Psychiatric Nurses 1 PSYCHIATRIC NURSES - College of Saint Mary

1
SEVENTEENTH REPORT OF THE INDEPENDENT REVIEWER
ON PROGRESS TOWARD IMPLEMENTATION OF THE SETTLEMENT
AGREEMENT BETWEEN THE KENTUCKY CABINET FOR HEALTH AND
FAMILY SERVICES AND KENTUCKY PROTECTION AND ADVOCACY
Submitted by Diane Brewer May 14, 2018
I. INTRODUCTION
This report addresses progress by the Kentucky Cabinet for Health and Family Services
(Cabinet) toward meeting the provisions and intent of the Interim and Amended
Settlement Agreements (Settlement) between the Cabinet and Kentucky Protection and
Advocacy (P&A). The information provided herein represents the cumulative progress
since September 1, 2013, with specific emphasis on the quarter year January 1, 2018 to
March 31, 2018.
The Settlement specifies that the Cabinet will have transitioned 675 persons with serious
mental illness (SMI), previously in personal care homes (PCH), to community-based
housing by October 1, 2018. Individuals in this disability group are to receive Housing
Assistance to attain and maintain integrated, affordable housing with full rights of
tenancy. Housing Assistance as described in the Settlement also includes the receipt of
needed tenancy support services to allow individuals to maintain their housing. October
1, 2018 represents the five-year mark of the Settlement with a total of $31 million
pledged by the Cabinet to meet the terms of the Settlement. There have been 519
individuals transitioned, and there are currently 346 still in their housing.
The DBHDID’s behavioral health division has worked to develop and expand Assertive
Community Treatment (ACT) services and Peer Support services within the 14
community mental heath center (CMHC) regions. These have been key areas on which
to focus for the purpose of influencing attitudes about recovery, and for understanding the
types of outcomes that can be expected when knowledgeable, recovery-oriented staffs
utilize evidence based practices. Another important effort aimed in part at achieving
these same goals, was contracting for the person centered planning learning collaborative
provided by expert consultants, Janis Tondora and Diane Grieder. In addition to
addressing the long-standing problem of treatment plan documentation not reflecting the
“golden thread” of medical necessity, the learning collaborative stressed the expectation
of recovery and client self-determination in planning for goal achievement. Influencing
attitudes about recovery within the leadership of provider agencies and the leadership of
the Cabinet and its Departments and Offices is a key piece in the success of the
Settlement. Section I.B. of the Settlement states that in addition to ensuring services are
provided in the most integrated setting, as defined in federal law, “the Parties intended
that steps to achieve the goal of community integration and self-determination would be
undertaken”. Stakeholders with a role in achieving this goal of the Settlement must work
from a place of knowing that persons in this identified disability group can experience
full community integration when provided with the necessary individualized supports and
services. The Cabinet must determine what that array of supports and services would

2
look like in order to take action to ensure access to, and availability of those supports and
services. As with any disability group, there is a wide range of support needs. This
reviewer has asked direct service staff what they believe the service system needs in
order to support high-need individuals with SMI in the community. Some have cited the
need for 24/7 staffed houses similar to the system available for persons with intellectual
and developmental disabilities. More often, these staffs talk about the desire for larger
ACT teams with supportive prescribers, or just the capacity to provide more frequent in-
home services by community support associates, peer specialists, and others. The
supports needed to avoid institutionalization can range from simple and minimal, to
extensive oversight with coordination of several resources. This reviewer spoke to a
woman who had been living on her own in a rural area with support from her brother who
would come by to “look in on her and take her to the store”. She stated that when “his
legs got bad” he was no longer able to come by and she was taken a PCH to live. On the
other end of the spectrum, a CMHC determined that they were unable to support a man
who had been living in a beautiful neighborhood home staffed 24 hours a day. There was
not a higher level of care available to him, though it is possible that additional resources
and natural supports wrapped around him in that environment could have made a
difference. He was sent to one of the most run-down PCHs in the state where he will
have less oversight and receive fewer services than where he was. Section I.J. of the
Settlement states that the Parties acknowledge that the terms of the Settlement are
voluntarily accepted for the purpose of refocusing the Cabinet’s use of PCHs. This
aspect of the Settlement remains largely unaddressed, in that there has been no change in
the extent to which PCHs are used as a housing solution. Studies on the benefits of
supported housing have been conducted since the late 1980’s. These studies have shown
that not only is housing crucial to the recovery process, but that custodial housing is
undesirable and has long-term negative affects on morale and well-being. “Assistance in
finding safe and affordable permanent housing that is consistent with consumer
preferences leads to better consumer outcomes” (Corrigan, Mueser, Bond, Drake,
Solomon (2008) Principles and Practice of Psychiatric Rehabilitation: An Empirical
Approach). The work toward achieving the goals and substantive provisions of the
Settlement will move Kentucky forward in its pursuit of an evidenced based service
system that upholds the civil rights of this disability group.
II. SOURCES OF INFORMATION
Information for this report was obtained though a combination of Cabinet reports, data
reports from the Kentucky ISA/ASA Tracking Tool, and participation in meetings.
KY ISA/ASA Tracking Tool reports:
Referrals
Aftercare report
User report 2 - Time
Referrals not transitioned after 119 days
Referrals currently transitioned
Other documentation:

3
DIVERTS EBP Status form and summaries
Meetings this quarter have included:
1 Cabinet level meeting
5 Regional Transition Team meetings
1 P&A/DBH meeting
1 meeting with P&A staff
1 DBH Statewide meeting
Observations in the field
visit to Centerstone staff and client
visit to Bluegrass staff and client
visit to Mountain Comp. staff and clients
visit to Venture Homes PCH
III. CABINET ACTIONS/PROGRESS
The Cabinet has made progress toward each of the Settlement’s substantive provisions.
A Compliance With Substantive Provisions Grid was included as part of the first
quarterly report and was first scored in the third quarterly report using a 5-point Likert
scale ranging from ‘No Progress’ to ‘Complete’. Some of the Cabinet’s ongoing ratings
of ‘Modest Progress’ (progress by roughly 50%) or ‘Minimal Progress’ (progress by
roughly 25%) have been a result of uneven implementation across the state. There are
pockets of excellence across the state where provider agencies do effective in-reach and
take action to transition individuals with high need, while other provider agencies might
determine similar individuals are inappropriate for Housing Assistance. There are
provider agencies that add and modify services when faced with barriers to maintaining
successful community tenure, while other provider agencies go directly to the PCH
system as a back-up housing solution. These differences, in part, reflect recovery
attitudes and the agencies’ prioritization of effective tenancy support services; but the
CMHCs also face barriers of poorly funded services and difficulties having services
authorized and/or reauthorized by the managed care organizations. As efforts continue
for the improvement of service quality and service access, the Cabinet must determine
how the service system for adults with SMI will move toward the evidence based practice
of permanent supportive housing and away from an antiquated system of large
congregate housing. This report is structured to address each of the sections in the
Compliance with Substantive Provisions Grid along with scoring explanations.
Section III.A.1 Adequate and Appropriate Public Services
This provision is measured by the extent to which the Cabinet has provided adequate and
appropriate community based services to persons residing in or at risk of entry into a
PCH, so that they have the choice to live in the community. This has been rated Modest
Progress, acknowledging that choice has been made available to 519 individuals. Areas
to improve are:

4
Availability of choice for community services upon discharge from state
psychiatric facilities to avoid trans-institutionalization.
Need for consistency of opportunity for community integration regardless of
which PCH you reside in.
Development of, and access to services that will allow choice to persons whose
needs exceed the capabilities of the service providers and/or the limits of existing
services.
Adequate tenancy support services that will allow choice to continue to live in the
community without being returned to a PCH.
In Regional Transition team meetings, the state hospital representatives report on the
numbers of discharges to the different PCHs. They have admitted that the discharge
location is often not the choice of the client, but instead, is due to the lack of community
based service options. State guardians have also stated that their decision to place a ward
in a PCH, or have them discharged to a PCH from a state psychiatric facility is based less
on client choice and more on whether or not they believe sufficient community services
will be available and ongoing for their ward. Many understand that this is not a ‘level of
care’ decision, in terms of the PCH offering a higher level of mental health and physical
health services; but instead, a decision based more on the availability of some
surveillance, meals, and medications at the PCH. An indicator of progress in the area of
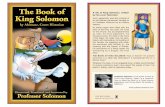
true client choice will be the reduction of hospital discharges to PCHs. This is one
indicator that has remained relatively unchanged throughout the time of the Settlement.
The chart below shows the quarterly comparisons between first time PCH discharges
from state psychiatric hospitals and total transitions. This quarter there were a total of
147 persons discharged from state hospitals to PCHs, with 40 of those being discharged
to a PCH for the first time.
3136
30
53 54
43
3235
30
18
44
2330
15
26
05
1015202530354045505560
10/14 1/15 4/15 7/15 10/15 1/16 4/16 7/16 10/16 1/17 4/17 7/17 10/17 1/18 4/18
Quarterly Comparison: Number of Transitions and
Number of Hospital Discharges to PCH-1st time
D/C to PCH
Transitions

5
The average annual percentages of PCH discharges across the 4 hospitals have been
consistent each year from FY ’15 to present. There has been an average of 52 discharges
to PCHs each year with an average of 14 not in a PCH prior to admission (or 28%
discharged to a PCH for the first time). The majority of PCH discharges are made by
ESH and WSH. The numbers of persons going to a PCH for the first time are a little
larger at ESH, but with the prevalence of PCHs in the WSH area, there is a greater
chance that the WSH patients have come to the hospital from a PCH.
Differences in opportunities for choice depending on the PCH in which you reside, can
be seen in the numbers of discharges from each of the free-standing PCHs. This chart
shows the number of transitions from each PCH, and one boarding home in the Bluegrass
region that was included in the Settlement. It is divided by service region and includes
the number of licensed PCH beds, the number of transitions, and the number of state
wards represented in the total number transitioned.
REGION PERSONAL CARE HOME PCH BEDS Number of
persons
transitioned
State
Guardianship
(from total)
1
Fern Terrace of Mayfield 104 38 2
Autumn Ridge Personal Care 24 5 0
Totals 128 43 2
2
Christian County Manor 78 21 3
Highland Homes 100 3 0
The Oaks PCH/Madisonville 58 6 2
Pennyrile Home 94 8 2
The Homestead 58 13 3
Trigg County Manor 68 2 0
Sparks Nursing Center 88 1 0
Totals 544 54 10
3
DAVECO Rest Home 92 10 1
Sunny Acres 32 7 4
Henderson Manor 64 2 0
The Oaks PCH/Lewisport 56 7 4
Bishop Soenneker Home 66 2 0
Fern Terrace of Owensboro 68 2 1
Totals 378 30 10
4
Fern Terrace of Bowling Green 114 20 5
Hart County Manor 54 11 5
Cornerstone Manor 36 23 9
Harper’s Home for The Aged 27 10 5
Scottsville Manor 40 8 2
Totals 271 72 26
5

