Severe necrotizing pancreatitis -...
42
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc
Transcript of Severe necrotizing pancreatitis -...
Severe necrotizing pancreatitis
ICU Fellowship Training Radboudumc

Acute pancreatitisPatients with acute pancreatitis
van Dijk SM. Gut 2017;66:2024-2032

Diagnosis
• Abdominal pain consistent with pancreatitis
• Serum amylase and/or lipase at least 3 times upper limit
• Findings consistent with acute pancreatitis on CECT, MRI or ultrasound
Revised Atlanta classification
At least two out of three criteria
Banks PA. Gut 2013;62:102-111

Severity classification
• Mild - no local or systemic complications
• Moderate - local (e.g. peripancreatic fluid collections or systemic complications or transient organ failure < 48 hrs
• Severe - persistent organ failure > 48 hrs
Banks PA. Gut 2013;62:102-111

Aetiology
15%
15%
20%
50%
Gallstones/sludge Alcohol Unknown Rest
• Medication • ERCP • Hypercalcaemia • Hypertriglyceridemia • Surgery • Trauma
Perform EUS later on
Sludge

Severity prediction• APACHE II score
• Ranson score
• Modified Glasgow/Imrie score
• SIRS criteria > 48 hrs
• Bedside Index for the Severity in Acute Pancreatitis
• Harmless in Acute Pancreatitis Score
• CRP
Mainly used to exclude the possibility of severe pancreatitis
Vasudevan S. Pancreas 2018;47:65-71

Treatment acute phase• Fluid resuscitation
• Pain management (no evidence for specific pain protocol)
• Antibiotics and probiotics
• Nutrition
• Endoscopic retrograde cholangiography in biliary pancreatictis
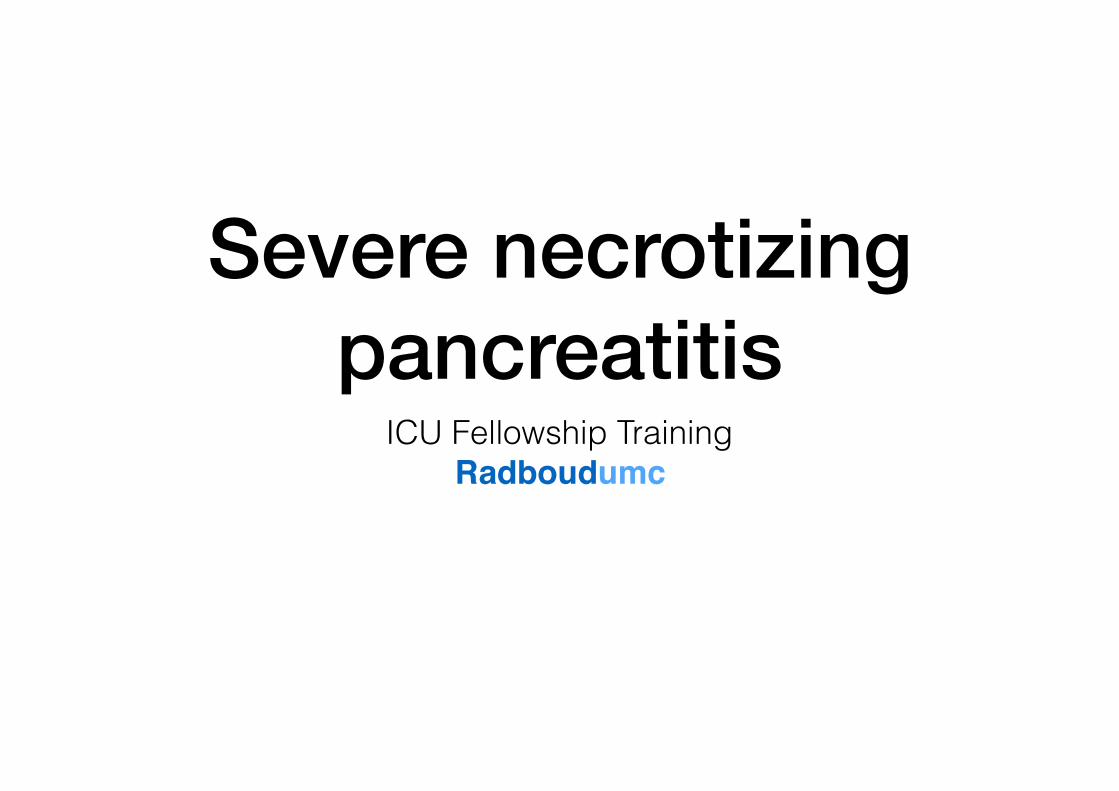
Fluid resuscitation• IAP/APA guidelines suggest using cristalloids in the form
of Ringer’s lactate or other balanced fluids (not confirmed in general ICU setting)
• End-points for early goal-directed therapy unknown - use SvO2, lactate, diuresis, capillary refill etc
% (S
IRS)
or m
g/dl
(CRP
)
-90-60-30
0306090
120
SIRS after 24 hrs CRP after 24 hrs
104
051,5
-84
RL NaCl 0.9%
p = 0.035
p = 0.02
N = 40
Wu BU. Clin Gastroenterol Hepatol 2011;9:710-717
Antibiotics and probiotics prophylaxis
• Aim is to prevent secondary infection of pancreatic or peripancreatic necrosis - result of bacterial translocation
• Antibiotic prophylaxis (several RCT’s) does not prevent secondary infection
• Probiotics increased mortality in a multicentre RCT

