

Shoulder Rehabilitation after Dislocation - Denver, …€¢ Site of instability and surgery ......
34
Shoulder Rehabilitation after Dislocation John Nyland DPT, SCS, EdD, ATC, CSCS, FACSM Professor Athletic Training Program Director Spalding University Louisville, Kentucky, USA
Transcript of Shoulder Rehabilitation after Dislocation - Denver, …€¢ Site of instability and surgery ......

Shoulder Rehabilitation after Dislocation
John Nyland DPT, SCS, EdD, ATC, CSCS, FACSM
Professor
Athletic Training Program Director
Spalding University
Louisville, Kentucky, USA

Normal Glenohumeral Capsulo-ligamentous Tightening
As the glenohumeral joint abducts and externally rotates, the capsuloligamentous structures gradually
tighten stimulating mechanoreceptors providing proprioceptive information.

The glenoid socket is considerably smaller than the humeral head

Glenohumeral Joint
• Site of instability and surgery -Capsulolabral procedures, RC Repairs
• Central positioning is dependent on contractile and non-contractile tissue integrity and length (posture)
• Considerable labral, capsulo- ligamentous, and musculo- tendinous tissue blending
• Nyland J, et al. Knee Surg Sports Traumatol Arthrosc 1998;6:50-61
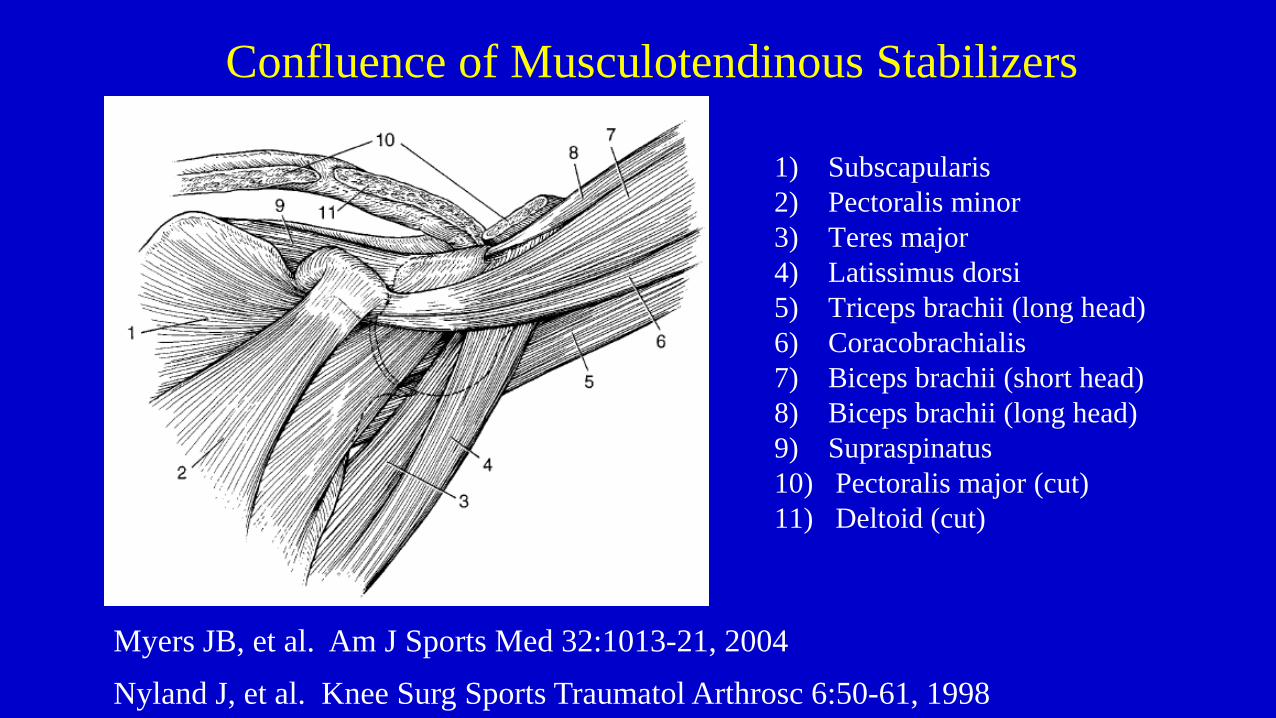
Confluence of Musculotendinous Stabilizers
1) Subscapularis
2) Pectoralis minor
3) Teres major
4) Latissimus dorsi
5) Triceps brachii (long head)
6) Coracobrachialis
7) Biceps brachii (short head)
8) Biceps brachii (long head)
9) Supraspinatus
10) Pectoralis major (cut)
11) Deltoid (cut)
Myers JB, et al. Am J Sports Med 32:1013-21, 2004
Nyland J, et al. Knee Surg Sports Traumatol Arthrosc 6:50-61, 1998

