
Shadowing Vulnerable Patients’ Encounters with Health Care · Shadowing Vulnerable Patients’...
27
49 Shadowing Vulnerable Patients’ Encounters with Health Care Background On Tuesday, following the morning interviews, we will assemble at the OU Family Medicine Center where we will participate in the patient care provided to patients with substantial medical and social vulnerability. We will see how the community outreach programs of the OU School of Community Medicine provide care to patients without health insurance and how this experience teaches teamwork and systems-based practice to medical, physician assistant, nursing, social work, and pharmacy students. Summer Institute students will shadow patients through their medical encounters. They will experience health care form the patient’s not the physician’s perspective. Each student will map the patient experience as a way to shape a vision of current health care and what is needed for a better future to emerge through us. On Tuesday evening, half of the medical students will experience triage as if they were patients seeking care from the Bedlam Free Clinic. They will then shadow third and fourth year medical students in providing care for actual patients who are seeking care. On Thursday evening, the other half of the medical students will have a similar experience. You will have many opportunities to learn the diagnosis and treatment of medical conditions. During the Summer Institute, it is important for students to put themselves in the patient’s shoes, understand their perspective, condition and needs. Patient-Centered Medical Home The attached essay describes the elements of the patient centered medical home. This is a microsystem of medical care that provides first-contact, comprehensive, coordinated, and continuing care for patients of a particular age group or for families. The goal of the School of Community Medicine is to provide students with an opportunity to learn how to provide care in a medical home and to understand the important role of attention to the systems-based practice, regardless of which specialty the student ultimately pursues. You are encouraged to read this essay and to use the analysis form during your visit to get an idea of how the practice-based systems actually work. You will identify many holes in the current system that will provide you with ideas of how you can contribute to improving the care delivered.
Transcript of Shadowing Vulnerable Patients’ Encounters with Health Care · Shadowing Vulnerable Patients’...
49
Shadowing Vulnerable Patients’
Encounters with Health Care
Background
On Tuesday, following the morning interviews, we will assemble at the OU Family
Medicine Center where we will participate in the patient care provided to patients with
substantial medical and social vulnerability. We will see how the community outreach
programs of the OU School of Community Medicine provide care to patients without
health insurance and how this experience teaches teamwork and systems-based practice
to medical, physician assistant, nursing, social work, and pharmacy students.
Summer Institute students will shadow patients through their medical encounters. They
will experience health care form the patient’s not the physician’s perspective. Each
student will map the patient experience as a way to shape a vision of current health care
and what is needed for a better future to emerge through us.
On Tuesday evening, half of the medical students will experience triage as if they were
patients seeking care from the Bedlam Free Clinic. They will then shadow third and
fourth year medical students in providing care for actual patients who are seeking care.
On Thursday evening, the other half of the medical students will have a similar
experience.
You will have many opportunities to learn the diagnosis and treatment of medical
conditions. During the Summer Institute, it is important for students to put themselves in
the patient’s shoes, understand their perspective, condition and needs.
Patient-Centered Medical Home
The attached essay describes the elements of the patient centered medical home. This is a
microsystem of medical care that provides first-contact, comprehensive, coordinated, and
continuing care for patients of a particular age group or for families. The goal of the
School of Community Medicine is to provide students with an opportunity to learn how
to provide care in a medical home and to understand the important role of attention to the
systems-based practice, regardless of which specialty the student ultimately pursues.
You are encouraged to read this essay and to use the analysis form during your visit to
get an idea of how the practice-based systems actually work. You will identify many
holes in the current system that will provide you with ideas of how you can contribute to
improving the care delivered.
50
Mapping Patient Experience with Health Care
You will experience the Bedlam clinics from both the patient and the medical student
perspective. When you arrive at the Bedlam Longitudinal clinic, you will have a brief
introduction to the system-based approach to care. You will experience the ―round-up‖
with a team.
You will then meet a patient in the lobby and introduce yourself, asking the patient
permission to follow them through their visit. You should engage in a dialogue with the
patient about their life situation and their expectations and needs for medical care. It will
be important for you to understand the barriers that the patient may have faced in getting
to the clinic for this appointment.
You will have time to spend with the patient and the family while the team is doing its
work. You may take notes for your journal during this visit. You may be interested in
noting the wait times for the patient and talk with the team about these so that we might
understand what this waiting is like for the patient.
You might be interested in drawing a map of the patient experience indicating the stops
that the patient must make during the visit and the time intervals between the stops.
Indicate on the map the various persons that the patient encountered, what they did, and
something about their attitude of helpfulness and clarity of information they gave to the
patient.

51
APPENDIX
Patient Centered Medical Home
Elements of a Practice Microsystem
An Introduction to Systems-Based Practice
This essay describes the structure of the Patient Centered Medical Home. It was written
to provide a background for novice health care professionals who are learning about the
structure of the systems and Microsystems that provide medical care. It is a doorway to
understanding how healthcare depends upon competent staff and clinicians working
within a well-organized front line systems designed to provide high quality care.
In 2002 the American College of Physicians, the American Academy of Family Practice,
the American Academy of Pediatrics, and the American Osteopathic Association jointly
defined the functional qualities of a patient-centered medical home. This model provides
novice health care professional students a map for finding their way through the complex
sites of care as they begin gaining competence in systems-based practice.
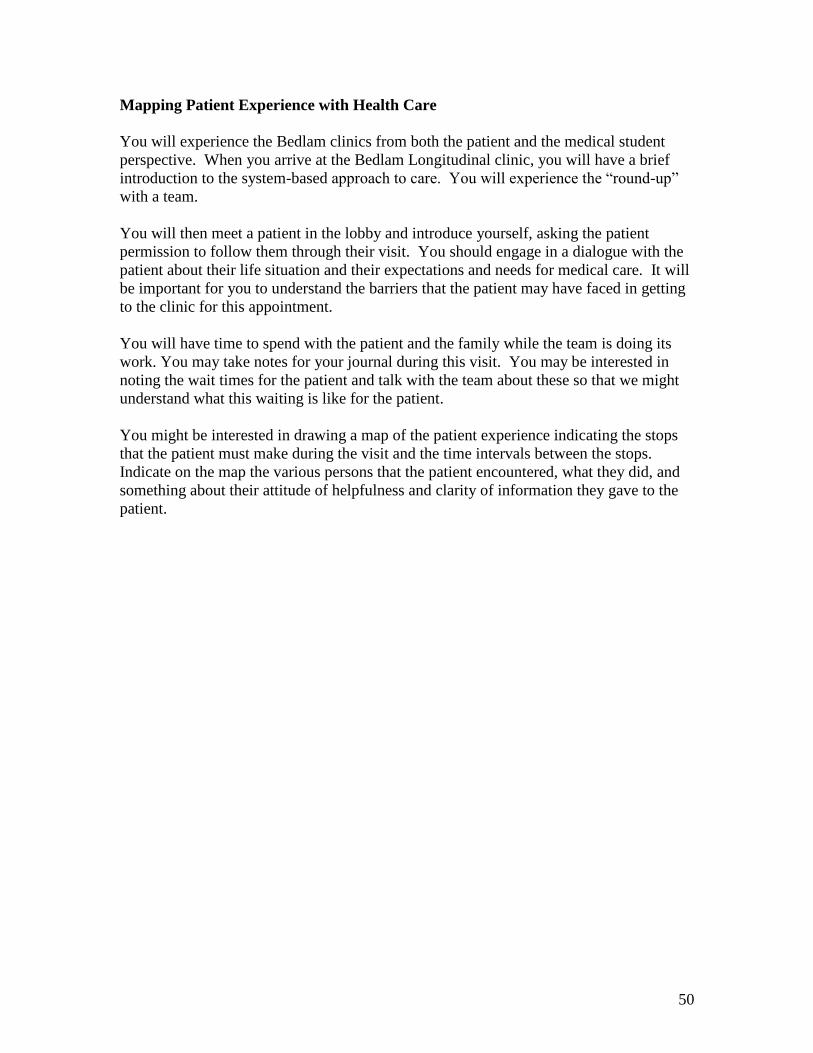
The model described in this paper merges a train of concepts into a unified picture of the
systems that result in health care. Figure 1 traces the origin of the model as it was built
upon the prior work of the Institute for Healthcare Improvement (IHI) idealized practice
project (Charles Kilo), the Wagner Chronic Care Model (IHI), the Institute of Medicine’s
Crossing the Quality Chasms paper on the elements of a quality health care system,
Batalden and Nelson’s Dartmouth model of the clinical microsystem, the National
Committee on Quality Assurance (NCQA) standards for recognition of a medical home
through the Physician Practice Connections award , and the American Board of Internal
Medicine’s (ABIM) Practice Improvement module practice system assessment. Like any
model, it is wrong but may be useful.
Several names are used throughout this paper for the practice organization we are
describing. ―Patient-Centered Medical Home‖ is used to describe the front-line
organization of people, site of care, and care processes experienced by the patient. This
is the place and the people the patient will contact first with any health related issues.
―Practice‖ is used more generically to describe this same organization. Probably the most
accurate term for what we are talking about is ―Clinical Microsystem.‖ This is the term
coined by Paul Batalden and Gene Nelson to describe the front line people and processes
that actually deliver care. A patient-centered medical home is a clinical microsystem.
Likewise, an emergency department, hospital inpatient unit, dialysis unit, or x-ray
department are all examples of other clinical Microsystems. A medical practice or a
patient centered medical home may have many Microsystems. A large health care
system is made up of multiple interdependent Microsystems.
52
Figure 1
Improved Outcomes
Informed,Activated
Patient
Productive
Interactions
Prepared,Proactive
Practice Team
Resources and Policies
Community
DeliverySystemDesign
Decision
Support
ClinicalInformation
Systems
Self-Management
Support
Health System
Health Care Organization
Idealized Design of
Clinical Office Practices
Chronic Care Model
ABIM Practice
System Model
Clinical Microsystem
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Access to
Practice
Access to
PracticeDiagnostic
Work-up
Diagnostic
Work-up
Treatment &
Monitoring
Treatment &
Monitoring
Self-Care
Support
Self-Care
Support
Leadership/citizenship - Quality InnovationLeadership/citizenship - Quality Innovation
Clinical Information ManagementClinical Information Management
Teamwork – Care ManagementTeamwork – Care Management
Tests – Consults – Referrals - Rx
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
IOM Crossing the
Quality Chasm
Clinical Microsystems
Origin of SystemsOrigin of Systems--Based Practice ModelBased Practice Model
From Charles Kilo, MD, September 2006
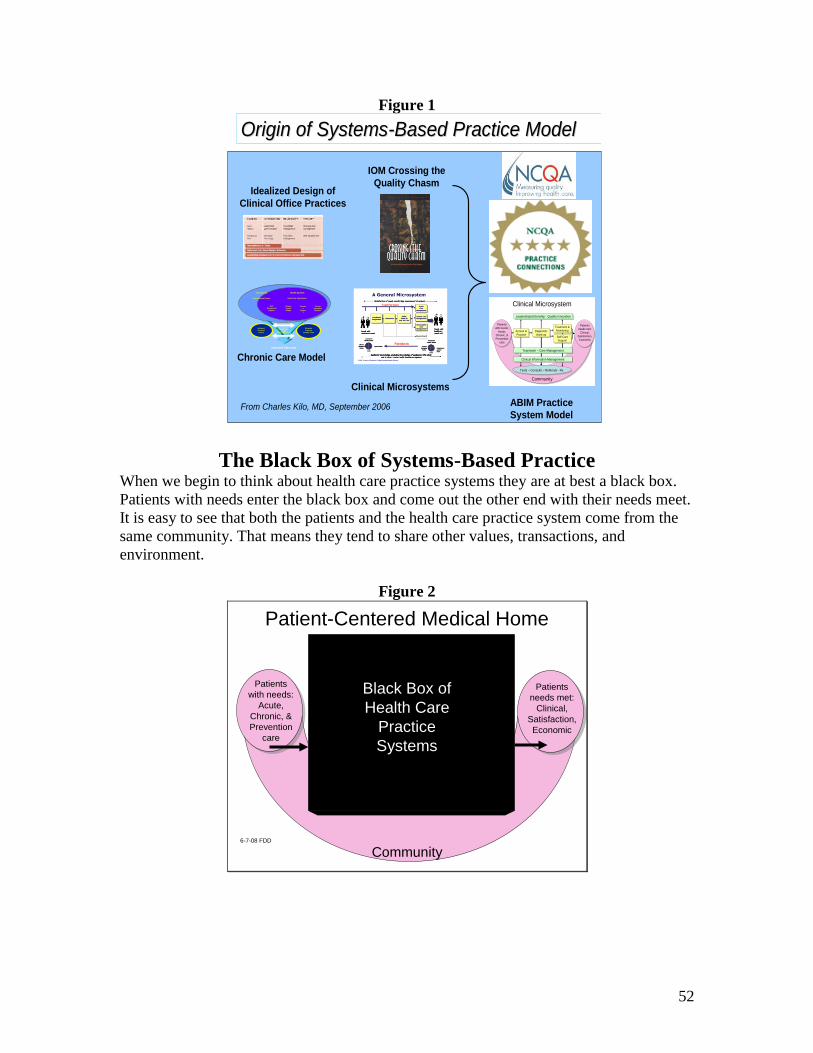
The Black Box of Systems-Based Practice When we begin to think about health care practice systems they are at best a black box.
