SEVERE POSTPARTUM HEMORRHAGE: Etiology, management …
119
Department of Obstetrics and Gynecology Helsinki University Hospital and University of Helsinki Finland Doctoral Program in Clinical Research SEVERE POSTPARTUM HEMORRHAGE: Etiology, management and long-term outcome with special emphasis on novel methods of management Maiju Grönvall DOCTORAL DISSERTATION To be presented for public discussion with the permission of the Faculty of Medicine of the University of Helsinki, in the Lecture Room 2, Haartman Institute, Haartmaninkatu 3, Helsinki, on the 3rd of April 2020, at 12 noon.
Transcript of SEVERE POSTPARTUM HEMORRHAGE: Etiology, management …

Department of Obstetrics and Gynecology
Helsinki University Hospital and University of Helsinki
Finland
Doctoral Program in Clinical Research
SEVERE POSTPARTUM HEMORRHAGE: Etiology, management and long-term outcome with special emphasis on novel methods of management
Maiju Grönvall
DOCTORAL DISSERTATION To be presented for public discussion with the permission of the Faculty of Medicine of the
University of Helsinki, in the Lecture Room 2, Haartman Institute, Haartmaninkatu 3, Helsinki, on the 3rd of April 2020, at 12 noon.

Supervised by: Adjunct Professor Vedran Stefanovic, M.D., Ph.D. Department of Obstetrics and Gynecology Helsinki University Hospital and University of Helsinki, Helsinki, Finland Adjunct Professor Minna Tikkanen, M.D., Ph.D. Department of Obstetrics and Gynecology Helsinki University Hospital and University of Helsinki, Helsinki, Finland
Reviewed by: Professor Per Olofsson, M.D., Ph.D., B.Sc. Institution of Clinical Sciences Lund University, Malmö, Sweden Adjunct Professor Anne Kuitunen, M.D., Ph.D. Department of Intensive Care Tampere University Hospital and University of Tampere, Tampere, Finland
Official Opponent: Adjunct Professor Jyrki Jalkanen, M.D., Ph.D. Department of Obstetrics and Gynecology Central Finland Central Hospital, Jyväskylä, Finland University of Tampere, Tampere, Finland
Drawings and cover design Katja Saastamoinen The Faculty of Medicine uses the Urkund system (plagiarism recognition) to examine all doctoral dissertations ISBN 978-951-51-5884-0 (paperback) ISBN 978-951-51-5885-7 (PDF) Unigrafia Helsinki 2020

To Aaro, Perttu, Urho and Ilmari

TABLE OF CONTENTS
ABSTRACT ............................................................................................................................................ 7
LIST OF ORIGINAL PUBLICATIONS ....................................................................................................... 9
ABBREVIATIONS ................................................................................................................................ 10
1 INTRODUCTION ........................................................................................................................... 11
2 REVIEW OF THE LITERATURE ...................................................................................................... 13
2.1 POSTPARTUM HEMORRHAGE ................................................................................................... 13 2.1.1 Definitions .......................................................................................................................... 13 2.1.2 Incidence ............................................................................................................................ 14 2.1.3 Etiology ............................................................................................................................... 14
Uterine atony ........................................................................................................................... 15 Placental retention ................................................................................................................... 15 Placenta previa ......................................................................................................................... 16 Abnormally invasive placenta .................................................................................................. 18 Genital tract trauma ................................................................................................................. 20 Coagulation disorders .............................................................................................................. 20
2.1.4 Risk factors ......................................................................................................................... 21 2.1.5 Prevention .......................................................................................................................... 24 2.1.6 Screening for placenta previa and antenatal diagnosis of abnormally invasive placenta . 25 2.1.7 Management ...................................................................................................................... 27
General principles .................................................................................................................... 27 Conservative management ...................................................................................................... 29 Tamponade .............................................................................................................................. 30 Pelvic arterial embolization ..................................................................................................... 30 Surgical management .............................................................................................................. 31
Uterine compression sutures .................................................................................................... 31 Artery ligation.................................................................................................................... 32 Hysterectomy .................................................................................................................... 32
Management of placenta previa .............................................................................................. 33 Management of abnormally invasive placenta ....................................................................... 34
2.1.8 Consequences..................................................................................................................... 36 Physical outcomes .................................................................................................................... 36 Psychological outcomes ........................................................................................................... 36
2.2 BAKRI BALLOON TAMPONADE .................................................................................................. 40 2.2.1 Device ................................................................................................................................. 40 2.2.2 Placement ........................................................................................................................... 40 2.2.3 Obstetric indications .......................................................................................................... 42 2.2.4 Contraindications ............................................................................................................... 43 2.2.5 Combination with other treatment methods .................................................................... 44

2.2.6 Success rate ........................................................................................................................ 45 2.2.7 Factors related to failure .................................................................................................... 46 2.2.8 Complications ..................................................................................................................... 46 2.2.9 Long-term outcomes .......................................................................................................... 47
2.3 INTERVENTIONAL RADIOLOGY PROCEDURES ........................................................................... 48 2.3.1 Obstetric indications .......................................................................................................... 48 2.3.2 Method ............................................................................................................................... 49
Acute postpartum hemorrhage ............................................................................................... 50 Anticipated postpartum hemorrhage due to abnormally invasive placenta .......................... 51
2.3.3 Embolization materials ....................................................................................................... 52 2.3.4 Success rate and factors related to failure ......................................................................... 52
Pelvic arterial embolization ..................................................................................................... 52 Temporary prophylactic balloon occlusion .............................................................................. 53
2.3.5 Short-term complications................................................................................................... 54 2.3.6 Long-term outcomes .......................................................................................................... 55
Fertility and menstruation ....................................................................................................... 55 Pregnancies .............................................................................................................................. 55 Psychological outcomes ........................................................................................................... 56
3 AIMS OF THE STUDY ....................................................................................................................... 57
4 MATERIALS AND METHODS ........................................................................................................... 58
4.1 STUDY I ...................................................................................................................................... 58 4.2 STUDY II ..................................................................................................................................... 59 4.3 STUDY III .................................................................................................................................... 59 4.4 STUDY IV .................................................................................................................................... 60 4.5 STATISTICAL ANALYSES ............................................................................................................. 61
5 RESULTS .......................................................................................................................................... 62
5.1 BASELINE CHARACTERISTICS OF THE STUDY POPULATION (STUDIES I- ̶ IV) ............................... 62 5.2 INDICATIONS, EFFECTIVENESS AND SAFETY OF BAKRI BALLOON TAMPONADE (I) ................... 63
5.2.1 Indications (I) ...................................................................................................................... 63 5.2.2 Hemorrhage (I) ................................................................................................................... 63 5.2.3 Technical aspects (I) ........................................................................................................... 64 5.2.4 Success rate and safety (I) .................................................................................................. 64
5.3 EFFECTIVENESS AND SAFETY OF PELVIC ARTERIAL EMBOLIZATION IN THE TREATMENT OF
EMERGENCY POSTPARTUM HEMORRHAGE (II) .............................................................................. 66 5.3.1 Indications (II) ..................................................................................................................... 66 5.3.2 Success rate and safety (II) ................................................................................................. 66
5.4 PSYCHOLOGICAL AND PHYSICAL OUTCOMES OF WOMEN MANAGED WITH INTERVENTIONAL
RADIOLOGY PROCEDURES (III) ........................................................................................................ 68 5.4.1 Psychological outcomes (III) ............................................................................................... 68

5.4.2 Physical outcomes (III) ........................................................................................................ 69 5.5 COMPARISON OF OBSTETRIC OUTCOMES BETWEEN WOMEN WITH MAJOR OR MINOR
PLACENTA PREVIA (IV) .................................................................................................................... 71 5.6 ACCURACY OF THE SCREENING AND FOLLOW-UP IN WOMEN WITH PLACENTA PREVIA (IV) ... 73 5.7 CHARACTERISTICS OF WOMEN WITH ABNORMALLY INVASIVE PLACENTA (I- ̶ IV) ..................... 74
6 DISCUSSION .................................................................................................................................... 75
6.1 IMPORTANCE OF THE STUDY (I ̶ IV) ............................................................................................ 75 6.2 INDICATIONS, EFFECTIVENESS AND SAFETY OF BAKRI BALLOON TAMPONADE (I) ................... 76 6.3 EFFECTIVENESS AND SAFETY OF PELVIC ARTERIAL EMBOLIZATION IN THE TREATMENT OF
EMERGENCY POSTPARTUM HEMORRHAGE (II) .............................................................................. 78 6.4 PSYCHOLOGICAL AND PHYSICAL LONG-TERM OUTCOMES OF WOMEN MANAGED WITH
INTERVENTIONAL RADIOLOGY PROCEDURES (III) ........................................................................... 80 6.5 COMPARISON OF WOMEN WITH MAJOR AND MINOR PLACENTA PREVIA (IV) ........................ 82 6.6 ACCURACY OF THE SCREENING AND FOLLOW-UP IN WOMEN WITH PLACENTA PREVIA (IV) ... 83 6.7 LIMITATIONS (I- ̶IV) .................................................................................................................... 84 6.8 CLINICAL IMPLICATIONS ............................................................................................................ 85 6.9 FUTURE ASPECTS ....................................................................................................................... 86
7 CONCLUSIONS ................................................................................................................................. 87
8 ACKNOWLEDGMENTS .................................................................................................................... 88
9 REFERENCES .................................................................................................................................... 90
APPENDIX I: QUESTIONNAIRE FOR WOMEN WITH HYSTERECTOMY ............................................ 112
APPENDIX II: QUESTIONNAIRE FOR WOMEN WITHOUT HYSTERECTOMY ................................... 115
APPENDIX III: THE ORIGINAL PUBLICATIONS ................................................................................. 120

7
ABSTRACT
Postpartum hemorrhage (PPH) complicates approximately 4% of all deliveries worldwide. It causes maternal morbidity and mortality even in high-income countries. The etiology of PPH includes uterine atony, genital tract lacerations, retention of placental tissue and coagulopathies. In recent years, abnormally invasive placenta (AIP) has emerged as an increasing cause of PPH. Women with a history of cesarean section (CS) and presenting with placenta previa (PP) are at high risk for AIP. Antenatal detection of PP and AIP diminishes the risk of massive PPH and other complications. It is inconclusive whether PP type (major or minor) makes a significant difference in obstetric outcomes. Although there are several known risk factors, PPH still occurs often in primiparous women without any detectable risk factors.
The treatment of PPH depends on the etiology and hospital facilities. First-line treatment includes volume replacement, the use of uterotonics and tranexamic acid, laceration repair and removal of placental tissue. If bleeding continues, the following treatment options have traditionally been surgical procedures: ligation of the uterine arteries, uterine compression sutures and hysterectomy. These procedures require advanced surgical skills. Avoiding hysterectomy, and thus infertility, is also one main goal, especially among primiparous women.
Readily available, simple, fertility-sparing treatment modalities are needed. Over the last two decades, the Bakri balloon (Cook® Medical Incorporated, Bloomington, IN, USA) tamponade (BBT) and interventional radiology procedures (IRP) have been used increasingly in the treatment of PPH. The Bakri balloon (BB) is exclusively designed for obstetric use. It can be inserted into the uterus or the vagina depending on the bleeding site. IRPs include pelvic arterial embolization (PAE) and the use of prophylactic balloon occlusion (PBO) in the pelvic arteries. IRPs can be used both in acute massive PPH and also prophylactically in women who are at high risk for PPH due to anticipated AIP.
The aims of the studies were to determine the effectiveness and safety of BBT and PAE. The long-term psychological and physical sequelae of IRPs were also studied. The accuracy of our screening and treatment protocol for PP was evaluated, and obstetric outcomes between major and minor PP were compared. The study data were collected retrospectively from Helsinki University Hospital (HUH) registers (years 2001 ̶ 2014). A structured questionnaire concerning long-term psychological and physical outcomes was sent to women who underwent IRP.
The results confirmed that both BBT and PAE are safe and effective procedures in the treatment of acute massive PPH, regardless of etiology. The success rate for BBT was 86% and for PAE 89%. None of the complications was related to BBT. Only one major PAE-related complication occurred (rupture of the iliac artery).
The results of the inquiry showed a high incidence of adverse psychological outcomes among women with complicated deliveries. The psychological problems did not depend on the volume of

8
bleeding, whether hysterectomy was performed or whether the nature of the IRP was elective or emergency. Many women consider counseling to be inadequate after a stressful delivery.
Due to our mid-pregnancy screening protocol, almost one-fifth of the women with major or minor PP at term had no follow-up after mid-pregnancy. The first bleeding episode occurred at 37 gestational weeks or later in 21.9% of these women. Additionally, two women without follow-up had AIP with a history of prior CS, and both underwent hysterectomy. These complications could possibly have been avoided if the diagnosis had been established earlier.
The incidence of AIP was equal in women with major and minor PP, and both types of PP showed that women were exposed to major complications. It was also remarkable that two out of seven women with BBT failure and three out of five with PAE failure had AIP as a cause of PPH.
In conclusion, BBT and PAE are safe and effective treatment modalities. The procedures had a significant role in the PPH treatment protocol. The availability of these procedures is mandatory due to the unpredictable nature of PPH and the increasing incidence of AIP. Our screening and follow-up protocols for PP are revised based on our results. A systematic counseling protocol for women who had PPH and a complicated delivery should be implemented in every delivery unit.

9
LIST OF ORIGINAL PUBLICATIONS
This thesis is based on the following publications, which are referred to in the text by their Roman numerals:
I Grönvall M, Tikkanen M, Tallberg E, Paavonen J, Stefanovic V. Use of Bakri balloon tamponade in the treatment of postpartum hemorrhage: A series of 50 cases from a tertiary teaching hospital. Acta Obstet Gynecol Scand. 2013;92:433 ̶ 8
II Grönvall M, Tikkanen M, Metsätähti M, Loukovaara M, Paavonen J, Stefanovic V. Pelvic arterial embolization in severe obstetric hemorrhage. Acta Obstet Gynecol Scand. 2014;93:716 ̶ 9
III Grönvall M, Tikkanen M, Paavonen J, Loukovaara M, Stefanovic V. Is there an association between postpartum hemorrhage, interventional radiology procedures and psychological sequelae? J Matern Fetal Neonatal Med. 2019;7:1 ̶5
IV Grönvall M, Stefanovic V, Paavonen J, Loukovaara M, Tikkanen M. Major or minor placenta previa: Does it make a difference? Placenta. 2019;85:9 ̶ 14
The original publications are reproduced with the permission of the copyright holders.

10
ABBREVIATIONS
ACOG The American College of Obstetricians and Gynecologists AIP Abnormally invasive placenta ART Artificial reproductive technology BB Bakri balloon BBT Bakri balloon tamponade BMI Body mass index CI Confidence interval CS Cesarean section DIC Disseminated intravascular coagulation HELLP Hemolysis, elevated liver enzyme levels and low platelet syndrome HUH Helsinki University Hospital ICD-10 10th revision of the International Statistical Classification of Diseases
and Related Health Problems IRP Interventional radiology procedures IS-AIP International Society for Abnormally Invasive Placenta NICE National Institute for Health and Care Excellence OR Odds ratio PAE Pelvic arterial embolization PBO Prophylactic balloon occlusion PP Placenta previa PPH Postpartum hemorrhage PTSD Post-traumatic stress disorder RCOG Royal College of Obstetricians and Gynecologists RR Relative risk SGA Small for gestational age THL Terveyden ja hyvinvoinnin laitos, Finnish National Institute for Health
and Welfare WHO World Health Organization

11
1 INTRODUCTION
Postpartum hemorrhage (PPH) causes maternal morbidity and even mortality worldwide (Waterstone et al. 2001, Say et al. 2014). Several risk factors for PPH are known, but PPH still occurs often in primiparous women with no detectable risk factors, which makes it difficult to prepare for bleeding (Wetta et al. 2013). The other major concern is the increasing incidence of placenta previa (PP) and abnormally invasive placenta (AIP) due to increasing maternal age, use of infertility treatments and especially increasing cesarean section (CS) rates (Jauniaux et al. 2018a). AIP is associated with massive PPH, resulting in major complications, infertility and even maternal death (Silver et al. 2015).
The primary treatment for PPH includes volume replacement, the use of uterotonics and tranexamic acid, laceration repair and removal of placental tissue. If bleeding continues, the following treatment options have traditionally been surgical procedures: ligation of the uterine arteries, uterine compression sutures and hysterectomy, which also means the loss of fertility. These procedures require advanced surgical skills (Ahonen et al. 2010).
Readily available, effective and uterus-preserving treatment modalities are needed. The Bakri balloon (Cook® Medical Incorporated, Bloomington, IN, USA) tamponade (BBT) and interventional radiology procedures (IRP) seem to fill these criteria. The Bakri balloon (BB) is exclusively designed for obstetric use (Bakri et al. 1992). IRPs include pelvic arterial embolization (PAE) in cases of emergency PPH and prophylactic balloon occlusion (PBO) of the pelvic arteries in cases of antenatally anticipated AIP. These methods have been used increasingly in the past two decades.
Antenatal diagnosis of AIP and scheduled delivery with a multidisciplinary team seem to diminish the amount of bleeding and complications (Tikkanen et al. 2011, Fitzpatrick et al. 2014, Silver et al. 2015, Jauniaux et al. 2017). The main risk factor for AIP is PP with previous CS (Fitzpatrick et al. 2014, Thurn et al. 2016). When screening for fetal structural anomalies in mid-pregnancy, the placental position is also determined. The resolution rate of minor PP is described to be as high as 90% before term, although it is more unlikely in women with prior CS (Heller et al. 2014, Lal et al. 2015). In our department, the follow-up after mid-pregnancy has been arranged only for women with PP overlapping the cervical os ≥15 mm, thus most of the PPs (especially minor PPs) have had no follow-up after mid-pregnancy. Our screening protocol is based on Taipale et al. (1998). On the contrary, recent literature has recommended a follow-up for women with minor PP (Copland et al. 2012, Kapoor et al. 2014).
There were only a few publications on BBT before our study commenced (2012). In our hospital, PAE had been used for 10 years without evaluating the effectiveness and safety of our own process. The psychological and physical outcomes of complicated deliveries and IRPs were also controversial and unclear.

12
The main goal was to determine the effectiveness and safety of BBT and PAE. Also, the effects on long-term psychological and physical outcomes were determined. Another goal was to critically evaluate the screening protocol for PP and the accuracy of follow-up. The outcomes between women with major and minor PP were compared to determine whether these conditions should be followed with the same intensity.

13
2 REVIEW OF THE LITERATURE
2.1 POSTPARTUM HEMORRHAGE
2.1.1 Definitions
Although it is a common obstetrical entity, the uniform definition of postpartum hemorrhage (PPH) is lacking. PPH is classically defined as a blood loss of more than 500 ml after vaginal delivery and more than 1000 ml after cesarean section (CS) (Dahlke et al. 2015, Mavrides et al. 2016). The American College of Obstetricians and Gynecologists (ACOG) has defined PPH as a cumulative blood loss of 1000 ml or more or blood loss with signs of hypovolemia (tachycardia, hypotension, etc.) regardless of the delivery route (Menard et al. 2014). An alternative proposed marker to define PPH is a 10% decrease in hematocrit (Combs et al. 1991a). However, determinations of hemoglobin or hematocrit concentrations are often delayed and do not reliably reflect the present hematologic status (Combs et al. 1991a).
PPH can also be determined by its severity. Severe PPH is determined as a blood loss of more than 1500 ml, a decline in hemoglobin of 4 g/l or more, acute transfusion of red blood cells of at least four units or a need for additional hemostatic intervention (Waterstone et al. 2001). The Royal College of Obstetricians and Gynecologists (RCOG) had used the terms minor (500 ̶1000 ml) and major (>1000 ml) to describe the severity of PPH. Major PPH can be further divided into moderate (1001 ̶2000 ml) and severe (>2000 ml) subgroups (Mavrides et al. 2016). Blood loss of more than 2500 ml is always a life-threatening obstetric emergency (Mavrides et al. 2016).
Depending on its timing, PPH is also classified as primary or secondary, which is useful when considering the etiologies of PPH. Primary PPH occurs within the first 24 hours of delivery, while secondary PPH means excessive bleeding between 24 hours and 12 weeks postpartum (Alexander et al. 2002, Mavrides et al. 2016).
However, estimating the amount of blood loss is often difficult, especially after vaginal birth. Many studies have reported that visual estimates are often inaccurate. Blood loss is overestimated in low volumes and underestimated in larger volumes. The magnitude of the underestimation typically increases as the volume of hemorrhage increases (Bose et al. 2006, Stafford et al. 2008, Zhang et al. 2010).

14
2.1.2 Incidence
The incidence of PPH varies widely depending on the definition used and the region of the world. A reasonable estimate of PPH in the United States and Europe is 1 ̶ 6% of all deliveries (Carroli et al. 2008, Bateman et al. 2010, Callaghan et al. 2010, Vendittelli et al. 2016, van Stralen et al. 2016, Merriam et al. 2018). PPH seems to have increased in high-income countries in recent years. In the United States, the rate of PPH was 2.3% in 1994 and 2.9% in 2006, which suggests an increase of 26%. The primary reason for this change was the increased rate of uterine atony (Callaghan et al. 2010). More recently, a large Dutch study reported that the incidence of PPH increased from 4.1% to 6.4% between 2000 and 2013 (van Stralen et al. 2016). In Finland, between 2006 and 2016, the incidence of deliveries requiring transfusions has varied between 1.8% and 2.5% (THL statistics, personal communication, Eija Vuori).
2.1.3 Etiology
PPH is usually caused by one or more of the following conditions: uterine atony, retention of placental tissue, lacerations of the genital tract or coagulopathies (Ahonen et al. 2010, Vendittelli et al. 2016, Nyflot et al. 2017). The causes can also be represented as the “Four Ts”: Tone for uterine atony, Tissue for retained products of conception, Trauma for lacerations and Thrombin for coagulopathies (Sebghati et al. 2017). In recent years, placenta previa (PP) and abnormally invasive placenta (AIP) have also been seen more often in cases of PPH (Silver 2015, Silver et al. 2015, Society of Gynecologic Oncology 2018).
Figure 1. Etiology of PPH.
70 %
10 %
18 %
2 %Atony
Placental retention
Genital tract trauma
Coagulationabnormality
(Vendittelli et al. 2016, Nyflot et al. 2017, Sebghati et al. 2017)

15
Uterine atony
Uterine atony is the leading cause of PPH (Vendittelli et al. 2016, Nyflot et al. 2017), with an incidence of approximately 3.6% of deliveries (Driessen et al. 2011). Atony occurs when the myometrium fails to contract after delivery of the placenta. This is often the result of an over-distended uterus. An atonic uterus cannot achieve necessary vasoconstriction in the placental implantation site, which rapidly leads to massive PPH because the uterine blood flow is approximately 600 ml per minute (Gibbs et al. 2008). Sometimes, despite the well-contracted uterine fundus, bleeding may continue from the lower uterine segment. This is common especially in cases of PP (Gibbs et al. 2008, Committee on Practice Bulletins-Obstetrics 2018).
Placental retention
The term “retained placenta” is used when the placenta is not totally or partially separated from the uterine wall 30 ̶60 minutes after vaginal delivery of the infant. Placental retention occurs in approximately 1 ̶ 4% of deliveries (Weeks 2008, Endler et al. 2014, Coviello et al. 2015, Greenbaum et al. 2017).
There are three main types of placental retention (Combs et al. 1991b, Weeks 2008, Coviello et al. 2015, Greenbaum et al. 2017):
1. Placenta is trapped behind the closed cervix 2. Placenta adheres to the uterine wall due to failed uterine contraction 3. Placenta abnormally invades the uterine wall The spontaneous median duration of placental separation is reported to be 5 ̶ 7 minutes, and only 3 ̶ 8% of women have it longer than 30 minutes (Combs et al. 1991b). The risk of hemorrhage is shown to increase significantly after 30 minutes of waiting (Combs et al. 1991b, Magann et al. 2005). The timing of placental retention diagnosis differs in different countries. In many Northern European countries, including Finland, the cut-off for diagnosis is 60 minutes. More than 80% of Finnish maternity units reported a protocol of waiting 60 minutes or more before proceeding to manually remove the placenta (Deneux-Tharaux et al. 2009).

16
Placenta previa
PP complicates approximately 0.5% of all pregnancies (Ananth et al. 2003, Rosenberg et al. 2011, Lal et al. 2015, Silver 2015). In recent years, there has been an increase in the incidence of PP, which is associated with advanced maternal age, use of artificial reproductive technologies (ART), smoking during pregnancy and, especially, increasing CS rates (Silver 2015).
The definition of PP is historically based on digital examination of the cervix and the placental edge during delivery (Barris 1926). Later, placental location was determined by transabdominal ultrasound (Jauniaux et al. 1990). Using these methods, PP was defined as complete or total if the placenta completely covered the internal cervical os. Partial PP covered the cervical os only partially, while marginal PP was determined if the placental edge reached the margin of the internal cervical os but did not cover any part of the dilated cervix (Dashe et al. 2013).
Transvaginal ultrasound was introduced in the 1980s and has allowed the precise determination of the distance between the internal cervical os and the placental edge. By this method, PP can also be determined as low-lying, which means it does not reach the internal cervical os but is 1 ̶ 20 mm from the os (Dashe et al. 2013).
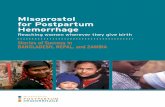
PP can also be defined as major or minor. When the placenta is overlying the cervical os totally or partially (includes complete PP and partial PP), it is called major PP. Minor PP is located 0 ̶20 mm away from the cervical os (includes marginal PP and low-lying PP) (Bahar et al. 2009, Jauniaux et al. 2017).
The resolution rate of minor PP is described to be as high as 90% before term, due to “placental migration” and the development of the lower uterine segment, although it is more unlikely in women with prior CS (Lal et al. 2015). The mechanism of migration is not fully understood. King introduced a hypothesis called “dynamic placentation,” a process in which part of the placental attachment to the uterine wall is constantly reformed throughout the pregnancy, while the lower uterine segment forms beneath the placenta. Dynamic placentation responds not only to the placental growth but also to the different growth rates of the placenta and the uterine wall (King 1973). Another hypothesis for placental migration is trophotropism, which refers to a process related to the atrophy of the thin placental edge due to deficient vascular supply, whereas the other placental parts continue to grow from the lower uterine segment toward the better vascularized uterine corpus (Benirschke et al. 2012).
Major PP has been associated with higher complication rates than minor PP. Women with major PP seem to have a higher incidence of antepartum hemorrhage, preterm deliveries, PPH, hysterectomies and AIP (Dola et al. 2003, Tuzovic et al. 2006, Bahar et al. 2009, Sekiguchi et al. 2013). Sekiguchi et al. showed the incidence of antepartum hemorrhage to be 59.1% among women with major PP and 17.6% among those with minor PP. Women with major PP were also at higher risk for preterm deliveries (45.1% versus 8.8%) (Sekiguchi et al. 2013). Bahar et al. had similar findings. They reported a significant association between antepartum hemorrhage (OR

17
3.18, CI 1.58–6.4) and preterm deliveries (OR 14.9, CI 4.9 ̶45.1) more commonly in women with major PP. In that same study, the incidences of AIP (OR 3.2, CI 1.22 ̶ 8.33) and of hysterectomies (OR 5.1, CI 1.31 ̶19.86) were higher in women with major PP (Bahar et al. 2009).
Figure 2. Different types of placenta previa.
MAJOR PLACENTA PREVIA
MINOR PLACENTA PREVIA
Complete Partial
Marginal Low-lying

18
Abnormally invasive placenta
AIP is a clinical situation in which the placenta abnormally invades into the myometrium (the muscular uterine wall) and does not separate easily at delivery, leading to hemorrhage (Collins et al. 2016, Jauniaux et al. 2017, Society of Gynecologic Oncology 2018, Jauniaux et al. 2018b). This condition is also called “placenta accreta spectrum disorder” and “morbidly adherent placenta” in the recent literature (Fox et al. 2015, Collins et al. 2019).
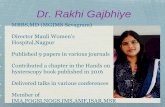
AIP can be divided into three forms, depending on the degree of invasion. The least severe, placenta accreta, is attached to the myometrium without an intervening decidua. Placenta increta is determined as a condition in which the chorionic villi invade deeper into the myometrium. Placenta percreta invades through the whole uterine wall and sometimes even to the adjacent organs, for example, the bladder or rectum (Jauniaux et al. 2017). Of all AIP cases, about 75% are represented by placenta accreta, followed by placenta increta (18%) and percreta (7%) (Miller et al. 1997).
Although these conditions are rare, the incidence is rapidly increasing worldwide, mostly due to advanced CS rates (Jauniaux et al. 2018c, Collins et al. 2019). In the United States, the incidence increased from 1 in 30 000 pregnancies in the 1960s to approximately 1 in 2500 pregnancies in a cohort from 1985 to 1994 (Miller et al. 1997). In recent years, the incidence of placenta accreta is described to be 0.01 ̶0.3% of deliveries (Morlando et al. 2013, Society of Gynecologic Oncology 2018).
AIP is often associated with massive PPH, resulting in surgical interventions, major complications, and even maternal death (Higgins et al. 2013, Silver et al. 2015, Jauniaux et al. 2017), with mortality rates reported to be 6 ̶ 7%. Intraoperative hemorrhage typically exceeds three liters (Baughman et al. 2008). Women with AIP are also more likely to have hysterectomies (OR 209.0, CI 19.9 ̶ 875.0) and loss of fertility (Farquhar et al. 2017).

