Sicu audit 2015
23
Dr. Muhammad Rizwan Critical Care Fellow AGA KHAN HOSPITAL DEPARTMENT OF ANAESTHESIOLOGY Karachi, Pakistan
-
Upload
tyfngnc -
Category
Health & Medicine
-
view
151 -
download
0
Transcript of Sicu audit 2015

Dr. Muhammad Rizwan
Critical Care Fellow
AGA KHAN HOSPITAL
DEPARTMENT OF ANAESTHESIOLOGY
Karachi, Pakistan

“Trauma work load of surgical intensive care unit
(SICU) at a university hospital in Pakistan - A six
month retrospective study”
TITLE OF THE STUDY

I N T R O D U C T I O N
Trauma is a worldwide public health problem.
It is the fourth leading cause of death in the western worldespecially in young population up to the age of forty.
Severe trauma, although small in number may need urgentlifesaving interventions.
Damage control surgical interventions & life sustainingorgan support in the intensive care unit consumesignificant resources and cause a huge economic burden tothe patient, healthcare system & society.
Introduction Continue
The 48 bedded state-of-the-art Emergency Department at Aga
Khan University hospital is a WHO Collaborating Center for
Trauma that handles around 60,000 patients annually.
The surgical ICU at the Aga Khan University has a capacity of
7 beds & major trauma victims requiring close monitoring or
organ support, with or without surgical interventions
constitute 30% of the admissions.
R A T I O N A L E
• Impact of trauma on our constraint resources in terms of
time, critical therapeutic interventions, advanced radiological
interventions, laboratory work load & blood product
utilization has not been previously documented in Pakistan.
• The results of this study will highlight the resources that are
required to safely & efficiently manage critically ill trauma
patients that can be utilized to plan future trauma
management facilities & improve the care of major trauma
patients in our country.

O B J E C T I V E
1. To identify trauma work load of SICU and to demonstrate
the resources utilized by the trauma admissions.
2. To compare the characteristics & outcome of trauma & non-
trauma patients.
M A T E R I A L & M E T H O D S
Settings:
SICU of Aga Khan University Hospital Karachi, Pakistan
Duration of the study: 6 months
Study Design: Retrospective study
S A M P L E S E L E C T I O N
Inclusion Criteria:
All adult admissions to SICU from 1st Jan 2014 till 30thJune 2014
Exclusion Criteria:
Age < 16 years
D A T A C O L L E C T I O N
• After Ethical Review Committee (ERC) approval, patientswere enrolled according to the inclusion & exclusion criteriadescribed above.
• Medical record numbers (MRN) of patients admitted duringthe study period were taken from the “admission recordregister” kept in the custody of the ICU head nurse.
• The variables collected from this register were age, gender,type of trauma, source of admission, length of stay in SICUand outcome.
Data Collection
Continue
Radiological investigations and interventions, laboratory
investigations, were collected from the Health information
management system (HIMS).
Blood and blood products utilized by patient were retrieved
from the blood-bank record.
D A T A A N A L Y S I S P R O C E D U R E
Statistical analyses performed using statistical software SPSS
version -16 (SPSS, Chicago, III).
Frequency & percentages were computed for qualitative
observations & analyzed by chi-square test. Mean & SD were
estimated for quantitative observations & analyzed by t-test. For
data which was not normally distributed Mann-Whitney U test
was used.
A ‘P’ value ≤ 0.05 was considered significant.

