Session 5: Niche brokering: finding new users for …Slide 1 Session 5: Niche brokering: finding new...
26
Slide 1 Session 5: Niche brokering: finding new users for old knowledge How Personalized Healthcare May Bring New Life to Failed Drugs OECD Expert Workshop on Knowledge Markets in Life Sciences National Academies of Science Washington, D.C. 16-17 October 2008
Transcript of Session 5: Niche brokering: finding new users for …Slide 1 Session 5: Niche brokering: finding new...

Slide 1
Session 5: Niche brokering: finding new users for old knowledge
How Personalized Healthcare May Bring New Life to Failed Drugs
OECD Expert Workshop on Knowledge Markets in Life SciencesNational Academies of Science
Washington, D.C.16-17 October 2008
2
Personalized Healthcare
Generating meaningful segmentation of patient populations, by whatever technology is appropriate (genomic, imaging, informatic), in order to increase the benefit of therapy

3
Everybody responds to therapy differently
Who suffers when therapies don’t work?
Patients
Physicians
Payers
Percentage Non-responders
4
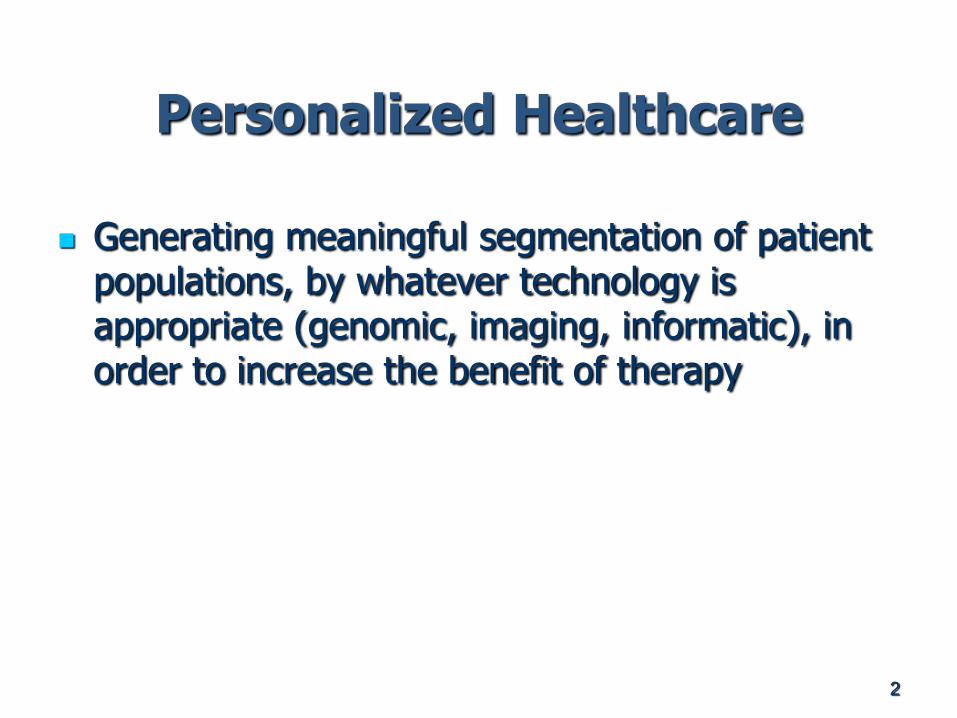
Targeted Clinical Trials
Estimated that drug companies could save up to $100’sM per drug by incorporating pharmacogenomics data into trials
Trials terminated early due to success in a genetically defined subset of breast cancer patients Interim analysis yielded
statistically significant results, exceeding the primary endpoint
5
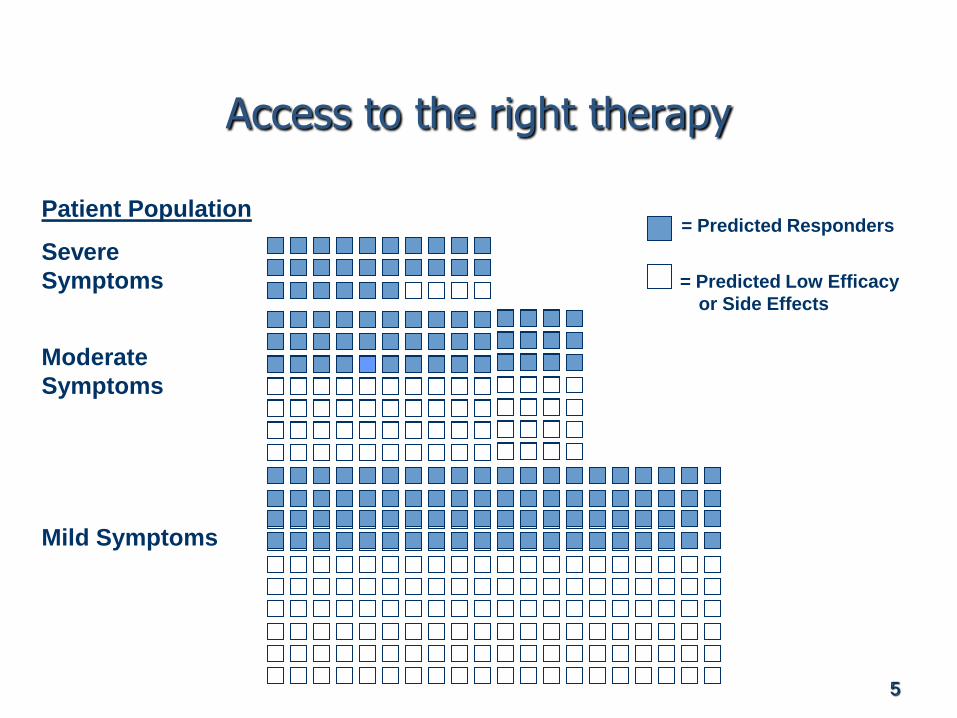
Access to the right therapy
Severe
Symptoms
Moderate
Symptoms
Mild Symptoms
Patient Population= Predicted Responders
= Predicted Low Efficacy
or Side Effects