Patients with needs enter the black box and come out the other end with their needs meet.
It is easy to see that both the patients and the health care practice system come from the
same community. That means they tend to share other values, transactions, and
environment.
Figure 2
Patient-Centered Medical Home
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Black Box of
Health Care
Practice
Systems
6-7-08 FDD
53
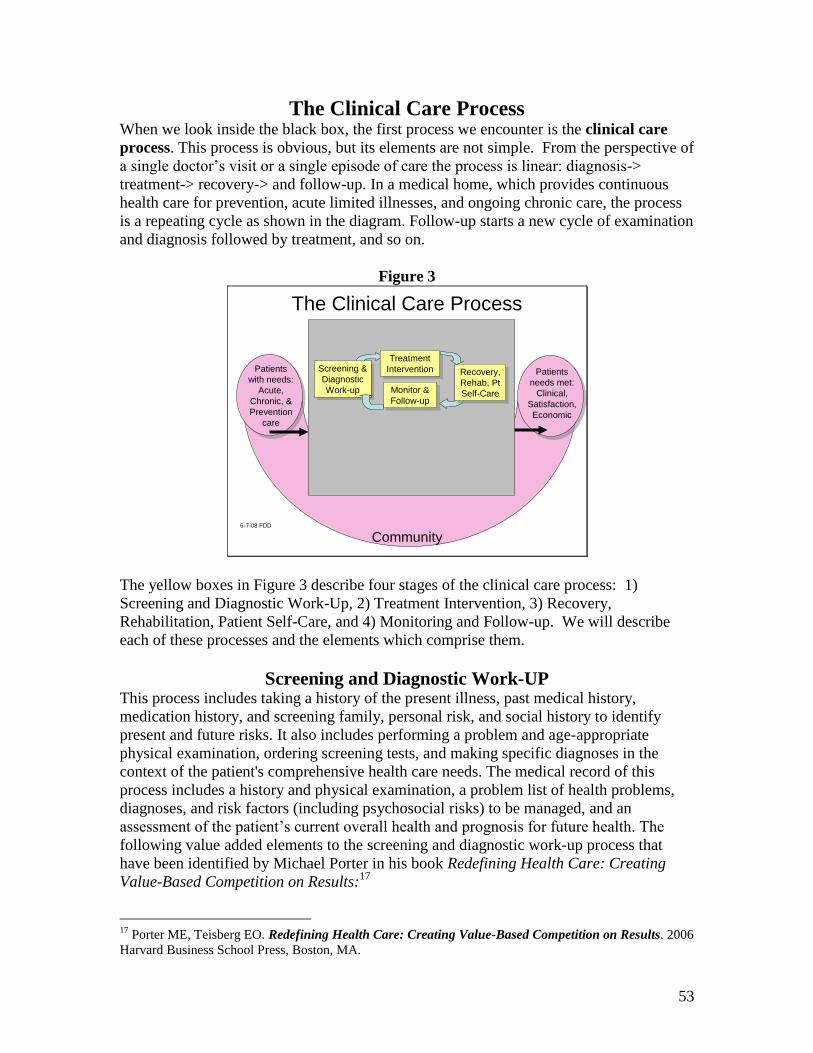
The Clinical Care Process When we look inside the black box, the first process we encounter is the clinical care
process. This process is obvious, but its elements are not simple. From the perspective of
a single doctor’s visit or a single episode of care the process is linear: diagnosis->
treatment-> recovery-> and follow-up. In a medical home, which provides continuous
health care for prevention, acute limited illnesses, and ongoing chronic care, the process
is a repeating cycle as shown in the diagram. Follow-up starts a new cycle of examination
and diagnosis followed by treatment, and so on.
Figure 3
The Clinical Care Process
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Recovery,
Rehab, Pt
Self-Care
Recovery,
Rehab, Pt
Self-Care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Screening &
Diagnostic
Work-up
Screening &
Diagnostic
Work-up
Treatment
Intervention
Treatment
Intervention
Monitor &
Follow-up
Monitor &
Follow-up
6-7-08 FDD
The yellow boxes in Figure 3 describe four stages of the clinical care process: 1)
Screening and Diagnostic Work-Up, 2) Treatment Intervention, 3) Recovery,
Rehabilitation, Patient Self-Care, and 4) Monitoring and Follow-up. We will describe
each of these processes and the elements which comprise them.
Screening and Diagnostic Work-UP This process includes taking a history of the present illness, past medical history,
medication history, and screening family, personal risk, and social history to identify
present and future risks. It also includes performing a problem and age-appropriate
physical examination, ordering screening tests, and making specific diagnoses in the
context of the patient's comprehensive health care needs. The medical record of this
process includes a history and physical examination, a problem list of health problems,
diagnoses, and risk factors (including psychosocial risks) to be managed, and an
assessment of the patient’s current overall health and prognosis for future health. The
following value added elements to the screening and diagnostic work-up process that
have been identified by Michael Porter in his book Redefining Health Care: Creating
Value-Based Competition on Results:17
17
Porter ME, Teisberg EO. Redefining Health Care: Creating Value-Based Competition on Results. 2006
Harvard Business School Press, Boston, MA.
54
Medical History – Taking a medical history is the core patient care competence
developed my medical and physicians assistant students. The process can be streamlined
by using patient questionnaires, assigning the registration clerk duties to administer
screening questions, and assigning rooming staff responsibility for routinely collecting
specific information.
Screening – Patient questionnaires standardize the screening history during the check-in
process for a medical visit, the registration staff can follow a screening decision
algorithm and alert office staff to take action on performing additional testing for
screening.
Identifying risk factors – An age-appropriate questionnaire combined with a decision
algorithm that can permit registration and rooming or nursing staff to identify risk factors
(e.g. smoking, sedentary lifestyle, medical illiteracy, psychosocial stress, etc.) for each
individual patient and for specific populations of patients using the medical home.
Specifying & organizing tests – Physicians, physicians assistants, and nurse clinicians
learn how to frame clinical problems, develop a differential diagnosis, and specify the
diagnostic tests that will confirm the correct diagnosis and rule out competing
possibilities. Decision support tools such as diagnostic criteria templates serve as useful
reminders to assure standardization of the common work-ups performed in the practice.
Nursing staff can organize the results of the diagnostic work-up and the reports from
consultants that permit the clinician to make the diagnosis and design an appropriate
therapeutic plan.
Interpreting Data (Making a Diagnosis and Prognosis) – Arguably the most important
value added process in the clinical method is making an accurate diagnosis based on the
clinical history, physical examination, and laboratory data. Physicians have the authority
to make a diagnosis and to supervise the diagnostic process of physicians assistants and
other midlevel clinicians. The diagnosis involves selecting the ICD-9 code that best fits
the physician’s interpretation of the information, explaining the illness according to
pathophysiologic theories, and assessing the prognosis of the condition for the patient’s
immediate and long-term health status.
Consulting with Specialists to Determine the Treatment Plan – For many problems,
the clinicians in a medical home will need to consult with medical and surgical specialists
to determine the most effective treatment for the patient’s condition. This process
involves framing the treatment questions for the consultant, making the referral for some
treatments, transferring the needed clinical information, and developing a personal
relationship with the consultant to determine the human and interpersonal factors that
may be important in coordinating the care in a patient-centered manner for each
individual patient.
Developing a Prevention Programs – Most routine risk factor reduction and prevention
programs for otherwise healthy individuals can be standardized and built into the routine
processes of the practice. The routine prevention programs can be initiated by the
55
nursing staff of the practice. For the patients with complex chronic conditions, the
clinicians in the practice must design an individualized prevention program. Patients
who have already suffered loss of health need to prevent further loss in order to retain a
high quality of life. Both the routine and customized prevention programs involve
coordinating community services for providing patient self-care support.
Treatment Intervention
The second clinical care process is treatment intervention. The physician or team
develops a health management plan for the treatment of diagnoses, diagnostic plan for
problems, and counseling or treatment to mitigate health risks. In a medical home, all of
the undiagnosed problems and risks factors are addressed in the treatment plan. The
record of the treatment intervention is a medication list, treatment plan (or orders sheet),
written patient instructions, prescriptions, and order forms for diagnostic tests,
consultations, or referrals. The value-added elements to the treatment Intervention
process are the responsibility of the clinicians in the practice, and include the following:
Ordering & administering drug therapy – The most common and arguably the most
treatment intervention is prescribing a specific medication, does, frequency, number or
volume to be dispensed, and number of refills authorized. An electronic prescription
writer and electronic prescription decision support tools make the process more accurate.
As will be described below, the use of clinical information management will make this
proc is the ordering and prescribing drug therapy.
Performing procedures – Clinicians perform both diagnostic and therapeutic procedures
in the medical practice. These include surgery, biopsy, needle injections and aspirations.
Medical and physicians assistants students learn simple procedures such as passing tubes
per os, drawing venous blood, giving intravenous infusions, administering inhalation
therapy, performing injections and needle aspirations, and suturing simple skin
lacerations. Competence in performing more advanced office or hospital procedures are
learned during residency training or on the job under direct supervision.
Performing counseling therapy – Basic competence in communication and
interpersonal skills includes conducting diagnostic and therapeutic conversations with
patients and their families. Making shared therapeutic decisions in which the patient’s
values are taken into consideration when planning the therapeutic intervention is an
essential value-added skill for this process. Additionally, physicians develop competence
in motivational interviewing to encourage patients to take self-care actions or to pursue
complex or even risky procedures that are likely to help them achieve their health goals.