19
Figure 3. Different types of abnormally invasive placenta.
Normal Placenta accreta
Placenta percreta Placenta increta

20
Genital tract trauma
Genital tract trauma includes perineal, vaginal and cervical lacerations and hematomas and uterine rupture. Trauma should always be suspected if bleeding occurs despite a well-contracted uterus. Sometimes, the only signs of hematoma might be pain and vital sign deterioration without obvious bleeding (Committee on Practice Bulletins-Obstetrics 2018). Uterine rupture is a rare (incidence 0.06 ̶ 0.14%) but is a severe complication associated with a high rate of perinatal morbidity and mortality (Walsh et al. 2007, Ronel et al. 2012, Sturzenegger et al. 2017).
Coagulation disorders
Coagulation disorders are relatively uncommon but serious causes of PPH (Silver et al. 2010, Evensen et al. 2017). Coagulopathy can be inherited or acquired. Inherited coagulopathies are usually determined before the delivery. The most common inherited causes of coagulopathies are hemophilia and von Willebrand disease (Evensen et al. 2017). Conditions leading to acquired coagulopathy include amniotic fluid embolism, placental abruption, sepsis, severe pre-eclampsia or HELLP. All these conditions may lead to disseminated intravascular coagulation (DIC) and hypofibrinogenemia (Gibbs et al. 2008). The use of anticoagulant medication such as aspirin or heparins also have an influence on coagulation (Gibbs et al. 2008).
The overall fibrinolytic capacity is attenuated during pregnancy, but in the uteroplacental circulation, significant activation of coagulation and fibrinolysis occurs simultaneously and leads to increased levels of fibrin degradation products (Ahonen et al. 2010). After childbirth, the early activation of fibrinolysis is recorded, possibly due to tissue damage during delivery (Kruithof et al. 1987). In a woman with PPH, the ongoing fibrinolysis and fibrin degradation products may impair the hemostatic outcome (Kruithof et al. 1987, Ahonen et al. 2010). Severe PPH may also lead to excessive loss of coagulation factors. Dilutional coagulopathy occurs if blood loss is replaced by a combination of crystalloids and red blood cells without clotting factors and platelets (Gibbs et al. 2008, Evensen et al. 2017).

21
2.1.4 Risk factors
Several risk factors for PPH are known (Tables 1 and 2). The strongest independent risk factor is a history of severe PPH in a previous pregnancy (OR 8.97, CI 5.25 ̶15.33) (Nyflot et al. 2017). Other significant risk factors include anticoagulation medication (OR 4.79, CI 2.72 ̶ 8.41), anemia (hemoglobin ≤90, OR 4.27, CI 2.79 ̶ 6.54), severe pre-eclampsia or HELLP syndrome (OR 3.03, CI 1.74–5.27), uterine fibromas (OR 2.71, CI 1.69–4.35) and multiple pregnancy (OR 2.11, CI 1.39–3.22) (Nyflot et al. 2017). However, two-thirds of women whose delivery is complicated with PPH are healthy and young, without obvious risk factors for developing PPH (Sheiner et al. 2005, Wetta et al. 2013). Risk assessment tools have been developed to help in the antenatal detection of women at high risk for PPH (Shields et al. 2011, Lyndon et al. 2015). The tools take several risk factors into consideration and divide women into low, medium and high-risk groups for PPH (Lyndon et al. 2015). Women in the low-risk group are those who had singleton pregnancies, fewer than four previous deliveries, an unscarred uterus and no history of PPH. At highest risk for PPH are women who have AIP, a known coagulation defect, history of PPH or significant bleeding when being admitted to the hospital (Lyndon et al. 2015). The risk assessment tools have been shown to identify 60–85% of women who will develop a significant PPH, although the specificity has been just below 60% (Shields et al. 2011, Lyndon et al. 2015). In Dilla et al. (2013), 0.8% of women in the low-risk group experienced massive PPH.
Women with a history of CS presenting with PP are at highest risk for AIP. The incidence of PP with AIP has shown to be 4.1% in women with one prior CS and 13.3% in women with two or more previous CSs (Jauniaux et al. 2017). Silver et al. reported the risk of AIP among women with PP to be as high as 67% if the woman has had more than five previous CSs. However, both PP and prior CS alone are also risk factors for AIP. AIP occurs in 3% of women who have PP without previous CS (Silver et al. 2006). A large study from Silver et al. included 30 132 women with a history of CS and an absence of PP. The results showed that placenta accreta was present in 0.24% of women undergoing their first CS and in 6.74% of women undergoing their sixth or higher (Silver et al. 2015). A prior CS alone and AIP without prior CS are also significant risk factors for uterine rupture (prior CS: OR 12.52, CI 5.21 ̶ 30.09; AIP without prior CS: OR 20.82, CI 2.48 ̶ 175.16) (Sturzenegger et al. 2017).

22
Table 1. Risk factors in relation to postpartum hemorrhage etiology (OR and CI are given if available)
Etiology Risk Factor OR (95% CI)
Atony Multiple pregnancy Birth weight ≥4000 g Polyhydramnion Uterine fibromas Induction of labor Augmentation of labor Prolonged second stage of labor Prolonged third stage of labor Chorioamnionitis Pre-eclampsia In-labor CS Anemia
2.6 (0.6 ̶ 12.0) (Wetta 2013) 1.1 (0.5 ̶ 2.3) (Wetta 2013) 1.9 (0.7 ̶ 5.0) (Wetta 2013) 2.71 (1.69 ̶ 4.35) (Nyflot 2017) 2.3 (1.2 ̶ 4.3) (Wetta 2013) 1.2 (0.7 ̶ 2.4) (Wetta 2013) 2.30 (1.2 ̶ 4.6) (Miller 2017) 1.9 (0.6 ̶ 5.4) (Wetta 2013) 2.5 (1.5 ̶ 4.4) (Wetta 2013) 2.8 (1.8 ̶ 4.4) (Wetta 2013) 1.95 (1.53 ̶ 2.47) (Nyflot 2017) 1.9 (0.6–2.8) (Wetta 2013)
Placental retention Previous placental retention Previous CS Previous curettage Preterm birth 32 ̶ 34 weeks Preterm birth 35 ̶ 36 weeks Pre-eclampsia Delivery of a SGA neonate Stillbirth in primipara/multipara Prolonged second stage of labor Vacuum delivery Endometritis Chorioamnionitis
21.72 (6.07 ̶ 77.7) (Klar 2013) 8.82 (8.35 ̶ 8.91) (Greenbaum 2017) 12.80 (10.57 ̶ 15.50) (Greenbaum 2017) 2.35 (1.97 ̶ 2.81) (Endler 2014) 1.55 (1.37 ̶ 1.75) (Endler 2014) 1.37 (1.21 ̶ 1.54) (Endler 2014) 1.47 (1.28 ̶ 1.70) (Endler 2014) 1.71 (1.28 ̶ 2.29) (Endler 2014) 2.03 (1.08 ̶ 3.82) (Greenbaum 2017) 1.89 (1.48 ̶ 2.41) (Ashwal 2014) 2.21 (1.64 ̶ 2.97) (Greenbaum 2017) 3.35 (2.78 ̶ 4.04) (Greenbaum 2017)
Genital tract trauma Primiparity Instrumental vaginal delivery Forceps delivery Previous CS Prolonged second stage of labor (≥2 hours) Precipitous delivery Fetal macrosomia Fetal occiput posterior position
10.0 (3.0 ̶ 33.3) (Christianson 2003) 2.24 (2.07 ̶ 2.42) (Simic 2017) 10.8 (5.2 ̶ 22.3) (Christianson 2003) 12.52 (5.21 ̶ 30.09) (Sturzenegger 2017) 1.42 (1.28 ̶ 1.58) (Simic 2017)
Coagulation abnormality Inherited coagulation factor deficiency Use of anticoagulation medication Severe infection Severe pre-eclampsia Placental abruption Amniotic fluid embolism
4.79 (2.72 ̶ 8.41) (Nyflot 2017) 3.03 (1.74 ̶ 5.27) (Nyflot 2017)
OR=odds ratio, CI=confidence interval, CS=cesarean section, SGA=small for gestational age

23
Table 2. Risk factors for placenta previa and abnormally invasive placenta (OR and CI are given if available)
Etiology Risk Factor OR (95% CI)
Placenta previa
One prior CS ≥Four prior CSs ART in singleton pregnancies Spontaneous abortion Induced abortion Smoking Cocaine use PP in previous pregnancy Multiple pregnancy
4.5 (3.6 ̶ 5.5) (Ananth 1997) 44.9 (13.5 ̶ 149.5) (Ananth 1997) 2.67 (2.01 ̶ 3.34) (Karami 2018) 1.6 (1.0 ̶ 2.6) (Ananth 1997) 1.7 (1.0 ̶ 2.9) (Ananth 1997) 1.42 (1.30 ̶ 1.54) (Shobeiri 2017) 1.4 (0.8 ̶ 2.4) (Handler 1994)
Abnormally invasive placenta PP One prior CS Two prior CSs ≥Three prior CSs PP and prior CS Age ≥40v in primiparous women ART PPH in previous pregnancy Multiple pregnancy
292 (196–400) (Thurn 2016) 6.6 (4.4 ̶ 9.8) (Thurn 2016) 17.4 (9.0 ̶ 31.4) (Thurn 2016) 55.9 (25.0 ̶ 110.3) (Thurn 2016) 614 (372 ̶ 844) (Thurn 2016) 19.1 (4.6 ̶ 80.3) (Farquhar 2017) 3.1 (1.6 ̶ 5.8) (Thurn 2016) 6.5 (3.7 ̶ 10.9) (Thurn 2016) 6.1 (1.1 ̶ 34.1) (Farquhar 2017)
OR=odds ratio, CI=confidence interval, CS=cesarean section, ART=artificial reproductive technology, PP=placenta previa, PPH=postpartum hemorrhage

24
2.1.5 Prevention
The third stage of labor should be actively managed to reduce the incidence of PPH (WHO 2012, Begley et al. 2019). A Cochrane systematic review reported the relative risk for PPH >1000 ml to be 0.34 (CI 0.14 ̶ 0.87) if the third stage was actively managed (Begley et al. 2019).
The three components of active management include (WHO 2012, Begley et al. 2019):
1. Routinely administered bolus of oxytocin 2. Uterine massage 3. Controlled umbilical cord traction Previously, oxytocin was determined to be the most effective medication with minimal side effects compared to other uterotonics (i.e., prostaglandins, ergot alkaloids) (Westhoff et al. 2013). Oxytocin is also currently recommended by the World Health Organization (WHO) as a PPH prophylactic (WHO 2012). The Cochrane systematic review from 2013 showed that the prophylactic use of oxytocin at any dose decreased the incidence of PPH (RR 0.53, CI 0.38 ̶0.74) and the need for therapeutic uterotonics (RR 0.56, CI 0.36 ̶0.87). Oxytocin was also a better choice than ergot alkaloids (Westhoff et al. 2013). The latest Cochrane systematic review from 2018 reported controversial results (Gallos et al. 2018), showing that ergot alkaloids in combination with oxytocin (RR 0.70, CI 0.59 ̶0.84), carbetocin (oxytocin analogue) alone (RR 0.72, CI 0.56 ̶ 0.93) and misoprostol (prostaglandin) in combination with oxytocin (RR 0.70, CI 0.58 ̶ 0.86) were more effective in the prevention of PPH ≥500 ml than oxytocin alone (Gallos et al. 2018), although combining medications is related to an increased risk for side effects (i.e., nausea, vomiting, hypertension, fever) (Gallos et al. 2018).
The Cochrane systematic reviews have also been assessed for the use of prostaglandins to prevent PPH (Tuncalp et al. 2012, Oladapo et al. 2012, Hofmeyr et al. 2013b). Misoprostol compared with placebo seemed to be effective in reducing PPH (RR 0.66, CI 0.45 ̶ 0.98) and the need for blood transfusions (RR 0.31, CI 0.10 ̶ 0.94) (Tuncalp et al. 2012). However, misoprostol was associated with a higher risk of PPH compared to other uterotonics (RR 1.33, CI 1.16 ̶ 1.52) (Tuncalp et al. 2012). Misoprostol is also associated with higher incidence of fever, especially in high doses (≥600 μg) (Hofmeyr et al. 2013b). In low-resource settings, the application of oxytocin is limited, and therefore, misoprostol is a considerable option for PPH prevention (Prata et al. 2013).
The effectiveness of uterine massage and controlled umbilical cord traction to prevent PPH are less clear. According to the Cochrane systematic reviews, controlled cord traction seems to reduce the need for manual removal of the placenta but does not prevent severe PPH (Hofmeyr et al. 2015). Also, uterine massage has no benefit in PPH prophylaxis (Hofmeyr et al. 2013a).
Antenatal anemia (hemoglobin ≤90 g/l) is associated with PPH (OR 4.27, CI 2.79 ̶ 6.54) (Nyflot et al. 2017). The National Institute for Health and Care Excellence (NICE) recommends screening for anemia in pregnant women (NICE 2008). Iron supplementation should be considered if

25
hemoglobin levels are lower than 110 g/l at first contact or lower than 105 g/l after 28 gestational weeks (NICE 2008).
2.1.6 Screening for placenta previa and antenatal diagnosis of abnormally invasive placenta
Finnish law has guaranteed a free-of-charge, midwife-conducted prenatal screening of fetal anomalies and aneuploidies for pregnant women since 2007 (Ministry of Social Affairs and Health). The uptake of the screening program is approximately 95% in the Helsinki metropolitan area (personal communication, Vedran Stefanovic). The screening for fetal structural anomalies is performed between 18+0 and 21+6 gestational weeks, at which time the placental position is also determined.
At Helsinki University Hospital (HUH), the protocol for the PP follow-up is based on a study of Taipale et al. (1998). In their study, 3696 pregnant women were systematically evaluated between 18 and 23 gestational weeks by transvaginal ultrasound to determine the placental location. In 57 women (1.5%), the placenta reached or overlapped the internal cervical os. The women were all called in for another ultrasound scan at 26–30 gestational weeks, and 91% of these women were re-scanned. Only ten women had PP at the time of re-scanning, and five had PP at term. In those five women, the placenta had covered the internal cervical os ≥15 mm at the mid-pregnancy screening. With 15 mm as a cut-off point, 27 women were screen-positive and all five PPs at term were found. Based on these results, if PP was suspected at a transabdominal ultrasound during the mid-pregnancy screening, Taipale et al. recommended a transvaginal ultrasound as well as a follow-up at 26 ̶30 gestational weeks for women whose placenta covered the internal cervical os ≥15 mm (Taipale et al. 1998).
Contrary to our follow-up protocol, the RCOG recommends a follow-up at 32 gestational weeks via a transvaginal ultrasound for all women who had major or minor PP at the mid-pregnancy screening (Jauniaux et al. 2018d, Jauniaux et al. 2018e). Kapoor et al. (2014) also recommended a follow-up for women whose placenta was <20 mm from the cervical os at screening. Their study included 181 women with minor PP. Composite outcomes were reported in 20 (11%) of these women, including PP (n=15), cord prolapse (n=3) and vasa previa (n=2) (Kapoor et al. 2014). If the repeat scan was only performed for the clinical indication of antenatal bleeding, fewer than half of these women with minor PP at term would have been identified (Kapoor et al. 2014). In Copland et al. (2012), 350 women with the placenta ≤20 mm from the cervical os were followed. At term, 9% had persistent PP (Copland et al. 2012). Robinson et al. (2012) also reported an increased risk of PPH ≥1000 ml in women whose placenta was 0–30 mm from the cervical os compared to those whose placenta was >30 mm from the cervical os (7.6% versus 4.7%, p<0.05).
Especially in women diagnosed with PP at the mid-pregnancy screening and with a history of CS, the existence of AIP should be evaluated carefully at the follow-up visit at 32 gestational weeks (Jauniaux et al. 2017, Jauniaux et al. 2018e). The AIP diagnosis is often missed during pregnancy;

26
for example, 70% of AIP cases were not diagnosed antenatally in a large Nordic study (Thurn et al. 2016).
Antenatal diagnosis of AIP and scheduled delivery with a multidisciplinary team is necessary to decrease PPH and complications related to AIP treatment (Tikkanen et al. 2011, Fitzpatrick et al. 2014, Silver et al. 2015, Jauniaux et al. 2017). Tikkanen et al. (2011) reported the median estimated blood loss at the time of CS to be 4500 ml (range 100 ̶ 15 000 ml) in women with antenatal diagnosis of AIP and 7500 ml (range 2500 ̶ 17 000 ml) in women whose AIP was not diagnosed antenatally.
The European working group for AIP (EW-AIP) has published standardized ultrasound descriptors to help diagnose AIP (Collins et al. 2016). A systematic review and meta-analysis from 2017 showed a sensitivity of 97% (CI 93.0–99.0) and a specificity of 97% (CI 97.0–98.0) for antenatal detection of AIP among women with prior CS and PP when using the standardized ultrasound signs (Jauniaux et al. 2017).

27
2.1.7 Management
Managing PPH requires a multidisciplinary approach that depends on the etiology of bleeding and the general condition of the patient. The amount of blood loss leads to the choice of optimal treatment, which includes early volume replacement, treatment of uterine atony, administration of tranexamic acid, removal of retained products and surgery for birth canal trauma. The main goal of management is not only to save lives but also to avoid complications and loss of fertility (Mousa et al. 2001, Ahonen et al. 2010, Mavrides et al. 2016). The protocol for PPH management is shown in Figure 4.
General principles
General principles in the management of PPH include:
- Recognition of PPH - Calling for assistance - Estimation of the amount of blood loss - Establishing access to several veins - Taking blood samples for basic diagnostic tests (blood count, coagulation
screen, kidney function, electrolytes, cross-matching test) - Replacing blood volume - Correction of coagulopathy - Monitoring vital parameters (pulse, blood pressure, urine output)

28
Active management of third stage of labor
Hemorrhage is estimated ≥500 ml, patient has deterioration of vital signs and bleeding continues
Etiology determinationTranexamic acid intravenously(not in cases of confirmed DIC)
Uterine atony
Uterine massage,uterotonics
Placental retention(total/partial)
Manual removal of placenta,curettage
Genital tract trauma
Suturation,hematoma drainage
Coagulopathy
Observe clotting and fibrinolysis,
clotting factors,frozen plasma,
platelets
- call for help- laboratory evaluation- venous access- blood volume replacement- coagulopathy correction- vital parameters monitoring- DIC score determination
Balloon tamponade
Pelvic artery embolization
Pelvic artery ligation, uterine compressive
sutures, hysterectomy
Pelvic artery embolization
Figure 4. Management protocol for PPH (Ahonen et al. 2010, Erez et al. 2014, Mavrides et al. 2016, Evensen et al. 2017).

29
Conservative management
Conservative management is primarily the treatment of uterine atony. When genital tract lacerations are excluded or sutured and the emptiness of the uterine cavity is ensured, the ongoing bleeding is due to uterine atony in most cases. First-line therapy consists of oxytocin infusion and uterine massage. Bladder emptiness must also be ensured. Second-line uterotonics include prostaglandins and ergot alkaloids (Ahonen et al. 2010, Mavrides et al. 2016).
Sulprostone (analogue of prostaglandin E2) has been used to treat both uterine atony and retained placenta without massive PPH (van Beekhuizen et al. 2006, Stefanovic et al. 2013). Two studies showed that there was less of a need for the manual removal of the placenta when using sulprostone infusion (49% and 40%, respectively) (van Beekhuizen et al. 2006, Stefanovic et al. 2013). In Stefanovic et al.’s study, the mean blood loss was significantly lower in women who were managed with sulprostone infusion compared to women who underwent manual removal of the placenta (582 ml versus 1275 ml). No adverse effects related to sulprostone infusion occurred. None of the women required intensive care, and there was no significant postpartum morbidity in either group (Stefanovic et al. 2013).
Tranexamic acid inhibits the enzymatic breakdown of fibrinogen and fibrin. A large (n=20 060) international randomized double-blind placebo-controlled trial showed that administration of tranexamic acid reduces deaths (RR 0.81, CI 0.65 ̶ 1.0, p=0.045) but does not reduce hysterectomies in women with PPH, regardless of the mode of delivery. Tranexamic acid was especially effective if given within three hours of delivery. No major adverse effects like thromboembolic complications occurred. This study confirmed that tranexamic acid should be given as soon as possible after bleeding onset (WOMAN Trial Collaborators 2017). The HUH recommendation for the use of tranexamic acid is to administer 1 g intravenously when bleeding reaches 500 ̶800 ml. A repeated dosage of 1 g is recommended if bleeding continues and reaches 1200 ̶ 1500 ml.

30
Tamponade
In stable patients, uterine or vaginal tamponade is a useful option for second-line therapy of PPH, depending on the site of bleeding. Packing with gauzes was the earliest method, but it was associated with an increased risk for infections and for difficulties detecting ongoing bleeding (Eastman 1950). In the last fifteen years, balloon tamponade has mostly replaced packing with gauzes.
There are few hypotheses about the mechanism of achieving hemostasis using uterine balloon tamponade (Belfort et al. 2011a, Kong et al. 2018a). Belfort et al. (2011a) suggest that the uterine tamponade balloons compress the uterine arteries and thus reduce uterine artery perfusion. Kong et al. reported opposite results. In a small cohort (n=20), they showed that intraluminal pressure of the uterine balloon (67 ̶ 92 mmHg) was lower than the patients’ systolic blood pressure. This implies that the mechanism of achieving hemostasis is probably due to compression of the vessels of the placental bed rather than exceeding systolic blood pressure or blocking blood flow in the uterine arteries (Kong et al. 2018a).
Several balloons have been introduced, including Foley’s catheter (De Loor et al. 1996), the Sengstaken-Blakemore tube (Chan et al. 1997), the Rusch catheter (Johanson et al. 2001), the condom catheter (Akhter et al. 2003), the Bakri balloon (BB) (Cook® Medical Incorporated, Bloomington, IN, USA) (Bakri et al. 2001) and the ebb complete tamponade system (ebb, Clinical Innovations, Salt Lake City, UT, USA) (Dildy et al. 2014). The difference between these catheters is mostly related to the balloon volume, material and presence of a cavity to drain blood. The BB and the ebb dual balloon are the only balloons exclusively designed to treat obstetric hemorrhage with good success rates. The largest case series included 407 patients and has reported a success of 91.7% (Wang et al. 2018).
Pelvic arterial embolization
When conservative management fails, proceeding to pelvic arterial embolization (PAE) or surgical procedures is mandatory without delay. PAE is a widely accepted and effective therapeutic approach in various etiologies of PPH (Lee et al. 2012). Success rates vary from 85% to 95% in recent publications (Chen et al. 2018).

31
Surgical management
Uterine compression sutures
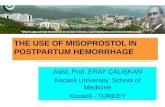
Uterine compression sutures have been used in the treatment of uterine atony. The best-known version of uterine compression sutures was introduced by B-Lynch in 1997. It requires hysterotomy for insertion and is thus a suitable method, especially during CS (B-Lynch et al. 1997). Since 1997, several compression suture modifications have been described, with the inventor’s name being used (Cho et al. 2000, Hayman et al. 2002, Pereira et al. 2005, Hwu et al. 2005, Ouahba et al. 2007, Hackethal et al. 2008). The success rate of achieving hemostasis with these methods has varied from 76% to 100% in the studies mentioned above. Complications related to uterine compression sutures are relatively rare, although often severe when they occur. They include uterine necrosis, uterine synechiae, pyometra and endometritis (Ochoa et al. 2002, Joshi et al. 2004, Wu et al. 2005, B-Lynch 2005, Suzuki et al. 2017). The influence on subsequent pregnancies seems to be minimal (An et al. 2013). An et al. did not find any differences in miscarriages (9.5% versus 10.1%) or preterm deliveries (4.7% versus 5.0%) between women who did or did not receive uterine compression sutures in their previous deliveries. The only difference between these groups was the rate of pelvic adhesions in repeat CS, which was significantly higher among women who were managed with uterine compression sutures compared to the control group (34.3% versus 17.5%) (An et al. 2013).
Figure 5. B-Lynch sutures.

