Should magnesium sulfate be administered to women with ... · tify descriptive study reports for...
13
Should magnesium sulfate be administered to women with mild pre-eclampsia? A systematic review of published reports on eclampsia Yifru Berhan and Asres Berhan Hawassa University College of Medicine and Health Sciences, Hawassa, Ethiopia Abstract Aim: Magnesium sulfate is an evidence-based anticonvulsant drug used to prevent and control eclampsia. Con- troversy persists on routine administration of magnesium sulfate in cases of pre-eclampsia without severe fea- tures. Our objective was to assess the pattern of blood pressure and maternal symptoms preceding eclamptic seizure based on the current published work. Material and Methods: A comprehensive computer-based publication search was conducted in the African Journals Online, Google scholar, HINARI, PubMed, and MEDLINE databases and the Cochrane library to iden- tify descriptive study reports for blood pressure, severity symptoms or stage of pregnancy during convulsion in women with eclampsia. Results: A total of 59 publications were eligible for this review. Overall, 21149 eclamptic women from 26 countries were included for the interest of one or more of the selected variables. Out of 18488 eclamptic women, the proportion of antepartum, intrapartum and post-partum eclampsia was 59%, 20% and 21%, re- spectively. Out of 3443 eclamptic women, 25% were normotensive; 20% had mild-to-moderate hypertension; 32% had severe hypertension; and 21% were hypertensive but unclassified. Out of 2163 eclamptic women, 66% and 27% had a headache and visual disturbance, respectively, preceding the occurrence of convulsion. Out of 2053 eclamptic women, 25% had epigastric area pain, and out of 1092 women with eclampsia, 25% were asymptomatic. Conclusion: Although eclampsia is known to result from severe pre-eclampsia with or without organ function derangement, this review has revealed that a significant number of eclamptic women had either normal blood pressure or mild-to-moderate hypertension immediately before seizure. The findings are apparently in support of initiating magnesium sulfate prophylaxis to all women with mild pre-eclampsia. Key words: descriptive studies, eclampsia, magnesium sulfate, mild pre-eclampsia, systematic publication review. Introduction Eclampsia is diagnosed in pregnant or post-partum women with the onset of generalized tonic–clonic sei- zure in light of pre-eclampsia, not attributable to other causes. 1,2 Although eclampsia was recognized as a dis- tinct disease entity (separate from epilepsy) during the unfolding of the 19th century 3 and different treatment modalities were attempted, 4 it is still not possible to completely prevent its occurrence, even in the best set- ting. 5 As a result, eclampsia remains one of the leading causes of maternal and perinatal mortality worldwide, with the majority of the disease burden in the developing world. 6 The incidence of eclampsia in developed nations Received: August 26 2014. Accepted: January 13 2015. Reprint request to: Professor Yifru Berhan, Hawassa University College of Medicine and Health Sciences, PO Box 1560, Hawassa, Ethiopia. Email: [email protected] © 2015 The Authors Journal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology 831 doi:10.1111/jog.12697 J. Obstet. Gynaecol. Res. Vol. 41, No. 6: 831–842, June 2015
Transcript of Should magnesium sulfate be administered to women with ... · tify descriptive study reports for...

Should magnesium sulfate be administered to women withmild pre-eclampsia? A systematic review of published reportson eclampsia
Yifru Berhan and Asres BerhanHawassa University College of Medicine and Health Sciences, Hawassa, Ethiopia
Abstract
Aim: Magnesium sulfate is an evidence-based anticonvulsant drug used to prevent and control eclampsia. Con-troversy persists on routine administration of magnesium sulfate in cases of pre-eclampsia without severe fea-tures. Our objective was to assess the pattern of blood pressure and maternal symptoms preceding eclampticseizure based on the current published work.Material and Methods: A comprehensive computer-based publication search was conducted in the AfricanJournals Online, Google scholar, HINARI, PubMed, and MEDLINE databases and the Cochrane library to iden-tify descriptive study reports for blood pressure, severity symptoms or stage of pregnancy during convulsion inwomen with eclampsia.Results: A total of 59 publications were eligible for this review. Overall, 21149 eclamptic women from 26countries were included for the interest of one or more of the selected variables. Out of 18488 eclampticwomen, the proportion of antepartum, intrapartum and post-partum eclampsia was 59%, 20% and 21%, re-spectively. Out of 3443 eclamptic women, 25% were normotensive; 20% had mild-to-moderate hypertension;32% had severe hypertension; and 21% were hypertensive but unclassified. Out of 2163 eclamptic women,66% and 27% had a headache and visual disturbance, respectively, preceding the occurrence of convulsion.Out of 2053 eclamptic women, 25% had epigastric area pain, and out of 1092 women with eclampsia, 25%were asymptomatic.Conclusion: Although eclampsia is known to result from severe pre-eclampsia with or without organ functionderangement, this review has revealed that a significant number of eclamptic women had either normal bloodpressure or mild-to-moderate hypertension immediately before seizure. The findings are apparently in supportof initiating magnesium sulfate prophylaxis to all women with mild pre-eclampsia.Key words: descriptive studies, eclampsia, magnesium sulfate, mild pre-eclampsia, systematic publicationreview.
Introduction
Eclampsia is diagnosed in pregnant or post-partumwomen with the onset of generalized tonic–clonic sei-zure in light of pre-eclampsia, not attributable to othercauses.1,2 Although eclampsia was recognized as a dis-tinct disease entity (separate from epilepsy) during the
unfolding of the 19th century3 and different treatmentmodalities were attempted,4 it is still not possible tocompletely prevent its occurrence, even in the best set-ting.5 As a result, eclampsia remains one of the leadingcauses of maternal and perinatal mortality worldwide,with themajority of the disease burden in the developingworld.6 The incidence of eclampsia in developed nations
Received: August 26 2014.Accepted: January 13 2015.Reprint request to: Professor Yifru Berhan, Hawassa University College of Medicine and Health Sciences, PO Box 1560, Hawassa, Ethiopia.Email: [email protected]
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
831
doi:10.1111/jog.12697 J. Obstet. Gynaecol. Res. Vol. 41, No. 6: 831–842, June 2015

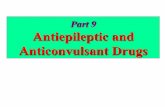
has declined over the past half century due to improvedantenatal care and early initiation of prevention andtreatment.7 The incidence of eclampsia in high-incomecountries is now significantly lower than that in low-and middle-income countries (Fig. 1).