6
Breckinridge Manor 40
(now closed)
5 2
Totals 5 2
6
Colonial House of Shepherdsville 62 25 3
Colonial Hall Manor 57 21 3
Totals 119 46 6
7
Colonial Gardens 80 1 1
Valley Haven Rest Home 45 7 2
Carrollton Manor 32 5 4
Jonesville Rest Home 26 0 0
Falmouth Nursing Home 28 5 0
Regency Manor North 30 4 1
Regency Manor 59 5 0
Front Gate 19 2 0
Totals 319 29 8
9/10
Russell Convalescent Home 28 15 6
Frasure’s Personal Care Home 61 16 8
Artrips Personal Care Home 22 3 2
Hamilton’s Personal Care Home 22 1 0
Hilltop Manor 36 1 0
Totals 169 36 16
11
Venture Home of Paintsville 56 12 2
Golden Years Rest Home 84 8 3
Totals 140 20 5
12
Caney Creek Rehabilitation
Complex
80
(now closed)
2 0
Totals 2 0
13
Generations Center of
Middlesboro
64 4 1
The Laurels 82 3 0
Totals 146 7 1
14
Dishman Personal Care Home 49 5 3
Somerview Personal Care Home 50 3 0
Cumberland Manor Rest Home 49 1 0
Totals 148 9 3
15
Rose Terrace Lodge 40 3 0
Central KY Recovery Center 32 69 10
Shady Lawn 75 3 1
Parkside Manor 51 3 1
Waynesburg Manor 28 0 0
Messner’s 38 1 1

7
Totals 264 79 13
Grand Total 2,626 432 102
The chart seems to show that opportunity for transition is greater in region 4, region 6, or
if you are at Central KY Recovery Center. Also affecting choice is whether or not the
opportunity exists to be sufficiently supported in the community. A region may have
several transitions from PCHs in their area, but then have for example, a 52% loss of
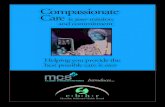
housing. The following chart reflects the number of transitions in each region with the
top shading indicating the number no longer in housing.
The relatively high percentage of persons no longer in housing as specified in the
Settlement is an indicator that the system cannot yet provide adequate and appropriate
public services and supports in the most integrated setting.
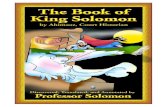
CMHCs enter a post transition code in the KY ISA Tracking Tool when someone is no
longer in their housing, to indicate the nature of the housing status change. The
following pie chart separates out seven categories of housing status changes within the
current total of all transitions.
05
101520253035404550556065707580859095
100105110
Total Transitioned by Serving Region Top Shading Indicates Number No Longer In Housing

8
Of the 519 total transitions, 173 persons (33%) are no longer in housing under the
Settlement. There have been 25 deaths. Ninety-two (92) have been re-institutionalized
in a PCH. Twenty-six (26) needed a higher level of care through staffed residences,
nursing homes, or SCL placement. Thirteen (13) left their housing to live with family or
friends. Fourteen (14) were evicted, left their housing, or otherwise were considered lost
by the CMHC. Three (3) lost housing due to incarceration.
Section III.A.2. Involvement of all guardians
All guardians are to receive information from the Cabinet to encourage their wards to
participate in decisions affecting them to the maximum extent of their abilities.
Decisions made by the guardian about where the individual will live are to reflect the
individual’s written preferences to the extent possible. This provision is rated Substantial
Progress due to the level of involvement of the Department of Aging and Independent
Living (DAIL) and their training of field workers to support transitions to the most
integrated setting appropriate to meet the needs of their wards. More work needs to be
done to get information to private guardians and the one public guardian in Paducah who
works with some of the persons referred for Housing Assistance. This could potentially
be addressed through brochures given to private guardian by CMHCs describing the
community based service they offer and through courts providing potential guardians
information on the Settlement’s services and on KRS 387.640.
Section III.B.1 Regulation
This provision is rated Complete. 908 KAR 2:065 was filed Dec. 2, 2015 and finalized
June 3, 2016.
Section III.C.1.2. Community Based Supported Housing
Status Changes after Transition
Still in housing that meetscriteria-346Deaths-25
Returned to PCH-92
To Staffed residences-8
To friends/family-13
Nursing home/SCL-18
Homeless/unable tolocate-14Incarcerated-3

9
This provision is evaluated by the extent to which eligible persons have access to
community based supported housing. The provision is rated Modest Progress,
acknowledging the Housing Assistance provided to 519 individuals, while also
acknowledging the extent of housing needed to accelerate transitions from PCHs and
allow hospital discharges to the community. CMHCs that have a designated staff person
for housing can do more toward developing relationships with local landlords and local
housing authorities; they can ensure a smooth process in submitting housing vouchers
and requests for OHI funding; and they can better manage existing vouchers being used
by the agency’s clients. The housing specialist’s supervisor and CSP Director must also
be knowledgeable about housing issues, so that when there is turnover in the housing
specialist position, it doesn’t result in loss of knowledge and in clients falling through the
cracks. Housing specialist turnover has at times left the job of training new CMHC staff,
and/or the job of intervening with local landlords, to the Kentucky Housing Corporation
(KHC). There are several CMHCs that have reported good relationships with local
landlords, so that the landlord calls them when apartments become available. The
landlord is able to trust that rent will be paid, that their tenants will receive on-going
support, and that there is someone to contact with any issues that may arise.
Section III.C.3.(a) Schedule for Housing Assistance
This provision spells out the target dates and benchmarks for the required number of
transitions to the community. The benchmark for Oct. 1, 2017 was 600 and the
benchmark for Oct. 1, 2018 is 675. At this second quarter of the Settlement year, the
benchmark is 637.5. This provision is rated Substantial Progress because 519 transitions
represents 81% of this quarter’s benchmark. The chart below shows the total number of
persons transitioned at the time of each reporting period in relation to the target goals as
specified in the Interim Settlement Agreement, then the Amended Settlement Agreement.
8 21 52 88118
171
225
268300
335
365383
427 450480
493 519
050
100150200250300350400450500550600650700
4/14 7/14 10/14 1/15 4/15 7/15 10/15 1/16 4/16 7/16 10/16 1/17
Number of Persons Transitioned in Relation to Target
(targets adjusted 10/19/15 retroactive to 10/1/15)
Target
Actual
4/17 7/17 10/17 1/18 4/18

