Shawn A. McClure D.M.D., M.D. - Baptist Health lesions.pdfShawn A. McClure D.M.D., M.D. Miami Oral &...
161
Shawn A. McClure D.M.D., M.D. Miami Oral & Maxillofacial Surgeon Associate Professor, Director of Research Department of Oral & Maxillofacial Surgery NOVA/NSU COLLEGE OF DENTAL MEDICINE 1
Transcript of Shawn A. McClure D.M.D., M.D. - Baptist Health lesions.pdfShawn A. McClure D.M.D., M.D. Miami Oral &...

Shawn A. McClure D.M.D., M.D.Miami Oral & Maxillofacial Surgeon
Associate Professor, Director of ResearchDepartment of Oral & Maxillofacial SurgeryNOVA/NSU COLLEGE OF DENTAL MEDICINE
1

Diseases of Head and Neck: What Should a Primary Care Physician Be Looking For?
June 22nd, 2012
If the patient complains of a painless mass or “lump” in the neck, what initial examination should the physician proceed to do immediately?
Look in the oral cavity
3
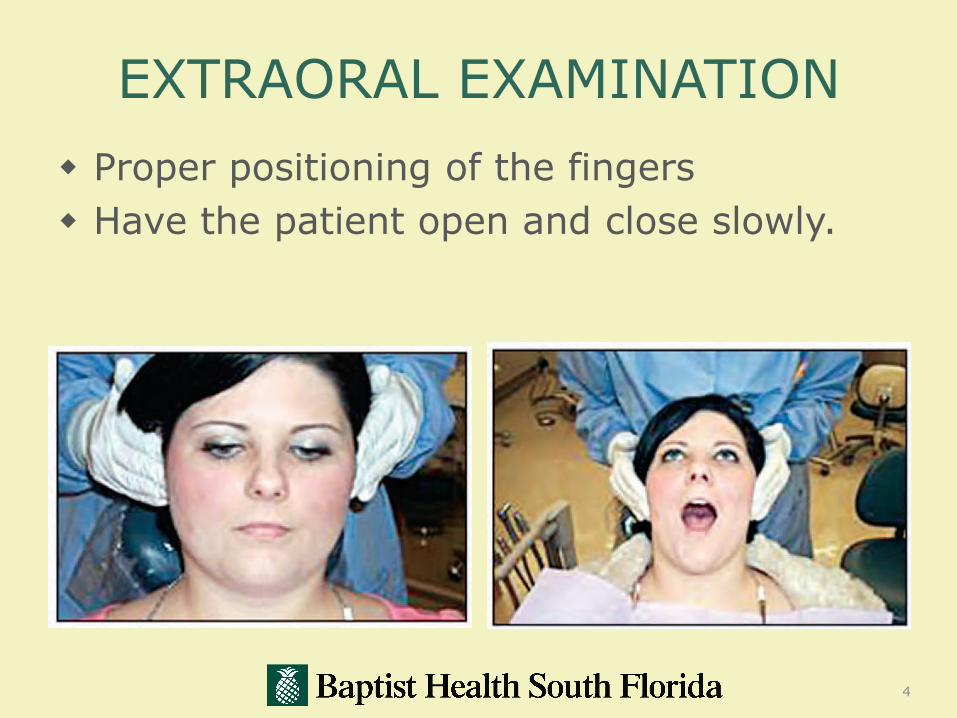
EXTRAORAL EXAMINATION
Proper positioning of the fingers
Have the patient open and close slowly.
4

EXTRAORAL EXAM
5

EXTRAORAL EXAMINATION
Preauricular nodes.
Palpation of the anterior cervical nodes.
6

EXTRAORAL EXAMINATION
Bilateral palpation of the occipital nodes. Be sure to also observe the skin in this area.
Postauricular nodes.
7

EXTRAORAL EXAMINATION
Palpation of the posterior cervical nodes.
Bilateral palpation of the supraclavicular lymph nodes.
8
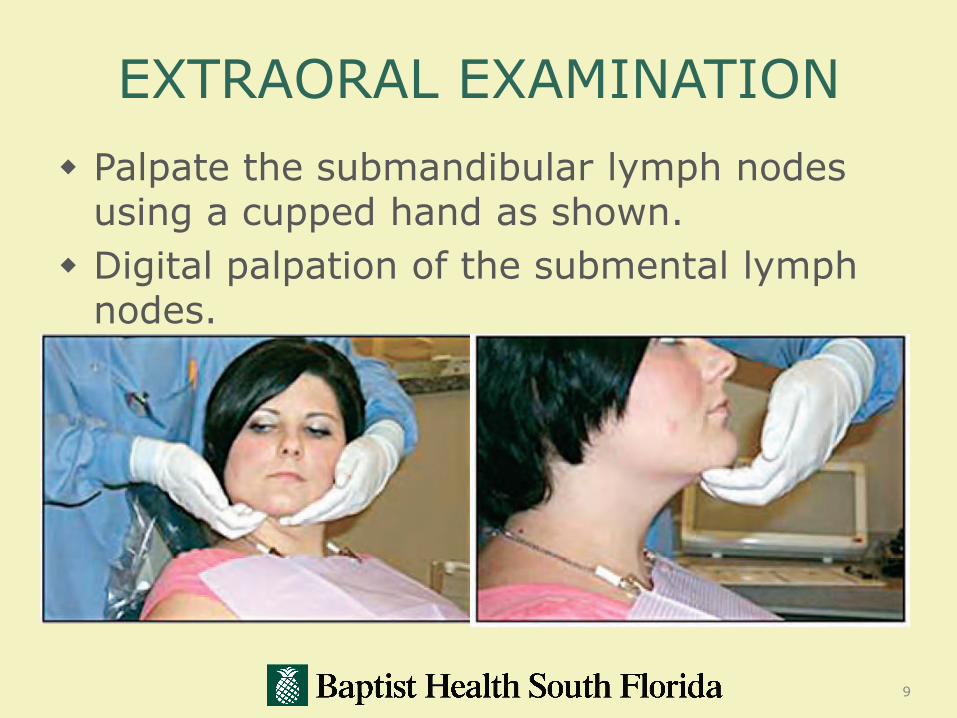
EXTRAORAL EXAMINATION
Palpate the submandibular lymph nodes using a cupped hand as shown.
Digital palpation of the submental lymphnodes.
9
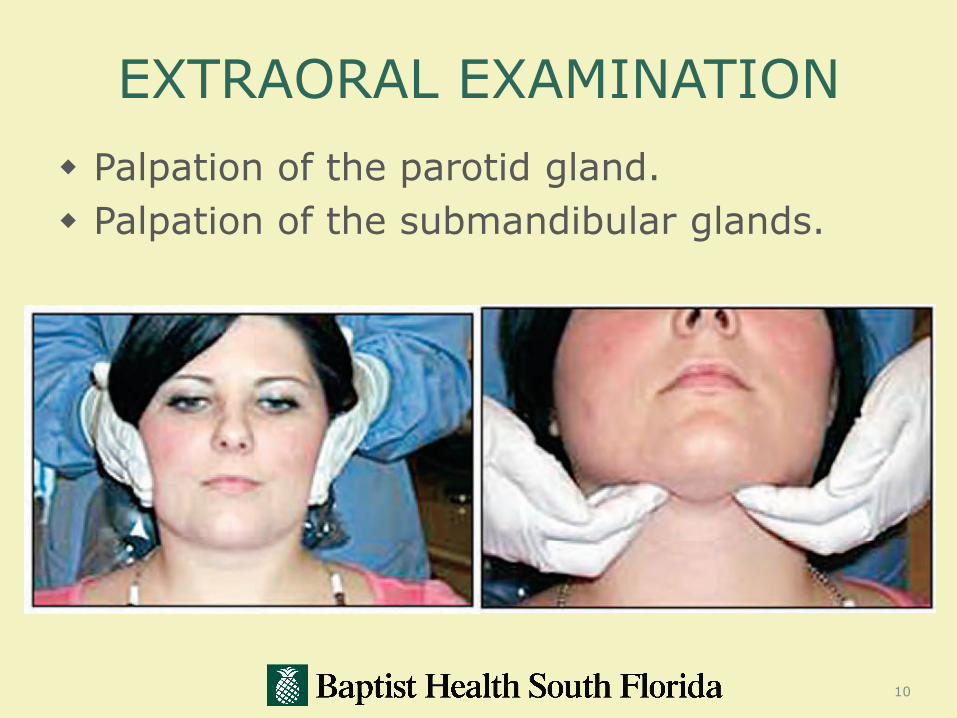
EXTRAORAL EXAMINATION
Palpation of the parotid gland.
Palpation of the submandibular glands.
10

EXTRAORAL EXAMINATION
Bimanual palpation of the thyroid gland.
Hold the fingers lightly over the gland while the patient swallows.
11
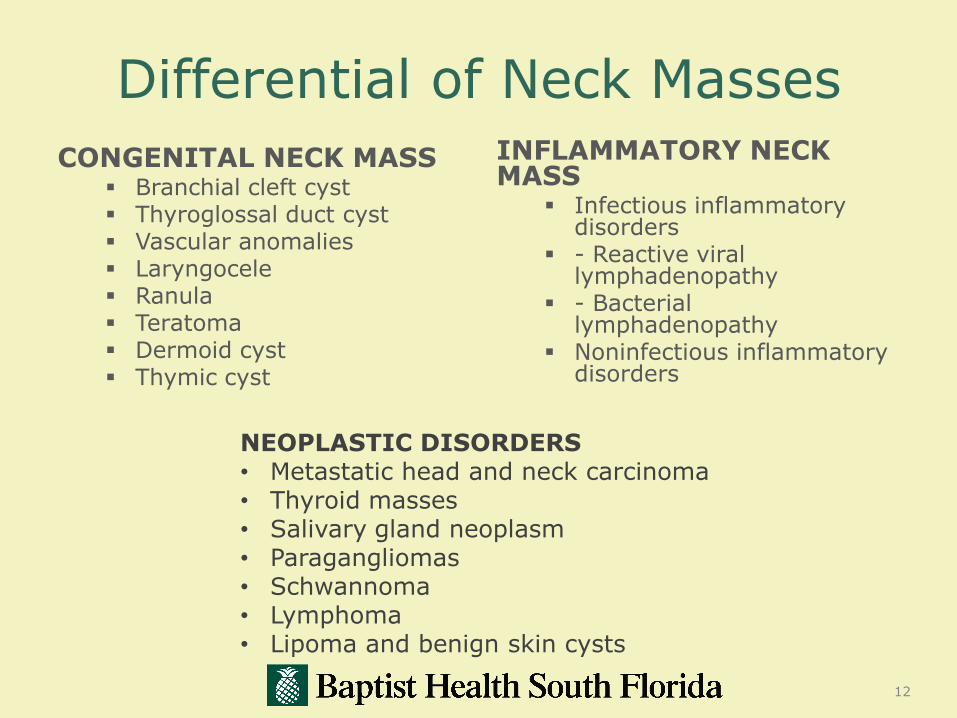
Differential of Neck Masses
CONGENITAL NECK MASS Branchial cleft cyst Thyroglossal duct cyst Vascular anomalies Laryngocele Ranula Teratoma Dermoid cyst Thymic cyst
INFLAMMATORY NECK MASS
Infectious inflammatory disorders
- Reactive virallymphadenopathy
- Bacteriallymphadenopathy
Noninfectious inflammatory disorders
12
NEOPLASTIC DISORDERS• Metastatic head and neck carcinoma• Thyroid masses• Salivary gland neoplasm• Paragangliomas• Schwannoma• Lymphoma• Lipoma and benign skin cysts