6
Quicker uptake of therapeutic value
Arimidex vs. Herceptin: Global Sales from launch
0
500
1,000
1,500
2,000
2,500
3,000
3,500
Year
1
Year
2
Year
3
Year
4
Year
5
Year
6
Year
7
Year
8
Year
9
Year
10
Year
11
Year
12
$m
Traditional
PHC
TASCO presentation of
adjuvant data (May 05)
Adjuvant approval
EMEA May 06, US
FDA Nov 06
Initial adjuvant
indication in US
5 year analysis of
ATAC data
Breast Cancer Therapies: Global Sales from Launch

7
Towards Preventive Medicine
Avoiding futile medicine
Predictable therapeutic response
Earlier intervention
Delay onset and minimize severity

8
Rescue Strategies
The Good: Herceptin/Herceptest
The Bad: Herceptin/Herceptest
The Ugly: Herceptin/Herceptest
The Really Ugly: Iressa

9
The Good - Herceptin
Large responder effect in pivotal trials
FDA will not approve without Dx
Genentech develops IHC (Immunohistochemistry) with Dako
Receives approval and launches Herceptin/Herceptest
First blockbuster Personalized Therapy
Arimidex vs. Herceptin: Global Sales from launch
0
500
1,000
1,500
2,000
2,500
3,000
3,500
Year
1
Year
2
Year
3
Year
4
Year
5
Year
6
Year
7
Year
8
Year
9
Year
10
Year
11
Year
12
$m
Traditional
PHC
T
ASCO presentation of
adjuvant data (May 05)
Adjuvant approval
EMEA May 06, US
FDA Nov 06
Initial adjuvant
indication in US
5 year analysis of
ATAC data
Breast Cancer Therapies: Global Sales from Launch