Infected pancreatic necrosis
Mortality
Lim CLL. J Gastrointest Surg 2015;19:480-491
Randomized controlled trials

Surgical intervention
Extra-pancreatic infection

Probiotics in predicted severe acute pancreatitis
• Multicentre randomized DB placebo-controlled trial (N = 298)
• Predicted severe acute pancreatitis (AP II ≥ 8, Imrie ≥ 3, CRP > 150 mg/L)
• < 72 hrs of onset of symptoms probiotics vs placebo 2 td for 28 days
• Primary outcome composite of infectious complications during admission and 90-D follow-up
Besselink MGH. Lancet 2008;371:651-659

Probiotics in predicted severe acute pancreatitis
0
7,5
15
22,5
30
Infectious complications Mortality Bowel ischemia
6
16
30
06
28
Placebo ProbioticsP = 0.80 P = 0.01 P = 0.004
Besselink MGH. Lancet 2008;371:651-659
Nutrition
• Enteral nutrition reduces rates of infection, organ failure and mortality compared to parenteral nutrition
• In patients with predicted severe pancreatitis, enteral can be limited to those who have an insufficient oral intake after 3 - 5 days
• Nasogastric feeding is non-inferior to nasojejunal feeding (3 RCT’s)
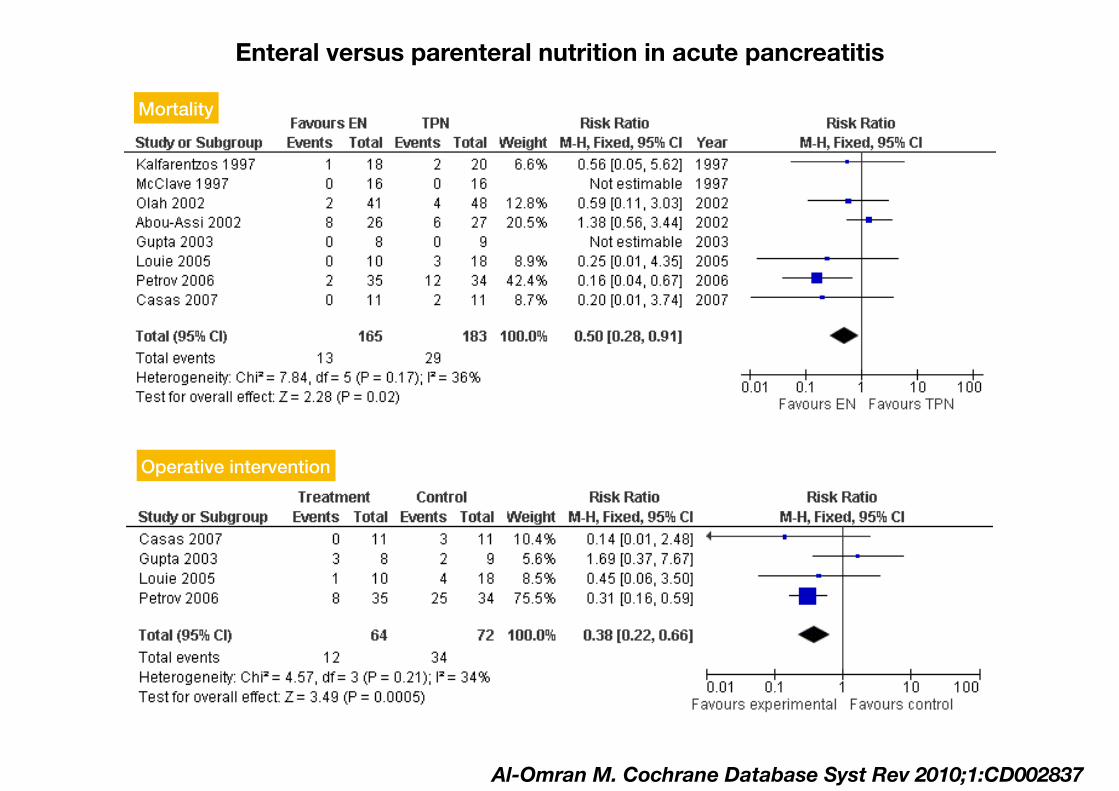
Mortality
Enteral versus parenteral nutrition in acute pancreatitis
Operative intervention
Al-Omran M. Cochrane Database Syst Rev 2010;1:CD002837

