
Severe degloving injury of the sole and heel treated by a ... · CASE REPORT Severe degloving...
6
CASE REPORT Severe degloving injury of the sole and heel treated by a reverse flow sural artery neurofasciocutaneous flap and a modified off-loading external fixation device Thomas Zgonis a, * , Douglas T. Cromack b , Thomas S. Roukis c , Joann Orphanos d , Vasilios D. Polyzois e a Department of Orthopaedics, University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Drive, MSC 7776, San Antonio, TX 78229, USA b Department of Orthopaedics, University of Texas Health Science Center at San Antonio, San Antonio, TX, USA c Limb Preservation Service, Vascular Surgery Service, Department of Surgery, Madigan Army Medical Center, Tacoma, WA, USA d University of Texas Health Science Center at San Antonio, San Antonio, TX, USA e Department of Orthopaedic Traumatology, KAT Hospital, Athens, Greece Accepted 16 August 2006 Introduction Degloving injuries about the foot and ankle present a significant reconstructive challenge due to the superficial nature of tendon, joint and neurovascu- lar structures essential for proper acceptance of weight bearing and shear forces associated with bipedal gait. A degloving injury to the sole and heel can cause serious functional limitations for the patient and make the use of specialized shoe gear and brace therapy difficult. In the past, free tissue transfer with miscrovascular anastomosis, random pattern local, cross-leg and pedicle flaps have been used for closure of acute traumatic soft tissue injuries about the lower extremity and heel. 2,4,5,7 We present a case report involving a crush injury to the osseous and soft tissue components of the heel with an associated large degloving defect and a simultaneous dislocation of the ankle. A reverse flow sural neurofasciocutaneous flap with an off- loading hybrid external fixation system was used to provide closure of the surgical site, aid in the reduc- tion of the ankle dislocation and hindfoot and off- load the soft tissue flap reconstruction. Case report A 54-year-old man was brought to the emergency room with complaints of left heel pain after sustain- ing a severe degloving injury while at work. The injury was sustained when his left foot was crushed Injury Extra (2007) 38, 187—192 www.elsevier.com/locate/inext * Corresponding author. Tel.: +1 210 567 0219; fax: +1 210 567 4916. E-mail address: [email protected] (T. Zgonis). 1572-3461 # 2006 Elsevier Ltd. doi:10.1016/j.injury.2006.08.067 Open access under the Elsevier OA license.
Transcript of Severe degloving injury of the sole and heel treated by a ... · CASE REPORT Severe degloving...

Injury Extra (2007) 38, 187—192
www.elsevier.com/locate/inext
CASE REPORT
Severe degloving injury of the sole and heeltreated by a reverse flow sural arteryneurofasciocutaneous flap and a modifiedoff-loading external fixation device
Thomas Zgonis a,*, Douglas T. Cromack b, Thomas S. Roukis c,Joann Orphanos d, Vasilios D. Polyzois e
aDepartment of Orthopaedics, University of Texas Health Science Center at San Antonio,7703 Floyd Curl Drive, MSC 7776, San Antonio, TX 78229, USAbDepartment of Orthopaedics, University of Texas Health Science Center at San Antonio,San Antonio, TX, USAc Limb Preservation Service, Vascular Surgery Service, Department of Surgery,Madigan Army Medical Center, Tacoma, WA, USAdUniversity of Texas Health Science Center at San Antonio, San Antonio, TX, USAeDepartment of Orthopaedic Traumatology, KAT Hospital, Athens, Greece
Accepted 16 August 2006
Introduction
Degloving injuries about the foot and ankle presenta significant reconstructive challenge due to thesuperficial nature of tendon, joint and neurovascu-lar structures essential for proper acceptance ofweight bearing and shear forces associated withbipedal gait. A degloving injury to the sole and heelcan cause serious functional limitations for thepatient and make the use of specialized shoe gearand brace therapy difficult. In the past, free tissuetransfer with miscrovascular anastomosis, randompattern local, cross-leg and pedicle flaps have beenused for closure of acute traumatic soft tissue
* Corresponding author. Tel.: +1 210 567 0219;fax: +1 210 567 4916.
E-mail address: [email protected] (T. Zgonis).
