
Sickle cell disease
17
SICKLE CELL SYNDROMES Brajesh Lahri Final Professional MBBS All India Institute of Medical Sciences (AIIMS).Bhopal
-
Upload
brajesh-lahri -
Category
Health & Medicine
-
view
110 -
download
9
Transcript of Sickle cell disease

SICKLE CELL SYNDROMES
Brajesh Lahri
Final Professional MBBS
All India Institute of Medical Sciences (AIIMS).Bhopal

INTRODUCTION• Sickle Cell Syndromes are structural
haemoglobinopathies
• Mutations alter the amino acid sequence of a globin chain (i.e. sixth amino acid Glutamate Valine)
• Cause alteration in physiological properties of variant haemoglobin and produce characteristic clinical abnormalities
TYPES OF SICKLE CELL SYNDROMES
• Sickle Cell Trait
• Sickle Cell Anaemia
• S/ß0 Thalassemia
• S/ß+ Thalassemia
• Haemoglobin SC

EPIDEMIOLOGY OF SICKLE CELL DISEASE
http://www.nature.com/ncomms/journal/v1/n8/images/ncomms1104-f2.jpg

WHY DOES IT OCCUR ?
• Autosomal recessive disease
• Occurs when mutated gene is transferred to the progeny from both the parents
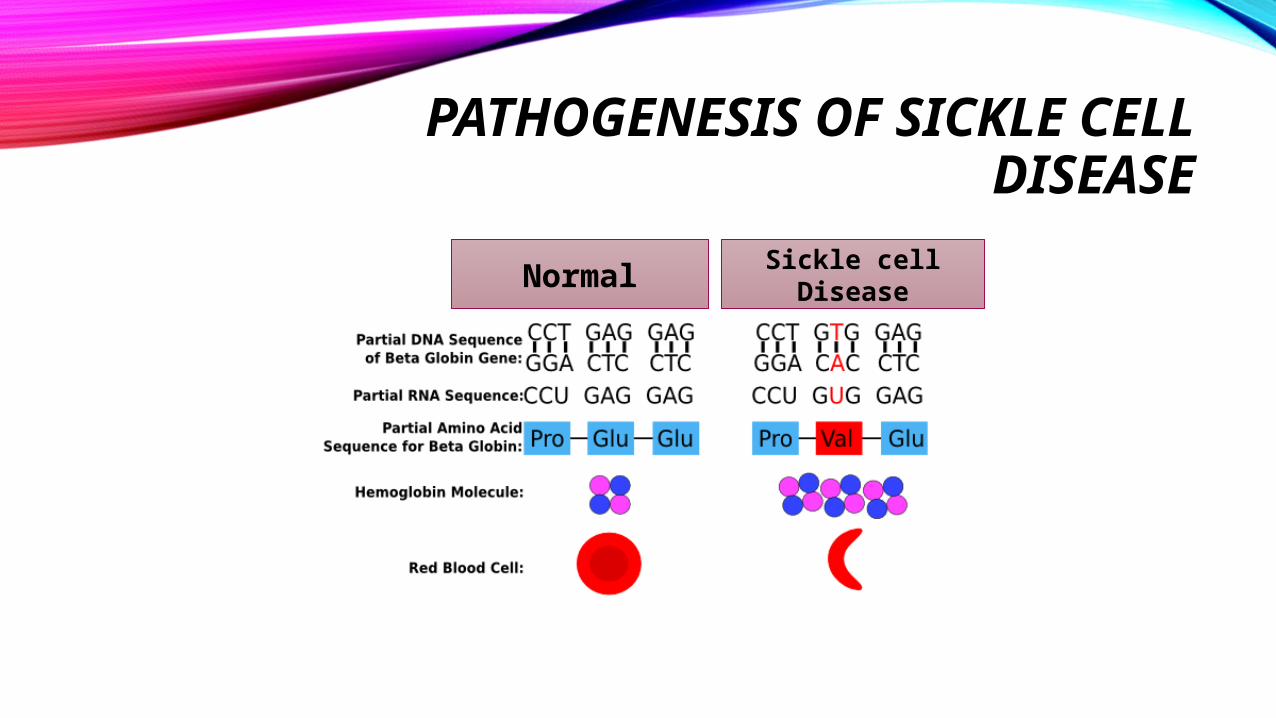
PATHOGENESIS OF SICKLE CELL DISEASE
Normal Sickle cell Disease