R E S U L T S
141 SICU admissions were reviewed. 22.7% (32/141) trauma
patients were identified during the 6 month study period.
Average age of the trauma cases was 35.81±13.11 years.
Male to female ratio was 7:1 in trauma cases.
Results cont…
Overall mortality of SICU was 39.7% and of the trauma
patients it was 31.3%.
Median length of stay was 5 (8) days [Median (IQR)].
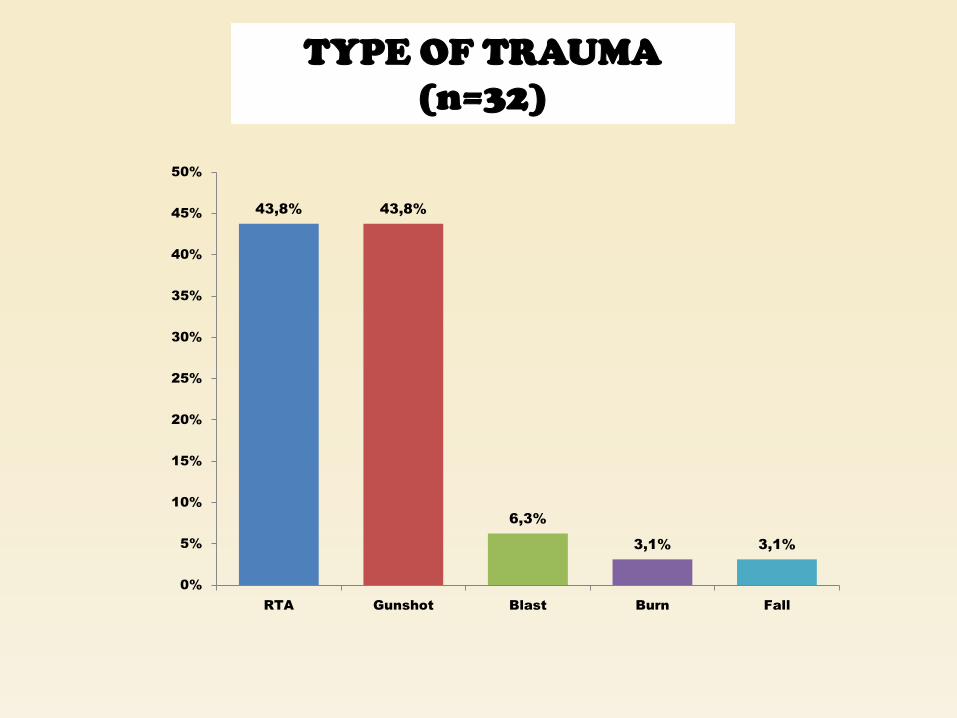
TYPE OF TRAUMA
(n=32)
43,8% 43,8%
6,3%
3,1% 3,1%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
RTA Gunshot Blast Burn Fall

SOURCES OF ADMISSION (n=32)
OR= Operating Room SCU = Special care unit
ER= Emergency room Other = Referred Cases
71,9%
9,4% 9,4%
6,3%
3,1%
0%
10%
20%
30%
40%
50%
60%
70%
80%
OR Ward ER SCU Others

Non-Operative
25%
Emergency
Operative
72%
Elective
Operative
3%
TYPE OF ADMISSION OF TRAUMA CASES
(n=32)

Variables
Trauma Non-Trauma
P-Valuen=32 n=109
Age (Years) 35.81±13.11 49.04±18.67 0.0005
Gender [M/F]
28/4 72/37
0.01987.5%/12.5% 66.1%/33.9%
Length of stay (days) 19.34±14.09 17.43±18.15 0.58
Outcome [Alive/Death]
22/10 63/46
0.2668.8%/31.3% 57.8%/42.2%