Early enteral feeding in predicted severe acute pancreatitis
• Multicentre randomized trial (N = 208)
• Predicted severe acute pancreatitis (AP II ≥ 8, Imrie ≥ 3, CRP > 150 mg/L)
• Nasoenteric tube feeding < 24 hrs after randomization vs oral diet after 72 hrs with tube feeding if not tolerated
• Primary outcome composite of major infection or death during 6 months follow-up
Bakker OJ. New Engl J Med 2014;371:1983-1993
PYTHON trial
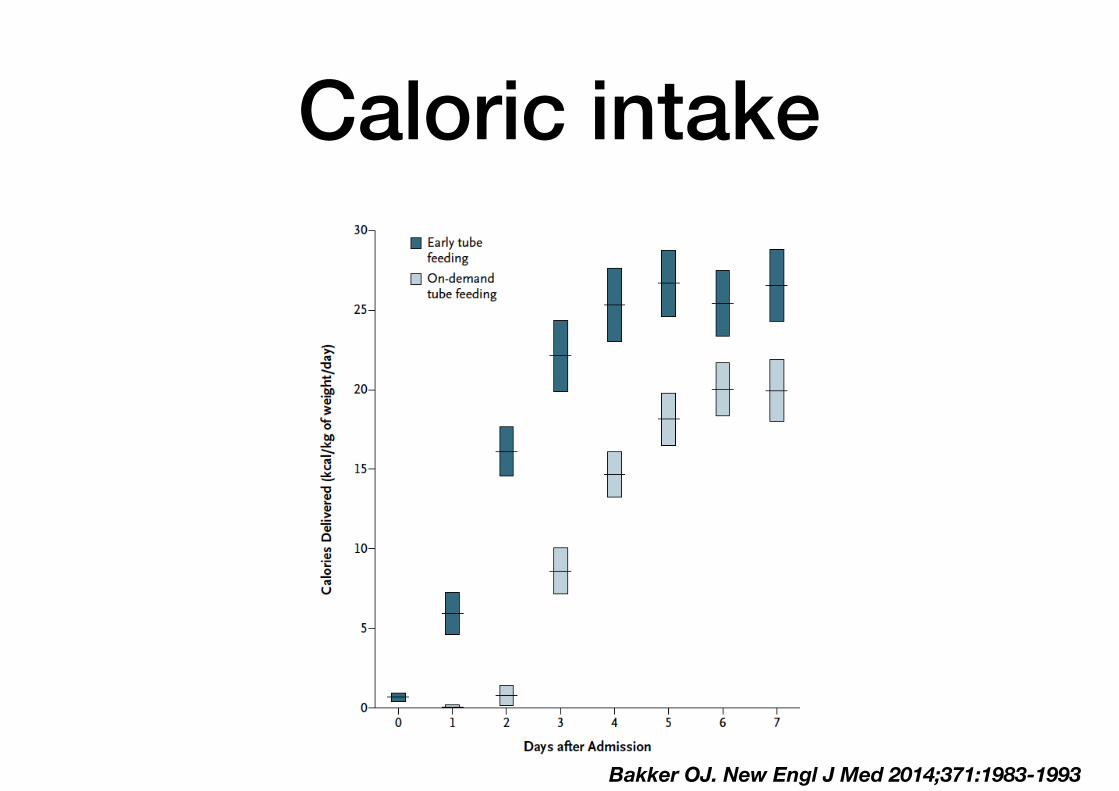
Caloric intake
Bakker OJ. New Engl J Med 2014;371:1983-1993
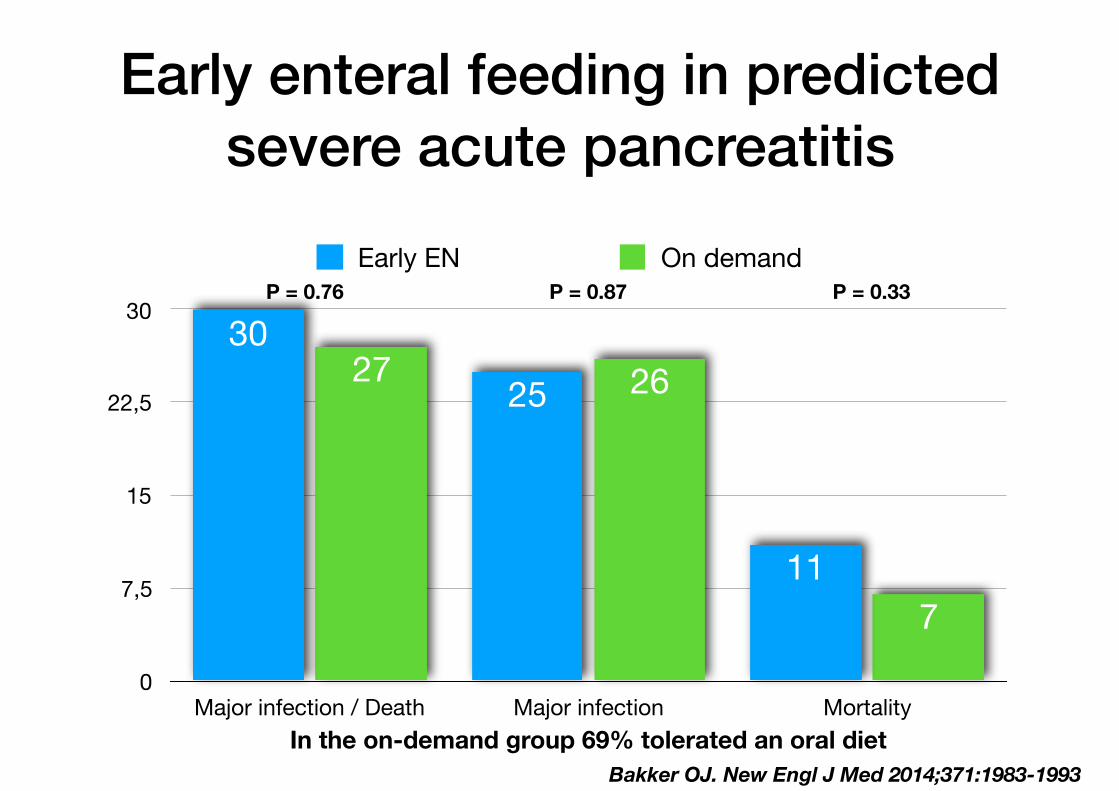
Early enteral feeding in predicted severe acute pancreatitis
0
7,5
15
22,5
30
Major infection / Death Major infection Mortality
7
2627
11
2530
Early EN On demandP = 0.76 P = 0.87 P = 0.33
Bakker OJ. New Engl J Med 2014;371:1983-1993In the on-demand group 69% tolerated an oral diet