CLINICAL MANIFESTATIONS OF SICKLE CELL ANAEMIA
Clinical Manifestations of Sickle Cell
Anaemia
Due to Haemolysis
Anaemia , Jaundice and Gall Stones
Due to Microvascular
Occlusion
Stroke, Pain crisis, Acute Chest
Syndrome, Hand-foot Syndrome
Osteonecrosis , Occlusion of retinal vessels, Priapism, Chronic leg ulcers
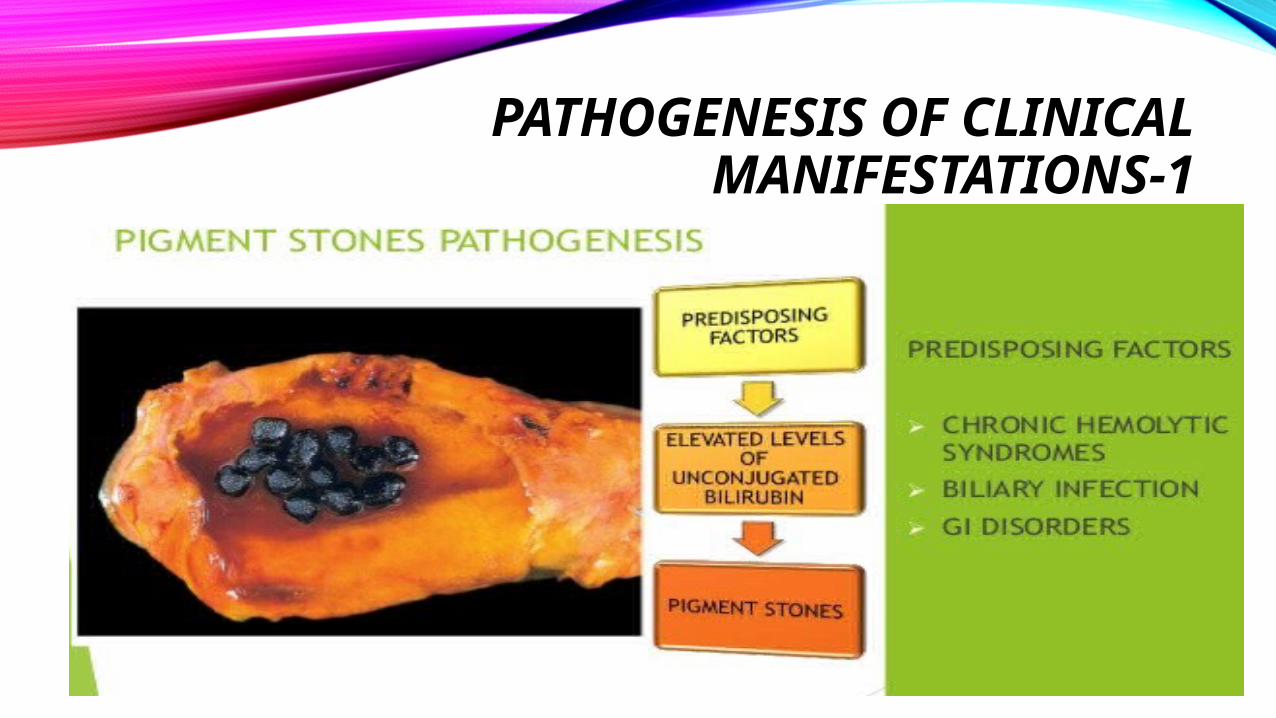
PATHOGENESIS OF CLINICAL MANIFESTATIONS-1
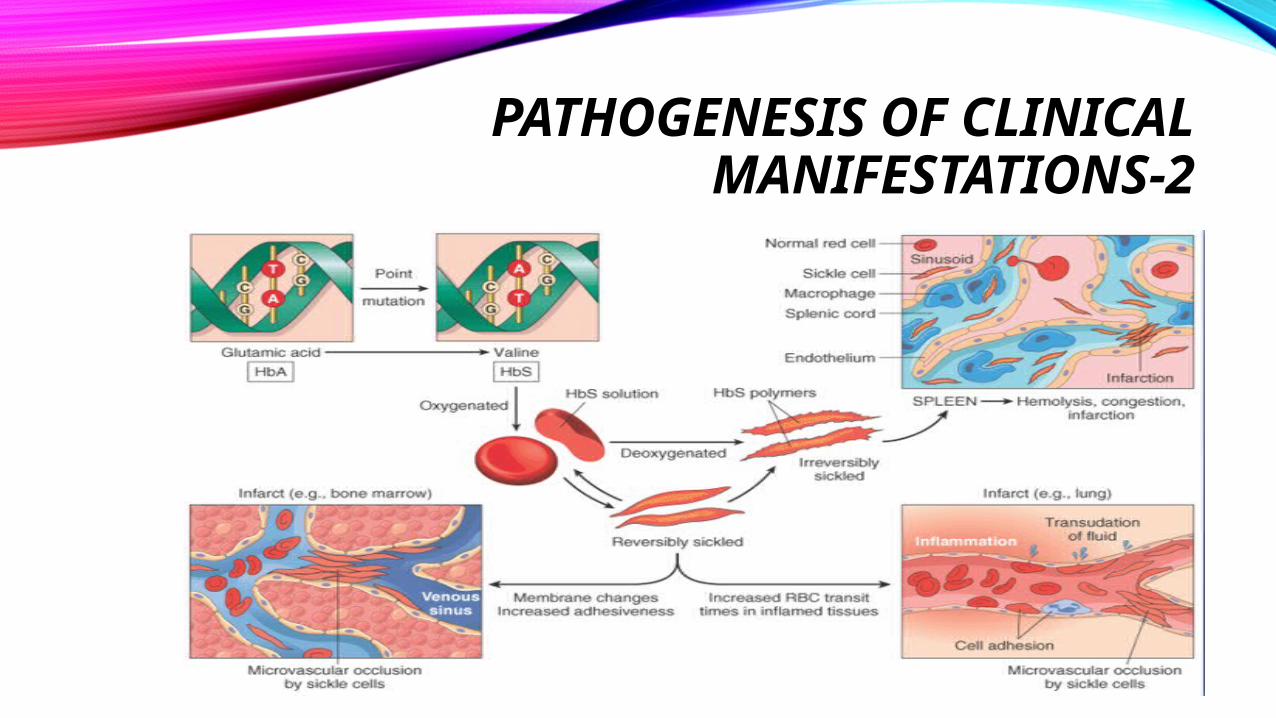
PATHOGENESIS OF CLINICAL MANIFESTATIONS-2