Counseling also involves developing the therapeutic relationship that permits reduction in
suffering from fear and anxiety, supporting patients during grief, and helping others gain
insight and coping skills in dealing with the health problems they face. These advanced
skills are learned in the context of the specific problems managed during residency
training.
Hospitalization – In a sense, a hospitalization is a complex therapeutic intervention. It is
a form of a health care ―Visit,‖ but it is also a standardized approach to diagnosis and

56
treatment of particular problems that require an organized system of staff and specialist
physicians using specialized technology to treat a problem. Medical students and other
student clinicians learn the hospital systems-based practice during school and during
specialized training. Coordination of admission to the hospital and following
hospitalization are essential elements of the therapeutic intervention process.
Recovery, Rehabilitation, and Patient Self-Care
The third clinical care process is recovery, rehabilitation and patient self-care. This
process is most easily seen to be a discrete form of care following a surgical procedure or
a course of chemotherapy. For patients with chronic illness or ongoing disability, this
process is part of the continuous cycle of clinical care in which self-care becomes an
essential skill. For all patients self-care is an important in changing health habits. The
medical record for this process is additional assessments of patient needs, plans for
intervention and progress notes for patient self-care instruction.
The value-added elements of the Recovery, Rehabilitation and Patient Self-Care process
are frequently given short shrift in medical student and even residency education. The
nursing profession focuses most on this stage of care both in hospital and ambulatory care.
Home health nursing is the profession most intimately focusing care on the rehabilitation
and recovery stage of illness.
Porter identifies some elements of this process and I have added others related to the
activation of patients in self-care, home-health coordination, and community resource
coordination. The physician specialties of Geriatrics and Physical Medicine and
Rehabilitation focus on this process of the clinical care method, but most others do not.
Inpatient recovery – Recovery from a surgical procedure or a serious medical illness is a
complex bio-psycho-social-spiritual process. There is the biological process of wound
and tissue repair, regeneration, and scarring. There is also the psychological
readjustment to pain, bodily dysfunction, and temporary or perhaps permanent disability.
All serious illness disrupts a patient’s social structure creating a period of vulnerability
and lost of role function and social status. All illness, particularly serious illness, calls
into question the meaning of life and the spiritual dimensions of our personhood.
Although these aspects of recovery often occur in the hospital, they continue following
discharge and must be handed-off to the medical home for seamless transfer of the
recovery and adaptation process. Nursing
Inpatient & outpatient rehabilitation – The value-added element of recovery is often
overlooked by the primary care medical home clinicians as well as specialty care
clinicians. It is even undervalued by hospital services. Nursing professionals perform this
process and in particular, cases such as stroke, amputation, or spine care by rehabilitation
specialist physicians. Handoff problems and coordination of care problems are
particularly problematic for the medical home, which may be less involved in this type of
care. It is important for a medical home to keep a registry of patients receiving
rehabilitation care to assure that case management is being provided.
57
Therapy fine-tuning – During the recovery and rehabilitation, process of clinical care
initial therapy must be repeatedly adjusted as the body heals. Doses of medications may
need to be changed or discontinued. Medical education programs are beginning to focus
on the importance of the hand-off of responsibility for this process of care. The
specialists often perform fine-tuning during this phase of care – but failure to coordinate
these changes in the treatment between the medical home and the specialists creates
confusion about who has the responsibility for these changes and communicating the
changes to others involved in the care.
Discharge plan – Following hospitalization or completion of treatment by a specialist the
discharge plan is the instrument for hand-off of responsibilities for care and coordinating
the information needed for the medical home to assume responsibility for care. This is a
complex process involving coordination of nursing, physician, pharmacy, home-health,
patient education, follow-up visit scheduling and transportation. Nursing services have
been assigned responsibility for the execution of the process following the physician’s
order to discharge the patient. What is often missing is the clear communication with the
medical home about the plans for follow-up and instructions for actions to be taken next.
As will be described below, systems for managing this transition must be developed to
assure safety and effectiveness of the transfer. Moreover, the engaging of the patient,
family and community agencies are essential to making sure that the hand-off form
nearly total care in the hospital system to the somewhat chaotic and uncoordinated
ambulatory setting is effective. The more complex the hand off the more important it is
for the medical home to have a complex case manager responsibility for receiving the
hand-off.
Activation and education in self-care – The chronic care model describes the
importance of having a prepared patient to engage in their own care.18
The patient, his or
her family, and possibly other caregivers are involved in the recovery and rehabilitation
process following an acute or serious episode of illness. Whether this involves a
hospitalization or is limited to coordinated ambulatory care for a serious illness, this
function is essential. The value-added element of patient activation and education in self-
care is best performed by medical home nursing and social work staff.
Home-health coordination – The nursing staff of the medical home and the nursing staff
of home health services and community nursing services add value to this process by
coordinating their efforts in accordance with the treatment plan. Unfortunately the home
health agencies have become separated from primary care medical homes; and except in
some cases in geriatrics care or in other special needs care, the coordination of these
services is haphazard, inefficiently, and ineffective.
Community agency service coordination – Most medical homes do not have social
work staff to perform this function. It is particularly important for obtaining reduced rate
18
Reference: Chronic Care Model: Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients
with chronic illness: the chronic care model, II. JAMA. 2002;288:1909-1914.
58
medications, obtaining mental health, legal, and social support services, and finding
financial aid. Although nursing home health services and some experience with this
function, they are usually exceeding the scope of their education. The medical home,
particularly those that serve poor and underserved populations or populations of patients
with chronic conditions can add substantial value to the clinical care process by adding
these social services.
Monitoring and Follow-up The fourth process in clinical care is monitoring and follow-up. It involves teamwork to
review laboratory results, consultation reports, revise the patient’s health assessment,
problem list, and modify the treatment plan and self-care plan. This process can occur in
a follow-up visit if it is important to perform monitoring physical examinations or to have
a face-to-face conversation with the patient. Otherwise, in the medical home much of the
follow-up or inter-visit care can be performed by the health care tem with telephone, e-
mail, and other non-visit engagement with the patient. The medical record of this process
is the monitoring flow sheet, the patient care registry for prevention and chronic illness
care, phone notes, and changes in prescriptions, medication lists, and progress notes.
The value-added elements to the Monitoring and Follow-up process of clinical care is
one of the most important yet poorly recognized functions. I have combined Porter’s
functions of ―Preparing‖ and ―Monitoring‖ into a single function that is conducted by
physicians and the medical home staff. It is in conducting this process of clinical care
that the medical home demonstrates its effectiveness in coordinating care and managing
the multiple resources necessary for high quality care.
Monitoring patient’s health condition – The medical home staff develops a plan for
monitoring the patients’ acute, chronic and preventive conditions. Patient registries make
tracking the schedule for when services are due efficient. Effective monitoring involves
pro-active contacting patients to make certain that they receive follow-up laboratory
testing, physical examinations, and other services recommended for the treatment of their
condition.
Monitoring complications with therapy – Guidelines for therapy usually include the
frequency and type of laboratory or clinical monitoring that should be done to recognize
complications early or to prevent them. Anticoagulation clinics have demonstrated their
effectiveness in preventing complications of therapy and more rapidly achieving desired
levels of anticoagulation. Most practices rely on the patient’s own interest and initiative
to arrange follow-up. Practices that have adopted pro-active monitoring not only
improve their performance measures, but also improve their patient satisfaction with the
service. ,
Monitoring lifestyle modification – Making lifestyle habit modifications is difficult and
regular and frequent monitoring provides the sort of accountability that most patients
need to stick to a change in lifestyle. A preventive care registry used by patient education
and self-care training nursing staff enhances the effectiveness of the medical home.
59
Pro-active preparation & coordination of resources – The medical home employs a
nursing and medical assistant staff that stays in contact with patients, consultants, and
vendor services to assure that the diagnostic and therapeutic plan is executed. The staff
pro-actively stays in contact with hospitalized patients and their caregivers and is
prepared to receive the hand-off upon discharge. Additionally, a patient-centered medical
home staff prepares for a patient visit to assure that services recommended by guidelines
are provided and that the results of tests and consultations are available for review with
the patient during the visit. Such pro-active planning requires tracking and monitoring
systems, case management for complex patients, and dividing the roles and
responsibilities so that anticipated patient care needs can be met in a timely manner.
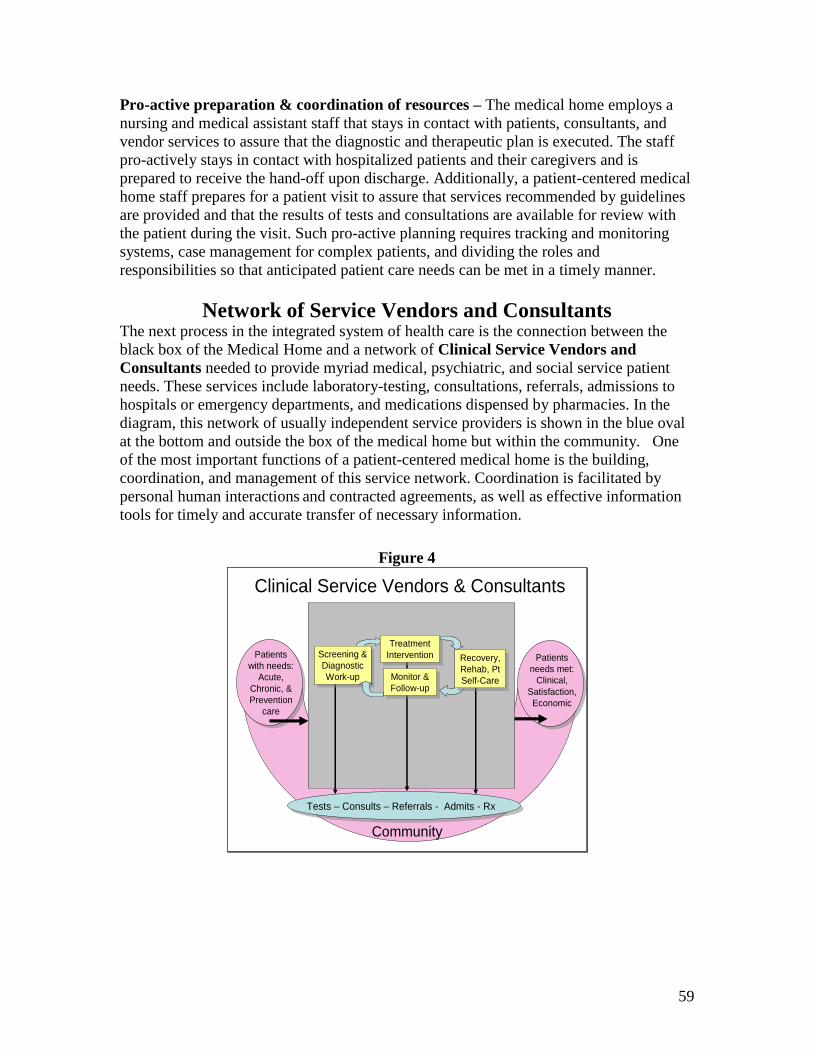
Network of Service Vendors and Consultants The next process in the integrated system of health care is the connection between the
black box of the Medical Home and a network of Clinical Service Vendors and
Consultants needed to provide myriad medical, psychiatric, and social service patient
needs. These services include laboratory-testing, consultations, referrals, admissions to
hospitals or emergency departments, and medications dispensed by pharmacies. In the
diagram, this network of usually independent service providers is shown in the blue oval
at the bottom and outside the box of the medical home but within the community. One
of the most important functions of a patient-centered medical home is the building,
coordination, and management of this service network. Coordination is facilitated by
personal human interactions and contracted agreements, as well as effective information
tools for timely and accurate transfer of necessary information.