32
Artery ligation
Ligation of the uterine arteries or the internal iliac arteries can be used in a selective group of women regardless of the etiology of PPH (Joshi et al. 2007). These procedures are technically difficult, and success rates to stop bleeding vary widely from 40% to 100%, depending on the experience of the surgeon (Clark et al. 1985, Chattopadhyay et al. 1990, AbdRabbo 1994, Joshi et al. 2007, Camuzcuoglu et al. 2010, Boynukalin et al. 2013). In approximately 50% of cases, hysterectomy can be avoided by using artery ligation (Gilstrap et al. 1994). Joshi et al. (2007) reported higher hysterectomy rates among women with uterine rupture managed with uterine artery ligation (79%) than in women with non-traumatic PPH (27%) managed with uterine artery ligation. In another study, the failure of internal iliac artery ligation was more common in women with atonic PPH (Chattopadhyay et al. 1990). Internal iliac artery ligation might also be beneficial after postpartum hysterectomy (Chattopadhyay et al. 1990), although Iwata et al. (2010) showed that, in cases with AIP, ligation of the internal iliac arteries did not significantly contribute to hemostasis during cesarean hysterectomy.
Complications are usually severe but quite rare (0 ̶ 4%). The severe complications include iliac vein ruptures and ureter injuries (Joshi et al. 2007, Boynukalin et al. 2013). Ligation of the internal iliac arteries may also lead to ischemic complications of the pelvic area (buttock claudication, buttock necrosis, spinal cord ischemia, colonic ischemia and bladder necrosis) (Chitraqari et al. 2015). Chitraqari et al. (2015) showed that these complications were less frequent in obstetric patients compared with oncology or vascular patients. Internal iliac artery ligation without hysterectomy seems to have no adverse effects on subsequent fertility or pregnancy outcomes, although the evaluation of fetal growth during the pregnancies is recommended (Nizard et al. 2003, Sziller et al. 2007, Unal et al. 2011, Doumouchtsis et al. 2014).
Hysterectomy
Hysterectomy is mandatory if a woman has life-threatening bleeding after delivery and if other methods have failed (Ahonen et al. 2010). According to two recent review articles, hysterectomy seems to complicate approximately 0.6 ̶ 0.7:1000 deliveries (van den Akker et al. 2016, Cheng et al. 2016). The most common indication for peripartum hysterectomy was AIP in both reviews. Also, uterine rupture and prior CS were major factors leading to hysterectomy (van den Akker et al. 2016). Van den Akker et al. (2016) reported a mortality rate of 5.2:100 hysterectomies. Hysterectomy also means a loss of fertility.
Hysterectomy requires surgical skills, and it may cause significant morbidity and iatrogenic lesions to the adjacent organs (ureter, urinary bladder, pelvic vessels) (Wani et al. 2014). Cheng et al. (2016) reported complication rates to be as high as 63%. Compared with non-obstetric hysterectomy, peripartum hysterectomy contains a higher rate of complications: bladder injury 9%

33
versus 1%, ureter injury 0.7% versus 0.1%, re-operation 4% versus 0.5%, transfusions 46% versus 4% and wound complications 10% versus 3% (Wright et al. 2010). Additionally, when comparing women with AIP undergoing hysterectomy to women with atony undergoing hysterectomy, the risk of bladder or ureter injury is two- to threefold higher in women with AIP (Wright et al. 2010).
Management of placenta previa
Mid-pregnancy fetal structural scanning includes the determination of the placental location. If major PP is suspected, the follow-up should be arranged at around 32 gestational weeks (Jauniaux et al. 2018e). The need for follow-up of minor PP is controversial (Taipale et al. 1998, Robinson et al. 2012, Copland et al. 2012, Kapoor et al. 2014, Heller et al. 2014). Taipale et al. (1998) recommend a follow-up after mid-pregnancy only for women with PP overlapping the cervical os ≥15 mm. However, a follow-up for women with minor PP was also recommended by the RCOG and two more recent studies (Copland et al. 2012, Kapoor et al. 2014, Jauniaux et al. 2017).
Women with asymptomatic PP can be cared for as outpatients (Silver 2015). In cases with recurrent bleeding episodes, hospitalization is needed. A retrospective study of 214 women showed that, as episodes of bleeding increased, preterm emergency CS was required more frequently. If a woman had one bleeding episode, the odds ratio (OR) for emergency CS was 7.5 (CI 2.5–23), and if she had three or more bleeding episodes, the OR was 27 (CI 8.3–90). The need for blood transfusions also increased (OR 6.4, CI 1.7–23) (Ruiter et al. 2016).
Routine antenatal corticosteroid therapy for diminishing neonatal respiratory morbidity is recommended between 34 and 35+6 weeks of gestation for women with PP, even without clinical symptoms (Jauniaux et al. 2017). The incidence of major hemorrhage is shown to increase after 36 gestational weeks. The risk for hemorrhage has been reported to be 4.7% by 35 gestational weeks, 30% by 37 gestational weeks and 59% by 38 gestational weeks (Zlatnik et al. 2007). Thus, elective CS for asymptomatic women should be planned between 36 and 37 gestational weeks. A late preterm (from 34 to 36+6 gestational weeks) delivery should be considered if several bleeding episodes have occurred or if a woman has other significant risk factors for preterm delivery (Zlatnik et al. 2010, ACOG 2013, Jauniaux et al. 2017).
In women with minor PP with no antepartum hemorrhage, vaginal delivery can be considered, especially when the placental edge is not thick and the distance between the internal cervical os and the placental edge is ≥10 mm (Nakamura et al. 2012, Al Wadi et al. 2014).
Women undergoing CS for PP are at increased risk of massive hemorrhage (Baba et al. 2014). Thus, CS should be arranged in a hospital with blood bank services and with an intensive care unit (Jauniaux et al. 2017). Also, an experienced surgeon and anesthesiologist should be present (Jauniaux et al. 2017). Additive treatment modalities are often needed to control PPH and avoid hysterectomy (Jauniaux et al. 2017). In recent years, intrauterine balloon tamponade has been

34
increasingly used either prophylactically to prevent PPH, or in cases of acute PPH due to PP (Cho et al. 2015, Maher et al. 2017).
Management of abnormally invasive placenta
Optimal management of AIP requires an antenatal diagnosis and a detailed management strategy (Allen et al. 2018, Collins et al. 2019). The International Society of Abnormally Invasive Placenta (IS-AIP) recently published evidence-based guidelines for AIP management (Collins et al. 2019).
An asymptomatic woman with AIP can be cared for as an outpatient. CS should take place in a tertiary center with a multidisciplinary team with significant experience managing AIP. Immediate availability of blood products and adult and neonatal intensive care units are mandatory. The timing of the delivery should be tailored individually (Allen et al. 2018, Collins et al. 2019). To avoid emergency CS, delivery between 34 and 35 gestational weeks has been suggested (Belfort 2011b, Jauniaux et al. 2017, Collins et al. 2019); to reduce the risk of neonatal morbidity, however, expectant management until 36 gestational weeks in women with no risk factors for preterm deliveries might be reasonable (Collins et al. 2019).
Antenatal steroid administration is always recommended if delivery occurs before 34 gestational weeks. Between 34 and 37 gestational weeks, administration should be considered on an individual basis, while taking other risk factors for neonatal respiratory problems into account. AIP itself does not seem to have an influence on neonatal respiratory morbidity or mortality (Collins et al. 2019).
During CS, after laparotomy, the uterine surface should be inspected for signs of AIP (bluish/distended uterine surface, placental tissue invasion through the uterine surface, abnormal neovascularization), and the uterine incision should be made avoiding placental transection. If the AIP diagnosis is still not clear after inspection and delivery of the infant, a gentle cord traction should be attempted. If the traction causes the uterine wall to pull inward without any sign of placental separation, no further traction is recommended. The next treatment options are expectant management (=leaving placenta in situ), hysterectomy or local uterine resection. If the diagnosis of AIP is unsure but not probable, manual removal of the placenta can also be attempted in combination with uterine-sparing surgery if needed (Sentilhes et al. 2018, Collins et al. 2019).
Kutuk et al. published a case series of 79 women with AIP (accreta n=33, increta n=18, percreta n=28) treated either with hysterectomy (group 1, n=27), expectant management (group 2, n=15) or manual removal of the placenta combined with conservative surgery (group 3, n=37). The results showed that total blood loss was lowest in women with expectant management (group 1: 2000 ml, group 2: 400 ml, group 3: 3000 ml). The difference was statistically significant compared to the other groups. A difference in surgical complication rates among the three groups was not found (group 1: 15%, group 2: 7%, group 3: 30%; p=0.119) (Kutuk et al. 2018). However, other

35
studies have reported severe complications related to expectant management, including uterine infection, placental abscess formation, sepsis, DIC and massive secondary PPH (Fox et al. 2015, Sentilhes et al. 2018).
Prophylactic balloon occlusion (PBO) of the iliac arteries, PAE and uterine balloon tamponade had been used in selective cases of AIP to control hemorrhage. These methods are described later.

36
2.1.8 Consequences
Physical outcomes
Of all maternal deaths, more than half occur within 24 hours after delivery. About three-quarters of deaths are suggested to be due to direct obstetric causes, with PPH being the leading single cause (WHO 2005, Say et al. 2014). It is estimated that, globally, a woman dies from PPH every four minutes, which is a total of 130 000 maternal deaths annually (ACOG 2006). Between 2003 and 2009, the estimated number of maternal deaths due to obstetric hemorrhage was 661 000 (27.1% of all maternal deaths) worldwide (Say et al. 2014). In high-income countries, the absolute risk of death is lower (1 ̶ 1.7:100 000 live births) compared to low-income countries (1:1000 live births) (Mousa et al. 2001, Creanga et al. 2017). Mortality from PPH has decreased since the late 1980s in the United States, and it accounted for 11.4% of maternal deaths between 2011 and 2013 (Creanga et al. 2017). In Finland, there were 37 maternal deaths between 1996 and 2010; six (16.2%) of these were related to PPH, which was the second most common reason for maternal deaths after thromboembolic complications (www.stat.fi).
PPH also causes maternal morbidity. The morbidity rate is estimated to be 6.7:1000 deliveries (Waterstone et al. 2001). Severe secondary morbidities include adult respiratory distress syndrome, acute renal failure, pituitary necrosis (Sheehan’s syndrome), cardiogenic shock, DIC and loss of fertility (Committee on Practice Bulletins-Obstetrics 2017).
Psychological outcomes
PPH, complicated delivery and hysterectomy may cause transient psychological stress or even long-term adverse psychological outcomes, including symptoms of post-traumatic stress disorder (PTSD) (Table 3). These problems affect not only women but also their partners and families (Sentilhes et al. 2011, Thompson et al. 2011, Elmir et al. 2012, Snowdon et al. 2012, de la Cruz et al. 2016, Eckerdal et al. 2016, Dunning et al. 2016, Carroll et al. 2016, Zaat et al. 2018). The diagnostic criteria for PTSD are shown in Table 4.
Sentilhes et al. reported that 67.6% of women who experienced PPH have negative memories of the delivery despite uterine preservation (Sentilhes et al. 2011). In Thompson’s study, over 20% of the women reported inadequate information and counseling after PPH (Thompson et al. 2011). The lack of information also affected partners (Snowdon et al. 2012, Dunning et al. 2016, van Stralen et al. 2010).
The review article from 2016 included six studies focusing on maternal morbidity after PPH. The main finding was a 13% incidence of postnatal depression and a 3% incidence of PTSD (Carroll et

37
al. 2016). Both PPH and postpartum hysterectomy seem to predispose to the development of PTSD (Carroll et al. 2016, Zaat et al. 2018). De la Cruz et al. (2016) showed that women were nearly 2.5 times more likely to have PTSD six months after delivery if they experienced peripartum hysterectomy (OR 2.46, CI 1.92 ̶ 3.16). Also, Tol et al. (2019) showed that women with antenatally diagnosed AIP seem to be at significant risk of developing PTSD compared to those who underwent uncomplicated CS for other indications (p=0.001).

38
Table 3. Psychological outcomes after postpartum hemorrhage and complicated delivery
Author, year, country
Study design Objective Cases (n) Study cohort Main results
Sentilhes, 2011, France
Semi-structured telephone interview
Long-term psychological impact of severe PPH
68 Women with PPH, women with EPH excluded
68% reported negative memories of the delivery
Thompson, 2011, Australasia
Validated questionnaires (EPDS, STAI, Milligan’s 10-item scale, 17-item PTDS checklist, SF36v2)
Experiences of care, concerns and needs after significant PPH
167 Women with PPH ≥1500ml and/or a decrease in hemoglobin concentration to 7 g/dl or less and/or of 4 g/dl more
20% reported lack of information, acknowledgment and reassurance after the delivery
Elmir, 2012, Australia
Semi-structured face-to-face, email or telephone interview
Experiences with EPH following a severe PPH
21 Women with PPH followed with EPH
Severe PPH is traumatic to women and their families
Snowdon, 2012, Great Britain
Semi-structured face-to-face interview
Experiences of severe PPH
9 women 6 partners
Women with severe PPH and their partners
Main experiences were communication difficulties, disempowerment and information deprivation
de la Cruz, 2016, USA
Retrospective cohort design, validated online screening for PTSD
Association between EPH and PTSD
74 (EPH) 335 (no EPH)
Women with EPH Statistically significant association with EPH and PTSD was found
Eckerdal, 2016, Sweden
Nested cohort study, validated questionnaire (EPDS)
Association between PPD and PPH
196 (≥1000 ml) 250 (<650 ml)
Women with PPH ≥1000 ml
No association with PPH and PPD was found
Dunning, 2016, Great Britain
Semi-structured interview
Emotional impact of PPH
11 women 6 partners
Women with minor (500–1000 ml), moderate (1000–2000 ml) and severe PPH (>2000 ml)
Women with PPH of any volume require more information
PPH=postpartum hemorrhage, EPH=emergency peripartum hysterectomy, PTSD=post-traumatic stress disorder, PPD=postpartum depression

39
Table 4. Diagnostic criteria for post-traumatic stress disorder (PTSD) (Modified from 10th revision of
the International Statistical Classification of Diseases and Related Health Problems, ICD-10)
Stressor criterion A.
1. Event is exceptionally threatening or catastrophic.
2. Event is likely to cause pervasive distress in almost anyone.
Symptom criterion Necessary symptoms:
B. Patient persistently remembers or “relives” the stressor in “flashbacks” or recurring dreams. Patient experiences distress when exposed to circumstances resembling the stressor or those associated with it. C. Patient has actual or preferred avoidance of circumstances associated with the stressor. D.
1. Patient is unable to recall some important aspects of the stressful event.
OR
2. Patient has persistent symptoms of increased psychological sensitivity and autonomic hyper-arousal (at least two of the following symptoms):
a. Difficulty falling or staying asleep
b. Irritability or anger
c. Concentrating difficulties
d. Hypervigilance
e. Exaggerated startle response.
Time frame Symptoms arise within six months of the traumatic event.

40
2.2 BAKRI BALLOON TAMPONADE
2.2.1 Device
The Bakri balloon (BB) (Cook® Medical Incorporated, Bloomington, IN, USA) was the first tamponade balloon designed exclusively for obstetric indication (Bakri et al. 2001).
The BB is a silicone-made, latex-free inflatable tamponade balloon. It is 58 cm long. The manufacturer’s maximum recommended inflation volume is 500 ml of sterile fluid, although the maximum filling volume has shown to be 2850 ml before the BB ruptures (Antony et al. 2017). The BB contains rapid installation components, which facilitate the inflation. The tip of the BB is designed with two holes for drainage, so ongoing bleeding is easy to detect (Bakri et al. 2001, www.cookmedical.com) (Figure 6).
2.2.2 Placement
The BB can be placed into the uterus or vagina depending on the bleeding site. Uterine placement can be performed through the cervical opening after vaginal delivery or abdominally through hysterotomy after CS. The correct placement after vaginal insertion should be confirmed via ultrasound. Traction (a maximum of 500 g) can be applied to the balloon shaft if needed. The maximum usage time is 24 hours, although the balloon can be removed earlier if bleeding is controlled and the patient is stable. While using the BB, routine antibiotic prophylaxis and urine output monitoring are recommended (www.cookmedical.com).
Inflation volume can be determined by a “tamponade test’” (Georgiou 2010, Yorifuji et al. 2011). If positive, it means that the BB is inflated gradually until the bleeding stops. If the bleeding does not stop when the maximum amount of fluid (500 ml) is filled, the test has failed and additional management is needed.

41
Figure 6. Bakri balloon.

42
2.2.3 Obstetric indications
The overall rate of Bakri balloon tamponade (BBT) use is estimated to be about 0.2% among all deliveries (Wright et al. 2014). Approximately 75% of the insertions have followed vaginal delivery according to a review of Said Ali et al. (2019).
The two main indications for BBT are uterine atony and PP (www.cookmedical.com, Wright et al. 2014, Said Ali et al. 2019). An increasing number of publications on the off-label BBT also highlight its use for other obstetrical emergencies (e.g., vaginal lacerations and paravaginal hematomas, uterine inversion and pelvic floor hemorrhage) (Gizzo et al. 2013, Kaya et al. 2014a, Charoenkwan et al. 2014, Alouini et al. 2015).
Most recent publications have assessed cases of uterine atony and PP (Table 5). BBT seems to decrease hysterectomy rates in both indications (Revert et al. 2018, Lo et al. 2017). Lo et al. reported hysterectomy rates in women with uterine atony to be 7.8:10 000 before BBT was routinely used and 2.3:10 000 after its regular implementation. This difference was statistically significant (p=0.01) (Lo et al. 2017).
In cases of uterine atony, BBT can be used when the primary treatment with uterotonics and uterine massage has failed (Kaya et al. 2014b, Lo et al. 2017). Early detection of PPH with rapid usage of BBT seems to be the most effective treatment modality (Wang et al. 2018). Wang et al. (2018) showed that, during vaginal deliveries, women with hemorrhage of >2000 ml before BBT had significantly more total blood loss (551.67 ± 635.17 ml versus 242.06 ± 313.69 ml) and lower maternal hemoglobin levels (73 ± 21.77 g/l versus 92.06 ± 19.60 g/l) than those with hemorrhage of <1000 ml before BBT.
In cases of PP, BBT can be inserted when acute PPH occurs, or it can be used prophylactically to prevent massive PPH in the placental site (Kumru et al. 2013, Beckmann et al. 2014, Cho et al. 2015, Maher et al. 2017, Soyama et al. 2017). In this indication, traction can be applied to the balloon shaft to increase the balloon pressure against the placental bed. Soyama et al. (2017) demonstrated that the routine rapid insertion of the BB during CS in women with PP significantly decreased intraoperative hemorrhage (991 g versus 1250 g) and postoperative hemorrhage (62 g versus 150 g) and shortened the duration of CS (30 min versus 50 min). On the contrary, Beckmann et al. (2014) did not find a significant reduction in hemorrhage using BBT prophylactically in women with PP, but they concluded that the method is beneficial with no evidence of increased complications.
Promising success rates in women with AIP have also been reported (Pala et al. 2018). Pala’s study included 36 patients diagnosed pre- or intraoperatively with placenta accreta or increta. Of the women, 19 were treated with BBT, while 17 were treated with hysterectomy. The success rate of BBT was 84.2%. The mean amount of blood loss (2694 ± 893 ml versus 1794 ± 725 ml) and the need for blood transfusion (5.7 ± 2.4 units versus 2.7 ± 2.6 units) was higher in the cesarean

43
hysterectomy group, and the operation time was longer (140 ± 51 min versus 64.5 ± 29 min). They concluded that, in cases with AIP, uterine balloon tamponade before hysterectomy is encouraging with its advantages compared to hysterectomy alone, especially when trying to preserve fertility (Pala et al. 2018).
Only a few case reports concerning indications other than uterine atony and PP exist. BBT seems to be effective in cases of vaginal tears or paravaginal hematomas, although the reported number of such cases is small (Tattersall et al. 2007, Gizzo et al. 2013, Alouini et al. 2015). In three reported cases, uterine inversion is treated successfully with reposition and BBT (Kaya et al. 2014a, Ida et al. 2015, Vivanti et al. 2017). One case report describes successful balloon insertion into a bicornuate uterus during CS (Abraham 2017), although the manufacturer does not recommend BBT for women with uterine anomalies. In that case, the right uterine horn was atonic compared to the left, and there was ongoing bleeding despite the use of uterotonic medication. The BB was inserted into the right horn and atony was solved (Abraham 2017).
2.2.4 Contraindications
The manufacturer stated a few contraindications of BBT use: uncontrollable bleeding needing additional treatment modalities; DIC; purulent infection in the vagina, cervix or uterus; untreated uterus anomaly; and cervical cancer (www.cookmedical.com).

44
2.2.5 Combination with other treatment methods
In cases of uterine atony, BBT has been combined with uterine compression sutures (=uterine sandwich technique) with good success rates (Nelson et al. 2007, Yoong et al. 2012, Diemert et al. 2012). Diemert et al. reported a cohort of 24 women treated with BBT alone or with the uterine sandwich technique. With BBT alone, 60% of women were treated successfully, and 30% were successful using BBT combined with uterine compression sutures (Diemert et al. 2012). In Yoong et al., 11 women had uterine atony due to PP. The combined technique was successful in all cases, and hysterectomy was avoided (Yoong et al. 2012). Guo et al. (2018) reported that BBT combined with vaginal tamponade and compression sutures (n=163, success rate 96.3%) was even more effective than BBT alone (n=142, success rate 87.3%).
Three small studies have compared the efficacy of BBT and uterine compression sutures in uterine atony during CS (Kavak et al. 2013, Kaya et al. 2016, Cekmez et al. 2015). The success rates were similar between these methods. However, the results concerning operation times were controversial. Kavak et al. (2013) reported shorter operation times (62.8 ± 3.9 min versus 78.3 ± 8.1 min) and less blood loss (intraoperative hemorrhage 1520 ± 92 ml versus 1946 ± 242 ml, postoperative hemorrhage 120 ± 56ml versus 351 ± 70ml) while using BBT. Their study was a randomized study including women with PP and atony. Six women were managed with uterine compression sutures and seven with BBT (Kavak et al. 2013). Kaya’s retrospective case series included 21 women managed with BBT and 24 managed with B-Lynch sutures. They reported a longer operation time with BBT, but they considered it a less invasive method and easier to learn (Kaya et al. 2016). Cekmez’s (case series study, n=32) results suggested that BBT in combination with uterine artery ligation and uterine compression sutures might be the most effective surgical approach in treating PPH due to uterine atony (Cekmez et al. 2015). These results confirm that the usage of BBT does not exclude the use of other methods, especially when BBT fails.

45
2.2.6 Success rate
BBT is considered successful if bleeding stops after balloon insertion and if no further interventions are needed. The reported hysterectomy rate is about 1% among women who required BBT (Said Ali et al. 2019). Previous studies have shown high success rates, which are summarized in Table 5.
Table 5. Success rates of Bakri balloon tamponade
Author, year, country Cases (n)
Indication of BBT Success rate (%)
Bakri, 2001, Saudi Arabia
5
PP
60
Vitthala, 2009, Great Britain 15 PP, accreta 80 Patacchiola, 2012, Italy 16 atony, PP 100 Laas, 2012, France 43 atony 86 Aibar, 2013, Spain 24 atony, PP, accreta 87.5 Kumru, 2013, Turkey 25 PP 88 Vrachnis, 2013, Greece 18 atony, PP, placental retention, trauma 94.4 Olsen, 2013, USA 35 N/A 67.6 Kong, 2013, Hong Kong 19 atony, PP 79 Kaya, 2014, Turkey Martin, 2015, France
45 49
atony atony, PP, placental abruption/retention
75.5 65
Cekmez, 2015, Turkey 32 atony 70 Alouini, 2015, France 61 atony, PP, placental retention, trauma 88 Alkis, 2015, Turkey 47 atony, PP, placental retention 91.4 Vintejoux, 2015, France and Austria 36 atony 69 Cho, 2015, Korea 64 PP 75 Kaya, 2016, Turkey and Germany 21 atony 80 Nagai, 2016, Japan 10 atony, PP 90 Brown, 2016, Kenya 58 atony 95 Maher, 2017, Saudi Arabia 72 PP 87.5 Mathur, 2018, Singapore 49 atony, accreta, placental retention 81.6 Pala, 2018, Turkey Revert, 2018, France
19 226
accreta and increta atony, PP
84.2 83.2
Wang, 2018, China 407 N/A 91.7 Grange, 2018, France 108 atony, PP, accreta, placental retention 74.1
BBT=Bakri balloon tamponade, PP=placenta previa, N/A=not applicable

46
2.2.7 Factors related to failure
Possible factors related to BBT failure seem to be undiagnosed AIP (p=0.011), hemorrhage of >1500 ml (p<0.001) or presence of coagulopathy (OR 5.6, CI 2.5 ̶13.0) at the time of BB insertion, history of CS (OR 8.90, CI 2.27 ̶34.83) and CS as a current mode of delivery (OR 3.5, CI 1.6 ̶ 7.5), anterior placentation in PP patients (OR 12.75, CI 1.04 ̶155.94) and catheter drainage volume of >500 ml within an hour after BB placement (p<0.01) (Olsen et al. 2013, Cho et al. 2015, Revert et al. 2017, Mathur et al. 2018, Grange et al. 2018). Grange et al. (2018) also reported obesity (BMI ≥30 kg/m2) as a predictive factor for BBT failure (OR 4.40, CI 1.06 ̶ 18.31) after vaginal delivery.
2.2.8 Complications
The majority of previous studies report no complications related to BBT (Patacchiola et al. 2012, Kumru et al. 2013, Beckmann et al. 2014, Vintejoux et al. 2015, Alkis et al. 2015). However, in some studies, a few minor complications have been documented, including endometritis (Laas et al. 2012, Revert et al. 2017) and pain (Aibar et al. 2013) in single cases. Several balloon prolapses after insertions have been described, although the BB was mostly successfully re-inserted, and cessation of bleeding was achieved (Vintejoux et al. 2015, Soyama et al. 2017). The incidence of displacement is described to be about 10% (Wright et al. 2014, Said Ali et al. 2019).
Five case reports have shown severe complications related to BBT. In one case, the drainage channel of the BB was blocked by a clot, which delayed the detection of massive ongoing bleeding, resulting in cardiogenic shock and hysterectomy. The authors recommended frequent ultrasound check-ups to avoid this kind of complication (Takahashi et al. 2015). In the other four cases, the authors described uterine rupture as a consequence of BBT insertion, leading to hemorrhage and hysterectomy (Ajayi et al. 2013, Leparco et al. 2013, Rocher et al. 2019).

47
2.2.9 Long-term outcomes
Little is known about the long-term effects of BBT. Only two studies have primarily been assessed to evaluate menstruation, fertility and pregnancy outcomes following the sole use of BBT (Georgiou 2014, Kong et al. 2018b).
Georgiou’s study included five women with uterine atony who were treated with BBT. Normal, regular menstruation returned to all women after the cessation of breastfeeding. Also, ultrasound appearances of the uterine cavities were normal. All of the women had subsequent pregnancies within 15 ̶29 months; no one complained about infertility. All pregnancies were uncomplicated, and the women had vaginal deliveries with no massive recurrent PPH (250 ̶ 1000 ml). One woman needed uterotonics for uterine atony (Georgiou 2014).
Kong et al. had similar results in their study of 39 women treated with BBT. The menses of all the women returned, and 87.2% reported normal menstrual patterns after 12 months of BBT. Nine subsequent pregnancies occurred, including two miscarriages, one uterine scar pregnancy and one induced abortion. The five remaining pregnancies were normal with full-term deliveries and normal-weighted infants (Kong et al. 2018b).
In addition to these two studies, few other pregnancies were reported after BBT. Alkis et al. followed 40 patients after BBT for subsequent deliveries. Of these, 15 had sterilization and 25 were trying for a subsequent pregnancy. Four of those 25 women became pregnant, and three delivered vaginally with no major complications (Alkis et al. 2015). In a French study, 61 women were treated with BBT; following treatment, 9 of the women had a new pregnancy, and 3 delivered healthy newborns (Alouini et al. 2015). In Martin et al.’s study, 49 women were treated with BBT, 38 of which had preserved uteri. Of these, 24 (63%) were contacted by telephone; two women wanted another pregnancy soon after BBT, and both became pregnant and had full-term pregnancies without recurrence of PPH (Martin et al. 2015). Pala et al. (2018) also reported two successful pregnancies after treatment of AIP with BBT.
These results implicate that BBT has minimal effects on menstruation and fertility. Subsequent pregnancies or deliveries do not seem to have major adverse outcomes.

48
2.3 INTERVENTIONAL RADIOLOGY PROCEDURES
The evolution of interventional radiology procedures (IRP) began over 50 years ago. Nowadays, IRPs include a wide variety of angiographic and non-angiographic procedures in almost every medical field performed by interventional radiologists. The main areas of IRPs are diagnostic angiography, transluminal balloon angioplasty with or without stent placement (coronary arteries, lower extremity arteries), controlling hemorrhage with embolization particles and inhibiting tumor growth with embolization or targeted cytotoxic therapy. There are also non-vascular interventions, for example, management of biliary system obstructions by stents, percutaneous abscess draining and percutaneous nephrostomy. IRPs have had a dramatic impact on the survival of patients in several fields (Baum et al. 2014).
2.3.1 Obstetric indications
In an obstetrical setting, IRPs include pelvic arterial embolization (PAE) and prophylactic balloon occlusion (PBO) of pelvic arteries. PAE was first introduced in 1979 by Brown et al., although using PAE in obstetric indications did not increase until the new millennium (Brown et al. 1979). Since that time, PAE has been accepted as a second-line treatment option in the management of acute PPH if conservative methods have failed (RCOG 2007). PBO of the pelvic arteries (common iliac arteries, internal iliac arteries, uterine arteries) or abdominal aorta with or without PAE has been used during CSs in women with anticipated AIP (Lee et al. 2012, Mei et al. 2015, Revert et al. 2018, Shahin et al. 2018). The main purpose of PBO is to prevent PPH, reduce the need for transfusions, shorten the operation time and enhance the ease of potentially complicated surgery (Shrivastava et al. 2018).