In the last 2 decades, magnesium sulfate has becomea very popular anticonvulsant drug across the worldto prevent and control eclampsia, particularly inwomen with severe pre-eclampsia.1,7 However, the rec-ommendation of magnesium sulfate to women withmild pre-eclampsia is remains controversial. Accordingto the American College of Obstetricians and Gynecol-ogists (ACOG) 2013 task force recommendation, mag-nesium sulfate should not be given universally forthe prevention of eclampsia in women with mild pre-eclampsia evidenced by systolic blood pressure (BP)of 140–160mmHg, a diastolic BP of <110mmHg andno maternal symptoms.8 The WHO also recommendsthe administration of magnesium sulfate for severepre-eclampsia, but reserves comment on mild pre-eclampsia.1
A randomized controlled trial ofmagnesium sulfate inwomen with mild pre-eclampsia showed statistically in-significant increased risk of severe pre-eclampsia in theplacebo group but no eclampsia in either the treatmentor placebo group.8 In contrast, Alexander et al. showedthat giving magnesium sulfate prophylaxis selectivelyto women with severe gestational hypertension was as-sociated with a significant increase of eclampsia in thewomen with mild hypertension.9 In another study, byFoong and Pollard, 53% of eclamptic episodes could
have been prevented if seizure prophylaxis was univer-sally administered for gestational hypertension fromthe time of diagnosis through 24h post-partum.10
As acknowledged by the ACOG 2013 task force, thereis a paucity of data on the importance of magnesiumsulfate prophylaxis for women with mild-to-moderatehypertension in the absence of severe features. Sibaialsonotes that evidence for the use ofmagnesium sulfate pro-phylaxis in mild pre-eclampsia remains uncertain.11
Based on data from two randomized trials,12,13 200womenwithmild pre-eclampsia would need to be givenmagnesium sulfate to prevent one case of eclampsia.14
According to some authors, if magnesium sulfate is rou-tinely administered to all, the adverse effects may out-weigh the risk of seizure.14
Due to lack of adequate data,8,11,15 controversy re-mains regarding routine administration of magnesiumsulfate towomenwithmild pre-eclampsia.16–19 This con-troversy may be settled in the future through meta-analysis of high-quality randomized double-blindclinical trials. To date, however, there are no adequaterandomized clinical trials with which to perform such ameta-analysis on mild pre-eclampsia. This review wasplanned to provide an answer to: how many eclampticwomen have mild-to-moderate hypertension and severesymptoms? Therefore, the purpose of this study was toassess the blood pressure and pattern of symptoms ofwomen with eclampsia from different parts of the worldas indirect evidence of the importance ofmagnesium sul-fate prophylaxis for women with mild pre-eclampsia ormild-to-moderate hypertension.
Figure 1 Incidence of eclampsia per1000 deliveries in some countriesacross the globe. Decimal numbersare rounded to the nearest tenth.
Y. Berhan and A. Berhan
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
832

MethodsStudy design and area of interest
A systematic review of descriptive publications oneclampsia was conducted using online available articlesfrom any part of the world. The incidence of eclampsiabetween 1998 and 2013 in select countries was analyzedfor trends. Blood pressure pattern of eclamptic womenbefore the occurrence of seizure was the main interestof this review. Symptoms of pre-eclampsia (headache,visual disturbance, epigastric area pain and vomiting)and type of eclampsia were also reviewed.
Publication search strategy
A comprehensive computer-based search of the pub-lished work was conducted by two investigators (Y.B.and A.B.) independently in the African Journals Online,Google scholar, HINARI, PubMed and MEDLINE data-bases and the Cochrane library to identify reports ofblood pressure and symptoms in women who devel-oped eclampsia during the antepartum, intrapartumand post-partum periods. The search was furtherstrengthened by searching the reference lists of re-trieved articles that reported types of blood pressure(mild range, moderate range, severe range), or relevantsymptoms during the study period. The search termswere: ‘eclampsia’, ‘pre-eclampsia’, ‘eclampsia hyperten-sion’, ‘eclampsia pre-eclampsia’, ‘eclampsia gestationalhypertension’, ‘eclampsia pre-eclampsia magnesiumsulfate’, ‘magnesium sulfate’, ‘eclampsia pre-eclampsiaseverity symptoms-headache, visual disturbance, epi-gastric pain, vomiting’, ‘type of eclampsia-antepartum,intrapartum, post-partum, late post-partum’ and ‘preg-nancy induced hypertension’. The selected search termswere combined alternatively with the Boolean logic(AND, OR and NOT).
Inclusion criteria and study selection
The predetermined inclusion criteria were: (i) studies oneclampsia that assessed the blood pressure or severitysymptoms or type of eclampsia; and (ii) studies thatwere published in English and conducted between1930 and 2013. Study selection was conducted in twostages. First the abstracts of all the retrieved reports werereviewed and then grouped as ‘eligible for full documentreview’ or ‘ineligible for full document review’. Second,all the reports grouped as ‘eligible for full document re-view’ were reviewed in detail and grouped as ‘eligiblefor this review’ or ‘ineligible for this review’.
From the included studies, the following informationwas abstracted: name of the first author, country study
conducted, study period, total eclampsia cases includedin the study, mean maternal age, type of eclampsia, dia-stolic and systolic blood pressure, and selected severitysymptoms of hypertension disorders (headache, blurredvision, epigastric area pain, vomiting).
Operational definitions
Mild-to-moderate hypertension during pregnancy orduring puerperiumwas defined as a systolic blood pres-sure of 140–160mmHg and/or diastolic blood pressureof 90–110mmHg immediately before seizure. Severehypertension was considered when the systolic bloodpressure was ≥160mmHg and/or diastolic blood pres-sure was ≥110mmHg.20 Presence of hypertension withproteinuria after 20weeks of gestation defines pre-eclampsia. Severe pre-eclampsia was defined as severehypertension or mild-to-moderate hypertension with se-vere symptoms and significant proteinuria (proteinuria>300mg in 24h urine or +2 and above in the dipsticktest). Mild pre-eclampsia was defined as mild-to-moderate hypertension without severe symptoms andwithout significant proteinuria. In this article, mild-to-moderate hypertension andmild pre-eclampsia are usedinterchangeably.
Data presentation
Data are presented in tables and summarized in figures.The actual values of each study were added and propor-tions were determined for the type of eclampsia, distri-bution of blood pressure and presence of severesymptoms. Similarly, when two or more studies werefound from the same country during 1998–2013, the de-nominators (total deliveries) and numerators (total casesof eclampsia) were added before the incidence ofeclampsia was estimated for that specific country.