Postural Imbalances
• Glenoid position is strongly influenced by the muscles that have scapular or humeral attachments. Many of these muscles originate from the trunk.
• Trunk posture strongly influences the position of the glenoid and pelvis position strongly influences the position of the trunk.

Glenohumeral Joint Capsulolabral Repair

Functional Glenohumeral Joint Anatomy
• Humeral head depression with elevation, ER
LaStayo P, et al. JOSPT 33:557-571, 2003 Perry J. In: Rowe C (ed): The Shoulder, 1988

Functional Scapulothoracic Anatomy
Dynamic Stability • The state of a joint or joints remaining or
promptly returning to proper alignment through an equalization of forces throughout the body (the goal is optimal sensorimotor function!)
• Dynamic joint stability is accomplished through a complementary relationship between static (non-contractile) and dynamic (contractıle) components throughout the body.
Functional Trunk Anatomy
• Antagonistic trunk muscle co-activation is strongly influenced by dynamic stability needs.
• Panjabi M. – 90 N (20 lbs) compressive loads cause spinal buckling when muscular contributions are absent.
• McGill S. – the spine and the trunk muscles function together like a fishing rod and supportive guide wires.

Functional Trunk Anatomy
• Panjabi has described interdependent spinal osseoligamentous, musculotendinous, and motor control components.
• Deficits in one system can be partially compensated for by contributions from the other two (cognitive engagement).
• The erector spinae make up the bulk of the dorsal lumbar musculature consisting of the iliocostalis, longissimus, and spinalis.
• The multifidus, quadratus lumborum, psoas, and iliacus muscles are also involved.

“Abdominal Hoop”
• The rectus abdominis, internal and external oblique and transversus
abdominis are directly involved with dynamic trunk stability and force
transfer between the upper and lower extremities.
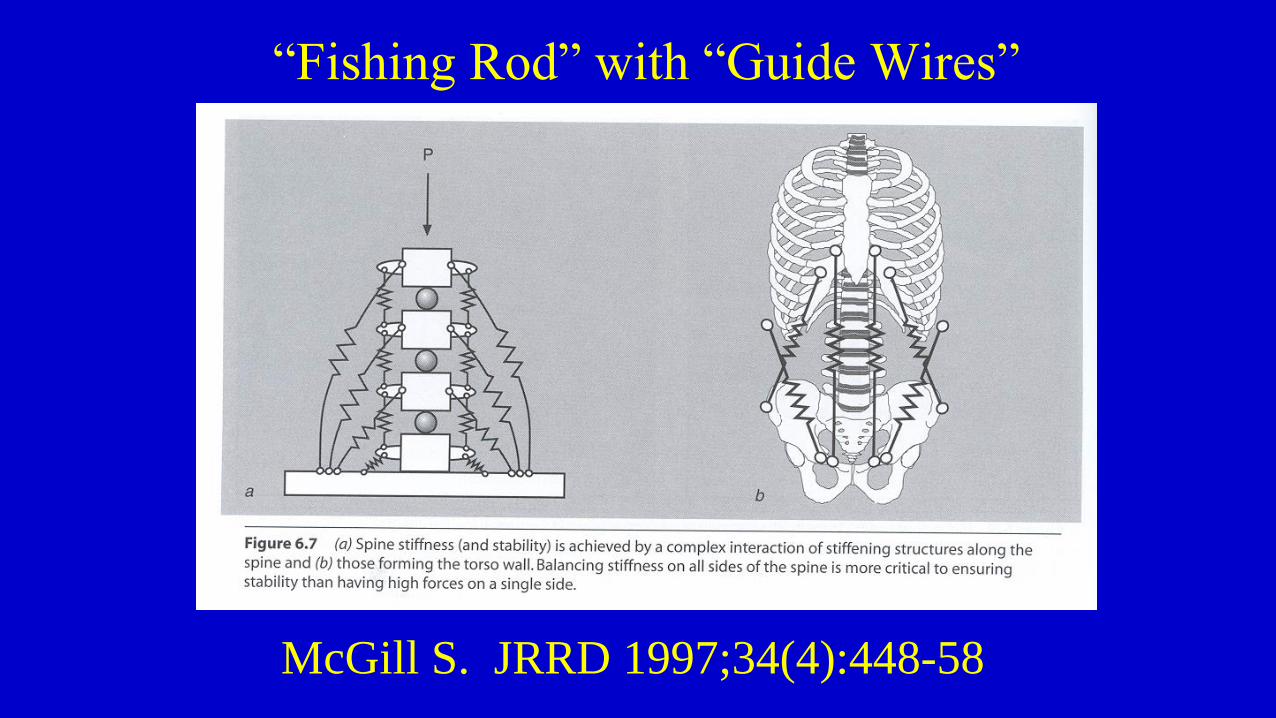
“Fishing Rod” with “Guide Wires”
McGill S. JRRD 1997;34(4):448-58