Dermoid Cyst
13
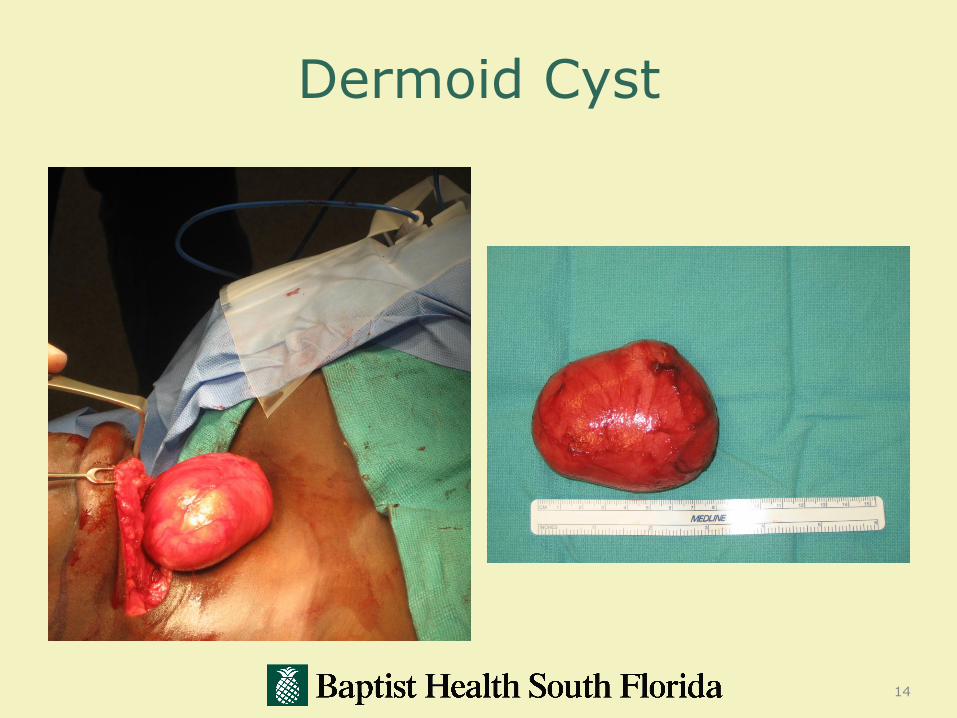
Dermoid Cyst
14

INTRAORAL EXAMINATION
15

Proper Head & Neck Examination
16

17
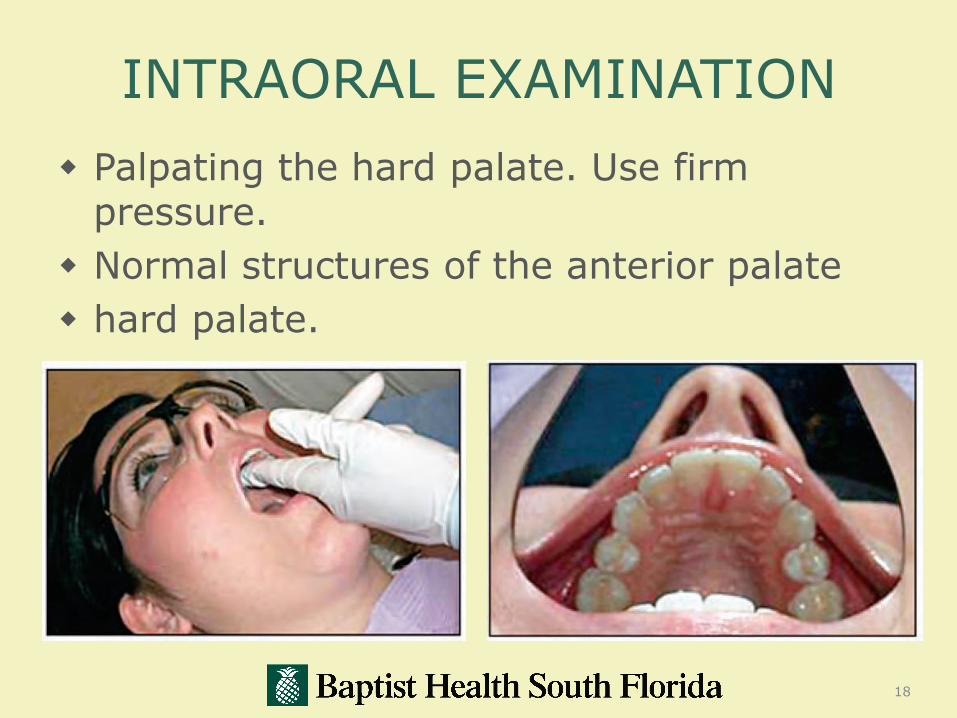
INTRAORAL EXAMINATION
Palpating the hard palate. Use firm pressure.
Normal structures of the anterior palate
hard palate.
18

INTRAORAL EXAMINATION Normal structures of the posterior hard
palate. Observe the dimensions (height and width) of the vault.
19
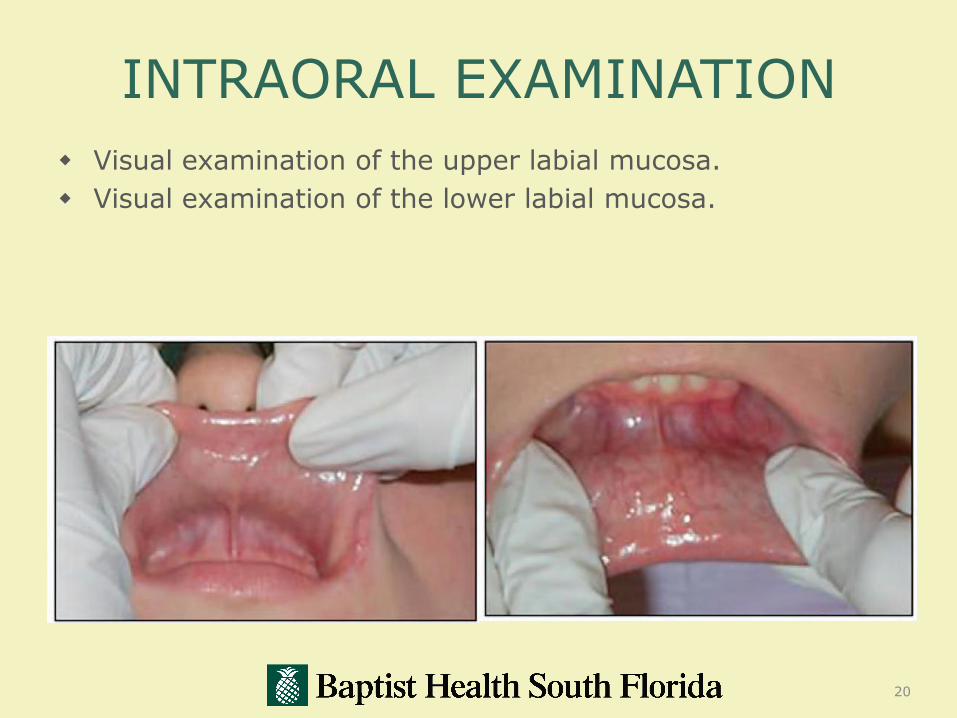
INTRAORAL EXAMINATION
Visual examination of the upper labial mucosa.
Visual examination of the lower labial mucosa.
20

INTRAORAL EXAMINATION
Use digital palpation pressing the tissues against the body of the mandible for both the lingual and the facial aspects.
The mirror is used to visualize the anterior lingual portion of the mandible.
21
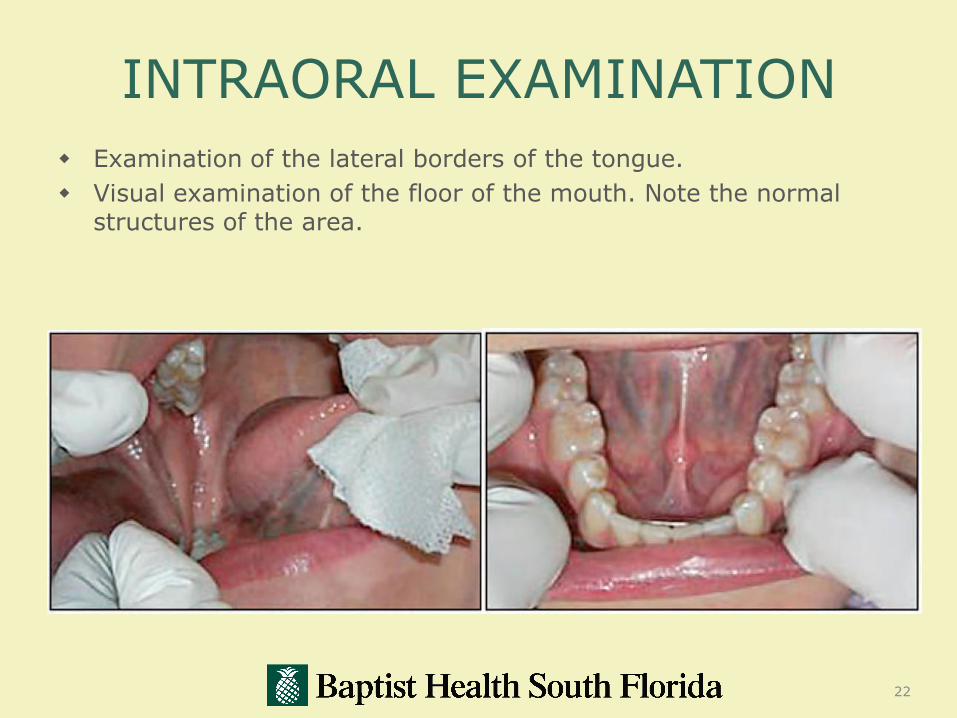
INTRAORAL EXAMINATION
Examination of the lateral borders of the tongue.
Visual examination of the floor of the mouth. Note the normal structures of the area.
22

23

First level bullet
Second level bullet
Third level bullet
Fourth level bullet
Fifth level bullet
24
25

Selected diseases of the oral mucosa
Inflammatory Disorders
Selected diseases of the oral mucosa
Inflammatory Disorders
Infections
Selected diseases of the oral mucosa
Inflammatory Disorders
Infections
Herpes Simplex

Selected diseases of the oral mucosa
Inflammatory disorders
Infections:
Herpes Simplex Majority of infections with HSV
are subclinical
Either HSV type 1 or 2 may be involved

Selected diseases of the oral mucosa
Inflammatory disorders
Infections:
Herpes SimplexPrimary herpetic gingivostomatitis
Infants, young children, immunosuppressed individuals