49
2.3.2 Method
Knowledge of the normal anatomy of the female genital tract and its vascularization is essential to performing PAE safely. The common iliac artery divides into internal and external branches. The internal iliac branch divides further into the anterior and posterior branches. The anterior branch gives rise to the umbilical, superior/inferior vesical, obturator, middle rectal, inferior gluteal, internal pudendal, uterine and vaginal arteries, while the posterior branch divides into the iliolumbar, lateral sacral and superior gluteal arteries.
Figure 7. Main pelvic arteries.

50
Acute postpartum hemorrhage
PAE is performed using a transfemoral approach. The femoral artery is usually catheterized unilaterally (Gonsalves et al. 2010, Soyer et al. 2015). However, in some clinical situations, bilateral catheterization may have advantages, such as less catheter manipulation, faster access to the internal iliac arteries and, thus, faster hemostasis achievement with less fluoroscopy time (Bratby et al. 2007). The femoral artery is accessed using the Seldinger technique with the help of palpation, fluoroscopy or ultrasound (Seldinger 1953). Unilateral catheterization of the common femoral artery allows the catheterization of both iliac arteries by using a Waltman loop (Shlansky-Goldberg et al. 2001). A 5 French scale (Fr) introducer with a 5 Fr Cobra catheter (Cook® Medical Incorporated, Bloomington, IN, USA) is most commonly used (Soyer et al. 2015). Microcatheters (3 Fr) are sometimes needed for super selective embolization (in only 3% of cases) (Pelage et al. 1999b).
After catheterization, angiography of the internal iliac arteries is performed to identify the uterine arteries or other sites of bleeding (Pelage et al. 1999a, Gonsalves et al. 2010, Lee et al. 2012, Lee et al. 2018). In approximately in one-third of women, the bleeding site is visible in angiography (Pelage et al. 1999a, Lee et al. 2012, Soyer et al. 2015, Lee et al. 2018). Visible extravasation of the contrast agent, artery cut-offs and pseudoaneurysms are considered active bleeding foci (Gonsalves et al. 2010, Lee et al. 2012). The absence of extravasation is quite common in women with uterine atony, whereas the bleeding site is more frequently observed in women with genital tract lacerations (Fargeaudou et al. 2009). Lee et al. (2012) reported the bleeding site to be visible more often in women who had undergone failed surgical procedures before PAE compared to those who did not have prior surgery (54.5% versus 35.4%). When extravasation is visible, the most common sources are the uterine and vaginal arteries (Pelage et al. 1999a, Gonsalves et al. 2010, Lee et al. 2012, Lee et al. 2018).
After angiography, the embolization is performed under the following principles (Pelage et al. 1999a, Gonsalves et al. 2010, Lee et al. 2012, Lee et al. 2018):
1. Selective arterial embolization when the active bleeding focus is visualized in angiography 2. Embolization of both uterine arteries when the active bleeding focus is not visualized in
angiography 3. Embolization of the anterior branch of the internal iliac arteries if catheterization of the
uterine arteries has failed, if hysterectomy is performed or if the bleeding continues despite embolization of the bilateral uterine arteries or other target arteries.
Bilateral embolization is typically required due to the rich collateral circulation in the pelvic area (Gonsalves et al. 2010, Soyer et al. 2015). It is sometimes necessary to skip microcatheterization and do non-selective embolization to achieve hemostasis more rapidly (Gonsalves et al. 2010). Aortography is needed in cases with persistent or recurrent bleeding after embolization of the

51
uterine or internal iliac arteries. Especially ovarian arteries and round ligament arteries are potential sites of continual bleeding (Leleup et al. 2017, Kim et al. 2018).
The reported mean overall procedure time is around 90 minutes (Soyer et al. 2015).
Anticipated postpartum hemorrhage due to abnormally invasive placenta
The common femoral arteries are catheterized bilaterally with the Seldinger technique under local anesthesia. Vascular sheaths are introduced to the pelvic arteries, usually to the internal iliac arteries. Exact placement of the balloon catheters depends on the terms by which the vascular tree is targeted. The balloons’ optimal inflation size is tested before the surgery. They are then deflated and inflated again, either routinely after the birth of the infant or sometimes only if needed. Catheter placement also allows for PAE after delivery. After hemostasis is secured (usually about 30 minutes), the balloons are deflated and catheters removed (Fox et al. 2015, Shrivastava et al. 2018, Kaufman et al. 2018). If PBO of the aorta is performed, the balloons can be left inflated for periods of only 5 ̶ 15 minutes followed by 1 ̶ 2 minutes of deflation to allow for distal perfusion (Wang et al. 2017). Sometimes, one of the femoral catheters is left for 24 hours in case of recurrent bleeding and if emergent PAE is necessary (Kaufman et al. 2018).
PAE, along with PBO, can be used in several indications (Fox et al. 2015, Kaufman et al. 2018, Collins et al. 2019):
1. Routinely before peripartum hysterectomy 2. In cases of continuous bleeding after peripartum hysterectomy 3. In the postoperative setting in cases of uterine preservation and PPH. Using PAE prophylactically is also thought to fasten placental resolution and to prevent secondary PPH in women with conservative management of AIP. Still, reliable evidence of the efficacy is lacking, and uterine necrosis related to PAE has been reported. Therefore, IS-AIP does not recommend the use of prophylactic PAE in the conservative management of AIP (Collins et al. 2019).

52
2.3.3 Embolization materials
The choice of embolization material depends on the site of bleeding, angiographic findings and the success of the catheterization of specific arteries. Embolic materials can be classified as permanent or temporary (Gonsalves et al. 2010, Das et al. 2014). Permanent materials include metallic coils, polyvinyl alcohol particles, n-butyl cyanoacrylate and microspheres. Temporary agents are usually the first choice because they allow the preservation of uterine perfusion and thus further fertility (Gonsalves et al. 2010). The gelatin sponge is the most commonly used material for PPH embolization; it allows for temporary occlusion of embolized arteries for three to six weeks, as well as recanalization (Gonsalves et al. 2010). It may have inadequate effectiveness in cases with DIC or pseudoaneurysms. The best choice in these cases is n-butyl cyanoacrylate (Park et al. 2015, Obata et al. 2017). N-butyl cyanoacrylate is also shown to be effective in cases of arterial ruptures, genital tract lacerations and arteriovenous fistulas (Kanematsu et al. 2011, Dohan et al. 2013). The use of small (150 ̶ 200 μm) polyvinyl alcohol particles is not recommended because they are related to a higher incidence of ischemic complications such as uterine necrosis (Cottier et al. 2002). Metallic coils are rarely needed; they are mainly used to occlude ruptured pseudoaneurysms (Dohan et al. 2013).
2.3.4 Success rate and factors related to failure
Pelvic arterial embolization
The overall success rate of PAE in women with acute PPH is 79 ̶ 100% (Pelage et al. 1999a, Gonsalves et al. 2010, Lee et al. 2012, Poujade et al. 2012, Mei et al. 2015, Soyer et al. 2015). In one of the largest published studies so far (n=251), the success rate after primary PAE was 86.45%, and it was 90.04% after repeated PAE (Lee et al. 2012). PAE has been demonstrated to be an effective treatment modality regardless of the etiology of acute PPH (Soyer et al. 2015).
Occasionally, PPH cannot be controlled even after a successful PAE. Reported clinical failure rates are between 5.2% and 11.0% (Sentilhes et al. 2010a, Bros et al. 2012, Poujade et al. 2012, Kim et al. 2013). Kim et al. had the largest cohort of women (n=257). In their study, PAE failed to treat PPH in 9.3%. They compared outcomes between women with either failed or successful PAE. In multivariate analysis, DIC was the only statistically significant independent factor related to PAE failure (OR 6.569, CI 1.602 ̶ 26.932). Other factors more frequently found in women with failed PAE included a hemoglobin level of <80 g/l and extravasation detected in angiography. Women with failed PAE experienced more major complications than women with successful PAE (37.5% versus 9.4%) (Kim et al. 2013). Bros et al. (2012) also found coagulation disorders significantly related to PAE failure (OR 12.08, p=0.006).

53
Other risk factors related to recurrent bleeding after PAE reported in the studies are: primiparity (OR 18.84, CI 1.81 ̶ 195.74, p=0.014), abnormal uterine artery anatomy (OR 9.83, CI 2.13 ̶45.32, p=0.003), presence of placenta accreta (p<0.005), amount of estimated blood loss >1500 ml (p<0.001) and transfusion of more than five red blood cell units (p<0.004) (Sentilhes et al. 2009, Bros et al. 2012, Poujade et al. 2012, Lee et al. 2012, Kim et al. 2013). The reported rate of PAE failure has been about 20% in women with PPH due to AIP (Soyer et al. 2011, Soyer et al. 2015).
Re-bleeding after PAE is usually a consequence of recanalization of the embolized arteries or the opening of the collateral arteries (Soyer et al. 2015). Repeated PAE is an effective option in treating re-bleeding. Lee et al. reported a 75% success rate of repeated PAE after one failed session. Permanent embolic materials are recommended in these cases (Lee et al. 2012).
Temporary prophylactic balloon occlusion
The effect of PBO on PPH is not yet confirmed, mainly due to the lack of randomized controlled trials, small study cohorts and mixed results in studies. Some serious complications have also been reported (iliac artery thrombosis or rupture and ischemic nerve injury) (Collins et al. 2019).
One small randomized controlled trial has compared outcomes between women whose AIP was managed with hysterectomy only (control group, n=14) or with hysterectomy combined with PBO of the internal iliac arteries (intervention group, n=13) (Salim et al. 2015). There were no statistically significant differences between the groups in blood loss (intervention group 4950 ml, control group 4709 ml), amount of transfused red blood cells (5.2 units versus 4.1 units) or complications. Feng et al. had similar results, although their cohort also included non-hysterectomized women. Hysterectomy rates were similar whether PBO was performed or not (43.4% in women with PBO versus 27.3% in women without PBO) (Feng et al. 2017).
On the contrary, a few small case-control studies have reported a significant difference in blood loss and the requirement of transfusions among women who had PBO of the pelvic arteries compared to women without PBO (Tan et al. 2007, Ballas et al. 2012, Cali et al. 2014, Cho et al. 2017). Cali et al. demonstrated PBO to be particularly useful in controlling hemorrhage in women with placenta percreta (n=13). The mean estimated blood loss and transfused red blood cell units were higher in women managed with hysterectomy only compared with women managed with PBO and hysterectomy (1507 ml versus 933 ml, 3.31 units versus 0.67 units) (Cali et al. 2014).
Shahin et al. recently published a review and meta-analysis concerning endovascular interventional modalities for controlling PPH in women with AIP. The meta-analysis included 1395 women, of which 470 (33.6%) had PBO of the internal iliac arteries, 460 (33%) of the aorta, 181 (13%) of the uterine arteries and 21 (1.5%) of the common iliac arteries. PAE was also performed in 263 (19.2%) women. They found IRPs to be significantly associated with less hemorrhage (p<0.001). PBO of the aorta was the most efficient method, associating with lower hysterectomy

54
rates and hemorrhage (Shahin et al. 2018). However, lower extremity arterial thromboses and ischemic injuries of the femoral nerves have been described to be related to PBO of the aorta (Wei et al. 2016).
2.3.5 Short-term complications
The complication rate related to IRPs is reported to be around 3 ̶ 4%. Complications can be divided into minor and major complications, as shown in Table 6.
Table 6. Complications related to interventional radiology procedures
Minor complications Major complications
Transient fever
Vessel rupture or dissection
Mild leukocytosis
Puncture site aneurysm
Endometritis
Deep venous thrombosis
Transient sciatic nerve paresis
Local necrosis (uterus, vagina, bladder)
Transient numbness in buttocks or lower extremities
Distant necrosis (due to migration of embolic particles)
Hematoma at the puncture site
Severe infection, sepsis
Synechiae
Ischemic nerve injury
Pelvic pain
Contrast agent reaction
(Sentilhes et al. 2009, Lee et al. 2012, Cheong et al. 2014, Soyer et al. 2015, Wei et al. 2016, Soro et al. 2017)

55
2.3.6 Long-term outcomes
Fertility and menstruation
One of the main advantages of PAE is that it allows uterine preservation. During PAE, the radiation dose to the ovaries depends on the protocol but is usually quite high (mean estimated dose 58.6 centigrays). This could potentially lead to transient or permanent ovarian failure (Eriksson et al. 2007). The other mechanism for ovarian failure is the possible migration of embolization particles from the uterine arteries into the ovarian arteries through collaterals. Embolization may also induce transient endometrial ischemia, which might affect implantation and future fertility (Soro et al. 2017).
Despite concerns about ovarian function, many studies have reported no adverse effects on the menstrual cycle or further fertility after PAE (Chauleur et al. 2008, Gaia et al. 2009, Delotte et al. 2009, Fiori et al. 2009, Hardeman et al. 2010, Lee et al. 2012, Cheng et al. 2017). In Soro et al.’s (2017) review, 81.3% (618/760) of women had normal menstrual cycles 1 ̶ 10 months after PAE, and only 10.9% (87/760) had oligo- or amenorrhea, probably due to PAE. Gaia et al. included 107 women in their follow-up after PAE for PPH. Normal menstruation returned in 92.5% of women. Six (5.6%) women reported amenorrhea and had uterine synechiae confirmed through hysteroscopy, which is probably a result of endometrial ischemia related to PAE (Gaia et al. 2009). Chitrit et al. (2006) described a single case with permanent amenorrhea due to uterine necrosis despite normal hormonal patterns. Follicle-stimulating hormonal levels are reported to be similar before and after PAE in the study of Alanis et al. (2006).
Pregnancies
In Soro et al.’s review, a total of 38 studies reported pregnancies after PAE. Altogether, 249 women (23.2%) had 234 pregnancies resulting in live births. The rate of miscarriage was 10%, which is comparable to the general population (Soro et al. 2017).
PAE may cause endometrial ischemia, which raises concerns about pathological placentation leading to placental dysfunction and fetal intrauterine growth restriction (Soro et al. 2017). However, only a few cases of fetal intrauterine growth restriction have been described (Cordonnier et al. 2002, Chauleur et al. 2008, Hardeman et al. 2010). The rest of the studies reported normal-weighted infants (mean weight 3250 g) (Soro et al. 2017). These findings suggest that PAE does not directly affect placental function. The use of resorbable particles and the development of collateral circulation probably ensures sufficient blood supply to the fetus (Soro et al. 2017).

56
Poggi et al. compared the obstetric outcomes of women whose PPH was treated with PAE (n=103) or uterus-sparing surgical interventions (n=189). Subsequent pregnancies were documented in 17/103 (16.5%) women treated with PAE and in 18/189 (9.5%) women treated with surgical methods. They did not find any difference in gestational weeks at the time of delivery or in the birthweight of the fetuses. Four women (23.5%) who were exposed to PAE had recurrent PPH due to placenta accreta. Among the unexposed women, only one (5.5%) had recurrent PPH due to PP and uterine rupture, and no one had placenta accreta. The difference in placenta accreta incidence (23.5% versus 0% p=0.04) was statistically significant. One woman with placenta accreta after PAE also had placenta accreta in her previous pregnancy (Poggi et al. 2015).
The effects of PAE on subsequent pregnancies seem to be minimal (Soro et al. 2017). However, the recurrence rate of AIP in subsequent pregnancies after conservative treatment of AIP has been reported to be around 22 ̶ 29% (Sentilhes et al. 2010b, Provansal et al. 2010). This may lead to recurrent PPH and complications.
Psychological outcomes
Few studies have explored long-term psychological recovery after PAE with contradictory results (Sentilhes et al. 2011, van Stralen et al. 2010, van Stralen et al. 2018).
Van Stralen et al. (2010, 2018) found no long-term effects on quality of life compared to the general population. From 1995 to 2005, van Stralen et al. (2010) conducted their first study, in which 21 women managed with PAE were asked to complete validated questionnaires (STAI, B-IPQ, SCL-90, UCL, RAND). In their second study (2004 ̶2006), 58 women filled out validated questionnaires (RAND-36, B-IPQ) and made drawings of their uteruses 6 ̶ 9 years after the index delivery. In this group, 24 women were managed with PAE and 34 with hysterectomy. After embolization, women seemed to have better quality of life compared to women who had undergone hysterectomy (van Stralen et al. 2018).
Sentilhes et al. used semi-structured telephone interviews to investigate women’s perceptions and memories of the delivery experience. Women were also asked about how their partners experienced the delivery and the postpartum period. Their study included 68 women who underwent PAE for PPH and whose uterus was preserved. They reported major adverse psychological outcomes despite uterine preservation. Two-thirds (67.6%) of the women and one-fifth (19.1%) of their partners reported negative memories. The main negative memory for women was a fear of dying (35%), and for partners, it was having a lack of information. Also, repercussions (41%), sexual problems (5.9%), marital problems (4.4%) and anxiety during uneventful subsequent pregnancies were reported. Altogether, 20.5% of women avoided a subsequent pregnancy because they feared recurrent PPH (Sentilhes et al. 2011).

57
3 AIMS OF THE STUDY
This study was undertaken to determine the effectiveness and safety of BBT and PAE. The long-term effects of IRPs were also determined. One important goal was to evaluate the accuracy of the current screening and follow-up protocols for women with PP.
The specific aims were to evaluate
1. The success rate and safety of BBT in the treatment of PPH in various etiologies (I).
2. The success rate and safety of PAE in women with severe PPH (II).
3. The development of postpartum psychological and physical long-term sequelae in a cohort of women managed with IRPs (III).
4. The obstetric outcomes of women with major or minor PP, and the accuracy of the persisting screening and follow-up protocol for PP (IV).

58
4 MATERIALS AND METHODS
The doctoral dissertation project was undertaken during 2011 ̶ 2019 at Helsinki University Hospital (HUH), a tertiary teaching hospital. The study protocols were approved by the Ethics Committee of HUH (140/13/03/03/2012, 25.4.2012) and the Department of Obstetrics and Gynecology (11.5.2012).
The study population consisted of all women who delivered at HUH during the study period. There were approximately 4500 ̶ 5500 deliveries annually. The study cases were retrospectively and systematically retrieved from hospital registers (Obstetrix and Miranda) using specific interventional codes (Nordic Classification of Surgical Procedures) or diagnosis codes (ICD-10):
- MBB10 uterine tamponade, MBC90 vaginal tamponade (I) - PC7NT endovascular occlusion of uterine arteries to stop puerperal bleeding (II, III) - O44.0 placenta previa without hemorrhage, O44.1 placenta previa with hemorrhage (IV)
Table 7. Summary of the study material
Study Number of cases Study period Source of material
I 50 10/2008 – 6/2011 HUH registry II 45 8/2001 – 4/2011 HUH registry III 73 8/2001 – 4/2011 Questionnaire IV 176 6/2010 – 9/2014 HUH registry
HUH=Helsinki University Hospital
4.1 STUDY I
This study included all women who were managed by BBT after vaginal delivery or after CS during the study period. The following information was collected retrospectively: the women’s baseline characteristics, etiologies of PPH leading to BBT, the amount of hemorrhage before and after BBT, the time the balloon was left in situ, inflation volume of the balloon, the need for additional treatment modalities and complications related to BBT.
BBT was defined as successful if hemostasis was achieved and if no other procedures were needed after BBT.

59
4.2 STUDY II
All women with acute PPH and managed with PAE during the study period were included. Hospital records were retrospectively reviewed to collect data on baseline characteristics and delivery-associated characteristics of the study cohort, etiology and amount of PPH, details about the PAE procedure and the need for additional procedures. The study included women with primary or secondary PPH. PPH was defined as ≥500 ml of hemorrhage after vaginal delivery and ≥1000 ml after CS. Primary PPH was managed according to general guidelines (Figure 4). All necessary conservative and surgical procedures were performed. If bleeding continued despite these procedures, PAE was performed based on the collaborative decision of the obstetrician, anesthesiologist and interventional radiologist.
In every woman, the femoral artery was catheterized and angiography was performed. When the site of bleeding was visible in angiography, selective embolization was attempted. If the bleeding site was not visible or if selective embolization failed, non-selective embolization was performed. Gelatin (Gelita-Spon®, Gelita Medical GmbH, Eberbach, Germany) was the primary embolization agent, but polyvinyl alcohol particles (Bead BlockTM, Terumo EMEA, Leuven, Belgium) and coils (InterlockTM, Boston Scientific Corporation, Natick, MA, USA) were also used.
PAE was considered successful if bleeding stopped, if no re-bleeding occurred and if no other interventions were needed for definitive hemostasis.
4.3 STUDY III
A structured, investigator-made questionnaire was sent to all women who underwent IRP during the study period to try to determine the psychological and physical outcomes after IRP. Women with hysterectomies were included, and therefore, there were two versions of the questionnaire (Appendices I and II). For women whose uterus was preserved, the questionnaire included questions about the menstrual cycle, fertility and further pregnancies after the index pregnancy. Women who had hysterectomy were asked about their experience. Both questionnaires inquired about the quality of life, incidence of psychological problems and the need for psychological support after the stressful delivery. Specific questions focused on the fear of conception, fear of subsequent pregnancy, fear of childbirth, fear of death, problems with intimate relationships and sexual problems. If the questionnaire was not returned within a month, it was sent once more with no further contact. The mean time between delivery and receiving the questionnaire was 72 months (range 25 ̶ 127 months). Women’s baseline characteristics were collected from hospital registers and were linked to answers received from the questionnaires. A long-term problem was defined as one existing longer than six months after delivery.

60
The study cohort included the same women as study II (n=45), but women at high risk for PPH due to anticipated AIP were also included (n=28). Women at high risk for PPH were treated electively with PBO of the iliac arteries. PAE was also performed if needed. These women had antenatal counseling concerning IRP and possible complications.
Women who reported psychological sequelae were compared to women who did not. We tried to determine a single significant factor that could have influenced the development of psychological problems. The tested variables were lack of counseling after delivery, occurrence of physical long-term problems, emergent nature of the IRP procedure, emergency CS as a mode of delivery, hysterectomy, bleeding ≥1500 ml, complications related to delivery management, primiparity, subsequent delivery after the index delivery and history of infertility.
Outcomes of women with an elective IRP and no hysterectomy were compared to all other women of the study cohort. The hypothesis was that this would likely be the group of women with the lowest incidence of long-term psychological problems because they were well-counseled beforehand, had fertility preserved and were able to avoid possible complications related to hysterectomy. Tested variables in this comparison were feeling fully recovered, frequency of psychological long-term problems, overall psychological problems, depression, fear of death, sexual problems, marital problems and lack of aftercare.
A validated questionnaire for PTSD was not used, but the answers were evaluated critically to determine which percentage of women filled the diagnosis criteria for PTSD (Table 4).
4.4 STUDY IV
The study included all women with PP at the time of delivery during the study period. The details of maternal baseline characteristics and pregnancy outcomes were collected retrospectively from the hospital registers. The type of PP (major or minor) was determined by the most recent ultrasound examination. All cases were evaluated to achieve the information about which PPs were diagnosed at the mid-pregnancy screening and which were diagnosed later in pregnancy. Our screening protocol arranged a follow-up after mid-pregnancy only for women whose placenta overlapped the cervix by ≥15 mm. Complications related to PP and the occurrence of hemorrhage were collected.
Obstetric outcomes between women diagnosed with PP at the mid-pregnancy ultrasound screening and those diagnosed later in pregnancy were compared. The rate of women who had PP at term but no follow-up after mid-pregnancy was also determined. Women with major and minor PP were compared to determine if women with major PP have more complications than those with minor PP.

61
4.5 STATISTICAL ANALYSES
In studies III and IV, statistical analyses were performed using the Statistical Package for the Social Sciences Software (IBM Corp., Armonk, New York, USA). A test value of p <0.05 was considered statistically significant. In both studies, Fisher’s exact test or the chi-squared test was used to compare categorical variables between the groups. In study IV, continuous variables were analyzed by the Mann-Whitney U test after the Shapiro-Wilk test evaluation of data normality.

62
5 RESULTS
5.1 BASELINE CHARACTERISTICS OF THE STUDY POPULATION (STUDIES I-̶ IV)
Table 8 describes the characteristics of the whole study population.
Table 8. Baseline characteristics of the women
Characteristic Study I n=50
Study II n=45
Study III1 n=49
Study IV n=176
Age; years (mean) 31.3 (range 19 ̶ 47)
31.2 (range 20 ̶ 40)
32.5 (range 22 ̶ 41)
34.4 (range 22 ̶ 49)
Parity (%) 0 ≥1
60.0 40.0
57.8 42.2
30.6 69.4
35.8 64.2
History of prior cesarean section (%)
12.0
13.3 42.9 26.7
Gestational weeks at the time of delivery (mean)
38+6 39+1 37+2 36+3
Mode of delivery (%) Vaginal Cesarean section Emergency cesarean section2
58.0 42.0 24.0
68.9 31.1 24.4
40.8 59.2 24.1
0.6 99.4 35.2
Total blood loss; ml (mean) 4812 (range 350 ̶16 100)
9315 (range 1500 ̶ 20 000)
6303 (range 100 ̶16 500)
1644 (range 150 ̶12 000)
Peripartum hysterectomy performed (%)
8.0 13.3 36.7 8.5
Abnormally invasive placenta (%) 10.0 13.3 46.9 14.8 1Including only women who returned the questionnaire 2Percentage of all cesarean sections

63
5.2 INDICATIONS, EFFECTIVENESS AND SAFETY OF BAKRI BALLOON TAMPONADE (I)
5.2.1 Indications (I)
The main etiologies of PPH leading to BBT are introduced in Table 9. Two women had two reasons for PPH: uterine atony and paravaginal hematoma. In both cases, uterine atony was managed with uterine compressive sutures and the BB was introduced into the vagina to achieve definitive hemostasis after surgical repair. In two other cases, BBT was used primarily during CS in combination with surgical treatment modalities, one case in combination with uterine compressive sutures and one in combination with uterine artery ligation. Two women were transferred from a local hospital with the BB in situ.
Table 9. Etiology of postpartum hemorrhage in women managed with Bakri balloon tamponade
Etiology n (%) Placental retention 15 (30) Vaginal rupture and/or paravaginal hematoma 11 (22) Placenta previa 9 (18) Uterine atony 8 (16) Cervical rupture 7 (14)
5.2.2 Hemorrhage (I)
The mean amount of total blood loss was 4812 ml (range 350–16 100 ml). Ten women had bleeding ≥5000 ml. Only two women with paravaginal hematomas had total blood loss <1000 ml (350 ml and 880 ml).
Six women had blood loss <1000 ml before BB insertion. Three had paravaginal hematomas, one had uterine atony, one had PP and one had cervical rupture. They all responded poorly to standard treatment, and therefore, the BB was inserted before bleeding exceeded 1000 ml.
The mean blood loss after BB insertion was 525 ml (range 0 ̶ 3250 ml), and 76% of women had bleeding <500 ml after BBT.

64
5.2.3 Technical aspects (I)
The mean inflation volume of the BB was 367 ml (30 ̶ 500 ml). In six women, the BB inflation volume was <250 ml. Five of these six women had PP, and the BB was placed in the lower uterine segment to compress the placental bed. None of the women with an inflation volume <250 ml needed additional treatment. The average time the BB was left in situ was 12.7 hours (range 1 ̶ 28 hours). The BB was expulsed spontaneously in four women, two of which needed no additional treatment. However, in the two other, BB re-insertion failed and hysterectomies were performed. The primary inflation volumes were 250 ml and 200 ml in the failed cases. After expulsion, the inflation volumes were 500 ml in both cases, but additional treatment was still needed.
5.2.4 Success rate and safety (I)
The overall success rate of BBT was 86%. Additional procedures were needed in seven women (Table 10), all of whom had several risk factors for PPH including obesity (n=1), multiparity (n=1), history of curettage (n=2), multiple pregnancy (n=2), stillbirth (n=1), pre-eclampsia (n=3), prolonged pregnancy ≥42 gestational weeks (n=3) and induction of labor (n=4). Altogether, three supravaginal uterine amputations and one hysterectomy were performed. None of the women was primiparous.
Six women had complications unrelated to BBT, including groin hematoma after PAE (n=1), wound infections (n=3), re-curettage and hysteroscopy due to secondary PPH and placental retention (n=2).