Results
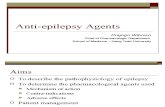
The database search retrieved 3424 reports for thesearch term ‘pre-eclampsia, eclampsia and blood pres-sure’. After screening the titles in each database, 389 ar-ticles were retrieved for abstract review. One hundredthirteen articles were excluded after reviewing the ab-stracts. Two hundred seventeen articles were excludedafter full document review; the majority of the excludedarticles were unrelated to the objective of this reviewand assessed the treatment outcome of different anti-convulsant and antihypertensive drugs. Finally, 59 arti-cles (20 from high-income, 30 from middle-income and
Systematic review of reports on eclampsia
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
833

nine from low-income countries) were eligible for thisreview (Fig. 2).7,9,16,21–76
Overall, 21155 women with eclampsia from 26 coun-tries were included. The majority of the included stud-ies were hospital-based and case series. Four studiesreported antepartum and intrapartum eclampsia to-gether.16,44,52,67 Three studies reported only post-partum eclampsia24,37,72 and nine studies with no dataon type of eclampsia were included for the interest ofother variables (blood pressure and severity symp-toms).9,29,33,34,54,60,65,68,71 With the exception of fourstudies,24,40,63,72 the majority of studies reported thateclampsia occurred during the antepartum period(range: 39–94%). Specifically, intrapartum eclampsiawas dominant in the reports by Ekele (67%) and Knonje(46%)24,72 and post-partum eclampsia was dominant inreports by Douglas (44%) and Obiechina (46%)(Table 1).40,63
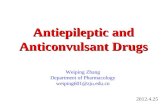
Figure 3 shows the summary of all the studies that re-ported type of eclampsia at three levels (antepartum,intrapartum and post-partum).7,21–24,26–28,30–32,35–43,45–51,53,55–59,61–64,66,69,70,72–75 Out of 18488 eclampsia cases,the proportion of antepartum, intrapartum and post-partum eclampsia was 59%, 20% and 21%, respectively.Two of the included studies reported 15% and 16% latepost-partum eclampsia.44,73
Table 2 shows the 26 studies that reported the bloodpressure (BP) pattern of eclamptic women. In sevenstudies,9,27,37,45,56,72 including one unpublished, BP wasclassified as normotensive (BP of< 140/90mmHg),mild-to-moderate hypertension (systolic BP of140–160mmHg and/or diastolic BP of 90–110mmHg),and severe hypertension (systolic BP of >160mmHgand/or diastolic BP of >110mmHg) with the exceptionof one study7 (systolic BP ≥ 170mmHg). In nine studies
(category A), the BP of eclamptic mothers was classifiedas mild-to-moderate hypertension and severe hyperten-sion.7,16,23,29,36,51,54,59,67 The other 10 studies classifiedthe BP of eclamptics as normotensive and hyperten-sive.25,31,33,38–40,60,68,70,73 Of the 1989 eclamptic women(category A), 7% had normal blood pressure; 35% hadmild-to-moderate hypertension, and 56% had severe hy-pertension. In category B, out of 1454 eclampticmothers, 48% and 50% were normotensive and hyper-tensive, respectively. With the exception of one study,36
most severe hypertension cases of eclampsia were re-ported from low-income and low–middle-incomecountries.16,23,27,29,45,51,56,72
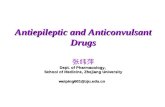
As shown in Figure 4,8–11,13,37,40,70,77–81 of 3443 eclamp-tic mothers, 25% were normotensive, 20% had mild-to-moderate hypertension, 32% had severe hypertension,and 21% were hypertensive but not otherwise classified.In total, about 45% of eclamptic women reviewed had ei-ther normal BP or mild-to-moderate hypertension.Sixteen studies reported some symptoms of pre-
eclampsia (Table 3,7,23,28,32,34,35,37–40,59,65,73,75,76 includingthe proportion of patients with headache and visual dis-turbance. Fourteen studies reported presence of epigas-tric area pain, and five studies reported vomiting. Inanother five studies, symptom-free cases were reported.Because some symptoms overlap and there were differ-ences in the denominators used across studies (somestudies did not include the presence or absence of someof the severity symptoms in their report), the percentageis not proportionally distributed.Headache was the commonest symptom in all in-
cluded studies (range: 45–80%). The second most com-monly reported symptom was visual disturbance. Of2163 eclamptic mothers, 66% and 27% had headacheand visual disturbance, respectively, preceding the
Figure 2 Flow diagram showing se-lection of studies.
Y. Berhan and A. Berhan
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
834

Table 1 General characteristics of the included studies. Total eclampsia cases = 21155
Author Country Study year Totaldeliveries
Totaleclampsia %
Antepartum%
Intrapartum%
Post-partum %
Zwart et al.7 Netherlands†† 2004–2006 358 874 222 (0.06) 39.0 33.0 28.0Alexander et al.9 USA†† 2000–2004 72 004 87 (0.1) ND ND NDNoor et al.16 Pakistan¶ 2000 3342 53 (1.6) 75.5† NA 24.5Abd El Aal21 Egypt¶ 1990–2010 ND 1998 79.8 4.6 15.7Conde-Agudelo et al.22 Colombia¶ 1993–1995 ND 125 57.6 21.6 20.8Cooray et al.23 Tanzania§ 2007–2008 3267 46 (1.4) 52.0 15.0 33.0Ekele et al.24 Nigeria¶ 1995–2004 15 318 657 (4.3) 26.3 67.3 6.4Al-Safi et al.§§25 USA†† 2003–2009 48 498 22 (0.05) NA NA 100.0Arora et al.26 India¶ 1984–1992 30 942 271 (0.9) 47.2 31.4 21.4Obed et al.27 Ghana¶ 1991 10 301 134 (1.3) 41.8 44.0 14.2Onuh et al.28 Nigeria¶ 1995–2002 7865 103 (1.3) 65.0 21.4 13.6Yaliwal et al.29 India¶ 2001–2010 5387 98 (1.8) ND ND NDAdenkale et al.30 Nigeria¶ 2005–2010 3952 83 (2.1) 54.2 22.9 22.9Rugarn et al.31 Sweden†† 1973–1999 53 782 39 (0.07) 41.0 33.0 27.0Sibai et al.32 USA†† 1977–1980 20 777 67 (0.3) 46.3 16.4 37.3Urassa et al.33 Tanzania§ 1999–2000 156 030 1077 (0.7) ND ND NDEkholm et al.34 Finland†† 1990–1994 324 658 77 (0.02) ND ND NDOkogbenin et al.35 Nigeria¶ 1999–2004 3095 74 (2.4) 41.8 31.1 27.0Andersgaaed et al.36 Scandinavia†† 1998–2000 420 309 210 (0.05) 40.0 29.0 31.0Katze et al.37 USA†† 2000 50 000 53 (0.1) 53.0 36.0 11.0Kayem et al.§§38 UK†† 2005–2006 779 437 75 (0.01) NA NA 100.0Knight et al.39 UK†† 2005–2006 ND 214 45.0 19.0 36.0Douglas et al.40 UK†† 1992 774 436 383 (0.05) 38.0 18.0 44.0Bhalerao et al.41 India¶ 2008–2010 6100 55 (0.9) 70.9 18.2 10.9Pal et al.42 India¶ 1999–2008 140 701 5991(4.3) 64.0 13.0 23.0Liu et al.43 Canada†† 2003–2010 1 910 729 1530 (0.08) 69.6 16.2 14.2Lubarsky et al.44 USA†† 1977–1992 112 500 334 (0.3) 71.0† NA 29.0Thapa et al.45 Nepal§ 2006–2007 5240 68 (1.3) 67.7 22.1 10.3Yakasai et al.46 Nigeria¶ 2008–2009 13 943 688 (4.9) 44.9 35.0 20.1Abdullah et al.47 Pakistan¶ 2009 2170 45 (2.0) 47.0 20.0 33.0Ndaboine et al.48 Tanzania§ 2009–2010 5562 76 (1.4) 67.1 22.4 10.5Adam et al.49 Sudan¶ 2007–2009 8894 45 (0.5)‡‡ 62.0 15.5 11.1Efetie et al.50 Nigeria¶ 2000–2005 5868 46 (0.8) 58.7 15.2 26.1Ade-Ojo et al.51 Nigeria¶ 1994–2003 13 682 124 (0.9) 56.5 25.0 18.5Buowari et al.52 Nigeria¶ 2004–2006 ND 58 81.0† NA 19.0Berhan et al.