Figure 4
Clinical Service Vendors & Consultants
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Recovery,
Rehab, Pt
Self-Care
Recovery,
Rehab, Pt
Self-Care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Screening &
Diagnostic
Work-up
Screening &
Diagnostic
Work-up
Treatment
Intervention
Treatment
Intervention
Monitor &
Follow-up
Monitor &
Follow-up
Tests – Consults – Referrals - Admits - Rx
60
The following elements shape and maintain the clinical service vendor and consultant
network. This list was developed at the ABIM Foundation’s Stepping Up to the Plate
conference held in Washington, DC, March 2007.19
Lab & Imaging Test Ordering & Tracking - Medical homes establish vendor contracts
with laboratory and imaging services. Within these contracts are the agreements for how
the order for the tests will be communicated to the vendor, who will draw blood and
transport it, and how the reports will be returned to the medical home. Electronic
transmission of the order to the laboratory and of the report to the medical home with a
computer application that tracks that status of the request permits careful monitoring of
the service according to the agreement.
Service Agreements and Referral Contracts – Agreements between medical homes
and specialty consultants have been introduced into the VA system, other integrated
health care systems, and some practicing communities. In these the primary care
physicians and the specialist physicians develop compact specifying expectations in
referral for services. The compact includes the aim for ―respecting‖ the coordinator of
the care which should be the primary care physician. It includes clear lines of
responsibility and accountability for the care of the patient and the expectation that all
members of the team will be informed of the actions of others. The compact is based on
the idea that each patient has an integrated management plan.
Integrated Treatment Plan, Fax-Back Reports, and Referral Database – The medical
home develops an integrated treatment plan for patients who are being co-managed with
specialist physicians. The practice sets up a system for receiving reports from the
specialist consults either in the form of fax-back reports or other electronically
transmitted information. Lastly the medical home keeps a referral database tracking the
service and quality performance of the consultants and referral specialists so that the
network may be refined and feedback may be provided to the network participants to
improve the services. Currently this practice is more theoretical than used in practice.
The Doc2Doc referral system being studied in the School of Community Medicine is an
early example of this process.
Referral & Consultation Request and Tracking - Medical Homes need a process for
standardizing the referral and consultation requesting process and tracking the progress of
the request until it is completed. The American Academy of Family Practice has
developed the Chronic Care Record (CCR) which is an HL-7 technology for transmitting
the core data needed for coordination of care between a consultant and a medical home.
Except in integrated health care systems this capability is not often available. The OU
School of Community Medicine is currently working on ways to implement this process
within its clinical services.
Nurse Care Management, Discharge Summary Fax Backs, & Medication
Reconciliation – Medical homes assign a nurse care manager to receive the hand-off
from hospitalization to the medical home. In addition to identifying the personnel to
19
http://www.abimfoundation.org/quality/suttp.shtm accessed July 5, 2008.
61
receive the handoff, the practice must establish a process for receiving discharge
summaries by fax and conduct a post-hospitalization medication reconciliation with the
pre-hospitalization medical home medications. This coordination of care activities
clarifies the delegation of responsibility for follow-up and continuing care.
Prescription Management Process – The medical home establishes vendor
relationships with pharmacies that will fill patient prescriptions. Faxing or e-transmitting
prescriptions directly to the pharmacy are highly desirable. Protocols for nursing staff to
authorize chronic medications can be instituted. Decision support for checking
medications for errors and identifying drug-drug interactions are also important safety
checks. (Revised April 25, 2007)
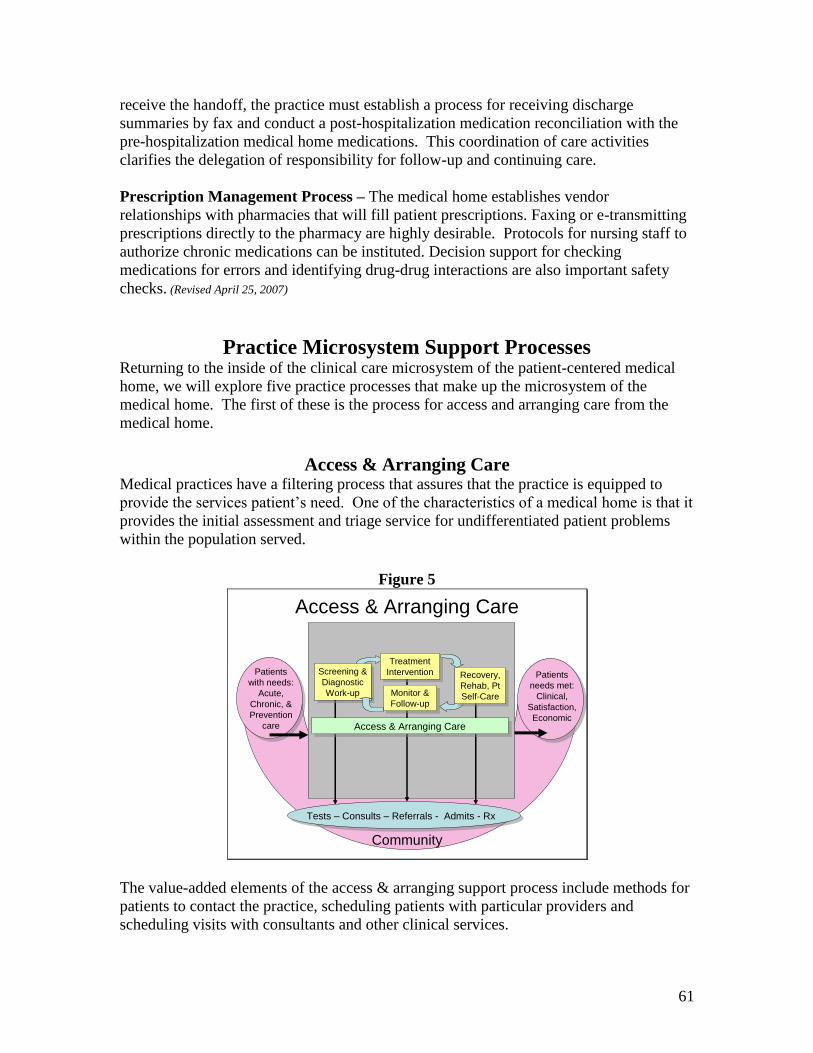
Practice Microsystem Support Processes Returning to the inside of the clinical care microsystem of the patient-centered medical
home, we will explore five practice processes that make up the microsystem of the
medical home. The first of these is the process for access and arranging care from the
medical home.
Access & Arranging Care Medical practices have a filtering process that assures that the practice is equipped to
provide the services patient’s need. One of the characteristics of a medical home is that it
provides the initial assessment and triage service for undifferentiated patient problems
within the population served.
Figure 5
Access & Arranging Care
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Recovery,
Rehab, Pt
Self-Care
Recovery,
Rehab, Pt
Self-Care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Screening &
Diagnostic
Work-up
Screening &
Diagnostic
Work-up
Treatment
Intervention
Treatment
Intervention
Monitor &
Follow-up
Monitor &
Follow-up
Tests – Consults – Referrals - Admits - Rx
Access & Arranging CareAccess & Arranging Care
The value-added elements of the access & arranging support process include methods for
patients to contact the practice, scheduling patients with particular providers and
scheduling visits with consultants and other clinical services.

62
Assignment to Primary Provider or Team – The medical home has a standardized
process that registration staff follows to make certain that every patient in the medical
home is assigned to a primary clinician and/or practice team. The practice establishes
policies and procedures for transferring patients to other primary providers, and has a
system for back up when the primary provider is unavailable. The practice has written
policies for provider assignment and uses measures to determine the degree of
compliance with its policies.
Routine- & After-hours Contact for Information – The medical home establishes
policies and processes to permit patients 24/7 telephone (or e-mail) access to a nurse or
clinician in the practice who has access to the patient’s medical record, integrated
treatment plan, and can answer medical questions or process questions about obtaining
services. The medical home has an agreement for the coordination of urgent visits within
24 hours for its patients. It also has an agreement with an emergency department for
coordination of emergency care for its patients and for the follow-up of that care in the
medical home. The medical home has policies guiding these processes and measures of
the effectiveness of the processes in adhering to the policies.
Scheduling Contact with the Primary Provider – Medical Home practices make every
effort to connect patients with their primary clinician or primary team. The practice
measures its compliance with its policies for continuity of care and reports its
performance in adhering to the policies while also providing urgent (24-hour) visit
availability to patients when needed. When someone other than the patient’s primary
clinician conducts a patient visit, the medical home has a process for assuring that the
primary clinician is informed of the actions taken in the visit conducted for him or her.
Coordinating Contact with Other Providers – Medical Home practices arrange the
visits with other primary providers in the absence of the patient’s assigned clinician.
They also arrange the visits with specialists and consultants. A patient case manager is
assigned to the coordination of multiple visits for high utilization patients.
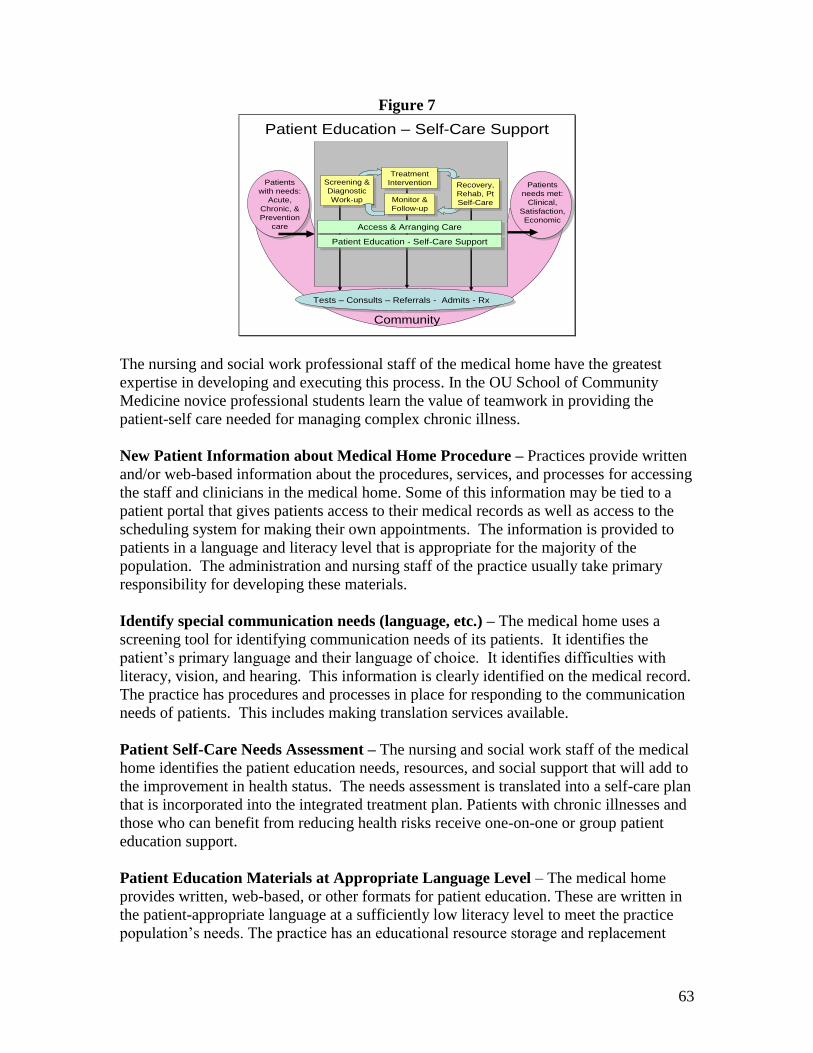
Patient Education and Self-Care Support The second support process, shown in figure 6, is the organization of the staff and
resources to provide Patient Education and Self-Care Support. Medical and physicians
assistant students learn to perform some of this function in providing patient self-care
instruction, but most of the value-added elements of this process are provided by practice
nursing and social work staff.20
20
Pare G, Jaana M, Sicotte C. Systematic Review of Home Telemonitoring for Chronic Diseases: The Evidence Base.
