
Significance of Chronic Sinus Bradyeardia in Elderly...
8
Significance of Chronic Sinus Bradyeardia in Elderly People By NEIL S. AGRUSS, M.D., ELAINE Y. RosIN, M.D., ROBERT J. ADOLPH, M.D., AND NOBLE 0. FOWLER, M.D. SUMMARY It may be difficult to evaluate sinus bradyeardia in the elderly since sinus rates below 50 beats/min may occur normally with aging. Seven asymptomatic bradyeardic subjects (heart rates 41-51 beats/min), ages 67-79 years, with no evidence of impaired cardiac performance and taking no drugs, were compared with four age-matched con- trols (heart rates 60-84 beats/min). Autonomic function was tested with the Valsalva maneuver, amyl nitrite inhalation, methoxamine infusion, head-up tilt, and atropine intravenously (2 mg). Cardiac index at rest was normal in bradyeardic subjects (2.4 0.1 SEM); in- creased cardiac stroke volume (SV) compensated for the slow heart rate. With supine bicycle exercise, increase in cardiac output per 100 ml increase in oxygen consumption was normal in bradyeardics (885 + 60 ml compared to 907 171 ml in controls). This exercise response was achieved mainly by increased SV in bradyeardics and by increased heart rate in controls. Significant increases in cardiac output occurred with both atropine and atrial pacing in bradyeardics, but not in controls. Autonomic im- pairment was not found. Increased vagal tone in bradyeardics was suggested by a lesser heart rate response to exercise and passive tilting. Hence, a heart rate below 50 beats/min in elderly people does not necessarily in- dicate depressed cardiac performance. Further evaluation of the significance of brady- cardia in these subjects requires long-term observation. Additional Indexing Words: Heart rate Cardiac output Response to atrial pacing RE Response to atropine S INUS bradyeardia in the adult may be defined as a heart rate below 60 beats/ min with a normal sequence of cardiac activation. Recent reports have emphasized chronic sinoatrial bradyeardia as a cause of From the Division of Cardiology, Department of Medicine, University of Cincinnati College of Medi- cine, Cincinnati General Hospital, Cincinnati, Ohio 45229. Supported in part by the National Institute of Health Grants HE-06307 and HE-5445, and the Heart Association of Southwestern Ohio. Address for reprints: Neil S. Agruss, M.D., Cardiac Research Laboratory, H/3, Cincinnati General Hos- pital, Cincinnati, Ohio 45229. Received: March 2, 1972; revision accepted for publication May 31, 1972. Autonomic function Exercise response 'esponse to passive head-up tilt cerebral dysfunction, syncope, and other symptoms of diminished cardiac output or regional blood flow.'-6 Most patients reported L have been over 50-60 years of age, with resting heart rates near 40-50 beats/min. Associated cardiac rhythm and AV conduction distur- bances have been frequent. Without these a decision as to whether or not sinus bradyear- dia causes symptoms may be difficult, since dizziness, fatigue, weakness, exertional dysp- nea and syncope can result from a variety of noncardiac disorders in the elderly, and the resting heart rate tends to diminish with age.7 This paper reports hemodynamic data obtained from seven elderly asymptomatic bradyeardic subjects during supine rest Circulation, Volume XLVI, November 1972 924 by guest on May 22, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Significance of Chronic Sinus Bradyeardia in Elderly...

Significance of Chronic Sinus Bradyeardiain Elderly People
By NEIL S. AGRUSS, M.D., ELAINE Y. RosIN, M.D., ROBERT J. ADOLPH, M.D.,AND NOBLE 0. FOWLER, M.D.
SUMMARYIt may be difficult to evaluate sinus bradyeardia in the elderly since sinus rates
below 50 beats/min may occur normally with aging. Seven asymptomatic bradyeardicsubjects (heart rates 41-51 beats/min), ages 67-79 years, with no evidence of impairedcardiac performance and taking no drugs, were compared with four age-matched con-trols (heart rates 60-84 beats/min). Autonomic function was tested with the Valsalvamaneuver, amyl nitrite inhalation, methoxamine infusion, head-up tilt, and atropineintravenously (2 mg).