10
The KY Housing Corporation has funding for approximately 25 housing vouchers,
depending on how many of the recently issued vouchers are used and how many tenants
discontinue use of current vouchers. It is anticipated that there will be a waiting list for
vouchers in the near future.
The work toward developing and expanding access to safe, affordable housing can
positively impact the overall costs of caring for this disability group. Stable housing has
long been considered one of the important social determinants of health, and there is
extensive literature linking housing instability and health care costs. A 2016 study
conducted by the Center for Outcomes Research and Education found that affordable
housing reduced overall health care expenditures by 12% for Medicaid recipients. This is
partly due to the increase in primary care visits that in turn, decrease emergency room
use. Persons that have supports attached to housing usually have increased monitoring of
health issues to avoid emergencies, and have assistance with general wellness activities,
thus decreasing health costs. (Health in Housing: Exploring the Intersection Between
Housing and Health Care, August 29, 2016)
Section III.C.3.(b) Transition of state wards
The Settlement was written that out of the 675 provided Housing Assistance,
approximately 335 are state wards and approximately 340 are not state wards. This
provision is rated Modest Progress. Currently 119 state wards have been transitioned
which represents 23% of all transitions. The 26 transitions this quarter included 9 state
wards. Of the 173 persons who transitioned but are no longer in housing as defined by
the Settlement, 54 (31%) are state wards.
Section III.C.6.7. Housing criteria
Housing under the Settlement is to be permanent with full Rights of Tenancy; it is to
include support services needed to maintain housing; and it is to be fully integrated,
scattered site housing. Housing cannot include group homes, boarding homes, or
supervised living settings. This provision is scored Substantial Progress. Transitions
counted under the Settlement have generally met these criteria. Exceptions would be
apartment complexes that may have had more than 25% of the units occupied by persons
transitioned, or situations where the transition was counted but there were insufficient
support services to maintain housing.
Section III.D.1.2. Array and intensity of services
Persons represented under the Settlement are to have access to the array and intensity of
services necessary to successfully transition to and live in community based housing.
The services are to:
a. be evidence-based, recovery-focused and community based;
b. be flexible and individualized to meet needs
c. help individuals recognize and deal with situations that may otherwise
result in crisis; and

11
d. increase and strengthen individuals’ networks of community and natural
supports.
This provision is rated Modest Progress due to uneven availability of services that meet
this criteria. There are service teams that are recovery focused and that strive to provide
evidence based services to fidelity. There are other areas where services are limited and
narrowly defined, such that the client must possess prerequisite skills or attitudes in order
to qualify, rather than individualizing services to meet client needs. ACT has been
described as requiring a “whatever it takes” approach by the service team. This is also
true when planning for, and coordinating other services and supports. The Cabinet must
determine the array and intensity of services needed across the state that will enable
persons to be supported in a less restrictive environment. The belief that a person must
stay in a PCH because they are incapable of “living on their own” or “living
independently” does not take into account the purpose of the Settlement. The expectation
should not be that the individual can succeed on their own, or that they will not be
dependent on a variety of supports. An individual’s support needs are to be identified
through assessment, with appropriate coordination of services occurring as part of the
person centered planning process. In addition to the Cabinet identifying and putting in
place the needed service array, areas for improvement include ensuring a thorough person
centered planning process that identifies needs and anticipates potential crises. There
also needs to be a stronger focus on the development of natural supports.
Section III.D.3. Five named services
The Settlement specifically requires that ACT, case management, crisis services, peer
support, and supported employment be available to persons transitioned to the
community. This provision is rated Substantial Progress in that these services are
available to some degree in almost all areas. Areas for improvement include ensuring
that services can be authorized and sufficiently reimbursed, and that services are not
siloed to the extent that clients are unaware of what is available to them.
Section III.D.4. ACT teams that meet fidelity
ACT is one of the oldest evidenced based practices in the field of psychiatric
rehabilitation, with over 40 years of research reporting outcomes that can be expected
when the service is provided to fidelity. All ACT teams are required to operate to fidelity
to either the Dartmouth Assertive Community Treatment (DACT) scale or the Tool for
Measurement of Assertive Community Treatment (TMACT) scale. This provision is
rated Minimal Progress based on the last fidelity reviews conducted that showed only
five ACT teams met a good or acceptable level of fidelity.
The success of ACT in Kentucky is a key component in achieving the goals of the
Settlement. Most of the ACT teams seem to be invested in the success of their clients,
though some may differ in who they believe can be successful or appropriate for their
services. ACT team members and other in-home service providers often have the “best
view of recovery” and serve as advocates within their own agencies for the community

12
integration of persons previously institutionalized. During this reviewer’s home visits to
persons who have transitioned, the tenants invariably credit ACT team staff for helping
them achieve their goal. ACT teams need the support of their agencies; a lessening of
barriers to service authorization and payment; a caseload size that will help cover service
costs; and on-going training in how to work with the high-need clients for which ACT
was designed. Solutions must be found to adequately address frequently encountered
issues such as substance use and diabetes so that these do not rule out clients from
receiving Housing Assistance. An ACT team leader at Centerstone talked about his harm
reduction approach with a client. He encouraged the client to “just stay sober” until the
ACT team staff arrived each day. After experiencing some repeated successes with that,
the client was asked to “just stay sober until your [substance abuse] group in the
evening”. This approach to his treatment has helped him greatly reduced the frequency
of his use. The client was not very verbal when visited but was able to say he liked
where he was living. He was someone who had previously moved, was returned to a
PCH, then moved again with more intense services. Another young man in Paintsville
was asked about his hopes for his life. He said he would like to meet a girl his own age
for company and said that his long-term goal was to go back to school and get a two-year
business degree. He stated that he wants to get a desk job and to wear a tie.
Below is the story of a man in Lexington receiving supports from the Bluegrass.Org ACT
team.
“I feel like I have succeeded quite a bit.”
A referral was made for Richard in June of 2016 so that he could receive Housing
Assistance and services that would allow him to live outside of the personal care home he
was in. The possibility of “guesting” in one of Bluegrass’ transitional housing units was
discussed with Richard in October of that year. After waiting for a unit to become
available, he guested for 3 days in March of 2017, then moved into the transitional unit in
April. When he left the PCH, the administrator gave him his card and told him that he
could come back. On September 5, 2017, Richard moved to his own apartment. I had
visited Richard last year when he was in the PCH and was able to visit him recently in his
home. He was comfortable talking about his life and how things have changed for him.
He said that the most difficult part of being in the PCH was being surrounded by people,
not being left alone, having difficulty getting along with some people, and having a
roommate who insisted on leaving the door open all the time. He also talked about
having a romantic relationship with one of the staff that resulted in the staff person being
fired. Richard shared that in his family home he had experienced his mother’s struggle
with untreated schizophrenia and his father’s drinking. He talked about living in the
dorm at Eastern Kentucky University for a couple of years where he studied Art and got
A’s in English; and then, the resulting panic of experiencing some of the same symptoms
he had seen in his father and mother. He was sent to the PCH after a psychiatric
hospitalization. When asked how he felt living in the PCH, he said “ashamed of myself
for letting my world crumble and having to be put in a place like that”. When asked how
he feels now, he was able to say that he believes he has “succeeded quite a bit”, though
he added that his family still does not yet see him that way.