10
The Bad - Herceptin
Genentech develops second test based on FISH (fluorescence in situ hybridization) with Vysis (now Abbott Molecular)
But: According to guidelines released by ASCO and the College of American
Pathologists, analyses of prospective, randomized, adjuvant trials of Herceptin show that testing algorithms to gauge HER2 expression have not been standardized and were developed “somewhat arbitrarily.”
An expert panel found “as many as 15 percent to 20 percent of the HER2 assays performed in the field may be incorrect when the same specimen was reevaluated in a high-volume, central laboratory.”
“Current testing methods for determination of the likelihood of benefit from Herceptin are not adequate,"
Third test, CISH (Chromogenic In Situ Hybridization), now available from Invitrogen
New test in the works from Monogram based on a proximity-based assay

11
The Ugly - Herceptin
Herceptin and HER-2 tests are reimbursed separately
Use of the HER-2 tests is not required by the label
Poor reliability and reduced trust in the HER-2 tests results in poor use of the tests by oncologists
Adverse (ultimately overturned) cost-effectiveness decision by NICE on use of Herceptin without HER-2 testing

12
The Really Ugly - Iressa
Iressa shows high levels of efficacy against non-small cell lung cancer in early trials
Very clear responder population in pivotal trials results in very limited label
AstraZeneca retracts the drug for all but compassionate use
Two academic labs suggest a role for EGFR in predicting drug response for Iressa and Tarceva
Iressa becomes the poster child for linked RxDx
But biological complexity rears its ugly head… Subsequent research indicates EGFR positivity doesn’t predict for
drug response, that the biology is much more complicated
Still no predictive test for Iressa

13
The Lesson – Herceptin/Iressa
Assuming the biology works:
No standards for sensitivity/specificity of Dx tests linked to therapeutics
Coverage/reimbursement decisions by public payers for new generation Dx, much less RxDx, antiquated and don’t provide ROI for clinical utility
Private payers want demonstration of clinical effectiveness
FDA indicating it will regulate this space
Business model for new generation Dx may be untenable
Could the Herceptin story replay today? Possibly
Could the Herceptin story replay tomorrow? Probably not
Retrofits of a Dx to a developed Rx are hard, start early

14
The PHC Landscape Today
PM has broad support but
will require changes in
how personalized
technologies are
evaluated, how health care
is financed and delivered,
and how clinicians and
consumers are prepared
Policy-makers,
researchers and
developers of PM
interventions need to
develop strategies to
overcome barriers to
clinical integration
Multi-stakeholder
collaborations, including
public-private
partnerships, will be
required
Stakeholders require
extensive and on-going
education in PM, in
particularly the
payer/purchaser
community and health
care delivery
organizations/providers
Source: Duke/ABT/PMC Landscape Analysis
15
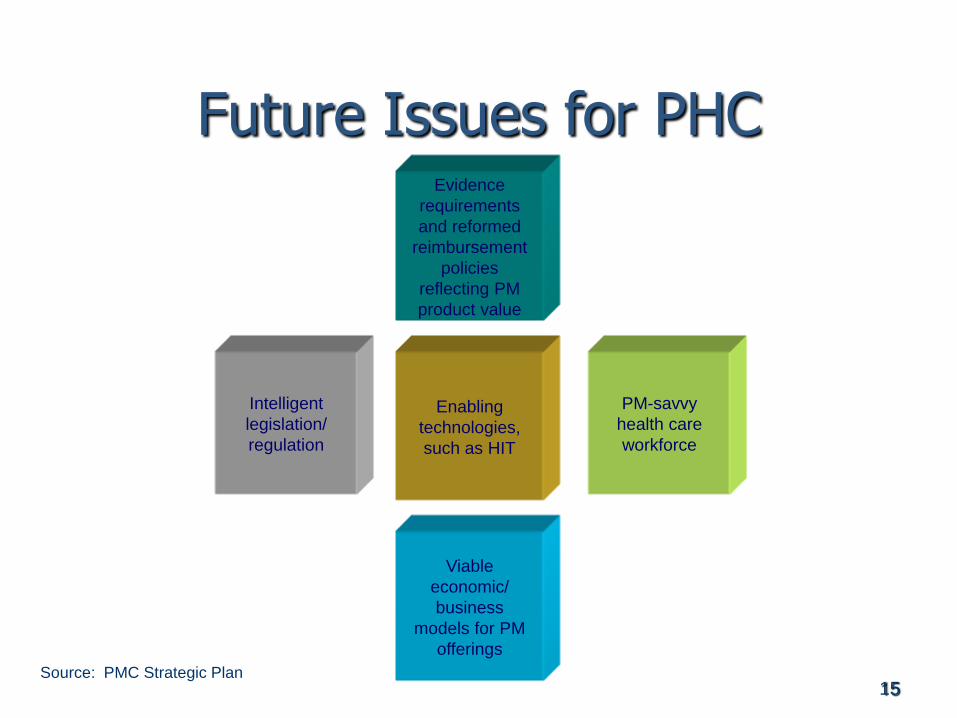
Future Issues for PHC
Intelligent
legislation/
regulation
Viable
economic/
business
models for PM
offerings
Evidence
requirements
and reformed
reimbursement
policies
reflecting PM
product value
PM-savvy
health care
workforce
Enabling
technologies,
such as HIT
Source: PMC Strategic Plan