‡ Ethiopia§ 2006–2013 12 432 342 (2.8) 45.0 26.0 29.0Tukur et al.53 Nigeria¶ 2002–2005 2197 207 (9.4) 54.1 32.9 13.0Adam-Hondegla et al.54 Togo§ 2007–2009 ND 170 ND ND NDMuganyizi et al.55 Tanzania§ 2008 ND 366 73.8 6.8 19.4Agida et al.56 Nigeria¶ 2005–2008 4471 59 (1.3)‡‡ 73.9 19.6 2.2Olatunji et al.57 Nigeria¶ 1988–1997 5423 93 (1.7) 93.5 4.3 2.2Eke et al.58 Nigeria¶ 2004–2009 13 536 212 (1.6) 75.5 15.1 9.4Noraihan et al.59 Malaysia¶ 1999 24 000 50 (0.2) 64.0 20.0 16.0Morikawa et al.60 Japan†† 2005–2009 301 735 225 (0.07) ND ND NDAdetoro et al.61 Nigeria¶ 1968–1987 183 365 788 (0.4) 41.4 32.7 25.9Acquaah-Arhin et al.62 Ghana¶ 1998–2000 34 685 543 (1.6) 59.9 24.5 15.6Obiechina et al.63 Nigeria§ 1991–2000 15 692 102 (0.7) 38.0 14.7 46.0Okafor et al.64 Nigeria¶ 2001–2005 4857 40 (0.8) 52.6 15.8 31.6Chames et al.65 USA†† 1996–2001 ND 89 ND ND NDMatter et al.66 USA†† 1977–1998 141 254 399 (0.3) 53.0 19.0 28.0Boudaya et al.67 Tunisia¶ ND ND 28 78.7† NA 21.4Ducarme et al.68 France†† 1996–2006 19 655 16 (0.08) ND ND NDLee et al.69 Canada†† 1981–2000 248 013 70 (0.03) 61.0 13.0 26.0Turck et al.70 French Guiana†† 1996–2008 21 525 69 (0.3) 59.0 6.0 35.0Ahmad et al.71 Pakistan¶ 2000–2001 3090 96 (3.1) ND ND ND
(Continues)
Systematic review of reports on eclampsia
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
835

occurrence of convulsion. Out of 2053 eclampticmothers, 25% had epigastric area pain. Out of 759mothers with eclampsia, 17% had vomiting. Out of1092 mothers with eclampsia, 25% were asymptomaticpreceding the occurrence of convulsion (Fig. 4).
Discussion
Hypertension has long been recognized as a manifesta-tion of pre-eclampsia and a warning sign for occurrenceof eclampsia.3 However, because of themarked variationin blood pressure among eclamptic mothers, the degreeof hypertension may not always predict risk of eclamp-sia, as this review has demonstrated. Almost half of theeclamptic women included in this multi-country reviewwere not in a state of severe hypertension immediatelybefore seizure. This finding is in line with some previousinvestigators’ findings9,10 but contradictory to other
reports of low rate of eclampsia among women withmild pre-eclampsia.13,77
Because of the variable degree of hypertension amongeclamptic women and varying opinions of previousauthors,8–13,82 the question remains: should magnesiumsulfate be administered to all women with pre-eclampsia?This controversy persists in the absence of large ran-
domized clinical trials ofmagnesium sulfate prophylaxisforwomenwithmild-to-moderate hypertensionwithoutsevere symptoms8,14 and because the cause of eclampsiacontinues to be poorly understood.68,83 Based on our cur-rent review, nearly half of the cases of eclampsia oc-curred in the absence of severe hypertension andwithout any warning symptom or sign.37,68,70 In this re-view, 25% of 1092 eclamptic women were symptom-freeand 25% of 3443 eclamptic women had normal bloodpressure when the seizure occurred. Out of 18488eclamptic mothers, 21% experienced post-partumeclampsia, including a significant number of cases of latepost-partum eclampsia, highlighting the unpredictablenature of this disorder.Previous authors have also noted the challenges in
predicting eclampsia.16,37,67 Katz et al. concluded thateclampsia was not a progression from severe pre-eclampsia and recommended reevaluation of the USpractice,37 where seizure prophylaxis is recommendedonly for severe pre-eclampsia cases.8,78 Furthermore, alarge-scale study in the UK identified that most eclamp-tic convulsions occurred in hospitals, presumably unher-alded by warning signs or symptoms that would havewarranted seizure prophylaxis.40
This high number of women experiencing eclampsiawithout prodromal symptoms and signs implies thatthe traditionally thought natural course of eclampsia(gestational hypertension to mild pre-eclampsia to se-vere pre-eclampsia to eclampsia) may not be the reality,as Katz et al.37 and Douglas et al.40 previously recog-nized. Turk et al. reported that only 10% of eclampsia
Table 1 (Continued)
Author Country Study year Totaldeliveries
Totaleclampsia %
Antepartum%
Intrapartum%
Post-partum %
Konje et al.72 Nigeria¶ 1975–1986 37 313 347 (0.9) 30.6 46.2 23.2Chhabra et al.§§73 India¶ 1998–2009 39 050 101 (1.0) NA NA 100.0Leitch et al.74 Scotland†† 1931–1990 320 645 1259 (0.4) 44.0 33.0 23.0Abate et al.75 Ethiopia§ 1994–1999 35 741 257 (0.7) 61.6 22.7 15.7Echendu76 Nigeria 2009 6262 57 (0.9) ND ND ND
†Including intrapartum. ‡Unpublished data. §Low-income country. ¶Middle-income country. ††High-income country (WHO2013). ‡‡Some caseswere reported as unknown. §§Included only post-partum eclampsia cases. NA, not applicable; ND, no data or not defined.
Figure 3 Distribution of eclampsia by type. n=18488.Studies that reported antepartum and intrapartumeclampsia together or only post-partum eclampsia wereexcluded from this graph.
Y. Berhan and A. Berhan
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
836

cases were preceded by severe pre-eclampsia; and theyalso cited other investigators’ finding that 40–60% ofeclampsia manifested without pre-eclamptic pro-drome.70 This review lends further evidence to that argu-ment. In the current review, there was a significantnumber of eclamptic seizures that appeared to be in di-rect progression from a state of normotensive and mildor moderate hypertension.
The argument is, till future investigators develop asensitive and specific biomarker, we cannot do muchto prevent the occurrence of eclampsia among asymp-tomatic and normotensive pregnant women in theantepartum and post-partum periods. This was also
well noted by Sibai et al. as there are non-preventableeclampsia cases.84 However, taking into account thehuge number of women with mild-to-moderate hyper-tension who were found to have eclampsia, should wecontinue observing these women without administer-ing magnesium sulfate prophylaxis?As the limited knowledge about the pathogenesis is
a major problem for preventing and treating eclamp-sia,85 lack of consistent clinical symptoms and signsalso seems to continue being the major challenge toprevent eclampsia. The argument is: unless the avail-able sign (mild-to-moderate hypertension for the inter-est of this review) is taken as a warning for eclampsia
Table 2 Pattern of hypertension among women with eclampsia
A.