Selected diseases of the oral mucosa
Inflammatory disorders
Infections:
Herpes Simplex
Primary herpetic gingivostomatitis
Multiple, painful, discrete vesicles that rupture to form ulcers
Cervical lymphadenopathy, malaise, and fever
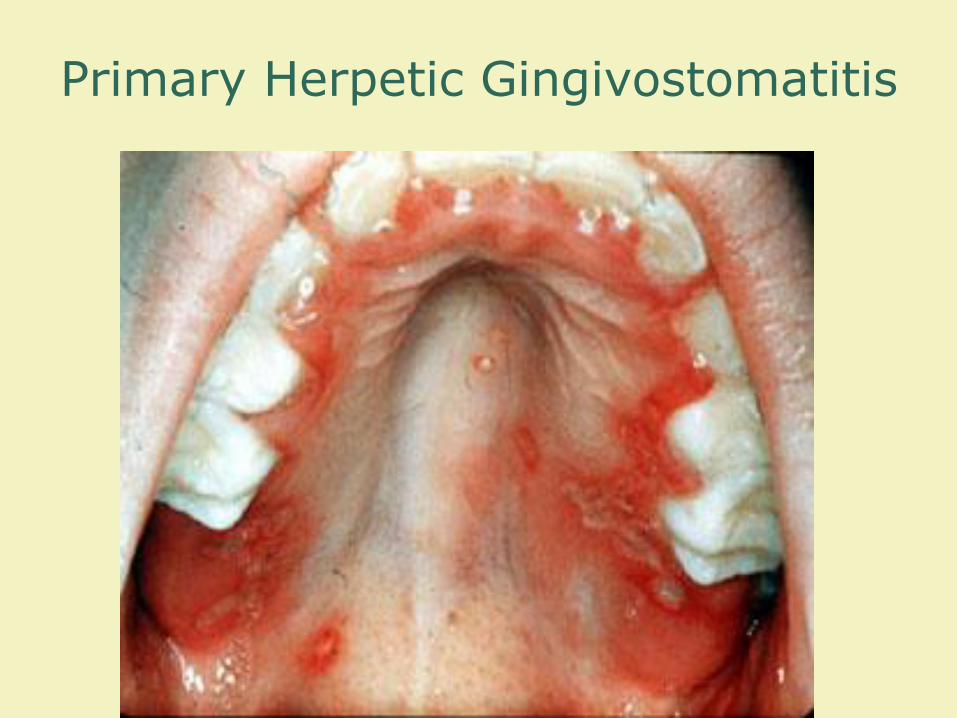
Primary Herpetic Gingivostomatitis

Selected diseases of the oral mucosa
Inflammatory Disorders
Infections:
Herpes Simplex
Recurrent herpetic infections
Viral latency after clinical or subclinical infection
Reactivated by febrile illness, trauma, or other forms of stress
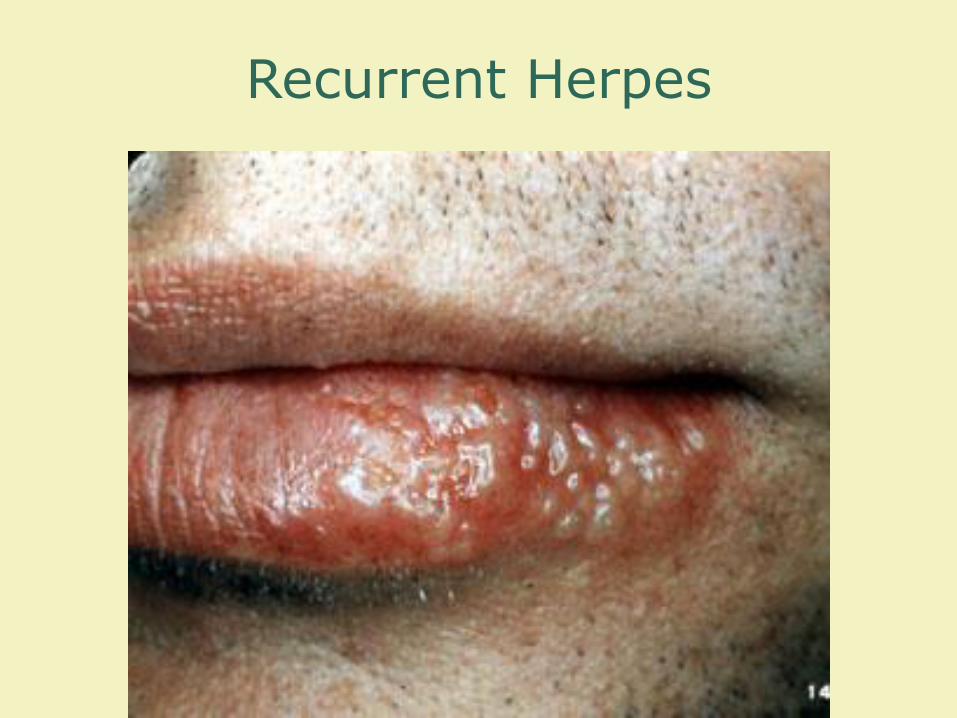
Recurrent Herpes

Recurrent Herpes
Selected diseases of the oral mucosa
Inflammatory Disorders
Infections:
Candida (Monilia) AlbicansStomatitis in young children and in
adults with debilitating diseases
prolonged broad spectrum antibiotics, or immunosuppressive therapy

Thrush
Selected diseases of the oral mucosa
Inflammatory Disorders
Infections:
Acute necrotizing ulcerative gingivitis
Severe necrotizing gingivitis occurring in patients with poor oral hygiene and decreased resistance to bacterial infection
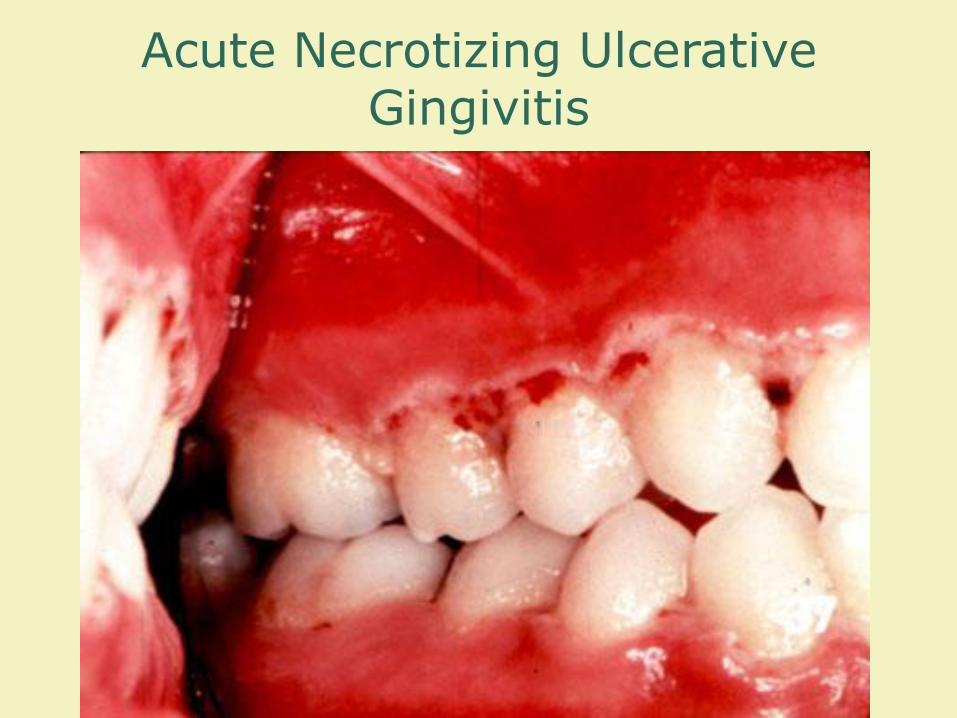
Acute Necrotizing Ulcerative Gingivitis
Relation of Periodontal Disease and Systemic Diseases
Periodontal disease, a chronic inflammatory disease, is linked to other health risks.
Heart Disease and Stroke
Pregnancy Problems
Diabetes
Respiratory Diseases
40
Selected diseases of the oral mucosa
Inflammatory Disorders
Infections:
Viral Papillary Lesions
Associated with Human Papilloma Virus
Exophytic and appear as cauliflower-like lesions
High rate of recurrence
41
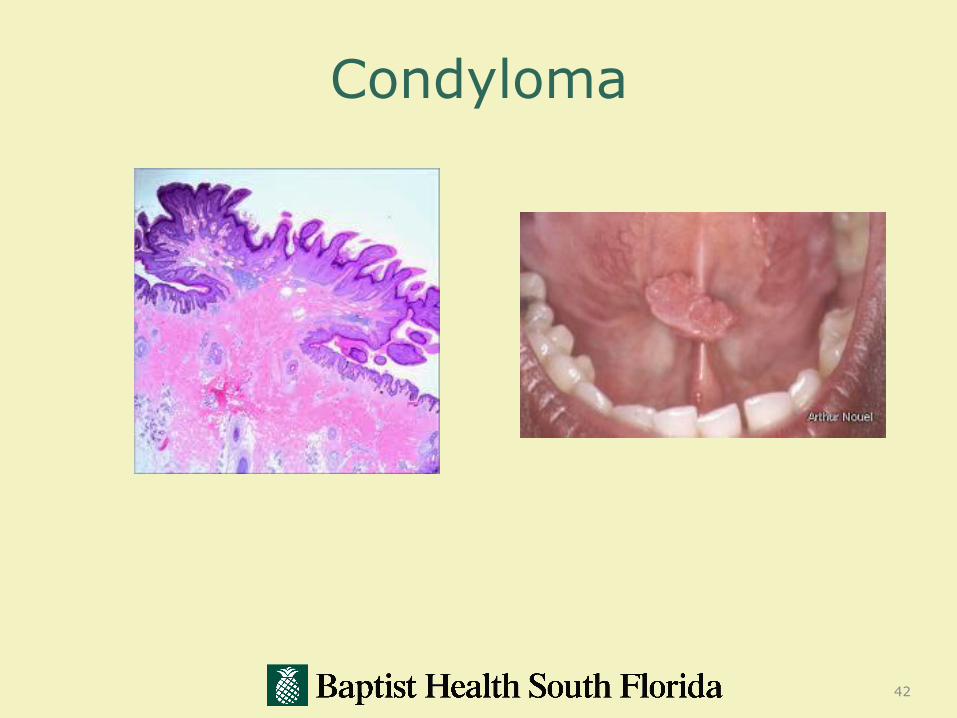
Condyloma
42


Selected diseases of the oral mucosa
Inflammatory Disorders
Recurrent Aphthous UlcersIdiopathic disorder characterized by
recurrent episodes of painful, round or oval yellow-white ulcers
surrounded by an erythematous halo