65
Table 10. Seven women with Bakri balloon tamponade failure
Etiology of PPH Mode of delivery Additional procedures
Total amount of blood loss (ml)
Atony Emergency CS Bilateral uterine artery embolization
6 900
Atony Emergency CS Uterine compressive sutures, supravaginal uterine amputation
15 000
Atony Emergency CS Supravaginal uterine amputation
12 000
Cervical rupture VD Bilateral uterine artery embolization
5 000
Placental retention VD Bilateral uterine artery embolization
2 000
Placental retention, AIP
VD Supravaginal uterine amputation
6 000
Placental retention, AIP
VD Bilateral uterine artery embolization, hysterectomy
16 100
PPH=postpartum hemorrhage, CS=cesarean section, VD=vaginal delivery, AIP=abnormally invasive placenta

66
5.3 EFFECTIVENESS AND SAFETY OF PELVIC ARTERIAL EMBOLIZATION IN THE TREATMENT OF EMERGENCY POSTPARTUM HEMORRHAGE (II)
5.3.1 Indications (II)
The etiologies of PPH are shown in Table 11. All women had severe PPH (mean 9315 ml) and needed red blood cell transfusions (mean 15.9 units). Lower genital tract injuries included 10 vaginal ruptures or paravaginal hematomas and four cervical ruptures, and four women had both. Almost half the women (44%) did not have obvious risk factors for PPH.
Table 11. Etiology of postpartum hemorrhage
Etiology n (%) Lower genital tract injury 18 (40.0) Placental retention 16 (35.6) Uterine atony 6 (13.3) Placenta previa 2 (4.4) Uterine rupture 1 (2.2) Placental abruption 1 (2.2) Disruption of parametrial adhesions 1 (2.2)
5.3.2 Success rate and safety (II)
The success rate of PAE was 89%. Additional treatment modalities were needed in five women (11%). The etiologies of PPH in these women were AIP (n=3), PP with atony (n=1) and cervical rupture (n=1). The mean amount of blood loss among these women was 13 250 ml. Additional treatment modalities included uterine artery ligation after technical failure of PAE in one woman and hysterectomies in three women. One woman had supravaginal uterine amputation before PAE. Bleeding continued from the cervix after PAE, and the cervix had to be removed to achieve definitive hemostasis.
Altogether, six hysterectomies or supravaginal uterine amputations were performed. In three women, PAE was performed after hysterectomy due to continual bleeding, and in three women, hysterectomy was performed after PAE failure.
Four women (8.9%) had complications related to PAE. There were also several other complications related to PPH and its management. Many women had several complications. All complications are summarized in Table 12.

67
Table 12. Short-term complications after pelvic arterial embolization and postpartum hemorrhage
Complications related to PAE Other complications Rupture of iliac artery during catheterization (n=1)
Postpartum infections: Urinary tract infection (n=2) Pelvic infection (n=9) Wound infection (n=3) Infected intra-abdominal hematoma (n=3) Pneumonia (n=3) Sepsis (n=1)
Inguinal hematoma and pain (n=3) DIC (n=4) Renal dysfunction (n=1) Pulmonary edema (n=4) Retinal ablation (n=1)
Liver laceration (n=1, consequence of resuscitation) Ileus (n=4)
PAE=pelvic arterial embolization, DIC=disseminated intravascular coagulation

68
5.4 PSYCHOLOGICAL AND PHYSICAL OUTCOMES OF WOMEN MANAGED WITH INTERVENTIONAL RADIOLOGY PROCEDURES (III)
The questionnaire was sent to 73 women and was completed by 49 (67%). Acute PPH was found in 27 women (55%), and 22 (45%) were at high risk of PPH due to anticipated AIP. Altogether, 18 women (37%) underwent hysterectomy; five of these women had acute PPH and 13 had an elective procedure. Massive PPH occurred in 86%. All women in the emergency IRP group had massive PPH (mean 8807 ml, range 1500─16 500 ml). In the elective group, 20 women had massive bleeding (4366 ml, range 100 ̶ 15 000 ml).
5.4.1 Psychological outcomes (III)
Psychological sequelae were reported by 63% (n=31) of all women. Nine (18%) fulfilled the criteria of PTSD. The mental symptoms included fear of death, depression, anxiety, problems with relationships and lack of confidence in the health care system in general. Over half the women (67%) described their deliveries as painful, traumatic, chaotic or frightening. Two women reported that the traumatic event contributed to their subsequent divorces. Of those who underwent hysterectomy, six of the 18 (33%) reported it as a major negative experience.
Almost one-third of the women (29%) reported a lack of any aftercare and counseling. Three women were disappointed with their follow-up visits in the maternity unit because the obstetrician who attended their delivery was not present. Fourteen women contacted someone outside the maternity unit (private gynecologist or general practitioner) to get help for their psychological problems. However, 20 women (41%) reported no need for special support during the recovery.
Women with elective IRP and no hysterectomy had less fear of death compared to the rest of the study group (0% versus 45%, p=0.018, OR 1.8, CI 1.4 ̶ 2.4). Otherwise, the outcomes were equal between these groups (including psychological and physical long-term problems, depression, sexual/marital problems and lack of aftercare).
Any specific factors to predict who will develop psychological problems after complicated delivery were not found (Table 13). The amount of hemorrhage, need for hysterectomy or the nature of the IRP did not explain the occurrence of psychological sequelae. Physical symptoms were more common in women who developed psychological sequelae (n=8) than in women who had none (n=1) (25.8% versus 5.6%), but the difference was not statistically significant.

69
Table 13. Psychological outcomes of women managed with interventional radiology procedures due to acute postpartum hemorrhage or anticipated abnormally invasive placenta
Psychological sequelae n=31 (%)
No psychological sequelae n=18 (%)
OR (95% CI) p-value
Parity ≥1 19 (61.3) 15 (83.3) 0.32 (0.075 ̶1.3) 0.107 Infertility before IRP 5 (16.1) 5 (27.8) 0.50 (0.1 ̶ 2.0) 0.329 Elective IRP 12 (38.7) 10 (55.6) 0.51 (0.16 ̶ 1.6) 0.253 Hysterectomy 11 (35.5) 7 (38.9) 0.86 (0.26 ̶ 2.9) 0.812 Bleeding ≥1500 ml 27 (87.1) 15 (83.3) 1.4 (0.27 ̶ 6.9) 0.697 Complications related to delivery management
20 (64.5) 11 (61.1) 1.2 (0.35 ̶ 3.8) 0.812
Emergency cesarean section
5 (16.1) 2 (11.1) 1.5 (0.27 ̶ 8.9) 1.0
Physical long-term problems
8 (25.8) 1 (5.6) 5.9 (0.67 ̶ 52) 0.127
Received counseling after delivery
12 (38.7)
3 (16.7) 3.2 (0.75 ̶ 13) 0.197
IRP=interventional radiology procedure, OR=odds ratio, CI=confidence interval
5.4.2 Physical outcomes (III)
Nine women (18%) reported long-term physical symptoms, including pelvic pain, inguinal pain, pain in the lower limb and dyspareunia. Problems with sexual intercourse were reported by 16 women (33%).
Of the 31 women with a preserved uterus, 19 (61%) reported regular menstrual cycles. Eight women had amenorrhea either due to subsequent hysterectomy (indication menorrhagia, n=2) or an intrauterine hormonal device (n=6). Irregular menstruation was reported by four women, and 11 reported changes in their menstrual patterns following IRP (heavier bleeding n=7, less bleeding n=2, dysmenorrhea n=2) (unpublished data).
Thirteen women had 16 pregnancies, 13 of which were to term (Table 14). None complained of infertility. The mean time to conception was 3.5 months (range <1─18 months). The mean gestational age at delivery was 39+4. All newborns were of normal birth weight (mean 3781 g). Six of the full-term women (46%) feared getting pregnant and reported anxiety and fear during their subsequent pregnancies. PPH recurred in three women (23%), and two of them had placental retention. In women whose uterus was preserved, six of the 31 did not want a new pregnancy because they feared recurrent PPH.

70
Table 14. Pregnancies after pelvic arterial embolization (unpublished data)
Pregnancy Need for ART before/after PAE
Pregnancy outcome
Mode of delivery
Gestational weeks at time of delivery, miscarriage or abortion
Birth weight (g)
Recurrence of PPH
1 no/no D VD 39 3 120 no 2 no/no D VD 39+1 3 240 no 3 no/no D VD 40+2 3 440 no 4 no/no D VD 41 4 370 no 5 yes/yes M 11 6 yes/yes D VD 40 4 200 no 7 yes/yes D VD 40 4 550 yes 8 no/no D CS 39 3 676 no 9 yes/yes not delivered
while returning the questionnaire
10 yes/no D CS 39 3 525 no 11 no/no D VD 41+5 4 425 yes 12 no/no D CS 39 3 360 no 13 no/no D VD 41 3 350 no 14 yes/no D VD 39 3 950 yes 15 no/no A 7 16 no/no D VD 39 3 942 no
ART=artificial reproductive technology, PAE=pelvic arterial embolization, PPH=postpartum hemorrhage, D=delivery, M=miscarriage, A=induced abortion, VD=vaginal delivery, CS=cesarean section

71
5.5 COMPARISON OF OBSTETRIC OUTCOMES BETWEEN WOMEN WITH MAJOR OR MINOR PLACENTA PREVIA (IV)
Among all parturients during the study period, there were 176 women who had a diagnosis of PP at the time of delivery. Altogether, 129 women (73.3%) had major PP and 47 (26.7%) had minor PP. There were no statistical differences between the baseline characteristics (age, parity, risk factors for PP) of women in each group.
Women with major PP had more blood loss at the time of delivery compared to women with minor PP (median 1310 ml versus 850 ml). They also delivered earlier. Otherwise, there were no statistical differences between the groups. The incidence of AIP was also equal (major PP 14.9% versus minor PP 14.7%) (Table 15).

72
Table 15. Comparison between outcomes of women with major or minor placenta previa
PP=placenta previa, OR=odds ratio, CI=confidence interval, IQR=interquartile range, AIP=abnormally invasive placenta, BBT=Bakri balloon tamponade, IRP=interventional radiology procedure
1 Fifteen women had several additional treatment modalities 2Postpartum complications include infections (wound, uterine, pelvic, urinary bladder), urinary bladder laceration, disseminated intravascular coagulation, thrombosis, ileus, re-laparotomy, hysteroscopy due to tamponade balloon rupture 3Comparison between emergency cesarean sections and other modes of delivery
Major PP n=129 (%)
Minor PP n=47 (%)
p-value OR (95% CI)
Gestational age at delivery (d) [median (IQR)] <32 32+0–36+6 ≥37
257 (245 ̶266) 8 (6.2) 60 (46.5) 61 (47.3)
260 (253 ̶268) 1 (2.1) 20 (42.6) 26 (55.3)
0.035 0.430
Mode of delivery Vaginal Cesarean section Elective Emergency
0 88 (68.2) 41 (31.8)
1 (2.1) 25 (53.2) 21 (44.7)
0.061 0.1133
1.7 (0.88 ̶ 3.4)
AIP 19 (14.7) 7 (14.9) 0.978 1.0 (0.40 ̶ 2.6) Blood loss (ml) [median (IQR)] <1500ml 1500–2499ml 2500–4999ml ≥5000ml
1310 (730 ̶ 2000) 68 (52.7) 36 (27.9) 16 (12.4) 9 (7.0)
850 (610 ̶1550) 35 (74.5) 7 (14.9) 3 (6.4) 2 (4.3)
0.032 0.081
Need for additional treatment1
Peripartum hysterectomy Other BBT Uterine artery ligation Uterine compression sutures IRP
47 (36.4) 12 (9.3) 49 (38.0) 34 (26.4) 0 (0) 3 (2.3) 12 (9.3)
12 (25.5) 3 (6.4) 12 (25.5) 9 (19.1) 1 (2.1) 1 (2.1) 1 (2.1)
0.175 0.762 0.125
0.60 (0.28 ̶ 1.3) 0.67 (0.18 ̶ 2.5) 0.56 (0.27 ̶ 1.2)
Postpartum complication2 20 (15.5) 3 (6.4) 0.135 0.37 (0.11 ̶ 1.3)

73
5.6 ACCURACY OF THE SCREENING AND FOLLOW-UP IN WOMEN WITH PLACENTA PREVIA (IV)
There were 32 women (18.2%) with major or minor PP who had no follow-up after the mid-pregnancy screening due to our protocol. The diagnosis of PP was not made until a woman was admitted to the hospital for bleeding (n=29, 90.6%) or for contractions later in pregnancy. Of these 32, 12 (37.5%) had major PP and 20 (62.5%) had minor PP. The first bleeding episode occurred at 37 gestational weeks or later in seven women (21.9%). Five women (15.6%) had a hemorrhage ≥2500 ml at the time of delivery. Two women without follow-up had AIP with a history of prior CS, and both underwent hysterectomy. There were no statistically significant differences between the adverse obstetric outcomes of women with or without follow-up (Table 16).
Table 16. Comparison between women who had PP with or without follow-up after the mid-pregnancy screening
PP without follow-up n=32 (%)
PP with follow-up n=144 (%)
p-value OR (CI 95%)
Gestational age at delivery (d) [median (IQR)] <32 32+0–36+6 ≥37
261 (252 ̶267)
0 13 (40.6) 19 (59.4)
258 (245 ̶266) 9 (6.3) 67 (46.5) 68 (47.2)
0.088 0.225
Blood loss (ml) [median (IQR)]
1050 (650 ̶ 1 763)
1250 (710 ̶ 2 000)
0.343
AIP 2 (6.3) 24 (16.7) 0.173 0.33 (0.075 ̶1.5) Hysterectomy 2 (6.3) 13 (9.0) 1.0 0.67 (0.14 ̶ 3.1) Need for additional treatment
6 (18.8) 53 (36.8) 0.050 0.40 (0.15 ̶ 1.0)
Postpartum complication 1 (3.1) 22 (15.3) 0.082 0.18 (0.023 ̶1.4) PP=placenta previa, OR=odds ratio, CI=confidence interval, IQR=interquartile range, AIP=abnormally invasive placenta

74
5.7 CHARACTERISTICS OF WOMEN WITH ABNORMALLY INVASIVE PLACENTA (I-̶ IV)
Our aim was not to determine the details of women with AIP, but in every study (I ̶IV), AIP played a significant role. The most severe PPH, the need for several treatment modalities, and treatment failures were often related to AIP. An antenatal diagnosis was missed in 39.7% of all AIP cases. Among all women with AIP, 16.2% were primiparous, 25% had AIP without PP and only 63.2% of women with AIP had a previous CS. Characteristics of AIP cases are displayed in Table 17. (unpublished data).
Table 17. Characteristics of women with abnormally invasive placenta (unpublished data)
Study I n (%)
Study II n (%)
Study III1
n (%) Study IV n (%)
AIP 5 (10.0) 6 (13.3) 31 (42.5) 26 (14.8) Antenatal diagnosis of AIP
0 0 25 (80.6) 16 (61.5)
PP 0 0 25 (80.6) 26 (100) Primiparous 2 (40.0) 1 (16.7) 6 (19.4) 2 (7.7) History of prior CS 1 (20.0) 1 (16.7) 23 (74.2) 18 (69.2) Hemorrhage, mean (ml)
8340 (range 5300 ̶ 16 100)
12 025 (range 2200 ̶ 20 000)
6255 (range 100 ̶20 000)
3249 (range 150 ̶12 000)
Hysterectomy or supravaginal uterine amputation
2 (40.0) 2 (33.3) 18 (58.1) 15 (57.7)
Postpartum complication 2 (40.0) 3 (50.0) 21 (67.7) 9 (34.6) AIP=abnormally invasive placenta, PP=placenta previa, CS=cesarean section 1Including all women who received the questionnaire

75
6 DISCUSSION
6.1 IMPORTANCE OF THE STUDY (I ̶ IV)
PPH is a significant contributor to maternal morbidity and mortality worldwide (Waterstone et al. 2001, Say et al. 2014). In low-income countries, the incidence of maternal deaths due to PPH is higher compared to high-income countries, but PPH-related deaths still occur annually in every high-income country (Say et al. 2014, www.stat.fi). Saving mothers’ lives is the most important goal of PPH treatment. Preserving fertility and good quality of life after complicated delivery also plays an increasingly important role, especially in high-income countries. The medical resources and availability of educated obstetricians are often scarce in developing countries, but the opposite is true in high-income countries, where the treatment facilities are usually good. Still, PPH often comes with surprising and difficult surgical procedures like artery ligations or hysterectomies. In Finland, it is mainly the tertiary centers that have specialists available 24 hours a day. In other hospitals, residents mostly take care of parturients, and specialists are at home, 30 minutes from the hospital.
These facts put demands on readily available, easy, safe and effective treatment modalities. The identification of risk factors is also essential in reducing complications. Based on previous literature, the incidence of AIP is increasing in many countries mainly due to increasing numbers of CSs. AIP is often a cause of major complications, especially if not diagnosed antenatally. PP and CS are the main risk factors for AIP, and therefore, screening for PP plays an important role in diagnosing AIP (Jauniaux et al. 2018e, Collins et al. 2019).
Before our study, there were only a few small case series about the effectiveness, indications and safety of BBT in the treatment of PPH (Bakri et al. 2001, Vitthala et al. 2009, Yoong et al. 2012). On the contrary, the effectiveness and safety of PAE were reported in many studies (Lee et al. 2012, Poujade et al. 2012, Mei et al. 2015, Soyer et al. 2015). However, in our hospital, PAE had been used for 10 years without evaluating the effectiveness and safety of our own process. The possible long-term effects of the procedure were not determined. The need to evaluate our screening protocol and follow-up for women with PP arose from the fact that our current protocol was old and the incidence of PP and AIP was increasing worldwide. In addition, previous studies were inconsistent regarding the severity of minor PP and the need for follow-up.

76
6.2 INDICATIONS, EFFECTIVENESS AND SAFETY OF BAKRI BALLOON TAMPONADE (I)
At the time of publication, our case series was the largest published cohort of women managed with BBT. Only a few small case reports were published previously (Bakri et al. 2001, Tattersall et al. 2007, Vitthala et al. 2009, Yoong et al. 2012). In our department, BB usage increased after 2007 (personal communication, Vedran Stefanovic). In 2015, our article became the most cited in the journal Acta Obstetricia et Gynecologica Scandinavica, which suggests the importance and timeliness of the study.
Our results provided new information about BBT in a larger cohort managed in a single tertiary center. The previous studies mostly discussed the treatment of uterine atony and/or placenta previa (Bakri et al. 2001, Vitthala et al. 2009). Tattersall et al. (2007) also reported a single case of vaginal rupture successfully managed with BBT. Our study demonstrated that BBT can be used successfully in various etiologies of PPH, not only in the treatment of uterine atony.
The overall success rate of our study was high at 86%. This is comparable to studies published before and after our own. Recent studies have reported risk factors related to BBT failure, including massive bleeding (≥1500 ml) before BBT, undiagnosed placenta accreta and CS as a mode of delivery (Olsen et al. 2013, Cho et al. 2015, Revert et al. 2017, Mathur et al. 2018, Grange et al. 2018). Our study had similar findings. All seven women with BBT failure had massive hemorrhage (mean 7571 ml); three of the seven (43%) had CS as a mode of delivery and two (29%) had placenta accreta. However, some studies have also reported promising results of BBT in cases of AIP (Pala et al. 2018). In our study, three out of five women (60%) with AIP were managed successfully with BBT.
The mean blood loss was relatively high (4218 ml), and it was even higher in women whose BBT failed to achieve hemostasis. Four women had total blood loss of over 10 000 ml, and three of them had BBT failure. In these cases, it would probably have been better to proceed to other treatment modalities more quickly to avoid the massive bleeding. Our study confirmed that the use of BBT does not exclude the possibility of using other treatment modalities, either simultaneously with the BB or separately after BBT failure. Also, in cases with failure, the BB may provide a temporary tamponade effect as well as time to prepare for other interventions or patient transfer.
Only minimal technical problems are related to BBT. The most common problem reported is spontaneous balloon expulsion before hemostasis achievement (Vintejoux et al. 2015, Soyama et al. 2017). In most cases, re-insertion has been successful without the need for additional procedures. It is still unclear as to whether the inflation volume of the balloon has a major influence on balloon expulsion. The manufacturer’s recommended inflation volume is 500 ml (www.cookmedical.com), although Antony et al. (2017) showed that the BB did not rupture until the inflation volume was 2850 ml. In our study, the mean inflation volume was 367 ml. Four expulsions occurred, leading to hysterectomy in two cases. Both failed cases had re-insertion with

77
500 ml of saline, but hysterectomies were still needed. Further studies are needed to determine if women will benefit from an inflation volume greater than 500 ml. BB expulsion with the recommended inflation volume (500 ml) might also indicate BBT failure.
In addition to BBT, other fertility-preserving methods are PAE, uterine compressive sutures and artery ligations. A comparison of these methods is displayed in Table 18. The success rates of PAE and uterine compressive sutures are reported to be as good as those of BBT (Hackethal et al. 2008, Lee et al. 2012, Poujade et al. 2012, Mei et al. 2015, Soyer et al. 2015). Artery ligations have lower success rates (Camuzcuoglu et al. 2010, Boynukalin et al. 2013). In Finland, PAE is not available at every hospital, and the method demands having an interventional radiologist on site. In our hospital, the patient has to be transferred to another department for PAE. Surgical procedures require laparotomy and advanced surgical skills. Additionally, these procedures have higher risks of complications than BBT (Lee et al. 2012, Boynukalin et al. 2013, Cheong et al. 2014, Soyer et al. 2015, Wei et al. 2016, Soro et al. 2017, Suzuki et al. 2017). In our study, there were no BBT-related complications. These facts argue that BBT should take precedence over other fertility-preserving methods.
Table 18. Comparison between fertility-preserving treatment methods for postpartum hemorrhage
Method Advantages Disadvantages Uterine compressive sutures
Fast Suitable for atony management
with simultaneous use of the Bakri balloon
Requires laparotomy Possible complications:
hematometra, uterine necrosis, bowel incarceration
Pelvic arterial ligation
Fast Requires advanced surgical skills
Requires laparotomy Embolization often not
possible afterwards Pelvic arterial embolization
Identifies small vessels that are not visible by surgery
Requires facilities (often far from the delivery unit)
Not available 24/7 in many hospitals
Bakri balloon tamponade Easy application Suitable for uterine and vaginal
tamponade Suitable during patient transfer Does not require laparotomy Does not exclude the use of
other methods of management
?

78
6.3 EFFECTIVENESS AND SAFETY OF PELVIC ARTERIAL EMBOLIZATION IN THE TREATMENT OF EMERGENCY POSTPARTUM HEMORRHAGE (II)
The good success rate (89%) and safety of PAE were confirmed. The strengths of our study were that all PAEs were performed in a single tertiary center with a constant protocol during a relatively long period (10 years).
Our success rate was comparable to previous studies (Pelage et al. 1999a, Gonsalves et al. 2010, Lee et al. 2012, Poujade et al. 2012, Mei et al. 2015, Soyer et al. 2015). The main difference was the amount of hemorrhage, which was much higher in our study (mean 9315 ml). One explanation for this might be that the interventional radiology operating room is not located in the maternity hospital, and therefore, patients need to be hemodynamically stabilized before transfer. Another explanation is the fact that interventional radiologists are not always immediately on site, for example, on nights or weekends.
The main causes of PPH leading to PAE were genital tract injuries (40.0%) and placental retention (35.6%) in our study, which differs from Lee et al. (2012), whose large study revealed the leading cause to be uterine atony (78.9%), followed by placental retention (9.6%) and lacerations (8.0%). This difference might also be related to the distance between our interventional radiology room and the obstetric unit. For uterine atony, there are other effective treatment options in addition to PAE (BBT, uterine compressive sutures). Especially BBT is used increasingly and successfully in our obstetric unit. BBT is always readily available and does not demand patient transfer, and this may affect the need for PAE in women with uterine atony in our unit. However, PAE has many advantages over surgical interventions in women with lower genital tract injuries. If bleeding continues after surgical reparation of the laceration, the site of bleeding can be detected in angiography and selective embolization can be performed. PAE is often an easier method to achieve definitive hemostasis in these cases.
Several studies have shown that hemodynamic instability, presence of DIC, the need for massive transfusions and the presence of AIP have predicted PAE failure (Lee et al. 2012, Poujade et al. 2012, Kim et al. 2013). In our study, PAE failed in five women, three of which had AIP. The mean amount of blood loss among women with PAE failure was 13 250 ml, which was higher than the mean amount of blood loss in the whole study population. Although our cohort was so small that definitive conclusions could not be reliably made, these results might strengthen the idea that massive bleeding and AIP may implicate the failure of PAE.
Lee et al. (2012) concluded that PAE should be considered early in PPH management and hemodynamic instability should not be a contraindication when the situation is life-threatening. In our study cohort, every woman was hemodynamically stable before transfer to an interventional radiology unit for PAE. Because of our interventional radiology facilities, all possible uterus-preserving surgical and conservative management options were usually performed before proceeding to PAE. In some cases, PAE was performed even after hysterectomy due to continual

79
bleeding. These results showed that, although PAE was not used as a first-line treatment and several women had massive bleeding, many still avoided hysterectomy, and hemostasis was achieved by PAE.
Our complication rate related to PAE was 8.9%, which is slightly higher than Lee et al.’s study (3.2%) (2012). Fortunately, we had only one severe complication (rupture of iliac artery), and no deaths occurred. Lee et al. (2012) reported five (2%) deaths among their large study cohort (n=251). Infections occurred in 33% of women after PAE in our cohort but were unlikely to be the direct result of PAE. Other procedures like curettages, manual removal of placentas and laceration suture probably had a greater impact.

80
6.4 PSYCHOLOGICAL AND PHYSICAL LONG-TERM OUTCOMES OF WOMEN MANAGED WITH INTERVENTIONAL RADIOLOGY PROCEDURES (III)
Our study reported long-term outcomes of women who had experienced exceptionally stressful and complicated deliveries and IRP. Such data cannot be retrieved from hospital databases or registers. That is the main strength of the study.
The primary goal was to determine both physical and psychological long-term effects after IRP, PPH and stressful deliveries. Surprisingly, the main adverse outcomes were psychological, and the physical outcomes did not play as significant a role. Two-thirds of women developed psychological sequelae, but they were not related to the amount of bleeding, whether hysterectomy was performed, or whether IRP was performed electively or in emergency.
Only a few previous studies have reported psychological outcomes after IRP with contradictory results (Sentilhes et al. 2011, van Stralen et al. 2010, van Stralen et al. 2018). Sentilhes et al. reported that 67% of women (n=68) had negative experiences after the management of severe PPH. This is in line with our results. Their cohort did not include women with hysterectomies, and only 43% of the women had massive PPH, strengthening the idea that it is not the volume of bleeding nor the hysterectomy that explains the psychological outcomes (Sentilhes et al. 2011).
Van Stralen et al. reported controversial results. They reported good quality of life after PAE in both of their studies (van Stralen et al. 2010, van Stralen et al. 2018). They compared outcomes of women whose PPH was managed with PAE or with hysterectomy. One of their main findings was that women whose uteruses were preserved had better qualities of life (van Stralen et al. 2018). This is contradictory to our results, although they also concluded that extensive counseling should follow severe PPH, which was also one of our main findings. In our department, aftercare and counseling were clearly inadequate. However, antenatal counseling of women with AIP seemed to be effective because this group of women had less fear of death.
In our study, one-fifth of women filled the criteria for PTSD. A review article published in 2018 showed a probable association between postpartum hysterectomy, PPH and PTSD (Zaat et al. 2018). Another review article reported the incidence of postnatal depression in 13% and the incidence of PTSD in 3% after PPH (Carrol et al. 2016). Women with AIP and anticipated traumatic delivery are also reported to be at increased risk of PTSD (Tol et al. 2019). These results confirm that PTSD does exist after stressful deliveries.
The partners’ perspectives have been studied in a few small studies (Snowdon et al. 2012, Dunning et al. 2016, van Stralen et al. 2018). The main findings have been the inadequacy of information during the delivery and, thus, the powerless feelings of partners. Sexual and marital problems were reported in our study as well as in previous studies (Sentilhes et al. 2011). Dyspareunia may be partly explained by trauma to the birth canal, but psychological aspects may also play a role.