Cardiac index at rest was normal in bradyeardic subjects (2.4 0.1 SEM); in-creased cardiac stroke volume (SV) compensated for the slow heart rate. With supinebicycle exercise, increase in cardiac output per 100 ml increase in oxygen consumptionwas normal in bradyeardics (885 + 60 ml compared to 907 171 ml in controls).This exercise response was achieved mainly by increased SV in bradyeardics and byincreased heart rate in controls. Significant increases in cardiac output occurred withboth atropine and atrial pacing in bradyeardics, but not in controls. Autonomic im-pairment was not found. Increased vagal tone in bradyeardics was suggested by alesser heart rate response to exercise and passive tilting.
Hence, a heart rate below 50 beats/min in elderly people does not necessarily in-dicate depressed cardiac performance. Further evaluation of the significance of brady-cardia in these subjects requires long-term observation.
Additional Indexing Words:Heart rate Cardiac outputResponse to atrial pacing REResponse to atropine
S INUS bradyeardia in the adult may bedefined as a heart rate below 60 beats/
min with a normal sequence of cardiacactivation. Recent reports have emphasizedchronic sinoatrial bradyeardia as a cause of
From the Division of Cardiology, Department ofMedicine, University of Cincinnati College of Medi-cine, Cincinnati General Hospital, Cincinnati, Ohio45229.
Supported in part by the National Institute ofHealth Grants HE-06307 and HE-5445, and the HeartAssociation of Southwestern Ohio.
Address for reprints: Neil S. Agruss, M.D., CardiacResearch Laboratory, H/3, Cincinnati General Hos-pital, Cincinnati, Ohio 45229.
Received: March 2, 1972; revision accepted forpublication May 31, 1972.
Autonomic function Exercise response'esponse to passive head-up tilt
cerebral dysfunction, syncope, and othersymptoms of diminished cardiac output orregional blood flow.'-6 Most patients reported
L have been over 50-60 years of age, with restingheart rates near 40-50 beats/min. Associatedcardiac rhythm and AV conduction distur-bances have been frequent. Without these adecision as to whether or not sinus bradyear-dia causes symptoms may be difficult, sincedizziness, fatigue, weakness, exertional dysp-nea and syncope can result from a variety ofnoncardiac disorders in the elderly, and theresting heart rate tends to diminish withage.7
This paper reports hemodynamic dataobtained from seven elderly asymptomaticbradyeardic subjects during supine rest
Circulation, Volume XLVI, November 1972924
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

SINUS BRADYCARDIA IN THE ELDERLY
supine bicycle exercise, and during sustainedincrease of the heart rate by atrial pacing.Autonomic nerve function was evaluated fromthe response of the heart rate and bloodpressure to head-up tilt, Valsalva maneuver,amyl nitrite inhalation, intravenous methoxa-mine, and a 2.0 mg intravenous dose ofatropine. The data were compared to thoseobtained from a group of age-matched con-trols.
MethodsThe bradycardic subjects were seven men, ages
67-79 years, with resting heart rates between 41and 51 beats/min. Each had chronic sinusbradyeardia as determined from two or moreelectrocardiograms recorded over a 6-month, orlonger period of time. Additional electrocardio-graphic findings were: first degree AV block intwo subjects (PR interval-0.24 sec in each);first degree AV block (PR interval 0.48 sec) andleft anterior hemiblock in one subject; intermit-tent RBBB (unrelated to heart rate) in onesubject; and possible left ventricular hypertrophy(voltage criteria only) in one subject. No subjectat any time had electrocardiographic evidence ofan atrial or ventricular tachyarrhythmia, SAblock, sinus arrest, AV junctional rhythm, orsecond or third degree AV block. All sevensubjects were asymptomatic and had no history ofheart disease or hypertension; none was takingmedication. No subject had athletic training orwas engaged in a prescribed exercise program.Chest roentgenograms were normal in eachsubject, and none had clinical or laboratoryevidence of impaired cardiac reserve, hypothy-roidism, diabetes, chronic renal disease, neurolog-ic disease, malignancy, hyperlipidemia, anemia,or electrolyte disturbance. Four healthy subjects,three men and one woman, ages 61-79 years, withresting heart rates between 60 and 84 beats/min,served as the control group. Each had normalelectrocardiograms and chest X-rays; none wastaking medication. Informed consent was ob-tained from all 11 subjects before the study. Onthe day before study each subject was acquaintedwith the equipment and procedures to beemployed, and trained in the Valsalva maneuver.