Selected diseases of the oral mucosa
Inflammatory Disorders
Recurrent aphthous stomatitis
Three forms
Minor type
Major type
Herpetiform type
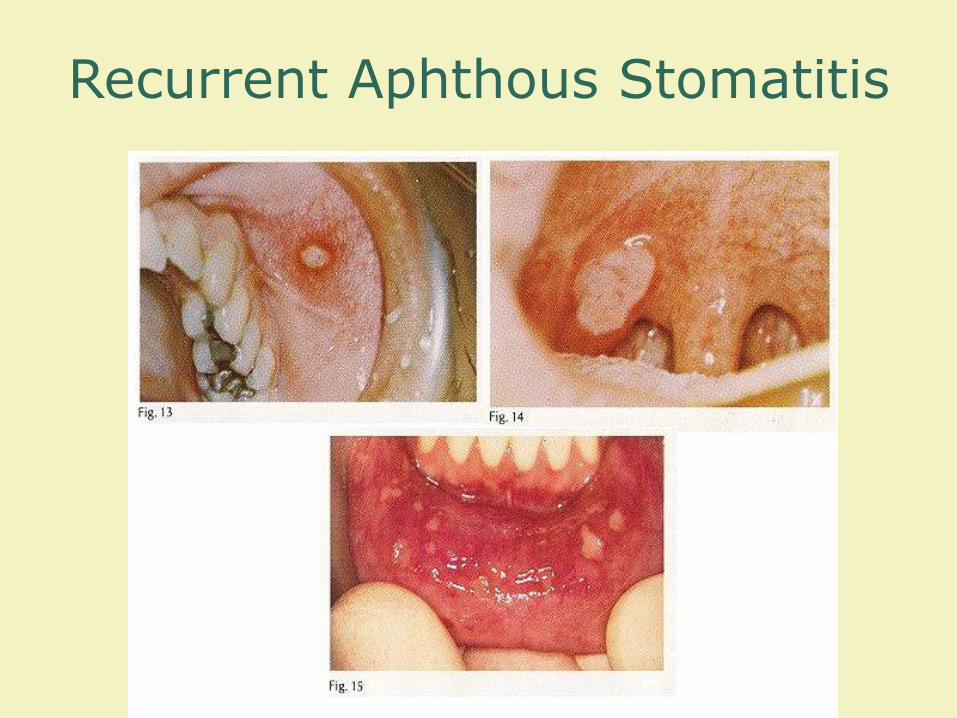
Recurrent Aphthous Stomatitis
Selected diseases of the oral mucosa
Inflammatory disorders
Pyogenic Granuloma
Asymptomatic tumescence composed of granulation tissue

Pyogenic granuloma
Selected diseases of the oral mucosa
Inflammatory disorders
Lichen planus
Selected diseases of the oral mucosa
Inflammatory disordersLichen Planus (autoimmune)
Common chronic inflammatory mucocutaneous disease
Oral lesions may be the only manifestation*
Disease of middle age that affects the sexes nearly equally
Selected diseases of the oral mucosa
Inflammatory disorders
Lichen planus
Several forms

Selected diseases of the oral mucosa
Inflammatory disorders
Lichen planus
Several forms
Reticular form

Lichen planus
Selected diseases of the oral mucosa
Inflammatory Disorders
Lichen planus
Several forms
Reticular form
Erosive form

Erosive Lichen Planus
PRECANCEROUS LESIONS?
Clinical appearance
Minimal pain during early growth phase.
Exophytic
Endophytic
Leukoplakia
Erythroplakic
Erythroleukoplakic

Premalignant Lesions
Leukoplakia:
A white patch or plaque that cannot be characterized clinically
A descriptive term, not a histological diagnosis.
Generally asymptomatic
Presents as a white lesion that may be flat, slightly elevated with rugatedor smooth texture
The buccal mucosa, lower lip vermilion and gingiva account for most oral cavity leukoplakia
More than 70% of patients with leukoplakia are smokers
The malignant transformation of these lesions has been studied extensively with no definitive conclusions

Leukoplakia
Premalignant LesionsErythroplakia
A red patch that cannot be characterized clinically
More likely to present with dysplasia or carcinoma in situ
Common sites are floor of the mouth and retromolarfossa.
Appearance can be bright red, homogenous, and may or may not have a sharply demarcated border
Often associated with areas of leukoplakia (Erythroleukoplakia)

Erythroplakia
HOW DOES ORAL CANCER
PRESENT IN THE MOUTH?

63

Oral Cancer
Oral cancer accounts for around 3% of all newly diagnosedcancers
Eighth most common cancer affecting males in the United States
Squamous cell carcinoma (SCC): 85-95% of all oral cancer
Other malignant lesions can be found in the oral cavity such as:Salivary Gland Tumors MelanomaSarcomaLymphomaMetastatic disease
Even with recent advances in locoregional control and adjunctive therapy, 5 year survival rates have not improved significantly
Risk Factors
No single causative agent can be attributed to the development of all oral cancers
Tobacco and alcohol appear to have a great impact on malignancy development
Smokers are 2 to 12 times more likely to develop malignancies in the oral cavity than non smokers
90% of individuals with oral cancer report a smoking history.

Exophytic lesion
Typically irregular or papillary surface forming the mass
Superficial color can be from NORMAL, to red, to white depending on keratinization or ulcerated
Tumor feels indurated

Endophytic lesion
Typically have depressed irregularly shaped ulcerated central area with surrounding rolled border of normal or white mucosa
Rolled border from invasion of tumor downward and laterally

Risk Factors
The United States has an aggressive anti-smoking campaign, resulting in the decrease of smokers and oropharyngeal malignancies………
but increase in the incidence of HNC in young men, non-smokers, and non-drinkers

HUMAN PAPILLOMA
VIRUS

Human Papillomavirus
85% of humans will have and HPV infection during their lifetime, enter via a break in the stratified squamous epithelium of the oral mucosa
90-95% are associated with HPV 16
Mork et al demonstrated 14 times greater risk in people testing positive for HPV 16
Human Papillomavirus
Enter the cell via endocytosis
Enter the nucleus and the viral genome is incorporated into the cell line
Main culprit, , has a higher affinity to bind to tumor suppression genes

Prognosis
HPV-positive patients have better overall survival outcomes than HPV-negative
HPV-positive tumors are much more radiosensitive
Tachezy et al, showed HPV-positive tumors have an absence of p53 mutations

Tongue
22 to 49% of all oral cancer
Anterior 2/3: 75% of cases
Posterior one-third: 25% of cases
Metastasis to level II, followed by levels III and I. Possibility of “skip”metastasis to level IV
About 40% will have cervical node metastasis at time of presentation
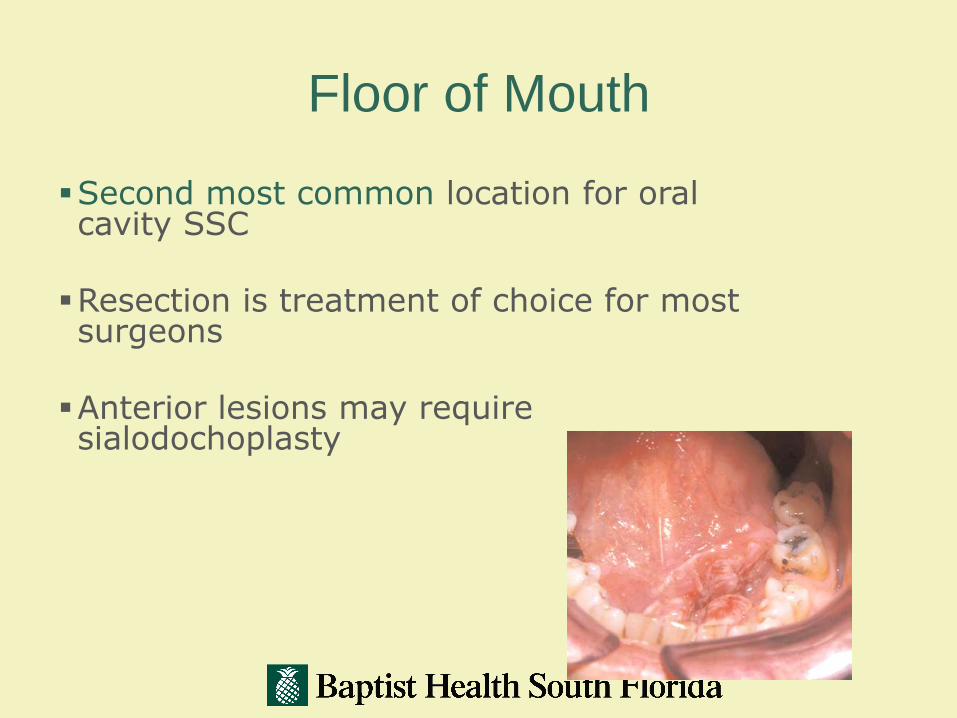
Floor of Mouth
Second most common location for oral cavity SSC
Resection is treatment of choice for most surgeons
Anterior lesions may require sialodochoplasty

Retromolar Trigone
Can resemble oropharyngealprimary cancer in behavior
Larger lesions may invade the pterygomandibular space and extend towards the skull base
Surgical Management:
-Wide local excision-Marginal mandibulectomy-Segmental Resection
Elective neck radiation or selective neck dissection should be considered in T2 or greater lesions

Lip Cancer
Approximately 2 to 42% of oral cavity cancers.
Often seen in white males with increased sun exposure
Metastasis from the lower lip: submental, submandibular, and perifacial nodes
Metastasis from upper lip and commisure: Preauricular, periparotid, and submandibular nodes