13
Section III.D.5. Person-Centered Plans
Each person transitioning is to have a person-centered service plan done with a qualified
professional who is clinically responsible for coordinating all aspects of the plan. The
Person Centered Recovery Plan (PCRP) learning collaborative has reached all 14 CMHC
regions, and to a lesser extent has involved MCOs, Peer Specialists, and prescribers.
Each CMHC has had to determine if, or how they would make changes within their
electronic health records to better capture aspects of this approach to planning, such as
goal statements in the client’s own words, the listing of strengths to be referenced within
objectives, and the inclusion of non-billable natural support interventions. This provision
is rated Modest Progress. A great deal of work has been done by DBHDID toward the
implementation of PCRPs. What is unknown at this point is the result of that work.
DBHDID has a PCRP Quality Indicator Tool that was developed by the consultants.
This tool is to guide practitioners in their work and is also to be used by Department staff
to conduct reviews of plans with follow-up feedback on points for improvement. This
reviewer has seen the results from the Department’s review of a small sample size from
three different CMHCs. More reviews will provide information needed to better evaluate
the success of the learning collaborative. Some CMHC compliance officers/performance
improvement staffs were a part of the trainings provided by the consultants. Their
understanding of the quality indicators and their involvement in intra-agency reviews and
training will be important for the continuation of the practice and dissemination of the
practice’s underlying values. The learning collaborative was not specific to working with
persons leaving PCHs or state psychiatric hospitals. Person-centered planning is written
into the Settlement to ensure that client wishes, and service and support needs have been
identified before leaving an institution; and that persons responsible for the safety and
success of an individual know the actions they need to take, with timelines for taking
action. In addition to treatment and care coordination, the plan would include the very
practical details of who is getting utilities turned on, who is ensuring food and
medications are at the apartment, who is visiting or calling the client that first weekend at
home, getting crisis numbers on the refrigerator, ensuring the client knows what to do in
the case of problems or perceived emergencies, etc.
Section III.D.6. Case Management
Case management has always been a key service in supporting persons with SMI. When
clients do not need the intensity of ACT, they typically receive case management. Some
CMHCs have used case management along with other services to wrap support around
persons who qualify for ACT, but do not have ACT services available to them where they
want to live. This provision is rated Substantial Progress. Case management has always
been a strength in Kentucky, but barriers to service authorization have recently been an
issue in maintaining client stability in the community. Clarifying these issues will be
essential for this service to be an available tenancy support to persons in need.
Section III.D.7. Crisis Services

14
Crisis services are to include mobile crisis teams, community-based residential crisis
services, and 24/7 crisis phone lines. The Cabinet is to monitor crisis services in order to
identify service gaps and implement effective measures to address any gaps or
weaknesses. Crisis services provided to persons who have transitioned are to be
consistent with an already developed individual crisis plan in order to prevent
unnecessary hospitalization, incarceration, or institutionalization. This provision is rated
between Modest and Substantial Progress. All regions have a 24/7 crisis phone line, but
not all regions have mobile crisis teams or community-based residential crisis services.
Areas of improvement include determining where service gaps exist and how those gaps
might affect the unnecessary hospitalization, incarceration, or institutionalization of
persons transitioned. Considering the role of crisis services can be an aspect of “post-
mortem” reviews of failed transitions, particularly those with very short community
tenure. It is important for the Cabinet to know if, and how individualized crisis plans are
completed and used, in order to assess crisis service needs in each region.
Section III.D.8 Peer Services
DBHDID’s push to expand peer support services in Kentucky has paid off. Every
CMHC region has at least one peer specialist employed, even if they do not have the
minimum .5 FTE on their ACT team (only one region does not) or the minimum 2.0 FTE
for services that are separate from ACT (four regions do not). Peer support certification
trainings have continued and there have been training opportunities for the required
continuing education. The PCRP consultants recently provided a training for peer
support specialists regarding their role in the person-centered planning process. This
provision is rated Substantial Progress. Areas of improvement include better clarifying
the peer support services provided to clients who have transitioned, and ensuring that
more CMHCs offer this separate service to persons transitioned. Nine regions report
providing peer support services to persons who have transitioned and five regions report
serving no one who has transitioned, separate from contact made by the ACT team staff.
Section III.D.9. Supported Employment
Supported employment services that meet fidelity to the Individual Placement and
Support (IPS) model are to be available to persons transitioned, for their pursuit and
maintenance of integrated, paid, competitive work opportunities. There are 11 IPS
supported employment programs across the state that have achieved Good or Exemplary
fidelity scores. These include 8 CMHCs and 3 other Behavioral Health Organizations.
This provision is rated Modest to Substantial Progress because of Kentucky’s strong
efforts over the years to establish this service and maintain regular fidelity reviews. The
concern in terms of the Settlement is that reports show only 15 persons statewide have
received the service post-transition. Verbal reports in regional transition team meetings
indicate fewer than 5 people are employed. It will be important to determine the causes
of this lack of service use and take actions needed to improve these numbers. A lack of
natural supports has often been cited when persons are unsuccessful post-transition.
Competitive employment offers a strong natural support. A 2008 study published in the
Psychiatric Rehabilitation Journal reported that participants were able to describe a