1572-3461 # 2006 Elsevier Ltd.doi:10.1016/j.injury.2006.08.067
Open access under the Elsevier OA lic
injuries about the lower extremity and heel.2,4,5,7
We present a case report involving a crush injury tothe osseous and soft tissue components of the heelwith an associated large degloving defect and asimultaneous dislocation of the ankle. A reverseflow sural neurofasciocutaneous flap with an off-loading hybrid external fixation system was used toprovide closure of the surgical site, aid in the reduc-tion of the ankle dislocation and hindfoot and off-load the soft tissue flap reconstruction.
Case report
A 54-year-old man was brought to the emergencyroom with complaints of left heel pain after sustain-ing a severe degloving injury while at work. Theinjury was sustained when his left foot was crushed
ense.

188 T. Zgonis et al.
between the forklift he was driving and a steel bar.This patient was a healthy male with no contribut-ing medical problems. Radiographic examinationrevealed a posterior calcaneal tubercle fractureand widening of the medial gutter of the left ankle.
Figure 1 Intra-operative appearance of the devascularizednegative pressure system (D) application.
The patient was taken to the operating room forincision and drainage with ORIF of the calcanealfracture. The medial side of the degloving heel padinjury was re-approximated and sutured back inplace. The remainder of the wound was left open
heel pad (A and B), external fixation placement (C) and
Severe degloving injury of the sole and heel 189
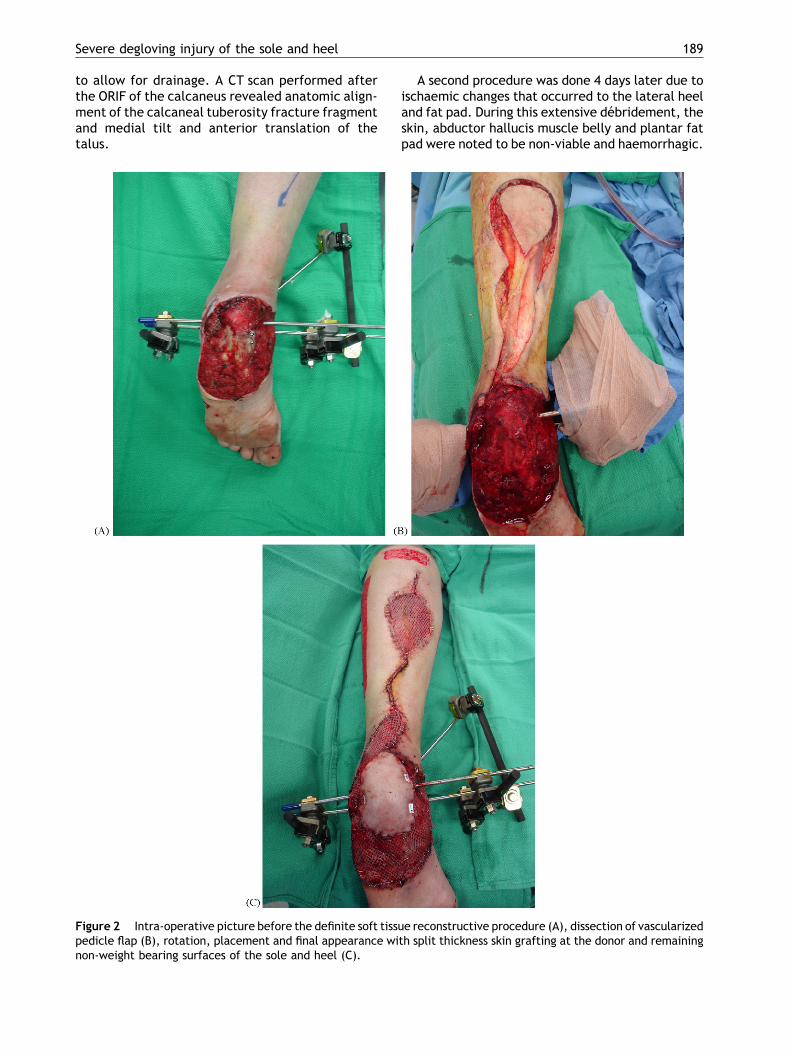
to allow for drainage. A CT scan performed afterthe ORIF of the calcaneus revealed anatomic align-ment of the calcaneal tuberosity fracture fragmentand medial tilt and anterior translation of thetalus.