Lip Cancer
Surgical Treatment:
-CO2 laser ablation
-Vermilionectomy
-“Wedge” resection
Infrequent nodal metastasis-
Neck dissection usually not indicated
Five-year survival of 90% for stage I and Stage II
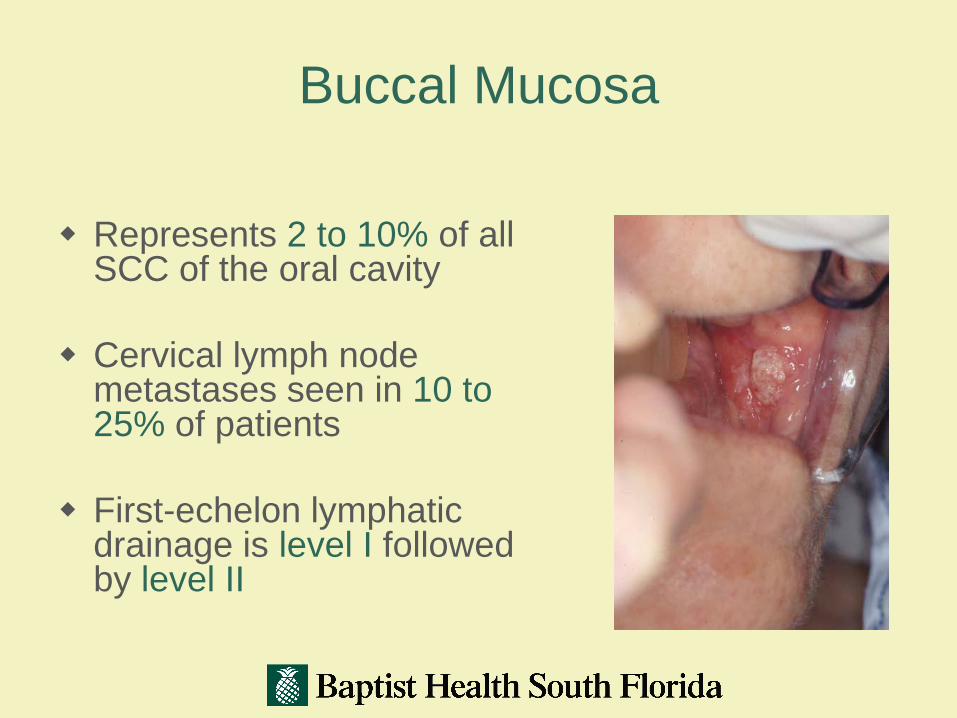
Buccal Mucosa
Represents 2 to 10% of all SCC of the oral cavity
Cervical lymph node metastases seen in 10 to 25% of patients
First-echelon lymphatic drainage is level I followed by level II
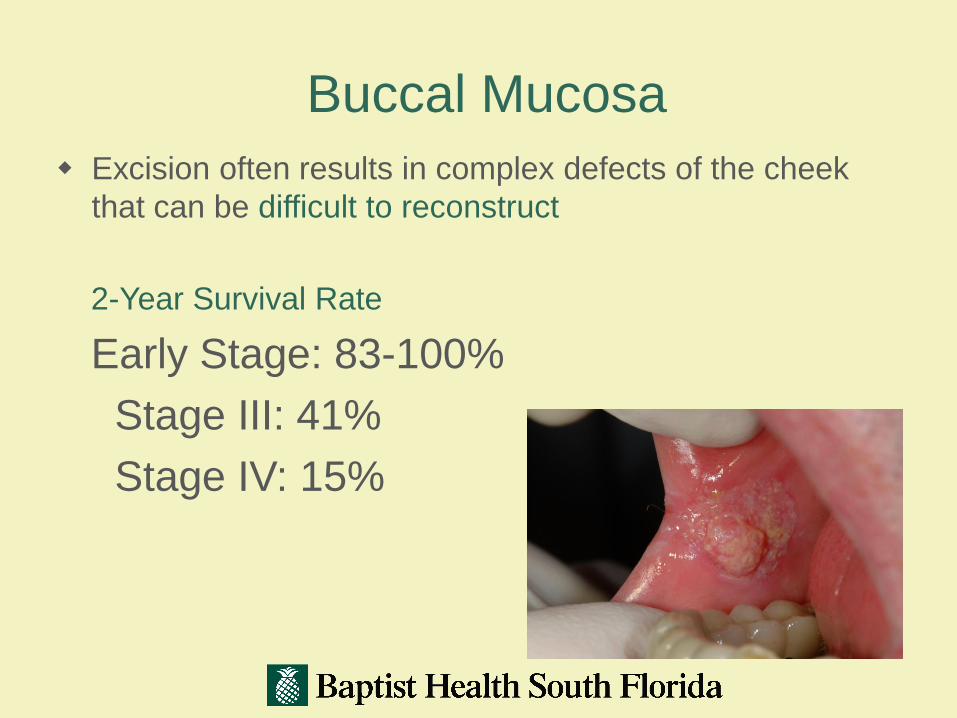
Buccal Mucosa
Excision often results in complex defects of the cheek
that can be difficult to reconstruct
2-Year Survival Rate
Early Stage: 83-100%
Stage III: 41%
Stage IV: 15%

Alveolar Ridge
2 to 18% of oral cancers
Mandible more common than maxilla
About 30% of these tumors will exhibit some bony involvement at time of presentation
Metastasis more common in mandibular ridge tumors than in maxillary tumors.
Nodal drainage most frequently to levels I and II (25 to 30% at diagnosis)

Alveolar Ridge
Surgical Management May Include:
-Partial or total maxillectomy
-Marginal Mandibulectomy
-Segmental Mandibulectomy
Overall 5-year survival rate is 50 to 65%
Poor outcome is associated with:
-advanced stage
-perineural spread
-positive margins

Hard Palate About 3 to 6% of all oral cavity SCC
Metastasis in 10-25% of patients at time of presentation
Metastasis usually to levels I and II
Metastaor nodes that are not palpable on a clinical examination
sis can be to retropharyngeal nodes Elective treatment of the neck mostly for
T3 or T4 lesions
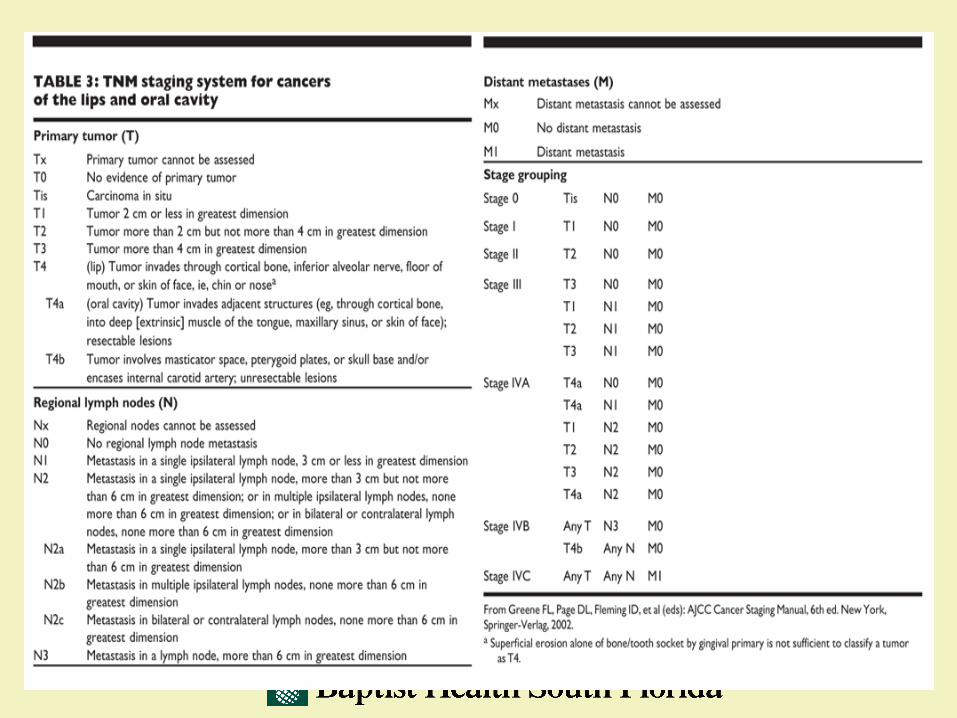
Staging
Pigmented Lesions
BLUE/PURPLE VASCULAR LESIONS:
Hemangioma
Varix
Angiosarcoma
Kaposi’s Sarcoma
Hereditary Hemorrhagic Telangiectasia
84

Hemangioma
85
Kaposi’s Sarcoma

Pigmented Lesions
BROWN MELANOTIC LESIONS Ephelis and Oral Melanotic Macule
Nevocellular Nevus and Blue Nevus Malignant Melanoma Drug-Induced Melanosis Physiologic Pigmentation Café au Lait Pigmentation Smoker’s Melanosis Pigmented Lichen Planus Endocrinopathic Pigmentation HIV Oral Melanosis Peutz-Jeghers Syndrome
86
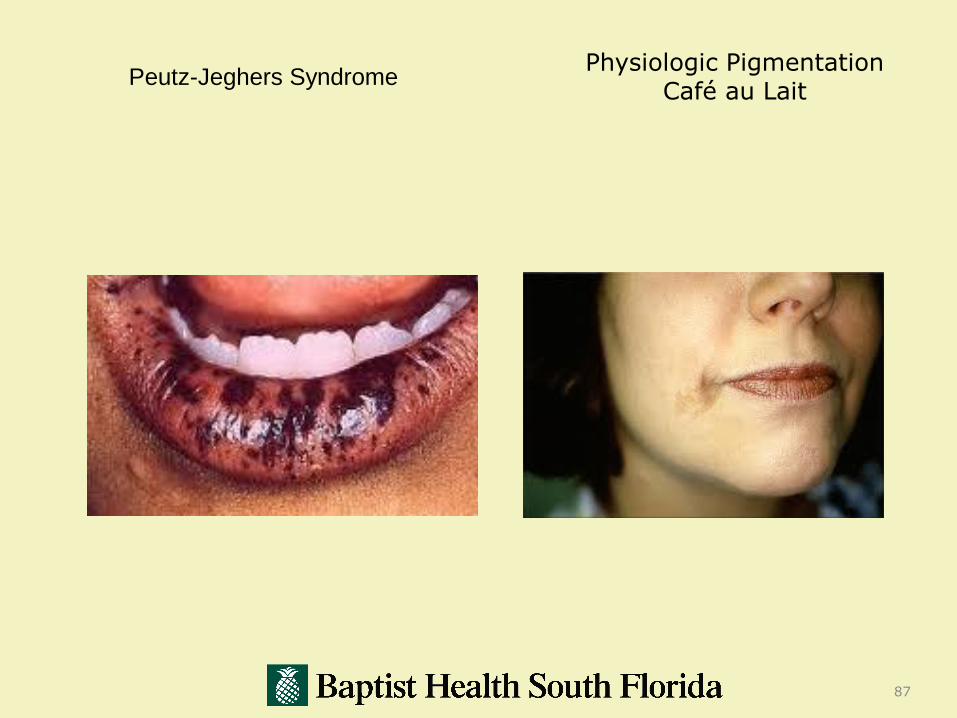
Peutz-Jeghers Syndrome
87
Physiologic Pigmentation Café au Lait
Pigmented Lesions
BROWN HEME-ASSOCIATED LESIONS
Ecchymosis
Petechia
Hemochromatosis
88

Ecchymosis
89

Pigmented Lesion
GRAY/BLACK PIGMENTATIONS
Amalgam Tattoo
Graphite Tattoo
Hairy Tongue
Pigmentation Related to Heavy-Metal Ingestion
90
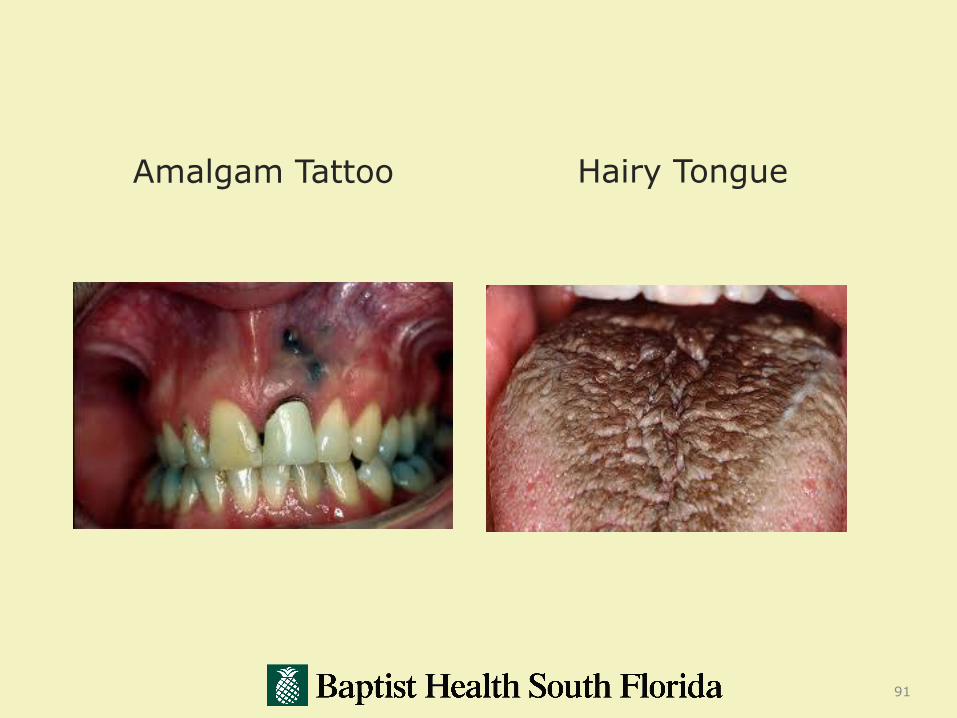
Amalgam Tattoo
91
Hairy Tongue