All subjects were studied in the postabsorptivestate without receiving premedication. Cardiacoutputs were measured by the dye-dilutiontechnic (indocyanine green). Methods for deter-mining heart rate, stroke volume, and oxygen
consumption have been previously reported.8Duplicate cardiac output determinations duringrest, head-up tilt, exercise, various rates of atrialpacing, or following atropine agreed within 10%Circulation, Volume XLVI, November 1972
and were averaged. No more than 2 min elapsedbetween duplicate cardiac output determinations.Systemic arterial and right atrial pressures wererecorded on an Electronics-for-Medicine photo-graphic recorder using Statham P23dB pressuretransducers. Gauges were leveled 10 cm abovethe table top for all supine studies, and at thelevel of the midright atrium, as determinedfluoroscopically, during head-up tilt. A bipolarelectrode catheter* was used for pacing the rightatrium.
Following placement of all catheters the restingcardiac output (CO), heart rate (1HR1), andbrachial artery (BA) pressure were measured.The HR and BA pressure xvere then continuouslyrecorded during the Valsalva maneuver,9 duringinhalation of amyl nitrite, and following a 2-minintravenous infusion of methoxamine, 0.06 mg/kg. The subject was then tilted head-up to a 450angle with the horizontal. CO, HR, and BApressure measurements were made after 3 min oftilt. Following return to the horizontal positionand after a 10-min rest, the atrial rate was slowlyincreased by atrial pacing. After at least 5 minhad elapsed at pacing rates of approximately 70and 90 beats/min in the bradycardic subjects,and 90 beats/min in controls, the CO, HR, andBA pressure were measured. The atrial rate wasthen increased by 10 beats/min increments to 150beats/min or until second degree AV block ap-
peared. The postpacing recovery time of thesinus node pacemaker was observed followingsudden cessation of the highest pacing rateattained. The subjects then exercised in thesupine position on a bicycle ergometer, maintain-ing a work rate of 150 kg-meters/min (1200 ftlbs/min). This work level increased oxygen
consumption two and a half to three timescontrol. During the sixth and seventh min ofexercise expired air was collected and CO, HR,and BA pressure were measured. After thesubjects rested 15 min, the circulatory response toexercise at a controlled heart rate was measuredin four of the seven bradyeardic subjects. Theresting HR was increased by atrial pacing to ratesslightly above those attained spontaneously dur-ing exercise; exercise was then performed as
before. The CO, HR, and BA pressure were againmeasured during the seventh minute of exercise.Following a 15-min rest period, each subjectreceived 2.0 mg of atropine intravenously in 2min. Four minutes after the injection CO, HR,and BA pressures were again measured. RestingCO, HR, and BA pressure measurements were
obtained in each subject before head-up tilt,
*NBIH Catheter, U. S. Catheter & InstrumiientCorporation, Clens Falls, New York.
925
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

AGRUSS ET AL.
before atrial pacing and exercise studies, andbefore atropine.
Results
Individual and group mean data for boththe bradyeardic and control subjects areshown in the figures. The mean age and bodysurface area were similar in both groups.Right atrial pressure was normal and notsignificantly different in the two groups at restand during subsequent interventions. Otherthan the HR and stroke index (SI), theresting baseline data for the two groups weresimilar (figs. 1 and 2). The mean heart ratesof the two groups differed significantly (P<0.001). There was no significant difference inmean resting cardiac index (fig. 1). Cardiacindex (CI) was similar to that reported fornormal subjects of similar age.7 10 The differ-ence in SI between the groups was statistical-
PACING
CONTROLS
0
I* 0
1..0
Tl
72±5 88±1(60-84) (86-90)
Beats/MinuteFigure 1
BRADYCARDIGS0@
I, I
0,Ge
I1
0
45±2 83±4
(41- 51) (69-91)
CI values at rest and during atrial pacing are shownfor each control and bradycardic subject ( ).