16
Repurposing Old Knowledge Informatic PHC
Can a large and fully integrated Electronic Health Record System (EHR) be used to demonstrate the value of antidiabetic therapy, in terms of comparative benefit and risk, in an environment reflecting actual clinical use of the therapy?

17
Cohort
>18 years old
Diagnosis of Diabetes in EHR.
Prescribed single oral hypoglycemic Agent.
– Patients with the metabolic syndrome and polycystic
ovarian syndrome excluded
– Patients on AGI excluded (n=146)
Baseline = Earliest Date of Hypoglycemic RX in
a diabetic patient.
Pts without follow-up were censored for all
outcomes except mortality.

18
Predictors
Measurements: Lipids, BMI, BP, LVEF, Hba1c,
eGFR, LFTs, Alb:Cr
Medical History: CHF, Liver Disease, Kidney
Disease, CAD, Stroke/TIA, Hepatitis B/C, Atrial
Fibrillation, New Diabetic?
Demographics: Age, Gender, Race
Oral Hypoglycemic Medication Class:
Meds: ACE / ARB, Cholesterol, ASA, Plavix
19
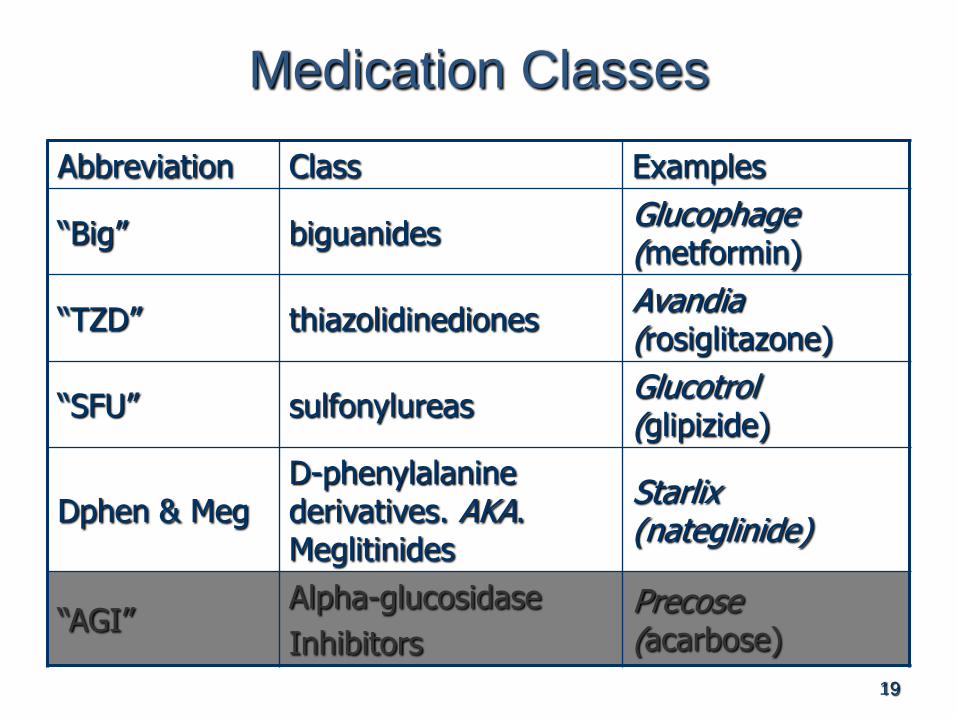
Medication Classes
Abbreviation Class Examples
“Big” biguanidesGlucophage (metformin)
“TZD” thiazolidinedionesAvandia (rosiglitazone)
“SFU” sulfonylureasGlucotrol (glipizide)
Dphen & MegD-phenylalanine derivatives. AKA. Meglitinides
Starlix (nateglinide)
“AGI”Alpha-glucosidase
Inhibitors
Precose (acarbose)