15
variety of positive benefits associated with paid employment. They discussed ways in
which work fostered pride and self-esteem, offered financial benefits, provided coping
strategies for psychiatric symptoms, and ultimately facilitated the process of recovery.
(Dunn, Wewiorski, Rogers. ‘The meaning and importance of employment to people in
recovery from serious mental illness: results of a qualitative study’, Psychiatric
Rehabilitation Journal, 2008 Summer;32(1):59-62). Some barriers are known, such as
minimal employment opportunities in rural areas, and potential hesitancy of the client to
take on another environmental goal soon after moving. Possible recommendations for
improvement include:
1. Ensure widespread benefits counseling to persons who are transitioning or who
have transitioned. This will often require persons outside of the supported
employment program such as in-reach workers, case managers, and ACT team
members, to understand how employment impacts benefits, and to also promote
the positive personal benefits of employment.
2. Improve statewide access to IPS supported employment services, including
Lexington and its surrounding counties.
3. Highlight the role of employment in fostering recovery, and the importance of
revisiting the goal of employment with persons who have adjusted to their new
living environment.
Section III.E.1. Informed Decision Making
The Cabinet is to ensure that individuals residing in or at risk of entry into a PCH are
accurately and fully informed in writing, and signed by the individual, about the
community based options provided under the Settlement. This provision is rated Modest
to Substantial Progress due to improvements made in getting information to persons in
PCHs. DBHDID has created posters that are displayed in PCHs regarding the
Settlement, and some CMHCs initially distributed brochures about ACT services. There
has not been a process for obtaining client signatures to indicate they have been fully
informed in writing. A complicating factor for compliance with this provision is that the
necessary community based options are not available to some persons wanting to leave
PCHs. This is particularly true for those being discharged from state psychiatric
facilities. Hospital staffs have reported patients wanting to be discharged to community
housing with services, but the only option available to them is discharge to a PCH.
Section III.E.2. Cabinet Level team
This provision was Complete with the establishment early on, of the Cabinet Level
Transition team. The team meets approximately twice a quarter and includes the Cabinet
Secretary’s office, representatives from key Cabinet Departments and Offices, P&A, and
the Independent Reviewer.
Section III.E.3.a. Development of Materials

16
DBHDID has developed requirements and materials for in-reach and transition teams so
this provision is rated Complete. The Cabinet must monitor for needed revisions or
adjustments, as these procedures were put in place early in the Settlement.
Section III.E.3.b. On-going in-reach
The Cabinet is to ensure that ongoing in-reach is occurring in PCHs and in state
psychiatric hospitals. This provision is rated Substantial Process due to overall
improvement in the frequency of in-reach. There are several issues that complicate full
compliance with this provision. Not all CMHCs regularly provide in-reach to all of the
free standing PCHs in their area, nor in the Cabinet owned or operated psychiatric
hospital in their area. There are also issues with the effectiveness of in-reach in some
areas. Effective in-reach can be negatively impacted by:
the lack of services available to address clients’ presenting needs;
the in-reach workers lack of knowledge about supports, services, or the
Community Integration Supplement;
a lack of experience with clients’ positive change and growth as a result of
change in their environment;
the inability to recognize recovery potential; or
working within an agency that does not prioritize full community integration of
persons in this disability group.
Section III.E.3.c. Assignment to Transition Team
Persons who request community housing and services are to be assigned to a transition
team within 15 days of initial contact by the CMHC. The Time report on the Tracking
Tool indicates that this reporting quarter, only 15% of eligible referrals were assigned to
a transition team in 30 days or less. This parameter takes into account that the CMHC
has 14 days to make their initial contact once a referral is made for a total of 29 days
from the time of referral until assignment to the transition team. This provision is rated
Minimal to Modest Progress considering the current percentage of 15%, and the overall
percentage of reaching the benchmark over the life of the Settlement of 52%.
Section III.E.3.d. Communicating available options
The Cabinet is required to share the in-reach and education materials with P&A, DAIL,
the MCOs, and Clerks of Court to ensure guardians understand the options available to
individuals under the Settlement. This provision is rated Complete, although it is unclear
if, or how materials are shared with Clerks of Court.
Section III.E.3.e. P&A’s representation
State guardians, P&A, and case managers are to work together to find the most integrated
setting appropriate to meet individual needs. This provision is rated Substantial Progress.

17
Efforts have been made throughout the time of the Settlement to improve communication
and better coordinate efforts.
Section III.E.3.f. Transition within 90 days
Transition and discharge planning is to be complete within 45 days after assignment to a
transition team. The actual discharge is to be completed within 90 days of assignment to
the transition team. This results in a combined total of 119 days when adding the 14-day
time frame for making the first contact, the 15-day timeframe for assignment to a
transition team after making the first contact, and the 90-day timeframe to transition. The
Tracking Tool’s ‘Total Time to Transition’ report shows only 15% of transitions meet
this required timeframe for discharge. There are currently 105 on the list of persons who
have been waiting between 120 days and 1,460 days for transition. There are additional
persons not on this list of 105, whose guardians do not approve transition from a PCH, or
the individual is coded as ‘clinically inappropriate’ to move, for example. This provision
is rated Minimal. Locating housing in a timely manner is one barrier to achieving
compliance with this provision. Improvements can be made by more quickly pulling
together a transition team of all persons who will play a role in ensuring a successful
transition. A more responsive person-centered transition planning process, along with the
strengthening of relationships with private landlords and local housing authorities, can
help improve the timeliness of transitions.
Section III.F.1. Quality Assurance and Performance Improvement
The Cabinet is required to have a quality assurance and performance improvement
monitoring system to ensure placements and services are developed in accordance with
the Settlement; and to ensure that the individuals who receive Housing Assistance are
provided the services and supports they need for their health, safety, and welfare.
Services and supports are to be “of good quality and sufficient to help individuals achieve
increased independence, gain greater integration into the community, obtain and maintain
stable housing, avoid harms, and decrease the incidence of hospital contacts and
institutionalization”. This provision is rated Modest Progress, acknowledging the
processes the Cabinet has put in place to:
1. prioritize housing vouchers for persons under the Settlement;
2. maintain standards of housing quality through inspection by KHC;
3. implement and monitor the practice of person centered recovery planning;
4. monitor ACT, supported employment, and peer support staffing, including the
numbers served;
5. regularly meet with CMHC and hospital representatives to review persons waiting
more than 119 days to transition, and persons discharged from the hospital to
PCHs; and
6. conduct Quality of Life surveys pre-transition, 6 months post transition, and I year
post transition.