Author Sample size Normotensive n (%) †Mild-to-moderatehypertension n (%)
‡Severehypertension %
Studyreported from
Agida et al.45 46¶ 1 (2.2) 11 (23.9) 32 (69.6) LMICKonje et al.56 347 37 (10.7) 105 (30.3) 205 (59.0) LMICObed et al.72 134 3 (2.2) 48 (35.8) 83 (62.0) LMICThapa et al.27 68 3 (4.4) 34 (50.0) 31 (45.6) LICKatze et al.37 53 45(85.0) 1 (2.0) 7 (13.0) HICBerhan†† 342 27 (7.9) 151 (44.1) 164(48.0) LICAlexander et al.9 87¶ 32 (36.8) 27 (31.0) 11 (12.6) HICCooray et al.23 46 16 (35.0) 30 (65.0) LICZwart et al.7 139 90 (64.8) 49 (35.2)§ HICNoor et al.16 53 18 (34.0) 35 (66.0) LMICAdama-Hondeglaet al.54
170 50 (29.4) 120 (70.6) LIC
Andersgaaedet al.36
210¶ 42 (20.0) 158 (75.0) HIC
Noraihan et al.59 50¶ 25 (50.0) 19 (38.0) UMICBoudaya et al.67 28 14 (50.0) 14 (50.0) UMICAde-Ojo et al.51 124 31 (25.0) 93 (75.0) LMICYaliwal et al.29 98 41 (41.8) 57 (58.2) LMICTotal 1995¶ 148 (7.4) 704 (35.3) 1108 (55.5)
B.
Author Sample size Normotensive n (%) Hypertensive (mild to severe)‡‡ n (%)
Douglas et al.40 294 112 (38.0) 182 (62.0) HICTurck et al.70 69 43 (62.0) 26 (37.8) HICUrassa et al.33 399 288 (72.2) 111 (27.8) LICAl-Safi et al.25 22 17 (77.3) 5 (22.7) HICRugarn et al.31 39 16 (41.0) 23 (59.0) HICChhabra et al.73 101¶ 5 (4.9) 85 (84.2) LMICKayem et al.38 75¶ 28 (37.3) 37 (49.3) HICKnight et al.39 214 113 (53.0) 101 (47.0) HICMorikawa et al.60 225 75 (33.3) 150 (66.7) HICDucarme et al.68 16 4 (25.0) 12 (75.0) HICTotal 1454¶ 701 (48.2) 732 (50.3)
†Includes patients with systolic blood pressure of 140–160mmHg and/or diastolic blood pressure of 90–110mmHg. ‡Includes patients with sys-tolic blood pressure of >160mmHg and/or diastolic blood pressure of >110mmHg. §Systolic Bp> =170mmHg. ¶Some cases are not reported(total = 56). ††Unpublished data. ‡‡The primary studies reported it as hypertensive. LIC, low-income country; LMIC, low–middle-income coun-try; UMIC, upper middle income country; HIC, high-income country (Source: WHO world health statistics 2013).
Systematic review of reports on eclampsia
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
837

and serious consideration is given for administeringmagnesium sulfate, several mothers may be at risk ofeclampsia. Thus, till a multicenter double-blind ran-domized clinical trial disproves it otherwise, adminis-tering magnesium sulfate prophylaxis for all womenwith evidences of pre-eclampsia seems imperativeand reasonable.
Similar recommendations were issued by several pre-vious authors.9,37,79–81 For instance, with the restrictiveadministration of magnesium sulfate, the study byAlexander et al. has demonstrated a potential doublingin the incidence of eclampsia and increased adversematernal and neonatal outcomes directly related to ex-cess seizures among women with mild gestational hy-pertension who were observed without magnesiumsulfate.9
Some authors have recommended restrictive use ofmagnesium sulfate due to low incidence of eclampsiain women with mild pre-eclampsia, and due to concernsthat adverse effects of magnesium sulfate could out-weigh the risk of eclampsia.11,14,18 However, other evi-dence may not support this conclusion.First, as several studies9,10,40,70 and this multi-country
article review have shown, the incidence of eclampsiais not lower among women with mild pre-eclampsia.Second, the two clinical trials12,13 that have been citedas evidence to withhold magnesium sulfate prophylaxisfor women with mild pre-eclampsia were done by en-rolling a small number of patients, which makes thepower too low for a valid conclusion.18 Third, seriousmagnesium sulfate toxicity is not as common as antici-pated by some authors.9,11,14,16,18,45,86–88 However, it
Figure 4Distribution of hypertensionand selected severe symptoms pre-ceding the onset of convulsionamong women diagnosed witheclampsia.
Y. Berhan and A. Berhan
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
838

should be noted that a significant reduction in fetal um-bilical artery andmiddle cerebral artery pulsatility indexwas seen in 24 women with mild pre-eclampsia treatedwith magnesium sulfate.89
Fourth, the complications due to eclampsia may bemore catastrophic to the mother and the baby than com-plications that may be attributed to magnesium sulfatetoxicity. Eclampsia accounts for about 63000 maternaldeaths worldwide; 99% of these deaths occurred in de-veloping countries, mainly because of late reportingand late initiation of seizure prophylaxis.90 Two largerandomized trials have shown very few life-threateningside-effects of magnesium sulfate, which were manage-able by discontinuing the drug or by administering cal-cium gluconate.86,87
While serious magnesium sulfate toxicity does rarelyoccur, such toxicity can be prevented and treated andcarries less long-term morbidity and mortality risk thaneclampsia. Adamu et al. noted that maternal outcomewas poor even after introduction of magnesium sulfatefor eclamptic women.91 As a concluding remark, theysaid, ‘Interventions for reduction ofmaternal and perina-tal mortality must emphasize strategies that prevent theoccurrence of eclampsia’, a view which is shared by theauthors of this review.
From the perspective of cost-effectiveness, the analysisfrom theMagpie Trial concluded thatmagnesium sulfatefor pre-eclampsia costs less and prevents more eclamp-sia in low gross national income (GNI) countries thanin high GNI countries.92
This review hasmultiple limitations. Almost all the in-cluded studies were based in one or a few hospitals,
which may not be representative of the general popula-tion in the study area or the cited country. The descrip-tive and case series nature of all the included studieslimited the possibility of conducting further analysis.The inconsistent classification of hypertension by someauthors has probably underestimated the proportion ofeclamptic women with mild-to-moderate hypertensionor severe hypertension. Because of the retrospective na-ture of the included studies, some of the eclampticwomen might have been misclassified due to inaccessi-bility immediately preceding the onset of seizure. Aseclampsia is characterized by generalized tonic–clonicseizure or coma, the severe symptoms are liable to be for-gotten by the patients themselves or might not be re-ported by relatives or accompaniers.In conclusion, in this rigorous review, antepartum
eclampsia accounted for nearly three-fifths of all eclamp-sia cases, and women with intrapartum and post-partum eclampsia were proportional. One-fourth of theeclamptic women were normotensive; one-fifth hadmild-to-moderate hypertension; and nearly one-thirdhad severe hypertension. Headache was the most com-mon symptom in all eclamptic women. Because of littleclinical trial evidence that objects to universal magne-sium sulfate prophylaxis, the high number of womenwith mild pre-eclampsia or without warning symptomswho developed eclampsia, and the relatively low andmanageable severe magnesium sulfate toxicity, it is im-perative to continue administering magnesium sulfateprophylaxis to women with mild pre-eclampsia till aconvincing randomized trial result contradicts or con-firms this strategy.