20
Outcomes
Nephropathy
Renal Insufficiency
Mortality
Coronary Artery Disease
Stroke/TIA
Liver Injury
Heart Failure
Continuous Outcomes: BMI, Hba1c, LDL, HDL, TG.

Anil Jain, MD Copyright 2007, Cleveland Clinic
Clinical Data
Repository
CCF DM
Data Set
Creating the Data Set…
CCF DM
Definitions
Social Security
Death Index
CCF has utilized an EHR since 2000.
EHR Tethered PHR ePrescribing Large Clinical Data
Repository 3.5 million patients 5 million prescriptions 89 million laboratory
results
Scope of Data Medications Demographics Diagnoses Procedures Laboratory Imaging

22
Conclusions
Successful use of the EHR to predict outcomes in type II diabetes
Models are very good at predicting clinical outcomes
Models for predicting continuous outcomes are better than simply relying on baseline alone.
Interactions allow for tailored treatment beyond AHRQ recommendations.
Potential to extend these techniques to other diseases.
23

24
Repurposing Old Knowledge for:Better understanding of the structure and interactions in
Clinical and Translational Science…STEM-01: Genetic medicine
STEM-02: Female
reproductive cell
biology STEM-03: Vascular disease
& control of cell proliferation
STEM-04: Controls
in early developmentSTEM-05: Gene
and cell therapy
STEM-06: Stem
cell therapy
STEM-07: Control
of hematopoiesis
STEM-08: Cell transplantation
& Tissue regeneration
STEM-09: Genetic
control of cell
differentiation
STEM-10: Diabetic
cell therapy
STEM-11: Molecular biology
of cell differentiation
STEM-12: Signaling
pathways in cell differentiation
STEM-13: Early development
and organ differentiation
STEM-14: Neural
regeneration
Stem Cell Science

25
Repurposing Old Knowledge for:Distinctive Competencies for Clinical and Translational Science
-omic understanding of disease

Slide 26
Thank-you
Wayne A. Rosenkrans, Jr., Ph.D.
Distinguished Fellow, MIT Center for Biomedical Innovation
Chairman & President, Personalized Medicine Coalition
Chief Applications Officer, SciTech Strategies




![Finding a Niche Report 2014 · Niche [nich] noun: a distinct segment of a market. In a nutshell, niche marketing involves serving one part of a market, not just promoting a single](https://static.fdocuments.net/doc/165x107/5f8910486b11cd717420fb84/finding-a-niche-report-2014-niche-nich-noun-a-distinct-segment-of-a-market-in.jpg)