Journal of the American Medical Informatics Association Volume 14 Number 3 May / June 2007.
63
Figure 7
Patient Education – Self-Care Support
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Recovery,
Rehab, Pt
Self-Care
Recovery,
Rehab, Pt
Self-Care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Screening &
Diagnostic
Work-up
Screening &
Diagnostic
Work-up
Treatment
Intervention
Treatment
Intervention
Monitor &
Follow-up
Monitor &
Follow-up
Tests – Consults – Referrals - Admits - Rx
Access & Arranging CareAccess & Arranging Care
Patient Education - Self-Care SupportPatient Education - Self-Care Support
The nursing and social work professional staff of the medical home have the greatest
expertise in developing and executing this process. In the OU School of Community
Medicine novice professional students learn the value of teamwork in providing the
patient-self care needed for managing complex chronic illness.
New Patient Information about Medical Home Procedure – Practices provide written
and/or web-based information about the procedures, services, and processes for accessing
the staff and clinicians in the medical home. Some of this information may be tied to a
patient portal that gives patients access to their medical records as well as access to the
scheduling system for making their own appointments. The information is provided to
patients in a language and literacy level that is appropriate for the majority of the
population. The administration and nursing staff of the practice usually take primary
responsibility for developing these materials.
Identify special communication needs (language, etc.) – The medical home uses a
screening tool for identifying communication needs of its patients. It identifies the
patient’s primary language and their language of choice. It identifies difficulties with
literacy, vision, and hearing. This information is clearly identified on the medical record.
The practice has procedures and processes in place for responding to the communication
needs of patients. This includes making translation services available.
Patient Self-Care Needs Assessment – The nursing and social work staff of the medical
home identifies the patient education needs, resources, and social support that will add to
the improvement in health status. The needs assessment is translated into a self-care plan
that is incorporated into the integrated treatment plan. Patients with chronic illnesses and
those who can benefit from reducing health risks receive one-on-one or group patient
education support.
Patient Education Materials at Appropriate Language Level – The medical home
provides written, web-based, or other formats for patient education. These are written in
the patient-appropriate language at a sufficiently low literacy level to meet the practice
population’s needs. The practice has an educational resource storage and replacement
64
process. The nursing staff of the practice manages the patient education resources in the
practice.
Patient Self-Monitoring Training and Use of Logs for Reporting – A medical home
teaches to perform self-monitoring of their progress in making lifestyle changes to
improve health and to monitor blood sugars in diabetes and blood pressure in
hypertension and congestive heart failure. Patient with asthma monitor their peak flows
and patients with arthritis and pain syndromes may keep logs of their pain and response
to treatment. Staff instructs patients in the proper monitoring technique and how to keep
the records of the results in logs or graphs. Technologically advanced practices provide
patients with monitoring and reporting tools that transmit data electronically to the
medical home.
Referral to Community education & support programs for self-care – The nursing
and social work staff accumulate the community education and support programs for
patient self-care support. Mental health groups, groups focused on learning coping skills,
disease peer support groups, web discussion groups, and behavioral therapy groups
augment the patient education provided in the medical home. Community-based care
management programs and case management can be very helpful. Medical Home
practices participate in the community services that support patient self-care.
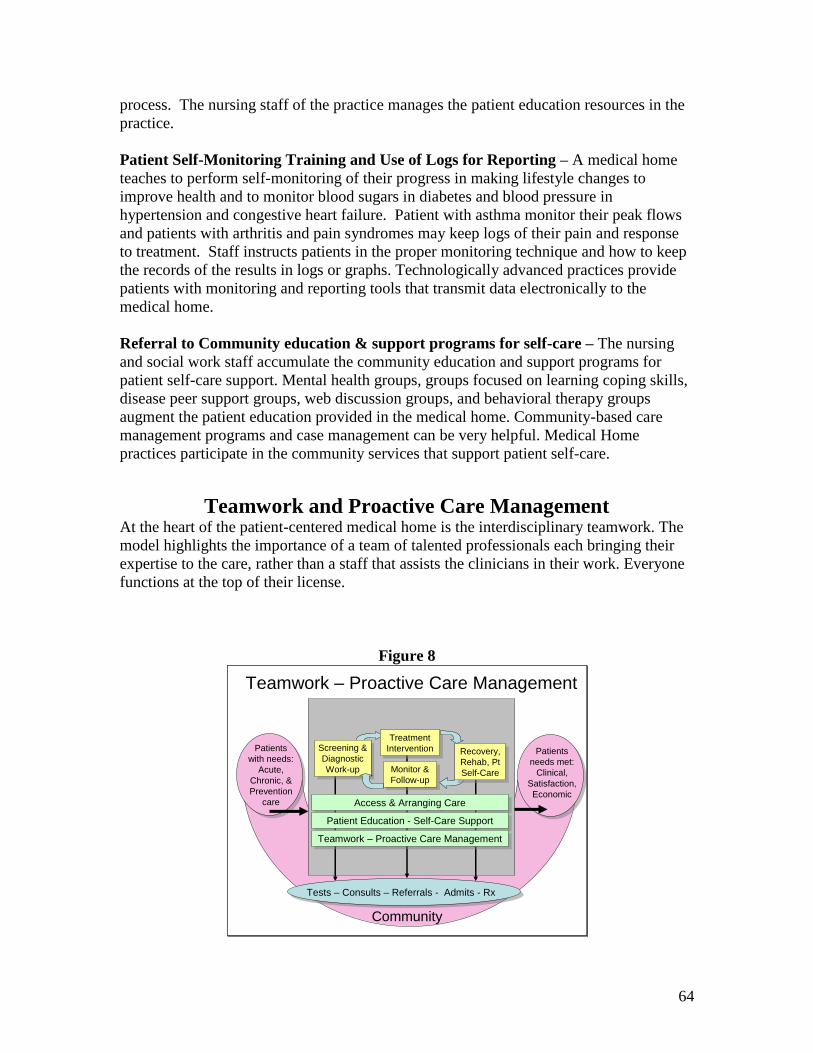
Teamwork and Proactive Care Management At the heart of the patient-centered medical home is the interdisciplinary teamwork. The
model highlights the importance of a team of talented professionals each bringing their
expertise to the care, rather than a staff that assists the clinicians in their work. Everyone
functions at the top of their license.
Figure 8
Teamwork – Proactive Care Management
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Recovery,
Rehab, Pt
Self-Care
Recovery,
Rehab, Pt
Self-Care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Screening &
Diagnostic
Work-up
Screening &
Diagnostic
Work-up
Treatment
Intervention
Treatment
Intervention
Monitor &
Follow-up
Monitor &
Follow-up
Tests – Consults – Referrals - Admits - Rx
Access & Arranging CareAccess & Arranging Care
Patient Education - Self-Care SupportPatient Education - Self-Care Support
Teamwork – Proactive Care ManagementTeamwork – Proactive Care Management

65
Pro-active care management is best performed by nursing and social work staff whose
professional education prepares them for coordination of services and integrating health
care plans into the patient’s daily life. The pro-active care management provides
anticipatory continuing care to patients with chronic conditions and provides preventive
services for screening and behavior change. Usually the care manager is a nurse or nurse
practitioner who is responsible for a number of patients with a common chronic illness or
for patients who are high utilizes of health care services, such as those with heart failure
or multiple chronic conditions. The value-added elements of the Teamwork and Proactive
Care Management process include:
Use Pro-Active Patient Contact and Follow-Up – Instead of relying on patient initiated
visits for care, the medical home’s care management team uses a care management
registry to plan contacts with patients to determine their progress and initiate the next
visit. They call the patient after the visit checking on how they are doing. They
coordinate community outreach, sending patient reminders for services that are due, and
coordinating the various components of the overall management plan. The Care
Management may be done within the office or may be delegated to services outside.
Regardless of the method used for delivering the services, the comprehensive care system
coordinates the services. It was not until the health plans organized external care or case
management organizations of services that this function became a structured entity. It
had formerly been a component of the basic clinical method for patients with chronic
disease. It was the failure of many practices to provide this service effectively and their
absence of the necessary data and information management infrastructure that led to data
rich health plans to organize nurse-hired and directed case management services. These
can be returned to the office system with the addition of advanced information
management and delegation of roles and responsibilities among the staff.
Use Standardized Health Assessment Questionnaire, History & PE form – The
medical home designs a standardized health assessment questionnaire and standardized
templates for history and physical examination. The staff team can participates in the
completion of the standardized health assessment by filling in cells of the templates.
Patients can complete a pre-visit questionnaire to provide screening health information.
Use Problem and Risk Factor List – The clinicians in the medical home generate a
comprehensive problem and risk factor list which contains diagnoses, undiagnosed
problems, and risks for future illness. The problem list is updated periodically and serves
as an index to the patient’s medical record.
Use Medication & Allergy List – A medication list and an allergy list are generated and
updated at nearly every visit. Reconciliation of the medication list should occur
following any hospitalization or consultation.
Use Integrated Care Management Plan – The clinicians, nursing staff and social work
staff operate from the same integrated care management plan. This plan indicates the
goals for therapy, the medications and other treatments, social services, patient education
and self-care support, patient home monitoring, and follow-up testing and intervals. The
66
integrated care management plan is a ―play book‖ guiding everyone’s participation in the
patient’s care.
Use Care Management Flow Sheets (Patient Registry) – Within the patient’s
individual medical record flow sheets contains the symptoms, physical examination
findings, and laboratory tests that are used to monitor the progress of the treatment and
recovery. At each visit the data is recorded in the flow sheet so that progress may be
tracked over time, trends detected, and variations from the expected easily visualized. A
patient registry electronically tracks measures of services due for preventive care and for
chronic illness care and permits notification of patients. The registry also provides
guidance for planning a visit. Finally the registry can calculate quality measures for
certain diseases and preventive services.