Table 3 Distribution of selected severity symptoms in women with eclampsia
Author Eclampsiacases
Headache%
Visual disturbance%
Epigastric pain%
Vomiting%
Symptom free%
Katze et al.37 53 64.0 30.0 ND NR NACooray et al.23 46 80.0 46.0 20.0 NR NAChames et al.65 89 70.0 30.0 12.0 NA NAEkholm et al.34 77 66.0 19.0 23.0 8.0 NASibai et al.32 67 82.5 44.4 19.0 NA NAOkogbenin et al.35 74 74.3 21.6 14.9 10.8 NAKnight et al.39 214 56.0 23.0 17.0 NA NAChhabra et al.73 101 57.4 6.9 3.9 NA 20.6Kayem et al.38 75 45.3 17.0 16.0 NA NANoraihan et al.59 50 66.0 24.0 36.0 28.0 14.0Douglas et al.40 383 50.0 19.0 19.0 NA 41.0Zwart et al.7 222 69.0 41.0 45.0 28.0 10.8Onuh et al.28 103 82.4 10.6 7.0 NA NAAbate et al.75 216 83.8 41.6 38.4 NA NAEchendu76 57 74.0 65.0 NA NA NABerhan† 342 74.9 42.1 34.9 11.3 19.0
†Unpublished data. NA, Not applicable; ND, No data; NR, Not reported.
Systematic review of reports on eclampsia
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
839

Disclosure
The authors would like to declare that there is no conflictof interest. There was no financial support for this work.
References
1. World Health Organization (WHO). WHO recommendationfor prevention of preeclampsia and eclampsia. 2011. Geneva.[Cited July 2014.] Available from URL: www.who.int/reproductivehealth/publications/maternal_perinatal_health/
2. Stoppler MC, Davis CP. Eclampsia. [Cited July 2014.] Availablefrom URL: http://www.emedicinehealth.com/eclampsia/
3. Bell MJ. A historical overview of preeclampsia-eclampsia. A JObstet Gynecol Neonatal Nurs 2010; 39: 510–518.
4. Duley L, Henderson-Smart D. Magnesium sulphate versus di-azepam for eclampsia. Cochrane Database Syst Rev 2003; 4:CD000127.
5. Abalos E, Cuesta C, Grosso AL, Chou D, Say L. Global and re-gional estimates of preeclampsia and eclampsia: A systematicreview. Eur J Obstet Gynecol Reprod Biol 2013; 170: 1–7.
6. Duley L. The global impact of pre-eclampsia and eclampsia.Semin Perinatol 2009; 33: 130–137.
7. Zwart JJ, Richters A, Ory F, de Vries JI, Bloemenkamp KW, vanRoosmalen J. Eclampsia in the Netherlands. Obstet Gynecol2008; 112: 820–827.
8. The American College of Obstetricians and Gynecologists(ACOG). Hypertension in pregnancy 2013. [Cited July 2014.]Available from URL: http://www.acog.org/Resources_And_Publications/
9. Alexander JM, McIntire DD, Leveno KJ, Cunningham FG. Se-lective magnesium sulfate prophylaxis for the prevention ofeclampsia in women with gestational hypertension. ObstetGynecol 2006; 108: 826–832.
10. Foong SC, Pollard JK. Eclampsia in Southern Alberta: Is there arole for seizure prophylaxis in all women with gestational hy-pertension? J Obstet Gynaecol Can 2003; 25: 385–389.
11. Rozenberg P. Magnesium sulfate for the management of pre-eclampsia. Gynecol Obstet Fertil 2006; 34: 54–59.
12. Livingston JC, Livingston LW, Ramsey R, Mabie BC, SibaiBM. Magnesium sulfate in women with mild preeclampsia:A randomized controlled trial. Obstet Gynecol 2003; 101:217–220.
13. Witlin AG, Friedman SA, Sibai BM. The effect of magnesiumsulfate therapy on the duration of labor in women with mildpreeclampsia at term: A randomized, double blind, placebo-controlled trial. Am J Obstet Gynecol 1997; 176: 623–627.
14. Sibai BM. Magnesium sulfate prophylaxis in preeclampsia:Evidence from randomized trials. Clin Obstet Gynecol 2005;48: 478–488.
15. Scott JR. Magnesium sulfate for mild preeclampsia. ObstetGynecol 2003; 101: 213.
16. Noor S, Halimi M, Faiz NR, Gull F, Akbar N. Magnesium sul-fate in the prophylaxis and treatment of eclampsia. J AyubMed Coll Abbottabad 2004; 16: 50–54.
17. Lim K-H, Steinberg G, Ramus RM. Preeclampsia. Updated 24February 2014. [Cited July 2014.] Available from URL:http://emedicine.medscape.com/
18. Sibai BM. Magnesium sulfate prophylaxis in preeclampsia:Lessons learned from recent trials. Am J Obstet Gynecol2004; 190: 1520–1526.
19. Royal College ofObstetricians andGynecologists. GuidelineNo.10 (A). The management of severe preeclampsia/eclampsia,2006. [Cited July 2014.] Available from URL: http://www.neonatalformulary.com/pdfs/uk_guidelines/
20. Abalos E, Duley L, Steyn DW. Antihypertensive drug therapyfor mild to moderate hypertension during pregnancy. CochraneDatabase Syst Rev 2014; CD002252. doi: 10.1002/14651858.CD002252.pub3.
21. Abd El Aal DE, Shahin AY. Management of eclampsia atAssiut University Hospital, Egypt. Int J Gynaecol Obstet2012; 116: 232–236.
22. Conde-Agudelo A, Kafury-Goeta AC. Case-control study ofrisk factors for complicated eclampsia. Obstet Gynecol 1997;90: 172–175.
23. Cooray SD, Edmonds SM, Tong S, Samarasekera SP,Whitehead CL. Characterization of symptoms immediatelypreceding eclampsia. Obstet Gynecol 2011; 118: 995–999.
24. Ekele BA, Bello SO, Adamu AN. Clusters of eclampsia in a Ni-gerian teaching hospital. Int J Gynaecol Obstet 2007; 96: 62–66.
25. Al-Safi Z, Imudia AN, Filetti LC, Hobson DT, Bahado-SinghRO, Awonuga AO. Delayed postpartum preeclampsia andeclampsia: Demographics, clinical course, and complications.Obstet Gynecol 2011; 118: 1102–1107.
26. Arora R, Ganguli RP, Swain S, Oumachigui A, Rajaram P. De-terminants of maternal mortality in eclampsia in India. AustNZ 3 Obstet Gynaecol 1994; 34: 537–539.