Endoscopic retrograde cholangiography
• Early ERC not effective in patients with predicted mild pancreatitis
• Emergency ERC with sphincterotomy < 24 hrs is indicated in case of concomitant cholangitis
• Routine early ERC with sphincterotomy in predicted severe biliary pancreatitis is controversial
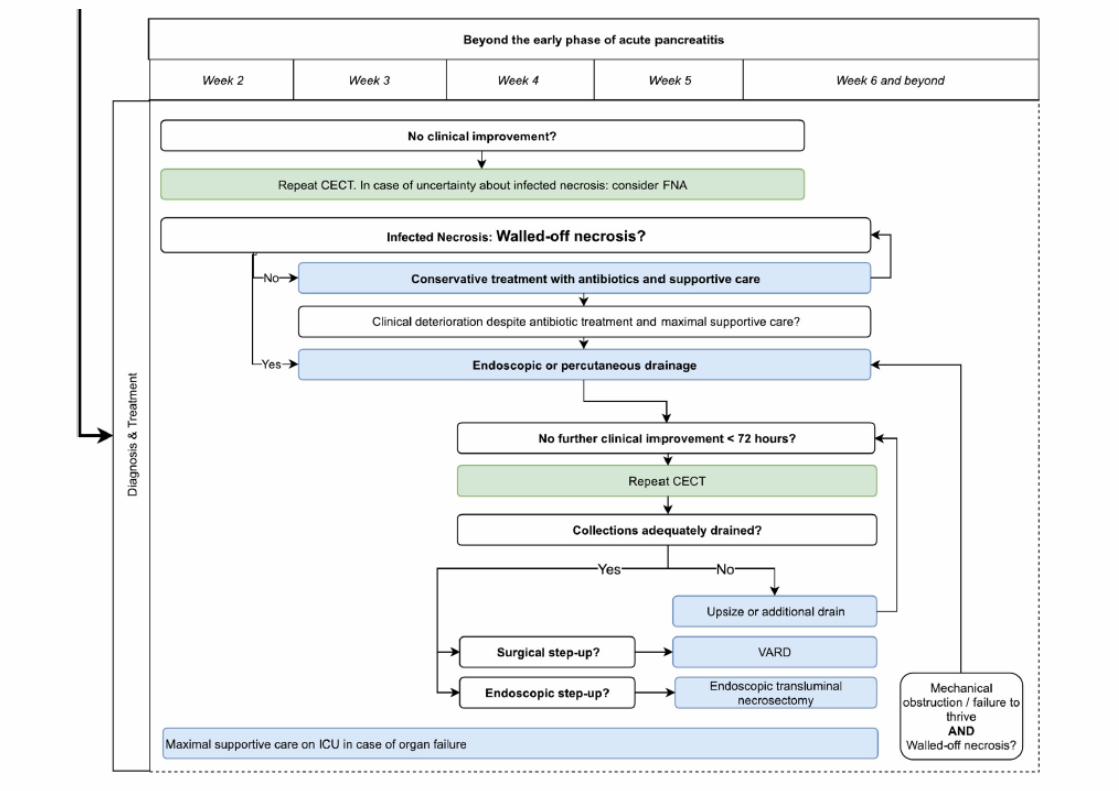
Beyond the early phase
• Imaging
• Infected necrotising pancreatitis