THERAPEUTIC INTERVENTIONS IN
PATIENTS ADMITTED TO SICU WITH
TRAUMA (n=32)
CVC= Central Venous Pressure
CRRT= Continuous Renal
Replacement Therapy
NIV= Non Invasive Ventilation
MV = Mechanical Ventilation
CVC= Central Venous
Catheterization
0% 20% 40% 60% 80% 100%
NIV
CRRT
Tracheostomy
Blood
Transfusion
CVC
Enteral Feeding
Intubation
MV
3,1%
6,3%
43,8%
65,6%
75,0%
84,4%
87,5%
96,9%
Blood product
utilization
Number of
Patients
% Meidan
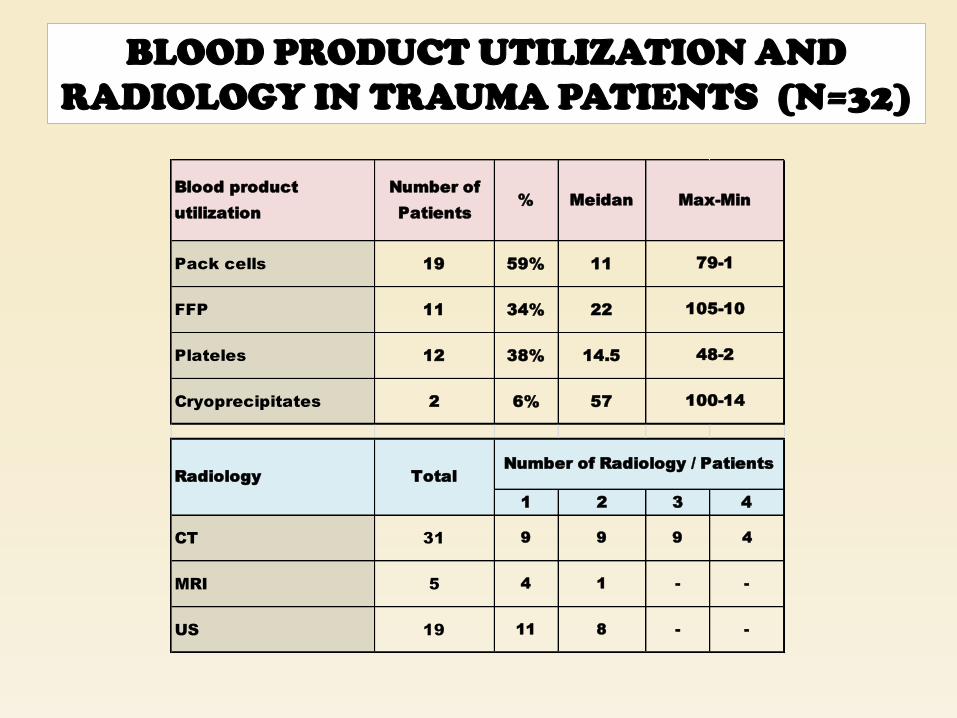
Pack cells 19 59% 11
FFP 11 34% 22
Plateles 12 38% 14.5
Cryoprecipitates 2 6% 57
1 2 3 4
CT 31 9 9 9 4
MRI 5 4 1 - -
US 19 11 8 - -
TotalRadiology
Number of Radiology / Patients
Max-Min
79-1
105-10
48-2
100-14
BLOOD PRODUCT UTILIZATION AND
RADIOLOGY IN TRAUMA PATIENTS (N=32)

Mean SD Minimum Maximum
CBC 17.03 13.87 3 60
BUN 16.56 14.85 2 58
Creatinie 18.69 17.17 2 70
Electrolytes 21.44 18.14 3 72
PT 11.75 12.81 1 51
APTT 11.41 12.80 1 51
LFT 1.31 2.28 0 8
ABGs 18.13 18.78 1 77
Lactic.Acid 2.09 2.41 0 8
Procalcitonin .00 .00 0 0
Blood.CS 4.28 4.62 0 16
Tracheal.CS 1.06 2.14 0 8
Urine.CS 1.81 1.75 0 7
LABORATORY INVESTIGATION IN
TRAUMA PATIENTS (n=32)
C O N C L U S I O N
• T r a u m a c o n s t i t u t e s a s i g n i f i c a n t w o r k l o a d
( 2 2 . 7 % ) f o r S I C U o f A g a K h a n U n i v e r s i t y ,
P a k i s t a n
• T r a u m a v i c t i m s a r e p r e d o m i n a n t l y y o u n g m a l e s
i n w h o m g u n s h o t i n j u r i e s a r e a s c o m m o n a s r o a d
t r a f f i c a c c i d e n t s
• B l o o d p r o d u c t s , r a d i o l o g i c a l a n d l a b o r a t o r y
i n v e s t i g a t i o n s a r e t h e m a j o r c o n t r i b u t e r s o f
r e s o u r c e s u t i l i z e d .

REFERENCES:
• 1) Chaira O, Cimbanissi S. Organized trauma care: does volume matter and do trauma centers save lives? Curr Opin Crit Care 2003; 9:510-4
• 2) Grossman MD. Introduction to trauma care. In Peitzman AB, Rhodes M, Schwab CW, Yealy DM, eds. The Trauma Manual. Philadelphia, Lippincott–Raven, 1998, pp 1–5
• 3) Mitchell VT, Scarlett MD. Trauma Admissions to the ICU of The University Hospital of the West Indies, Kingston, Jamaica. ITACCS. 2001;86-89

Thank you