27. Obed SA, Wilson JB, Elkins TE. Eclampsia: 134 consecutivecases. Int J Gynaecol Obstet 1994; 45: 97–103.
28. Onuh SO, Aisien AO. Maternal and fetal outcome ineclamptic patients in Benin City, Nigeria. J Obstet Gynaecol2004; 24: 765–768.
29. Yaliwal RG, Jaju PB, VanishreeM. Eclampsia and perinatal out-come: A retrospective study in a teaching hospital. J Clin DiagnRes 2011; 5: 1056–1059.
30. Adekanle DA,Akinbile TO. Eclampsia andpregnancy outcomeat Lautech Teaching Hospital, Osogbo, South West, Nigeria.Clin Mother Child Health 2012; 9. doi: 10.4303/cmch/C120301.
31. Rugarn O, Carling Moen S, Berg G. Eclampsia at a tertiary hos-pital 1973-99. Acta Obstet Gynecol Scand 2004; 83: 240–245.
32. Sibai BM, McCubbin JH, Anderson GD, Lipshitz J, Dilts PV Jr..Eclampsia I. Observations from 67 recent cases. Obstet Gynecol1981; 58: 609–613.
33. Urassa DP, Carlstedt A, Nyström L, Massawe SN, LindmarkG. Eclampsia in Dar es Salaam, Tanzania: Incidence, out-come, and the role of antenatal care. Acta Obstet GynecolScand 2006; 85: 571–578.
34. Ekholm E, Salmi MM, Erkkola R. Eclampsia in Finland in1990-1994. Acta Obstet Gynecol Scand 1999; 78: 877–882.
35. Okogbenin SA, Eigbefoh JO, Omorogbe F, Okogbo F, OkontaPI, Ohihoin AG. Eclampsia in Irrua Specialist Teaching Hospi-tal: A five-year review. Niger J Clin Pract 2010; 13: 149–153.
36. Andersgaard AB, Herbst A, Johansen M et al. Eclampsia inScandinavia: Incidence, substandard care, and potentially pre-ventable cases. Acta Obstet Gynecol Scand 2006; 85: 929–936.
37. Katz VL, Farmer R, Kuller JA. Preeclampsia into eclampsia: To-ward a newparadigm.Am JObstet Gynecol 2000; 182: 1389–1396.
38. Kayem G, Kurinczuk JJ, Spark P, Brocklehurst P, Knight M,UK Obstetric Surveillance System (UKOSS). Maternal and
Y. Berhan and A. Berhan
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
840

obstetric factors associated with delayed postpartum eclamp-sia: A national study population. Acta Obstet Gynecol Scand2011; 90: 1017–1023.
39. Knight M , UKOSS. Eclampsia in the United Kingdom 2005.BJOG 2007; 114: 1072–1078.
40. Douglas KA, Redman CWG. Eclampsia in the United King-dom. BMJ 1994; 309: 1395–1400.
41. Bhalerao A, Kulkarni S, Ghike S, Kawthalkar A, Joshi S,Somalwar S. Eclampsia: Maternal and Fetal Outcome. J SouthAsian Feder Obst Gynae 2013; 5: 19–21.
42. Pal A, Bhattacharyya R, Adhikari S et al. Eclampsia-scenario ina hospital: a ten years study. Bangladesh Med Res Counc Bull2011; 37: 66–70.
43. Liu S, Joseph KS, Liston RM et al. Incidence, risk factors, andassociated complications of eclampsia. Obstet Gynecol 2011;118: 987–994.
44. Lubarsky SL, Barton JR, Friedman SA, Nasreddine S, RamadanMK, Sibai BM. Late postpartum eclampsia revisited. ObstetGynecol 1994; 83: 502–505.
45. Thapa K, Jha R. Magnesium sulfate: A lifesaving drug. JNMA JNepal Med Assoc 2008; 47: 104–108.
46. Yakasai IA, Gaya SA. Maternal and fetal outcome in patientswith eclampsia at Murtala Muhammad Specialist HospitalKano, Nigeria. Ann Afr Med 2011; 10: 305–309.
47. Abdullah A, Shaikh AA, Jamro B. Maternal and perinatal out-come associated with eclampsia in a teaching hospital, Sukkur.Rawal Med J 2010; 35: 23–26.
48. Ndaboine EM, Kihunrwa A, Rumanyika R, Im HB, MassindeAN. Maternal and perinatal outcomes among eclampticpatients admitted to Bugando Medical Centre, Mwanza,Tanzania. Afr J Reprod Health 2012; 16: 35–41.
49. Adam GK, Bakheit KH, Adam I. Maternal and perinataloutcomes of eclampsia in Gadarif Hospital, Sudan. J ObstetGynaecol 2009; 29: 619–620.
50. Efetie ER, Okafor UV. Maternal outcome in eclamptic pa-tients in Abuja, Nigeria: A 5 year review. Niger J Clin Pract2007; 10: 309–313.
51. Ade-Ojo IP, Loto OM. Outcome of eclampsia at the ObafemiAwolowo University Teaching Hospital Complex, Ile-Ife. NigerJ Clin Pract 2008; 11: 279–284.
52. Buowari YD. Pattern and outcome of eclampsia managed at ageneral hospital in North-West, Nigeria. Niger Health J 2012;12: 86–89.
53. Tukur J, Umar BA, Rabi’u A. Pattern of eclampsia in a tertiaryhealth facility situated in a semi-rural town in NorthernNigeria. Ann Afr Med 2007; 6: 164–167.
54. Adama-Hondegla AB, Lawson-Evi K, Bassowa A, Modji S,EgblaK-F, AkbadzaK. Perinatalmortality risk factors of infantsborn from eclamptic mothers at Tokoin teaching hospital ofLome. J Med Sci 2013; 13: 391–395.
55. Muganyizi PS, Shagdara MS. Predictors of extra care amongmagnesium sulfate treated eclamptic patients at MuhimbiliNational Hospital, Tanzania. BMC Pregnancy Childbirth 2011;11: 41.
56. Agida ET, Adeka BI, Jibril KA. Pregnancy outcome ineclamptics at the University of Abuja Teaching Hospital,Gwagwalada, Abuja: A 3 year review. Niger J Clin Pract2010; 13: 394–398.
57. Olatunji AO, Sule-Odu AO. Presentation and outcome ofeclampsia at a Nigerian university hospital. Niger J Clin Pract2007; 10: 1–4.
58. Eke AC, Ezebialu IU, Okafor C. Presentation and outcome ofeclampsia at a tertiary center in South East Nigeria: A 6-year re-view. Hypertens Pregnancy 2011; 30: 125–132.
59. Noraihan MN, Sharda P, Jammal AB. Report of 50 cases ofeclampsia. J Obstet Gynaecol Res 2005; 31: 302–309.
60. Morikawa M, Cho K, Yamada T, Yamada T, Sato S, MinakamiH. Risk factors for eclampsia in Japan between 2005 and 2009.Int J Gynaecol Obstet 2012; 117: 66–68.