92

Oral Mucosal Melanoma
Mucosal melanoma of the head and neck is a relatively rare condition, representing 8-15% of all malignant melanomas of the head and neck region and accounting for less than 1% of all melanomas.
The prognosis is grim, with most published reports documenting a dismal 5-year survival rate of 10-15%.
93

94

95

96
97
98

99

Selected diseases of the oral mucosa
Tumor like conditions
Fibroma
Selected diseases of the oral mucosa
Tumor like conditions
Fibroma
Hyperplastic fibrous lesion resulting
from trauma or chronic irritation
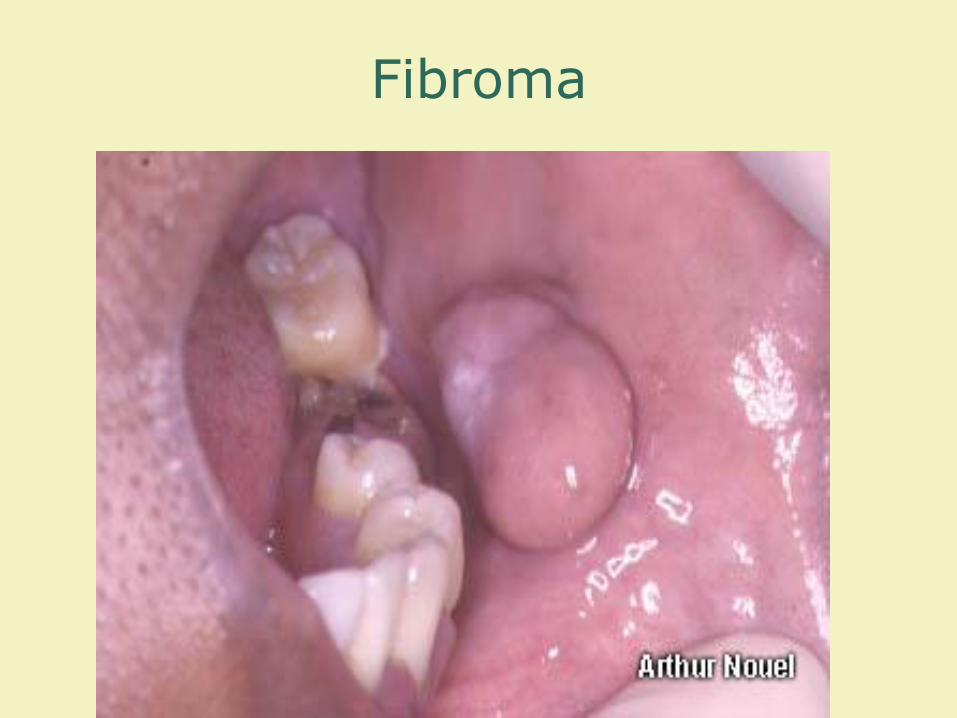
Fibroma

Selected diseases of the tongue
Geographic tongue
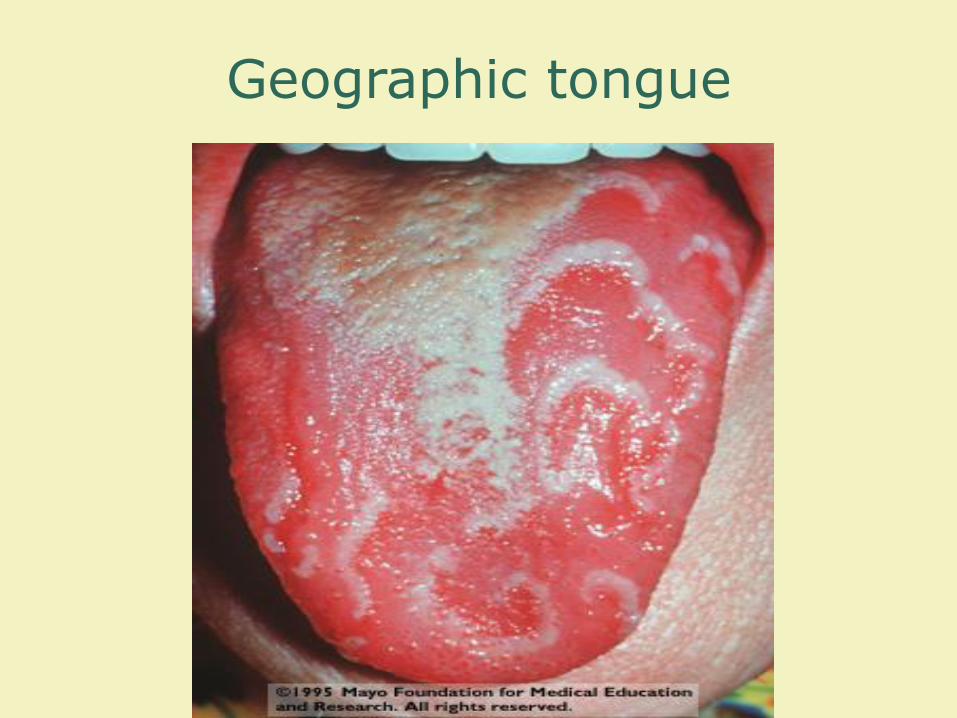
Geographic tongue
Selected Diseases of the Tongue
Geographic Tongue
Median Rhomboid Glossitis

Median Rhomboid Glossitis

Selected diseases of the tongue
Geographic tongue
Median rhomboid glossitis
Hairy tongue

Black Hairy Tongue

Selected diseases of the tongue
Geographic tongue
Median rhomboid glossitis
Hairy tongue
Fissured ( scrotal ) tongue

Fissured Tongue

Paget’s disease

Paget’s Disease
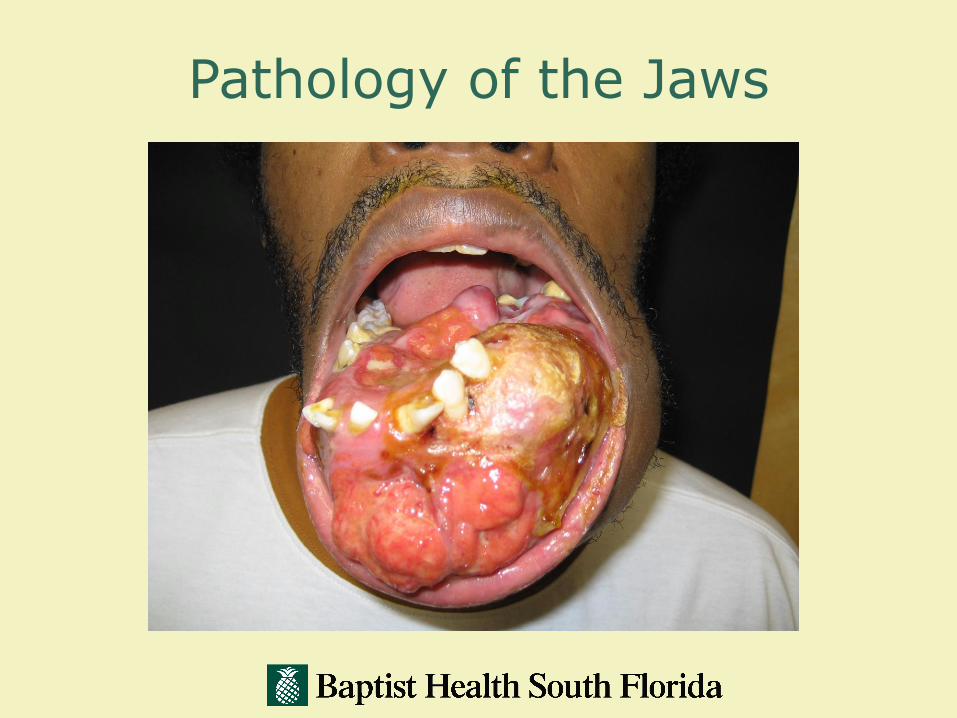
Pathology of the Jaws
Pathology of the Jaws
Miscellaneous Jaw LesionsOvergrowth of Mature Bone
Tori ( torus )Midline of palate

Maxillary Tori
Pathology of the Jaws
Miscellaneous Jaw LesionsOvergrowth of mature bone
Tori ( torus )
Midline of palateLingual surface of mandible
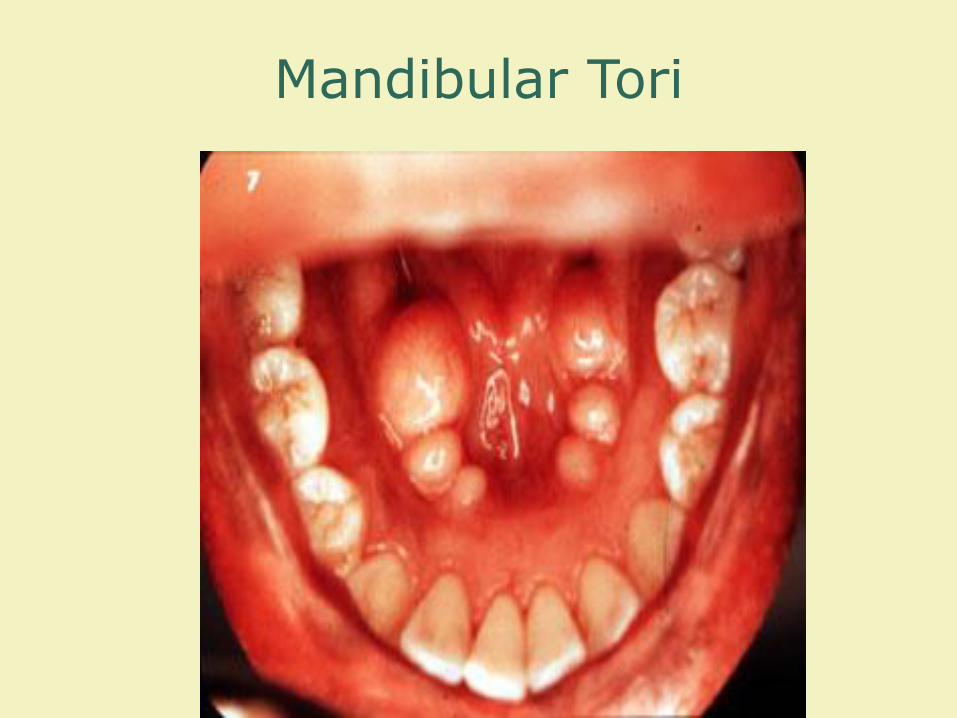
Mandibular Tori