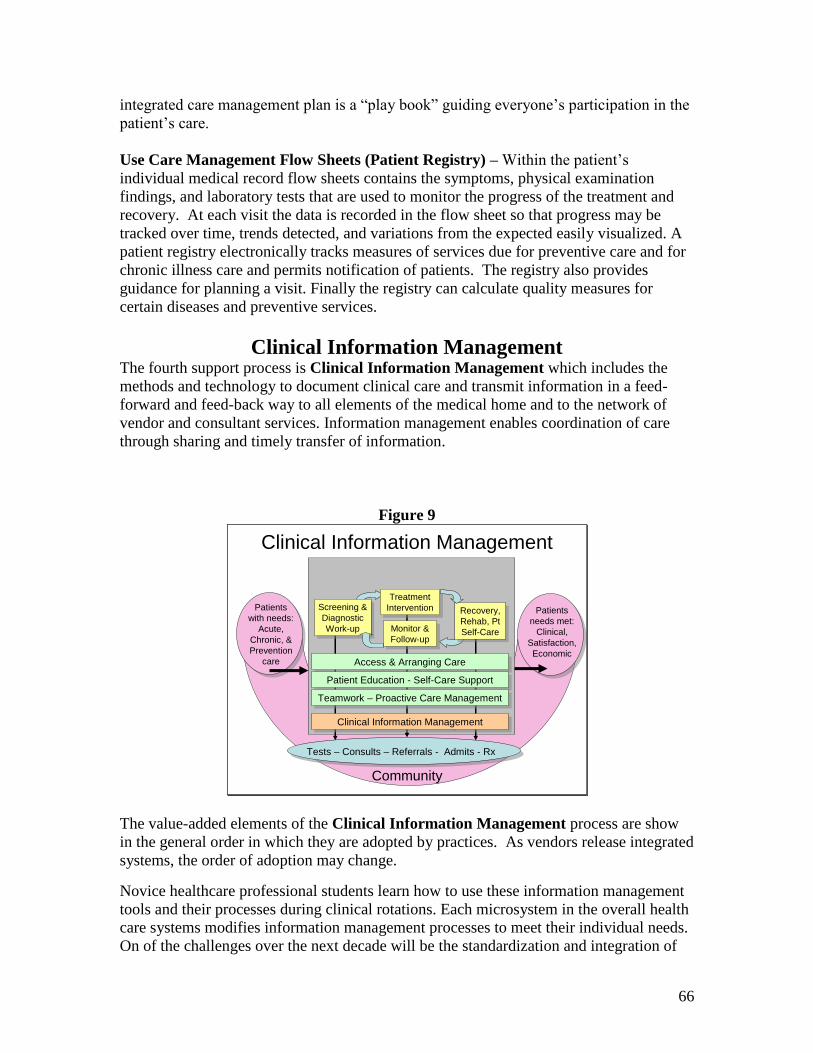
Clinical Information Management The fourth support process is Clinical Information Management which includes the
methods and technology to document clinical care and transmit information in a feed-
forward and feed-back way to all elements of the medical home and to the network of
vendor and consultant services. Information management enables coordination of care
through sharing and timely transfer of information.
Figure 9
Clinical Information Management
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Recovery,
Rehab, Pt
Self-Care
Recovery,
Rehab, Pt
Self-Care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Screening &
Diagnostic
Work-up
Screening &
Diagnostic
Work-up
Treatment
Intervention
Treatment
Intervention
Monitor &
Follow-up
Monitor &
Follow-up
Tests – Consults – Referrals - Admits - Rx
Access & Arranging CareAccess & Arranging Care
Patient Education - Self-Care SupportPatient Education - Self-Care Support
Teamwork – Proactive Care ManagementTeamwork – Proactive Care Management
Clinical Information ManagementClinical Information Management
The value-added elements of the Clinical Information Management process are show
in the general order in which they are adopted by practices. As vendors release integrated
systems, the order of adoption may change.
Novice healthcare professional students learn how to use these information management
tools and their processes during clinical rotations. Each microsystem in the overall health
care systems modifies information management processes to meet their individual needs.
On of the challenges over the next decade will be the standardization and integration of
67
clinical information management processes. A new medical specialty of Medical
Informatics has emerged to tackle this problem.
Practice management system – an electronic system which tracks patient registration
demographics, billing information, ICD-9 and CPT codes used for submitting insurance
claims and bills has been adopted by nearly every practice. The more sophisticated
practice management systems generate financial reports for planning and projecting
revenues. Some systems also track office purchases, expenses, personnel records, payroll,
and other business operations of the practice.
Patient Visit Scheduling – the first addition to most practice management systems is
usually a visit scheduling program which permits scheduling multiple clinicians in the
practice with varying lengths of appointment times for patients.
Phone Message Management Systems – include automated answering, routing
algorithms, and voice mail. More advanced systems track efficiency of calls. Some
sophisticated systems provide call logs and branching call-triage systems. As of 2008,
most practices use a paper record of telephone messages, and rely on pagers, cell-phones,
and answering services for after hours calls.
Medical Record & Document file, fax and scan system – Paper medical records are
kept in a record file system. The individual patient record holds all of the clinical
documents about the patient’s care. The greatest advantage of the electronic medical
record is reducing the physical space and time required for filing and locating missing
records and handing the stacks of paper that must be filed into the record. Unfortunately,
until all reports are received electronically, it will be necessary to track and scan into the
EMR a large number of documents that are still mailed and faxed to offices.
Consult and Referral Tracking Process– Medical homes track the status of the consults
and referrals to other physicians. In most practices the tracking is performed manually by
nurses who keep a paper record or tickler file of important pending consultations that
may require a call to the consultant to follow-up when an expected call or report has not
been received in a timely manner. Safety-net health care systems have a particularly
difficult time tracking consultation because the network of referring physicians and
consultants has not been established.
Test Tracking Process – Almost all practices order a large number of laboratory tests for
diagnosis and follow-up monitoring of treatment. As test ordering and reporting systems
become automated, the tracking becomes less important. In patient-centered medical
homes the practices critical laboratory testing reports to assure that they have been
completed, and the results have been reported back to the patient.
Image Tracking System – As x-rays, scans, ultrasounds, ECG’s and other imaging
examinations become digitized they can be transmitted, retrieved, and stored
electronically. Patient-Centered Medical Homes use a process for tracking the critical
68
imaging requests. The most sophisticated integrated systems permit the clinician to
access the actual image electronically.
Care Management Registry – As stated above, the single most important tool for
providing pro-active care management for a Patient-Centered Medical Home is the care
management registry. This is a paper or electronic tool that keeps a record of all of the
patients with a particular chronic condition or a particular risk category for prevention
services. There are three types of care management registries: high risk patient registry
(these are the patients who have frequent hospital admissions or ER visits and whose care
can benefit from aggressive care management); prevention registry (this is particularly
useful for assuring that the well-child screening and adult preventive services are
provided to patients according to a specified schedule); and a chronic care registry (for
patients with chronic conditions, e.g. diabetes, asthma, CKD, etc. who require close
follow-up monitoring for quality care). Registries perform three functions: 1) visit
planning – providing a list of the services that a patient is due to receive at a particular
visit, 2) patient reminder lists of services for which the patient should be notified to make
an appointment to receive, and 3) the next element – providing quality measure reports of
practice performance.
Reports for Clinical and Financial Practice Improvement – Improvement in the
efficiency and effectiveness of the practice requires receiving performance measurement
reports. The care management registry and practice management system can feed data
into a process that calculates performance measures and provides the leadership of the
practice with a management dashboard of quality metrics. The calculation of quality and
financially performance measures does not happen automatically, and even when
integrated electronic records deliver these reports, the practice must build a Quality
Improvement process into the practice. That Patient Centered Medical Home process
will be discussed in the next section.
Electronic Health Record – Coded Clinical Data – We have not discussed the
electronic medical record (EMR) or electronic health record (HER) before now, because
many electronic medical records are simple word processors which permit the
documentation of large volumes of text data and eliminate the need for paper storage
cabinets. The real strength in the EHR is the collection of clinical data in coded,
electronically retrievable form. Data must be recorded as codes in templates rather than
as text. Moreover, these templates must use standardized codes so that the data can be
transmitted to other clinicians’ EHRs and may be used to calculate the measures and
actions needed for the care management registry and even the practice management
system.
Patient Portal – As more patients use the internet for communication, they also wish to
communicate with their medical home through e-mail. A patient portal permits two-way
communication between the patient and the staff or clinician in the medical home. Some
practices provide electronic visits through the patient portal (DocVia and RelayHealth).
Some portals permit patients to select appointment times on the internet; others collect
69
registration and even clinical data through the portal. Some patient portals provide nurse
consultations, patient education, and prescription refill services.
E-Prescription Management – Probably the most timesaving information management
process is an electronic prescription management system, which include prescription
writer that is tied to drug prescribing information databases with or without clinical
decision support tools. The most efficient models are actually tied to the patients’
demographic and clinical data so that specific decision support may be provided for drug
interactions and potential adverse events. When the prescription management system is
tied to the patient’s health plan formulary specific medications can be selected at the time
of prescription and when these formularies change, the changes can be automatically
updated in the patient’s care process. In addition to having a printed prescription at the
time of the visit, some prescription management systems are connected to the patient’s
pharmacy and the transmission of the prescription information is completely automated
electronically.
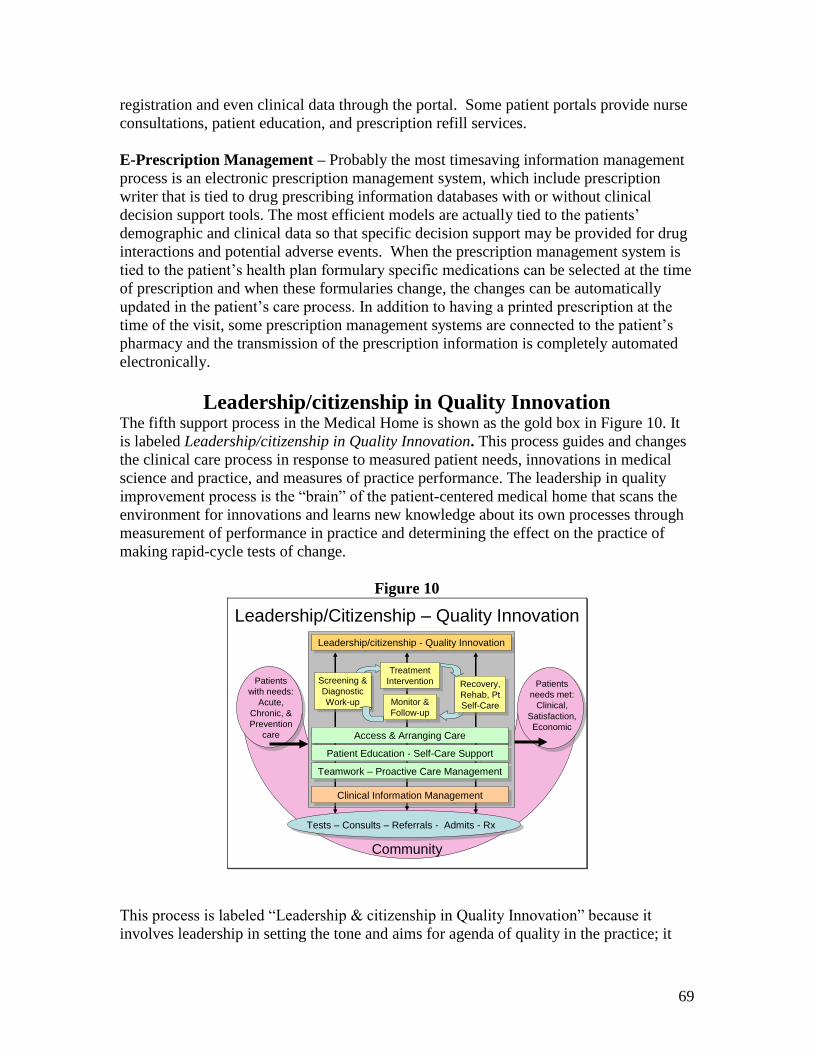
Leadership/citizenship in Quality Innovation The fifth support process in the Medical Home is shown as the gold box in Figure 10. It
is labeled Leadership/citizenship in Quality Innovation. This process guides and changes
the clinical care process in response to measured patient needs, innovations in medical
science and practice, and measures of practice performance. The leadership in quality
improvement process is the ―brain‖ of the patient-centered medical home that scans the
environment for innovations and learns new knowledge about its own processes through
measurement of performance in practice and determining the effect on the practice of
making rapid-cycle tests of change.