81
PPH has been shown to prevent couples from planning future pregnancies, although several studies have reported relatively good outcomes of subsequent pregnancies after PPH and IRP (Soro et al. 2017). The main fear among women and their partners was recurrent PPH (Soro et al. 2017). The recurrence rate of PPH in subsequent pregnancies after PAE is reported to be 19.2% in Soro et al.’s review (Soro et al. 2017). Our study supports these findings. Poggi et al. (2015) reported an increased risk for AIP after IRP, but this is not in line with our findings. No one in our study had AIP in their subsequent pregnancies. However, it is known that women with AIP are at increased risk (22 ̶29%) of recurrent AIP and complications related to AIP in subsequent pregnancies (Collins et al. 2019).

82
6.5 COMPARISON OF WOMEN WITH MAJOR AND MINOR PLACENTA PREVIA (IV)
The previous literature has reported more adverse obstetric outcomes among women with major PP compared to women with minor PP (Dola et al. 2003, Tuzovic et al. 2006, Bahar et al. 2009, Sekiguchi et al. 2013). The reported adverse outcomes of major PP include a higher incidence and amount of antepartum and postpartum hemorrhage and a higher incidence of preterm deliveries, AIP and hysterectomies. In our study, women with major PP had a slightly greater amount of hemorrhage, as well as a higher incidence of preterm births. However, the incidence of very preterm births (<32 gestational weeks) was similar compared to women with minor PP, and the hemorrhage did not lead to further severe complications or a need for additional treatment modalities in women with major PP.
In our study, the rate of AIP was similar in women with major PP (14.9%) or minor PP (14.7%). Also, the incidence of hysterectomies was similar among these groups (9.3% versus 6.3%, p=0.762). These results are inconsistent with previous studies (Tuzovic et al. 2006, Bahar et al. 2009). The reported rate of AIP among women with major PP was 15.2%, and among women with minor PP, it was 2.9% in Tuzovic et al.’s study, which also revealed that most of the hysterectomies were performed in women with major PP (10.6% versus 0.7%) (Tuzovic et al. 2006). Another study of Bahar et al. (2009) had equal findings; major PP was significantly associated with placenta accreta (OR 3.2, CI 1.22 ̶8.33) and hysterectomies (OR 5.1, CI 1.31 ̶ 19.86).
Women with minor PP had a higher incidence of emergency CSs compared to women with major PP in our study. Pivano et al. showed different reported results. In their study, major PP was one of the main causes leading to emergency CS (Pivano et al. 2015). One explanation for this difference may be that some of the women with minor PP attempted vaginal delivery with the consequence of profuse bleeding and emergency CS.
Based on the results, pregnancies with PP should always be considered as high risk, whether the PP is major or minor. Both are risk factors for massive PPH, AIP and postpartum complications.

83
6.6 ACCURACY OF THE SCREENING AND FOLLOW-UP IN WOMEN WITH PLACENTA PREVIA (IV)
The main finding of this study was that, due to our screening protocol (based on study of Taipale et al. 1998), almost one-fifth of women with major or minor PP at term did not have a follow-up after mid-pregnancy. Almost 40% of these cases had major PP at term, which suggests that a proportion of women with placenta overlapping the cervix by 1 ̶14 mm at mid-pregnancy will still have major PP at term.
Taipale et al. (1998) reported a positive predictive value for PP at the time of delivery to be 19% if the placental edge was ≥15 mm overlapping the cervical os at the mid-pregnancy screening. The sensitivity was 100%. The resolution rate for minor PP has been demonstrated to be as high as 94.8% (Heller et al. 2014). Placental resolution is more likely if the woman does not have a history of prior CS (Lal et al. 2012). In Lal et al. (2012), the placental resolution rate was 61% in women with prior CS and 90% in women without.
There were no statistical differences between the outcomes of women who were diagnosed with PP at the mid-pregnancy screening and those who were not. However, two women without a follow-up and with a history of CS underwent hysterectomy due to hemorrhage and AIP. Additionally, one-fifth of the women without a follow-up did not have the first bleeding episode until 37 gestational weeks. Perhaps these adverse events would have been avoided if the follow-up had been arranged and the diagnosis of PP had been established earlier.
CS is a known risk factor for both PP and AIP. PP is also a major risk factor for AIP. If some of the women with PP do not have a follow-up after mid-pregnancy, we heighten the risk of missing some AIP cases and may therefore see severe complications. We found no difference in AIP rates between major and minor PP, which strengthens the idea that follow-up for women with major and minor PP is equally essential and important. In the Helsinki metropolitan area, the uptake of the prenatal screening program is very high, which also allows systematic screening for PP.

84
6.7 LIMITATIONS (I-̶ IV)
The main limitation of studies I and II is their retrospective nature and lack of predefined control groups. However, randomization is not possible in an emergency situation like PPH. Our study cohorts (I, II) were also relatively small. However, our cohort of 50 women was the largest BBT study when it was published (2013), and women managed with PAE were collected during a relatively long time interval (10 years). Definitive conclusions cannot be made from such small cohorts, but the clinical value of these results is unquestionable.
The overrepresentation of psychological sequelae in study III was not expected. Therefore, data about women’s psychiatric history or their partners’ perspectives were not collected, and the validated questionnaires were not used (for example, quality of life questionnaire [QOL], screening tool for PTSD or questionnaire for depression screening [EPDS]). However, the previous studies also did not often use validated questionnaires, and there are no validated questionnaires for screening specifically for psychological outcomes after stressful deliveries.
The time interval between the index delivery and the study was somewhat long in study III. This could lead to recall bias. However, women still reported traumatic memories many years after the index event, which suggests the severity of the adverse psychological sequelae. Also, the response rate was relatively low (III), which may reflect the negative memories of the stressful event. Due to the low response rate, the study cohort was smaller than we hoped, but it was higher than that of a previous comparable study (31%, van Stralen et al. 2018).
The major limitation of study IV was that not all women who had PP at the time of the mid-pregnancy screening could be retrieved from hospital databases. Women who had placenta <15 mm overlapping the cervix were not diagnosed with PP at mid-pregnancy, and they did not have a follow-up. Some of these women were admitted to the hospital later in pregnancy due to bleeding or other problems, but there are certainly some women who had a marginal or low-lying placenta at term without antenatal complications and with an uneventful delivery. This is the group of women we could not find in hospital databases. The main reason is that the screening ultrasound examinations are mainly performed by midwives, and they do not assess ICD-10 diagnosis codes in patient medical records.

85
6.8 CLINICAL IMPLICATIONS
It was confirmed that the effectiveness of BBT and PAE in the treatment of PPH are not dependent on the etiology of PPH. BBT should be used with low threshold and without delay before bleeding reaches life-threatening volumes. PAE is a good option after other treatment modalities have failed and even after hysterectomy when hemorrhage continues. Every delivery unit should include BBT and, if possible, PAE should also be included in their PPH treatment protocols. BBT and PAE have established a major role in our clinic, and our results also confirmed the safety of these procedures.
Physical long-term outcomes after IRPs seemed to be relatively good. However, after complicated deliveries, adverse psychological outcomes were common, and many women considered aftercare to be inadequate. This strongly suggests a need for better-organized counseling, which should include information about good obstetric outcomes as well as the risks for recurrent PPH and AIP in subsequent pregnancies. Women should also be aware of the high incidence of psychological postpartum problems and should know who to contact if special psychological support is needed. A postpartum counseling protocol for such women should be implemented in every obstetric unit. Counseling before an anticipated complicated delivery is an important and effective way to diminish psychological problems postpartum. There have also been further attempts to improve the antenatal counseling protocol.
Our screening protocol for PP missed a remarkable number of women who still had PP at the time of delivery and left them without a follow-up. This may also lead to undiagnosed AIP cases; thus, PP is one of the major risk factors for AIP. Minor PP proved to be as significant a contributor to obstetric complications as major PP. Our screening protocol was changed after these findings, and all women with major PP and some of the women with minor PP (placenta 0─10 mm from the internal cervical os) are now called for a follow-up ultrasound scan at 32 gestational weeks.

86
6.9 FUTURE ASPECTS
It seems that the prevalence of PP and AIP is increasing and that obstetricians will be faced with such pregnancy complications more frequently. Future research should continue to focus on finding even better antenatal diagnostic tools to recognize these conditions. Patient counseling plays a major role in reducing CS rates for non-medical indications (for example, fear of childbirth). Women should be informed about how CS, especially repeated CS, may influence their future pregnancies and health outcomes. Counseling should be structured and systematic, and current methods of postnatal counseling and screening for adverse psychological outcomes should be evaluated. There is a need to develop a structured questionnaire for women and their partners to evaluate psychiatric outcomes after stressful deliveries. Different antenatal counseling and postnatal debriefing protocols should be tested and outcomes analyzed to find the best methods to prevent adverse obstetric outcomes and psychological sequelae.

87
7 CONCLUSIONS
Based on the studies, the following conclusions can be drawn:
1. BBT is an effective, readily available and safe treatment option for PPH of any etiology. In every obstetric unit, BBT should be included in the first-line PPH treatment protocol.
2. PAE is an effective and safe procedure in the treatment of PPH when other standard procedures have failed. Hysterectomy and other demanding surgical procedures might be avoided in many cases.
3. A high rate of adverse psychological outcomes was associated with complicated deliveries and IRPs. There is a need for systematic aftercare and counseling. Women should be counseled by the obstetrician who attended their delivery. Counseling should include information about fertility, subsequent pregnancy outcomes and possible long-term physical and psychological sequelae. Antenatal counseling for women with AIP has positive effects on reducing the fear of death during pregnancy and delivery.
4. Almost one-fifth of women with major or minor PP went without a follow-up after their mid-
pregnancy screening due to our old screening protocol. Regardless of the type of PP, it is always a high-risk condition and predisposes women to massive PPH and postpartum complications. Both minor and major PP are risk factors for AIP, especially in women with previous CS. The follow-up is essential for both types of PP.

88
8 ACKNOWLEDGMENTS
This study was carried out at the Department of Obstetrics and Gynecology, Helsinki University Hospital, during 2011 ̶ 2019. I want to express my gratitude to the former and present heads of the institution for offering me the chance to perform and finish my thesis project.
My deepest gratitude goes to my supervisors, Adjunct Professor Vedran Stefanovic and Adjunct Professor Minna Tikkanen. They both have given me invaluable guidance in the world of clinical research. I admire their scientific skills. They have always had patience and time for my questions and problems. During the years, their belief in me and in this thesis project has been encouraging, especially in those moments when nothing worked right and the project seemed like it would never end. Vedran, with his effervescent temperament, and Minna, with her preciseness, created an invigorating and balanced atmosphere for discussions and research.
My appreciation also goes to the reviewers of the thesis, Professor Per Olofsson and Adjunct Professor Anne Kuitunen. Their valuable comments and constructive criticism have greatly improved the final version of my thesis, and they also gave me good advice for further research.
I warmly thank Professor Oskari Heikinheimo, Adjunct Professor Jouni Ahonen and Adjunct Professor Jukka Uotila for forming my follow-up group.
I express my gratitude to my co-operators, Professor Jorma Paavonen and Adjunct Professor Mikko Loukovaara. Without their expertise, this project could not have been completed. Jorma’s academic advice and Mikko’s statistical help have been invaluable to my project.
The drawings and cover design of the thesis were created by my dear and talented friend, Katja Saastamoinen. I am very grateful for her.
My sincere appreciation goes to my all colleagues at Kymenlaakso Central Hospital. I have been fortunate to do motivational and challenging clinical work along with my scientifing work in such a positive and encouraging atmosphere. I owe my gratitude to Marja-Liisa Mäntymaa, the former head of the Department of Obstetrics and Gynecology, for supporting my scientific work during these years. My deepest appreciation also goes to Liisa Tikkala, the present head of the department. She has been the most important person for teaching me clinical skills.
I am privileged to have so many dear friends. Without the long conversations, sympathy and hearing me through difficult moments, I would not have survived. I want to deeply thank them all: Anna Jaakola (M.D.), Kristi Juhmen (M.D.), Elina Perälahti (M.D.), Johanna Melin (M.D., Ph.D.), Laura Missuray and Anna Lehtinen. I also want to thank Johanna for the translation of the questionnaires into Swedish.

89
I owe my love to my parents Eeva and Kari Savolainen. They have always believed in me and have taught me to appreciate hard work, perseverance and the academic world. My dad has always said to me, “Tyhjän saa pyytämättäkin.” That sentence has been my brightest guideline through my whole life. I also want to thank Hanna-Kaisa Häsä and Liisa Savolainen for being my brilliant and loving sisters.
Finally, my deepest love and gratitude goes to my husband Ilmari and my sons Aaro, Perttu and Urho. You fill my life with sunshine and thunderstorms. You make me feel alive, you are my everything.
This study was financially supported by Helsinki University Hospital research grants, the Emil Aaltonen Foundation, the Orion Research Foundation SR and the Kymenlaakso Cultural Foundation.
Kotka, March 2020
Maiju Grönvall

90
9 REFERENCES AbdRabbo SA. Stepwise uterine devascularization: A novel technique for management of uncontrolled postpartum hemorrhage with preservation of the uterus. Am J Obstet Gynecol. 1994;171:694 ̶ 700
Abraham C. Bakri balloon placement in the successful management of postpartum hemorrhage in a bicornuate uterus: A case report. Int J Surg Case Rep. 2017;31:218 ̶20
Ahonen J, Stefanovic V, Lassila R. Management of post-partum haemorrhage. Acta Anaesthesiol Scand. 2010;54:1164 ̶ 78
Aibar L, Aguilar MT, Puertas A, Valverde M. Bakri balloon for the management of postpartum hemorrhage. Acta Obstet Gynecol Scand. 2013;92:465 ̶ 7
Ajayi OA, Sant M, Ikhena S, Bako A. Uterine rupture complicating sequential curettage and Bakri balloon tamponade to control secondary PPH. BMJ Case Rep. 2013;2013:10.1136/bcr-007709
Akhter S, Begum MR, Kabir Z, Rashid M, Laila TR, Zabeen F. Use of a condom to control massive postpartum hemorrhage. MedGenMed. 2003;5:38
Al Wadi K, Schneider C, Burym C, Reid G, Hunt J, Menticoglou S. Evaluating the safety of labour in women with a placental edge 11 to 20 mm from the internal cervical Os. J Obstet Gynaecol Can. 2014;36:674 ̶ 7
Alanis M, Hurst BS, Marshburn PB, Matthews ML. Conservative management of placenta increta with selective arterial embolization preserves future fertility and results in a favorable outcome in subsequent pregnancies. Fertil Steril. 2006;86:1514.e3 ̶ 1514.e7
Alexander J, Thomas P, Sanghera J. Treatments for secondary postpartum haemorrhage. Cochrane Database Syst Rev. 2002;(1):CD002867. doi:CD002867
Alkis I, Karaman E, Han A, Ark HC, Buyukkaya B. The fertility sparing management of postpartum hemorrhage: A series of 47 cases of Bakri balloon tamponade. Taiwan J Obstet Gynecol. 2015;54:232 ̶ 5
Allen L, Jauniaux E, Hobson S, Papillon-Smith J, Belfort MA, FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO consensus guidelines on placenta accreta spectrum disorders: Nonconservative surgical management. Int J Gynaecol Obstet. 2018;140:281 ̶ 90
Alouini S, Bedouet L, Ramos A, Ceccaldi C, Evrard ML, Khadre K. Bakri balloon tamponade for severe post-partum haemorrhage: efficiency and fertility outcomes. J Gynecol Obstet Biol Reprod (Paris). 2015;44:171 ̶ 5
American College of Obstetricians and Gynecologists. ACOG committee opinion no. 560: Medically indicated late-preterm and early-term deliveries. Obstet Gynecol. 2013;121:908 ̶ 10

91
American College of Obstetricians and Gynecologists. ACOG Practice Bulletin: Clinical Management Guidelines for Obstetrician-Gynecologists Number 76, October 2006: Postpartum hemorrhage. Obstet Gynecol. 2006;108:1039 ̶ 47
An GH, Ryu HM, Kim MY, Han JY, Chung JH, Kim MH. Outcomes of subsequent pregnancies after uterine compression sutures for postpartum hemorrhage. Obstet Gynecol. 2013;122:565 ̶ 70
Ananth CV, Smulian JC, Vintzileos AM. The effect of placenta previa on neonatal mortality: A population-based study in the United States, 1989 through 1997. Am J Obstet Gynecol. 2003;188:1299 ̶304
Ananth CV, Smulian JC, Vintzileos AM. The association of placenta previa with history of cesarean delivery and abortion: A metaanalysis. Am J Obstet Gynecol. 1997;177:1071 ̶ 8
Antony KM, Racusin DA, Belfort MA, Dildy GA. Under Pressure: Intraluminal Filling Pressures of Postpartum Hemorrhage Tamponade Balloons. AJP Rep. 2017;7:e86 ̶ 92
Ashwal E, Melamed N, Hiersch L, Wiznitzer A, Yogev Y, Peled Y. The incidence and risk factors for retained placenta after vaginal delivery - a single center experience. J Matern Fetal Neonatal Med. 2014;27:1897 ̶ 900
Baba Y, Matsubara S, Ohkuchi A, Usui R, Kuwata T, Suzuki H, Takahashi H, Suzuki M. Anterior placentation as a risk factor for massive hemorrhage during cesarean section in patients with placenta previa. J Obstet Gynaecol Res. 2014;40:1243 ̶ 8
Bahar A, Abusham A, Eskandar M, Sobande A, Alsunaidi M. Risk factors and pregnancy outcome in different types of placenta previa. J Obstet Gynaecol Can. 2009;31:126 ̶31
Bakri YN. Uterine tamponade-drain for hemorrhage secondary to placenta previa-accreta. Int J Gynaecol Obstet. 1992;37:302 ̶ 3.
Bakri YN, Amri A, Abdul Jabbar F. Tamponade-balloon for obstetrical bleeding. Int J Gynaecol Obstet. 2001;74:139 ̶42.
Ballas J, Hull AD, Saenz C, Warshak CR, Roberts AC, Resnik RR, Moore TR, Ramos GA. Preoperative intravascular balloon catheters and surgical outcomes in pregnancies complicated by placenta accreta: A management paradox. Am J Obstet Gynecol. 2012;207:216.e1 ̶ 216.e5.
Barris J. A British Medical Association Lecture on the Diagnosis and Treatment of Placenta Praevia. Br Med J. 1926;2:583 ̶ 6
Bateman BT, Berman MF, Riley LE, Leffert LR. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesth Analg. 2010;110:1368 ̶ 73
Baughman WC, Corteville JE, Shah RR. Placenta accreta: Spectrum of US and MR imaging findings. Radiographics. 2008;28:1905 ̶ 16

92
Baum RA, Baum S. Interventional radiology: A half century of innovation. Radiology. 2014;273:75
Beckmann MM, Chaplin J. Bakri balloon during cesarean delivery for placenta previa. Int J Gynaecol Obstet. 2014;124:118 ̶22
Begley CM, Gyte GM, Devane D, McGuire W, Weeks A, Biesty LM. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2019;(2):CD007412
Belfort MA. Indicated preterm birth for placenta accreta. Semin Perinatol. 2011;35:252 ̶ 6 (b)
Belfort MA, Dildy GA, Garrido J, White GL. Intraluminal pressure in a uterine tamponade balloon is curvilinearly related to the volume of fluid infused. Am J Perinatol. 2011;28:659 ̶ 66 (a)
Benirschke K, Burton GJ, Baergen RN. Pathology of the human placenta. 2012. 6th edition. Springer. New York
B-Lynch C. Partial ischemic necrosis of the uterus following a uterine brace compression suture. BJOG. 2005;112:126 ̶ 7
B-Lynch C, Coker A, Lawal AH, Abu J, Cowen MJ. The B-Lynch surgical technique for the control of massive postpartum haemorrhage: An alternative to hysterectomy? Five cases reported. Br J Obstet Gynaecol. 1997;104:372 ̶ 5
Bose P, Regan F, Paterson-Brown S. Improving the accuracy of estimated blood loss at obstetric haemorrhage using clinical reconstructions. BJOG. 2006;113:919 ̶24
Boynukalin FK, Boyar H, Gormus H, Aral AI, Boyar N. Bilateral hypogastric artery ligation in emergency setting for intractable postpartum hemorrhage: A secondary care center experience. Clin Exp Obstet Gynecol. 2013;40:85 ̶ 8
Bratby MJ, Ramachandran N, Sheppard N, Kyriou J, Munneke GM, Belli AM. Prospective study of elective bilateral versus unilateral femoral arterial puncture for uterine artery embolization. Cardiovasc Intervent Radiol. 2007;30:1139 ̶ 43
Bros S, Chabrot P, Kastler A, Ouchchane L, Cassagnes L, Gallot D, Boyer L. Recurrent bleeding within 24 hours after uterine artery embolization for severe postpartum hemorrhage: Are there predictive factors? Cardiovasc Intervent Radiol. 2012;35:508 ̶14
Brown BJ, Heaston DK, Poulson AM, Gabert HA, Mineau DE, Miller FJ. Uncontrollable postpartum bleeding: A new approach to hemostasis through angiographic arterial embolization. Obstet Gynecol. 1979;54:361 ̶ 5
Brown H, Okeyo S, Mabeya H, Wilkinson J, Schmitt J. The Bakri tamponade balloon as an adjunct treatment for refractory postpartum hemorrhage. Int J Gynaecol Obstet. 2016;135:276 ̶ 80

93
Cali G, Forlani F, Giambanco L, Amico ML, Vallone M, Puccio G, Alio L. Prophylactic use of intravascular balloon catheters in women with placenta accreta, increta and percreta. Eur J Obstet Gynecol Reprod Biol. 2014;179:36 ̶ 41
Callaghan WM, Kuklina EV, Berg CJ. Trends in postpartum hemorrhage: United States, 1994-2006. Am J Obstet Gynecol. 2010;202:353.e1 ̶ 353.e6
Camuzcuoglu H, Toy H, Vural M, Yildiz F, Aydin H. Internal iliac artery ligation for severe postpartum hemorrhage and severe hemorrhage after postpartum hysterectomy. J Obstet Gynaecol Res. 2010;36:538 ̶ 43
Carroli G, Cuesta C, Abalos E, Gulmezoglu AM. Epidemiology of postpartum haemorrhage: A systematic review. Best Pract Res Clin Obstet Gynaecol. 2008;22:999 ̶ 1012
Carroll M, Daly D, Begley CM. The prevalence of women's emotional and physical health problems following a postpartum haemorrhage: A systematic review. BMC Pregnancy Childbirth. 2016;16:261
Cekmez Y, Ozkaya E, Ocal FD, Kucukozkan T. Experience with different techniques for the management of postpartum hemorrhage due to uterine atony: Compression sutures, artery ligation and Bakri balloon. Ir J Med Sci. 2015;184:399 ̶402
Chan C, Razvi K, Tham KF, Arulkumaran S. The use of a Sengstaken-Blakemore tube to control post-partum hemorrhage. Int J Gynaecol Obstet. 1997;58:251 ̶2
Charoenkwan K. Effective use of the Bakri postpartum balloon for posthysterectomy pelvic floor hemorrhage. Am J Obstet Gynecol. 2014;210:586.e1 ̶ 586.e3
Chattopadhyay SK, Deb Roy B, Edrees YB. Surgical control of obstetric hemorrhage: Hypogastric artery ligation or hysterectomy? Int J Gynaecol Obstet. 1990;32:345 ̶51
Chauleur C, Fanget C, Tourne G, Levy R, Larchez C, Seffert P. Serious primary post-partum hemorrhage, arterial embolization and future fertility: A retrospective study of 46 cases. Hum Reprod. 2008;23:1553 ̶9
Chen C, Lee SM, Kim JW, Shin JH. Recent Update of Embolization of Postpartum Hemorrhage. Korean J Radiol. 2018;19:585 ̶ 96
Cheng HC, Pelecanos A, Sekar R. Review of peripartum hysterectomy rates at a tertiary Australian hospital. Aust N Z J Obstet Gynaecol. 2016;56:614 ̶ 8
Cheng HH, Tsang LL, Hsu TY, Kung CT, Ou CY, Chang CD, Tsai CC, Cheng YF, Kung FT. Transcatheter arterial embolization as first-line rescue in intractable primary postpartum hemorrhage: Assessment, outcome, and subsequent fertility. J Formos Med Assoc. 2017;116:380 ̶ 7

94
Cheong JY, Kong TW, Son JH, Won JH, Yang JI, Kim HS. Outcome of pelvic arterial embolization for postpartum hemorrhage: A retrospective review of 117 cases. Obstet Gynecol Sci. 2014;57:17 ̶ 27
Chitragari G, Schlosser FJ, Ochoa Chaar CI, Sumpio BE. Consequences of hypogastric artery ligation, embolization, or coverage. J Vasc Surg. 2015;62:1340,7.e1
Chitrit Y, Zafy S, Pelage JP, Ledref O, Khoury R, Caubel P. Amenorrhea due to partial uterine necrosis after uterine artery embolization for control of refractory postpartum hemorrhage. Eur J Obstet Gynecol Reprod Biol. 2006;127:140 ̶2
Cho HY, Park YW, Kim YH, Jung I, Kwon JY. Efficacy of Intrauterine Bakri Balloon Tamponade in Cesarean Section for Placenta Previa Patients. PLoS One. 2015;10:e0134282
Cho JH, Jun HS, Lee CN. Hemostatic suturing technique for uterine bleeding during cesarean delivery. Obstet Gynecol. 2000;96:129 ̶ 31
Cho YJ, Oh YT, Kim SY, Kim JY, Jung SY, Chon SJ, Kim JH, Byun SS. The efficacy of pre-delivery prophylactic trans-catheter arterial balloon occlusion of bilateral internal iliac artery in patients with suspected placental adhesion. Obstet Gynecol Sci. 2017;60:18 ̶ 25
Christianson LM, Bovbjerg VE, McDavitt EC, Hullfish KL. Risk factors for perineal injury during delivery. Am J Obstet Gynecol. 2003;189:255 ̶ 60
Clark SL, Phelan JP, Yeh SY, Bruce SR, Paul RH. Hypogastric artery ligation for obstetric hemorrhage. Obstet Gynecol. 1985;66:353 ̶ 6
Collins SL, Alemdar B, van Beekhuizen HJ, Bertholdt C, Braun T, Calda P, Delorme P, Duvekot JJ, Gronbeck L, Kayem G, Langhoff-Roos J, Marcellin L, Martinelli P, Morel O, Mhallem M, Morlando M, Noergaard LN, Nonnenmacher A, Pateisky P, Petit P, Rijken MJ, Ropacka-Lesiak M, Schlembach D, Sentilhes L, Stefanovic V, Strindfors G, Tutschek B, Vangen S, Weichert A, Weizsacker K, Chantraine F, International Society for Abnormally Invasive Placenta, (IS-AIP). Evidence-based guidelines for the management of abnormally invasive placenta: Recommendations from the International Society for Abnormally Invasive Placenta. Am J Obstet Gynecol. 2019;220:511 ̶ 26
Collins SL, Ashcroft A, Braun T, Calda P, Langhoff-Roos J, Morel O, Stefanovic V, Tutschek B, Chantraine F, European Working Group on Abnormally Invasive Placenta, (EW-AIP). Proposal for standardized ultrasound descriptors of abnormally invasive placenta (AIP). Ultrasound Obstet Gynecol. 2016;47:271 ̶ 5
Combs CA, Laros RK. Prolonged third stage of labor: morbidity and risk factors. Obstet Gynecol. 1991;77:863 ̶ 7 (b)
Combs CA, Murphy EL, Laros RK. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol. 1991;77:69 ̶ 76 (a)