“Hollowing vs. Bracing”

Hodges P, Richardson C.
Spine 1996;21(22):2640-50
• Transversus abdominus is the
first trunk muscle activated
with upper extremity
movements.
• Delayed transversus
abdominus activation =
inefficient dynamic spinal
stabilization.

Stokes I, et al. Spine 2000;25:1957-64
• Greater dependence on trunk muscle pre-activation increases stability at the expense of mobility.
• Efficient neuromuscular trunk muscle responsiveness to sudden perturbation reduces the need for pre-activation.
Gardner-Morse M, Stokes I. Spine 1998;23(1):86-91
• Activated spinal muscles serve as stabilizing springs rather than force generators
• Increased dynamic trunk stability through muscular co-activation occurs at the cost of increased fatigue rates (should not be on all the time!)

McGill S. JRRD 1997;34(4):448-58
• To maintain a healthy low back exercises should use
low to moderate load, high repetitions. There is no
single exercise that challenges all of the abdominal
muscles. Rx of more than one exercise is required!

Functional Trunk Anatomy
• Fatigue, inflammation, de-conditioning, and pain in the trunk musculature is related to trunk and shoulder muscular dysfunction and atrophy.
• Maladaptive transversus abdominis and multifidus motor control may be related to altered posture, muscle imbalances, and shoulder injuries.
3D Matrix, Long-Axis Rotation, Fascial System Optimization
•Progressive eccentric loading
•“Takes-up” fascial slack
throughout trunk and extremities
•Has a secondary muscle tone
regulatory effect
•Create, appreciate, and learn how
to control shoulder instability and
knee wobbles

3D Matrix (Concentric-Eccentric-Concentric)
• Progressive vertical loads (weighted vest)
• Progressive cadence (metronome)
• Progressive heights (incremented steps)
• Progressive duration (stopwatch)
• Progressive rotational loads (medicine balls, dumbbells, bars, etc)
• Consideration of metabolic energy systems (sport, style)
• Movement Quality

Matrix Variations and Lunges

Neuromuscular Activation, Tissue Extensibility Training
• Evolution
• Postures,
movements
• Muscles,
exercises
• Core integration
in positions of
function!

Extereceptive Denial

Impairment Level
• ROM, extensibility
• Endurant Strength - Power
• GHJ dynamic stability
• Frequent re-evaluation, maintenance training