CECT-scan
• In the first 3 - 4 days unreliable for detection of extent of necrosis or presence of collections
• Urgent CECT only in case of suspected abdominal catastrophe including perforation, bleeding and ischemia
• If a patient does not improve after 5 - 7 days CECT is indicated to determine the presence and extent of necrosis

Revised Atlanta criteria
• Interstitial oedematous pancreatitis
• Necrotising pancreatitis
✓ parenchymal
✓ peripancreatic
✓ both
Banks. PA. Gut 2013;62:102-111
“Acute pancreatic fluid collections”

Complications of interstitial oedematous pancreatitis
• Rare
• Usually after > 4 weeks
• Well circumscribed (round/oval)
• Homogenous fluid density
• Well defined wallPancreatic pseudocyst
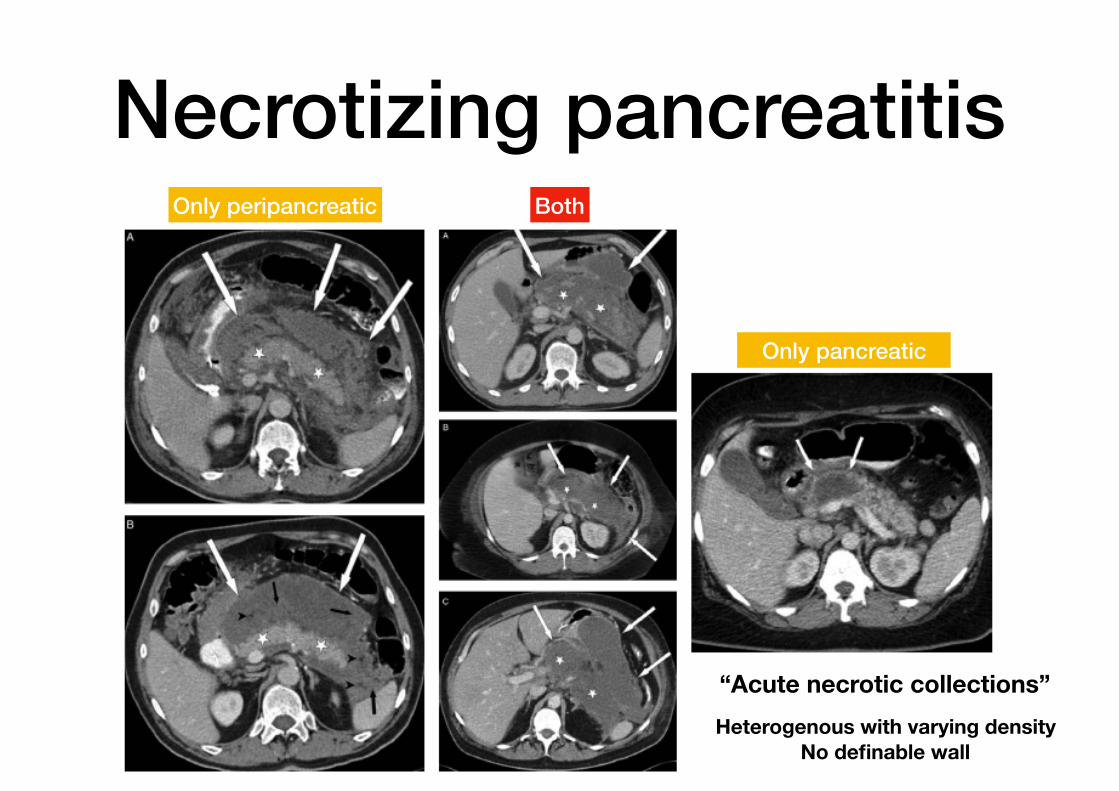
Necrotizing pancreatitisOnly peripancreatic Both
Only pancreatic
“Acute necrotic collections”Heterogenous with varying density
No definable wall