The mean values are shown by (o) and SEM byvertical bars. The mean resting HR of the controlsubjects was 72 + 5 beats/min (range: 60-84); themean HR during atrial pacing was 88 ±+1 beats/min(range: 86-90). The mean resting HR of the brady-cardic group was 45 + 2 beats/min (range: 41-51);the mean HR during pacing was 83 + 4 beats/mmn(range: 69-91).
ly significant (P < 0.001). Although there wasno significant difference in the mean brachialartery pressure, the pulse pressure, as expect-ed, was greater in the bradyeardic group.Oxygen consumption of the groups weresimilar (fig. 3), and both values were normalfor the age of the subjects.7 10
Atrial pacing was successful in significantlyincreasing the HR in six of seven bradyeardicsubjects. One (C.S.) developed second-degreeAV block at a paced rate of 52 beats/min. Thedifference in mean paced HR between thegroups was not significant. Atrial pacingsignificantly increased the CI of the bradyear-dic group, but not in the controls (fig. 1). Themean paced CI in bradyeardic subjects wasnot significantly different from that of thecontrol group.The response of the HR, CI, and SI to
muscular exercise is summarized in figure 2.The CI rose to similar levels in the twogroups. Although the differences between thegroups for HR and SI were not statisticallysignificant, the bradyeardic subjects tended toachieve a higher stroke output and lower HRduring exercise than did the control subjects,findings similar to those at rest. Oxygenconsumption increased comparably in both
80
70--9
60 8
50 7
N~~~~~~~~~H ( ET4,MI
40 --
----
30 -4
Theresponse of the HR, Sl nd CI to muscular320~~~~~~~~~~~~~~~~~~~~~
40 60 80 100 120 0(HR (BEATS/MIN)
____&d.ycardics
Figure 2
The response of the HR, Si, and CI to muscularexercise is shown in the control (.--- -e) and brady-cardic (.---*) subjects. The SI is plotted on theordinate and the HR on the abscissa; the isoplethsrepresent levels of CI. The closed circle to the leftof each connected pair represents resting values andthe closed circle to the right represents exercise values.
Circulation, Volume XLVI, November 1972
3.0
-3
' 2.5
2t.
2.0
926
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

SINUS BRADYCARDIA IN THE ELDERLY
*- *Bradycardicx-x Control
200 400 600 800 1000vo2 (cc /minute)
Figure 3
The relationship between CO and oxygen consumption (VQ2) at rest and during exercise is
shown for the control (X X) and bradycardic ( ) subjects. The symbols (. or x)on the left represent resting values and those on the right, exercise values. (The slope of eachline is a function of the exercise factor.)
groups during exercise. In addition, theincreases in CO per 100 ml increase in oxygenconsumption (exercise factor) were similar(fig. 3). The bradycardic group had an
exercise factor of 907 171 ml/ 100 ml and thecontrol group, 885 + 60 ml/ 100 ml. Theexercise factors compare closely to thosefound by Granath and associates10 in a group
of normal elderly individuals. Figure 3 showsthe relation of oxygen consumption to cardiacoutput for all subjects.The ability of the heart to increase stroke
volume during exercise while maintainingthe HR constant, at a rate just above thatachieved during the previous exercise period,was evaluated in four bradycardic subjects. Asfigure 4 shows, the increase in CI for each ofthe subjects was similar to that during theCirculation, Volume XLVI, November 1972
preceding exercise period, when HR was notcontrolled, and resulted almost entirely froman increase in stroke volume.With 2.0 mg atropine intravenously, HR
increased significantly in both groups ofsubjects (fig. 5). The bradycardic subjects hada significantly greater absolute and percentageincrease in HR than did the controls(P < 0.05). Bradycardic subjects tended tohave a more limited HR response during ex-
ercise than to atropine when compared to thecontrol subjects.
Following atropine mean CI did not differsignificantly between the two groups (fig. 5).A statistically significant increase in mean CIwas found in the bradycardic group (P <0.001). The difference between the mean
resting CI and postatropine CI in the controlgroup was not significant.
13
11
9
7
5
3
927
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

AGRUSS ET AL.
8Or\ Eae,c,se
-\\ S\\,<-Cs~~~~~~~~~~'I-5 -
- X s W,
30f_
ATROPINE
*\ £EAelcise -Pace
W,H. FH -_
*9 B.G._I
Rest-Pace
60 80 100
HR (BEATS /MIN)
Figure 4
CONTROLS9
8
7 c'9
6 115 -..J
4
3
2
120 140
At the left of the figure the relationship of HR, SI,and CI is shown in four bradycardic subjects at restand during exercise. To the right are plotted the HR,SI, and CI for these same four subjects during atrialpacing, while at rest (Rest-Pace) and while exercising(Exercise-Pace). The solid lines connecting the solidcircles show the change from rest to exercise, andfrom rest-pace to rest-exercise. The straight dashedlines connecting the solid circles show the changefrom rest to rest-pace.