Pathology of the Jaws
Miscellaneous Jaw LesionsOvergrowth of mature bone
Tori (Torus)
Midline of palateLingual surface of mandible
Exostosis ( exostoses )Buccal surfaces of maxilla and mandible
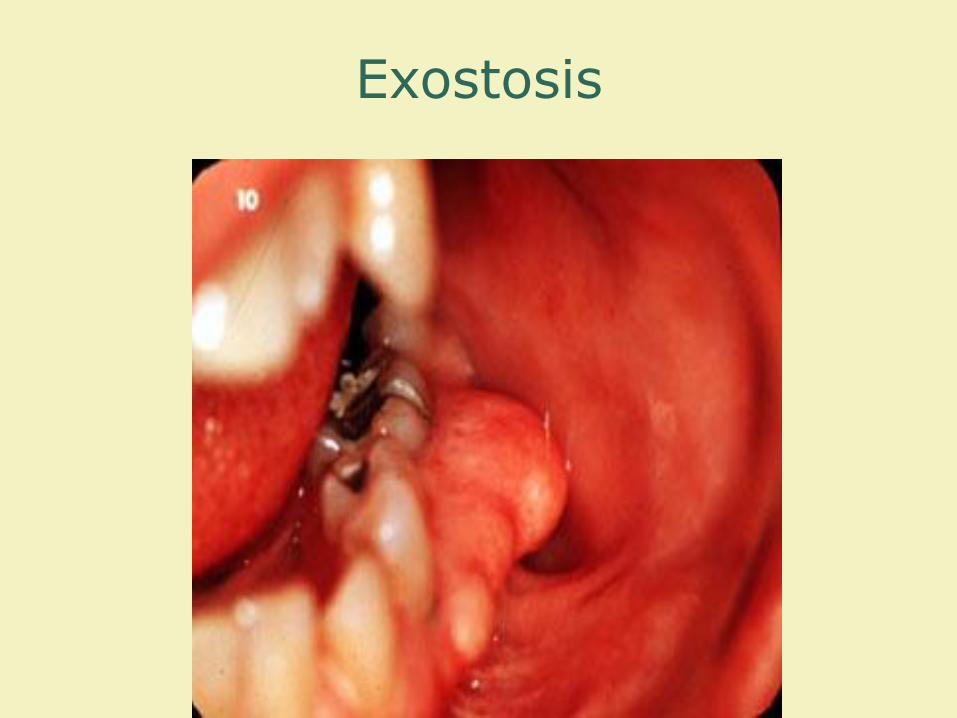
Exostosis
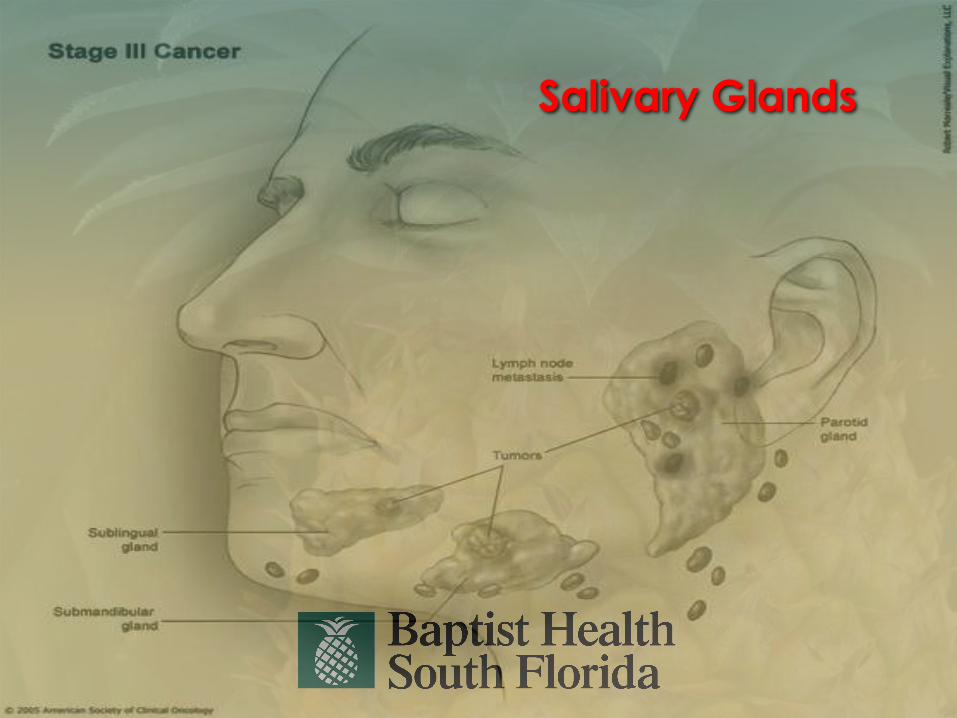
Salivary Glands

Salivary Glands
3 paired glands
Parotid
Submandibular
Sublingual
121

MINOR SALIVARY GLANDS
• 700-800 Minor salivary glands are located beneath the mucosa
– Tongue
– Buccal mucosa
– Floor of the mouth
– Oropharynx
– Upper and lower lip
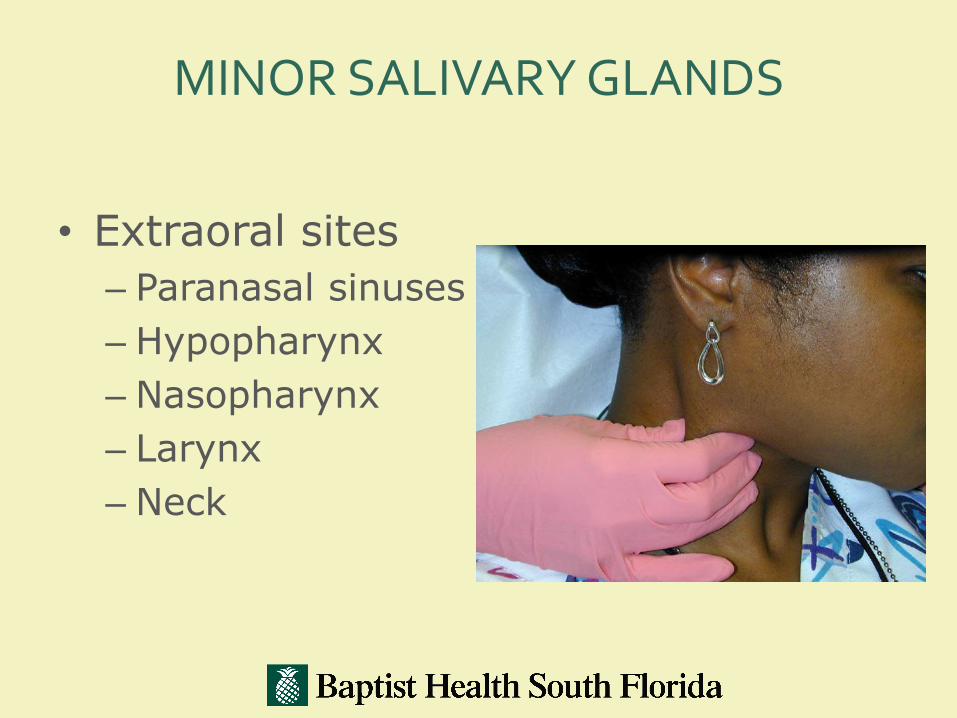
MINOR SALIVARY GLANDS
• Extraoral sites
– Paranasal sinuses
– Hypopharynx
– Nasopharynx
– Larynx
– Neck

Pathology of the Salivary Glands
Inflammatory diseasesAcute bacterial infection
Signs and symptoms: Pain, tenderness, and swelling
Red, swollen duct orifice
Pus may be expressed by massageof the gland or duct

Pathology of the Salivary Glands
Obstructive disordersSialolithiasis:
Ductal inflammation or stasis can lead to the formation of salivary stones (sialoliths) that obstruct the flow of saliva
Most common in the submandibular gland

Pathology of the Salivary Glands
Obstructive Disorders:
SialolithiasisMucocele:
Involves minor salivary glands
Results from obstruction or damage to the duct releasing mucus to form a cyst like pool of mucus
Most common location is lower lip

Mucocele
Pathology of the Salivary Glands
Obstructive disordersSialolithiasisMucoceleRanula:
Involves, most frequently, the sublingual gland and, less frequently, the submandibular gland
Pathology of the Salivary Glands
Obstructive disordersSialolithiasisMucoceleRanula:
Relatively large blue to transparent mass in the floor of the mouth that displaces the tongue
Obstruction due to a sialolith or mucus plug that results in mucus extravasation that pools superior to the mylohyoid muscle

Ranula

Epidemiological Data
Salivary gland tumors comprise:
3-6% of all tumors of the head and neck (Shah)
Less than 1% of all malignancies of the head and neck

Epidemiological Data
65% Parotid glands
22% minor salivary glands
8% submandibular glands

Pathology of the Salivary Glands
Salivary Gland Tumors:Benign Vs. Malignant
Parotid: 80/20
Submandibular 50/50
Sublingual 20/80
Minor depends on location

First level bullet
Second level bullet
Third level bullet
Fourth level bullet
Fifth level bullet
134

Aetiological and Risk Factors of Salivary Gland Tumors
1. In contrast to majority of head and neck tumors: not related to tobacco and alcohol
2. Chronic inflammation is not clearly defined as a risk factor
Licitra, Oncology 2003

Pathology of the salivary glands
Salivary gland tumorsBenign:
Pleomorphic adenoma
Most common salivary gland tumor*Variable mix of epithelial and mesenchymal elements
Slow growing, but can reach considerable size
Pleomorphic Adenoma
Pathology of the salivary glands
Salivary gland tumorsBenign
Papillary cystadenomalymphomatosum ( Warthin’s tumor )

Pathology of the Salivary Glands
Salivary gland tumorsBenign
Papillary cystadenomalymphomatosum ( Warthin’s tumor )
Occurs most frequently in the “tail”
of the parotid gland of white, middle aged men
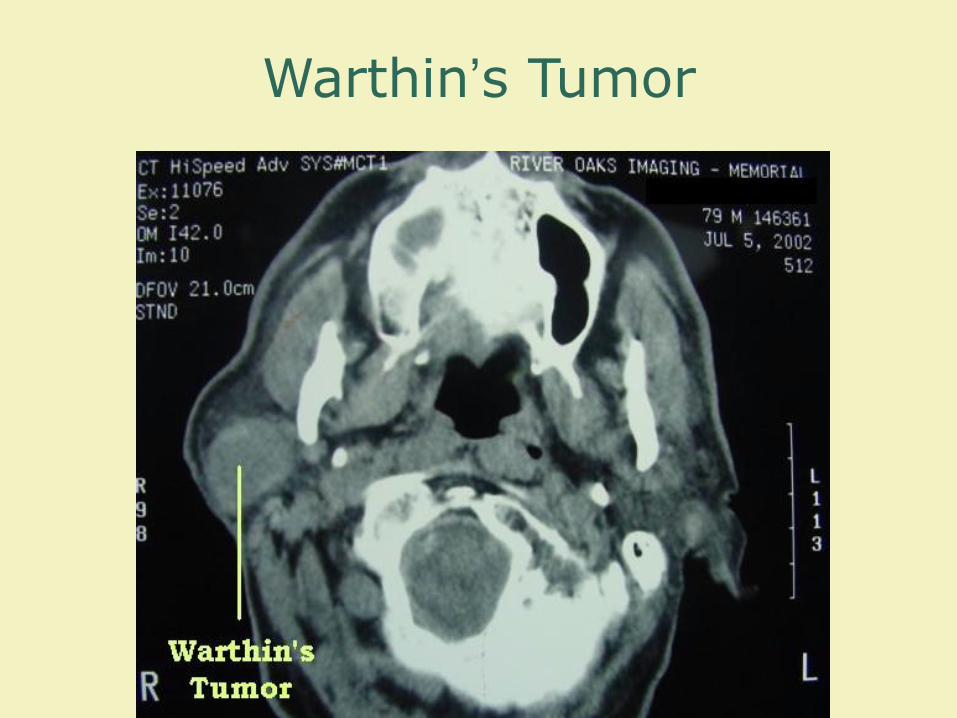
Warthin’s Tumor