Local-Regional-Global
• Local (AROM, rhythmic stabilization)
• Keep humeral head well-centered and approximated in the glenoid fossa
• Position Sense, Co-contraction, Rhythmic Stabilization, Reaction Time
• Protected Overhead Motion
• Teach patient the safe, protected ROM zone
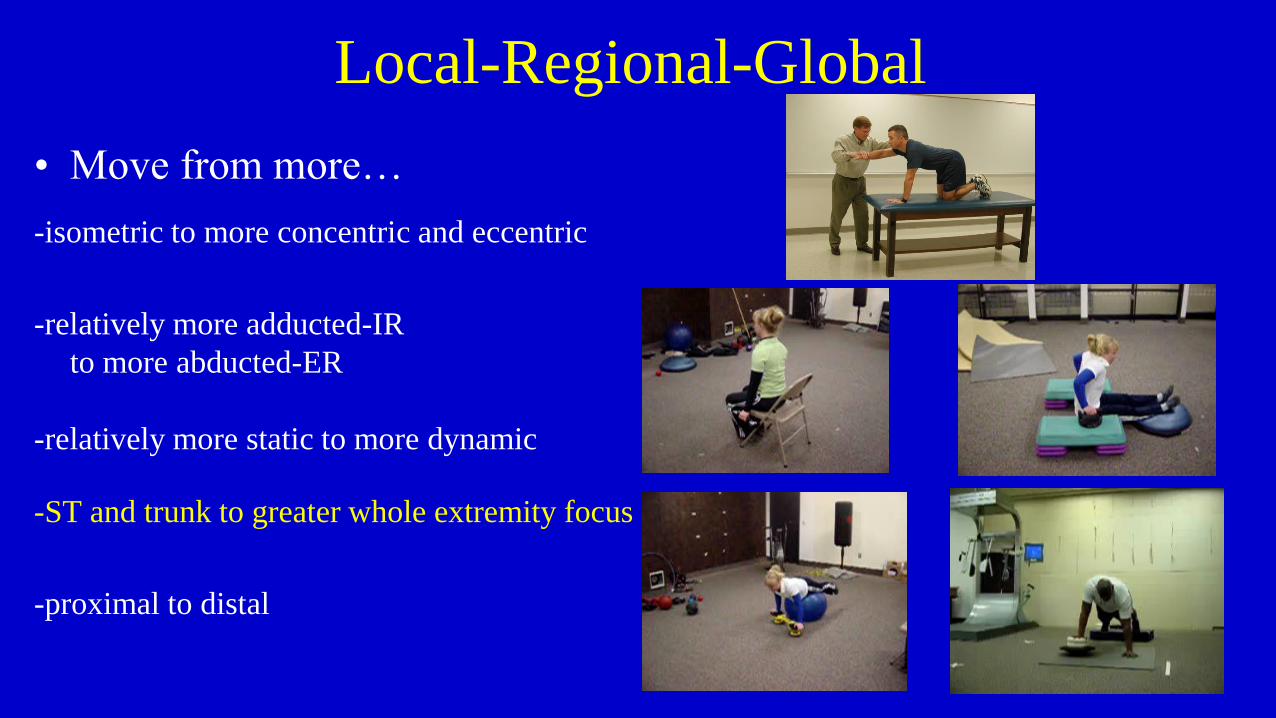
Local-Regional-Global
• Move from more…
-isometric to more concentric and eccentric
-relatively more adducted-IR
to more abducted-ER
-relatively more static to more dynamic
-ST and trunk to greater whole extremity focus
-proximal to distal

Injury Prevention Training Philosophy
• Increase intrinsic muscle
stiffness – viscosity (pre-set)
• Improve reflex responsiveness
(pre-plan or pre-set)
• SAID Principle (sport, position,
style, etc)

Falling, Rolling, Slidıng • Work hardening
simulations
• Total body posture
• Lower extremity agility training
• Upper extremity positioning
• Falling / Sommersaults

Neuromuscular Activation, Tissue Extensibility Training
• Revolution
Nyland J, et al. Phys Ther Sport. 2014;15(1):26-32.
Nyland J, et al. Clin Biomech. 2011;26(4):363-70.
Nyland J, et al. J Electromyogr Kinesiol. 2011;21(2):348-55.
Summary
• From Local-Regional-Global
• Re-establish…
• non-impaired tissue extensibility (ROM)
• normal impairment level strength (isometrics, concentrics, eccentric continuum)
• Normal power (high end concentrics, eccentric bias)
• Re-evaluate often (and teach self-evaluation)

Rehabilitation Pearls
• The first, second and third priority is restoration of pain-free active glenohumeral joint range of motion
• Proximal stability (trunk and scapulo-thoracic joint) precedes distal mobility
• Focus on strength training within mid-ranges to not adversely strain the non-contractile stabilizing tissues (this is particularly important in patients with recurrent shoulder instability and/or genetically-induced joint laxity.
• The shoulder functions as a component of the entire kinetic or kinematic chain. Exclusive focus on the shoulder without consideration of the entire chain-reaction is likely to produce a poor treatment result.


