18
Improvements are needed in tracking whether or not there is greater access to safe,
affordable housing, and whether or not services are sufficient to obtain and maintain
stable housing.
Section III.F.2. Data for performance improvement
The Cabinet is required to collect, aggregate, and analyze data related to in-reach and
person-centered discharge and community placement efforts. The KY ISA Tracking
Tool has largely accomplished this. The tool also tracks persons who maintain
community tenure for 6 months and for 1-year post transition. This provision also
requires the identification of problems and barriers to placing and keeping individuals in
the community so that the Cabinet can review this information every 6 months, then
develop and implement measures to overcome those problems and barriers. This
information is currently not captured in a way that can inform performance improvement
actions. This provision is rated between Modest and Substantial Progress. The quality
assurance and performance improvement system must be able to inform actions
necessary to achieve the outcomes described in the Settlement.
Section III.F.3. Sharing of data
The Quality Assurance System is to be shared with P&A on at least a quarterly basis
unless requested sooner. This provision is rated Modest Progress. The Cabinet has been
responsive in getting the information they have to P&A, but is lacking in needed
information about improved housing access, the quality and sufficiency of services, the
problems that result in re-institutionalization, and the needed action steps to address
service gaps. This is the last substantive provision included in the Compliance with
Substantive Provisions Grid.
Section III.G.3. requires an accounting of the original expressers, indicating where they
are in the process of being transitioned from PCHs. There have been no reported changes
since last quarter. P&A reported speaking with 9 original expressers (including 1 who
transitioned then returned to a PCH) who want to leave the PCH they are in.
Since the start of the Settlement, Housing Assistance has been provided to 29 (including
4 potential plaintiffs) of the original 133 expressers. For these 29:
18 are still in housing
4 returned to a PCH
3 are deceased
2 to a nursing home
1 to a staffed resident
1 to family
Of the remaining 96:
12 died before transitioning 22 received ID/DD Supports for Community Living 10 went to nursing homes

19
7 could no longer be located 3 were deemed ineligible for services 6 were deemed clinically inappropriate, and 36 changed their original request to leave the PCH (or guardian intervened to
prevent them from leaving)
IV. SUMMARY/RECOMMENDATIONS
Several recommendations have been made throughout this report and do not need to be
repeated in this section. The Cabinet has expressed its desire to meet the terms of the
Settlement for the benefit of Kentuckians with psychiatric disabilities. This requires a
well-coordinated effort that will need to include sufficient service reimbursement, a
determination on how provider agencies can best be utilized, and a system that allows for
the funding of provider agencies based on the achievement of meaningful outcomes.
COMPLIANCE WITH SUBSTANTIVE PROVISIONS GRID
April 1, 2018
Ratings 4 - Complete – fully met as determined by Agreement
3 - Substantial Progress – progress by roughly 75%
2 - Modest Progress – progress by roughly 50%
1 - Minimal Progress – some progress made, approx. 25%
0 - No Progress – no progress made
Amended
Settlement
Agreement
Reference
Provision Rating
0-4
Rating What’s being monitored
III.A.1
Appropriate
Supports and
Services in the
Most
Integrated
Setting
The Cabinet will continue to
develop and implement
effective measures to provide
adequate and appropriate public
services and supports identified
through person centered
planning in the most integrated
setting appropriate to meet the
needs of individuals with SMI,
and who are residing in or at
risk of entry into a PCH.
2 Modest
Progress
The extent to which
services and supports
are adequate to meet the
needs of persons with
SMI in the most
integrated setting
appropriate, as
evidenced by persons
able to leave PCHs
and/or having
community options
other than PCHs.
III.A.2 All guardians shall receive
information from the Cabinet to
encourage their wards…to
participate to the maximum
3 Substantial
Progress
The extent to which all
guardians have
information from
Cabinet about allowing

20
extent of his/her abilities in all
decisions that will affect
him/her…including…treatment
discussions and discharge
planning…Any decisions made
by the guardian about where the
individual will live should
reflect the individual’s written
preferences, to the extent
possible.
wards to be a part of all
discussions/decisions
affecting them and that
decisions reflects the
preferences of the wards
Averaged score 2.5
III.B.1
Regulation
Cabinet agrees to promulgate a
new regulation encompassing
and further describing the
services and supports in the ISA
and this Settlement Agreement
prior to December 1, 2015.
4 Complete Existence of Regulation
filed Dec. 2, 2015 and
finalized June 3, 2016
Averaged score 4
III.C.1.2.
Community
Based
Supported
Housing
Assistance
Cabinet will develop and
implement measures to provide
individuals outlined in
III.C.2.a-c access to
community-based supported
housing.
2 Modest The extent to which
there is access to
supported housing and
access to state or federal
housing vouchers or
subsidies.
III.C.3. The Cabinet will provide
Housing Assistance to 150
individuals by Oct. 1, 2015; 350
individuals by Oct. 1, 2016; 600
individuals by Oct. 1, 2017; and
675 individuals by Oct. 1, 2018
3 Substantial
Progress
Achievement of
benchmark numbers.
Currently 80%
III.C.3. …with approximately half
given to state wards and half to
others
2 Modest
Progress
Achievement of
benchmark percentage.
Currently 22%
III.C.6,7
Housing is permanent with
Tenancy Rights; Tenancy
support services enable
residents to attain and maintain
housing; Services are available
but not a condition of tenancy;
Individuals with and without
disabilities have opportunities
to interact; Does not limit
ability to access community
activities; Scattered site housing
with no more than 25% of units
in development occupied by
3 Substantial
Progress
Extent to which housing
meets all specified
criteria.