MANAGEMENT
Management of Acute Painful
Crisis
Management of Acute Chest Syndrome
Management of cases suffering
from severe disease
MANAGEMENT OF ACUTE PAINFUL CRISIS
• Vigorous hydration and thorough evaluation for underlying cause (such as infection )
• Aggressive analgesia should be given
• Morphine- for severe pain.Dose: 0.1-0.15 mg/kg every 6-8 hr
• Ketorolac-for bone pain. Dose-30-60 mg initial dose then15-30 mg every 6-8 hr
• NO- can be used to provide short term pain relief
• Blood transfusion should be reserved for extreme cases

MANAGEMENT OF ACUTE CHEST SYNDROME
• Medical emergency requiring management in ICU
• Continuous monitoring of hydration is essential to avoid development of pulmonary edema
• Vigorous oxygen therapy for protection of arterial oxygen saturation
• Blood transfusion should be given to maintain a hematocrit of >30
• Emergency exchange transfusion if arterial saturation drops to <90%
MANAGEMENT OF CASES SUFFERING FROM SEVERE DISEASE
•Use of Hydroxyurea
•Blood Transfusion
•Bone marrow Transplantation

HYDROXYUREA
• Mainstay of therapy for patients with severe symptoms
• Mechanism of Action :
Increases fetal hemoglobin(HbF).Beneficial effects on RBC hydration and vascular wall adherence.Suppression of the granulocytes and reticulocytes.
• Dose:10-30 mg/kg per day.

BLOOD TRANSFUSION
• Simple Transfusion: Indications of simple transfusion- Splenic sequestration Aplastic crisis Acute chest syndrome
• Exchange Transfusion:Indicated in children who have suffered from cerebrovascular accident , to
reduce the risk of stroke in future

ADDITIONAL PROPHYLACTIC MEASURES
Children should be vaccinated against capsulated organisms like pneumococcus, meningococcus , H.influenza-B, Hepatitis B and seasonal influenza.
Regular slit lamp examination to monitor retinopathy.
Antibiotic prophylaxis for splenectomized patient during dental or invasive procedures.
Vigorous oral hydration during periods of extreme exercise,exposure to hot and cold,emotional stress or infection.

Thank You !


