Walled-off necrosis
• Encapsulation of necrotic tissue
• Usually around 4 - 6 weeks
• Intervention only in case of infection!
• Consider intervention after 6-8 weeks in case of mechanical obstruction or failure to thrive
Heterogenous with liquid/non-liquid density - well defined complete wall

Walled-off necrosis

Outcome acute collections
Acute pancreatitis N = 189
Acute interstitial pancreatitis (36)
Acute necrotic pancreatitis (153)
Acute peripancreatic fluid collection
(N = 8)Pseudocyst
(N = 1)
Acute necrotic collection (143)
23 died 21 resolved collection
WON (N = 84)
8 died 53 intervention 23 conservative
Manrai M. Ann Surg 2018;267:357-363

CECT-scan infected necrosis
• Extraluminal gas in pancreas and peripancreatic tissues
• Positive gram stain/culture after FNA

Infected necrotizing pancreatitis
• Acute necrotic collections or walled-off necrosis become infected in one third of patients
• With proven infection or high clinical suspicion antibiotics are indicated
• Although antibiotics only may be successful, further intervention (catheter drainage / necrosectomy) is usually necessary

Intervention
• Delay intervention until stage of WON
• Catheter drainage followed by necrosectomy if clinically indicated
• Endosonography-guided transgastric necrosectomy may be the preferred technique
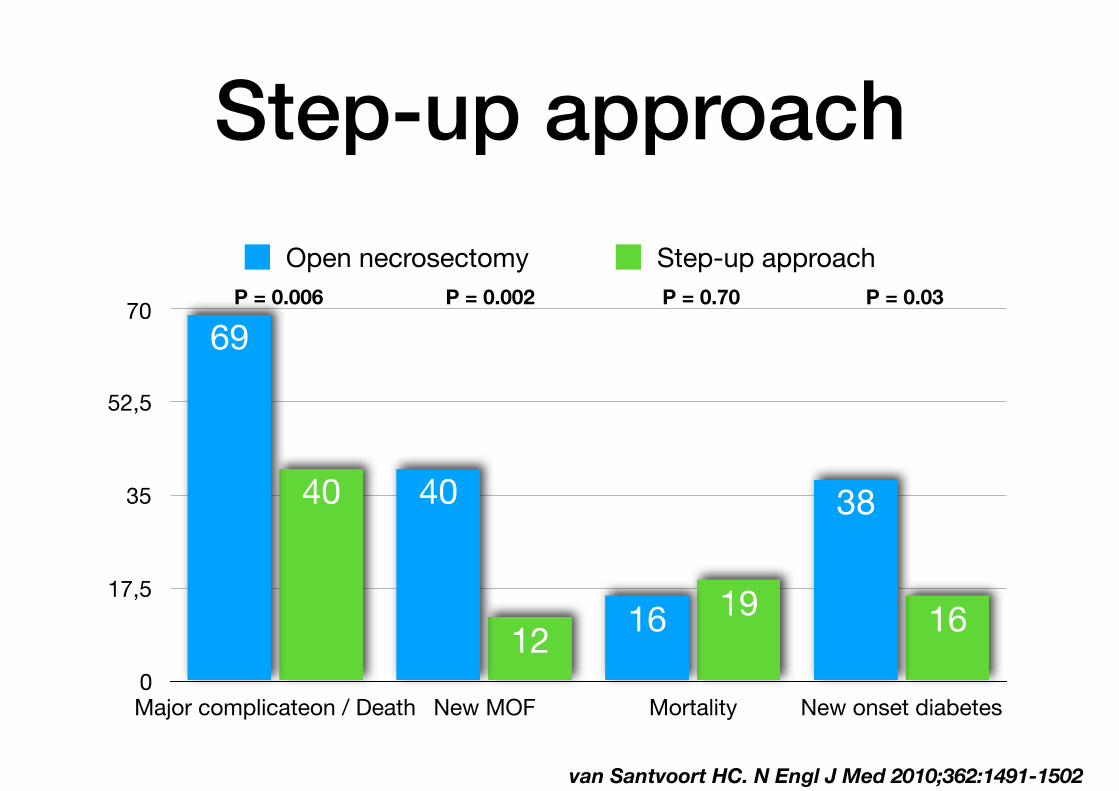
Step-up approach
• Multicentre randomized trial (N = 88)
• Necrotizing pancreatitis with confirmed or suspected infection
• Primary open necrosectomy vs step-up approach (percutaneous drainage, minimally invasive retroperitoneal necrosectomy)
• Primary outcome composite of major complications or death
van Santvoort HC. N Engl J Med 2010;362:1491-1502
Step-up approach
0
17,5
35
52,5
70
Major complicateon / Death New MOF Mortality New onset diabetes
161912
40 38
16
40
69
Open necrosectomy Step-up approachP = 0.006 P = 0.002 P = 0.70 P = 0.03
van Santvoort HC. N Engl J Med 2010;362:1491-1502