21
individuals with a disability
known to the Cabinet; Choice
in daily life activities; Priority
of single-occupancy housing;
cannot be PCHs, group homes,
nursing facilities, boarding
homes, assisted living
residences, supervised living
settings, or any setting required
to be licensed. Averaged score 2.5
III.D.1.2.
Behavioral
Health
Services
Access to services and supports
which are evidence-based,
recovery-focused and
community-based; Flexible and
individualized; Help individuals
to increase their ability to
recognize and deal with
situations that may otherwise
result in crises; Increase and
strengthen individuals’
networks of community and
natural supports
2.0 Modest
Progress
Extent to which services
are accessible and meet
listed criteria, allowing
persons to live in
community-based
settings.
III.D.3. Community mental health
services of ACT teams, case
management services, crisis
services, peer support services,
and Supported Employment
Services
3 Substantial
Progress
Number of regions
providing all 5 services.
III.D.4. ACT teams meet fidelity 1 Minimal
Progress
Number of teams
achieving fidelity to
EBP and serving
persons under
settlement. Last fidelity
reviews showed 5 teams
at acceptable to good
fidelity.
III.D.5. Person-centered plans with
coordinating professional which
include psych. advance
directives and/or crisis plans
2 Modest
Progress
Evidence of person-
centered planning for
persons under
settlement. Small
sample sizes from 3
CMHCs averaged 40 out
of 52 possible points on
the Quality Indicator
Tool. All CMHCs have

22
received TA
III.D.6. Case management services
leading to goal achievement
3 Substantial
Progress
Case management
services sufficient to
support community
tenure.
III.D.7. Crisis service systems are
timely and accessible, crisis
services monitored and service
gaps are addressed, services are
in least restrictive setting.
2.5 Modest
Progress
Extent to which crisis
services are accessible
and extent to which
Cabinet monitors
service gaps.
III.D.8. Provision of peer support
services
3 Substantial
Progress
Number of regions
offering peer support
services to persons
under settlement
III.D.9. Will develop and implement
measures to provide Supported
Employment with fidelity to
IPS
2.5 Modest
Progress
Number of programs
meeting fidelity and
serving persons under
settlement. Averaged score 2.38
III.E.1.
Discharge and
Transition
Process
Individuals are accurately and
fully informed in writing and
signed by individual about
community-based options
2.5 Modest
Progress
Evidence of the extent
to which persons are
fully informed about
community-based
options available to
them under the
Settlement.
III.E.2. DBHDID will create an overall
transition team at the Cabinet
level which will provide
oversight and assist local
transition teams in overcoming
identified barriers to transition
4 Complete Cabinet level team
formed
III.E.3.a. DBHDID will develop
requirements and materials for
in-reach and transition
coordinators and teams.
4 Complete Requirements and
materials may need
revisions over time.
III.E.3.b. DBHDID will ensure on-going
in-reach to individuals in PCHs
and Cabinet owned and
operated psychiatric hospitals
for individuals meeting
requirements of Amended
Agreement.
3 Substantial
Progress
Extent to which regular,
effective in-reach occurs
in all free-standing
PCHs and state
psychiatric hospitals
III.E.3.c. Within 15 days of initial
contact, individuals who have
indicated they do not want to
1.5 Minimal
Progress
For this reporting
quarter, the benchmark
was met 15% of the

23
receive services in a PCH shall
be assigned to a transition team.
time. The overall
percentage for all
quarters is 52%
III.E.3.d. P&A, DAIL, Clerks of Court
receive in-reach and education
materials to ensure guardians
understand options available to
individuals
4 Complete Has occurred, but must
continue
III.E.3.e. State guardians will cooperate
with P&A and CMHC case
managers in finding the most
integrated setting and allow
P&A to represent wards
3 Substantial
Progress
Level of cooperation
among state guardians,
P&A, and CMHCs in
finding the most
integrated setting and
accessing services.
III.E.3.f. Transition and discharge
planning completed within 45
days of assignment to transition
team. Discharge if appropriate
will occur within 90 days of
assignment to transition team.
1 Minimal
Progress
90 day benchmark + 29
days. Overall 20%
completed within 119
days (12% this quarter)
Averaged score 2.88
III.F.1. Cabinet will develop and
implement a quality assurance
and performance improvement
monitoring system to ensure a
quality service system sufficient
to help individuals achieve
increased independence, gain
greater integration into the
community, obtain and
maintain stable housing, avoid
harms, and decrease the
incidence of hospital contacts
and institutionalization.
2 Modest
Progress
Implementation of a
quality assurance and
performance
improvement
monitoring system for
service quality and
effectiveness.
III.F.2. Collect, aggregate, and analyze
data related to in-reach and
person-centered discharge and
community placement efforts
(successful and unsuccessful
placements, problems/barriers
to integration). Review semi-
annually and develop and
implement measures to
overcome barriers
2.5 Modest
Progress
Extent to which data
identifies
problems/barriers to
integration and
measures are
implemented to
overcome barriers.
III.F.3. Quality Assurance System
information will be shared with
2.5 Modest
Progress
Availability of
performance

24
P&A quarterly unless requested
sooner
improvement data.
Averaged score 2.3
Overall average 2.76