Figure 2 Intra-operative picture before the definite soft tissupedicle flap (B), rotation, placement and final appearance winon-weight bearing surfaces of the sole and heel (C).
A second procedure was done 4 days later due toischaemic changes that occurred to the lateral heeland fat pad. During this extensive debridement, theskin, abductor hallucis muscle belly and plantar fatpad were noted to be non-viable and haemorrhagic.
e reconstructive procedure (A), dissection of vascularizedth split thickness skin grafting at the donor and remaining

190 T. Zgonis et al.
The debrided skin, muscle and soft tissue were sentto pathology for further evaluation. Resultsrevealed superficial and deep acute inflammation,haemorrhage, necrosis and focal epidermal necro-sis consistent with progression of his severely trau-matized soft tissues. During this surgical procedure,attention was also directed to the dislocated anklejoint and talus. Under image intensification andmanual manipulation, the ankle joint was reposi-tioned and the talus was reducedwith the help of anexternal fixation device and transfixion pins thruthe talus and calcaneus which also provided main-tenance of the reduction. A negative pressuredevice was further applied to the plantar aspectof the sole and heel to stimulate granulation tissue,provide drainage and reduce bacterial bioburden
Figure 3 Intra-operative application of an off-loadingexternal fixation foot ring (A) and post-operative appear-ance maintaining visual monitoring of the pedicle flap (B).
prior to the final reconstructive procedure. Intra-operative cultures revealed no bacterial growth(Fig. 1).
The patient was brought back for the definitivesoft tissue reconstructive procedure 10 days afterthe initial injury. Pre-operatively, the presence of apatent perforating peroneal artery was performedby a Doppler examination and a lesser saphenousvein mapping was also performed to further assistwith the dissection of the vascular pedicle flap. Thepedicle flap was raised to the pivot point 5 cmproximal to the lateral malleolus and rotated 1808without kinking the neurovascular pedicle. The flapwas sutured to the deep tissues using buried simpleinterrupted absorbable sutures in order to firmlyseat the flap and limit the potential for post-opera-tive haematoma formation. The cutaneous portionof the flap was then sutured to the perimeter of thewound using multiple, widely spaced simple inter-rupted non-absorbable sutures. Multiple split thick-ness skin grafts were then taken from themedial andlateral aspect of the ipsilateral lower extremity tocover the donor site as well as the remaining non-weight bearing surfaces of the sole and heel. Abolster type dressing was used to provide compres-sion at the recipient skin grafting sites. The pedicleflap was left exposed to allow for immediate post-operative monitoring (Fig. 2).
Figure 4 Final post-operative picture before patientwas allowed to full weight bear in a supportive shoe gear.

Severe degloving injury of the sole and heel 191
With the traditional bulky post-operative dres-sings and off-loading methods, visual monitoring ofthe vascular pedicle flap becomes extremely diffi-cult. Therefore, a modification was made to theexisted external fixation device that remained inplace. An additional foot ring was attached to theexternal fixation device to allow for quick andrepeated evaluation of the flap while maintainingsound immobilisation of the lower limb, ankle andfoot. Post-operatively, the pedicle flap and splitthickness skin grafts remained viable and went onto heal without complications (Fig. 3).
The final stage of the procedure involved removalof the external fixation device at approximately 6weeks. The bolster dressings were removed at about4 weeks. A below the knee cast immobilisation wasapplied after the modified external fixation systemwas removed. The patient remained non-weightbearing for a total of 12 weeks. He was then allowedto apply light weight to the affected limb with anassistance device. At 4 months, the patient wasallowed to take full weight in a supportive shoegear (Fig. 4).
Discussion
Reconstructive procedures for complex hindfoot andankle fractureswith soft tissue injuryareexceedinglydifficult to treat. Regardless of approach, the goal isto provide a stable, durable and well-contouredweight bearing surface that canbeplaced inamodestshoe with or without brace support. In this casereport, a calcaneal fracture with a severe deglovinginjury and a simultaneous ankle dislocation was pre-sented. A sural neurofasciocutaneous flap with amodified off-loading external fixation device wasused for the treatment of this severe injury.