644 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 84 • NUMBER 8 AUGUST 2017
NECROTIZING PANCREATITIS
Antibiotic therapy may provide a bridge to intervention
atic necrosis. Antibiotics with gram-negative coverage and appropriate penetration such as carbapenems, metronidazole, fl uoroquino-lones, and selected cephalosporins are most commonly used. Meropenem is the antibiotic of choice at our institution. CT-guided fi ne-needle aspiration is often done if suspected infected pancreatic ne-crosis fails to respond to empiric antibiotic therapy. Debridement or drainage. Generally, the diagnosis or suspicion of infected pancreatic necrosis (suggestive signs are high fever, el-evated white blood cell count, and sepsis) warrants an intervention to debride or drain infected pancreatic tissue and control sepsis.21 While source control is integral to the suc-cessful treatment of infected pancreatic ne-crosis, antibiotic therapy may provide a bridge to intervention for critically ill patients by suppressing bacteremia and subsequent sep-sis. A 2013 meta-analysis found that 324 of 409 patients with suspected infected pancre-atic necrosis were successfully stabilized with antibiotic treatment.21,22 The trend toward conservative management and promising out-comes with antibiotic therapy alone or with minimally invasive techniques has lessened the need for diagnostic CT-guided fi ne-needle aspiration.
HemorrhageSpontaneous hemorrhage into pancreatic ne-crosis is a rare but life-threatening complica-tion. Because CT is almost always performed with contrast enhancement, this complica-tion is rarely identifi ed with imaging. The di-agnosis is made by noting a drop in hemoglo-bin and hematocrit. Hemorrhage into the retroperitoneum or the peritoneal cavity, or both, can occur when an infl ammatory process erodes into a nearby artery. Luminal gastrointestinal bleeding can occur from gastric varices arising from splenic vein thrombosis and resulting left-sided por-tal hypertension, or from pseudoaneurysms. These can also bleed into the pancreatic duct (hemosuccus pancreaticus). Pseudoaneurysm is a later complication that occurs when an arterial wall (most commonly the splenic or gastroduodenal artery) is weakened by pan-creatic enzymes.23
FIGURE 4. Treatment of infected walled-off necrosis in the patient shown in Figure 3. Under computed tomographic guidance, 3 large-bore catheters were placed in the left fl ank (arrows).
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 84 • NUMBER 8 AUGUST 2017 645
CHUA AND COLLEAGUES
Prompt recognition of hemorrhagic events and consultation with an interventional ra-diologist or surgeon are required to prevent death.
Infl ammation and abdominal compartment syndromeInfl ammation from necrotizing pancreatitis can cause further complications by blocking nearby structures. Reported complications in-clude jaundice from biliary compression, hy-dronephrosis from ureteral compression, bowel obstruction, and gastric outlet obstruction. Abdominal compartment syndrome is an increasingly recognized complication of acute pancreatitis. Abdominal pressure can rise due to a number of factors, including fl uid collec-tions, ascites, ileus, and overly aggressive fl uid resuscitation.24 Elevated abdominal pressure is associated with complications such as de-creased respiratory compliance, increased peak airway pressure, decreased cardiac preload, hy-potension, mesenteric and intestinal ischemia, feeding intolerance, and lower-extremity isch-emia and thrombosis. Patients with necrotizing pancreatitis who have abdominal compartment syndrome have a mortality rate 5 times higher than patients without abdominal compartment syndrome.25 Abdominal pressures should be monitored using a bladder pressure sensor in critically ill or ventilated patients with acute pancreatitis. If the abdominal pressure rises above 20 mm Hg, medical and surgical interventions should be offered in a stepwise fashion to decrease it. Interventions include decompression by naso-gastric and rectal tube, sedation or paralysis to relax abdominal wall tension, minimization of intravenous fl uids, percutaneous drainage of ascites, and (rarely) surgical midline or subcos-tal laparotomy.
■ ROLE OF INTERVENTIONThe treatment of necrotizing pancreatitis has changed rapidly, thanks to a growing experi-ence with minimally invasive techniques.
Indications for interventionInfected pancreatic necrosis is the primary indication for surgical, percutaneous, or endo-scopic intervention. In sterile necrosis, the threshold for inter-
Infl ammation from necrotizing pancreatitis can cause further complications by blocking nearby structures
FIGURE 5. Further treatment of infected walled-off necrosis in the patient shown in Figures 3 and 4. At 10 weeks after symptom onset and 6 weeks after catheter placement, laparoscopic-assisted debride-ment was done via the catheter sites. Computed tomography without contrast enhancement shows the results of debride-ment. Large drains (arrows) were placed after debridement.
VARDCatheter drainage