The atrioventricular conduction system was
stressed by atrial pacing. Four bradyeardicsubjects developed second-degree AV block atpaced rates of 105 beats/min or less (105, 100,91 and 52 beats/min, respectively). Thelowest rate at which AV block occurred in thecontrol subjects was 107 beats/min. Followingsudden cessation of pacing, at the highest rateattainable, spontaneous sinoatrial activity re-
turned within 1.1 sec (range 0.6-1.1) in eachsubject. AV junctional rhythm was not seen inany subject following the administration ofatropine.Blood pressure responded normally9' 11 dur-
ing the Valsalva maneuver in all control andbradyeardic subjects. All individuals showed a
narrowing of the pulse pressure during phaseII and an overshoot of the BP during phaseIV. The average percentage increase in HRduring the strain (phase II) was similar inboth groups: 27% for controls and 26% forbradycardic subjects. Slowing of the HRoccurred during phase IV in all subjects, butin the bradyeardic group the rate usually didnot decrease below the control HR. Followingamyl nitrite inhalation or intravenous meth-
6.
'311
3.0
BRADYCARDICS
n
2.5
2.072±5 108±12
(60-84) (90-143)45±2 91±4
(41-51) (70-101)
Beats/ Minute
Figure 5
Cl values at rest and after intravenous administrationof atropine are shown for each control and bradycardicsubject. (- *). The mean values are shownby (o) and SEM by vertical bars. The mean restingand postatropine heart rates for each group are shownat the bottom of the figure. The range of HR isshown in parentheses.
oxamine no significant difference in per centof HR change existed between the groups.
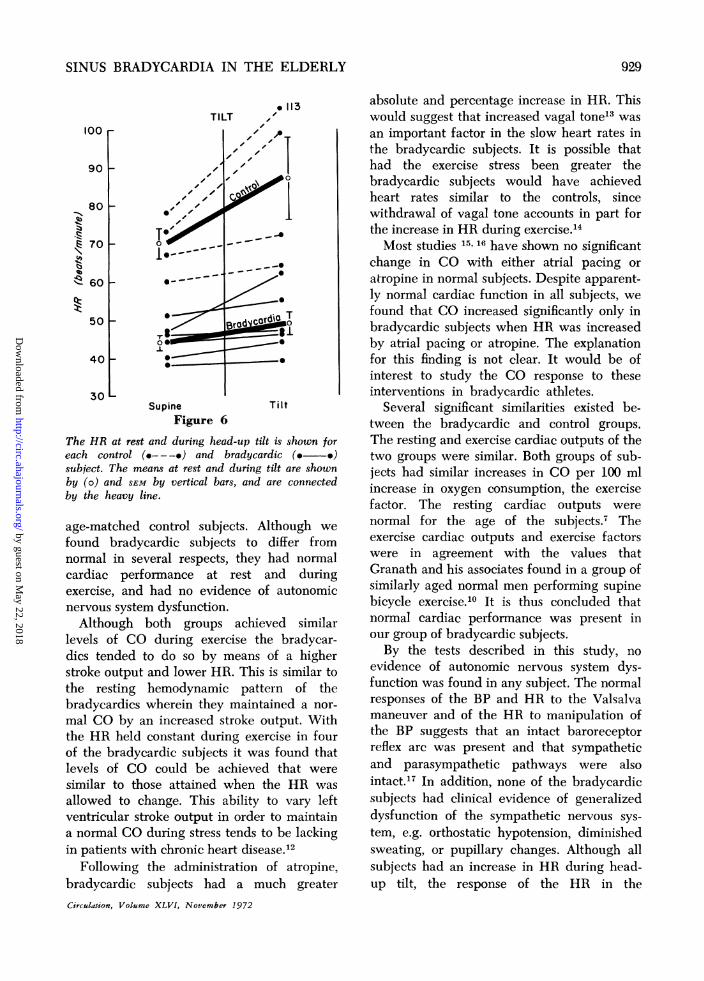
Figure 6 shows the response of the HR tohead-up tilt in both groups of subjects. Thecontrol subjects had a significantly greaterpercentage increase in HR during tilt (24%)than did the bradyeardic subjects (11%). TheCI decreased to similar levels in both groupsduring tilt. In neither group did the mean BApressure change significantly.