61. Adetoro OO. The pattern of eclampsia at the University ofIlorin Teaching Hospital (U.I.T.H.) Ilorin, Nigeria. Int J GynaecolObstet 1990; 31: 221–226.
62. Acquaah-Arhin R, Kwawukume EY. Trends in eclampsia atKorle Bu teaching hospital, Accra Ghana. Niger J Clin Pract2003; 6: 1–4.
63. Obiechina NJ, Udigwe GO. Pattern of eclampsia in Onitsha,Nigeria. Orient J Med 2004; 16: 16–20.
64. Okafor UV, Efetie RE. Critical care management of eclamptics:Challenges in an African setting. Trop Doct 2008; 38: 11–13.
65. Chames MC, Livingston JC, Ivester TS, Barton JR, Sibai BM.Late postpartum eclampsia: A preventable disease?Am J ObstetGynecol 2002; 186: 1174–1177.
66. Mattar F, Sibai BM. Eclampsia. VIII. Risk factors for maternalmorbidity. Am J Obstet Gynecol 2000; 182: 307–312.
67. Boudaya F, Zouaoui B, Ghodhbene I et al. Eclampsia: Epidemi-ological aspects and management of 28 patients. Tunis Med2008; 86: 685–688.
68. Ducarme G, Herrnberger S, Pharisien I, Carbillon L, Uzan M.Eclampsia: Retrospective study about 16 cases. Gynecol ObstetFertil 2009; 37: 11–17.
69. Lee W, O’Connell CM, Baskett TF. Maternal and perinatal out-comes of eclampsia: Nova Scotia, 1981-2000. J Obstet GynaecolCan 2004; 26: 119–123.
70. Turck M, Carles G, El Guindi W, Helou G, Alassas N, DreyfusM. Sixty-nine consecutive cases of eclampsia: Prodromesand circumstances. J Gynecol Obstet Biol Reprod (Paris) 2011;40: 340–347.
71. Ahmad S, Nazli R, Lutfullah G. Frequency of eclampsia andmaternal complications in a tertiary care facility of Peshawar.Pak J Med Res2008; 47. [Cited July 2014.] Available from URL:http://www.pmrc.org.pk/eclampsia-peshawar.htm
72. Konje JC, Obisesan KA, Odukoya OA, Ladipo OA. Presenta-tion and management of eclampsia. Int J Gynecol Obstet 1992;38: 31–35.
73. Chhabra S, Tyagi S, Bhavani M, Gosawi M. Late postpartumeclampsia. J Obstet Gynaecol 2012; 32: 264–266.
74. Leitch CR, Cameron AD, Walker JJ. The changing pattern ofeclampsia over a 60-year period. Br J Obstet Gynaecol 1997;104: 917–922.
75. Abate M, Lakew Z. Eclampsia a 5 years retrospective review of216 cases managed in two teaching hospitals in Addis Ababa.Ethiop Med J 2006; 44: 27–31.
76. Echendu DA. Pattern of clinical presentation of eclampsia atNnamdi Azikiwe University Teaching Hospital, Nnewi, South-eastern Nigeria. Niger J Med 2012; 21: 313–316.
77. Hall DR, Odendaal HJ, Smith M. Is the prophylactic adminis-tration of magnesium sulfate in women with pre-eclampsia in-dicated prior to labour? BJOG 2000; 107: 903–908.
78. The American College of Obstetricians and Gynecologists(ACOG). Clinical management guidelines for obstetrician-Gynecologists number 33, 2002. Diagnosis and managementof preeclampsia and eclampsia. ACOG practice bulletin 2002;
Systematic review of reports on eclampsia
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
841

99. [Cited July 2014.] Available from URL: http://www.acog.org/Resources_And_Publications/
79. Wolfe DS, Williams SF, Ross MG, Beall MH, Apuzzio JJ. Doespreeclampsia predict the risk of late postpartum eclampsia?AJP Rep 2013; 3: 13–16.
80. Scott JR. Preventing eclampsia: Magnesium sulfate regimensrevisited. Obst Gynecol 2006; 108: 824–825.
81. Barclay L, NghiemHT.Magnesium sulfatemay benefit patientswith mild gestational hypertension. Medscape 2006; [Cited July2014.] Available from URL: http://www.medscape.org/viewarticle/545483.
82. Appleton MP, Kuchl TJ, Rebel MA, Adams HR, Knight AB,GoldWR.Magnesium sulfate versus phenytoin for seizure pro-phylaxis in pregnancy induced hypertension.Am JObst Gynecol1991; 165: 907–913.
83. Mathew R, Raj RS, Sudha P. Late postpartum eclampsia with-out prodroma. Neurol India 2003; 51: 539–540.
84. Sibai BM, Abdella TN, Spinnato JA, Anderson GD. Eclampsia.V. The incidence of nonpreventable eclampsia. Am J ObstetGynecol 1986; 154: 581–586.
85. Aagaard-TilleryKM, BelfortMA. Eclampsia:Morbidity,mortal-ity, and management. Clin Obstet Gynecol 2005; 48: 12–23.
86. The Eclampsia Trial Collaborative Group. Which anticonvul-sant for women with eclampsia? Evidence from the Collabora-tive Eclampsia Trial. Lancet 1995; 345: 1455–1463.
87. Altman D, Carroli G, Duley L et al. Magpie Trial CollaborationGroup. Dowomenwith pre-eclampsia, and their babies, benefitfrom magnesium sulfate? The Magpie Trial: A randomizedplacebo-controlled trial. Lancet 2002; 359: 1877–1890.
88. Umezurike CC, Feyi-Waboso PA, Whittaker RC. Treatment ofeclampsia with magnesium sulfate in Aba, South-EasternNigeria. Trop J Obstet Gynaecol 2006; 25: 20–22.
89. Dasgupta S, Ghosh D, Seal SL, Kamilya G, Karmakar M,Saha D. Randomized controlled study comparing effect ofmagnesium sulfate with placebo on fetal umbilical arteryand middle cerebral artery blood flow in mild preeclampsiaat ≥ 34weeks gestational age. J Obstet Gynaecol Res 2012; 38:763–771.
90. Langer A, Villar J, Tell K, Kim T, Kennedy S. Reducingeclampsia-related deaths: A call to action. Lancet 2008;371: 705–706.
91. Adamu AN, Ekele BA, Ahmed Y, Mohammed BA, IsezuoSA, Abdullahpi AA. Pregnancy outcome in women witheclampsia at a tertiary centre in northern Nigeria. Afr J MedSci 2012; 41: 211–219.
92. Simon J, Gray A, Duley L. Magpie Trial CollaborativeGroup. Cost-effectiveness of prophylactic magnesiumsulphate for 9996 women with pre-eclampsia from 33countries: Economic evaluation of the Magpie Trial. BJOG2006; 113: 144–151.
Y. Berhan and A. Berhan
© 2015 The AuthorsJournal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology
842

Copyright of Journal of Obstetrics & Gynaecology Research is the property of Wiley-Blackwell and its content may not be copied or emailed to multiple sites or posted to a listservwithout the copyright holder's express written permission. However, users may print,download, or email articles for individual use.