95
Committee on Practice Bulletins-Obstetrics. ACOG Practice Bulletin No. 198: Prevention and Management of Obstetric Lacerations at Vaginal Delivery. Obstet Gynecol. 2018;132:e87-e102
Committee on Practice Bulletins-Obstetrics. Practice Bulletin No. 183: Postpartum Hemorrhage. Obstet Gynecol. 2017;130:e168 ̶ e86
Copland JA, Craw SM, Herbison P. Low-lying placenta: Who should be recalled for a follow-up scan? J Med Imaging Radiat Oncol. 2012;56:158 ̶ 62
Cordonnier C, Ha-Vien DE, Depret S, Houfflin-Debarge V, Provost N, Subtil D. Foetal growth restriction in the next pregnancy after uterine artery embolisation for post-partum haemorrhage. Eur J Obstet Gynecol Reprod Biol. 2002;103:183 ̶4
Cottier JP, Fignon A, Tranquart F, Herbreteau D. Uterine necrosis after arterial embolization for postpartum hemorrhage. Obstet Gynecol. 2002;100:1074 ̶ 7
Coviello EM, Grantz KL, Huang CC, Kelly TE, Landy HJ. Risk factors for retained placenta. Am J Obstet Gynecol. 2015;213:864.e1 ̶ 864.e11.
Creanga AA, Syverson C, Seed K, Callaghan WM. Pregnancy-Related Mortality in the United States, 2011-2013. Obstet Gynecol. 2017;130:366 ̶73
Dahlke JD, Mendez-Figueroa H, Maggio L, Hauspurg AK, Sperling JD, Chauhan SP, Rouse DJ. Prevention and management of postpartum hemorrhage: A comparison of 4 national guidelines. Am J Obstet Gynecol. 2015;213:76.e1 ̶ 76.e10
Das R, Champaneria R, Daniels JP, Belli AM. Comparison of embolic agents used in uterine artery embolisation: A systematic review and meta-analysis. Cardiovasc Intervent Radiol. 2014;37:1179 ̶ 90
Dashe JS. Toward consistent terminology of placental location. Semin Perinatol. 2013;37:375 ̶9
de la Cruz CZ, Coulter M, O'Rourke K, Mbah AK, Salihu HM. Post-traumatic stress disorder following emergency peripartum hysterectomy. Arch Gynecol Obstet. 2016;294:681 ̶ 8
De Loor JA, van Dam PA. Foley catheters for uncontrollable obstetric or gynecologic hemorrhage. Obstet Gynecol. 1996;88:737 ̶ 5
Delotte J, Novellas S, Koh C, Bongain A, Chevallier P. Obstetrical prognosis and pregnancy outcome following pelvic arterial embolisation for post-partum hemorrhage. Eur J Obstet Gynecol Reprod Biol. 2009;145:129 ̶ 32
Deneux-Tharaux C, Macfarlane A, Winter C, Zhang WH, Alexander S, Bouvier-Colle MH, EUPHRATES Group. Policies for manual removal of placenta at vaginal delivery: Variations in timing within Europe. BJOG. 2009;116:119 ̶24

96
Diemert A, Ortmeyer G, Hollwitz B, Lotz M, Somville T, Glosemeyer P, Diehl W, Hecher K. The combination of intrauterine balloon tamponade and the B-Lynch procedure for the treatment of severe postpartum hemorrhage. Am J Obstet Gynecol. 2012;206:65.e1 ̶ 65.e4
Dildy GA, Belfort MA, Adair CD, Destefano K, Robinson D, Lam G, Strong TH, Polon C, Massaro R, Bukkapatnam J, Van Hook JW, Kassis I, Sunderji S, ebb Surveillance Study Team. Initial experience with a dual-balloon catheter for the management of postpartum hemorrhage. Am J Obstet Gynecol. 2014;210:136.e1 ̶ 136.e6
Dilla AJ, Waters JH, Yazer MH. Clinical validation of risk stratification criteria for peripartum hemorrhage. Obstet Gynecol. 2013;122:120 ̶ 6
Dohan A, Soyer P, Subhani A, Hequet D, Fargeaudou Y, Morel O, Boudiaf M, Gayat E, Barranger E, Le Dref O, Sirol M. Postpartum hemorrhage resulting from pelvic pseudoaneurysm: A retrospective analysis of 588 consecutive cases treated by arterial embolization. Cardiovasc Intervent Radiol. 2013;36:1247 ̶ 55
Dola CP, Garite TJ, Dowling DD, Friend D, Ahdoot D, Asrat T. Placenta previa: Does its type affect pregnancy outcome? Am J Perinatol. 2003;20:353 ̶ 60
Doumouchtsis SK, Nikolopoulos K, Talaulikar V, Krishna A, Arulkumaran S. Menstrual and fertility outcomes following the surgical management of postpartum haemorrhage: A systematic review. BJOG. 2014;121:382 ̶ 8
Driessen M, Bouvier-Colle MH, Dupont C, Khoshnood B, Rudigoz RC, Deneux-Tharaux C, Pithagore6 Group. Postpartum hemorrhage resulting from uterine atony after vaginal delivery: Factors associated with severity. Obstet Gynecol. 2011;117:21 ̶ 31
Dunning T, Harris JM, Sandall J. Women and their birth partners' experiences following a primary postpartum haemorrhage: A qualitative study. BMC Pregnancy Childbirth. 2016;16:80 ̶ 7
Eastman NJ. Williams Obstetrics. 1950. 10th edition. Appleton-Century-Crofts. New York
Eckerdal P, Kollia N, Lofblad J, Hellgren C, Karlsson L, Hogberg U, Wikstrom AK, Skalkidou A. Delineating the Association between Heavy Postpartum Haemorrhage and Postpartum Depression. PLoS One. 2016;11:e0144274
Elmir R, Schmied V, Jackson D, Wilkes L. Between life and death: women's experiences of coming close to death, and surviving a severe postpartum haemorrhage and emergency hysterectomy. Midwifery. 2012;28:228 ̶ 35
Endler M, Saltvedt S, Cnattingius S, Stephansson O, Wikstrom AK. Retained placenta is associated with pre-eclampsia, stillbirth, giving birth to a small-for-gestational-age infant, and spontaneous preterm birth: A national register-based study. BJOG. 2014;121:1462 ̶70

97
Erez O, Novack L, Beer-Weisel R, Dukler D, Press F, Zlotnik A, Than NG, Tomer A, Mazor M. DIC score in pregnant women - a population based modification of the International Society on Thrombosis and Hemostasis score. PLoS One. 2014;9:e93240
Eriksson LG, Mulic-Lutvica A, Jangland L, Nyman R. Massive postpartum hemorrhage treated with transcatheter arterial embolization: technical aspects and long-term effects on fertility and menstrual cycle. Acta Radiol. 2007;48:635 ̶ 42
Evensen A, Anderson JM, Fontaine P. Postpartum Hemorrhage: Prevention and Treatment. Am Fam Physician. 2017;95:442 ̶ 9
Fargeaudou Y, Soyer P, Morel O, Sirol M, le Dref O, Boudiaf M, Dahan H, Rymer R. Severe primary postpartum hemorrhage due to genital tract laceration after operative vaginal delivery: Successful treatment with transcatheter arterial embolization. Eur Radiol. 2009;19:2197 ̶203
Farquhar CM, Li Z, Lensen S, McLintock C, Pollock W, Peek MJ, Ellwood D, Knight M, Homer CS, Vaughan G, Wang A, Sullivan E. Incidence, risk factors and perinatal outcomes for placenta accreta in Australia and New Zealand: A case-control study. BMJ Open. 2017;7:e017713
Feng S, Liao Z, Huang H. Effect of prophylactic placement of internal iliac artery balloon catheters on outcomes of women with placenta accreta: An impact study. Anaesthesia. 2017;72:853 ̶ 8
Fiori O, Deux JF, Kambale JC, Uzan S, Bougdhene F, Berkane N. Impact of pelvic arterial embolization for intractable postpartum hemorrhage on fertility. Am J Obstet Gynecol. 2009;200:384.e1 ̶ 384.e4
Fitzpatrick KE, Sellers S, Spark P, Kurinczuk JJ, Brocklehurst P, Knight M. The management and outcomes of placenta accreta, increta, and percreta in the UK: A population-based descriptive study. BJOG. 2014;121:62 ̶ 70
Fox KA, Shamshirsaz AA, Carusi D, Secord AA, Lee P, Turan OM, Huls C, Abuhamad A, Simhan H, Barton J, Wright J, Silver R, Belfort MA. Conservative management of morbidly adherent placenta: Expert review. Am J Obstet Gynecol. 2015;213:755 ̶ 60
Gaia G, Chabrot P, Cassagnes L, Calcagno A, Gallot D, Botchorishvili R, Canis M, Mage G, Boyer L. Menses recovery and fertility after artery embolization for PPH: A single-center retrospective observational study. Eur Radiol. 2009;19:481 ̶7
Gallos ID, Williams HM, Price MJ, Merriel A, Gee H, Lissauer D, Moorthy V, Tobias A, Deeks JJ, Widmer M, Tuncalp O, Gulmezoglu AM, Hofmeyr GJ, Coomarasamy A. Uterotonic agents for preventing postpartum haemorrhage: A network meta-analysis. Cochrane Database Syst Rev. 2018;(4):CD011689
Georgiou C. Menses, fertility and pregnancy following the use of balloon tamponade technology in the management of postpartum haemorrhage. Aust N Z J Obstet Gynaecol. 2014;54:287 ̶ 90

98
Georgiou C. Intraluminal pressure readings during the establishment of a positive 'tamponade test' in the management of postpartum haemorrhage. BJOG. 2010;117:295 ̶ 303
Gibbs R, Karlan B, Haney A, Nygaard I. Danfort’s Obstetrics and Gynecology. 2008. 10th edition. Lippincott Williams & Wilkins, a Wolters Kluwer business. Philadelphia
Gilstrap LC, Ramin SM. Postpartum hemorrhage. Clin Obstet Gynecol. 1994;37:824 ̶ 30
Gizzo S, Saccardi C, Patrelli TS, Di Gangi S, D'Antona D, Battista Nardelli G. Bakri balloon in vaginal-perineal hematomas complicating vaginal delivery: A new therapeutic approach. J Low Genit Tract Dis. 2013;17:125 ̶8
Gonsalves M, Belli A. The role of interventional radiology in obstetric hemorrhage. Cardiovasc Intervent Radiol. 2010;33:887 ̶ 95
Grange J, Chatellier M, Cheve MT, Paumier A, Launay-Bourillon C, Legendre G, Olivier M, Ducarme G. Predictors of failed intrauterine balloon tamponade for persistent postpartum hemorrhage after vaginal delivery. PLoS One. 2018;13:e0206663
Greenbaum S, Wainstock T, Dukler D, Leron E, Erez O. Underlying mechanisms of retained placenta: Evidence from a population based cohort study. Eur J Obstet Gynecol Reprod Biol. 2017;216:12 ̶ 7
Guo Y, Hua R, Bian S, Xie X, Ma J, Cai Y, Sooranna SR, Cheng W. Intrauterine Bakri Balloon and Vaginal Tamponade Combined with Abdominal Compression for the Management of Postpartum Hemorrhage. J Obstet Gynaecol Can. 2018;40:561 ̶ 5
Hackethal A, Brueggmann D, Oehmke F, Tinneberg HR, Zygmunt MT, Muenstedt K. Uterine compression U-sutures in primary postpartum hemorrhage after Cesarean section: Fertility preservation with a simple and effective technique. Hum Reprod. 2008;23:74 ̶ 9
Handler AS, Mason ED, Rosenberg DL, Davis FG. The relationship between exposure during pregnancy to cigarette smoking and cocaine use and placenta previa. Am J Obstet Gynecol. 1994;170:884 ̶ 9
Hardeman S, Decroisette E, Marin B, Vincelot A, Aubard Y, Pouquet M, Maubon A. Fertility after embolization of the uterine arteries to treat obstetrical hemorrhage: A review of 53 cases. Fertil Steril. 2010;94:2574 ̶9
Hayman RG, Arulkumaran S, Steer PJ. Uterine compression sutures: surgical management of postpartum hemorrhage. Obstet Gynecol. 2002;99:502 ̶ 6
Heller HT, Mullen KM, Gordon RW, Reiss RE, Benson CB. Outcomes of pregnancies with a low-lying placenta diagnosed on second-trimester sonography. J Ultrasound Med. 2014;33:691 ̶6

99
Higgins MF, Monteith C, Foley M, O'Herlihy C. Real increasing incidence of hysterectomy for placenta accreta following previous caesarean section. Eur J Obstet Gynecol Reprod Biol. 2013;171:54 ̶ 6
Hofmeyr GJ, Abdel-Aleem H, Abdel-Aleem MA. Uterine massage for preventing postpartum haemorrhage. Cochrane Database Syst Rev. 2013;(7):CD006431 (b)
Hofmeyr GJ, Gulmezoglu AM, Novikova N, Lawrie TA. Postpartum misoprostol for preventing maternal mortality and morbidity. Cochrane Database Syst Rev. 2013;(7):CD008982 (a)
Hofmeyr GJ, Mshweshwe NT, Gulmezoglu AM. Controlled cord traction for the third stage of labour. Cochrane Database Syst Rev. 2015;(1):CD008020
Hwu YM, Chen CP, Chen HS, Su TH. Parallel vertical compression sutures: A technique to control bleeding from placenta praevia or accreta during caesarean section. BJOG. 2005;112:1420 ̶ 3
Ida A, Ito K, Kubota Y, Nosaka M, Kato H, Tsuji Y. Successful reduction of acute puerperal uterine inversion with the use of a bakri postpartum balloon. Case Rep Obstet Gynecol. 2015;2015:424891
Iwata A, Murayama Y, Itakura A, Baba K, Seki H, Takeda S. Limitations of internal iliac artery ligation for the reduction of intraoperative hemorrhage during cesarean hysterectomy in cases of placenta previa accreta. J Obstet Gynaecol Res. 2010;36:254 ̶9
Jauniaux E, Alfirevic Z, Bhide AG, Belfort MA, Burton GJ, Collins SL, Dornan S, Jurkovic D, Kayem G, Kingdom J, Silver R, Sentilhes L, Royal College of Obstetricians and Gynaecologists. Placenta Praevia and Placenta Accreta: Diagnosis and Management: Green-top Guideline No. 27a. BJOG. 2018;126:e1 ̶ e48 (d)
Jauniaux E, Ayres-de-Campos D, FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO consensus guidelines on placenta accreta spectrum disorders: Introduction. Int J Gynaecol Obstet. 2018;140:261 ̶4 (a)
Jauniaux E, Bhide A. Prenatal ultrasound diagnosis and outcome of placenta previa accreta after cesarean delivery: A systematic review and meta-analysis. Am J Obstet Gynecol. 2017;217:27 ̶ 36
Jauniaux E, Bhide A, Kennedy A, Woodward P, Hubinont C, Collins S, FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO consensus guidelines on placenta accreta spectrum disorders: Prenatal diagnosis and screening. Int J Gynaecol Obstet. 2018;140:274 ̶ 80 (e)
Jauniaux E, Campbell S. Ultrasonographic assessment of placental abnormalities. Am J Obstet Gynecol. 1990;163:1650 ̶ 8
Jauniaux E, Chantraine F, Silver RM, Langhoff-Roos J, FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO consensus guidelines on placenta accreta spectrum disorders: Epidemiology. Int J Gynaecol Obstet. 2018;140:265 ̶ 73 (c)

100
Jauniaux E, Collins S, Burton GJ. Placenta accreta spectrum: Pathophysiology and evidence-based anatomy for prenatal ultrasound imaging. Am J Obstet Gynecol. 2018;218:75 ̶ 87 (b)
Johanson R, Kumar M, Obhrai M, Young P. Management of massive postpartum haemorrhage: Use of a hydrostatic balloon catheter to avoid laparotomy. BJOG. 2001;108:420 ̶ 2
Joshi VM, Otiv SR, Majumder R, Nikam YA, Shrivastava M. Internal iliac artery ligation for arresting postpartum haemorrhage. BJOG. 2007;114:356 ̶ 61
Joshi VM, Shrivastava M. Partial ischemic necrosis of the uterus following a uterine brace compression suture. BJOG. 2004;111:279 ̶ 80
Kanematsu M, Watanabe H, Kondo H, Goshima S, Kato H, Furui T, Toyoki H, Morishige K. Postpartum hemorrhage in coagulopathic patients: preliminary experience with uterine arterial embolization with N-butyl cyanoacrylate. J Vasc Interv Radiol. 2011;22:1773 ̶ 6
Kapoor S, Thomas JT, Petersen SG, Gardener GJ. Is the third trimester repeat ultrasound scan for placental localisation needed if the placenta is low lying but clear of the os at the mid-trimester morphology scan? Aust N Z J Obstet Gynaecol. 2014;54:428 ̶32
Karami M, Jenabi E, Fereidooni B. The association of placenta previa and assisted reproductive techniques: A meta-analysis. J Matern Fetal Neonatal Med. 2018;31:1940 ̶7
Kaufman C, Tadros A. Endovascular Interventions for the Morbidly Adherent Placenta. J Clin Med. 2018;7:10.3390/jcm7050092
Kavak SB, Atilgan R, Demirel I, Celik E, Ilhan R, Sapmaz E. Endouterine hemostatic square suture vs. Bakri balloon tamponade for intractable hemorrhage due to complete placenta previa. J Perinat Med. 2013;41:705 ̶ 9
Kaya B, Guralp O, Tuten A, Unal O, Celik MO, Dogan A. Which uterine sparing technique should be used for uterine atony during cesarean section? The Bakri balloon or the B-Lynch suture? Arch Gynecol Obstet. 2016;294:511 ̶ 7
Kaya B, Tuten A, Celik H, Misirlioglu M, Unal O. Non-invasive management of acute recurrent puerperal uterine inversion with Bakri postpartum balloon. Arch Gynecol Obstet. 2014;289:695 ̶ 6 (a)
Kaya B, Tuten A, Daglar K, Misirlioglu M, Polat M, Yildirim Y, Unal O, Kilic GS, Guralp O. Balloon tamponade for the management of postpartum uterine hemorrhage. J Perinat Med. 2014;42:745 ̶ 53 (b)
Kim JE, So YH, Kim BJ, Kim SM, Choi YH, Sung CK. Postpartum hemorrhage from non-uterine arteries: Clinical importance of their detection and the results of selective embolization. Acta Radiol. 2018;59:932 ̶8

101
Kim YJ, Yoon CJ, Seong NJ, Kang SG, An SW, Kim YS, Woo YN. Failed pelvic arterial embolization for postpartum hemorrhage: Clinical outcomes and predictive factors. J Vasc Interv Radiol. 2013;24:703 ̶ 9
King DL. Placental migration demonstrated by ultrasonography. A hypothesis of dynamic placentation. Radiology. 1973;109:167 ̶ 70
Klar M, Laub M, Schulte-Moenting J, Proempeler H, Kunze M. Clinical risk factors for complete and partial placental retention - a case-control study. J Perinat Med. 2013;41:529 ̶ 34
Kong CW, To WWK. Intraluminal pressure of uterine balloon tamponade in the management of severe post-partum hemorrhage. J Obstet Gynaecol Res. 2018;44:914 ̶ 21 (a)
Kong CW, To WWK. Menstrual and reproductive outcomes after use of balloon tamponade for severe postpartum hemorrhage. BMC Pregnancy Childbirth. 2018;18:451 ̶6 (b)
Kong MC, To WW. Balloon tamponade for postpartum haemorrhage: Case series and literature review. Hong Kong Med J. 2013;19:484 ̶ 90
Kruithof EK, Tran-Thang C, Gudinchet A, Hauert J, Nicoloso G, Genton C, Welti H, Bachmann F. Fibrinolysis in pregnancy: A study of plasminogen activator inhibitors. Blood. 1987;69:460 ̶6
Kumru P, Demirci O, Erdogdu E, Arisoy R, Ertekin AA, Tugrul S, Pekin O. The Bakri balloon for the management of postpartum hemorrhage in cases with placenta previa. Eur J Obstet Gynecol Reprod Biol. 2013;167:167 ̶ 70
Kutuk MS, Ak M, Ozgun MT. Leaving the placenta in situ versus conservative and radical surgery in the treatment of placenta accreta spectrum disorders. Int J Gynaecol Obstet. 2018;140:338 ̶ 44
Laas E, Bui C, Popowski T, Mbaku OM, Rozenberg P. Trends in the rate of invasive procedures after the addition of the intrauterine tamponade test to a protocol for management of severe postpartum hemorrhage. Am J Obstet Gynecol. 2012;207:281.e1 ̶ 281.e7
Lal AK, Hibbard JU. Placenta previa: an outcome-based cohort study in a contemporary obstetric population. Arch Gynecol Obstet. 2015;292:299 ̶ 305
Lal AK, Nyholm J, Wax J, Rose CH, Watson WJ. Resolution of complete placenta previa: Does prior cesarean delivery matter? J Ultrasound Med. 2012;31:577 ̶ 80
Lee HY, Shin JH, Kim J, Yoon HK, Ko GY, Won HS, Gwon DI, Kim JH, Cho KS, Sung KB. Primary postpartum hemorrhage: Outcome of pelvic arterial embolization in 251 patients at a single institution. Radiology. 2012;264:903 ̶9
Lee SM, Shin JH, Shim JJ, Yoon KW, Cho YJ, Kim JW, Ko HK. Postpartum haemorrhage due to genital tract injury after vaginal delivery: Safety and efficacy of transcatheter arterial embolisation. Eur Radiol. 2018;28:4800 ̶ 9

102
Leleup G, Fohlen A, Dohan A, Bryan-Rest L, Le Pennec V, Limot O, Le Dref O, Soyer P, Pelage JP. Value of Round Ligament Artery Embolization in the Management of Postpartum Hemorrhage. J Vasc Interv Radiol. 2017;28:696 ̶ 701
Leparco S, Viot A, Benachi A, Deffieux X. Migration of Bakri balloon through an unsuspected uterine perforation during the treatment of secondary postpartum hemorrhage. Am J Obstet Gynecol. 2013;208:6
Lo A, St Marie P, Yadav P, Belisle E, Markenson G. The impact of Bakri balloon tamponade on the rate of postpartum hysterectomy for uterine atony. J Matern Fetal Neonatal Med. 2017;30:1163 ̶ 6
Lyndon A, Lagrew D, Shields L, Main E, Cape V. Improving health care response to obstetric hemorrhage. (California maternal quality care collaborative toolkit to transform maternity care) Developed under contract #11-10006 with the California Department of Public Health; Maternal, child and adolescent health division; Published by the California maternal quality care collaborative, 3/17/15
Magann EF, Evans S, Chauhan SP, Lanneau G, Fisk AD, Morrison JC. The length of the third stage of labor and the risk of postpartum hemorrhage. Obstet Gynecol. 2005;105:290 ̶ 3
Maher MA, Abdelaziz A. Comparison between two management protocols for postpartum hemorrhage during cesarean section in placenta previa: Balloon protocol versus non-balloon protocol. J Obstet Gynaecol Res. 2017;43:447 ̶ 55
Martin E, Legendre G, Bouet PE, Cheve MT, Multon O, Sentilhes L. Maternal outcomes after uterine balloon tamponade for postpartum hemorrhage. Acta Obstet Gynecol Scand. 2015;94:399 ̶ 404
Mathur M, Ng QJ, Tagore S. Use of Bakri balloon tamponade (BBT) for conservative management of postpartum haemorrhage: A tertiary referral centre case series. J Obstet Gynaecol. 2018;38:66 ̶ 70
Mavrides E, Allard S, Chandraharan E, Collins P, Green L, Hunt BJ, Riris S, Thomson AJ on behalf of The Royal College of Obstetricians and Gynaecologists. Prevention and management of postpartum hemorrhage. BJOG. 2016;124:e106 ̶ 49
Mei J, Wang Y, Zou B, Hou Y, Ma T, Chen M, Xie L. Systematic review of uterus-preserving treatment modalities for abnormally invasive placenta. J Obstet Gynaecol. 2015;35:777 ̶ 82
Menard MK, Main EK, Currigan SM. Executive summary of the reVITALize initiative: Standardizing obstetric data definitions. Obstet Gynecol. 2014;124:150 ̶3
Merriam AA, Wright JD, Siddiq Z, D'Alton ME, Friedman AM, Ananth CV, Bateman BT. Risk for postpartum hemorrhage, transfusion, and hemorrhage-related morbidity at low, moderate, and high volume hospitals. J Matern Fetal Neonatal Med. 2018;31:1025 ̶34

103
Miller CM, Cohn S, Akdagli S, Carvalho B, Blumenfeld YJ, Butwick AJ. Postpartum hemorrhage following vaginal delivery: Risk factors and maternal outcomes. J Perinatol. 2017;37:243 ̶ 8
Miller DA, Chollet JA, Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997;177:210 ̶ 4
Ministry of social affairs and health, prenatal screening, https://stm.fi/en/prenatal-screening
Morlando M, Sarno L, Napolitano R, Capone A, Tessitore G, Maruotti GM, Martinelli P. Placenta accreta: Incidence and risk factors in an area with a particularly high rate of cesarean section. Acta Obstet Gynecol Scand. 2013;92:457 ̶60
Mousa HA, Walkinshaw S. Major postpartum haemorrhage. Curr Opin Obstet Gynecol. 2001;13:595 ̶ 603
Nagai S, Kobayashi H, Nagata T, Hiwatashi S, Kawamura T, Yokomine D, Orita Y, Oki T, Yoshinaga M, Douchi T. Clinical Usefulness of Bakri Balloon Tamponade in the Treatment of Massive Postpartum Uterine Hemorrhage. Kurume Med J. 2016;62:17 ̶21
Nakamura M, Hasegawa J, Matsuaka R, Mimura T, Ichizuka K, Sekizawa A, Okai T. Amount of hemorrhage during vaginal delivery correlates with length from placental edge to external os in cases with low-lying placenta whose length between placental edge and internal os was 1-2 cm. J Obstet Gynaecol Res. 2012;38:1041 ̶ 5
National Institute for Health and Care Excellence. Antenatal care for uncomplicated pregnancies. NICE clinical guideline 62. 2008. Manchester: NICE
Nelson WL, O'Brien JM. The uterine sandwich for persistent uterine atony: Combining the B-Lynch compression suture and an intrauterine Bakri balloon. Am J Obstet Gynecol. 2007;196:9
Nizard J, Barrinque L, Frydman R, Fernandez H. Fertility and pregnancy outcomes following hypogastric artery ligation for severe post-partum haemorrhage. Hum Reprod. 2003;18:844 ̶ 8
Nyflot LT, Sandven I, Stray-Pedersen B, Pettersen S, Al-Zirqi I, Rosenberg M, Jacobsen AF, Vangen S. Risk factors for severe postpartum hemorrhage: A case-control study. BMC Pregnancy Childbirth. 2017;17:17
Obata S, Kasai M, Kasai J, Seki K, Sekikawa Z, Torimoto I, Takebayashi S, Hirahara F, Aoki S. Emergent Uterine Arterial Embolization Using N-Butyl Cyanoacrylate in Postpartum Hemorrhage with Disseminated Intravascular Coagulation. Biomed Res Int. 2017;2017:1562432
Ochoa M, Allaire AD, Stitely ML. Pyometria after hemostatic square suture technique. Obstet Gynecol. 2002;99:506 ̶ 9
Oladapo OT, Fawole B, Blum J, Abalos E. Advance misoprostol distribution for preventing and treating postpartum haemorrhage. Cochrane Database Syst Rev. 2012;(2):CD009336