Endoscopic necrosectomy
• Multicentre randomized trial (N = 98)
• Necrotizing pancreatitis with confirmed or suspected infection and indication for invasive intervention
• Endoscopic (transluminal drainage, necrosectomy) versus surgical (percutaneous catheter drainage, VARD)
• Primary outcome composite of major complications or death (6 M)
van Brunschot S. Lancet 2018

Endoscopic necrosectomy
0
12,5
25
37,5
50
Major complicateon / Death Mortality
13
45
18
43
Endoscopic SurgicalP = 0.88 P = 0.50
van Brunschot S. Lancet 2018
Decreased incidence of pancreatic fistula and decreased hospital LOS

Candida infection
Hall AM. Crit Care 2013;17:R49
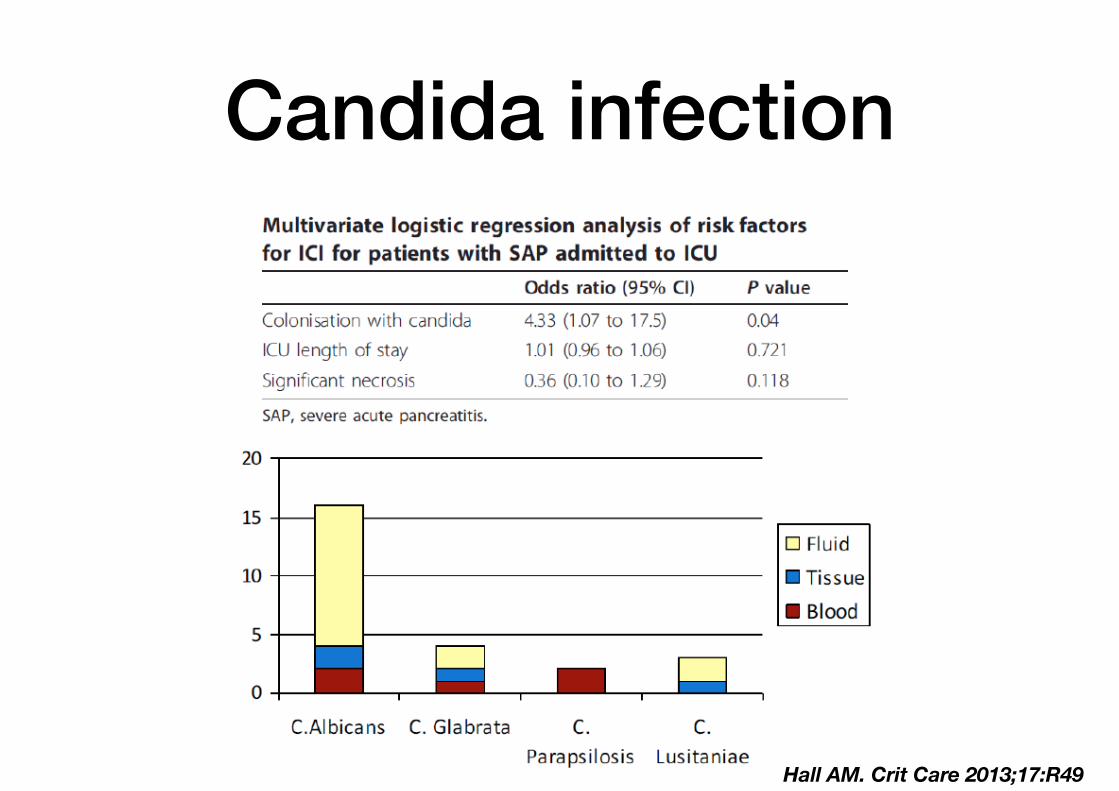
Candida infection
Hall AM. Crit Care 2013;17:R49

Local complications• Acute peripancreatic fluid collection
• Pancreatic pseudocyst
• Acute necrotic collection
• Walled-off necrosis
• Gastric outlet dysfunction
• Splenic and portal vein thrombosis
• Colonic necrosis

Aftercare• Prevention of recurrence
• Exocrine and endocrine insufficiency (19 - 80%)

Prevention of recurrence• In total 17 - 22% recurrence of pancreatitis and 8 - 16%
chronic pancreatitis
• Refrain from alcohol and cigarettes
• Cholecystectomy (severe pancreatitis - wait until recovery or 6 weeks after discharge, mild pancreatitis - during same hospital admission)
%
0
5
10
15
20
Gallstone related complications Recurrent pancreatitis
Same hospital admission Interval after 4 weeks
Mild pancreatitis
0.002 0.03

Conclusion