Figure 10
Leadership/Citizenship – Quality Innovation
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Recovery,
Rehab, Pt
Self-Care
Recovery,
Rehab, Pt
Self-Care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Screening &
Diagnostic
Work-up
Screening &
Diagnostic
Work-up
Treatment
Intervention
Treatment
Intervention
Monitor &
Follow-up
Monitor &
Follow-up
Tests – Consults – Referrals - Admits - Rx
Access & Arranging CareAccess & Arranging Care
Patient Education - Self-Care SupportPatient Education - Self-Care Support
Teamwork – Proactive Care ManagementTeamwork – Proactive Care Management
Clinical Information ManagementClinical Information Management
Leadership/citizenship - Quality InnovationLeadership/citizenship - Quality Innovation
This process is labeled ―Leadership & citizenship in Quality Innovation‖ because it
involves leadership in setting the tone and aims for agenda of quality in the practice; it

70
also involves citizenship of every staff and clinician member of the medical home in
doing their part to value and embrace continuous improvement of the quality of care
provided in the practice. Such citizenship requires both knowledge and instrumental skills
in using measurement data, testing change ideas in rapid-cycle tests of change, and
selecting those proved to be improvements for implementation across the medical home.
The name Quality Innovation was inspired by the concept of permanent innovation.21
This concept of innovation includes not only improvement, but also life-long learning,
creativity, and remaining economic viable to one’s clients or customers. What is most
important here is that both leadership and citizenship in quality innovation are essential
elements of a clinical microsystem. The value-added element s of the
Leadership/citizenship in Quality Innovation process includes:
Identified Clinical Quality and Resource Management Roles – High quality medical
practices identify persons with specific roles and responsibilities for the clinical quality
and resource management of the practice. Although everyone one the team has specified
roles and responsibilities for teamwork, one person is identified with the role and
responsibility for the overall performance of the team. This person helps the team set the
aims for quality and safety, motivates the team, counsels and support team activity and
facilities the resolution of conflicts within the team. Likewise the well functioning team
has an identified person with the role and responsibility for assuring that the resources
needed by the team, including the personnel, are available for the team to do its work.
The resource leader also has responsibility for assuring the financial viability of the
practice.
Quality Aim & Objectives for a Culture of Safety – The aim of the patient-centered
medical home is to improve the quality of care as defined by the Institute of Medicine’s
construct for a quality system: patient-centeredness, efficiency, effectiveness, equity,
timeliness and safety.22
One of the leadership responsibilities is to set the theme for
improvement in the medical home. The specific aim that the practice is tackling will
change from time to time. As one aim is achieved and maintained another is tackled.
This continuous cycle of improvement energizes the practice and joy to the clinicians and
staff. Another task of the leader is to build a culture of safety in which mistakes and
errors are seen as opportunities to explore the root cause and to build a fail-safe system.
Such a culture looks for system failures rather than blaming the last person who touched
a process before it failed.
Quality Measure Dashboard & Control Charts – The quality improvement process
relies on measures of the microsystem’s performance. These measure can be the
reliability of the care processes (e.g. the percentage of hyperlimidemic patients who have
had an LDL cholesterol measured within the past year). Or they may be outcome
measures (e.g. the percentage of patients with diabetes who have an A1c less than 7.0%).
21
Morris L. Permanent Innovation: The Definitive Guide to the Principles, Strategies and Methods of
Successful Innovators. 2006. http://www.permanentinnovation.com/downloads.html accesses July 5, 2008. 22
Institute of Medicine: Crossing the Quality Chasm. 2002 National Academy of Sciences Press,
Washington, DC.
71
Measures of practice timeliness (e.g. availability of the third next new patient visit) or
patient-centeredness (e.g. time to return patient phone calls) are also necessary. Once the
practice has determined the spectrum of measures it will track, these should be displayed
in a prominent place in the practice as a dashboard of microsystem performance. This
dashboard stimulates everyone to take the actions within their license to improve
performance.
Rapid-cycle Tests of Change Improvement & Innovation teams – Change won’t
happen only through the good intentions of the staff, practice processes will need to be
engineered and re-engineered to accomplish the aims of the practice. Novice health
professional students will learn how to apply the quality Improvement methods of rapid-
cycle tests of change in learning how to improve the system of care. This disciplined
approach makes certain that good ideas are tested in small steps and shown to be
improvements. The opposite approach of imposing a good idea without testing more
often than not disrupts other aspects of the system or doesn’t work as intended. Making
changes without testing them first threatens safety, creates chaos and staff stress and
dissatisfaction.
Spread of Innovation – Once the team has demonstrated that the rapid-cycle test of
change has resulted in an improvement, the team sets out to engage all of the other
members of the practice in learning how to adopt the process change into their practice.
This spread of the innovation is not simple. It takes time, education to help other
understand the basis for the change and how to adopt the habits and skills needed to
implement it. Change is difficult and teams often underestimate the resistance and even
sabotage that will occur when spreading innovations. Here is the role for leadership and
citizenship in helping everyone strive for the common aim of improved health care.
Financial Plan for Practice Viability – Although this is the last element described, it is
essential to staying in practice. Each microsystem must have a business or administrative
manager who looks after the financial and organizational health of the practice. Keeping
up with insurance and government regulations, accurately filing charges, tracking
supplies and getting the best price from vendors, and maintaining effective personnel
policies are all essential to maintaining the financial health and viability of the practice.
These are important aspects of the leadership role. The quality measure of efficiency
involves providing the highest quality of care while using the fewest resources to do so.
Measures of efficiency require the merging of quality and financial data.
72
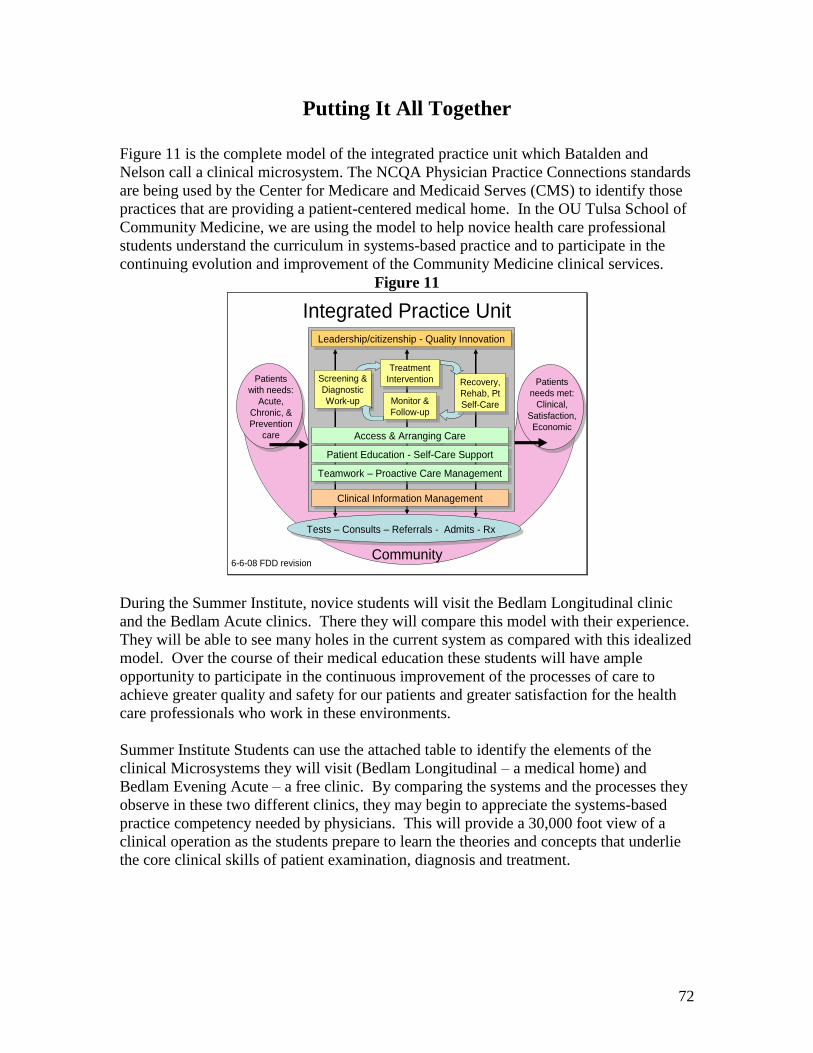
Putting It All Together
Figure 11 is the complete model of the integrated practice unit which Batalden and
Nelson call a clinical microsystem. The NCQA Physician Practice Connections standards
are being used by the Center for Medicare and Medicaid Serves (CMS) to identify those
practices that are providing a patient-centered medical home. In the OU Tulsa School of
Community Medicine, we are using the model to help novice health care professional
students understand the curriculum in systems-based practice and to participate in the
continuing evolution and improvement of the Community Medicine clinical services.
Figure 11
Integrated Practice Unit
Patients
with needs:
Acute,
Chronic, &
Prevention
care
Recovery,
Rehab, Pt
Self-Care
Recovery,
Rehab, Pt
Self-Care
Patients
needs met:
Clinical,
Satisfaction,
Economic
Community
Screening &
Diagnostic
Work-up
Screening &
Diagnostic
Work-up
Treatment
Intervention
Treatment
Intervention
Monitor &
Follow-up
Monitor &
Follow-up
Tests – Consults – Referrals - Admits - Rx
Access & Arranging CareAccess & Arranging Care
Patient Education - Self-Care SupportPatient Education - Self-Care Support
Teamwork – Proactive Care ManagementTeamwork – Proactive Care Management
Clinical Information ManagementClinical Information Management
Leadership/citizenship - Quality InnovationLeadership/citizenship - Quality Innovation
6-6-08 FDD revision
During the Summer Institute, novice students will visit the Bedlam Longitudinal clinic
and the Bedlam Acute clinics. There they will compare this model with their experience.
They will be able to see many holes in the current system as compared with this idealized
model. Over the course of their medical education these students will have ample
opportunity to participate in the continuous improvement of the processes of care to
achieve greater quality and safety for our patients and greater satisfaction for the health
care professionals who work in these environments.
Summer Institute Students can use the attached table to identify the elements of the
clinical Microsystems they will visit (Bedlam Longitudinal – a medical home) and
Bedlam Evening Acute – a free clinic. By comparing the systems and the processes they
observe in these two different clinics, they may begin to appreciate the systems-based
practice competency needed by physicians. This will provide a 30,000 foot view of a
clinical operation as the students prepare to learn the theories and concepts that underlie
the core clinical skills of patient examination, diagnosis and treatment.
