion
in Pediatrics 2002; 14: 3541.
79. Knudtzon J & Aarskog D. Estrogen treatment of excessively tall girls with Marfan syndrome. Acta
Paediatrica Scandinavica 1988; 77: 537541.
80. Braverman AC. Exercise and the Marfan syndrome. Medicine and Science in Sports and Exercise 1998; 30:
S387S395.
Ehlers-Danlos syndromes and Marfan syndrome 189