Discussion
It is known that the resting HR and COtend to diminish with age,7 but data relatingto the cardiac performance of asymptomaticelderly patients with resting heart rates of40-50 beats/min are lacking. We thereforestudied seven asymptomatic elderly subjectswith sinus bradycardia and compared theircardiac performance with that of a group of
Circulation, Volume XLVI, November 1972
70
60
50
40
20
IV' '-
928
-1
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
SINUS BRADYCARDIA IN THE ELDERLY
TILT100 r
90
80 F
70
60
50
40
30Supine Tilt
Figure 6
The HR at rest and during head-up tilt is shown foreach control (---a-) and bradycardic ( )
subject. The means at rest and during tilt are shownby (o) and SEM by vertical bars, and are connectedby the heavy line.
age-matched control subjects. Although we
found bradyeardic subjects to differ fromnormal in several respects, they had normalcardiac performance at rest and duringexercise, and had no evidence of autonomicnervous system dysfunction.Although both groups achieved similar
levels of CO during exercise the bradyear-dics tended to do so by means of a higherstroke output and lower HR. This is similar tothe resting hemodynamic pattern of thebradyeardics wherein they maintained a nor-
mal CO by an increased stroke output. Withthe HR held constant during exercise in fourof the bradyeardic subjects it was found thatlevels of CO could be achieved that were
similar to those attained when the HR was
allowed to change. This ability to vary leftventricular stroke output in order to maintaina normal CO during stress tends to be lackingin patients with chronic heart disease.'2
Following the administration of atropine,bradyeardic subjects had a much greater
Circulation, Volume XLVI, November 1972
absolute and percentage increase in HR. Thiswould suggest that increased vagal tone13 wasan important factor in the slow heart rates inthe bradyeardic subjects. It is possible thathad the exercise stress been greater thebradycardic subjects would have achievedheart rates similar to the controls, sincewithdrawal of vagal tone accounts in part forthe increase in HR during exercise.14Most studies 15, 16 have shown no signfficant
change in CO with either atrial pacing oratropine in normal subjects. Despite apparent-ly normal cardiac function in all subjects, wefound that CO increased significantly only inbradyeardic subjects when HR was increasedby atrial pacing or atropine. The explanationfor this finding is not clear. It would be ofinterest to study the CO response to theseinterventions in bradyeardic athletes.
Several significant similarities existed be-tween the bradyeardic and control groups.The resting and exercise cardiac outputs of thetwo groups were similar. Both groups of sub-jects had similar increases in CO per 100 mlincrease in oxygen consumption, the exercisefactor. The resting cardiac outputs werenormal for the age of the subjects.7 Theexercise cardiac outputs and exercise factorswere in agreement with the values thatGranath and his associates found in a group ofsimilarly aged normal men performing supinebicycle exercise.10 It is thus concluded thatnormal cardiac performance was present inour group of bradyeardic subjects.By the tests described in this study, no
evidence of autonomic nervous system dys-function was found in any subject. The normalresponses of the BP and HR to the Valsalvamaneuver and of the HR to manipulation ofthe BP suggests that an intact baroreceptorreflex arc was present and that sympatheticand parasympathetic pathways were alsointact.17 In addition, none of the bradyeardicsubjects had clinical evidence of generalizeddysfunction of the sympathetic nervous sys-tem, e.g. orthostatic hypotension, diminishedsweating, or pupillary changes. Although allsubjects had an increase in HR during head-up tilt, the response of the HR in the
929
-1.1qll.14-1.c
tq)11.
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

AGRUSS ET AL.
bradyeardic subjects was significantly lessthan that of the control subjects. A dimin-ished increase in HR during head-up tilt canbe seen in patients who are in congestive heartfailure."' 19 However, none of the bradycardicsubjects had any evidence of impaired cardiacperformance. It is possible that an increasedlevel of vagal tone accounted for the bluntedHR response to tilt in the bradyeardicsubjects.