73
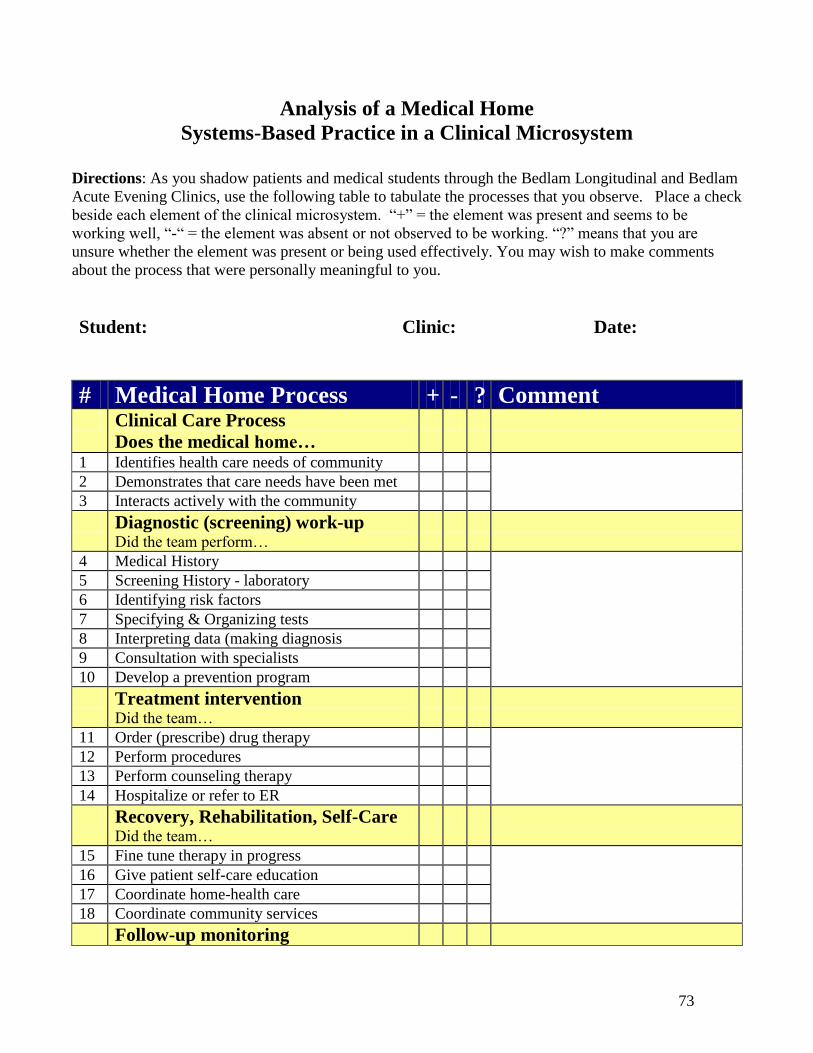
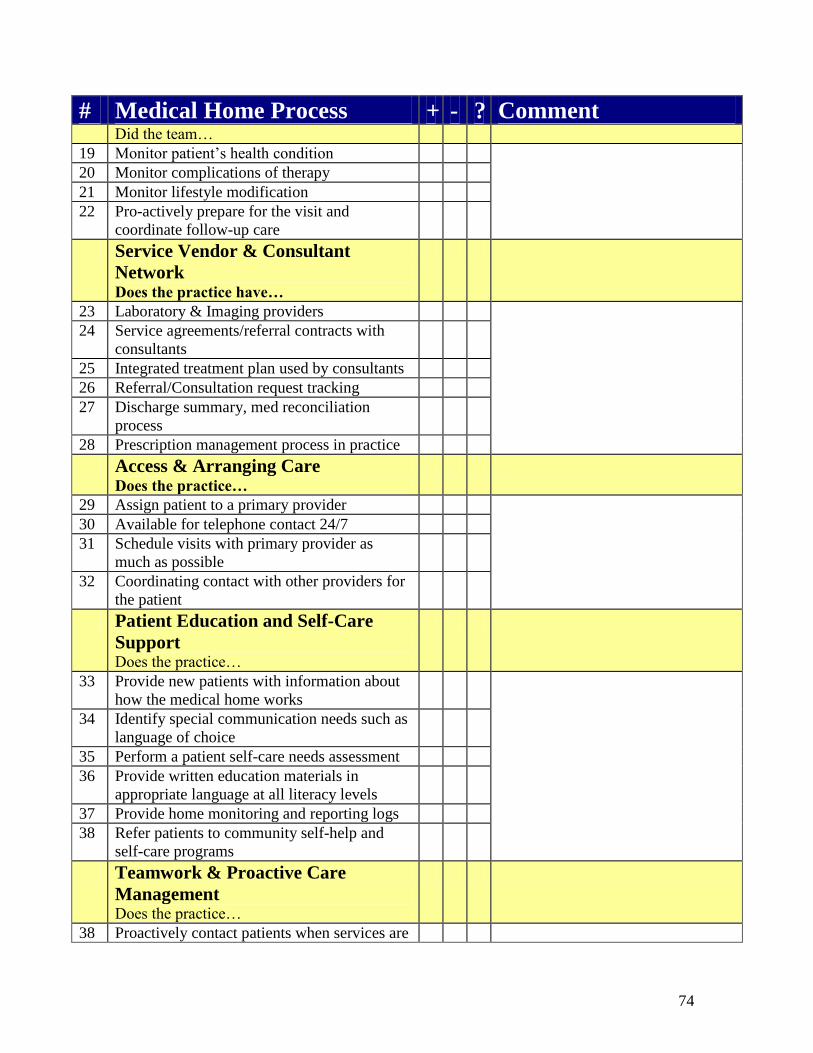
Analysis of a Medical Home
Systems-Based Practice in a Clinical Microsystem
Directions: As you shadow patients and medical students through the Bedlam Longitudinal and Bedlam
Acute Evening Clinics, use the following table to tabulate the processes that you observe. Place a check
beside each element of the clinical microsystem. ―+‖ = the element was present and seems to be
working well, ―-― = the element was absent or not observed to be working. ―?‖ means that you are
unsure whether the element was present or being used effectively. You may wish to make comments
about the process that were personally meaningful to you.
Student: Clinic: Date:
# Medical Home Process + - ? Comment Clinical Care Process
Does the medical home…
1 Identifies health care needs of community
2 Demonstrates that care needs have been met
3 Interacts actively with the community
Diagnostic (screening) work-up Did the team perform…
4 Medical History
5 Screening History - laboratory
6 Identifying risk factors
7 Specifying & Organizing tests
8 Interpreting data (making diagnosis
9 Consultation with specialists
10 Develop a prevention program
Treatment intervention Did the team…
11 Order (prescribe) drug therapy
12 Perform procedures
13 Perform counseling therapy
14 Hospitalize or refer to ER
Recovery, Rehabilitation, Self-Care Did the team…
15 Fine tune therapy in progress
16 Give patient self-care education
17 Coordinate home-health care
18 Coordinate community services
Follow-up monitoring
74
# Medical Home Process + - ? Comment Did the team…
19 Monitor patient’s health condition
20 Monitor complications of therapy
21 Monitor lifestyle modification
22 Pro-actively prepare for the visit and
coordinate follow-up care
Service Vendor & Consultant
Network Does the practice have…
23 Laboratory & Imaging providers
24 Service agreements/referral contracts with
consultants
25 Integrated treatment plan used by consultants
26 Referral/Consultation request tracking
27 Discharge summary, med reconciliation
process
28 Prescription management process in practice
Access & Arranging Care Does the practice…
29 Assign patient to a primary provider
30 Available for telephone contact 24/7
31 Schedule visits with primary provider as
much as possible
32 Coordinating contact with other providers for
the patient
Patient Education and Self-Care
Support Does the practice…
33 Provide new patients with information about
how the medical home works
34 Identify special communication needs such as
language of choice
35 Perform a patient self-care needs assessment
36 Provide written education materials in
appropriate language at all literacy levels
37 Provide home monitoring and reporting logs
38 Refer patients to community self-help and
self-care programs
Teamwork & Proactive Care
Management Does the practice…
38 Proactively contact patients when services are
Copyright © 2008. F. DANIEL DUFFY, M.D., THE UNIVERSITY OF OKLAHOMA-TULSA. All rights reserved. 75
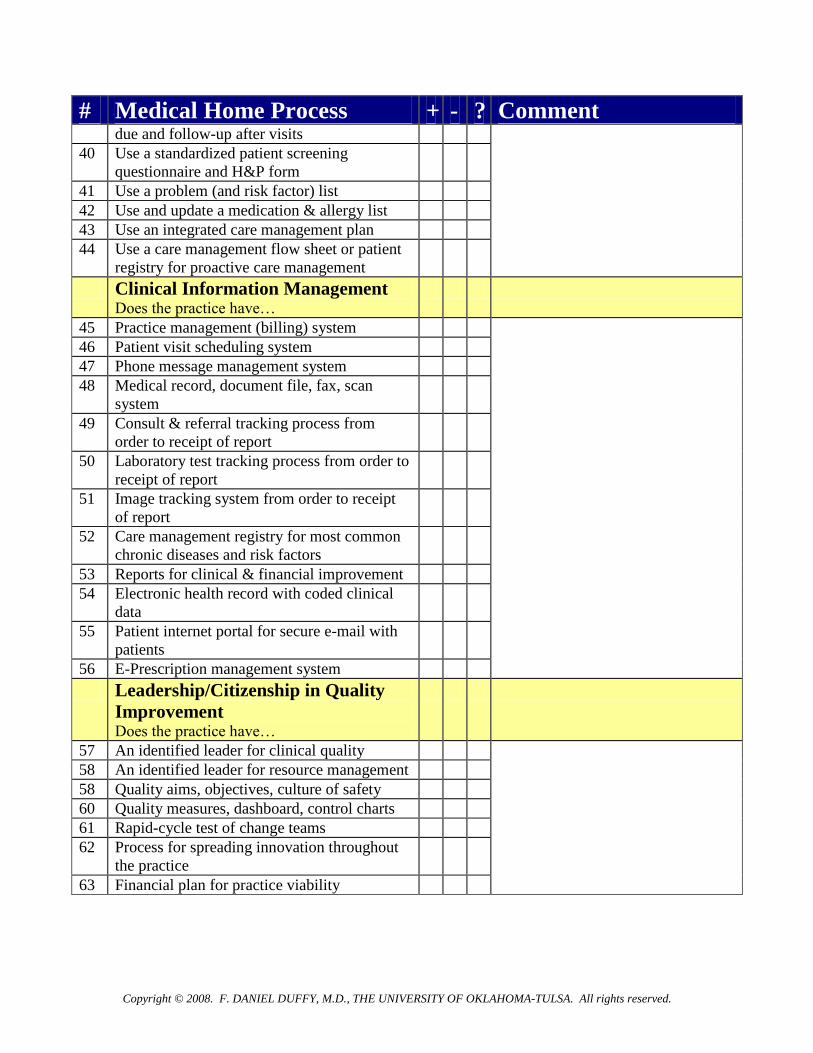
# Medical Home Process + - ? Comment due and follow-up after visits
40 Use a standardized patient screening
questionnaire and H&P form
41 Use a problem (and risk factor) list
42 Use and update a medication & allergy list
43 Use an integrated care management plan
44 Use a care management flow sheet or patient
registry for proactive care management
Clinical Information Management Does the practice have…
45 Practice management (billing) system
46 Patient visit scheduling system
47 Phone message management system
48 Medical record, document file, fax, scan
system
49 Consult & referral tracking process from
order to receipt of report
50 Laboratory test tracking process from order to
receipt of report
51 Image tracking system from order to receipt
of report
52 Care management registry for most common
chronic diseases and risk factors
53 Reports for clinical & financial improvement
54 Electronic health record with coded clinical
data
55 Patient internet portal for secure e-mail with
patients
56 E-Prescription management system
Leadership/Citizenship in Quality
Improvement Does the practice have…
57 An identified leader for clinical quality
58 An identified leader for resource management
58 Quality aims, objectives, culture of safety
60 Quality measures, dashboard, control charts
61 Rapid-cycle test of change teams
62 Process for spreading innovation throughout
the practice
63 Financial plan for practice viability


