The sural artery flap has been used as the recon-structive choice for small to medium soft tissueinjuries in the lower leg, ankle and heel.1,9 Priorto performing this procedure, it is important torequest non-invasive vascular studies and vein map-ping in order to aid in the surgical dissection of thelesser saphenous vein as it courses to the perforatingartery.10 The anatomic structures that supply thesural flap are the peroneal artery, lesser saphenousvein and sural nerve. The arc of rotation of thispedicle flap is 5 cm above the lateral malleolus.3,6
At this level, the peroneal artery can maintain itsintegrity and provide adequate vascular supply tothe reverse flow sural flap.3,6 If the pedicle donorsite from the proximal leg is small in size, it can beclosed primarily. Due to the size of the soft tissuedefect on the heel, it was necessary to close thedonor site with a split thickness skin graft from the
lower leg. This flap has a good arterial supply and itis important to monitor venous congestion post-operatively. If venous congestion occurs, the areaof necrosis is usually the distal tip of the flap. It hasbeen documented that venous congestion can beavoided in most cases when the pedicle is not buriedwithin a subcutaneous tunnel. This flap survivesbetter when it is transferred and laid directly onthe defect area.3,6,8,10
The ankle dislocation was corrected and main-tained with an external fixator and transfixion pinsthru the talus and calcaneus. This external fixationdevice was converted into an off-loading frame byattaching several clamps and a circular ring to theinferior aspect of the pre-existing device. The off-loading aspect to this device was crutial to thehealing process of the vascularized pedicle flap.The off-loading frame helped insure that therewould be no direct pressure to the sole and heelthat would cause the flap to fail.
Conclusion
The sural artery flap can be successful in the treat-ment of large soft tissue defects about the posteriorand plantar heel. It is a reliable, durable and rela-tively easy to perform procedure without sacrificinga major neurovascular bundle(s). However, a com-mon problem during the post-operative recoveryperiod for sural artery flaps has been preventingpressure over the flap, pedicle and donor site thatcome in direct contact with the splint, pillows andbedding.10 A new modified off-loading external fixa-tion device is presented on a severe degloving injuryof the sole and heel with a simultaneous calcanealfracture and ankle dislocation. This is a novel tech-nique that allows increased stability, ability to per-form concomitant osseous surgery and weight-shearing according to the individual patients needs.
References
1. Almeida MF, Da Costa PR, Okawa RY. Reverse-flow island suralflap. Plast Reconstr Surg 2002;109:583—91.
2. Al-Qattan MM. Lower limb reconstruction utilizing thereverse sural artery flap gastrocnemius muscle cuff techni-que. Ann Plast Surg 2005;55:174—8.
3. Angelats J, Albert LT. Sural nerve neurocutaneous croff-footflap. Ann Plat Surg 1984;13:239—42.
4. Graf P, Kalpen A, Biemer E. Revascularisation versus recon-struction of degloving injuries of the heel: case report.Microsurgery 1995;16:149—54.
5. Lai MF. Degloved sole and heel. Med J Aust 1979;1:598—9.6. Maffi TR, Knoetgen J, Turner NS, Moran SL. Enhanced survival
using the distally based sural artery interpolation flap. AnnPlast Surg 2005;54:302—5.

192 T. Zgonis et al.
7. Singh S, Naasan A. Use of distally based superficial sural islandartery flaps in acute open fractures of the lower leg. Ann PlastSurg 2001;47:505—10.
8. Tosum Z, Ozkam A, Karacor Z, Savaci N. Delaying thereverse sural flap provides predictable results for compli-cated wounds in diabetic foot. Ann Plast Surg 2005;55:169—73.
9. Yildirim S, Gideroglu K, Akoz T. The simple and effectivechoice for treatment of chronic calcaneal osteomyelitis:neurocutanous flaps. Plast Reconstr Surg 2003;111:753—60.
10. Zgonis T, Roukis TS. Off-loading large posterior heel defectsafter sural artery soft tissue flap coverage with a stackedTaylor spatial frame foot plate system. Oper Tech Orthop2006;16:32—7.


