Pathology of the Salivary Glands
Salivary gland tumorsMalignant (20%)

Pathology of the Salivary Glands
Salivary gland tumorsMalignant
Mucoepidermoid carcinomaMost common malignant salivarygland tumor*Parotid glands ( 60% to 70% )Minor glands ( 15% to 20% )Submandibular glands ( 10% )

Pathology of the salivary glands
Salivary gland tumorsMalignant
Mucoepidermoid carcinomaMost common salivary malignancy in children*
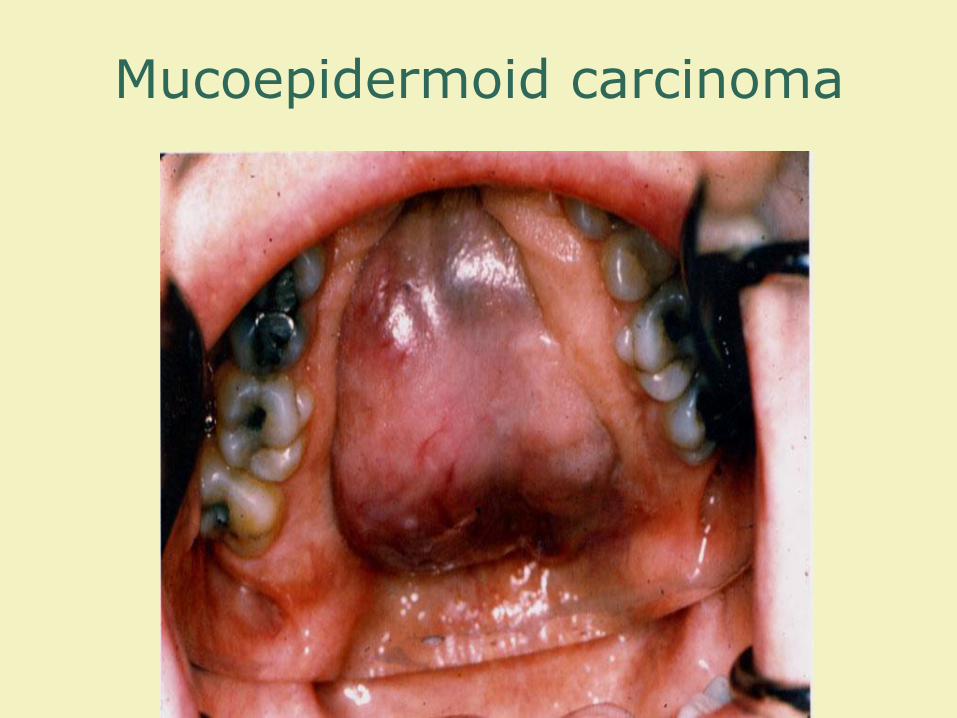
Mucoepidermoid carcinoma
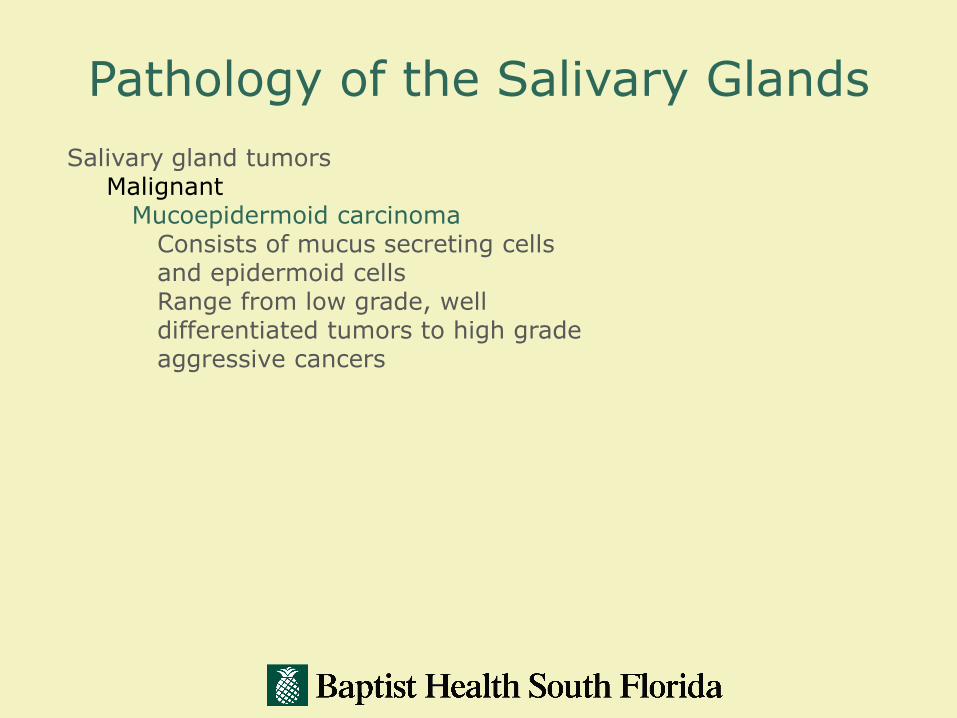
Pathology of the Salivary Glands
Salivary gland tumorsMalignant
Mucoepidermoid carcinomaConsists of mucus secreting cells and epidermoid cellsRange from low grade, well differentiated tumors to high grade aggressive cancers

Mucoepidermoid carcinoma
Pathology of the Salivary Glands
Salivary gland tumorsMalignant
Malignant mixed tumors

148

Pathology of the salivary glands
Salivary gland tumorsMalignant
Malignant mixed tumorsRepresents the malignant form of pleomorphic adenomaInvolves the parotid glands, less often the submandibular glands, and rarely the minor salivary glands

Pathology of the Salivary Glands
Salivary gland tumorsMalignant
Adenoid cystic carcinomas

Pathology of the Salivary Glands
Salivary gland tumorsMalignant
Adenoid cystic carcinomas
Most frequent neoplasms of minor salivary glands*
16% to 25% of all tumors50% of all malignant tumors
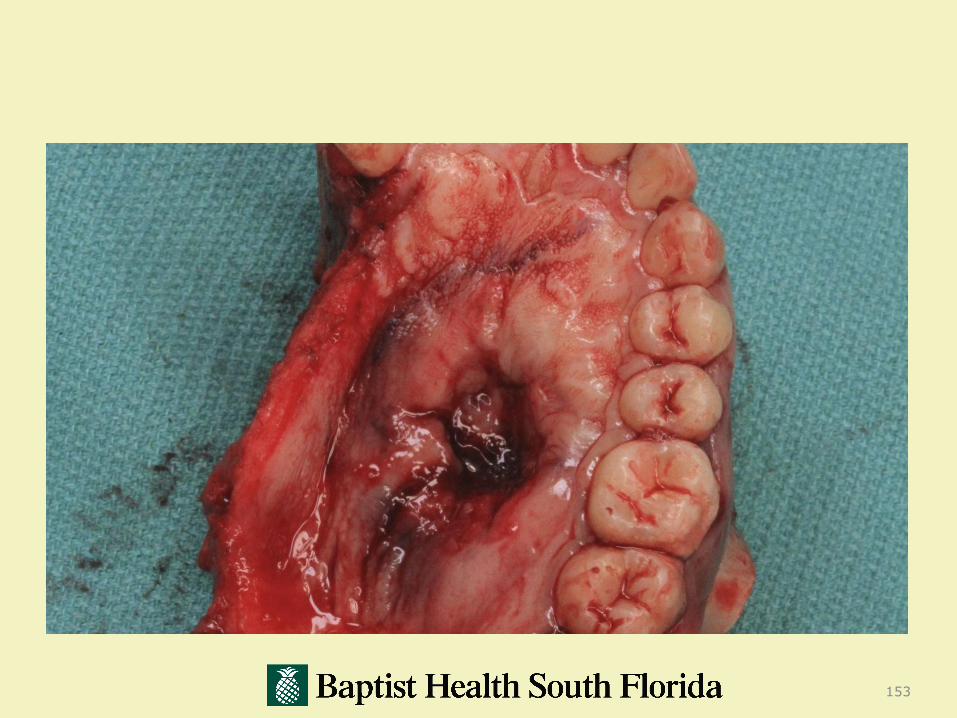
Pathology of the salivary glands
Salivary gland tumorsMalignant
Adenoid cystic carcinomas
Slow growing, but have a relentless course
Affinity for perineural invasionRecurrence is common and ultimate prognosis is poor
153

154

Maxillofacial Metastasis
Metastasis to the maxillofacial region is a rare
occurrence, with most of the literature considering 1% of all new head and neck cancers to be metastasis from distant sites.
Hirshberg,A.
Oral Oncology, Eur J Cancer 1995

Primary Tumor
According to the literature in larger series the most common sources of primary tumors are:
1. Breast2. Lung3. Kidney4. Bone5. Colon
Hirshberg, A.
Oral Oncol, Eur J Cancer 1995

Maxillofacial Metastasis
Overall there were twenty six patients.
16 Males
10 Females
Average age of 63.8 yrs (45-87)
Average age of Males 64 yrs
Average age of Females 64 yrs
MF mets (n=26)
Males (16) Females (10)
Ave age 64 Ave age 64

Clinical Presentation
Facial Swelling 10 38.4%Gingival Swelling 9 34.6%Pain 7 26.9%Paresthesia 5 19.2%Pathologic Fracture 3 11.5%TMD 3 11.5%Non-Healing Extraction 2 7.6%Facial Nerve Palsy 1 3.8%Loose Teeth 1 3.8%

Primary Tumor
According to the literature in larger series the most common sources of primary tumors are:
1. Breast2. Lung3. Kidney4. Bone5. Colon
Hirshberg, A.
Oral Oncol, Eur J Cancer 1995
At the time of presentation:
16 (62%) had unknown primaries and the metastasis led to the diagnosis of the primary tumor
10 patients had known primaries
- average time of diagnosis of a metastatic lesion 31.5 months
- range of 0-103 months