104
Olsen R, Reisner DP, Benedetti TJ, Dunsmoor-Su RF. Bakri balloon effectiveness for postpartum hemorrhage: A "real world experience". J Matern Fetal Neonatal Med. 2013;26:1720 ̶ 3
Ouahba J, Piketty M, Huel C, Azarian M, Feraud O, Luton D, Sibony O, Oury JF. Uterine compression sutures for postpartum bleeding with uterine atony. BJOG. 2007;114:619 ̶ 22
Pala S, Atilgan R, Baspinar M, Kavak EC, Yavuzkir S, Akyol A, Kavak B. Comparison of results of Bakri balloon tamponade and caesarean hysterectomy in management of placenta accreta and increta: A retrospective study. J Obstet Gynaecol. 2018;38:194 ̶ 9
Park KJ, Shin JH, Yoon HK, Gwon DI, Ko GY, Sung KB. Postpartum hemorrhage from extravasation or pseudoaneurysm: Efficacy of transcatheter arterial embolization using N-butyl cyanoacrylate and comparison with gelatin sponge particle. J Vasc Interv Radiol. 2015;26:154 ̶ 61
Patacchiola F, D'Alfonso A, Di Fonso A, Di Febbo G, Kaliakoudas D, Carta G. Intrauterine balloon tamponade as management of postpartum haemorrhage and prevention of haemorrhage related to low-lying placenta. Clin Exp Obstet Gynecol. 2012;39:498 ̶ 9
Pelage JP, Le Dref O, Jacob D, Soyer P, Herbreteau D, Rymer R. Selective arterial embolization of the uterine arteries in the management of intractable post-partum hemorrhage. Acta Obstet Gynecol Scand. 1999;78:698 ̶703 (a)
Pelage JP, Soyer P, Le Dref O, Dahan H, Coumbaras J, Kardache M, Rymer R. Uterine arteries: Bilateral catheterization with a single femoral approach and a single 5-F catheter - technical note. Radiology. 1999;210:573 ̶ 5 (b)
Pereira A, Nunes F, Pedroso S, Saraiva J, Retto H, Meirinho M. Compressive uterine sutures to treat postpartum bleeding secondary to uterine atony. Obstet Gynecol. 2005;106:569 ̶ 72
Pivano A, Alessandrini M, Desbriere R, Agostini A, Opinel P, d'Ercole C, Haumonte JB. A score to predict the risk of emergency caesarean delivery in women with antepartum bleeding and placenta praevia. Eur J Obstet Gynecol Reprod Biol. 2015;195:173 ̶6
Poggi SH, Yaeger A, Wahdan Y, Ghidini A. Outcome of pregnancies after pelvic artery embolization for postpartum hemorrhage: Retrospective cohort study. Am J Obstet Gynecol. 2015;213:576.e1 ̶ 576.e5
Poujade O, Zappa M, Letendre I, Ceccaldi PF, Vilgrain V, Luton D. Predictive factors for failure of pelvic arterial embolization for postpartum hemorrhage. Int J Gynaecol Obstet. 2012;117:119 ̶ 23
Prata N, Bell S, Weidert K. Prevention of postpartum hemorrhage in low-resource settings: Current perspectives. Int J Womens Health. 2013;5:737 ̶52
Provansal M, Courbiere B, Agostini A, D'Ercole C, Boubli L, Bretelle F. Fertility and obstetric outcome after conservative management of placenta accreta. Int J Gynaecol Obstet. 2010;109:147 ̶ 50

105
Revert M, Cottenet J, Raynal P, Cibot E, Quantin C, Rozenberg P. Intrauterine balloon tamponade for management of severe postpartum haemorrhage in a perinatal network: A prospective cohort study. BJOG. 2017;124:1255 ̶62
Revert M, Rozenberg P, Cottenet J, Quantin C. Intrauterine Balloon Tamponade for Severe Postpartum Hemorrhage. Obstet Gynecol. 2018;131:143 ̶ 9
Robinson AJ, Muller PR, Allan R, Ross R, Baghurst PA, Keirse MJ. Precise mid-trimester placenta localisation: Does it predict adverse outcomes? Aust N Z J Obstet Gynaecol. 2012;52:156 ̶ 60
Rocher G, Panel P, Rollin I, Wormser A, Souiai-Hidoussi A, Raynal P, Niro J. Massive hemoperitoneum due to uterine perforation by the Bakri Balloon, during the treatment of postpartum hemorrhage. J Gynecol Obstet Hum Reprod. 2019;48:75 ̶ 6
Ronel D, Wiznitzer A, Sergienko R, Zlotnik A, Sheiner E. Trends, risk factors and pregnancy outcome in women with uterine rupture. Arch Gynecol Obstet. 2012;285:317 ̶ 21
Rosenberg T, Pariente G, Sergienko R, Wiznitzer A, Sheiner E. Critical analysis of risk factors and outcome of placenta previa. Arch Gynecol Obstet. 2011;284:47 ̶ 51
Royal College of Obstetricians and Gynaecologists (RCOG). The role of emergency and elective interventional radiology in postpartum hemorrhage. Royal College of Obstetricians and Gynaecologists Good Practice Guideline No. 6. London, 2007
Ruiter L, Eschbach SJ, Burgers M, Rengerink KO, van Pampus MG, Goes BY, Mol BW, Graaf IM, Pajkrt E. Predictors for Emergency Cesarean Delivery in Women with Placenta Previa. Am J Perinatol. 2016;33:1407 ̶ 14
Said Ali A, Faraag E, Mohammed M, Elmarghany Z, Helaly M, Gadallah A, Taymour MA, Ahmad Y, Ibrahim Eissa A, Ibrahim Ogila A, Ali MK, Abou-Taleb HA, Samy A, Abbas AM. The safety and effectiveness of Bakri balloon in the management of postpartum hemorrhage: A systematic review. J Matern Fetal Neonatal Med. 2019;epub:1 ̶ 8
Salim R, Chulski A, Romano S, Garmi G, Rudin M, Shalev E. Precesarean Prophylactic Balloon Catheters for Suspected Placenta Accreta: A Randomized Controlled Trial. Obstet Gynecol. 2015;126:1022 ̶ 8
Say L, Chou D, Gemmill A, Tuncalp O, Moller AB, Daniels J, Gulmezoglu AM, Temmerman M, Alkema L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob Health. 2014;2:323
Sebghati M, Chandraharan E. An update on the risk factors for and management of obstetric haemorrhage. Womens Health (Lond). 2017;13:34 ̶ 40
Sekiguchi A, Nakai A, Kawabata I, Hayashi M, Takeshita T. Type and location of placenta previa affect preterm delivery risk related to antepartum hemorrhage. Int J Med Sci. 2013;10:1683 ̶ 8

106
Seldinger SI. Catheter replacement of the needle in percutaneous arteriography; a new technique. Acta Radiol. 1953;39:368 ̶ ̶ 76
Sentilhes L, Ambroselli C, Kayem G, Provansal M, Fernandez H, Perrotin F, Winer N, Pierre F, Benachi A, Dreyfus M, Bauville E, Mahieu-Caputo D, Marpeau L, Descamps P, Goffinet F, Bretelle F. Maternal outcome after conservative treatment of placenta accreta. Obstet Gynecol. 2010;115:526 ̶ 34 (a)
Sentilhes L, Gromez A, Clavier E, Resch B, Descamps P, Marpeau L. Long-term psychological impact of severe postpartum hemorrhage. Acta Obstet Gynecol Scand. 2011;90:615 ̶ 20
Sentilhes L, Gromez A, Clavier E, Resch B, Verspyck E, Marpeau L. Fertility and pregnancy following pelvic arterial embolisation for postpartum haemorrhage. BJOG. 2010;117:84 ̶93 (b)
Sentilhes L, Gromez A, Clavier E, Resch B, Verspyck E, Marpeau L. Predictors of failed pelvic arterial embolization for severe postpartum hemorrhage. Obstet Gynecol. 2009;113:992 ̶ 9
Sentilhes L, Kayem G, Silver RM. Conservative Management of Placenta Accreta Spectrum. Clin Obstet Gynecol. 2018;61:783 ̶ 94
Shahin Y, Pang CL. Endovascular interventional modalities for haemorrhage control in abnormal placental implantation deliveries: A systematic review and meta-analysis. Eur Radiol. 2018;28:2713 ̶ 26
Sheiner E, Sarid L, Levy A, Seidman DS, Hallak M. Obstetric risk factors and outcome of pregnancies complicated with early postpartum hemorrhage: A population-based study. J Matern Fetal Neonatal Med. 2005;18:149 ̶54
Shields LE, Smalarz K, Reffigee L, Mugg S, Burdumy TJ, Propst M. Comprehensive maternal hemorrhage protocols improve patient safety and reduce utilization of blood products. Am J Obstet Gynecol. 2011;205:368.e1 ̶368.e8
Shlansky-Goldberg R, Cope C. A new twist on the Waltman loop for uterine fibroid embolization. J Vasc Interv Radiol. 2001;12:997 ̶ 1000
Shobeiri F, Jenabi E. Smoking and placenta previa: A meta-analysis. J Matern Fetal Neonatal Med. 2017;30:2985 ̶ 90
Shrivastava VK, Nageotte MP. The Utilization of Interventional Radiologic Procedures in the Surgical Management of Placenta Accreta Syndrome. Clin Obstet Gynecol. 2018;61:795 ̶ 807
Silver RM. Abnormal Placentation: Placenta Previa, Vasa Previa, and Placenta Accreta. Obstet Gynecol. 2015;126:654 ̶ 68
Silver RM, Barbour KD. Placenta accreta spectrum: Accreta, increta, and percreta. Obstet Gynecol Clin North Am. 2015;42:381 ̶402

107
Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, Thom EA, Moawad AH, Caritis SN, Harper M, Wapner RJ, Sorokin Y, Miodovnik M, Carpenter M, Peaceman AM, O'Sullivan MJ, Sibai B, Langer O, Thorp JM, Ramin SM, Mercer BM, National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Maternal morbidity associated with multiple repeat cesarean deliveries. Obstet Gynecol. 2006;107:1226 ̶ 32
Silver RM, Major H. Maternal coagulation disorders and postpartum hemorrhage. Clin Obstet Gynecol. 2010;53:252 ̶ 64
Simic M, Cnattingius S, Petersson G, Sandstrom A, Stephansson O. Duration of second stage of labor and instrumental delivery as risk factors for severe perineal lacerations: Population-based study. BMC Pregnancy Childbirth. 2017;17:72 ̶6
Snowdon C, Elbourne D, Forsey M, Alfirevic Z. Information-hungry and disempowered: A qualitative study of women and their partners' experiences of severe postpartum haemorrhage. Midwifery. 2012;28:791 ̶ 9
Society of Gynecologic Oncology, American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine, Cahill AG, Beigi R, Heine RP, Silver RM, Wax JR. Placenta Accreta Spectrum. Am J Obstet Gynecol. 2018;219:B2 ̶ B16
Soro MP, Denys A, de Rham M, Baud D. Short & long term adverse outcomes after arterial embolisation for the treatment of postpartum haemorrhage: A systematic review. Eur Radiol. 2017;27:749 ̶ 62
Soyama H, Miyamoto M, Sasa H, Ishibashi H, Yoshida M, Nakatsuka M, Takano M, Furuya K. Effect of routine rapid insertion of Bakri balloon tamponade on reducing hemorrhage from placenta previa during and after cesarean section. Arch Gynecol Obstet. 2017;296:469 ̶ 74
Soyer P, Dohan A, Dautry R, Guerrache Y, Ricbourg A, Gayat E, Boudiaf M, Sirol M, Ledref O. Transcatheter Arterial Embolization for Postpartum Hemorrhage: Indications, Technique, Results, and Complications. Cardiovasc Intervent Radiol. 2015;38:1068 ̶ 81
Soyer P, Morel O, Fargeaudou Y, Sirol M, Staub F, Boudiaf M, Dahan H, Mebazaa A, Barranger E, le Dref O. Value of pelvic embolization in the management of severe postpartum hemorrhage due to placenta accreta, increta or percreta. Eur J Radiol. 2011;80:729 ̶ 35
Stafford I, Dildy GA, Clark SL, Belfort MA. Visually estimated and calculated blood loss in vaginal and cesarean delivery. Am J Obstet Gynecol. 2008;199:519.e1 ̶ 519.e7
Stefanovic V, Paavonen J, Loukovaara M, Halmesmaki E, Ahonen J, Tikkanen M. Intravenous sulprostone infusion in the treatment of retained placenta. Acta Obstet Gynecol Scand. 2013;92:426 ̶ 32
Sturzenegger K, Schaffer L, Zimmermann R, Haslinger C. Risk factors of uterine rupture with a special interest to uterine fundal pressure. J Perinat Med. 2017;45:309 ̶ 13

108
Suzuki Y, Matsuzaki S, Mimura K, Kumasawa K, Tomimatsu T, Endo M, Kimura T. Investigation of perioperative complications associated with use of uterine compression sutures. Int J Gynaecol Obstet. 2017;139:28 ̶33
Sziller I, Hupuczi P, Papp Z. Hypogastric artery ligation for severe hemorrhage in obstetric patients. J Perinat Med. 2007;35:187 ̶ 92
Taipale P, Hiilesmaa V, Ylostalo P. Transvaginal ultrasonography at 18-23 weeks in predicting placenta previa at delivery. Ultrasound Obstet Gynecol. 1998;12:422 ̶ 5
Takahashi H, Matsubara S, Kobayashi M, Ohkuchi A. Drainage failure of Bakri balloon: No drainage does not indicate no bleeding. Acta Obstet Gynecol Scand. 2015;94:336
Tan CH, Tay KH, Sheah K, Kwek K, Wong K, Tan HK, Tan BS. Perioperative endovascular internal iliac artery occlusion balloon placement in management of placenta accreta. AJR Am J Roentgenol. 2007;189:1158 ̶ 63
Tattersall M, Braithwaite W. Balloon tamponade for vaginal lacerations causing severe postpartum haemorrhage. BJOG. 2007;114:647 ̶ 8
Thompson JF, Ford JB, Raynes-Greenow CH, Roberts CL, Ellwood DA. Women's experiences of care and their concerns and needs following a significant primary postpartum hemorrhage. Birth. 2011;38:327 ̶ 35
Thurn L, Lindqvist PG, Jakobsson M, Colmorn LB, Klungsoyr K, Bjarnadottir RI, Tapper AM, Bordahl PE, Gottvall K, Petersen KB, Krebs L, Gissler M, Langhoff-Roos J, Kallen K. Abnormally invasive placenta-prevalence, risk factors and antenatal suspicion: Results from a large population-based pregnancy cohort study in the Nordic countries. BJOG. 2016;123:1348 ̶55
Tikkanen M, Paavonen J, Loukovaara M, Stefanovic V. Antenatal diagnosis of placenta accreta leads to reduced blood loss. Acta Obstet Gynecol Scand. 2011;90:1140 ̶6
Tol ID, Yousif M, Collins SL. Post traumatic stress disorder (PTSD): The psychological sequelae of abnormally invasive placenta (AIP). Placenta. 2019;81:42 ̶5
Tuncalp O, Hofmeyr GJ, Gulmezoglu AM. Prostaglandins for preventing postpartum haemorrhage. Cochrane Database Syst Rev. 2012;(8):CD000494
Tuzovic L. Complete versus incomplete placenta previa and obstetric outcome. Int J Gynaecol Obstet. 2006;93:110 ̶7
Unal O, Kars B, Buyukbayrak EE, Karsidag AY, Turan C. The effectiveness of bilateral hypogastric artery ligation for obstetric hemorrhage in three different underlying conditions and its impact on future fertility. J Matern Fetal Neonatal Med. 2011;24:1273 ̶ 6

109
van Beekhuizen HJ, de Groot AN, De Boo T, Burger D, Jansen N, Lotgering FK. Sulprostone reduces the need for the manual removal of the placenta in patients with retained placenta: A randomized controlled trial. Am J Obstet Gynecol. 2006;194:446 ̶ 50
van den Akker T, Brobbel C, Dekkers OM, Bloemenkamp KW. Prevalence, Indications, Risk Indicators, and Outcomes of Emergency Peripartum Hysterectomy Worldwide: A Systematic Review and Meta-analysis. Obstet Gynecol. 2016;128:1281 ̶ 94
van Stralen G, Ruijten LLM, Kaptein AA, Wolterbeek R, van Roosmalen J. Major obstetric hemorrhage: A follow-up survey on quality of life of women and their partners. J Psychosom Obstet Gynaecol. 2018;39:38 ̶ 46
van Stralen G, van Stralen-Ruijten LL, Spaargaren CF, Broadbent E, Kaptein AA, Scherjon SA. Good quality of life after emergency embolisation in postpartum haemorrhage. J Psychosom Obstet Gynaecol. 2010;31:285 ̶8
van Stralen G, von Schmidt Auf Altenstadt, J F, Bloemenkamp KW, van Roosmalen J, Hukkelhoven CW. Increasing incidence of postpartum hemorrhage: The Dutch piece of the puzzle. Acta Obstet Gynecol Scand. 2016;95:1104 ̶ 10
Vendittelli F, Barasinski C, Pereira B, Lemery D, HERA Group. Incidence of immediate postpartum hemorrhages in French maternity units: A prospective observational study (HERA study). BMC Pregnancy Childbirth. 2016;16:242 ̶ 7
Vintejoux E, Ulrich D, Mousty E, Masia F, Mares P, de Tayrac R, Letouzey V. Success factors for Bakri balloon usage secondary to uterine atony: A retrospective, multicentre study. Aust N Z J Obstet Gynaecol. 2015;55:572 ̶ 7
Vitthala S, Tsoumpou I, Anjum ZK, Aziz NA. Use of Bakri balloon in post-partum haemorrhage: A series of 15 cases. Aust N Z J Obstet Gynaecol. 2009;49:191 ̶ 4
Vivanti AJ, Furet E, Nizard J. Successful use of a Bakri Tamponade Balloon in the treatment of puerperal uterine inversion during caesarean section. J Gynecol Obstet Hum Reprod. 2017;46:101 ̶ 2
Vrachnis N, Salakos N, Iavazzo C, Grigoriadis C, Iliodromiti Z, Siristatidis C, Katsetos C, Creatsas G. Bakri balloon tamponade for the management of postpartum hemorrhage. Int J Gynaecol Obstet. 2013;122:265 ̶ 6
Walsh CA, Baxi LV. Rupture of the primigravid uterus: A review of the literature. Obstet Gynecol Surv. 2007;62:327 ̶4
Wang D, Xu S, Qiu X, Zhu C, Li Z, Wang Z, Hou H, Gao Y, Wang X, He P, Qin Y, Liu L. Early usage of Bakri postpartum balloon in the management of postpartum hemorrhage: A large prospective, observational multicenter clinical study in South China. J Perinat Med. 2018;46:649 ̶ 56

110
Wang YL, Su FM, Zhang HY, Wang F, Zhe RL, Shen XY. Aortic balloon occlusion for controlling intraoperative hemorrhage in patients with placenta previa increta/percreta. J Matern Fetal Neonatal Med. 2017;30:2564 ̶ 8
Wani RV, Abu-Hudra NM, Al-Tahir SI. Emergency peripartum hysterectomy: A 13-year review at a tertiary center in kuwait. J Obstet Gynaecol India. 2014;64:403 ̶ 8
Waterstone M, Bewley S, Wolfe C. Incidence and predictors of severe obstetric morbidity: Case-control study. BMJ. 2001;322:1089 ̶ 4
Weeks AD. The retained placenta. Best Pract Res Clin Obstet Gynaecol. 2008;22:1103 ̶ 17
Wei X, Zhang J, Chu Q, Du Y, Xing N, Xu X, Zhou Y, Zhang W. Prophylactic abdominal aorta balloon occlusion during caesarean section: A retrospective case series. Int J Obstet Anesth. 2016;27:3 ̶ 8
Westhoff G, Cotter AM, Tolosa JE. Prophylactic oxytocin for the third stage of labour to prevent postpartum haemorrhage. Cochrane Database Syst Rev. 2013;(10):CD001808
Wetta LA, Szychowski JM, Seals S, Mancuso MS, Biggio JR, Tita AT. Risk factors for uterine atony/postpartum hemorrhage requiring treatment after vaginal delivery. Am J Obstet Gynecol. 2013;209:51.e1 ̶ 51.e6
WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): An international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389:2105 ̶ 16
World Health Organization (WHO). Make every mother and child count: The world health report 2005. World Health organization, Geneva, 2005:62 ̶ 3
World Health Organization (WHO). WHO recommendations for the prevention and treatment of postpartum hemorrhage. Geneva: WHO; 2012
Wright CE, Chauhan SP, Abuhamad AZ. Bakri balloon in the management of postpartum hemorrhage: A review. Am J Perinatol. 2014;31:957 ̶ 64
Wright JD, Devine P, Shah M, Gaddipati S, Lewin SN, Simpson LL, Bonanno C, Sun X, D'Alton ME, Herzog TJ. Morbidity and mortality of peripartum hysterectomy. Obstet Gynecol. 2010;115:1187 ̶ 93
Wu HH, Yeh GP. Uterine cavity synechiae after hemostatic square suturing technique. Obstet Gynecol. 2005;105:1176 ̶ 8
www.cookmedical.com
www.stat.fi

111
Yoong W, Ridout A, Memtsa M, Stavroulis A, Aref-Adib M, Ramsay-Marcelle Z, Fakokunde A. Application of uterine compression suture in association with intrauterine balloon tamponade ('uterine sandwich') for postpartum hemorrhage. Acta Obstet Gynecol Scand. 2012;91:147 ̶ 51
Yorifuji T, Tanaka T, Makino S, Koshiishi T, Sugimura M, Takeda S. Balloon tamponade in atonic bleeding induces uterine contraction: Attempt to quantify uterine stiffness using acoustic radiation force impulse elastography before and after balloon tamponade. Acta Obstet Gynecol Scand. 2011;90:1171 ̶ 2
Zaat TR, van Steijn ME, de Haan-Jebbink JM, Olff M, Stramrood CAI, van Pampus MG. Posttraumatic stress disorder related to postpartum haemorrhage: A systematic review. Eur J Obstet Gynecol Reprod Biol. 2018;225:214 ̶20
Zlatnik MG, Cheng YW, Norton ME, Thiet MP, Caughey AB. Placenta previa and the risk of preterm delivery. J Matern Fetal Neonatal Med. 2007;20:719 ̶ 23
Zlatnik MG, Little SE, Kohli P, Kaimal AJ, Stotland NE, Caughey AB. When should women with placenta previa be delivered? A decision analysis. J Reprod Med. 2010;55:373 ̶ 81

112
APPENDIX I: Questionnaire for women with hysterectomy

113
Dear ________________________________,
You have delivered in Naistenklinikka. Because of bleeding problem or high risk of heavy bleeding during your delivery you had hysterectomy. You also experienced catheterization of femoral arteries and possible embolization of pelvic arteries.
Currently, we are performing an inquiry to all the patients treated by these procedures. The purpose is to evaluate whether the procedures had influence on your further health and quality of life. We hope to get more information about long-term effects of these procedures. By obtaining this information we can recognize better possible problems related to this procedure and provide more accurate counseling.
We would be very grateful if you could answer the following questionnaire. It will take about 10 minutes. We wish that you will be able return the filled questionnaire by 30.6.2013. Postal charge is already paid on behalf of you. All information will be handled confidentially and if you prefer not to answer, it will not influence to your further medical treatment.
Helsinki 29.5.2013
Yours Sincerely,
Maiju Grönvall MD, Specialist in Obstetrics and Gynecology HYKS, Naistenklinikka email. [email protected]
Vedran Stefanovic PhD, Specialist in Obstetrics, Gynecology and Perinatal Medicine HYKS, Naistenklinikka email. [email protected] tel. 050- 427 1230

114
Questionnaire: 1) Have you recovered totally of the delivery (in which you had the catheterization procedure and hysterectomy) (circle)?
Yes / No
2) If you feel that you do not have recovered totally, what kind of physical or mental symptoms or problems you still have? 3) What kind of experience your delivery was to you? 4) Was the hysterectomy hard experience to you? If yes, how? 5) Have you had some of the following symptoms after your delivery (circle):
a. depression b. fear of death c. sexual problems d. problems with intimate relationship e. hard to accept that You are not able to get pregnant again
6) If you have had physical or mental problems after embolization, have you got help to your problems? Where did you get help? Thank you very much for your time and answers!

115
APPENDIX II: Questionnaire for women without hysterectomy

116
Dear_________________________, You delivered in Naistenklinikka or in Kätilöopisto and experienced bleeding problems which was treated, among other measurements, by procedure called uterine artery embolization. The procedure’s goal is the temporary closure of uterine arteries in order to stop bleeding. We currently are performing an inquiry to all the patients treated by this procedure. The purpose is to evaluate whether the embolization of uterine arteries had an influence on your menstrual cycle, possible pregnancies and mental health. We hope to get more information about long-term effects of this procedure. By obtaining this information we can recognize better possible problems related to this procedure and give counseling to patients. We would be very grateful if you could answer the following questionnaire. It will take about 10-15 minutes. We wish that you will be able return the filled questionnaire by 19.12.2012. Postal charge is already paid on behalf of you. All information will be handled confidentially and if you prefer not to answer, it will not influence to your further medical treatment. Helsinki 19.11.2012 Maiju Grönvall MD Specializing Doctor in Obstetrics and Gynecology HYKS, Naistenklinikka email. [email protected] tel. 050- 427 1216 Vedran Stefanovic PhD, Specialist in Obstetrics, Gynecology and Perinatal Medicine HYKS, Naistenklinikka email. [email protected] tel. 050- 427 1230

117
A. Menstrual cycle 1) Is your menstrual cycle nowadays regular (circle)? Yes / No 2) How long is your period (days)? 3) Is the amount of menstrual bleeding (circle) Spare / Normal / Heavy 4) Have you noticed any change in your period after embolization procedure? What kind of change? 5) Have you had sterilization during your delivery (circle)? Yes / No If answer is yes, you do not have to answer questions A6, B4-10, C. 6) Do you use contraception? What kind of contraception? For how long? B. Fertility 1) Did you have problems to get pregnant before embolization (circle)? Yes / No 2) Did you have any examinations because of infertility before embolization (circle)? Yes / No 3) Have you had artificial reproductive treatment (IVF or any kind of assisted reproductive techniques) before embolization (circle)? Yes / No 4) Have you tried to conceive after embolization (circle)? Yes / No 5) Have you had pregnancies after embolization (circle)? Yes / No 6) If you have tried to get pregnant without succeeding, how long have you tried (months)? 7) If you have not tried to conceive after embolization procedure, why?

118
8) Have you had examinations because of infertility after embolization (circle)? Yes / No 9) Have the doctors found some reason for your infertility? What was the reason? 10) Have you had artificial reproductive treatment after embolization? What kind of treatment? C. Pregnancies after embolization You do not have to answer this section if you have not had pregnancies after embolization 1) How many pregnancies have you had after embolization? 2) For how long did you try to conceive before you got pregnant (months)? 3) How many of your pregnancies ended up with (you can but the number after each item a-c) a. Miscarriage? b. Abortion? c. Delivery? 4) If your pregnancy ended up to miscarriage, in which pregnancy week the miscarriage happened? 5) If you had artificial abortion, what was the reason for it and in which pregnancy week that happened? 6) If you had delivery, a. In which pregnancy week the baby was born? b. What was the birth weight of the baby? c. Was there any problem during the pregnancy, what kind of problems? d. Did you have vaginal delivery or cesarean section as a mode of delivery? If cesarean, why? e. Did the massive hemorrhage happen again? What was the amount of blood loss? What was the reason for blood loss?

119
D. Quality of life 1) Have you recovered totally of the delivery (in which you had the embolization) (circle)? Yes / No 2) If you feel that you do not have recovered totally, what kind of symptoms or problems you still have? 3) What kind of experience your delivery was to you? 4) Have you had some of the following symptoms after your delivery (circle): a. depression b. fear to get pregnant again c. anxiety during a new pregnancy d. fear of delivery e. fear of death f. sexual problems g. problems with intimate relationship 5) If you have had physical or mental problems after embolization, have you got help to your problems? Where did you get help? Thank you very much for your time and answers!