Although a significant number of ourbradycardic subjects had evidence of impairedAV conduction, this was the only evidencesuggestive of cardiac disease. Unlike thefindings in patients with so called "sick sinusnode" disease, serial electrocardiogramsshowed normal sinus node activity, therecovery time of sinoatrial discharge followingatrial pacing was normal, and our studiesshowed normal left ventricular performance.Because of the patient's age, however, coro-nary artery disease or degenerative disease inthe SA node or atrial muscle must beconsidered. Only by long term followup ofthese asymptomatic bradyeardic subjects willwe learn whether their bradycardia willremain benign. There is a need for compara-ble studies in a symptomatic group of subjectswith sinus bradyeardia, especially with regardto the effects of atrial pacing, exercise andatropine.As shown in this report, significant degrees
of sinus bradyeardia may be associated withaging. In this latter setting, increased vagaltone may be a significant contributing factorto the bradyeardia, and more importantly,normal cardiac performance can be present.Therefore, the implications and managementof sinus bradycardia depend upon the settingin which it occurs.
References1. FOWLER NO, FENTrON JC, CONWAY GF: Syncope
and cerebral dysfunction caused by bradyear-dia without atrioventricular block. Amer HeartJ 80: 303, 1970
2. WALTER PF, REID SD JR, WENGER NK:Transient cerebral ischemia due to arrhythmia.Ann Intern Med 72: 471, 1970
3. RASMUSSEN K: Chronic sinoatrial heart block.Amer Heart J 81: 38, 1971
4. FERRER MI: The sick sinus syndrome in atrialdisease. JAMA 206: 645, 1968
5. SCHUILMAN CL, RUBENSTEIN JJ, YURCHAK PM,DESANCTIs RW: The `sick sinus" syndrome:Clinical spectrum. (Abstr) Circulation 42(suppl III): III-42, 1970
6. FRUEHAN CT, OBEID AI, SMULYAN H, EIcH RH:Sick sinus syndrome: One year's experience.(Abstr) Circulation 42 (suppl III): III-154,1970
7. BRANDFONBREN-ER M, LANDOWNE M, SHOCK NW:Changes in cardiac output with age. Circula-tion 12: 557, 1955
8. ADOLPH RJ, HOLMES JC, FUKUSUMI H: Hemo-dynamic studies in patients with chronicallyimplanted pacemakers. Amer Heart J 76: 829,1968
9. GoRLIN R, KNOWLES JH, STOREY CF: TheValsalva maneuver as a test of cardiacfunction. Amer J Med 22: 197, 1957
10. GRANATH A, JONSSON B, STRANDELL T: Circula-tion in healthy old men, studied by right heartcatheterization at rest and during exercise insupine and sitting position. Acta Med Scand176: 425, 1964
11. STONE DJ, LYON AF, TEIRSTEIN AS: A reap-praisal of the circulatory effects of the Valsalvamaneuver. Amer J Med 39: 923, 1965
12. BICKELMANN AG, LIPPSCHurz EJ, WEINSTEINL: The response of the normal and abnormalheart to exercise. Circulation 28: 238, 1963
13. CHAMBERLAIN DA, TURNER P, SNEDDON JM:Effects of atropine on heart rate in healthymen. Lancet 2: 12, 1967
14. ROBINSON BF, EPSTELN SE, BEISER GD,BRAUNWALD E: Control of heart rate by theautonomic nervous system. Circ Res 19: 400,1966
15. Ross J JR, LINHART JW, BRAUNWALD E: Effectsof changing heart rate in man by electricalstimulation of the right atrium. Circulation32: 549, 1965
16. KosowsKY BD, STEIN E, LAU SH, LISTER JW,HAF-1 JI, DAMIATO AN: A comparison of thehemodynamic effects of tachycardia producedby atrial pacing and atropine. Amer Heart J72: 594, 1966
17. THOMSON PD, MELMON KL: Clinical assessmentof autonomic function. Anesthesiology 29:724, 1968
18. HICKLER RB, HOSKINS RG, HAMLIN JT III: Theclinical evaluation of faulty orthostatis mecha-nisms. Med Clin Amer 44: 1237, 1960
19. ABELMANN WH, FAREEDUDDIN K: Increasedtolerance of orthostatic stress in patients withheart disease. Amer J Cardiol 23: 354, 1969
Circulation, Volume XLVI, November 1972
930
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

FOWLERNEIL S. AGRUSS, ELAINE Y. ROSIN, ROBERT J. ADOLPH and NOBLE O.
Significance of Chronic Sinus Bradycardia in Elderly People
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1972 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.46.5.9241972;46:924-930Circulation.
http://circ.ahajournals.org/content/46/5/924located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from


















